Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Exploring the Nexus Between Ankle-Brachial Index and Atherosclerosis: A Bibliometric Analysis From 1989 to 2024
Authors Wang J ![]() , Tao Y, Tao Y, Ke X, Wang L, Zhang S, Hong W
, Tao Y, Tao Y, Ke X, Wang L, Zhang S, Hong W ![]()
Received 30 April 2025
Accepted for publication 12 August 2025
Published 29 August 2025 Volume 2025:18 Pages 5371—5380
DOI https://doi.org/10.2147/JMDH.S537831
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Professor Charles V Pollack
Jun Wang,1,* Yanfei Tao,2,* Yongjun Tao,1 Xiaoyong Ke,1 Liaojun Wang,1 Shu Zhang,3 Weiyong Hong4
1Department of Neurology, Municipal Hospital Affiliated to Taizhou University, Taizhou, 318000, People’s Republic of China; 2Department of Gynaecology and Obstetrics, Municipal Hospital Affiliated to Taizhou University, Taizhou, 318000, People’s Republic of China; 3Department of Ultrasound, Municipal Hospital Affiliated to Taizhou University, Taizhou, 318000, People’s Republic of China; 4Department of Pharmacy, Municipal Hospital Affiliated to Taizhou University, Taizhou, 318000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Weiyong Hong, Email [email protected] Shu Zhang, Email [email protected]
Purpose: Cardiovascular and cerebrovascular diseases related to atherosclerosis represent a leading global health burden, contributing substantially to morbidity, disability, and premature mortality. The Ankle-Brachial Index (ABI) has emerged as a valuable non-invasive tool for screening peripheral artery disease and assessing the burden of systemic atherosclerosis. This bibliometric analysis aims to evaluate the research landscape, key contributors, and evolving trends in ABI and atherosclerosis studies.
Patients and Methods: A bibliometric analysis was conducted using data from the Web of Science Core Collection from 1989 to 2024. The data were analyzed using the R package “bibliometrix”, CiteSpace, and VOSviewer to identify research outputs, influential institutions, journals, authors, and keywords.
Results: This study included a total of 1896 eligible publications. The number of publications on ABI and atherosclerosis has steadily increased, peaking in 2021. The United States led in research output (n = 448) and citation impact (n = 29,980), followed by China and Japan. University of California System contributed the most publications, while Circulation and Atherosclerosis were the most influential journals. Criqui Michael H. emerged as the most cited author, with 5848 citations. Keyword analyses showed that the terms “cardiovascular disease”, “mortality”, “risk factors”, and “prevalence” terms had a high co-occurrence rate, while burst analyses showed that key terms such as “disease”, “epidemiology” and “events” were prominent in recent studies.
Conclusion: This bibliometric analysis offers a comprehensive perspective on the role of the ABI in the field of atherosclerosis research, and it offers crucial support for guiding future research directions.
Keywords: ankle-brachial index, atherosclerosis, bibliometric analysis
Introduction
Atherosclerosis, a leading cause of cardiovascular and cerebrovascular diseases, increases with age, placing a significant burden on society and healthcare systems. It involves the deposition of lipid and fibrous tissue in vessel walls, leading to arterial narrowing and hardening, which can result in myocardial infarction, stroke, and peripheral arterial disease.1 Atherosclerosis often lacks early symptoms, making timely diagnosis vital to reduce cardiovascular risks. The Ankle-Brachial Index (ABI), a non-invasive, cost-effective tool, is widely used to screen for peripheral arterial disease and assess systemic atherosclerosis burden. Its standardization enhances its role in cardiovascular risk evaluation.2 Recent studies suggest that a low ABI (<0.9) is associated not only with peripheral artery disease (PAD) but also with systemic atherosclerosis, including coronary artery disease, cerebrovascular events, and increased carotid intima-media thickness.3 Furthermore, ABI values are inversely correlated with systemic inflammation markers such as hsCRP, which may reflect the underlying systemic burden of atherosclerosis.4
ABI effectively reflects systemic atherosclerotic burden and is strongly linked to vascular calcification, plaque formation, arterial stiffness, and cardiovascular events.5 In recent years, research has expanded beyond ABI’s role in diagnosing PAD, exploring its association with systemic atherosclerosis, inflammatory markers, and metabolic syndrome.6 Furthermore, several recent studies and clinical recommendations support ABI measurement as a cardiovascular risk modifier, even in individuals without known atherosclerotic cardiovascular disease, thereby aiding in risk stratification and early preventive intervention.7 Given the growing body of research on ABI and atherosclerosis, it is essential to systematically evaluate the existing literature in order to identify research trends in this field.
Bibliometric analysis is a quantitative method used to assess research output and trends in a given scientific domain. It allows researchers to evaluate publication patterns, collaboration networks, and emerging research themes, providing valuable insights into the development of a field.8 Previous bibliometric studies have successfully mapped the research landscapes of various medical fields. For instance, existing bibliometric analyses have highlighted the interest in monoclonal antibodies targeting inflammation in atherosclerosis.9 Additionally, research trends have identified the NLRP3 inflammasome as a key hotspot in atherosclerosis-related inflammation.10 Despite prior analyses on atherosclerosis topics, no study has specifically explored ABI’s expanding scientific discourse beyond PAD. A targeted bibliometric analysis is essential to uncover underexplored connections between ABI and systemic atherosclerosis, highlight leading contributors, and guide future interdisciplinary collaboration. To address this gap, our study aims to conduct a bibliometric analysis of ABI and atherosclerosis, with the goal of identifying key themes and suggesting potential future research directions.
