Back to Journals » Drug Design, Development and Therapy » Volume 19
Exploring the Combination of Traditional Chinese and Allopathic Medicine in the Treatment of Polycystic Ovary Syndrome from the Perspective of Modern Medicine
Authors Hu X, Zhu M ![]() , Zhou Q, Li Z, Luo L, Liang W, Chen S, Pu X
, Zhou Q, Li Z, Luo L, Liang W, Chen S, Pu X ![]() , Du J
, Du J ![]()
Received 17 October 2025
Accepted for publication 14 December 2025
Published 20 December 2025 Volume 2025:19 Pages 11395—11410
DOI https://doi.org/10.2147/DDDT.S574929
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Xiang Hu,1 Mingya Zhu,2 Qin Zhou,2 Zimo Li,2 Liping Luo,2 Wanzhi Liang,2 Shujun Chen,2 Xingwei Pu,3 Juan Du4
1TCM Prevention and Treatment of Metabolic and Chronic Diseases Key Laboratory of Sichuan Province, Hospital of Chengdu University of Traditional Chinese Medicine, Chengdu, Sichuan Province, People’s Republic of China; 2Clinical Medical College of Affiliated Hospital of Chengdu University of Traditional Chinese Medicine, Chengdu, Sichuan Province, People’s Republic of China; 3Suining Data Group Co., Ltd., Suining, Sichuan Province, People’s Republic of China; 4School of Medicine and Life Sciences, Chengdu University of Traditional Chinese Medicine, Chengdu, Sichuan Province, People’s Republic of China
Correspondence: Juan Du, School of Medicine and Life Sciences, Chengdu University of Traditional Chinese Medicine, Chengdu, Sichuan Province, 611137, People’s Republic of China, Email [email protected]
Abstract: Polycystic ovary syndrome (PCOS) is a prevalent and multifaceted endocrine disorder characterized by hyperandrogenism, ovarian dysfunction, and insulin resistance. This review aims to synthesize current evidence from both allopathic medicine and Traditional Chinese Medicine (TCM) to clarify the pathophysiological mechanisms of PCOS and evaluate the therapeutic potential of integrative management strategies. We first outline key epidemiological, genetic, and hormonal features that underpin PCOS, with particular emphasis on insulin resistance, chronic inflammation, and dysregulated gonadotropin secretion. We then summarize core TCM treatment principles and describe how herbal medicine, acupuncture, and combined therapies modulate endocrine pathways, improve metabolic homeostasis, and regulate immune–inflammatory responses. Clinical studies further suggest that TCM-based interventions may enhance ovulatory function, improve metabolic parameters, and alleviate hyperandrogenic symptoms, supporting their complementary role alongside allopathic treatments. Finally, current limitations—including variability in TCM pattern diagnosis, heterogeneity of herbal preparations, and methodological constraints in mechanistic research—are highlighted to guide future investigations. Overall, this review underscores the clinical relevance and potential value of integrative approaches that bridge traditional and modern medical frameworks in the comprehensive management of PCOS.
Keywords: PCOS, insulin resistance, hyperandrogenism, integrative medicine, traditional Chinese medicine, herbal therapy
Introduction
Polycystic ovary syndrome (PCOS) is a multifaceted endocrine disorder characterized by hyperandrogenism, menstrual irregularities, and polycystic ovaries.1 Globally, PCOS affects approximately 11–13% of women, imposing a significant health and economic burden worldwide.2–5 According to the International Evidence-based Guidelines for the Assessment and Management of Polycystic Ovary Syndrome, adult diagnosis requires at least two of these three features, whereas adolescent diagnosis necessitates the concurrent presence of hyperandrogenism and persistent menstrual irregularity due to developmental variability in ovarian morphology and anti-Müllerian hormone (AMH) levels.2
Beyond its reproductive manifestations, PCOS is strongly associated with insulin resistance, compensatory hyperinsulinemia, dysglycemia, obesity, dyslipidemia, metabolic dysfunction-associated steatotic liver disease (MASLD), and an elevated lifetime risk of type 2 diabetes mellitus.6–9 The syndrome’s presentation varies across phenotypes, ages, and ethnicities, reflecting its multifactorial pathogenesis involving endocrine, metabolic, inflammatory, and genetic factors. Despite ongoing revisions to diagnostic criteria, current frameworks remain primarily expert-opinion–based and often insufficiently capture the complexity of metabolic dysfunction in PCOS.
Given this heterogeneity, conventional allopathic therapies may not fully address the diverse clinical needs of affected women. In contrast, Traditional Chinese Medicine (TCM), with its holistic theoretical system and syndrome differentiation-guided individualized treatment, has been increasingly recognized as a potentially valuable complementary approach in PCOS management. Emerging evidence suggests that TCM may modulate multiple biological pathways relevant to PCOS, offering a multi-target regulatory framework aligned with the disorder’s multifaceted nature.
Therefore, this review aims to provide a comprehensive synthesis of current epidemiological, genetic, and pathophysiological insights into PCOS while simultaneously evaluating the theoretical foundations, mechanistic pathways, and clinical applications of TCM within the context of contemporary biomedical research. In addition, the review explores the rationale and potential advantages of integrative approaches that combine TCM with allopathic therapies to support more holistic and effective management strategies for PCOS. By articulating these objectives clearly at the outset, the review offers a structured and interdisciplinary framework intended to guide future research development and inform individualized, multimodal treatment practices for women affected by PCOS.
Epidemiology
PCOS is the most prevalent chronic endocrine disorder among women, with diagnostic criteria yet its reported prevalence varies substantially depending on diagnostic criteria, population characteristics, and methodological considerations.10,11 Population-based studies applying the Rotterdam criteria estimate a prevalence of 14%-19%,12,13 markedly higher than the 10–13% reported in earlier studies applying more restrictive definitions.14 This discrepancy underscores the strong impact of diagnostic frameworks—particularly the inclusion of polycystic ovary morphology (PCOM)—on epidemiological estimates. However, PCOM has limited specificity due to the continuous distribution of follicle numbers, age-related ovarian morphological changes, improved imaging resolution, and lack of standardized reporting.11 Similarly, AMH, despite its emerging diagnostic utility, is constrained by assay heterogeneity, absence of universally accepted cut-offs, and population-specific variability. These limitations contribute to inconsistent prevalence estimates and challenge cross-study comparisons.
Epidemiological studies also highlight notable geographic and ethnic disparities: for instance, Hispanic and African American women with PCOS exhibit higher degrees of insulin resistance than other ethnic groups,15,16 suggesting that metabolic risk profiles vary across racial backgrounds. Age is another major determinant of PCOS prevalence. Data from China indicate an increase from 10% in adolescents aged 10–20 years to 17% in women aged 21–30 years,16–18 with similar patterns observed in other cohorts.19,20 During adolescence, physiological menstrual irregularity and PCOM are common; therefore, current international guidelines advise that diagnosis in this age group be based solely on hyperandrogenism and persistent ovulatory dysfunction to avoid overdiagnosis.2,21 Conversely, in midlife, declining androgen levels and normalization of ovarian morphology may mask the phenotype, complicating diagnosis in women over 50 years,8 even though long-term cardiometabolic risks persist into perimenopause and beyond.22,23
Taken together, these epidemiological patterns demonstrate that PCOS is highly prevalent but diagnostically heterogeneous. Variability across age, ethnicity, and diagnostic methodology emphasizes the need for individualized assessment strategies. This heterogeneity also reinforces the importance of flexible, multimodal therapeutic frameworks—such as integrative approaches combining allopathic and TCM—to meet the diverse clinical presentations of PCOS.
