Back to Journals » Psychology Research and Behavior Management » Volume 16
Exploring the Relationship Between Intolerance of Uncertainty and Trust in Physicians from Spousal and Parent-Child Perspectives
Authors Gao P, Wu H ![]() , Fan Z
, Fan Z ![]() , Tao M
, Tao M ![]()
Received 11 April 2023
Accepted for publication 16 May 2023
Published 13 June 2023 Volume 2023:16 Pages 2173—2186
DOI https://doi.org/10.2147/PRBM.S413821
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mei-Chun Cheung
Peng Gao,1 Hanwei Wu,2 Zhiguang Fan,3 Min Tao4
1Department of Chinese Medicine, Changchun University of Chinese Medicine, Changchun, Jilin, People’s Republic of China; 2Department of Foreign Studies, Hunan Normal University, Changsha, Hunan, People’s Republic of China; 3Department of Psychology, School of Teacher Education, Shaoxing University, Shaoxing, Zhejiang, People’s Republic of China; 4Department of Education, Jilin International Studies University, Changchun, Jilin, People’s Republic of China
Correspondence: Zhiguang Fan, Department of Teacher Education, Shaoxing University, No. 900, Chengnan Avenue, Shaoxing, Zhejiang, 312000, People’s Republic of China, Tel +86-0431-84924101, Fax +86 1 594-831-4623, Email [email protected]
Objective: The present study aimed to probe the intergenerational transmission of intolerance of uncertainty (IU) and trust in physicians. Besides, through the actor-partner interdependence model (APIM), the predictive effect of parents’ IU on their own and their spouses’ trust in physicians was examined. A mediation model was further constructed to probe the mechanisms by which parents’ IU affects children’s trust in physicians.
Methods: The Intolerance of Uncertainty Scale-12 (IUS-12) and the Wake Forest Physician Trust Scale (WFPTS) were employed to conduct the questionnaire survey among 384 families (each family with a father, mother, and one child).
Results: IU and trust in physicians were found to be intergenerationally transmitted. The results of the APIM analyses showed that fathers’ total IUS-12 scores negatively predicted their own (β = − 0.419, p < 0.01) and mothers’ (β = − 0.235, p < 0.01) total WFPTS scores. Mothers’ total IUS-12 scores negatively predicted their own (β = − 0.353, p < 0.01) and fathers’ (β = − 0.138, p = 0.017) total WFPTS scores. The results of mediation analyses indicated that parents’ total WFPTS scores and children’s total IUS-12 scores mediated the effect of parents’ total IUS-12 scores on children’s total WFPTS scores.
Conclusion: The public’s IU is a crucial influencing factor of their trust in physicians. Besides, the IU between couples and between parents and children could be mutually affected. On the one hand, husbands’ IU could affect their own and their wives’ trust in physicians, and vice versa. On the other hand, parents’ IU and trust in physicians could affect their children’s IU and trust in physicians, respectively.
Keywords: intolerance of uncertainty, trust in physicians, intergenerational transmission, the actor-partner interdependence model, mediation analysis
Introduction
Currently, a severe trust crisis has existed in the healthcare field, taking the form of mistrust between physicians and the public.1,2 In the past decade, Chinese public trust in physicians has continued to decline, posing a great threat to the achievement of healthcare system reform. In a national survey, the proportion of the Chinese public reported to trust or strongly trust physicians reached 83.4% in 2011, while it decreased to 64.2% in 2016.3 A latest national survey in China indicates that 57% of the Chinese public strongly trusted physicians.4 Trust in physicians is associated with people’s confidence in physicians’ professionalism and motivation for treating patients, as well as people’s expectations of and faith in physicians’ actions for protecting patients’ interests.5 A paucity of trust in physicians can trigger reduced satisfaction with medical services,6 frequent medical conflicts,7 and even violence against healthcare workers.8
The factors affecting public trust in physicians can be roughly divided into three aspects: the characteristics of trustors (patients), the characteristics of trustees (physicians) and interpersonal interaction. The characteristics of trustors are mainly dependent on their general trust, medical history, and prior knowledge.9 For instance, people with good public health literacy generally show higher trust in physicians’ diagnosis, advice, and treatment.10 The characteristics of trustees comprise physicians’ professionalism,11 as well as factors beyond technical competency such as physicians’ empathy,12 communication, fairness, honesty, and confidentiality.13 Interpersonal interaction refers to physician-related information obtained by individuals through interpersonal communication. For instance, the public seeking health information or comments on physicians on the Internet can affect their trust in physicians.14 Besides, as the main channel for social interaction, media coverage can also largely affect public trust in physicians.15
According to previous literature, trust in physicians can be categorized into interpersonal trust and general trust.16 Interpersonal trust refers to patients’ trust levels in their physicians in an established and specific physician-patient relationship. General trust comes to public trust in the whole group of physicians, not in a particular physician. Interpersonal trust is mainly derived from the direct experience acquired by patients during their diagnosis and treatment.17,18 In addition to direct experience, general trust is also influenced by medical policies, family members, friends, or media reports.19,20 Everyone is likely to be a patient because of illness. Public trust in physicians is salient in the formation of patients’ trust in their physicians during treatment. It’s noteworthy that public trust in physicians may differ from patients’ trust in physicians. A study indicated that American public trust in physicians was declining year by year, while patients’ trust in physicians remained relatively stable at a high level.21 The same conclusion was also drawn in the research on Chinese public trust in physicians.3
The present study was with the purpose to probe the effect of IU on trust in physicians and analyzed the mutual effect between couples and the effect of parents on children. Specifically, drawing on the cognitive model of pathological worry, we first investigated the relationship between IU and trust in physicians. Besides, according to the family systems theory, we discussed the intergenerational transformation of IU and trust in physicians.22 Moreover, drawing on the APIM, we probed the effect of parents’ IU on their own and their spouses’ trust in physicians.23 With the above-mentioned explorations, we further constructed a mediation model to have insights into the effect of parents’ IU on their children’s trust in physicians, and the mediating roles of parents’ trust in physicians and children’s IU.
Relationship Between Intolerance of Uncertainty and Trust in Physicians
Individuals’ trust in physicians is also affected by their own health condition and cognition, among which intolerance of uncertainty (IU) is considered as one of the factors predicting individuals’ trust in physicians.24 IU is defined as a dispositional trait caused by negative attitude toward uncertainty and its consequences, which refers to the propensity to negatively respond to uncertain events.25 Uncertainty of medicine not only shows in the development of medical models, treatment, and concepts, but also in the complexity of illness, the limitations of cognition, and the change in the disease spectrum. In most cases, physicians can hardly give an unambiguous and specific explanation of the etiology, diagnosis, treatment, and prognosis of the illness.26 This uncertainty may lower patients’ and their relatives’ trust in and satisfaction with physicians.27
The cognitive model of pathological worry assumes that IU is crucial in the occurrence and maintenance of worry.28 Uncertain situations and events can usually bring nervousness, anxiety, and stress, subsequently leading individuals to pathologically worry about possible negative results.29 Individuals with high IU have the propensity to pay extra attention to uncertain information, consider uncertain situations as hazardous, and anticipate the results being disastrous.30 They also show inclination to view unpredictable events as unfair and questionable.31 This may cause people’s deficient confidence in physicians’ professionalism, doubt about the reasonability of treatment, and even suspicion of the authenticity of diagnosis.32 Accordingly, we extrapolated that IU could negatively predict trust in physicians.
Intergenerational Transmission of Intolerance of Uncertainty and Trust in Physicians
Family systems theory posits that one’s character traits, behavior patterns, psychological quality, and judgment are largely affected by his parents.22 Parents’ personality traits usually have a great predictive effect on their children’s, which may lead to children sharing similar IU and trust with their parents.33 Generally, the characteristics of parents can greatly predict the characteristics of children.33 In China where familism is ingrained, intergenerational transmission is particularly salient.34 Parents’ trust in physicians can affect children’s trust in physicians by means of intergenerational transmission. Family members’ attitude and evaluation are crucial source of individuals’ prior knowledge about physicians.35 Parents’ negative healthcare experiences, dissatisfaction with and grumbles about physicians can cause children’s doubt on and mistrust in physicians.36 Besides, in addition to patients’ past misdiagnosis experiences, other family members’ misdiagnosis experiences can decrease children’s trust in physicians.37 Hence, trust in physicians probably can be intergenerationally transmitted.