Materials and Methods
Search Strategies and Data Collection
A literature search was conducted in the Web of Science Core Collection (WoSCC), specifically using the Science Citation Index Expanded (SCIE) and the Social Sciences Citation Index (SSCI).11 The search strategy was designed to ensure both comprehensiveness and specificity to the research theme: (TS = (“ankle brachial index” OR “ankle brachial Pressure Index” OR “ankle arm index”)) AND TS = (“Atheroscleros*” OR “Atherogenesis*”).12,13 To ensure a comprehensive overview of the research landscape, the time frame was set from the publication date of the first relevant article (January 1, 1989) to the date of data retrieval (December 31, 2024). Only articles published in English were considered. Data was collected in text format, including publication and citation counts, article titles, author information, institutional affiliations, countries/regions, journals, and keywords, all of which were used for the subsequent bibliometric analysis.
Statistical Analysis
The bibliometric analysis was conducted using VOSviewer (V 1.6.20), CiteSpace (V 6.3.R1), and the R package “bibliometrix” (V 4.3.3). VOSviewer is a multifunctional software tool that plays a key role in mapping collaborations between countries, institutions, and authors, as well as journal co-authorship, coupling, and keyword co-occurrence.14 Using VOSviewer, we can visualize and explore the complex networks of cooperation and relationships within academic fields, gaining deep insights into the connections between authors, institutions, publications, and keywords. In the co-occurrence network map, the size of the nodes represents the number of objects, the thickness of the lines indicates the strength of the links, and the color of the nodes reflects different clusters or time trends.
CiteSpace was used to conduct a time-slice analysis of burst keywords from January 2004 to December 2024. The time slice was set to one year, with nodes designated as keywords. For keyword analysis, the threshold was set to the top 5 entries per slice, and the Pathfinder algorithm combined with network merging was applied for pruning optimization.
Additionally, the R package “bibliometrix” is a crucial tool for comprehensive bibliometric analysis.15 It supports the entire process of data import, transformation, analysis, and scientific visualization, making it well-suited to meet the needs of bibliometric research.
The h-index, m-index, and g-index are used to quantitatively assess the academic impact of individuals and journals,16,17 while the 2023 impact factor (IF) and journal ranking, or quartile (JCR), obtained from Journal Citation Reports (Clarivate Analytics), were employed to evaluate journal influence.18
Results
An Overview of Publications
The initial dataset comprised 2328 records. After excluding 432 non-article or non-English publications, 1896 eligible publications remained, as illustrated in the flowchart in Figure 1. The analysis revealed that 10,758 authors from 7152 institutions across 87 countries/regions contributed to the research. These publications appeared in 563 journals and cited 40,424 references.
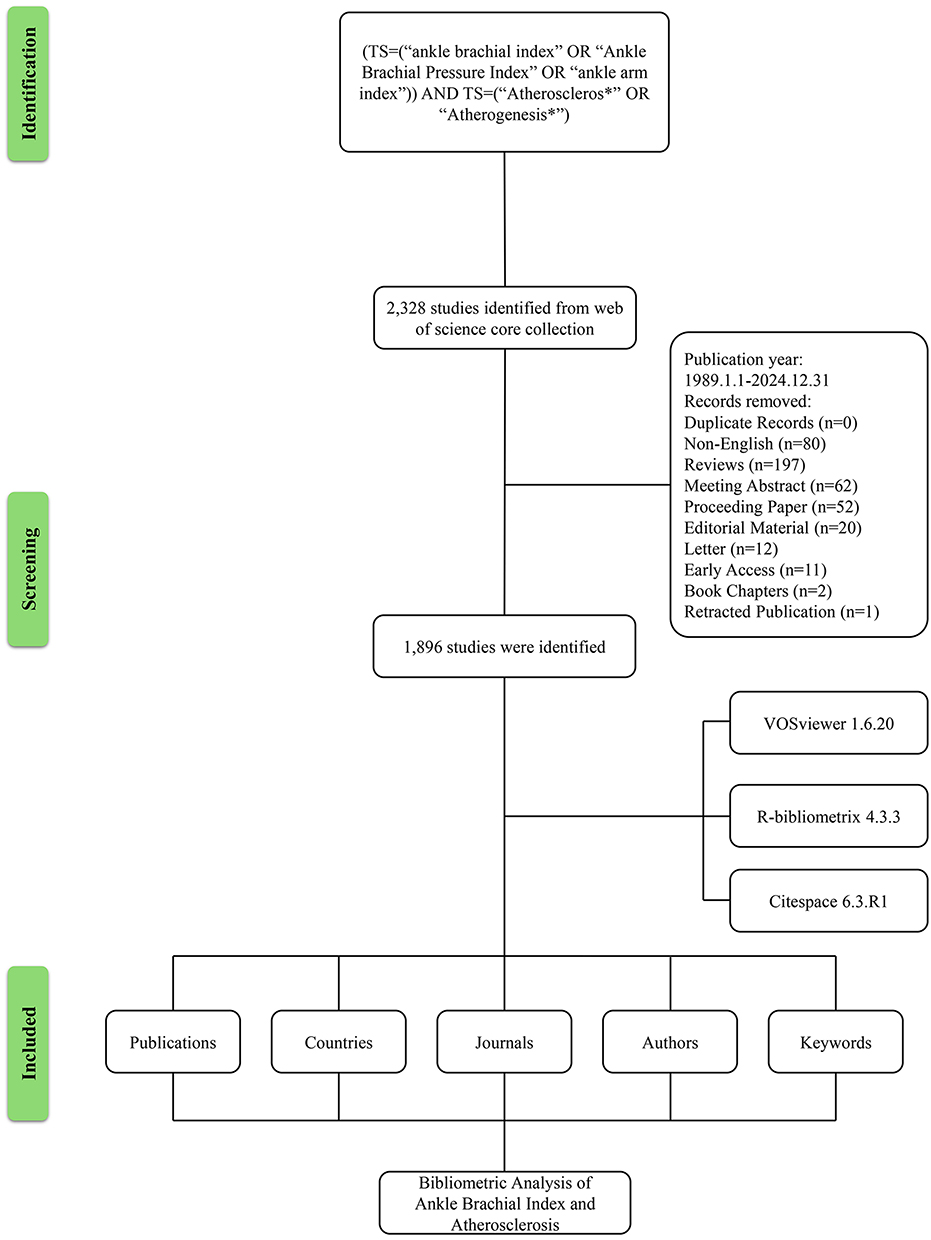 |
Figure 1 Flowchart. Flow diagram illustrating the identification, screening, eligibility, and inclusion of articles retrieved from the Web of Science Core Collection. Note: Some articles were classified under multiple document types but excluded only once, which may explain the discrepancy in exclusion counts. |
The number of publications related to ABI and atherosclerosis has shown a steady growth trend. The line chart indicates a noticeable increase in the number of publications with several significant inflection points. In 2020, the annual number of publications experienced the highest increase with an addition of 25 articles compared to the previous year. The maximum annual count was reached in 2021 when the number of articles peaked at 113 (Figure S1).
National Landscape and Research Distribution