Diagnostic Criteria
Current international evidence-based guidelines reaffirm that the three major diagnostic systems for PCOS—the National Institutes of Health (NIH) 1990 criteria,24 the Rotterdam Consensus,10 and the Androgen Excess and PCOS Society25—remain valid, with the Rotterdam framework being the most widely adopted in clinical practice (Figure 1). By allowing diagnosis based on any two of the following features—hyperandrogenism, ovulatory dysfunction, or PCOM—the Rotterdam criteria broaden phenotypic classification beyond the classic NIH definition and result in higher prevalence estimates and greater heterogeneity.11 The 2023 International Guidelines further introduce AMH levels as an alternative to ultrasound-based assessment of PCOM in adult women, although its use remains constrained by variability in assay platforms, lack of universal cut-off values, and limited validation across diverse populations.2
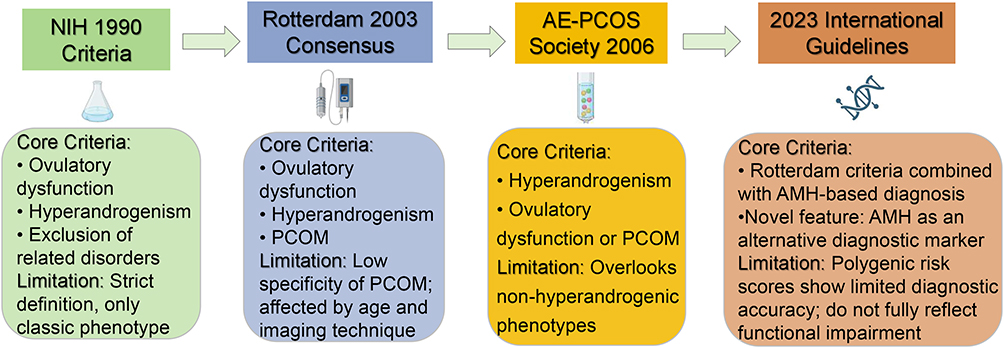 |
Figure 1 Evolution of Diagnostic Criteria for PCOS. This figure summarizes the evolution of the major diagnostic criteria for PCOS from 1990 to 2023. The NIH 1990 criteria first established PCOS diagnosis based on ovulatory dysfunction and hyperandrogenism, defining a strict, classic phenotype. The Rotterdam 2003 Consensus expanded diagnostic coverage by including PCOM, resulting in higher prevalence estimates but lower specificity. The AE-PCOS Society 2006 criteria emphasized hyperandrogenism as an essential feature while de-emphasizing PCOM. The 2023 International Guidelines integrated AMH as a new diagnostic biomarker alongside Rotterdam criteria, highlighting genetic risk and functional interpretation, but limitations remain due to population heterogeneity and the modest diagnostic power of polygenic risk scores. |
Despite their utility, current diagnostic approaches are largely consensus-based and insufficiently supported by robust empirical evidence, as noted in the 2023 guidelines.2 Notably, polygenic risk scores derived from the largest genome-wide association analyses of PCOS demonstrate modest diagnostic performance (AUC < 0.72) even among women of European ancestry, underscoring the inability of genetic profiles alone to accurately distinguish affected individuals under either the NIH or Rotterdam definitions.26,27 In summary, these limitations reveal that existing diagnostic systems capture reproductive phenotypes effectively but incompletely reflect the metabolic and functional impairments central to PCOS.
Genetics and Epigenetics of PCOS
Family and twin studies demonstrate that PCOS has a strong heritable component, with heritability estimates exceeding 70%.28,29 Early candidate-gene studies produced inconsistent findings, but advances in large-scale genome-wide association studies (GWAS) have established a robust polygenic architecture.30 Across multiple populations, including Han Chinese and European cohorts, more than a dozen reproducible susceptibility loci have been identified, particularly involving genes related to gonadotropin signaling (eg, FSHR, LHCGR, FSHB) and metabolic regulation (eg, INSR, THADA, HMGA2).31–34 Recent meta-analyses have further validated several shared and population-specific variants, reinforcing the view that PCOS arises from converging endocrine and metabolic genetic pathways.35,36 Clinically, genetic stratification studies reveal two major PCOS subtypes—“reproductive” and “metabolic”—that differ in BMI, hormonal features, and insulin resistance profiles.37–40 These genetically informed phenotypes align with emerging precision-medicine approaches and underscore the importance of individualized management strategies.
Environmental and epigenetic influences also contribute to PCOS susceptibility.41,42 Maternal hyperandrogenemia, elevated AMH levels during pregnancy, and metabolic disturbances may alter placental steroidogenesis and program PCOS-like traits in offspring.43–47 Consistent with the developmental origins hypothesis, daughters of women with PCOS exhibit increased anogenital distance and higher lifetime risk of PCOS, whereas sons demonstrate increased metabolic vulnerability.48–54 These findings imply that PCOS embodies a distinct epigenetic signature that predisposes individuals to a spectrum of reproductive, metabolic, and neuropsychiatric disorders.55,56
Epigenetic modifications involving DNA methylation, transcriptional dysregulation, and altered gamete-derived small RNAs have been observed across human and animal studies, supporting a transgenerational contribution to PCOS etiology.50,51,53 These findings help explain the heterogeneous clinical presentations of PCOS and highlight the potential role of integrative, early-life and systemic interventions—such as TCM-based metabolic and inflammatory regulation—in modifying disease expression and long-term risk.
Pathophysiology of PCOS
The pathophysiology of PCOS is complex and arises from the interplay of genetic susceptibility, developmental programming, environmental exposures, and metabolic disturbances (Figure 2). Rather than being driven by a single defect, PCOS reflects a network of interconnected abnormalities involving gonadotropin dysregulation, hyperandrogenism, insulin resistance, adipose tissue dysfunction, and chronic low-grade inflammation. These mechanisms reinforce one another, creating a self-perpetuating cycle that contributes to the heterogeneous clinical presentation of the syndrome.57
 |
Figure 2 Integrated Pathophysiological Mechanisms of PCOS. This schematic illustrates the multifactorial pathophysiology of PCOS and the interactions among endocrine, metabolic, and inflammatory disturbances. (1) Disordered gonadotropin secretion (increased GnRH pulse frequency and elevated LH/FSH ratio) stimulates excessive ovarian androgen production. (2) Hyperandrogenemia disrupts follicular maturation, inhibits ovulation, and promotes adipocyte hypertrophy with enhanced local androgen activation. (3) Adipose tissue dysfunction involves reduced GLUT4 expression and increased AKR1C3 activity, leading to impaired insulin sensitivity and abnormal lipolysis. (4) Insulin resistance arises from defective insulin signaling in skeletal muscle, liver, and adipose tissue but persists in the ovary and adrenal glands, further aggravating hyperandrogenism. (5) Chronic inflammation and oxidative stress imbalance (mediated by macrophage M1 polarization, NF-κB activation, and elevated ROS) amplify insulin resistance and ovarian dysfunction. Together, these mechanisms form a vicious cycle that perpetuates the endocrine-metabolic disturbance characteristic of PCOS. In this figure, ↑ denotes an increase or upregulation and ↓ denotes a decrease or downregulation. |
Insulin Resistance
Insulin resistance (IR) is a common but non-universal metabolic abnormality observed in women with PCOS, and importantly, it is not a diagnostic criterion for the syndrome. Nonetheless, IR contributes substantially to the metabolic and reproductive disturbances seen in many affected individuals. Gold-standard hyperinsulinemic–euglycemic clamp studies demonstrate that intrinsic defects in insulin signaling are present in approximately 60% of lean and nearly 90% of obese women with PCOS, indicating that IR can occur independently of body weight.58,59 While peripheral tissues such as skeletal muscle, adipose tissue, and the liver display blunted insulin responsiveness, the ovaries and adrenal glands retain insulin sensitivity, enabling hyperinsulinemia to directly stimulate androgen production.60,61 This tissue-specific divergence helps explain why hyperinsulinemia contributes simultaneously to metabolic dysfunction and reproductive disturbance.