A spectrum of studies have demonstrated the intergenerational transmission of IU.38 For instance, the attitude of different family members toward uncertainty of illness can be mutually affected.39 High-IU parents’ negative emotional experience and behavioral reaction in dealing with uncertain events may cause children’s low tolerance of uncertain information.40 Parenting refers to a kind of relatively stable behavioral style exhibited in the process of parents raising and educating their children.41 According to previous literature, parents with high IU are prone to adopt negative parenting styles like treating their children harshly and highly harshly, which probably decreases children’s tolerance of uncertain information.42 If parents show limited love and warmth to their children, and rearing their children in a negative parenting style such as frequently criticizing and controlling their children, children’s sense of controllability and self-efficacy would be impaired, and then their excessive worry and their repugnance and avoidance of uncertain events might be triggered. In addition, children tend to regard their parents as role models for learning43,44 and gradually learn similar characteristics by observing and learning their parents’ emotional reactions and behavior styles when dealing with uncertain events.45 For instance, Gioia found that parents’ IU can indirectly affect daughters’ IU with daughters’ psychological distress as the mediator.46 In addition to parenting styles and observational learning, genetic factors may also be one of the reasons for the similarity in IU between parents and their children.47 For example, insula is closely linked to uncertainty and anxiety.48 In the uncertain context, the activation of a person’s insula can enhance his detestation of uncertainty.49 Therefore, we inferred that parents’ IU could positively predict children’s IU.
APIM Analysis of Intolerance of Uncertainty and Trust in Physicians
The family systems theory assumes that family is comprised of three subsystems: marital (or couple), parental, and sibling. Among them, marital relationships underlie parental and sibling relationships.50 As a closely linked whole, couples are highly interdependent on each other in terms of cognition and behavior.51 Besides, fathers and mothers cooperatively rather than independently raise their children.52 In most cases, couples mutually influence each other, and jointly affect the psychology and behavior of their children.53 Spousal and parent-child relationships are typical dyadic relationships in which one party’s psychological quality and behavioral pattern can affect their own and another party’s outcome variables. Therefore, the interdependence between family members should not be neglected in analyzing the associations between IU and trust in physicians from the familial perspective. As such, we employed actor-partner interdependent model (APIM) to investigate the reciprocal effect between spouses. The APIM is a theoretical framework designed for analyzing dyadic relationships (namely, committed and intimate two-person relationships) such as leader-follower and parent-child relationships, in which actor and partner effects are distinguished.23 In the present study, the actor effect describes the effect of one party’s IU on his or her own trust in physicians, while the partner effect represents the trust in physicians of one party affected by another party’s IU. The family systems theory considers a family as one whole system in which the members are interrelated and interacted. In other words, family members show strong interdependence. As such, based on the family systems theory, we adopted the APIM to explore the effect of couple’s IU on their own and their spouses’ trust in physicians.
The APIM has been extensively used in the research on marriage and family fields.54 Previous studies found that patients’ negative coping approaches are positively connected with their own and their spouses’ anxiety and depression.55 The interaction between couples’ uncertainty of illness and life quality has also been proved in the longitudinal research.56 However, hitherto, no study has employed the APIM to investigate the impact of couples’ IU on their trust in physicians. We hypothesized that husbands’ IU not only could negatively predict their own trust in physicians (the actor effect) but also their wives’ trust in physicians (the partner effect), and vice versa.
Gaps in Existing Literature and Establishment of Current Hypotheses
A further analysis of the factors and mechanisms affecting trust in physicians is of great significance to improve physician-patient relationship and promote the achievement of healthcare system reform. It’s noteworthy that the public are potential patients, since everyone may become a patient for suffering from disease. Public trust in physicians can affect their behaviors in seeking medical advice, which is also a crucial influencing factor of physician-patient relationship.9 Previous studies on the factors influencing trust in physicians mainly took patients as participants,20 hence neglecting the different features shared by patients’ and public trust in physicians.57 At present, a few studies have probed the factors affecting general population’s trust physicians.50 Therefore, the present study set family as the fundamental unit and examined the effect of parents’ IU on children’s trust in physicians by constructing a mediation model on the basis of the analysis of the intergenerational transmission of IU and trust in physicians, as well as the effect of parents’ IU on their own and spouses’ trust in physicians. The findings could help better understand the influencing factors of public trust in physicians from the familial perspective.
To sum up, IU and trust in physicians are closely associated and intergenerationally transmitted, but scant studies have investigated these variables among the public. As such, the present study aimed to explore the relationship between IU and trust in physicians from spousal and parent-child perspectives among the public to provide theoretical references for the relevant studies. Specifically, according the analysis of the existing literature, we hypothesized: (1) IU could negatively predict trust in physicians; (2) IU could be intergenerationally transmitted; (3) trust in physicians could be intergenerationally transmitted; (4) couples’ IU could predict their own and their spouses’ trust in physicians. Based on the analysis of the relationship between IU and trust in physicians as well as the intergenerational transmission, we hypothesized: (5) parents’ IU could influence their children’s IU through intergenerational transmission, and then children’s IU could influence their own trust in physicians; (6) parents’ IU could influence their own trust in physicians, and then their trust in physicians could influence their children’s trust in physicians through intergenerational transmission. After analyzing the APIM and the intergenerational transmission, we further hypothesized: (7) parents’ IU could negatively predict their spouses’ trust in physicians, and parents’ trust in physicians could influence their children’s trust in physicians through intergenerational transmission.
Materials and Methods
Study Design and Participants
College students were recruited for this study by the advertisement placed in two colleges. The inclusion criteria are as follows: (1) age≥18; (2) participants were voluntary for the survey; (3) parents were not divorced; (4) parents agreed to participate in the survey; (5) participants had no serious mental illness in recent three months; (6) participants did not experience serious traumatic events in recent three months. In the demographic information questionnaire, three statements were set to examine whether participants had serious mental illness or experienced serious traumatic events in recent three months. The three statements were: “In recent three months, I have been diagnosed with serious mental illness”, “In recent three months, I have taken drugs to treat mental illness”, and “In recent three months, I have experienced serious traumatic events”. If participants responded “yes” to any of the above statements, they would be excluded. The survey was conducted through the Internet. Before the survey, participants carefully read and signed the informed consent in which the purpose and procedure of the survey and the anonymity and confidentiality of the data were detailed. The study protocol complied with the Declaration of Helsinki. Ethical approval for the present study was obtained from the Ethics Committee of Jilin International Studies University.
The questionnaire comprised the children-report version and the parents-report version. College students were required to complete the children-report version and send the link of the parents-report version to their parents. A code was given to each family for data matching. Four hundred and eighty-three college students were recruited in the present study. The criteria for removing invalid data are as follows: (1) the data could not be matched; (2) the data from one parent was missing; (3) the response time was too short (less than 2 SDs; SD represents standard deviation, and similarly hereinafter), or too long (more than 2 SDs);58,59 (4) positive and negative items were reacted to identically. With the criteria, we collected 462 valid children-report questionnaires, 401 valid father-report questionnaires and 436 valid mother-report questionnaires. Finally, we collected 367 questionnaires valid in both parents and children.
The description of participants is presented in Table 1. Specifically, 257 families resided in the city, and 110 resided in the countryside. 120 families had relatives as medical practitioners, and 247 had not relatives as medical practitioners. In the sample of children, participants were aged from 18 to 23 (Mean ± SD=19.25 ± 1.03) with 134 males and 233 females. In the sample of fathers, participants were aged from 40 to 58 (Mean ± SD=47.54 ± 4.01). In the sample of mothers, participants were aged from 38 to 58 (Mean ± SD=46.12 ± 4.09).