A total of 87 countries published articles in this field. The top 20 productive countries generated 1698 articles, accounting for 89.6% of the papers worldwide. The United States was the most prolific country, publishing 448 articles, followed by China (277) and Japan (189). In terms of total citations, the United States ranked first with 29,980 citations, followed by the United Kingdom (7549) and the Netherlands (6349). The highest average citations per article were observed in the United Kingdom (88.8), followed by the Netherlands (73.8) and the United States (66.9) (Table S1). In terms of publications across multiple countries, the United States ranks first with 78,448 publications, followed by China (36,277) and the Netherlands (17,861). (Figure S2a). In addition, 56 countries with a minimum of 3 document in co-occurrence network were analyzed with VOSviewer (Figure S2b). Among them, the United States (282) had the highest total link strength with other countries, followed by and the United Kingdom (154) and Italy (116).
Institutional Contributions to ABI and Atherosclerosis
A total of 7152 institutions contributed to this field. The top 10 institutions with the highest research outputs were displayed in Figure S2c. University of California System in the United States was the leading institution with a total publication number of 232, followed by Johns Hopkins University in the United States (184) and Harvard University (164). In addition, the study revealed the cooperative relationship among 117 institutions that published a minimum of 8 documents. Among total link strength, University of Washington had the highest number of collaborations with other countries (344), followed by University of California San Diego (334) and Johns Hopkins University (242) (Figure S2d).
Journal Contributions and Impact Analysis
A total of 672 (35.4%) of the studies were published in top 20 journal based on H-index (Table S2). Among the analyzed journals, Atherosclerosis (H-index: 40), Circulation (H-index: 28), and Vascular Medicine (H-index: 23) held the top three positions in H-index rankings. In terms of total publications, Atherosclerosis ranked first with 136 publications, followed by Angiology (58), and Vascular Medicine (53). For total citations, Circulation ranked first with 5913 citations, Atherosclerosis was second with 2627, and Journal of the American College of Cardiology ranked third with 2272 citations. High-impact journals such as Circulation (IF: 35.5) and Diabetes Care (IF: 14.8) also stood out in the analysis. Most of the journals analyzed were placed in JCR Q1 and Q2. Besides, the co-occurrence networks of journals contained 99 journals with at least 4 publications. The three key journals with the highest total link strength in co-occurrence networks were Atherosclerosis (779), Circulation (656), and Journal of the American College of Cardiology (325) (Figure S3a). Additionally, the coupling network of journals contained 99 journals with at least 4 publications. The three key journals with the highest total link strength in coupling networks were the Atherosclerosis (58,476), Vascular Medicine (27,785), and Angiology (23,012) (Figure S3b).
Analysis of Publications and Cooperation Among Authors
A total of 10,755 authors contributed to this field’s publications. The top 20 authors ranked by the highest H-index were listed in Table S3. Among the analyzed authors, Criqui Michael H. had the highest H-index (30), followed by Fowkes FGR (23) and Allison Matthew A. (22). In terms of total publications, Criqui Michael H. ranked first with 65 publications, followed by Allison Matthew A. with 40, and Matsushita Kunihiro and McDermott Mary M. with 31 each. Regarding total citations, Criqui Michael H. was the most cited author (5848), followed by McDermott Mary M. (4115) and Hofman A. (3983). Additionally, the M-index indicated significant scientific advancements for Criqui Michael H. (1.50), Matsushita Kunihiro (1.25), and Allison Matthew A. (1.10). The co-occurrence network of research findings on ABI and atherosclerosis was visualized in Figure S3c, with the research results broadly categorized into 6 groups. The most collaborations with others were made by Criqui Michael H. (219), followed by Allison Matthew A. (123) and Mcdermott Mary M. (114), in order of total link strength.
