Back to Journals » Research and Reports in Tropical Medicine » Volume 14
Exploring the Funding Challenges Faced by Small NGOs: Perspectives from an Organization with Practical Experience of Working in Rural Malawi
Authors Kermani F ![]() , Reandi STA
, Reandi STA
Received 12 June 2023
Accepted for publication 26 August 2023
Published 1 September 2023 Volume 2023:14 Pages 99—110
DOI https://doi.org/10.2147/RRTM.S424075
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Mario Rodríguez-Pérez
Video abstract of "Funding challenges faced by small NGOs" [ID 424075].
Views: 89
Faiz Kermani, Sbita Tia Anna Reandi
World Medical Fund, Norfolk, UK
Correspondence: Faiz Kermani, World Medical Fund, St Helen’s, Low Road, Norfolk, PE34 3FN, UK, Tel +44 1553 617 166, Email [email protected]
Abstract: Malawi is a small landlocked country in Southern Africa, which faces a number of development challenges. It is one of the world’s poorest nations and over 70% of the population live below the International Poverty Line of $2.15 per day. Health inequalities are a well-documented problem and those most affected are women and children. Non-governmental organizations (NGOs) play a vital role in supplementing government efforts to provide health services to vulnerable people in areas that are difficult to reach. The World Medical Fund (WMF) is a small medical charity that operates in the central, rural, Nkhotakota region of Malawi where many children lack access to even basic health services. To date, WMF has successfully provided free care and treatment for over 400,000 sick children, but its initiatives, such as mobile clinics, rely entirely on external donations. Since 2000, the funding resources available to small NGOs have declined and efforts to attract funding have become increasingly competitive. Frequently, the criteria used for funding decisions are too rigid, and do not reflect the difficult operating conditions on the ground in rural Africa. As one of the world’s most highly resource constrained healthcare environments, Malawi illustrates the need for more flexible funding criteria from donors so that NGOs can carry out their work to save children’s lives.
Keywords: Africa, neglected tropical diseases, mobile clinics, healthcare access, medical charities
Introduction
Malawi is a small landlocked country in Southern Africa that faces considerable ongoing challenges in its development.1–6 The country, one-third of whose surface area is made up by Lake Malawi, is frequently described as being one of the world’s poorest nations.1–3 Most of its people are rural, smallholder farmers who grow their own food and are dependent on highly variable environmental conditions and poor soil fertility.7 The economy is heavily reliant on small hold agriculture, with key crops including maize, cassava, beans, groundnuts, sweet potatoes, and several green and leafy vegetables.7 The country’s reliance on subsistence and rain-fed agriculture is viewed as limiting Malawi’s growth potential. Food insecurity is a real and constant problem.2
A comparison of Malawi with other nations in Africa (upper middle income, lower income and low income as classified by the World Bank) highlights the country’s development challenges (Table 1).5,6,8 Despite some improvements in living conditions, over 70% of the population still fall below the International Poverty Line of $2.15 per day (Table 1).5,6,8 Further complicating the situation is the widening inequalities across different levels of society. The United Nation’s 2021/2022 Human Development Report in Malawi shows that the income share held by the poorest 40%, richest 10%, and richest 1% in 2021 was 17.9%, 31.0%, and 28.0%, respectively.9
 |
Table 1 Situational Analysis: Indicators Putting Malawi into Context with Other Regional Countries (Latest Data Available)5,6,8 |
Malawi’s fragile economy continues to struggle in the face of numerous factors such as poor governance, corruption, climate shocks, high disease burden and low agricultural productivity.1,6 Like many low-income countries in Africa, health inequalities are a well-documented problem in Malawi and despite some improvements, those most affected are its women and children.10,11 For example, Malawi still has one of the highest maternal mortality rates globally, at 381 maternal deaths per 100,000 live births (Table 1).8 Child mortality is also high, with the under-5 year old mortality rate standing at nearly 42 deaths per 1,000 live births (Table 1).8
Malawi is still afflicted by a myriad of disease threats that have been successfully combatted elsewhere in the world. For example, malaria is endemic in Malawi, with an estimated 4.4 million cases reported in 2020.12 It is a leading cause of morbidity and mortality among children under 5 years in Malawi, with its prevalence in this group being 35.4%.13 In highly industrialized countries, the impact of malaria is barely recognized among the public. For example, malaria elimination (at least 3 consecutive years of zero indigenous cases as classified by the World Health Organization [WHO]) was achieved by many European countries in the early 1960s.14 In Malawi, there is a high rate of enteric pathogens and this has been related to child malnutrition.15 One study found that the rates of selected viruses and parasites in a population of asymptomatic 6, 12 and 18-month-old Malawian children, were much higher than corresponding rates for industrialized nations.15 The high rates in Malawi were linked to the poor sanitary conditions in which many children still live.15
Most of the population rely on the public health care system in Malawi which is free. It is divided into primary, secondary and tertiary levels, which are linked through a referral system.16 At face value, the system appears well set up, but in practice is beset by a range of problems, characterized by poor management, inadequate infrastructure, and a lack of resources.1,16,17 The health system has suffered from underfunding and a lack of qualified staff for a number of years which contribute to suboptimal care.16,18 Shortages of drugs and equipment in hospitals are commonplace and staff dissatisfaction and absenteeism are high.16,18 Primary care level services are overstretched and struggle to cope with patient demand.16,18 In principle, they are meant to serve an average population of 10,000 people, but some facilities may be serving up to 237,000 people.19
In this Perspectives article, based on their personal experiences, the authors wish to highlight some of the practical difficulties that small charities are facing when trying to deliver urgently needed health care in Malawi, while also highlighting opportunities to improve the funding available to such organizations. Without adequate funding, given that Malawi is one of the poorest countries in the world, charities may struggle to maintain their current abilities to provide care which will have a devastating impact on rural communities who rely on their services.