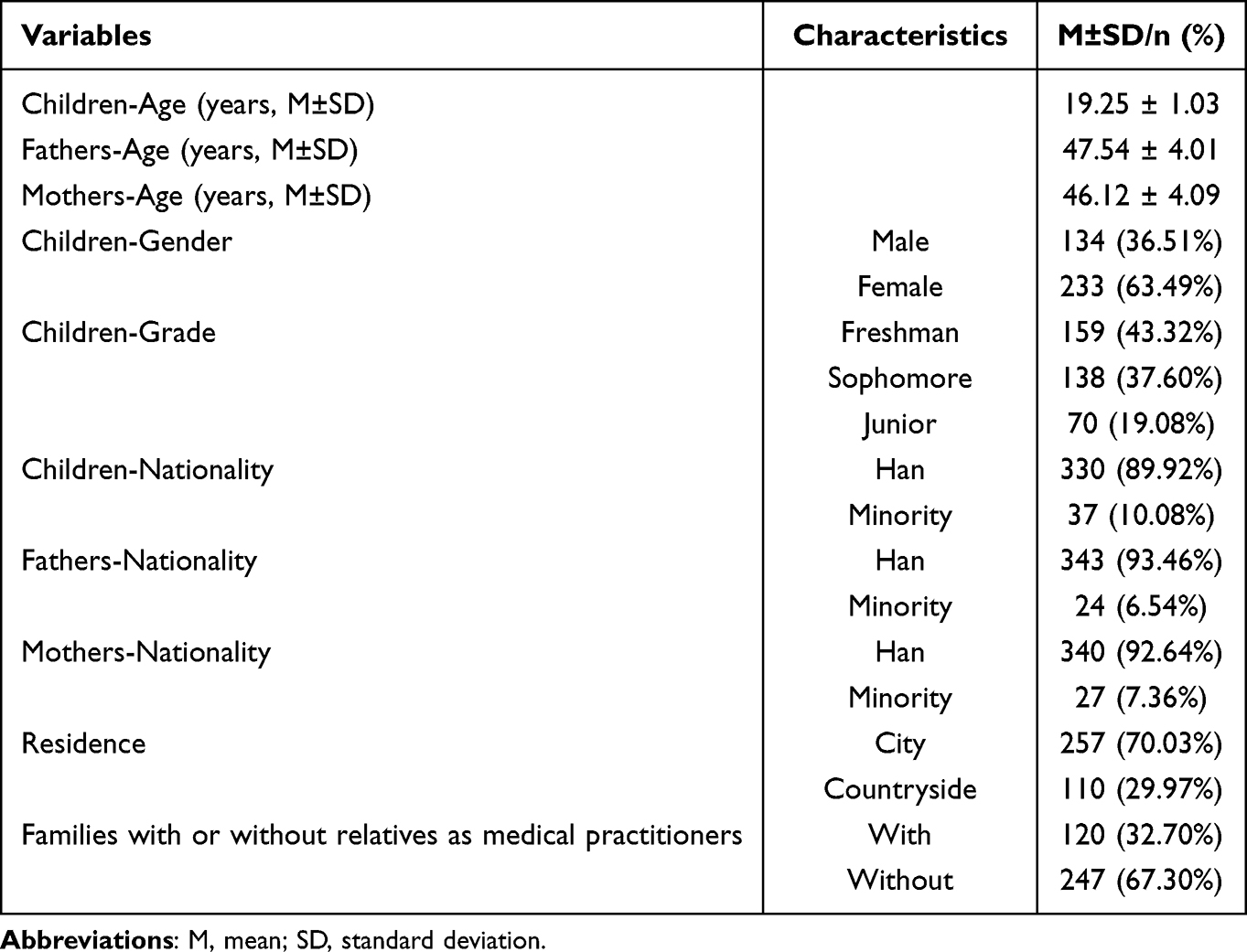 |
Table 1 Description of Participants (n=367) |
Instruments
Intolerance of Uncertainty Scale-12 (IUS-12)
The IUS-12 was developed by Carleton et al, comprising 12 items subsumed into 2 dimensions: prospective anxiety and inhibitory anxiety.25 All items are responded on a Likert scale from 1 (not at all) to 5 (entirely). In other words, individuals who scored higher showed lower tolerance of uncertainty. The Chinese IUS-12 has great reliability and validity.60 The Chinese IUS-12 is identical to its English counterpart in item number and content, but different in the naming of dimensions. In the Chinese IUS-12, the two dimensions are named anticipatory anxiety and debilitating anxiety, respectively. In the present study, the Cronbach’ s α in the sample of fathers, mothers and children were 0.93, 0.92 and 0.93, respectively.
Wake Forest Physician Trust Scale (WFPTS)
The WFPTS is developed by Hall et al, including 10 items, and all items are rated on a Likert scale from 1 (strongly agree) to 5 (strongly disagree).36 This scale is initially for evaluating patients’ trust in physicians, with the statements such as “For sake of my health, my doctor will do whatever I need”. In the present study, “I” in the items were substituted by “patients” so that the scale could be applied to assess public trust in physicians. For instance, the above item was changed into “For sake of patients’ health, physicians will do whatever patients need”. Katz found that the WFPTS showed satisfactory psychometric properties among general population older than 18.61 In other words, individuals who scored higher indicated higher trust in physicians. In the present study, the Cronbach’ s α in the sample of fathers, mothers and children were 0.87, 0.88 and 0.87, respectively.
Data Analysis
SPSS 26.0 was utilized for data analysis. Since the present study mainly aimed to explore the relationship between the IU and trust in physicians of parents and children, we only focused on the total IU and WFPTS scores of parents and children instead of probing the relationship between diverse dimensions when analyzing the correlations, integrational transmission, APIM, and mediation effects. Considering the strong interdependence between family members, the data collected from all participants were not independent. Hence, we employed linear mixed effects models in which the family-level intercept is entered as a random effect to examine the predictive effect of parents on children. In the mixed linear regression analysis, we set the sex of children (0=male, 1=female), residence (0=urban, 1=rural), and whether there are medical workers in relatives (0=none, 1=yes) as covariates.
APIM_SEM, an online free application was employed to test the APIM.62 The analyses used structural equation modeling (SEM) with maximum likelihood estimation using the R package lavaan.63 The APIM of the impact of parents’ IUS-12 scores on their own and their spouses’ WFPTS scores was constructed. There are three general dyadic patterns, namely, the actor-only, the couple, and the contrast patterns. As the ratio of the partner effect to the actor effect, k values were utilized to assess dyadic patterns.23 K values can be calculated with the prerequisite of the actor effect’s standardized values statistically significant and higher than 0.10. The analysis of the APIM mainly refers to three steps. Firstly, parents’ actor and partner effects should be computed. Their actor and partner effects are set as the same so that a comparison between the restricted model and the unrestricted model can be performed to test whether the actor and partner effects can be distinguished.64 Δχ2>0.20 suggests that the effects of fathers and mothers are equal, so as to test them as distinguishable dyads in the following analysis. Δχ2>0.20 suggests to test them as indistinguishable dyads in the following analysis.23 Secondly, the dyadic pattern of fathers and mothers should be figured out. Using 5000 bootstrap resamples, the confidence interval (CI) for k values is calculated. Specifically, the CI including 0 indicates the actor-only pattern; the CI including 1 suggests the couple pattern; the CI including −1 represents the contrast pattern; the CI between 0 and 1 shows the APIM between the actor-only and the couple patterns.23 Thirdly, Whether the dyad members are sexually distinguishable should be examined. To this end, a completely indistinguishable model is constructed.65 Afterward, using a chi-square test between one model with distinguishable dyads and its counterpart with indistinguishable dyads, model comparison is conducted to examine whether sex contributes to statistically significant differences. If Δχ2 < 0.05, it suggests that dyads are sexually distinguishable.
AMOS 24.0 was adopted to examine the mediation model. In the mediation model, parents’ total IUS-12 scores were set as predictor variables; parents’ total WFPTS scores and children’s total IUS-12 scores were set as mediator variables; children’s total WFPTS scores were set as outcome variables. χ2/df<3, RMSEA<0.08, SRMR<0.05, CFI, TFI, IFI, and GFI>0.90 were set as the criteria for a well-fitted model.66 To examine mediation, indirect effects were estimated using bootstrapping with 5000 iterations. If 0 is not in the 95% CI, it suggests that indirect effects are significant. p < 0.05 was set as the acceptable statistical significance.