Research Hot Spots and Trend Analysis
The study included 126 keywords with a minimum frequency of 20 occurrences. The top five keywords with the most frequent occurrence were “mortality” (561 occurrences), “risk-factors” (426 occurrences), “prevalence” (386 occurrences), “cardiovascular-disease” (362 occurrences), and “association” (326 occurrences). From 2010 to 2012, “c-reaction protein (CRP)”, “arm index”, and “vascular disease” emerged as key themes. Between 2012 and 2014, the “mortality”, “prevalence”, “stroke” and “blood pressure” became prominent keywords in related studies. From 2014 to 2016, the research focus deepened further, such as “prediction”, “meta analysis”, “events” and “risk” became a major topic during this period (Figure S4a).
The burst analysis of keywords in a slice from 2004 to 2024 was performed to reveal the evolution trend. The blue lines stood for the time span. The red lines represented the burst period. The strength of the top 20 keywords with the strongest bursts varied from 6.40 to 16.58 (Figure S4b). This study revealed that the term “arm index” exhibited the highest burst intensity, followed by “peripheral vascular disease”, “arterial stiffness”, and “disease”. Terms like “random forest”, “arm index” and “peripheral vascular disease” had the longest time span of outbreaks. Since 2017, the keywords “disease”, “subclinical atherosclerosis”, “arterial stiffness”, “epidemiology”, “management” and “events” had been more prominently concentrated, indicating promising developments. It was worth noting that “disease”, “epidemiology” and “events” burst lasted until 2024.
Discussion
General Information
This bibliometric analysis reveals significant growth in ABI and atherosclerosis research, with close collaboration patterns within the field. Keyword analysis suggests that future research hotspots will continue to focus on epidemiology and related areas, providing researchers with reliable insights for identifying research frontiers.
The United States leads in this field due to substantial funding, notably from the NIH. Major institutions, such as Johns Hopkins University and the University of California system, have contributed significantly through multi-center studies like the Multi-Ethnic Study of Atherosclerosis (MESA), which helped validate the ABI as a crucial tool for cardiovascular risk assessment.19 The increasing focus on ABI in countries like China and Japan reflects a growing recognition of its utility, though citation impact remains relatively lower compared to the United States.20
In Europe, institutions in the United Kingdom and the Netherlands have advanced ABI research through population-based studies, reinforcing its role as a non-invasive method for early disease detection.7 High-impact journals such as Circulation and Atherosclerosis have played a central role in disseminating influential ABI-related findings.21
Leading researchers, notably Criqui Michael H. and McDermott Mary M., have been pivotal in establishing ABI’s role in cardiovascular risk assessment. Their work in large-scale epidemiological studies, particularly MESA, provided strong evidence linking ABI abnormalities with atherosclerosis progression and adverse outcomes.22 Collaborations through institutions such as the University of California System and Northwestern University facilitated interdisciplinary studies that bridged diagnostic innovation and clinical application.
Research Hotspots and Trends Analysis
Co-Occurrence Analysis
Keyword co-occurrence analysis of ABI and atherosclerosis research from 1989 to 2024 revealed an evolving focus, highlighting how the field has expanded from basic epidemiological assessments to more specialized clinical applications. To contextualize this evolution in keyword trends, recent clinical and mechanistic studies further reinforce this trajectory. ABI has consistently been associated with subclinical carotid and coronary atherosclerosis, as demonstrated in large-scale studies such as MESA and ARIC.23,24 Moreover, experimental work suggests that abnormal ABI reflects both intimal atherosclerotic plaque and medial calcification, particularly in diabetes, offering insight into arterial remodeling mechanisms.25 These findings provide a translational bridge linking vascular biomechanics with systemic cardiovascular outcomes.
In parallel, literature over the past two decades has revealed both consensus and ongoing debate within ABI research. It is widely agreed that a low ABI (<0.9) serves as a strong and independent predictor of cardiovascular disease and subclinical atherosclerosis. Large-scale cohorts such as MESA and ARIC have consistently demonstrated that individuals with low ABI values are at elevated risk for coronary artery calcium, increased carotid intima-media thickness, and adverse cardiovascular events.23,26 However, important discrepancies remain. There is no universally accepted standard for ABI measurement, as some studies calculate ABI using the higher ankle systolic pressure while others use the lower, leading to inconsistent thresholds and comparability issues across studies.27 Furthermore, the prognostic interpretation of high ABI values (>1.4) remains controversial. While initially thought to reflect healthy arterial function, high ABI is now recognized in some populations—particularly those with diabetes or chronic kidney disease—as a marker of arterial medial calcification and reduced arterial compressibility.25 Moreover, emerging research suggests that ABI trajectories over time—such as persistent decline—may better predict myocardial infarction and heart failure risk than a single static measurement, especially in high-risk populations.28 These unresolved methodological and interpretive issues underscore the need for standardized measurement protocols and population-specific thresholds.