Many small non-Governmental Organizations (NGOs) work across Africa, but there are relatively few published detailed reports on exactly how they deal with practical challenges − which could serve as a guide for Malawi. It would be particularly useful to see how NGOs in Africa have tackled funding issues during the COVID-19 pandemic and the ongoing global economic slowdown. Nevertheless, it is interesting to see the similar challenges they face to NGOs operating in Malawi.
One recent report looking at Zimbabwe does reveal some common points for NGOs working in Malawi.20 Many NGOs in Zimbabwe, like in Malawi, have been unable to extend their work beyond urban settings and are hampered by poor road conditions during the rainy season (Supplementary Figure 1A and B).20 This limits their ability to reach people in rural areas, who do not have regular access to healthcare because of their location (Supplementary Figure 2).20 Obtaining funding was also highlighted as a key challenge for these NGOs, with their survival dependent on how they competed with others to reach donors.20 Even if donors were found, some of the funding criteria were so restrictive that money could only be used in a highly specific way.20 If an NGO needed to adapt to an emerging situation on the ground, it would not be able to use these funds to respond quickly as they were never originally intended for that purpose.20 Even a consultation with the donor might not lead to permission to use the funds in a new manner.20
It is also worth noting that in some other African regions, the published reports highlight very different challenges to those encountered in Malawi. One earlier report, focusing on North Darfur State in Sudan, described NGOs as facing similar challenges to raise funds but very different operational challenges in expanding their services to those in need, as armed conflict was limiting their reach.21 These organisations were stepping in to provide healthcare services in rural areas that the government was unable to because of the security situation, but then found their limited resources to be targets for armed groups.21
What is clear from other published experience in Africa is that like in Malawi (Supplementary Figure 3), with appropriate support, NGOs can strengthen healthcare systems and expand reach. For example, in Mali, between 2004 and 2018, one NGO was able to expand diabetes care as well as decentralize services.22 Previously, many of those suffering from diabetes who were surveyed had felt they had been abandoned by the healthcare system.22 Similarly, through partnership with state partners, case studies show that NGOs in Ghana helped expand services in underserved regional areas for eye care, HIV/AIDS, mental health and women’s health.23
A Role for Non-Governmental Organizations in Malawi
In 1978, 134 national government members of the World Health Organization (WHO) signed the Alma Ata Declaration.24,25 This important healthcare agreement defined primary health care as essential care and formalized this as the official health policy of all WHO member countries.24,26 Importantly, it recognized the role that non-governmental organizations (NGOs) could play in strengthening primary healthcare.26 In Africa, NGOs play an important role in the achievement of the Sustainable Development Goals (SDGs) as defined by the United Nations.22,27 To be effective, NGOs may find that they have to play a variety of roles to strengthen healthcare systems, dealing with practical challenges and collaborating with other partners they encounter in the local context.22 Africa is a region where many NGOs operate, but the scale of the challenges they face is huge and the situations in different countries, can be highly variable. This often complicates the evaluation of the effectiveness of healthcare initiatives that have been established by NGOs.
In Malawi, NGOs have a highly visible role in the healthcare system and the number of NGOs operating in the country has increased considerably since 1994.28 One such organization is the World Medical Fund (WMF), which is a small medical charity (UK Charity 1063756; SCO46207 IN Scotland) founded in 1997.3,17 The organization’s founders discovered that children in rural areas of central Malawi were effectively being denied access to medical care, due to their remote location in villages which are often over 20 kilometers away from the nearest tarmac road.3,17 Transport is extremely difficult for those in rural areas (Supplementary Figures 1A, B and 2). Although about 26% of Malawi’s total road network is paved, the rest remains unpaved and usually in very poor condition.29
WMF decided to focus on the serious healthcare challenges in the central Nkhotakota region of Malawi (Supplementary Figure 4), by the shore of Lake Malawi, an area with a high proportion of individuals who have been classed as multidimensionally poor.3,17,30 Multidimensional poverty shows how people experience poverty in multiple, overlapping ways and refers to a situation where a person who is poor suffers from multiple deprivations at the same time (such as acute deprivations in health, education, and living standards).31,32 To date, WMF has successfully provided free care and treatment for over 400,000 sick children through its regional healthcare programs, but these initiatives rely entirely on external donations.3,17
WMF’s main program involves two mobile clinic vehicles that make multiple journeys to deliver free life-saving care to sick children in rural areas (Supplementary Figures 2, and 5–7).3,17 The mobile clinic medical teams visit each village group on a 4-weekly schedule and cover a 140-kilometer distance across central Malawi (Supplementary Figure 7).3,17 NGOs working in the Nkhotakota region can face considerable challenges before being able to deliver medical treatment, given the lack of infrastructure such as paved roads, running water and reliable electricity.3,17 Extreme weather, such as Cyclone Freddy in May 2023, destroyed roads and bridges, making rural villages inaccessible. Additional factors such as economic crises affecting availability of food and fuel also hamper the work of WMF and its fellow NGOs. For example, in August 2023, The Malawi Energy Regulatory Authority confirmed continuing difficulties with maintaining the country’s fuel supply caused by foreign exchange challenges.33 Without a reliable availability of fuel, it is not possible to operate WMF’s vehicles, meaning that certain villages will miss out on a vitally required mobile clinic visit, and this could potentially increase the burden of disease in the location concerned.