Clinically, the centrality of IR to PCOS pathogenesis is underscored by parallels with severe insulin-resistant disorders. Women with type A or type B insulin resistance exhibit hyperandrogenism, menstrual irregularities, and polycystic ovarian morphology—hallmarks indistinguishable from PCOS.62–64 Hyperinsulinemia also contributes to the increased prevalence of PCOS-like features in women with obesity, type 2 diabetes mellitus, and congenital hyperinsulinemic states.8,18,65 Interventions that improve insulin sensitivity, such as metformin, are effective in lowering circulating androgen levels, restoring ovulatory function, and enhancing fertility outcomes in many women with PCOS.14 Together, these findings support the important—though not diagnostic—role of insulin resistance in the metabolic and reproductive disturbances associated with the disorder.
Gonadotropin Secretion Disorder
A defining neuroendocrine feature of PCOS is an increase in hypothalamic GnRH pulse frequency, which preferentially stimulates luteinizing hormone (LH) synthesis and results in an elevated LH/FSH ratio.66 Although the upstream mechanisms are not fully understood, growing evidence suggests that impaired negative feedback from estradiol and progesterone—partly driven by androgen excess—reduces the sensitivity of the GnRH pulse generator.67 Because GnRH neurons themselves lack sex steroid receptors, these effects are mediated through upstream kisspeptin, neurokinin B, and dynorphin A (KNDy) neurons in the arcuate nucleus.68 Dysregulation of this network promotes heightened GnRH pulsatility and amplifies LH secretion, which in turn stimulates ovarian theca cells to overproduce androgens.
In addition to these steroid–neuropeptide interactions, elevated anti-Müllerian hormone (AMH) levels—commonly seen in women with PCOS due to increased secretion from small follicles—can further potentiate GnRH activity and reinforce neuroendocrine imbalance.69,70 Clinically, these abnormalities help explain the characteristic anovulation and hyperandrogenism observed in PCOS. This neuroendocrine framework also provides a rationale for integrative therapeutic strategies: allopathic treatments focus on hormonal modulation, while TCM approaches, such as acupuncture and targeted herbal formulations, have been shown to influence hypothalamic–pituitary signaling and support menstrual cycle regulation.
Adipose Tissue Dysfunction
Adipose tissue dysfunction represents a central metabolic disturbance in PCOS and contributes to insulin resistance, chronic inflammation, and androgen excess. Advanced imaging studies indicate that visceral fat levels may not differ significantly between women with PCOS and BMI-matched controls.19,71–73 Nonetheless, accumulating evidence indicates the presence of adipocyte abnormalities and dysfunction in women with PCOS, which contributes to insulin resistance and subclinical inflammation.74–77 Women with PCOS exhibit enlarged adipocytes, and the degree of hypertrophy correlates with hyperandrogenism severity.78 Experimental data suggest that androgens impair adipocyte differentiation, reduce lipogenic capacity, and hinder the maturation of preadipocytes, thereby contributing to dysfunctional adipose expansion.79,80
Metabolic defects within adipose tissue further drive systemic insulin resistance. Despite preserved insulin receptor binding, adipocytes from women with PCOS display impaired insulin-stimulated glucose uptake linked to reduced GLUT4 expression.20 Dysregulated lipolysis increases circulating free fatty acids, promoting ectopic lipid accumulation, lipotoxicity, and inflammatory responses in non-adipose tissues.81 Elevated expression and activity of AKR1C3 in subcutaneous adipose tissue enhance local conversion of androstenedione to testosterone, augmenting androgenic tone and creating a feed-forward loop in which hyperandrogenism worsens adipocyte dysfunction and insulin resistance.82 This reciprocal relationship between adipose dysfunction, hyperinsulinemia, and androgen excess contributes substantially to the metabolic heterogeneity of PCOS.
Recognizing adipose dysfunction as a core driver of PCOS highlights the importance of multimodal management strategies. Allopathic interventions such as insulin sensitizers address metabolic deficits, whereas TCM-based approaches—including herbal therapies that modulate lipid metabolism and acupuncture protocols targeting inflammation—may provide complementary benefits by improving adipose tissue function and metabolic homeostasis.
Hyperandrogenism
Hyperandrogenism is a key endocrine hallmark of PCOS and affects approximately 60–75% of diagnosed women.83,84 Intrinsic abnormalities within ovarian theca cells—particularly enhanced expression and activity of steroidogenic enzymes—result in exaggerated androgen production, which is further amplified by the heightened sensitivity of these cells to LH stimulation.85 Although the ovary remains the primary source of androgen excess, 20–30% of women with PCOS exhibit adrenal-derived hyperandrogenism, reflecting increased ACTH responsiveness without defects in steroidogenic capacity.85
Elevated androgen levels disrupt normal folliculogenesis by promoting excessive primordial follicle recruitment and accelerating early follicle growth. This shift increases gonadotropin-independent small follicles while impairing the selection of a dominant follicle, ultimately contributing to chronic anovulation.85 Beyond reproductive dysfunction, androgen excess plays a significant role in metabolic abnormalities. Hyperandrogenism is strongly associated with adipose tissue dysfunction, characterized by enlarged adipocytes, impaired lipogenic–lipolytic balance, and dysregulated secretion of adipokines that normally support insulin sensitivity.86 These adipose changes contribute to reduced insulin-mediated glucose uptake in skeletal muscle and heighten the risk of metabolic dysfunction-associated steatotic liver disease (MASLD) in women with PCOS, even in the absence of obesity and insulin resistance.86 Emerging data also suggest that androgens may act directly on central neuroendocrine pathways, influencing energy balance and glucocorticoid signaling.86
Collectively, the reproductive and metabolic effects of androgen excess illustrate the interconnected nature of PCOS pathophysiology. These interactions underscore the rationale for multimodal interventions targeting endocrine, metabolic, and inflammatory pathways—an approach elaborated in subsequent clinical management sections.