Inflammation and Diagnostic Tools Exploration
From 2010 to 2012, research trends highlighted the critical role of inflammatory processes in atherosclerosis, alongside significant advancements in diagnostic tool development. For instance, CRP, a prominent inflammatory biomarker, gained recognition for its potential in diagnosing vascular diseases such as atherosclerosis.29 Alongside this, the “arm index” was explored as a diagnostic tool for assessing blood flow and detecting vascular conditions. This focus significantly advanced the understanding of atherosclerosis mechanisms, leading to early detection tools that contributed to more accurate diagnostics and subsequent treatment strategies.30
Transition From Diagnostic Tools to Prognostic Indicators
From 2012 to 2014, research trends underscored the growing significance of the ABI as a potential prognostic indicator, highlighting its increasing role in predicting long-term outcomes such as stroke and cardiovascular events.12,31 However, it is important to clarify that these are associative findings derived primarily from observational cohort studies rather than causal inferences. For example, in a recent prospective cohort, individuals with ABI values at the lower end of the reference range exhibited significantly higher incidence of stroke and cardiovascular events, even after adjusting for traditional risk factors.32 Such findings support ABI’s utility as a risk stratification tool, but do not establish a direct causal relationship with adverse outcomes. Nonetheless, the consistent associations observed across diverse cohorts have informed preventive health strategies, particularly for individuals with borderline or declining ABI values.
These bibliometric trends reflect not only academic interest but also parallel changes in clinical practice. ABI has been increasingly integrated into cardiovascular risk stratification frameworks, particularly for early identification of subclinical atherosclerosis and prediction of long-term outcomes. For example, large cohort studies have demonstrated that a low ABI (<0.9) is associated with increased risk of first-onset heart failure, stroke, and coronary heart disease, especially in older adults and individuals with comorbidities. Moreover, recent evaluations support ABI as a practical and non-invasive diagnostic and prognostic tool, with high applicability in primary care and outpatient settings.33 Integrating ABI into traditional risk models, such as Framingham-REGICOR, has been shown to significantly improve cardiovascular event prediction among intermediate-risk populations.34 These findings have contributed to ABI being recognized as a risk-enhancing factor in preventive guidelines, though its implementation in routine care remains variable. Together, these developments illustrate how bibliometric growth in ABI research is increasingly aligned with its clinical adoption and utility in cardiovascular prevention strategies.
Building on these clinical recommendations, recent longitudinal evidence has increasingly emphasized ABI’s relevance to clinical outcomes. In a large national cohort, individuals with borderline ABI (0.91–0.99) had significantly elevated risk for stroke, myocardial infarction, and cardiovascular death compared to those with normal ABI, particularly in the presence of diabetes or chronic kidney disease.35 Moreover, ABI decline over time was associated with higher rates of kidney function deterioration and heart failure hospitalizations,36 highlighting its potential role in long-term disease surveillance beyond atherosclerosis.
Standardization and Precision Medicine
By 2014–2016, the field of ABI research embraced a new era centered on “prediction”, “meta-analysis”, “events” and “risk”, signifying the maturation of ABI as an essential tool for cardiovascular risk stratification. Large-scale meta-analyses began to consolidate the value of ABI in predicting cardiovascular events.12,37 Furthermore, ABI was integrated into prediction models alongside traditional risk factors, significantly improving cardiovascular risk assessments in clinical settings. For example, one study that included the ABI in a risk prediction model along with traditional risk factors, such as those used in the Framingham Risk Score, demonstrated an improvement in net reclassification, particularly in intermediate-risk subjects.38
The field has shifted from biomarker discovery, such as C-reactive protein and ABI, to epidemiological studies, and now to predictive model development. Early research focused on biomarkers’ diagnostic potential, followed by epidemiological validation and clinical integration of predictive models. Current efforts emphasize advanced statistical models to enhance ABI’s predictive accuracy for atherosclerosis mechanisms and risk stratification.
Burst Keyword Analysis and Future Directions
Burst keyword analysis reveals evolving research priorities. From 2004–2011, PVD research surged alongside advances in non-invasive diagnostics and ABI’s validation as a prognostic tool. The MESA study linked low ABI (<0.9) to subclinical atherosclerosis, solidifying PVD’s role in cardiovascular risk stratification.39 Post-2011, focus shifted to early vascular dysfunction markers, prioritizing preclinical risk prediction over late-stage disease management, with arterial stiffness emerging as a key biomarker for vascular aging before symptomatic PVD.40,41
Between 2018 and 2022, “arterial stiffness” gained prominence as an independent predictor of cardiovascular events (eg, hypertension, stroke, heart failure) and was linked to chronic diseases and early vascular aging. Advances in non-invasive methods like CAVI and ultrafast ultrasound facilitated its clinical integration.42,43 After 2022, its research declined as arterial stiffness became routine in clinical risk models, reducing its novelty.44
Since 2018, the keyword “management” reflects a shift to tailored PAD therapies, combining ABI with other vascular assessments (eg, toe-brachial index) for improved diagnostics, especially in non-compressible arteries. Aggressive risk factor control (eg, BP <130 mmHg, LDL-C <70 mg/dL) reduced cardiovascular events by 37% in high-risk patients (ABI <0.9).45,46
The 2024 focus on epidemiology highlights persistent PAD burden disparities. The ARIC study shows African Americans have a 2.1-fold higher PAD prevalence than non-Hispanic Whites, despite controlling for risk factors.47 A 10% ABI decline over 5 years predicts a 3.5-fold increased myocardial infarction risk in diabetic individuals.26 Dynamic risk models integrating ABI trends with sociodemographic factors are needed (33). Static ABI thresholds (<0.9) may be inadequate for diverse populations, requiring adaptive guidelines for race, comorbidities, and disease progression.45 While ABI is validated for PAD and cardiovascular risk, gaps remain. Low-normal ABI values correlate with higher cardiovascular event rates, but high ABI (>1.3), possibly indicating arterial calcification, is debated.32 Sex- and ethnicity-specific thresholds are underexplored, with distinct ABI risk patterns in women and non-White groups.48 Addressing these gaps is vital for tailored prevention and better risk prediction.