NGOs play a vital role in countries, such as Malawi, which have resource-constrained healthcare environments.34 As staff shortages are a constant issue, many NGOs have sponsored the primary care training of selected individuals from rural communities to improve their skills.34 WMF works with around 150 volunteers who act as Village Health Assistants and runs a sponsorship program to support higher education for students who are studying medicine and nursing.3
NGOs can also help by improving the quality of data used to determine the effectiveness of primary care programs and should work closely with local government agencies.34 The Malawian Government uses data from NGOs, including the WMF Thandizo HIV/AIDS Center, as part of its efforts to build a national picture for the HIV/AIDS situation in Malawi. WMF has also been gathering data on other healthcare conditions using its mobile clinics, but has run into some practical issues across the region. For example, the recent COVID-19 pandemic caused severe disruption of services and the ability to collect such data. Similarly, irregular fuel supply and damage to paved roads by extreme weather has interfered with such efforts. From the available healthcare data, the team were able to collect for the period 2013 to 2019, the mobile clinics treated 223,903 children for a range of conditions across the Nkhotakota region.3 This included 73,496 cases of malaria, nearly 47,469 cases of respiratory tract infection, just under 15,000 cases of bacterial eye infections and 6,663 cases of sepsis.3
NGOs can also help by engaging with and empowering local communities in Malawi, as they have previously done for HIV/AIDS.34 To do this, NGOs must have the trust of local communities and this means understanding cultural, religious and societal issues and not making assumptions.34–36 NGO local staff can provide excellent input on regional matters. For WMF, during the COVID-19 pandemic, local staff conversations with communities in the Nkhotakota region proved essential to understand the level of misinformation and fear about this situation and how it could be addressed in a structured and sustainable way. This enabled better cooperation with local government agencies.
In Malawi, it is also important to engage with Traditional leaders, as they are influential leaders of the community.36 WMF has received valuable support from Traditional Chiefs for proposed healthcare programs in the Nkhotakota region which has contributed to their success (Supplementary Figure 3). Across the Nkhotakota region, the Traditional Chiefs are split into three clusters (north, central and south) and if WMF cannot arrange individual consultations then arrangements would be made for them to travel to a convenient location for a single meeting.
The Funding Conundrum for Small NGOs
Since 2000, the funding resources available to small NGOs have declined and the efforts to attract finances have become increasingly competitive among those operating in Malawi.28 For small NGOs, it is not possible to run the expensive public relations, marketing and social media campaigns that bigger organizations can do to attract funding, as this reduces the amount of money and time available for ongoing projects.
The restrictive funding environment has led to increasing donor demands to provide data-driven evidence that show results.28,37 This is only natural, given that funding organizations need some level of criteria by which they can assess applications from a growing number of charities. Charities that can provide information that suit such criteria are in the best position to gain funding. Yet few administrators in charge of developing the application forms for funding are likely to have first-hand experience of working in developing areas such as rural Malawi and understand the cultures and communities. This means that the information requested and provided on these forms might not be as relevant as the person evaluating the application thinks and this often leads to incorrect conclusions being drawn. Being more understanding of the practicalities and nuances of working in different areas of rural Africa could improve the process for their funding to create maximum impact.
It is a tremendous pity for those donors who are even in charge of modest funds to have their efforts misdirected by attractively displayed but flawed information, as not all projects need to be exorbitant to improve conditions on the ground. For example, mass treatment for the elimination of a number of neglected tropical diseases has been estimated at less than US$ 0.50 per person.38 Bilharzia, also called schistosomiasis, is a water-borne disease caused by a parasitic worm and can be transmitted by snails living in fresh water.3 It is highly prevalent in the lakeshore regions of Malawi, where WMF operates.3 Between 2013 and 2019, WMF’s mobile clinic teams treated nearly 9,000 cases of bilharzia.3 The drugs that can be used to treat it cost between US$ 0.03 and US$ 0.21 per person and can reduce the number of worm eggs by over 95%.39 Despite this low treatment cost and high success rate, WMF’s experience is that it remains difficult to attract even modest funding for projects to combat bilharzia in central Malawi.
In Malawi, many widely quoted statistics and data are inaccurate and simply cannot reflect the prevailing local situations faced by NGO teams on the ground.3 The poor quality of data across Africa leading to skewed conclusions has been independently documented,40–42 yet many decisions for funding continue to be made on inaccurate information. If outcome models receive poor-quality data or incorrect data, then the results will also be of poor quality. A 2018 joint report by the OECD, World Health Organization (WHO) and the World Bank concluded that poor quality healthcare was increasing the burden of illness and health costs globally.43 WMF believes that it would wise for donors to critically assess the basis of the presented data in submitted proposals as it may influence their decisions and so have a knock-on impact on healthcare on the ground.