Results
Analysis for Correlations Among Variables
The results of correlation analysis (see Table 2) indicate that the IU and trust in physicians of parents were significantly and positively correlated with those of children, and IU was significantly and negatively correlated with trust in physicians.
 |
Table 2 Correlation Analysis for Parents’ and Children’s IUS-12 and WFPTS |
Analysis for Intergenerational Transmission
Linear mixed effects models were employed to analyze the intergenerational transmission of IU and trust in physicians. The results indicated that fathers’ total IUS-12 scores (β=0.28, SE=0.05; F(367)=34.63, p<0.001; t=5.89, p<0.001) and mothers’ total IUS-12 scores (β=0.43, SE=0.05; F(367)=75.39, p<0.001; t=8.68, p<0.001) could significantly and positively predict children’s total IUS-12. Besides, fathers’ total WFPTS scores (β=0.30, SE=0.05; F(367)=34.16, p<0.001; t=5.85, p<0.001) and mothers’ total WFPTS scores (β=0.37, SE=0.05; F(367)=57.23, p<0.001; t=7.57, p<0.001) could also significantly and positively predict children’s total WFPTS scores.
Analysis for the APIM
The APIM for the effect of the total IUS-12 scores on the total WFPTS scores was constructed. The results are presented in Table 3. Fathers’ actor effect size was −0.327 (p<0.001, 95% CI [−0.43, −0.23]), and the standardized actor effect size was −0.411; mothers’ actor effect size was −0.290 (p<0.001, 95% CI [−0.39, −0.19]), and the standardized actor effect size was −0.364. Restricted and unrestricted models showed no significant difference when examining the measurement invariance of fathers’ and mothers’ actor effects (p=0.600, 95% CI [−0.18, 0.10]).
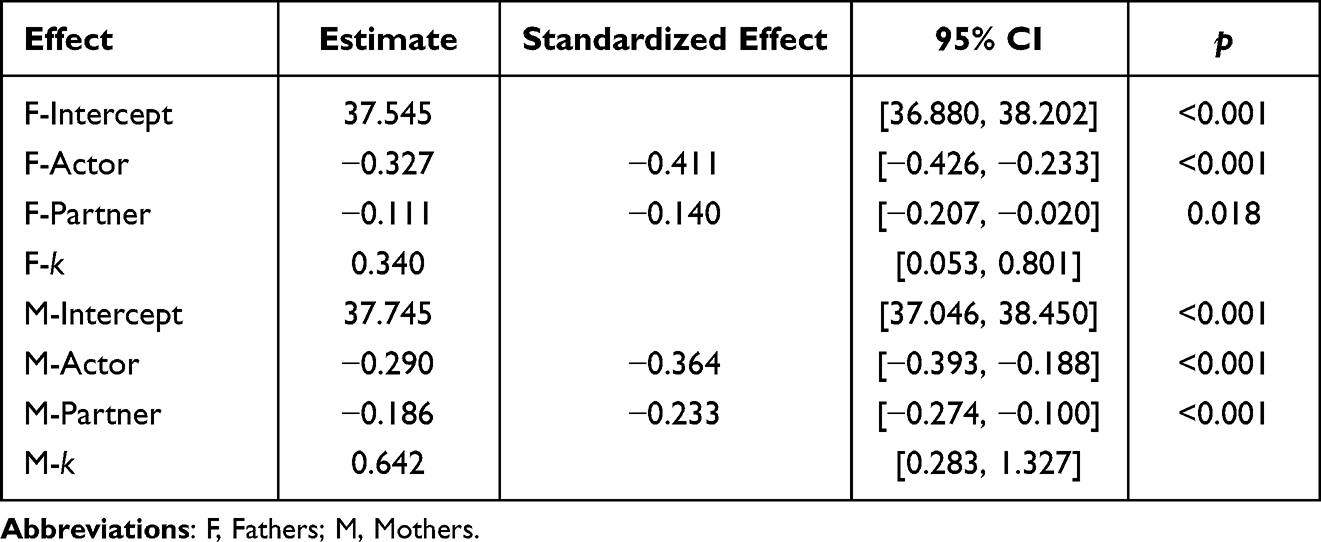 |
Table 3 Parameter Estimates for Paths of the APIM |
Fathers’ partner effect size was −0.111 (p=0.018, 95% CI [−0.21, −0.02]), and the standardized partner effect size was −0.140; mothers’ partner effect size was −0.186 (p<0.001, 95% CI [−0.27, −0.10]), and the standardized partner effect size was −0.233. Restricted and unrestricted models showed no significant difference when examining the measurement invariance of fathers’ and mothers’ partner effects (p=0.251, 95% CI [−0.05, 0.20]).
Both fathers’ and mothers’ standardized actor effects were significant (effect size>0.1), which met the premise of computing k values. Fathers’ k value was 0.340 and mothers’ k value was 0.642. Adopting the bootstrap method to analyze the dyadic pattern, it was found that the 95% CI of fathers’ k value was between 0.05 and 0.80; the 95% CI of mothers’ k value was between 0.28 and 1.33. A further test revealed that the k values of fathers and mothers were not significant (p=0.391, 95% CI [--1.10, 0.32]).
The results of model comparison showed that χ2(6) =3.983, p=0.679, suggesting that the effect of IU on trust in physicians was sexually distinguishable dyads.
Analysis for Mediation Effects
The results of mediation analysis are presented in Figure 1. Fathers’ total IUS scores negatively predicted their own (β = −0.43, p < 0.01) and mothers’ (β = −0.23, p < 0.01) total WFPTS’ scores; mothers’ total IUS-12 scores negatively predicted their own (β = −0.35, p < 0.01) and fathers’ total (β = −0.14, p = 0.012) WFPTS scores; fathers’ (β = 0.30, p < 0.01) and mothers’ total (β = 0.43, p < 0.01) IUS-12 scores positively predicted children’s total IUS-12 scores; fathers’ (β = 0.24, p < 0.01) and mothers’ (β = 0.32, p < 0.01) total WFPTS scores positively predicted children’s total WFPTS scores; children’s total IUS-12 scores negatively predicted their own total WFPTS scores (β = −0.24, p < 0.01). The model’s fit indices were: χ2/df=2.716, RMSEA=0.068, SRMR=0.028, CFI=0.992, TLI=0.970, IFI=0.992, GFI=0.990.
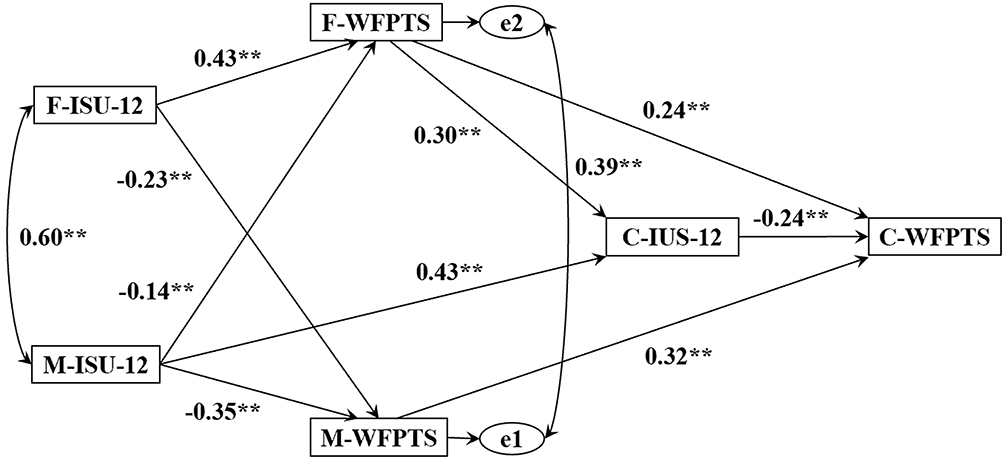 |
Figure 1 The proposed mediation model. Abbreviations: F, fathers; M, mothers; C, children; IUS-12, Intolerance of Uncertainty Scale-12; WFPTS, Wake Forest Physician Trust Scale. Note: **p < 0.01; All coefficients were standardized. |
The results of bootstrapping for indirect effects are shown in Table 4. The 95% bootstrap CI of all paths did not include 0, suggesting that all paths were significant. Among them, the total indirect effect of fathers’ total IUS scores on children’s total WFPTS scores was −0.249, and that of mothers’ total IUS-12 scores on children’s total WFPTS scores was −0.246.