Dysregulation of Inflammation, Oxidative Stress, and Complement Activation
PCOS is increasingly recognized as a systemic inflammatory condition, with affected women exhibiting elevated leukocyte counts, higher circulating levels of C-reactive protein, and increased proinflammatory cytokines such as IL-6 and TNF-α compared with controls.86 Adipose tissue plays a central role in in this process: infiltration by M1 macrophages is consistently observed in both lean and obese women with PCOS, contributing to localized inflammation and systemic metabolic dysfunction.87
Oxidative stress is closely intertwined with chronic inflammation in PCOS. Elevated markers of oxidative damage have been documented across multiple studies, and both oxidative stress and inflammation impair insulin signaling at the post-receptor level, thereby reinforcing insulin resistance.88 Hyperandrogenism further correlates with heightened oxidative stress and inflammatory markers, although the causal relationships among these abnormalities are still being defined.88,89
Complement system dysregulation represents an additional immune pathway implicated in PCOS. Increased activation of alternative complement components—particularly C3 and properdin—has been reported and is amplified in the presence of obesity and insulin resistance.90–92 These findings together highlight a multi-layered disturbance in immune and inflammatory regulation that contributes to reproductive dysfunction, metabolic derangements, and cardiovascular risk in PCOS. The convergence of endocrine, metabolic, and immune mechanisms also supports the use of therapeutic approaches capable of modulating multiple biological pathways.
Basic Theory of TCM Treatment of PCOS
Although TCM does not contain a disease entity directly corresponding to PCOS, its clinical manifestations align with several classical categories, including “amenorrhea”, “irregular uterine bleeding”, and “infertility”, as well as related conditions such as “obesity”, “phlegm–dampness accumulation”, and “acne”.93 Within the TCM theoretical framework, the development of PCOS is attributed to a combination of constitutional weaknesses and acquired dysfunctions involving the kidney, liver, and spleen systems—functional constructs that describe reproductive capacity, emotional regulation, metabolic transformation, and fluid transport.
TCM identifies several core pathological patterns in PCOS (Figure 3), including kidney deficiency (encompassing both yin and yang deficiency, reflected clinically in impaired reproductive function), liver qi stagnation (associated with emotional constraint and disrupted hormonal regulation), and phlegm–dampness accumulation (corresponding to metabolic disturbances such as obesity and insulin resistance). Additional pathological factors such as blood stasis, internal heat, and qi deficiency may coexist and contribute to the heterogeneity of clinical presentations. Treatment principles therefore focus on strengthening the kidney to support reproductive function, regulating qi and soothing the liver to promote hormonal balance, resolving phlegm–dampness to improve metabolic homeostasis, and invigorating blood circulation to restore ovulatory regularity.94
 |
Figure 3 TCM Theoretical Treatment for PCOS. This diagram illustrates the TCM understanding of PCOS pathogenesis and syndrome differentiation. In TCM theory, PCOS is considered a disorder “rooted in kidney deficiency”, with manifestations involving liver Qi stagnation, phlegm-dampness, and blood stasis. Pathogenic factors such as Qi deficiency, Yang deficiency, Yin deficiency, Qi stagnation, phlegm-dampness, fire heat, and blood stasis contribute to reproductive and metabolic imbalance. According to syndrome differentiation, PCOS can be classified into three predominant patterns: (1) Phlegm-dampness retention, often associated with obesity and metabolic disturbance, treated by strengthening the spleen, resolving phlegm, and eliminating dampness; (2) Liver-stagnation transforming into heat, typically linked to emotional constraint and menstrual irregularity, treated by soothing the liver, relieving stagnation, clearing heat, and regulating menstruation; (3) Kidney-Yang deficiency, associated with cold intolerance, low vitality, and subfertility, treated by warming and tonifying the kidney-yang, reinforcing Qi, and nourishing the blood. This theoretical model embodies the TCM principle of “treating both the root and the manifestations”, providing a holistic approach for individualized treatment of PCOS. |
According to the 2024 Guidelines for the Diagnosis and Treatment of Polycystic Ovary Syndrome with Integrated Traditional Chinese and Western Medicine, PCOS is primarily categorized into three major syndrome patterns: phlegm-dampness retention, kidney-yang deficiency, and liver meridian stagnation heat.93 These standardized syndrome types help guide individualized therapeutic approaches. Although rooted in traditional theory, these patterns show conceptual parallels with modern biomedical subtypes—such as metabolic-dominant PCOS or HPO axis–dominant PCOS—supporting the rationale for integrative treatment strategies that combine TCM’s holistic regulation with targeted allopathic interventions.
Mechanism of TCM in the Treatment of PCOS
TCM exerts therapeutic effects on PCOS through multi-target and multi-system regulation that aligns closely with the complex endocrine–metabolic disturbances characterizing the disorder. Rather than acting through a single pathway, TCM formulations and bioactive compounds modulate the hypothalamic–pituitary–ovarian (HPO) axis, improve insulin sensitivity, attenuate chronic inflammation, reduce oxidative stress, and influence the gut microbiota (Figure 4). These mechanisms parallel contemporary biomedical understanding of PCOS as a systemic condition driven by interacting metabolic, hormonal, and immune pathways.
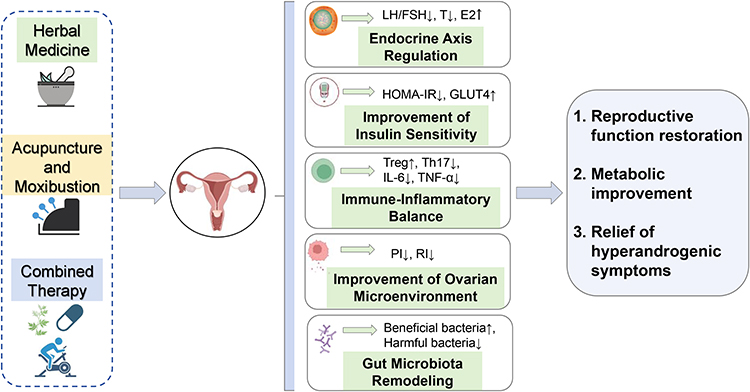 |
Figure 4 Integrated Mechanistic of TCM Treatment for PCOS. This figure illustrates the multi-target therapeutic effects of TCM interventions—including herbal medicine, acupuncture and moxibustion, and combined therapies—on PCOS. These regimens synergistically modulate multiple pathophysiological processes: (1) Endocrine axis regulation, reflected by improvements in LH/FSH balance and normalization of sex steroid levels (eg, reductions in testosterone with appropriate modulation of estradiol); (2) Improvement of insulin sensitivity, including reductions in insulin resistance indices such as HOMA-IR and upregulation of GLUT4; (3) Immune-inflammatory balance, characterized by increased Treg, decreased Th17 cells, and lowered inflammatory cytokines such as IL-6 and TNF-α; (4) Improvement of the ovarian microenvironment, including better ovarian blood flow and perfusion, often reflected by reductions in Doppler indices such as pulsatility index (PI) and resistance index (RI); and (5) Gut microbiota remodeling, with increased beneficial bacteria and decreased potentially harmful taxa. Collectively, these mechanisms restore reproductive function, improve metabolic parameters, and alleviate hyperandrogenic symptoms in women with PCOS. In this figure, ↑ denotes an increase or upregulation and ↓ denotes a decrease or downregulation. |
Several herbal compounds regulate neuroendocrine activity and restore ovulation by influencing kisspeptin–GnRH–LH signaling, a pathway central to anovulation in PCOS.95 In a study by Mingsan et al,96 total flavonoids from Cuscuta chinensis have been shown to normalize estrogen and androgen secretion and modulate HPO activity in PCOS models, providing a mechanistic explanation for traditional TCM strategies such as “tonifying the kidney” and “regulating the Chong–Ren meridians”, which aim to re-establish reproductive axis balance.