From WMF’s own experience of trying to access accurate information, data on rural locations in Malawi are often outdated and incomplete which hampers attempts to fill out proposals to the satisfaction of some funding organizations. For example, despite the commendable array of information collected by Malawi’s National Statistics Office, its latest available report (2021) still cites data from as far back as 2015 and 2016 for certain key demographic and health indicators.44
Given that Malawi’s illiteracy rate stands at 35%45 and that corruption is acknowledged in various spheres of public life by Malawians themselves,46 it is puzzling how some charities are able to gather specific and granular data over years to suit their local projects and appear to retain funding on this basis. For small NGOs like WMF, totally reliant on external funding, this creates huge difficulties as potential donors continue to request the data and reports they are accustomed to, regardless that such information is often likely to be fragmented, or simply unrealistic, for regions like central Malawi.
Inflexible reporting structures in funding applications create a hurdle for small NGOs when trying to communicate the impact of their projects.28,37 As a result, when potential donors do not see the information they desire, they reject funding applications outright. In the absence of an actual visit by potential donors to the region to experience conditions first-hand, evaluating photographic and video evidence of conditions and outcomes might actually be a better guide, or at least a supplement, for decision-making for funding. WMF does collect data from its mobile clinic visits to villages, but caution is required in making conclusions as situations on the ground can change rapidly.3 For example, in 2018, WMF’s mobile clinics treated 12,907 cases of malaria, but this suddenly dropped to 10,986 cases in 2019.3 However, rather than claiming success against the disease, staff remained vigilant since the Nkhotakota region is a high-risk area for malaria, due to its location on the shores of Lake Malawi, which provides a breeding ground for mosquitoes.3,47 In fact, recent extreme weather events have driven very sharp rises in malaria infections and deaths across Malawi.48 On a related note, the ability to gather regular data also relies on the ability of mobile clinics to reach scheduled locations. Severe weather or lack of fuel supplies may require a cancellation or postponements of visits. Without an understanding of such factors, funders may make wrong assumption about gaps in healthcare data.
Another shortcoming is potential funding bodies overlooking the impact of investing in operational items such as logistics and staff training. Many projects may simply not sound “exciting” enough to potential donors or it may be difficult to explain their relevance to people with no previous exposure to the challenges of working in the stated region. For example, WMF staff discovered that the health of a number of the young patients at its Thandizo HIV/AIDS Center was under threat. Based on visits to the children in isolated rural areas, staff discovered that this was not because the treatments were failing, but simply because their families could not afford the very modest monthly public transport costs to the center. As a result, some of the children who had been making good progress on medication were beginning to show signs of deterioration again and subsequently performing poorly in school. In an effort to raise ring-fenced funds to cover these basic travel costs, WMF launched an initiative called the Thandizo Transport Buddy scheme whereby donors could fund individual children’s transportation costs of UK£5 per month (Supplementary Figure 8). However, in practice, and despite having case studies of its success with vulnerable children, it has proved very difficult to gain mainstream interest in this transport-focused proposal. In addition, no funding application form seems ideally structured to describe it, despite the major difference this low-cost initiative would make in ensuring children can be compliant with their various medications, particularly in the face of problems with regional and global antimicrobial resistance. With funding in place, there would no longer be the problem of missed appointments, meaning that these children could be looked after properly and carry on with their daily lives and attend school.
Developing New Healthcare Initiatives for Rural Malawi
Faced with the challenge of showcasing an evaluation framework by potential donors, WMF has been attempting to develop a model named the Passport to Health initiative (Health Education and Top-to-Toe Wellbeing Screen- Evaluation Framework).49 Since a major challenge for WMF has been to address the well-documented high morbidity and mortality rates in children, the primary focus of the initiative is to empower women and children in rural Malawi with knowledge and skills to improve health standards for themselves and their families. The Passport to Health initiative employs a two-pronged approach to achieve its objectives. Based on WMF’s previous experiences in combatting HIV/AIDS, the initiative would feature a health education program (targeted to, but not restricted to, women and children) focusing on disease reduction and good health promotion. This would be coupled with a so-called “Top-To-Toe” wellbeing screening for early recognition, detection and management of common disease and illnesses, particularly infectious diseases (Table 2).49 The “Top-To-Toe” wellbeing screening document was designed for practical use in the field by the WMF medical team (and can be made available to other NGOs by request to WMF).49 Alongside this initiative, a community flyer with the tag line “5 steps to health” has been developed to promote during the mobile clinic visits to rural villages (Supplementary Figure 9).