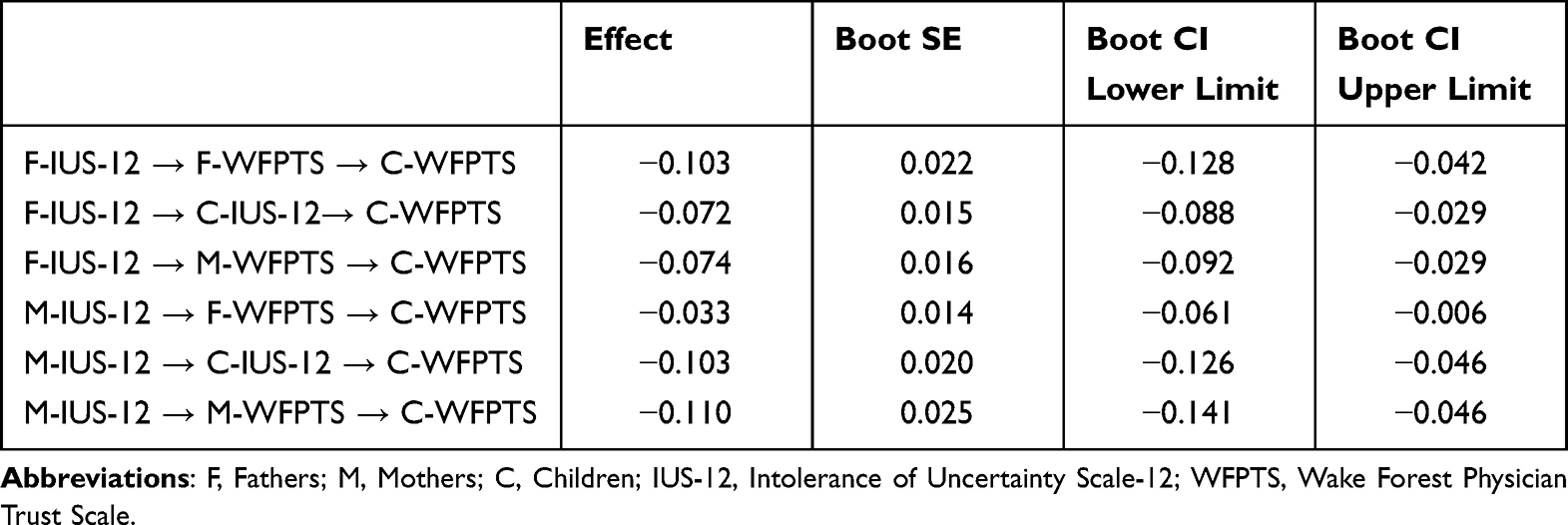 |
Table 4 Indirect Effects of Parents’ IU on Children’s Trust in Physicians |
Discussion
Trust has a pivotal role in measuring healthcare service quality and establishing a harmonious physician-patient relationship.12 If the public tends to mistrust physicians’ professionalism, treatment, and ethics, they are more likely to act defensive and dishonest, have malicious complaints,67 or even violently harm physicians when seeking medical advice.68 Explorations into the factors affecting trust in physicians help better meet people’s needs for health and improve the increasingly tense physician-patient relationship. From the intergenerational perspective, we investigated the relationship between parents’ IU and trust in physicians, and then further probed the mechanisms by which parents’ IU affects children’s trust in physicians. It was found that individuals’ IU were significantly and negatively correlated with their trust in physicians. Besides, IU and trust in physicians could be intergenerational transmitted. Moreover, the analysis of the APIM indicated that parents’ IU could significantly and negatively predict their own and their spouses’ trust in physicians. The analysis of the mediation model revealed that parents’ trust in physicians and children’s IU played mediating roles in the predictive effect of parents’ IU on children’s trust in physicians. The findings have certain theoretical and practical significance for improving public trust in physicians.
The results of the present study indicated that individuals’ IU was significantly and negatively correlated with their trust in physicians, supporting Hypothesis 1. Lu et al found that patients’ IU was negatively predictive of trust in physicians.69 Torbit et al found that the interaction between IU and trust in physicians could affect patients’ worry about their illness.70 With non-patients as participants, the present study drew the same conclusion, thus extending the applicability of this conclusion from patients to general population. Our findings imply that individuals’ attitude toward and acceptance of medical IU need to be focused, when carrying out interventions in public trust in physicians. Besides, a gulf exists in the cognition of uncertainty of medicine between the public and physicians. Generally, the public’s expectations of the progress and effect of treatment are much higher than physicians, with the belief that medicine can cure most illnesses.71 Individuals with high IU may doubt physicians’ professionalism when experiencing slow treatment progress, poor treatment effect, or misdiagnosis, thus reducing their trust in physicians.37
The total IUS-12 scores of fathers and mothers could positively predict the total IUS-12 scores of their children, suggesting that IU could be intergenerationally transmitted, in line with Hypothesis 2. It has been found in both general population and patients that parents’ IU could positively predict children’s IU.46,72 However, these studies were conducted in the context of western culture. To our best knowledge, the present study is the first one that explored the intergenerational transmission of IU in the Chinese context and drew the similar conclusion. Mothers’ effects on children were greater than fathers’, probably because fathers and mothers play different roles in raising their children. In most cases, mothers would spend more time on taking care of children, so that mothers form a stronger bond with and exert a greater effect on their children.73
Mothers’ predictive effects in the present research were found to be greater than those in previous research,38 which may be justified by the distinction in familism between the west and China.74 Authority-subordinate relationships are the prototypical characteristic of parent-child relationships in China.75 Filial piety, the core of Confucianism, assumes that children should show absolute respect and obedience to their parents’ notions, behavior, and will.76 Parental overprotection and psychological control might hinder children from meeting their psychological needs, decreasing their perceived self-control, and increasing their IU levels.77,78 A comparative study on China, America, and Turkey found that Chinese mothers usually adopt an authoritative parenting style, and more commonly control and meddle in their children’s affairs,79 which may also be one of the reasons why Chinese mothers have greater effects on children’s IU than their western counterparts. Besides, the differences in family structures between China and the west are possibly another contributor. In China, grandparents would also foster their grandchildren, and even serve as the main caregivers.80 Grandparents’ participation in bringing up their grandchildren could negatively influence parents’ parenting, thus leading to their grandchildren’s worse psychological health, higher anxiety, and more worries.81
With a probe into the intergenerational transmission of trust in physicians, the present study found that parents’ WFPTS scores could positively predict children’s WFPTS scores, echoing Hypothesis 3. Trust can be divided into general trust and special trust. Concerning general trust, as a pervasive and relatively stable trait, its intergenerational transformation has been widely demonstrated.82 However, scant studies have explored the intergenerational transmission of public trust in physicians. As a special form of interpersonal trust, public trust in physicians is a product of high expectations of physicians.83 Patients’ trust in physicians mainly derives from their direct experience of interaction with physicians in treatment,84 whereas public trust in physicians mainly stems from indirect experience.15 Previous studies overlooked the impact of family factors since they considered media reports on physician-patient events as the main source of individuals’ indirect experience.85 Apart from parents, the interaction and communication between other family members can also affect individuals’ trust in physicians.
The present study has its novelty in that the interaction between parents’ IU and trust in physicians was tested using the APIM for dyadic data. The present study found that fathers’ dyadic pattern was between the actor-only pattern and the couple pattern, whilst mothers’ dyadic pattern was the couple pattern, confirming Hypothesis 4. The couple pattern refers to individuals’ outcome variables are affected by both their own and their spouses’ predictor variables. The mixed pattern, as a special couple pattern, shows the greater actor effect than the partner effect.23 In other words, fathers’ and mothers’ IU played the same vital role in affecting mothers’ trust in physicians. By contrast, in terms of fathers’ trust in physicians, fathers’ IU exerted a greater impact than mothers’ IU on it, although it was affected by both. Hence, asymmetry existed in the impact of parents’ IU on each other’s trust in physicians. A similar asymmetry has also been found in previous research on marital satisfaction.86 The possible reason is that males usually have a higher independent self-construal, while females usually have a higher interdependent self-construal.87 Individuals high in independent self-construal prioritize themselves and seek separateness from others to maintain their uniqueness, while those high in interdependent self-construal prioritize others, seek connection with others, and volunteer to understand others’ ideas and feelings.88
Based on the exploration into intergenerational transmission and the APIM, we constructed a mediation model to investigate the mechanisms by which parents’ IU affects children’s trust in physicians. The results showed that parents’ trust in physicians and children’s IU mediated the effect of parents’ IU on children’s trust in physicians. Specifically, on the one hand, through intergenerational transmission, parents’ IU had an impact on children’s IU, consequently affecting their trust in physicians. On the other hand, parents’ IU negatively predicted their own and their spouses’ physicians, subsequently influencing children’s trust in physicians through the intergenerational transmission of trust in physicians, echoing Hypotheses 6 and 7, but only partly supporting Hypothesis 5. It suggests that interventions in both parents’ IU and trust in physicians could affect children’s IU and trust in physicians.