TCM formulations and monomeric constituents demonstrate insulin-sensitizing actions that complement allopathic therapies. Icariin (from Epimedium) ameliorates weight gain, improves ovarian morphology, and reduces fasting insulin and inflammatory markers in PCOS models.97 Berberine, isolated from Rhizoma Coptidis, has been shown to enhance insulin sensitivity, reduce hyperandrogenism, improve dyslipidemia, and restore estrous cyclicity.98 These findings support the TCM principles of “resolving phlegm-dampness” and “harmonizing the spleen”, which traditionally address metabolic stagnation and damp accumulation—now understood to parallel insulin signaling defects and adipose dysfunction.
Chronic low-grade inflammation contributes to anovulation and metabolic dysfunction in PCOS.99 Several TCM compounds suppress proinflammatory cytokines and modulate toll-like receptor (TLR) and NF-κB pathways. Glycyrrhizic acid (from licorice) inhibits TLR9/MyD88/NF-κB signaling and improves insulin receptor and GLUT4 activity,100–104 while emodin (from rhubarb) regulates HMGB1/TLR4/NF-κB signaling, resulting in improved metabolic profile and ovarian function.101,102 These findings correspond to TCM concepts of “clearing heat”, “resolving toxin”, and “regulating qi and blood”, offering a biomedical basis for the anti-inflammatory nature of many classical formulations.
Oxidative stress is also a significant contributor to the pathophysiology of PCOS, with elevated ROS and compromised antioxidant defenses leading to reproductive and metabolic dysfunction.105 Research has shown that Moringa oleifera extracts have demonstrated antioxidant activity that restores estrous cyclicity, improves insulin resistance, and helps normalize sex hormone profiles in animal models.106 These effects align with traditional principles of “nourishing yin” and “protecting qi”, which aim to restore internal equilibrium disrupted by oxidative injury.
Homeostasis of intestinal microbiota is integral to human health, and dysbiosis has been implicated in various diseases. In a rat model of PCOS insulin resistance, an intestinal flora imbalance was observed. Treatment with Banxia Xiexin Decoction for two weeks significantly increased the abundance of Proteobacteria, Akkermansia, and Eubacterium, while decreasing Clostridium levels. This intervention improves microbial diversity and metabolic disturbances, thereby ameliorating PCOS-associated insulin resistance.107 These findings highlight the systemic regulatory effects of herbal therapy and provide a mechanistic bridge between TCM concepts of “phlegm–dampness” and modern metabolic homeostasis.
Furthermore, TCM influences reproductive outcomes by acting on endometrial physiology.108 Salvia miltiorrhiza, a traditional Chinese medicinal herb frequently used in gynecological practice, contains cryptotanshinone as its principal bioactive constituent. Administration of 97% pure cryptotanshinone to PCOS rat models modulated endometrial tissue proliferation via the estrogen signaling pathway and improved obesity and insulin resistance parameters.109 Such actions support individualized fertility management strategies aimed at correcting ovulatory and implantation dysfunction.
Together, these findings demonstrate that TCM possesses multi-mechanistic regulatory properties that align with the interconnected endocrine, metabolic, immune, and reproductive abnormalities of PCOS. By targeting multiple biological pathways simultaneously—an inherent advantage of TCM formulations—these mechanisms provide a scientific rationale for integrative treatment strategies combining TCM with allopathic interventions, especially for phenotypes characterized by metabolic dysfunction, inflammation, or ovulatory disruption.
Extensive Practice of TCM in the Treatment of PCOS
Treatment of PCOS with TCM
Recent reproductive prognosis research underscores the importance of individualized and multifactorial management strategies for women with PCOS-related infertility. Ribeiro et al110 demonstrated that although AMH levels contribute to predicting ovarian response during IVF, age remains a stronger determinant of live birth outcomes, with markedly reduced success rates in women over 35. The study also emphasized the value of assessing cumulative rather than single-cycle live birth rates, highlighting the complexity of reproductive decision-making in PCOS. These findings reinforce the need for holistic approaches that integrate hormonal, metabolic, and age-related factors—an orientation that aligns closely with the multifactorial and individualized treatment philosophy of Traditional Chinese Medicine.
A growing body of clinical research supports the use of TCM in managing the reproductive, endocrine, and metabolic disturbances associated with PCOS. These studies, many of which adopt randomized controlled designs, suggest that TCM—whether used alone or in combination with allopathic therapies—may improve ovulatory function, metabolic profiles, endometrial receptivity, and inflammatory status. The following representative findings highlight key therapeutic patterns and their clinical implications (Table 1).
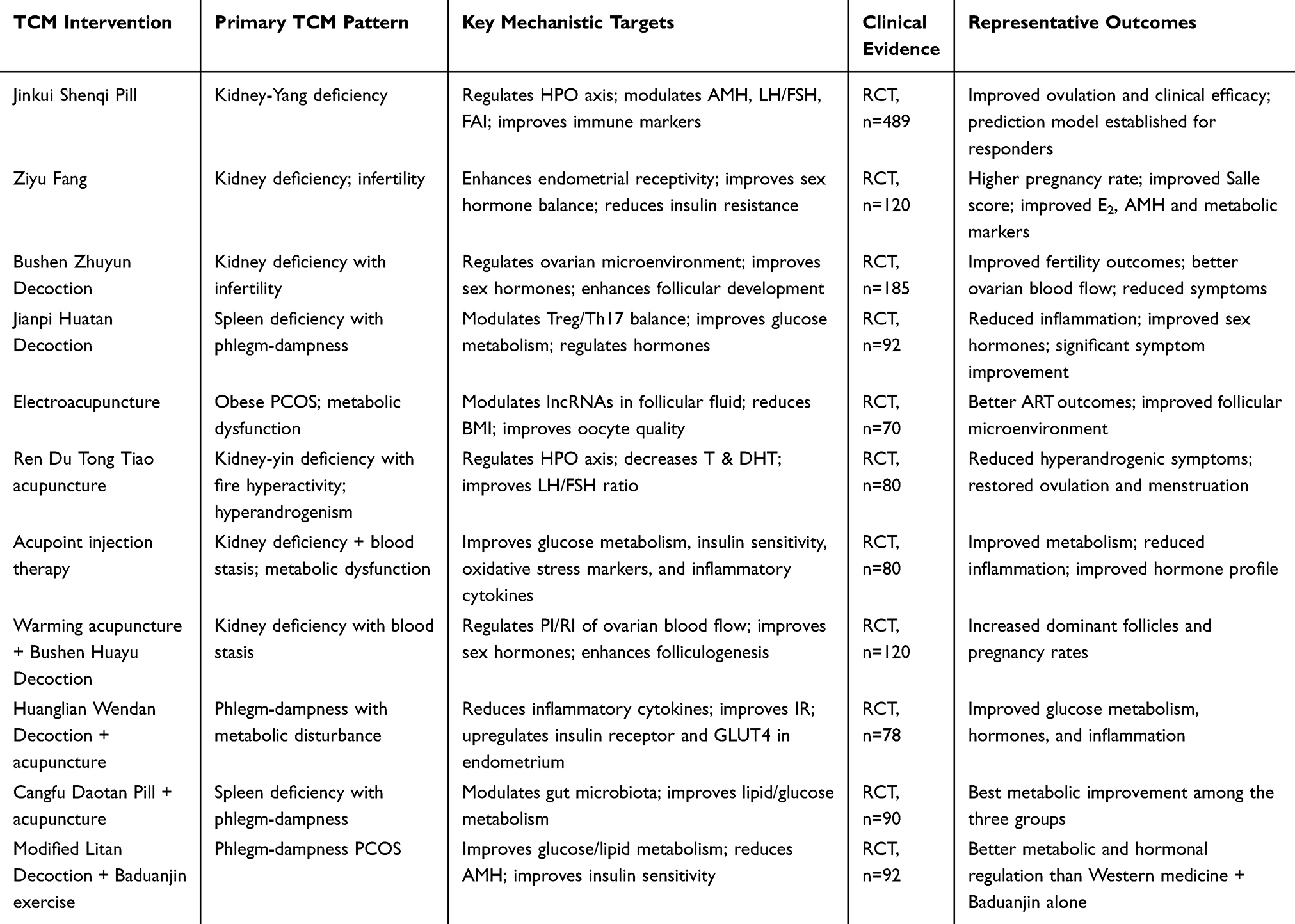 |
Table 1 Summary of Major TCM Interventions for PCOS, Their Mechanistic Targets, and Supporting Clinical Evidence |
Kidney-yang deficiency is one of the most frequently identified TCM patterns in PCOS. In a large randomized study, Jinkui Shenqi Pill combined with standard hormonal therapy improved ovulatory and clinical outcomes in patients with this pattern. The study further identified baseline factors such as AMH, FAI, LH/FSH ratio, and SHBG as predictors of treatment response, emphasizing the importance of individualized therapy within both TCM and integrative frameworks.111 Similarly, Ziyu Fang demonstrated significant improvements in clinical pregnancy rates and endometrial receptivity among infertile PCOS patients with kidney deficiency, along with favorable modulation of sex hormones and insulin resistance.112 These findings reinforce the relevance of kidney-based therapeutic strategies for reproductive dysfunction in PCOS.