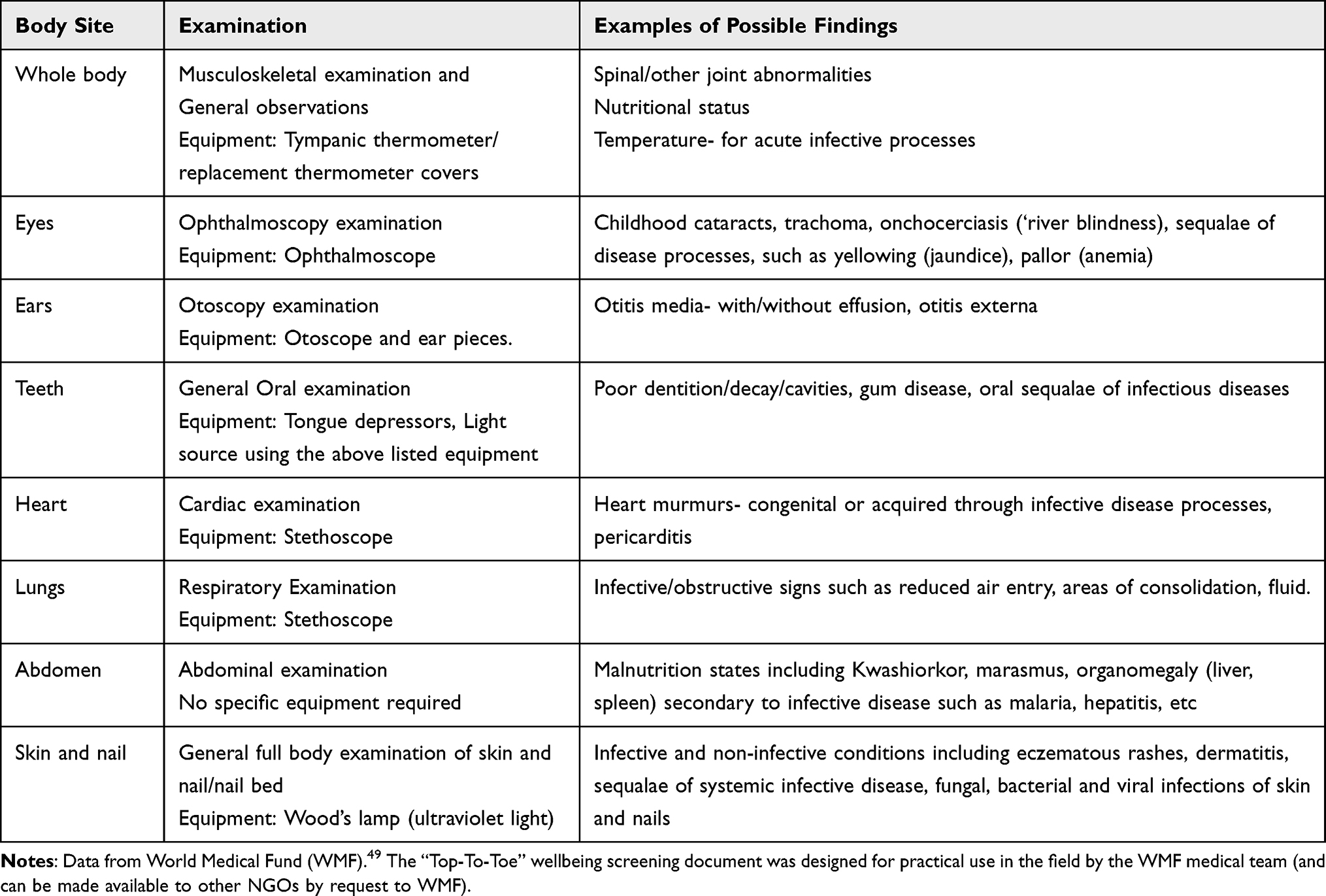 |
Table 2 WMF “Top-to-Toe” Wellbeing Screening examination |
From a review of available evaluation frameworks, WMF believes that the value and effectiveness of the Passport to Health initiative could be initially assessed under a documented 6-point evaluation framework, adapted from the Organisation for Economic Co-operation and Development (OECD) Evaluation Criteria.50 The attractiveness of the OECD framework is its international context and emphasis on practicalities and context in local settings.50 For example, the United Nations Children’s Fund (UNICEF) has had a longstanding position that its impact evaluations should be in line with these criteria.51 The OECD framework features and considerations for WMF’s Passport to Health initiative are summarized in Table 3.
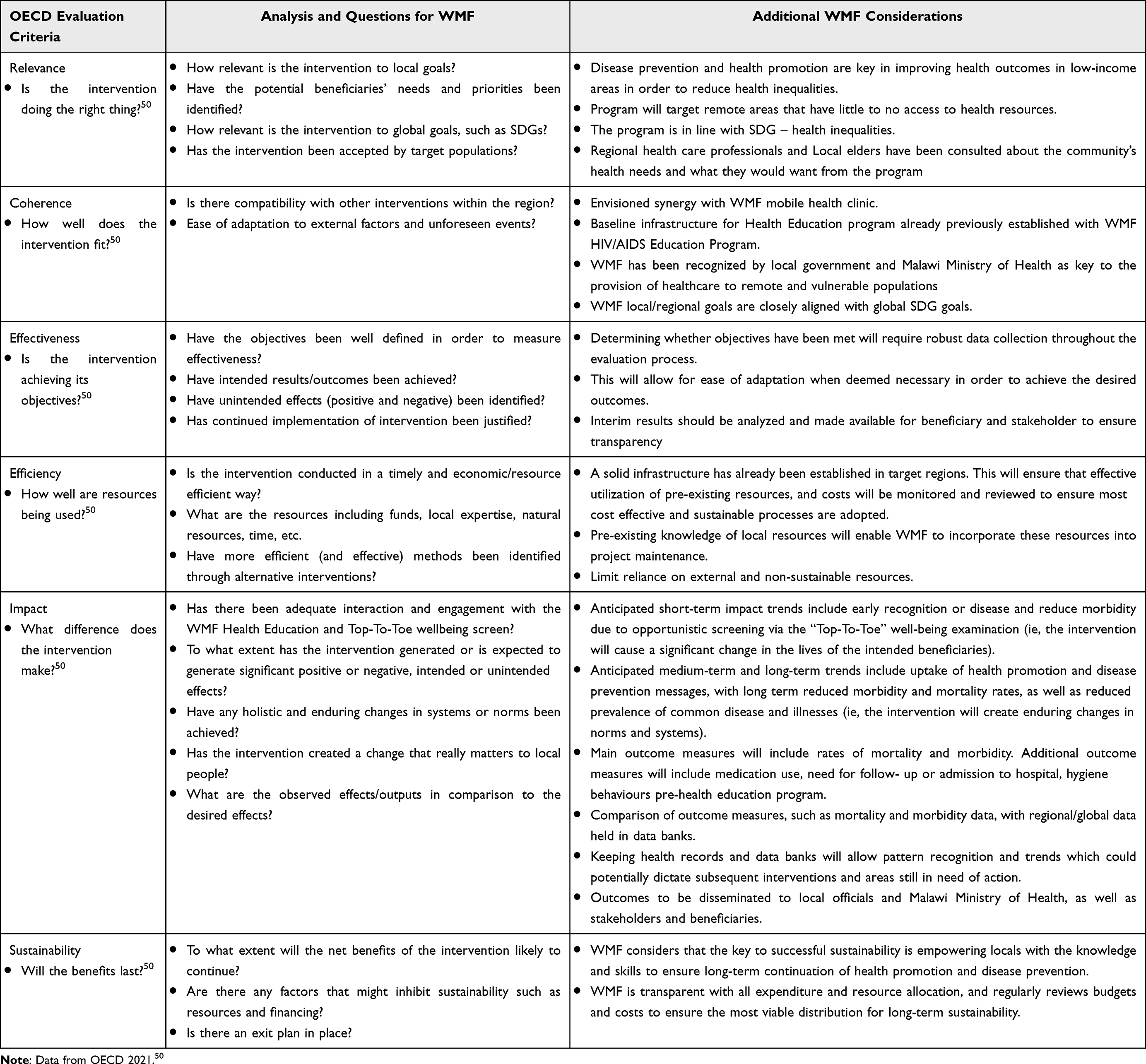 |
Table 3 Applying the OECD Evaluation criteria to WMF’s Passport to Health Initiative |
The OECD’s criteria are used to identify evaluation questions, with each criterion providing a different perspective on the intervention in question, its implementation, and its results.50 The basis of the framework are six evaluation criteria – relevance, coherence, effectiveness, efficiency, impact and sustainability, which are linked to two principles for their use.50 Principle 1 states that the criteria should be applied carefully to support high quality, useful evaluation and that they should be contextualized, such as taking into consideration the intervention being evaluated, and the stakeholders involved. Principle 2 states that the use of the criteria depends on the purpose of the evaluation.50 The criteria should not be applied mechanistically as a default. Instead, they should be covered according to the needs of the relevant stakeholders and the context of the evaluation.50
Improving the Outlook for Funding Small NGOs
In the current global economic climate, WMF is facing extreme difficulties to raise funds and meet the requirements of donors, while continuing ongoing work with its programs such as the mobile clinics. For small NGOs, such as WMF, it is not feasible to run expensive public relations, marketing and social media campaigns to attract funding, as this reduces the amount of money and time available for ongoing projects.
From the perspective of WMF, while outcome models can be helpful, they must be viewed in terms of the practical conditions faced on the ground, such as those faced by NGOs operating in rural Malawi. Funding organizations should also take careful account of factors that create operational difficulties and impact completion of application forms or hamper the generation of outcome data.28,37 For example, in Malawi, daily challenges include lack of paved roads, extreme weather conditions, lack of running water and electricity, and a shortage of suitably trained staff – all