Research on ABI and atherosclerosis highlights the need to optimize measurement techniques. As a non-invasive tool, ABI’s measurement methods remain uncertain. A single reading may underestimate conditions, with bilateral ankle artery measurements recommended for better accuracy.49 Statistical methods like Bland-Altman analysis could reduce errors, enhancing reliability.50 The economic feasibility of large-scale ABI screening needs exploration. While cost-effective for cardiovascular risk prediction, its cost-benefit ratio for populations like those with diabetes or chronic kidney disease requires refinement.51
Strengths and Limitations
There are several highlights of our study. First, this is the first bibliometric analysis to assess the results of 35 years of research in the field of ABI and atherosclerosis worldwide. While previous bibliometric studies in related fields have mapped research outputs and trends, our analysis uniquely contributes by focusing specifically on the landscape of ABI and atherosclerosis. Second, this study provides comprehensive information such as the countries, authors, institutions and journals with the most results. However, this study has several important limitations. First, reliance solely on the WoSCC may have excluded relevant literature indexed in other major databases, such as Scopus, Embase, and PubMed, potentially affecting the comprehensiveness of the results. Second, only English-language publications were included, which may result in a geographic and linguistic bias, favoring literature from Western countries and underrepresenting emerging research from non-English-speaking regions where interest in ABI and atherosclerosis is increasing. Third, citation-based metrics are inherently biased toward older publications, which naturally have more time to accumulate citations. Finally, while tools such as VOSviewer and CiteSpace provide valuable bibliometric visualizations, their co-occurrence-based clustering does not necessarily imply conceptual or thematic agreement among clustered nodes, and should be interpreted with caution.
Conclusion
This bibliometric analysis provides an overview of research trends in ABI and atherosclerosis from 1989 to 2024. The number of publications has grown steadily, with significant contributions from the United States, China, and Japan. Co-occurrence and burst keyword analyses demonstrated a shift from basic diagnostics to epidemiological modeling and risk prediction. Future research should focus on three critical directions: (1) integrating ABI into dynamic risk prediction models using machine learning; (2) investigating population-specific disparities in ABI interpretation, particularly across sex, ethnicity, and comorbidities; and (3) re-evaluating ABI cut-off thresholds to improve diagnostic sensitivity and applicability across diverse populations.
Data Sharing Statement
All data generated or analysed during this study are included in this published article.
Acknowledgments
Jun Wang and Yanfei Tao are co-first authors for this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study was supported by Science and Technology Plan Project of Taizhou, grant number: 23ywa37 (Weiyong Hong), 23ywa41 (Jun Wang), 24ywa40 (Shu Zhang); Zhejiang Medical and Health Science and Technology Plan Project, grant number: 2024KY536 (Yanfei Tao).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Lysenko R, Riabushko R, Oksak H, Shcherban D, Skrypnyk HY, Stepanchuk A. Diagnosis and treatment of peripheral arterial disease in patients with diabetes mellitus. Актуальні проблеми сучасної медицини. 2023;23(3):198–202.
2. Aboyans V, McClelland RL, Allison MA, et al. Lower extremity peripheral artery disease in the absence of traditional risk factors. The multi-ethnic study of atherosclerosis. Atherosclerosis. 2011;214(1):169–173.
3. Brasileiro ACL, Oliveira D, Victor EG, Oliveira DAGC, Batista LL. Association between ankle-brachial index and carotid atherosclerotic disease. Arquivos brasileiros de cardiologia. 2013;100(5):422–428.
4. T KO, R MS, D G, C SP, Kumar KMP. A study of association of Ankle Brachial Index (ABI) and the Highly Sensitive C - Reactive Protein (hsCRP) in type 2 diabetic patients and in normal subjects. J Clin Diagn Res. 2013;7(1):46–50. doi:10.7860/JCDR/2012/4854.2667
5. Garg PK, Bhatia HS, Allen TS, et al. Assessment of subclinical atherosclerosis in asymptomatic people in vivo: measurements suitable for biomarker and mendelian randomization studies. Arterioscler Thromb Vasc Biol. 2024;44(1):24–47.
6. Salles Barbosa H, Tavares Contim M, Gomes Bastos M. Ankle‐brachial index and carotid ultrasound as surrogates for coronary artery disease diagnosis. J Clin Ultrasound. 2024;52(9):1296–1303. doi:10.1002/jcu.23793
7. Poredos P, Stanek A, Catalano M, Boc V. Ankle-brachial index: diagnostic tool of peripheral arterial disease and predictor of cardiovascular risk—an update of current knowledge. Angiology. 2024;00033197241226512. doi:10.1177/00033197241226512
8. Lazarides MK, Lazaridou I-Z, Papanas N. Bibliometric analysis: bridging informatics with science. Int J Low Extrem Wounds. 15347346231153538.