Bushen Zhuyun Decoction, when administered alongside conventional Western treatment, was shown to improve sex hormone levels, enhance ovarian microenvironment indicators, and increase overall fertility outcomes in RCTs involving PCOS-related infertility.113 This synergistic effect aligns with integrative medicine principles, in which TCM’s systemic regulatory actions complement the targeted effects of allopathic agents such as ovulation inducers.
PCOS patients presenting with spleen deficiency and phlegm-dampness often exhibit prominent metabolic dysfunction and inflammatory activation. Jianpi Huatan Decoction significantly improved metabolic parameters, hormonal profiles, and clinical symptom scores in this population.114 Notably, it modulated the balance between Treg and Th17 cells—immune pathways increasingly recognized as relevant to PCOS pathophysiology—suggesting potential immunomodulatory benefits complementary to metabolic and endocrine regulation.
Taken together, these clinical studies indicate that TCM interventions can beneficially influence multiple biological systems implicated in PCOS, including reproductive endocrinology, glucose–insulin homeostasis, immune–inflammatory pathways, and endometrial receptivity. Importantly, several trials demonstrate enhanced outcomes when TCM is used adjunctively with allopathic therapies, supporting the broader integrative medicine framework emphasized throughout this review.
Treatment of PCOS with Acupuncture and Moxibustion
Acupuncture and related external TCM therapies have been increasingly studied as complementary approaches for improving reproductive, metabolic, and endocrine outcomes in PCOS. Evidence from randomized controlled trials suggests that acupuncture may regulate neuroendocrine pathways, reduce hyperandrogenism, improve insulin sensitivity, and enhance fertility—particularly when integrated with conventional therapies.
In obese women with PCOS undergoing assisted reproductive treatment, electroacupuncture has demonstrated beneficial effects on reproductive outcomes and metabolic status. An RCT involving 70 patients reported that electroacupuncture improved oocyte quality, enhanced assisted reproduction outcomes, reduced BMI, and modulated key exosomal long non-coding RNAs in follicular fluid, including TPT1-AS1, PTOV1-AS1, PTPRG-AS1, and SNHG14.115 These findings suggest that acupuncture may influence follicular microenvironment regulation and obesity-related reproductive dysfunction through molecular pathways associated with metabolic and inflammatory processes.
Ren Du Tong Tiao acupuncture has been evaluated in PCOS patients with hyperandrogenism and kidney-yin deficiency with fire hyperactivity. In an RCT enrolling 80 patients, acupuncture produced significant reductions in serum testosterone and dihydrotestosterone, improved the LH/FSH ratio, alleviated acne and hirsutism, and increased rates of ovulation and menstrual cycle restoration compared with standard hormonal therapy.116 These outcomes indicate that acupuncture may help normalize hypothalamic–pituitary–ovarian axis function and improve both clinical symptoms and ovulatory physiology.
Acupoint injection has also shown therapeutic potential in PCOS patients with metabolic abnormalities and blood stasis patterns. An RCT of 80 newly diagnosed patients found that adding acupoint injection to lifestyle intervention significantly improved glucose metabolism, insulin sensitivity (as assessed by OGTT indices and clamp-derived measures), oxidative stress markers, inflammatory cytokines, BMI, and reproductive hormone profiles compared with lifestyle modification alone.117 These findings suggest that acupoint-based therapies may support metabolic homeostasis and reduce systemic inflammation in PCOS.
TCM Combined Therapy for PCOS
Integrative approaches that combine internal herbal therapy with external TCM techniques or Western medical treatment have shown promising outcomes in managing the multifactorial reproductive, endocrine, and metabolic abnormalities of PCOS. Evidence from randomized controlled trials indicates that such combined therapies may yield superior clinical results compared with single-modality interventions.
In women with PCOS presenting with kidney deficiency and blood stasis, warming acupuncture based on the midnight–noon ebb-flow method combined with Bushen Huayu Decoction demonstrated enhanced therapeutic benefits. In a 120-patient RCT, this integrative TCM regimen improved ovarian function recovery, increased dominant follicle development, improved endometrial parameters, regulated serum sex hormone levels, and significantly increased pregnancy success rates compared with standard hormonal therapy alone.118 These findings suggest that combining targeted herbal therapy with acupuncture may optimize both ovarian and uterine environments for conception.
A second RCT evaluated the combined effect of Huanglian Wendan Decoction and acupuncture in PCOS patients characterized by metabolic disturbance. Compared with herbal medicine alone, the combined treatment produced greater reductions in LH, FSH, testosterone, fasting glucose, fasting insulin, and HOMA-IR, while also decreasing inflammatory cytokines (IL-18, IL-6, TNF-α) and enhancing endometrial insulin receptor and GLUT4 expression.119 These results highlight the potential of integrative TCM therapies to simultaneously modulate metabolic, endocrine, and inflammatory pathways.
In PCOS patients with spleen deficiency and phlegm-dampness, a 3-arm RCT demonstrated that combining Cangfu Daotan Pill with acupuncture resulted in the most substantial improvements in intestinal microbiota composition and glucose–lipid metabolism compared with either therapy alone.120 This integrative approach appears to enhance gut–metabolic regulation, supporting the emerging gut–ovary axis framework in PCOS pathophysiology.