which can have a huge bearing on the impact of daily operations such as the mobile clinics. What funding organizations should always take notice of when dealing with NGOs is evidence of first hand, local knowledge and strong, established links to the community (Supplementary Figure 3), as these are the essential factors to success and sustainability in areas such as central Malawi, which may even vary from other parts of the country. Regarding outcomes, evaluation frameworks do clearly have a role to play for funding decisions and WMF is attempting to use its local knowledge to adapt available evaluation frameworks and develop the Passport to Health initiative for use in central Malawi.
Funding organizations are faced with an array of charities seeking finances and it is understandable that they have to make difficult decisions on where to direct their resources. Nevertheless, we urge potential funding bodies to show more flexibility when making their decisions on initiatives and to open a dialogue with small NGOs to better appreciate local operating conditions. NGOs like WMF have invited representatives from funding organizations to visit Malawi for themselves and see the conditions first hand, but it is rare that such offers are taken up. If there were opportunities for potential funders to experience the conditions NGOs work in and meet local communities, it would be clear how even modest, but targeted, funding could achieve meaningful results. By creating a more open-minded discussion forum with small NGOs, greater impact could be achieved on the ground, such as improving the lives of the children living in rural areas of central Malawi.
As has been shown across Africa, with the right support, NGOs can expand health services and strengthen healthcare systems (Supplementary Figure 3). In its latest national health policy report, with actions to be implemented up to 2030, the government of Malawi has acknowledged the beneficial role that local NGOs could play for its ambitions of universal health coverage.52 The government is particularly keen to provide healthcare to the estimated 3 million citizens estimated to be living outside an 8 kilometer radius of a mainstream public healthcare facility52 and this is where NGOs have particular expertise in reaching hard-to-reach populations. With the right support these NGOs could further partner with the government to ensure that it can achieve health-related SDGs and other health-related international commitments that the Government of Malawi is a signatory to.
Acknowledgments
The authors would like to thank their fellow colleagues in the World Medical Fund for their support with this paper.
Disclosure
Faiz Kermani is a Voluntary Trustee of the World Medical Fund (WMF); both authors are volunteers for the World Medical Fund (WMF). The authors report no other conflicts of interest in this work.