9. Ma J, Zhao K, Zhu Y, et al. Bibliometric analysis of monoclonal antibodies for atherosclerosis. Hum Vaccin Immunother. 2023;19(3):2266926. doi:10.1080/21645515.2023.2266926
10. Tian W, Zhang T, Wang X, Zhang J, Ju J, Xu H. Research landscape on atherosclerotic cardiovascular disease and inflammation: a bibliometric and visualized study. Rev Cardiovasc Med. 2022;23(9):317.
11. Yeung AWK. Comparison between Scopus, Web of Science, PubMed and publishers for mislabelled review papers. Curr Sci. 2019;116(11):1909–1914.
12. Hong JB, Leonards CO, Endres M, Siegerink B, Liman TG. Ankle-brachial index and recurrent stroke risk: meta-analysis. Stroke. 2016;47(2):317–322.
13. Wei N, Xu Y, Yn L, et al. A bibliometric analysis of T cell and atherosclerosis. Front Immunol. 2022;13:948314. doi:10.3389/fimmu.2022.948314
14. van Eck NJ, Waltman L. Software survey: vOSviewer, a computer program for bibliometric mapping. Scientometrics. 2010;84(2):523–538.
15. Chen Y, Lin M, Zhuang D. Wastewater treatment and emerging contaminants: bibliometric analysis. Chemosphere. 2022;297:133932.
16. Bertoli-Barsotti L, Lando T. A theoretical model of the relationship between the h-index and other simple citation indicators. Scientometrics. 2017;111(3):1415–1448.
17. Hirsch JE. An index to quantify an individual’s scientific research output. Proc Natl Acad Sci U S A. 2005;102(46):16569–16572.
18. Bornmann L, Mutz R, Daniel HD. Are there better indices for evaluation purposes than the h index? A comparison of nine different variants of the h index using data from biomedicine. J Am Soc Inf Sci Tec. 2008;59(5):830–837.
19. Miura T, Minamisawa M, Ueki Y, et al. Impressive predictive value of ankle-brachial index for very long-term outcomes in patients with cardiovascular disease: IMPACT-ABI study. PLoS One. 2017;12.
20. Wang A, Jiang R, Su Z, et al. A low ankle-brachial index is associated with cognitive impairment: the APAC study. Atherosclerosis. 2016;255:90–95. doi:10.1016/j.atherosclerosis.2016.11.005
21. Wassel CL, Berardi C, Pankow JS, et al. Soluble P-selectin predicts lower extremity peripheral artery disease incidence and change in the ankle brachial index: the multi-ethnic study of atherosclerosis (Mesa). Atherosclerosis. 2015;239(2):405–411. doi:10.1016/j.atherosclerosis.2015.01.022
22. Criqui MH, McClelland RL, McDermott MM, et al. The ankle-brachial index and incident cardiovascular events in the mesa (Multi-Ethnic Study of Atherosclerosis). J Am Coll Cardiol. 2010;56(18):1506–1512. doi:10.1016/j.jacc.2010.04.060
23. McDermott MM, Liu K, Criqui MH, et al. Ankle-brachial index and subclinical cardiac and carotid disease: the multi-ethnic study of atherosclerosis. Am J Epidemiol. 2005;162(1):33–41. doi:10.1093/aje/kwi167
24. Zheng ZJ, Sharrett AR, Chambless L, et al. Associations of ankle-brachial index with clinical coronary heart disease, stroke and preclinical carotid and popliteal atherosclerosis: the Atherosclerosis Risk in Communities (ARIC) study. Atherosclerosis. 1997;131(1):115–125. doi:10.1016/S0021-9150(97)06089-9
25. Lima A, Gonçalves MF, Rocha EV, D’Avila LBO, Mascarenhas AN. Ankle-brachial index and subclinical atherosclerosis in type 1 diabetes. Revista da Associacao Medica Brasileira. 2021;67(4):505–510.
26. Espinola-Klein C, Dopheide JF, Gori T. Change of ankle-brachial index and progression of atherosclerosis. VASA. 2013;42(2):86–87.
27. Khan TH, Farooqui FA, Niazi KA. Critical review of the ankle brachial index. Curr Cardiol Rev. 2008;4:101–106.
28. Wassel CL, Ellis AM, Suder NC, et al. Femoral artery atherosclerosis is associated with physical function across the spectrum of the ankle‐brachial index: the San Diego population study. J Am Heart Assoc. 2017;6.
29. Chotik-anuchit S, Nilanont Y, Poungvarin N. Relationship between ankle brachial index (ABI), high sensitivity C-reactive protein (hs-CRP) and initial disability level in acute ischemic stroke. J Med Assoc Thai. 2011;94(Suppl 1):S94–98.
30. Beckman JA, Preis O, Ridker PM, Gerhard-Herman MD. Comparison of usefulness of inflammatory markers in patients with versus without peripheral arterial disease in predicting adverse cardiovascular outcomes (myocardial infarction, stroke, and death). Am J Cardiol. 2005;96(10):1374–1378.