Lifestyle-oriented integrative therapies have also been explored. In an RCT of 92 women with phlegm-dampness PCOS, modified Litan Decoction combined with Baduanjin exercise significantly improved clinical symptoms, fasting and postprandial glucose levels, HbA1c, lipid profiles, insulin resistance indices, and sex hormone levels compared with standard Western therapy plus Baduanjin.121 These findings indicate that integrating herbal therapy with mind–body exercise may provide additional benefits for metabolic and endocrine regulation.
Limitations and Future Directions
Despite growing interest and expanding research on the role of TCM in PCOS management, several limitations constrain the current evidence base. First, the absence of internationally standardized diagnostic criteria for TCM syndrome differentiation leads to considerable heterogeneity in patient classification, limiting comparability across studies and reducing the generalizability of findings. Second, variability in herbal formulations—including differences in sourcing, processing, dosage, and preparation methods—poses challenges for reproducibility and quality control, particularly in multi-center clinical research. Third, mechanistic studies often rely on animal models or simplified in vitro systems, which may not fully capture the complex endocrine–metabolic interactions present in human PCOS. Additionally, many clinical trials to date have small sample sizes, short follow-up durations, limited blinding, and inconsistencies in outcome measures, hindering the ability to draw firm conclusions regarding efficacy and safety.
Future research should prioritize the development of standardized and validated TCM diagnostic criteria, enabling more reliable syndrome differentiation and improving the methodological rigor of clinical investigations. Establishing unified herbal preparation standards, including chromatographic profiling, quality control benchmarks, and precise formulation documentation, will further strengthen reproducibility. Mechanistic studies would benefit from integrative approaches that combine molecular, cellular, multi-omics, and systems biology analyses to elucidate the multi-target regulatory effects of TCM interventions in human PCOS. Large-scale, multi-center, randomized controlled trials with longer follow-up periods, robust blinding, and harmonized clinical endpoints—such as ovulation rate, live birth rate, metabolic restoration, and quality of life—are necessary to validate therapeutic benefits.
In parallel, integrative research frameworks that systematically combine TCM with modern biomedical therapies should be advanced, as such strategies may better address the heterogeneous endocrine, metabolic, inflammatory, and reproductive features of PCOS. Through the refinement of diagnostic systems, methodological standardization, and mechanism-driven clinical trials, the field can move toward more precise, evidence-based, and personalized integrative treatments for PCOS.
Conclusion
PCOS is a complex endocrine–metabolic disorder characterized by interconnected disturbances in reproductive, metabolic, inflammatory, and neuroendocrine pathways. Traditional Chinese Medicine, through its holistic theoretical framework and syndrome differentiation–based clinical strategies, offers multi-target regulatory effects that align with the multifactorial nature of PCOS. Evidence from clinical studies indicates that TCM formulations, acupuncture, and combined integrative approaches can improve ovulatory function, metabolic parameters, hormonal balance, endometrial receptivity, and overall symptom burden.
While the mechanisms of action vary across interventions, TCM’s capacity to modulate multiple biological systems provides a complementary therapeutic dimension to allopathic treatments, supporting its value within an integrative management model. Collectively, available findings suggest that incorporating TCM into individualized, multifaceted treatment strategies may enhance clinical outcomes for women with PCOS. Further refinement of integrative approaches and continued strengthening of clinical evidence will help maximize their contribution to comprehensive PCOS care.
Acknowledgments
The authors report no acknowledgments.
Funding
Mechanism of Bushen Tianjing Therapy in Restoring Ovarian Function in a POI Mouse Model by Inducing Directed Differentiation of Ovarian Germline Stem Cells Based on the “Kidneys Govern Reproduction” Theory (2022YFS0402); Natural Science Foundation of Sichuan Province (2024NSFSC1825); Medical Research Project of the Health Commission of Sichuan Province (24QNMP002); Chengdu University of Traditional Chinese Medicine Joint Innovation Fund (WXLH202403153); Clinical experience mining research of Professor Liu Minru, master of traditional Chinese Medicine, in the treatment of polycystic ovary syndrome (syndrome of congestion of lipid membrane in the cytoplasm), a special project of Science and Technology Research of Sichuan Provincial Administration of Traditional Chinese Medicine (2023MS603).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Pereira-Eshraghi CF, Vuguin PP. Polycystic ovary syndrome. Pediatr Rev. 2024;45(6):363–365. doi:10.1542/pir.2023-006036
2. Teede HJ, Tay CT, Laven J, et al. Recommendations from the 2023 international evidence-based guideline for the assessment and management of polycystic ovary syndrome. Fertil Steril. 2023;120(4):767–793. doi:10.1016/j.fertnstert.2023.07.025
3. Azziz R, Marin C, Hoq L, et al. Health care-related economic burden of the polycystic ovary syndrome during the reproductive life span. J Clin Endocrinol Metab. 2005;90(8):4650–4658. doi:10.1210/jc.2005-0628
4. Riestenberg C, Jagasia A, Markovic D, et al. Health care-related economic burden of polycystic ovary syndrome in the United States: pregnancy-related and long-term health consequences. J Clin Endocrinol Metab. 2022;107(2):575–585. doi:10.1210/clinem/dgab613
5. Yadav S, Delau O, Bonner AJ, et al. Direct economic burden of mental health disorders associated with polycystic ovary syndrome: systematic review and meta-analysis. eLife. 2023;12:e85338. doi:10.7554/eLife.85338
6. Liu Q, Tang B, Zhu Z, et al. A genome-wide cross-trait analysis identifies shared loci and causal relationships of type 2 diabetes and glycaemic traits with polycystic ovary syndrome. Diabetologia. 2022;65(9):1483–1494. doi:10.1007/s00125-022-05746-x
7. Ruth KS, Day FR, Tyrrell J, et al. Using human genetics to understand the disease impacts of testosterone in men and women. Nat Med. 2020;26(2):252–258. doi:10.1038/s41591-020-0751-5
8. Long C, Feng H, Duan W, et al. Prevalence of polycystic ovary syndrome in patients with type 2 diabetes: a systematic review and meta-analysis. Front Endocrinol. 2022;13:980405. doi:10.3389/fendo.2022.980405