References
1. Masefield SC, Msosa A, Grugel J. Challenges to effective governance in a low income healthcare system: a qualitative study of stakeholder perceptions in Malawi. BMC Health Serv Res. 2020;20(1):1142. doi:10.1186/s12913-020-06002-x
2. World Bank. Malawi overview. Washington, D.C: World Bank; 2023. Available from: https://www.worldbank.org/en/country/malawi/overview.
3. World Medical Fund. Health Data Report; 2020. Available from: https://www.worldmedicalfund.org/post/wmf-health-data-report-capturing-our-life-saving-work-in-numbers.
4. Zere E, Moeti M, Kirigia J, Mwase T, Kataika E. Equity in health and healthcare in Malawi: analysis of trends. BMC Public Health. 2007;7:78. doi:10.1186/1471-2458-7-78
5. World Bank. DataBank. Available from: https://databank.worldbank.org/home.aspx.
6. World Bank. The world by income and region. Available from: https://datatopics.worldbank.org/world-development-indicators/the-world-by-income-and-region.html.
7. Kerr RB, Chilanga E, Nyantakyi-Frimpong H, Luginaah I, Lupafya E. Integrated agriculture programs to address malnutrition in northern Malawi. BMC Public Health. 2016;16(1):1197. doi:10.1186/s12889-016-3840-0
8. World Health Organization. World health statistics 2023: monitoring health for the SDGs, sustainable development goals; 2023. Available from: https://www.who.int/publications/i/item/9789240074323.
9. United Nations Development Programme (UNDP). Human development report 2021/2022: uncertain times, unsettled lives - Shaping our future in a transforming world; 2022. Available from: https://hdr.undp.org/content/human-development-report-2021-22.
10. UNICEF Malawi. The situation of children and women in Malawi; 2020. Available from: https://www.unicef.org/malawi/situation-children-and-women-malawi.
11. UNICEF. Malawi Country profile. Key demographic indicators. Available from: https://data.unicef.org/country/mwi/#child-survival.
12. Mangani C, Mzilahowa T, Cohee L, et al. Malawi ICEMR malaria research: interactions and results influencing health policies and practices. Am J Trop Med Hyg. 2022;107(4_Suppl):49–54. doi:10.4269/ajtmh.21-1265
13. Chilanga E, Collin-Vézina D, MacIntosh H, Mitchell C, Cherney K. Prevalence and determinants of malaria infection among children of local farmers in Central Malawi. Malar J. 2020;19(1):308. doi:10.1186/s12936-020-03382-7
14. World Health Organization (WHO). Countries and territories certified malaria-free by WHO. Certification of malaria elimination, 1955–2023; 2023. Available from: https://www.who.int/teams/global-malaria-programme/elimination/countries-and-territories-certified-malaria-free-by-who.
15. Fan YM, Oikarinen S, Lehto KM, et al. High prevalence of selected viruses and parasites and their predictors in Malawian children. Epidemiol Infect. 2019;147:e90. doi:10.1017/S0950268819000025
16. Makwero MT. Delivery of primary health care in Malawi. Afr J Prim Health Care Fam Med. 2018;10(1):e1–e3. doi:10.4102/phcfm.v10i1.1799
17. World Medical Fund (WMF). About us. Available from: https://www.worldmedicalfund.org.
18. Hanif R, Musvoto WS. An evaluation of funding challenges in the Malawian public healthcare delivery sector. Afr Public Serv Deliv Perform Rev. 2023;11(1):a654. doi:10.4102/apsdpr.v11i1.654
19. Schmiedeknecht K, Perera M, Schell E, Jere J, Geoffroy E, Rankin S. Predictors of workforce retention among Malawian nurse graduates of a scholarship program: a mixed-methods study. Glob Health Sci Pract. 2015;3(1):85–96. doi:10.9745/GHSP-D-14-00170
20. Kabonga I. NGOs and poverty reduction in Zimbabwe: challenges and the way forward. SN Soc Sci. 2023;3(6):90. doi:10.1007/s43545-023-00678-8
21. Yagub AI, Mtshali K. The role of non-governmental organizations in providing curative health services in North Darfur State, Sudan. Afr Health Sci. 2015;15(3):1049–1055. doi:10.4314/ahs.v15i3.48
22. Besançon S, Sidibé A, Sow DS, et al. The role of non-governmental organizations in strengthening healthcare systems in low- and middle-income countries: lessons from Santé Diabète in Mali. Glob Health Action. 2022;15(1):2061239. doi:10.1080/16549716.2022.2061239
23. Hushie M. Public-non-governmental organisation partnerships for health: an exploratory study with case studies from recent Ghanaian experience. BMC Public Health. 2016;16(1):963. doi:10.1186/s12889-016-3636-2
24. World Health Organization. Declaration of Alma-Ata.
25. World Health Organization. Declaration of Astana.
26. Rifkin SB. Alma Ata after 40 years: primary health care and health for all-from consensus to complexity. BMJ Glob Health. 2018;3(Suppl 3):e001188. doi:10.1136/bmjgh-2018-001188
27. United Nations (UN). Transforming our world: the 2030 Agenda for sustainable development. general assembly resolution A/RES/70/1. New York, USA; 2015.