The present study is theoretically significant to some extent, since to our best knowledge, it pioneered to investigate the relationship between parents’ and children’s IU and trust in physicians among the public from the intergenerational perspective. Considering Chinese people’s deep-seated familism, such perspective allows to have in-depth insights into the psychological mechanisms by which they form their trust in physicians.
Drawing on the family systems theory, the present study explored the intergenerational transmission of IU and trust in physicians, discussed the mutual interaction between parents, and analyzed the proposed mediation model. The findings supported the view that marital subsystem could affect the development of parental subsystem, which enriches and expands the family systems theory. Besides, based on the cognitive model of pathological worry, the present study probed the associations between IU and trust in physicians among three groups: fathers, mothers, and children. This model initially emphasizes the effect of IU on worry. Further including trust in physicians in this model, the present study found that the excessive worry of individuals with high IU probably influences their trust in physicians. Hence, the present study extends the applicability of this model to the field of physician-patient relationships.
The present study is also practically significant in a sense, since it could provide references for conducting interventional studies. The findings suggested that improving the public’s acceptance of uncertainty and leading them to rationally treat the uncertainty in diagnosis and treatment can be conducive to reducing their high expectation of medicine and enhancing their trust in physicians.29 According to previous research, the IU of the public gets lower when they obtain the information pertinent to diseases and physicians on the Internet.89 Hence, publicizing health-related knowledge to the public and implementing medical education may help improve the public’s tolerance of medical uncertainty. Moreover, both the influence of family factors and parents’ attitude toward physicians should be considered when intervening in public trust in physicians. Our findings imply that when performing interventions in public trust in physicians, the family should be regarded as a fundamental unit. During treatment, physicians should establish a great relationship with patients and have good communication with their relatives.
The limitations of the present study are as follows. Firstly, the participants were students only from two colleges and their parents, so the sample might not be representative enough. Therefore, whether our findings are applicable to other groups needs to be further tested. Secondly, our cross-sectional study can hardly explain the causality between the variables, so a longitudinal study can be carried out in the future to further demonstrate the associations between IU and trust in physicians. Besides, the adoption of self-report measures might cause social desirability effect. Hence, questionnaire surveys, the implicit association test, and interviews need to be combined in our future work to make the findings more scientific. Thirdly, in the present study, children’s IU and trust in physicians were set as outcome variables to explore the impact of parental characteristics on offspring characteristics. However, children’s IU and trust in physicians may also exert an influence on parents. Accordingly, cross-lagged panel models need to be employed to investigate the reciprocal relationship between parents’ and children’s IU and trust in physicians.
Conclusion
In the present study, we found that individuals’ IU was significantly and negatively correlated with their trust in physicians. The APIM indicated that parents’ IU could negatively predict their own and their spouses’ trust in physicians. Besides, the predictive effect of parents’ IU on children’s trust in physicians was mediated by parents’ trust in physicians and children’s IU. The present study helps better understand the mechanisms by which IU and trust in physicians are intergenerationally transmitted. These findings are theoretically and practically significant to the improvement of public trust in physicians.
Acknowledgments
The authors are grateful for all the researchers and participants for their contributions in this research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Social Science Research Project of the Educational Department of Jilin Province (JJKH20211014JY).
Disclosure
The authors declare that they don’t have any competing financial interests or personal relationships that have an impact on this research.
References
1. Sun JJ, Zheng ZB, Jiang XL, et al. Research on management of doctor-patient risk and status of the perceived behaviors of physician trust in the patient in China: new perspective of management of doctor-patient risk. Math Probl Eng. 2020;2020:2145029. doi:10.1155/2020/2145029
2. Wang W, Zhang H, Washburn DJ, et al. Factors influencing trust towards physicians among patients from 12 hospitals in China. Am J Health Behav. 2018;42(6):19–30. doi:10.5993/ajhb.42.6.3
3. Zhao D, Zhang Z. Changes in public trust in physicians: empirical evidence from China. Front Med. 2019;13(4):504–510. doi:10.1007/s11684-018-0666-4
4. Li C, Khan MM. Public trust in physicians: empirical analysis of patient-related factors affecting trust in physicians in China. BMC Prim Care. 2022;23(1):217. doi:10.1186/s12875-022-01832-6
5. Dong E, Bao Y. Reliability and validity of the Chinese version of wake forest physician trust scale. Chin Ment Health J. 2012;26(3):171–175. doi:10.3969/j.issn.1000-6729.2012.03.003
6. Tang C, Tian B, Zhang X, et al. The influence of cultural competence of nurses on patient satisfaction and the mediating effect of patient trust. J Adv Nurs. 2019;75(4):749–759. doi:10.1111/jan.13854
7. Du Y, Wang W, Washburn DJ, et al. Violence against healthcare workers and other serious responses to medical disputes in China: surveys of patients at 12 public hospitals. BMC Health Serv Res. 2020;20(1):253. doi:10.1186/s12913-020-05104-w
8. Zhou Y, Chen S, Liao Y, et al. General perception of doctor-patient relationship from patients during the COVID-19 pandemic in China: a cross-sectional study. Front Public Health. 2021;9:646486. doi:10.3389/fpubh.2021.646486
9. Hogikyan ND, Kana LA, Shuman AG, Firn JI. Patient perceptions of trust formation in the surgeon-patient relationship: a thematic analysis. Patient Educ Couns. 2021;104(9):2338–2343. doi:10.1016/j.pec.2021.02.002
10. Chen D, Zhou Q, Pratt CB, Su Z, Gu Z. Investigating the relationships between public health literacy and public trust in physicians in China’s control of COVID-19: a cross-sectional Study. Front Public Health. 2021;9:758529. doi:10.3389/fpubh.2021.758529
11. Khullar D, Prasad K, Neprash H, et al. Factors associated with patient trust in their clinicians: results from the healthy work place study. Health Care Manage Rev. 2022;47(4):289–296. doi:10.1097/hmr.0000000000000336
12. Wu Q, Jin Z, Wang P. The relationship between the physician-patient relationship, physician empathy, and patient trust. J Gen Intern Med. 2022;37(6):1388–1393. doi:10.1007/s11606-021-07008-9
13. Ozawa S, Sripad P. How do you measure trust in the health system? A systematic review of the literature. Soc Sci Med. 2013;91:10–14. doi:10.1016/j.socscimed.2013.05.005
14. Luo A, Qin L, Yuan Y, et al. The effect of online health information seeking on physician-patient relationships: systematic review. J Med Internet Res. 2022;24:e23354. doi:10.2196/23354
15. Sun J, Liu S, Liu Q, et al. Impact of adverse media reporting on public perceptions of the doctor-patient relationship in China: an analysis with propensity score matching method. BMJ Open. 2018;8(8):e022455. doi:10.1136/bmjopen-2018-022455
16. Hall MA, Camacho F, Dugan E, Balkrishnan R. Trust in the medical profession: conceptual and measurement issues. Health Serv Res. 2002;37(5):1419–1439. doi:10.1111/1475-6773.01070
17. Hillen M, Smets E. Cancer patients’ trust in their physician - a review. Psycho-Oncology. 2010;20:227–241. doi:10.1002/pon.1745
18. Golden S, Ono S, Thakurta S, et al. “I’m putting my trust in their hands”: a qualitative study of patients’ views on clinician initial communication about lung cancer screening. Chest. 2020;158. doi:10.1016/j.chest.2020.02.072