31. Tsivgoulis G, Bogiatzi C, Heliopoulos I, et al. Low ankle-brachial index predicts early risk of recurrent stroke in patients with acute cerebral ischemia. Atherosclerosis. 2012;220(2):407–412. doi:10.1016/j.atherosclerosis.2011.11.009
32. Wang FM, Yang C, Ballew SH, et al. Ankle-brachial index and subsequent risk of incident and recurrent cardiovascular events in older adults: the Atherosclerosis Risk in Communities (ARIC) study. Atherosclerosis. 2021;336:39–47. doi:10.1016/j.atherosclerosis.2021.09.028
33. Bendermacher BLW, Teijink JAW, Willigendael EM, et al. Applicability of the ankle-brachial-index measurement as screening device for high cardiovascular risk: an observational study. BMC Cardiovasc Disord. 2012;12(59):59. doi:10.1186/1471-2261-12-59
34. Velescu A, Clará A, Peñafiel J, et al. Adding low ankle brachial index to classical risk factors improves the prediction of major cardiovascular events. The REGICOR study. Atherosclerosis. 2015;241(2):357–363. doi:10.1016/j.atherosclerosis.2015.05.017
35. Suwannasom P, Phinyo P, Leemasawat K, et al. Prognostic value of ankle-brachial index in prediction of cardiovascular events in an asian population with multiple atherosclerotic risk factors. Angiology. 2022;74:848–858.
36. Aiumtrakul N, Supasyndh O, Krittayaphong R, Phrommintikul A, Satirapoj B. Ankle-brachial index predicts renal outcomes and all-cause mortality in high cardiovascular risk population: a nationwide prospective cohort study in CORE project. Int Urol Nephrol. 2021;54:1641–1652.
37. Xu D, Zou L, Xing Y, et al. Diagnostic value of ankle-brachial index in peripheral arterial disease: a meta-analysis. Can J Cardiol. 2013;29(4):492–498.
38. Fowkes F, Murray G, Butcher I, et al. Development and validation of an ankle brachial index risk model for the prediction of cardiovascular events. Eur J Prev Cardiol. 2020;21(3):310–320.
39. Kals J, Zagura M, Serg M, et al. β2-microglobulin, a novel biomarker of peripheral arterial disease, independently predicts aortic stiffness in these patients. Scand J Clin Lab Invest. 2011;71:257–263.
40. Ma T, Gu Y, Guo L, X-f L, Tong Z, Guo J-M. Trends in lower extremity peripheral arterial disease treatments and prognosis: a 10 years’ experience in single center. Zhonghua Wai Ke Za Zhi. 2015;53(4):305–309.
41. Kreutzburg T, Peters F, Rieß HC, et al. Comorbidity patterns among patients with peripheral arterial occlusive disease in Germany: a trend analysis of health insurance claims data. Eur J Vasc Endovasc Surg. 2019;59(1):59–66. doi:10.1016/j.ejvs.2019.08.006
42. Paapstel K, Kals J. Metabolomics of arterial stiffness. Metabolites. 2022;12(5):370.
43. Wang Y, Wang R, Bai L, et al. The leukocyte subtype counts and ratios can effectively predict the risk of arterial stiffness assessed by cardio-ankle vascular index: a retrospective study. Front Cardiovasc Med. 2021;8:671885.
44. Oyenuga AO, Folsom AR, Cheng S, Tanaka H, Meyer ML. Greater adherence to life’s simple 7 is associated with less arterial stiffness: the atherosclerosis risk in communities (ARIC) study. Am J Hypertens. 2019;32(8):769–776. doi:10.1093/ajh/hpz057
45. Garimella PS, Ix JH, Katz R, et al. Association of albumin-creatinine ratio and cystatin C with change in ankle-brachial index: the Multi-Ethnic Study of Atherosclerosis (Mesa). Am J Kidney Dis. 2015;65(1):33–40. doi:10.1053/j.ajkd.2014.05.014
46. Tanaka M, Ishii H, Aoyama T, et al. Ankle brachial pressure index but not brachial-ankle pulse wave velocity is a strong predictor of systemic atherosclerotic morbidity and mortality in patients on maintenance hemodialysis. Atherosclerosis. 2011;219(2):643–647.
47. Weatherley BD, Nelson JJ, Heiss G, et al. The association of the ankle-brachial index with incident coronary heart disease: the Atherosclerosis Risk In Communities (ARIC) study, 1987–2001. BMC Cardiovasc Disord. 2007;7:1–10. doi:10.1186/1471-2261-7-3
48. Singla A, Chobufo MD, Meesum A, et al. Prevalence and outcomes of low ankle brachial index by atherosclerotic cardiovascular disease risk level: insights from the National Health and Nutrition Examination Survey (NHANES). Am J Med Sci. 2023;365(2):121–129. doi:10.1016/j.amjms.2022.08.022
49. Unkart JT, Allison MA, Araneta MRG, Ix JH, Matsushita K, Criqui MH. Burden of peripheral artery disease on mortality and incident cardiovascular events: the multi-ethnic study of atherosclerosis. Am J Epidemiol. 2020;189(9):951–962. doi:10.1093/aje/kwaa051
50. Alnaji A, Law GR. PP39 research using ankle brachial pressure index statistically reassessed. J Epidemiol Community Health. 2013;67:A64–A64.
51. Maiti-abudureyimu M. Clinical application of ankle-brachial index. Adv Cardiovasc Dis. 2009.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.