28. Gooding K, Newell JN, Emmel N. Capacity to conduct health research among NGOs in Malawi: diverse strengths, needs and opportunities for development. PLoS One. 2018;13(7):e0198721. doi:10.1371/journal.pone.0198721
29. World Bank. Measuring rural access; 2017. Available from: https://documents1.worldbank.org/curated/en/543621569435525309/pdf/World-Measuring-Rural-Access-Update-2017-18.pdf.
30. The Government of Malawi National Statistical Office. The Malawi multidimensional poverty index report; 2021.
31. UNDP. What makes one poor – understanding the multidimensional poverty index; 2022. Available from: https://www.undp.org/india/stories/what-makes-one-poor-understanding-multidimensional-poverty-index.
32. Oxford Poverty & Human Development Initiative (OPHI). Global multidimensional poverty index. Available from: https://ophi.org.uk/multidimensional-poverty-index/.
33. Mhone. The Malawi energy regulatory authority. caution against fuel trade malpractices. Available from: https://mera.mw/2023/08/09/caution-against-fuel-trading-malpractices/.
34. Landes M, Pfaff C, Zerihun M, et al. Calling non-governmental organisations to strengthen primary health care: lessons following Alma-Ata. Afr J Prim Health Care Fam Med. 2019;11(1):e1–e2. doi:10.4102/phcfm.v11i1.1945
35. MacIntyre LM, Waters CM, Rankin SH, Schell E, Laviwa J, Luhanga MR. How community trust was gained by an NGO in Malawi, Central Africa, to mitigate the impact of HIV/AIDS. J Transcult Nurs. 2013;24(3):263–270. doi:10.1177/1043659613482002
36. Walsh A, Matthews A, Manda-Taylor L, et al. The role of the traditional leader in implementing maternal, newborn and child health policy in Malawi. Health Policy Plan. 2018;33(8):879–887. doi:10.1093/heapol/czy059
37. Sawadogo-Lewis T, Bryant R, Roberton T. NGO perspectives on the challenges and opportunities for real-world evaluation: a qualitative study. Glob Health Action. 2022;15(1):2088083. doi:10.1080/16549716.2022.2088083
38. Fitzpatrick C, Fleming FM, Madin-Warburton M, et al. Benchmarking the cost per person of mass treatment for selected neglected tropical diseases: an approach based on literature review and meta-regression with web-based software application. PLoS Negl Trop Dis. 2016;10(12):e0005037. doi:10.1371/journal.pntd.0005037
39. Richter R. Stanford medicine: news. Ramping up treatment of parasitic worm disease cost-effective, researchers find; 2016. Available from: https://med.stanford.edu/news/all-news/2016/06/ramping-up-treatment-of-parasitic-worm-disease-cost-effective.html.
40. Glassman A, Sandefur J. Center for global development. Why African stats are often wrong. Available from: https://www.cgdev.org/blog/why-african-stats-are-often-wrong.
41. Beguy D. Poor data hurts African countries’ ability to make good policy decisions. Quartz; 2016. Available from: https://qz.com/africa/762729/poor-data-is-hurting-african-countries-ability-to-make-good-policy-decisions.
42. Rousselot F. Africa’s health won’t improve without reliable data and collaboration. The Conversation; 2016. Available from: https://theconversation.com/africas-health-wont-improve-without-reliable-data-and-collaboration-68988.
43. World Health Organization. Low quality healthcare is increasing the burden of illness and health costs globally; 2018. Available from: https://www.who.int/news/item/05-07-2018-low-quality-healthcare-is-increasing-The-burden-of-illness-and-health-costs-globally.
44. Malawi National Statistical Office. Statistical Yearbook; 2021. Available from: http://www.nsomalawi.mw/images/stories/data_on_line/general/yearbook/Statistical_Year_Book_2021.pdf.
45. Malawi National Commission for UNESCO. Malawi’s illiteracy rate stands at 35%; 2023. Available from: https://www.malawinatcom.mw/index.php?option=com_content&view=article&id=198:malawi-s-illiteracy-rate-stand-at-35&catid=88&Itemid=280.
46. Chunga JJ, Nedi R. Malawians dissatisfied with government efforts on corruption, want swift action against corrupt officials. Afrobarometer Dispatch No. 522; 2022. Available from: https://www.afrobarometer.org/wp-content/uploads/2022/05/AD522-Malawians-demand-swift-action-against-corrupt-officials-Afrobarometer-dispatch-25may22.pdf.
47. Mategula D, Mitambo C, Sheahan W, et al. Malaria burden stratification in Malawi- A report of a consultative workshop to inform the 2023–2030 Malawi malaria strategic plan. Wellcome Open Research; 2023. Available from: https://wellcomeopenresearch.org/articles/8-178/v1.
48. Rédaction Africanews. Malaria cases spike in Malawi after deadly climate-driven disaster. Africa News; 2023. Available from: https://www.africanews.com/2023/04/24/malaria-cases-spike-in-malawi-after-deadly-climate-driven-disaster.
49. World Medical Fund (WMF). Top-to-Toe wellbeing screen- evaluation framework. A practical field document developed by WMF teams for use in the field (can be made available to other NGOs by request to WMF). Available from: https://www.worldmedicalfund.org/.
50. OECD. Applying Evaluation Criteria Thoughtfully. Paris: OECD Publishing; 2021.
51. Peersman G. Evaluative Criteria, Methodological Briefs: Impact Evaluation 3. Florence, Italy: UNICEF Office of Research; 2014.
52. The Government of Malawi. Ministry of Health. National health policy; 2023. Available from: https://www.health.gov.mw/download/national-health-policy-2/.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.