19. Shaya B, Al Homsi N, Eid K, et al. Factors associated with the public’s trust in physicians in the context of the Lebanese healthcare system: a qualitative study. BMC Health Serv Res. 2019;19(1):525. doi:10.1186/s12913-019-4354-0
20. Wilk AS, Platt JE. Measuring physicians’ trust: a scoping review with implications for public policy. Soc Sci Med. 2016;165:75–81. doi:10.1016/j.socscimed.2016.07.039
21. Blendon RJ, Benson JM. Americans’ views on health policy: a fifty-year historical perspective. Health Aff. 2001;20(2):33–46. doi:10.1377/hlthaff.20.2.33
22. Erdem G, Safi O. The cultural lens approach to Bowen family systems theory: contributions of family change theory. J Fam Theory Rev. 2018;10(2):469–483. doi:10.1111/jftr.12258
23. Kenny DA, Ledermann T. Detecting, measuring, and testing dyadic patterns in the actor-partner interdependence model. J Fam Psychol. 2010;24(3):359–366. doi:10.1037/a0019651
24. Blanch-Hartigan D, van Eeden M, Verdam MGE, Han PKJ, Smets EMA, Hillen MA. Effects of communication about uncertainty and oncologist gender on the physician-patient relationship. Patient Educ Couns. 2019;102(9):1613–1620. doi:10.1016/j.pec.2019.05.002
25. Carleton RN, Norton MA, Asmundson GJ. Fearing the unknown: a short version of the Intolerance of Uncertainty Scale. J Anxiety Disord. 2007;21(1):105–117. doi:10.1016/j.janxdis.2006.03.014
26. McGovern R, Harmon D. Patient response to physician expressions of uncertainty: a systematic review. Ir J Med Sci. 2017;186(4):1061–1065. doi:10.1007/s11845-017-1592-1
27. Bhise V, Meyer AND, Menon S, et al. Patient perspectives on how physicians communicate diagnostic uncertainty: an experimental vignette study. Int J Qual Health Care. 2018;30(1):2–8. doi:10.1093/intqhc/mzx170
28. Hirsch CR, Mathews A. A cognitive model of pathological worry. Behav Res Ther. 2012;50(10):636–646. doi:10.1016/j.brat.2012.06.007
29. Songco A, Hudson JL, Fox E. A cognitive model of pathological worry in children and adolescents: a systematic review. Clin Child Fam Psychol Rev. 2020;23(2):229–249. doi:10.1007/s10567-020-00311-7
30. Dugas M, Gosselin P, Ladouceur R. Intolerance of uncertainty and worry: investigating specificity in a nonclinical sample. Cognit Ther Res. 2001;25(5):551–558. doi:10.1023/A:
31. Sexton KA, Dugas MJ. Defining distinct negative beliefs about uncertainty: validating the factor structure of the Intolerance of Uncertainty Scale. Psychol Assess. 2009;21(2):176–186. doi:10.1037/a0015827
32. Yang Z, Zhao X, Zhu Z, Fu Y, Hu Y. How patients with an uncertain diagnosis experience intolerance of uncertainty: a grounded theory study. Psychol Res Behav Manag. 2021;14:1269–1279. doi:10.2147/prbm.S318263
33. Calatrava M, Martins MV, Schweer-Collins M, Duch-Ceballos C, Rodríguez-González M. Differentiation of self: a scoping review of Bowen family systems theory’s core construct. Clin Psychol Rev. 2022;91:102101. doi:10.1016/j.cpr.2021.102101
34. Wijaya Y. The prospect of familism in the global era: a study on the recent development of the ethnic-Chinese business, with particular attention to the Indonesian context. J Bus Ethics. 2008;79(3):311–317. doi:10.1007/s10551-007-9399-z
35. Lemmers AL, van der Voort PHJ. Trust in intensive care patients, family, and healthcare professionals: the development of a conceptual framework followed by a case study. Healthcare. 2021;9(2):208. doi:10.3390/healthcare9020208
36. Hall MA, Zheng B, Dugan E, et al. Measuring patients’ trust in their primary care providers. Med Care Res Rev. 2002;59(3):293–318. doi:10.1177/1077558702059003004
37. Suzuki R, Yajima N, Sakurai K, et al. Association of patients’ past misdiagnosis experiences with trust in their current physician among Japanese adults. J Gen Intern Med. 2022;37(5):1115–1121. doi:10.1007/s11606-021-06950-y
38. Sanchez AL, Kendall PC, Comer JS. Evaluating the intergenerational link between maternal and child intolerance of uncertainty: a preliminary cross-sectional examination. Cognit Ther Res. 2016;40(4):532–539. doi:10.1007/s10608-016-9757-1
39. Connolly T, Coats H, DeSanto K, Jones J. The experience of uncertainty for patients, families and healthcare providers in post-stroke palliative and end-of-life care: a qualitative meta-synthesis. Age Ageing. 2020;50(2):534–545. doi:10.1093/ageing/afaa229
40. Aktar E, Nikolić M, Bögels SM. Environmental transmission of generalized anxiety disorder from parents to children: worries, experiential avoidance, and intolerance of uncertainty. Dialogues Clin Neurosci. 2017;19(2):137–147. doi:10.31887/DCNS.2017.19.2/eaktar
41. Neel MLM, Stark AR, Maitre NL. Parenting style impacts cognitive and behavioural outcomes of former preterm infants: a systematic review. Child Care Health Dev. 2018;44(4):507–515. doi:10.1111/cch.12561
42. Shen Y, Luo Z, Fu D, Qie M, Wang L. Parenting profiles, intolerance of uncertainty, and worry among Chinese primary school children. J Child Fam Stud. 2020;29(8):2303–2313. doi:10.1007/s10826-020-01755-9
43. Chorpita BF, Barlow DH. The development of anxiety: the role of control in the early environment. Psychol Bull. 1998;124(1):3–21. doi:10.1037/0033-2909.124.1.3
44. Zlomke K, Young J. A retrospective examination of the role of parental anxious rearing behaviors in contributing to intolerance of uncertainty. J Child Fam Stud. 2009;18:670–679. doi:10.1007/s10826-009-9269-7
45. O’Connor T, Matias C, Futh A, Tantam G, Scott S. Social learning theory parenting intervention promotes attachment-based caregiving in young children: randomized clinical trial. J Clin Child Adolesc Psychol. 2012;42(3):358–370. doi:10.1080/15374416.2012.723262
46. Bottesi G, Gürdere C, Cerea S, Sica C, Ghisi M. Familial patterns of intolerance of uncertainty: preliminary evidence in female university students. Int J Cogn Ther. 2020;13(1):30–41. doi:10.1007/s41811-019-00063-5
47. Vasa RA, Kreiser NL, Keefer A, Singh V, Mostofsky SH. Relationships between autism spectrum disorder and intolerance of uncertainty. Autism Res. 2018;11(4):636–644. doi:10.1002/aur.1916
48. Simmons A, Matthews SC, Paulus MP, Stein MB. Intolerance of uncertainty correlates with insula activation during affective ambiguity. Neurosci Lett. 2008;430(2):92–97. doi:10.1016/j.neulet.2007.10.030
49. Paulus MP, Stein MB. An insular view of anxiety. Biol Psychiatry. 2006;60(4):383–387. doi:10.1016/j.biopsych.2006.03.042
50. Nikodem K, Ćurković M, Borovečki A. Trust in the healthcare system and physicians in Croatia: a survey of the general population. Int J Environ Res Public Health. 2022;19(2):993. doi:10.3390/ijerph19020993
51. Weidmann R, Ledermann T, Grob A. The interdependence of personality and satisfaction in couples: a review. Eur Psychol. 2016;21:284–295. doi:10.1027/1016-9040/a000261
52. Eira Nunes C, de Roten Y, El Ghaziri N, Favez N, Darwiche J. Co‐parenting programs: a systematic review and meta‐analysis. Fam Relat. 2020;70. doi:10.1111/fare.12438
53. Chen Z, Ellis A. Crossover of daily job stressors among dual‐career couples: a dyadic examination. J Organ Behav. 2021;42(5):668–683. doi:10.1002/job.2520
54. Pollock Star A, Cohn-Schwartz E, O’Rourke N. Reciprocal effects of marital idealization and marital satisfaction between long-wed spouses over time. Int J Aging Hum Dev. 2022;95:440–454. doi:10.1177/00914150221077953
55. Bodschwinna D, Ernst J, Mehnert-Theuerkauf A, Gündel H, Weissflog G, Hönig K. Dyadic coping and social support: various types of support in hematooncological patients and their spouses-Associations with psychological distress. Psychooncology. 2021;30(7):1041–1050. doi:10.1002/pon.5631
56. Varner S, Lloyd G, Ranby KW, Callan S, Robertson C, Lipkus IM. Illness uncertainty, partner support, and quality of life: a dyadic longitudinal investigation of couples facing prostate cancer. Psychooncology. 2019;28(11):2188–2194. doi:10.1002/pon.5205
57. Blendon RJ, Benson JM, Hero JO. Public trust in physicians--U.S. medicine in international perspective. N Engl J Med. 2014;371(17):1570–1572. doi:10.1056/NEJMp1407373
58. Barge S, Gehlbach H. Using the theory of satisficing to evaluate the quality of survey data. Res High Educ. 2012;53:182–200. doi:10.1007/s11162-011-9251-2
59. Mayerl J. Response latency measurement in surveys. detecting strong attitudes and response effects. Survey Methods: Insights from the Field; 2013. Available from: https://surveyinsights.org/?p=1063.
60. Zhang Y, Song J, Gao Y, Wu S, Song L, Miao D. Reliability and validity of the intolerance of uncertainty scale-short form in university students. Chin J Clin Psychol. 2017;25(2):285–288. doi:10.16128/j.cnki.1005-3611.2017.02.020
61. Katz E, Edelstein B. Psychometric properties of the wake forest physician trust scale with young and older adults. Innov Aging. 2018;2(1):978. doi:10.1093/geroni/igy031.3621
62. Stas L, Kenny DA, Mayer A, Loeys T. Giving dyadic data analysis away: a user-friendly app for actor-partner interdependence models. Pers Relatsh. 2018;25(1):103–119. doi:10.1111/pere.12230
63. Rosseel Y. lavaan: an R package for structural equation modeling. J Stat Softw. 2011;48(2):1–36. doi:10.18637/jss.v048.i02
64. Cook WL, Kenny DA. The actor–partner interdependence model: a model of bidirectional effects in developmental studies. Int J Behav Dev. 2005;29(2):101–109. doi:10.1080/01650250444000405
65. Olsen JA, Kenny DA. Structural equation modeling with interchangeable dyads. Psychol Methods. 2006;11(2):127–141. doi:10.1037/1082-989x.11.2.127
66. Bentler PM, Bonett DG. Significance tests and goodness of fit in the analysis of covariance structures. Psychol Bull. 1980;88:588–606. doi:10.1037/0033-2909.88.3.588
67. Nie JB, Cheng Y, Zou X, et al. The vicious circle of patient-physician mistrust in China: health professionals’ perspectives, institutional conflict of interest, and building trust through medical professionalism. Dev World Bioeth. 2018;18(1):26–36. doi:10.1111/dewb.12170
68. Nie JB, Li L, Gillett G, Tucker JD, Kleinman A. The crisis of patient-physician trust and bioethics: lessons and inspirations from China. Dev World Bioeth. 2018;18(1):56–64. doi:10.1111/dewb.12169
69. Lyu X, Fu C, Wang X. Effect and underlying mechanism of refutation texts on the trust and moral judgment of patients. Acta Psychol Sin. 2019;51(10):1171–1186. doi:10.3724/sp.J.1041.2019.01171
70. Torbit LA, Albiani JJ, Aronson M, et al. Physician trust moderates the relationship between intolerance of uncertainty and cancer worry interference among women with Lynch syndrome. J Behav Med. 2016;39(3):420–428. doi:10.1007/s10865-016-9711-4
71. Wu D, Lam TP, Lam KF, Zhou XD, Sun KS. Doctors’ views of patient expectations of medical care in Zhejiang Province, China. Int J Qual Health Care. 2017;29(6):867–873. doi:10.1093/intqhc/mzx119
72. Neville A, Kopala-Sibley DC, Soltani S, et al. A longitudinal examination of the interpersonal fear avoidance model of pain: the role of intolerance of uncertainty. Pain. 2021;162(1):152–160. doi:10.1097/j.pain.0000000000002009
73. Bridgett DJ, Burt NM, Edwards ES, Deater-Deckard K. Intergenerational transmission of self-regulation: a multidisciplinary review and integrative conceptual framework. Psychol Bull. 2015;141:602–654. doi:10.1037/a0038662
74. Lu P, Kong D, Shelley M. Child–parent relationships and older adults’ health: a cross-cultural comparison between China and the United States. J Fam Issues. 2022. doi:10.1177/0192513X211064866
75. Lin L, Wang Q. Adolescents’ filial piety attitudes in relation to their perceived parenting styles: an urban-rural comparative longitudinal study in China. Front Psychol. 2021;12:750751. doi:10.3389/fpsyg.2021.750751
76. Yang SJ. The reconciliation of filial piety and political authority in early China. Dao. 2017;16(2):187–203. doi:10.1007/s11712-017-9546-x
77. Mullins LL, Wolfe-Christensen C, Pai AL, et al. The relationship of parental overprotection, perceived child vulnerability, and parenting stress to uncertainty in youth with chronic illness. J Pediatr Psychol. 2007;32(8):973–982. doi:10.1093/jpepsy/jsm044
78. Li J, Zhang L, Wen Z, Huang R, Dong S. The influence of parental psychological control on social anxiety of migrant children: chain mediating effect analysis. Chin J Clin Psychol. 2021;29(1):139–143+103. doi:10.16128/j.cnki.1005-3611.2021.01.027
79. Luo Y, Chen F, Zhang X, et al. Profiles of maternal and paternal parenting styles in Chinese families: relations to preschoolers’ psychological adjustment. Child Youth Serv Rev. 2021;121:105787. doi:10.1016/j.childyouth.2020.105787
80. Lo S, Lindsay J. “My children”, “my grandchildren”: navigating intergenerational ambivalence in grandparent childcare arrangements in Hong Kong. Fam Relat. 2022;71(4):1834–1851. doi:10.1111/fare.12678
81. Kaminski P, Kaminski PL. Grandparents raising their grandchildren: a review of the literature and suggestions for practice. Gerontol. 2005;45:262–269. doi:10.1093/geront/45.2.262
82. Dawson C. How persistent is generalised trust? Sociology. 2017;53(3):590–599. doi:10.1177/0038038517718991
83. Dahlhaus C, Schlösser T. The interplay of social status and trust: a critical review of concepts, operationalizations, and findings. Rev Gen Psychol. 2021;25(2):203–220. doi:10.1177/10892680211007405
84. Nguyen AL, Schwei RJ, Zhao YQ, Rathouz PJ, Jacobs EA. What matters when it comes to trust in one’s physician: race/ethnicity, sociodemographic factors, and/or access to and experiences with health care? Health Equity. 2020;4(1):280–289. doi:10.1089/heq.2019.0101
85. Gong W, Guo Q. Framing public opinion on physician-patient conflicts on microblog: a comparative content analysis. Front Public Health. 2022;10:831638. doi:10.3389/fpubh.2022.831638
86. Maroufizadeh S, Hosseini M, Rahimi Foroushani A, Omani-Samani R, Amini P. The relationship between marital satisfaction and depression in infertile couples: an actor-partner interdependence model approach. BMC Psychiatry. 2018;18(1):310. doi:10.1186/s12888-018-1893-6
87. Hansen L, Petrakis M. The self in motherhood: a systematised review of relational self-construal and wellbeing in mothers. Adv Ment Health. 2018;17(1):1–13. doi:10.1080/18387357.2018.1476066
88. Cross SE, Hardin EE, Gercek-Swing B. The what, how, why, and where of self-construal. Pers Soc Psychol Rev. 2011;15(2):142–179. doi:10.1177/1088868310373752
89. Dong W, Lei X, Liu Y. The mediating role of patients’ trust between web-based health information seeking and patients’ uncertainty in China: cross-sectional web-based survey. J Med Internet Res. 2022;24(3):e25275. doi:10.2196/25275
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.