9. Azziz R, Carmina E, Chen Z, et al. Polycystic ovary syndrome. Nat Rev Dis Primers. 2016;2:16057. doi:10.1038/nrdp.2016.57
10. Rotterdam ESHRE/ASRM-Sponsored PCOS consensus workshop group. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome. Hum Reprod. 2004;19(1):41–47. doi:10.1093/humrep/deh098
11. Lizneva D, Suturina L, Walker W, et al. Criteria, prevalence, and phenotypes of polycystic ovary syndrome. Fertil Steril. 2016;106(1):6–15. doi:10.1016/j.fertnstert.2016.05.003
12. March WA, Moore VM, Willson KJ, et al. The prevalence of polycystic ovary syndrome in a community sample assessed under contrasting diagnostic criteria. Hum Reprod. 2010;25(2):544–551. doi:10.1093/humrep/dep399
13. Piltonen TT, Komsi E, Morin-Papunen LC, et al. AMH as part of the diagnostic PCOS workup in large epidemiological studies. Eur J Endocrinol. 2023;188(6):547–554. doi:10.1093/ejendo/lvad065
14. Teede HJ, Tay CT, Laven JJE, et al. Recommendations from the 2023 International Evidence-based guideline for the assessment and management of polycystic ovary syndrome. J Clin Endocrinol Metab. 2023;108(10):2447–2469. doi:10.1210/clinem/dgad463
15. Wu Q, Gao J, Bai D, et al. The prevalence of polycystic ovarian syndrome in Chinese women: a meta-analysis. Ann Palliat Med. 2021;10(1):74–87. doi:10.21037/apm-20-1893
16. Moran C, Arriaga M, Rodriguez G, et al. Obesity differentially affects phenotypes of polycystic ovary syndrome. Int J Endocrinol. 2012;2012:317241. doi:10.1155/2012/317241
17. Teede HJ, Joham AE, Paul E, et al. Longitudinal weight gain in women identified with polycystic ovary syndrome: results of an observational study in young women. Obesity. 2013;21(8):1526–1532. doi:10.1002/oby.20213
18. Kataoka J, Larsson I, Björkman S, et al. Prevalence of polycystic ovary syndrome in women with severe obesity: effects of a structured weight loss programme. Clin Endocrinol. 2019;91(6):750–758. doi:10.1111/cen.14098
19. Zhu S, Li Z, Hu C, et al. Imaging-based body fat distribution in polycystic ovary syndrome: a systematic review and meta-analysis. Front Endocrinol. 2021;12:697223. doi:10.3389/fendo.2021.697223
20. Bril F, Ezeh U, Amiri M, et al. Adipose tissue dysfunction in polycystic ovary syndrome. J Clin Endocrinol Metab. 2023;109(1):10–24. doi:10.1210/clinem/dgad356
21. Van Keizerswaard J, Dietz de Loos ALP, Louwers YV, et al. Changes in individual polycystic ovary syndrome phenotypical characteristics over time: a long-term follow-up study. Fertil Steril. 2022;117(5):1059–1066. doi:10.1016/j.fertnstert.2022.01.014
22. Kujanpää L, Arffman RK, Pesonen P, et al. Women with polycystic ovary syndrome are burdened with multimorbidity and medication use independent of body mass index at late fertile age: a population-based cohort study. Acta Obstet Gynecol Scand. 2022;101(7):728–736. doi:10.1111/aogs.14382
23. Ollila MM, Arffman RK, Korhonen E, et al. Women with PCOS have an increased risk for cardiovascular disease regardless of diagnostic criteria: a prospective population-based cohort study. Eur J Endocrinol. 2023;189(1):96–105. doi:10.1093/ejendo/lvad077
24. Zawadzki JK, Dunaif. Diagnostic criteria for polycystic ovary syndrome: towards a rational approach. In: Polycystic Ovary Syndrome. Boston; 1992:77–84.
25. Azziz R, Carmina E, Dewailly D, et al. Criteria for defining polycystic ovary syndrome as a predominantly hyperandrogenic syndrome: an Androgen Excess Society guideline. J Clin Endocrinol Metab. 2006;91(11):4237–4245.
26. Day F, Karaderi T, Jones MR, et al. Large-scale genome-wide meta-analysis of polycystic ovary syndrome suggests shared genetic architecture for different diagnosis criteria. PLoS Genet. 2018;14(12):e1007813. doi:10.1371/journal.pgen.1007813
27. Joo YY, Actkins K, Pacheco JA, et al. Polygenic and phenotypic risk prediction for polycystic ovary syndrome evaluated by phenome-wide association studies. J Clin Endocrinol Metab. 2020;105(6):1918–1936. doi:10.1210/clinem/dgz326
28. Legro RS, Driscoll D, Strauss JF III, et al. Evidence for a genetic basis for hyperandrogenemia in polycystic ovary syndrome. Proc Natl Acad Sci USA. 1998;95(25):14956–14960. doi:10.1073/pnas.95.25.14956
29. Vink JM, Sadrzadeh S, Lambalk CB, et al. Heritability of polycystic ovary syndrome in a Dutch twin-family study. J Clin Endocrinol Metab. 2006;91(6):2100–2104. doi:10.1210/jc.2005-1494
30. Laven JSE. Follicle-stimulating hormone receptor (FSHR) polymorphisms and polycystic ovary syndrome (PCOS). Front Endocrinol. 2019;10:23. doi:10.3389/fendo.2019.00023
31. Chen ZJ, Zhao H, He L, et al. Genome-wide association study identifies susceptibility loci for polycystic ovary syndrome on chromosome 2p16.3, 2p21, and 9q33.3. Nat Genet. 2011;43(1):55–59. doi:10.1038/ng.732
32. Day FR, Hinds DA, Tung JY, et al. Causal mechanisms and balancing selection inferred from genetic associations with polycystic ovary syndrome. Nat Commun. 2015;6:8464. doi:10.1038/ncomms9464
33. Hayes MG, Urbanek M, Ehrmann DA, et al. Genome-wide association of polycystic ovary syndrome implicates alterations in gonadotropin secretion in European ancestry populations. Nat Commun. 2015;6:7502. doi:10.1038/ncomms8502
34. Shi Y, Zhao H, Shi Y, et al. Genome-wide association study identifies eight new risk loci for polycystic ovary syndrome. Nat Genet. 2012;44(9):1020–1025. doi:10.1038/ng.2384
35. Sharma P, Bhatia K, Singh Kapoor H, et al. Genetic variants of metabolism and inflammatory pathways and PCOS risk: systematic review, meta-analysis, and in-silico analysis. Gene. 2023;888:147796. doi:10.1016/j.gene.2023.147796
36. Sharma P, Kumar Singh A, Senapati S, et al. Genetic variants of steroidogenesis and gonadotropin pathways and polycystic ovary syndrome susceptibility: a systematic review and meta-analysis. Metab Syndr Relat Disord. 2024;22(1):15–26. doi:10.1089/met.2023.0127
37. Goodarzi MO. Genetics of common endocrine disease: the present and the future. J Clin Endocrinol Metab. 2016;101(3):787–794. doi:10.1210/jc.2015-3640
38. Dapas M, Lin FTJ, Nadkarni GN, et al. Distinct subtypes of polycystic ovary syndrome with novel genetic associations: an unsupervised phenotypic clustering analysis. PLoS Med. 2020;17(6):e1003132. doi:10.1371/journal.pmed.1003132
39. Burns K, Mullin BH, Moolhuijsen LME, et al. Body mass index–stratified meta-analysis of genome-wide association studies of polycystic ovary syndrome in women of European ancestry. BMC Genomics. 2024;25(1):208. doi:10.1186/s12864-024-09990-w
40. Zhu J, Pujol-Gualdo N, Wittemans LBL, et al. Evidence from men for ovary-independent effects of genetic risk factors for polycystic ovary syndrome. J Clin Endocrinol Metab. 2022;107(4):e1577–e1587. doi:10.1210/clinem/dgab838
41. Cesta CE, Öberg AS, Ibrahimson A, et al. Maternal polycystic ovary syndrome and risk of neuropsychiatric disorders in offspring: prenatal androgen exposure or genetic confounding? Psychol Med. 2020;50(4):616–624. doi:10.1017/s0033291719000424
42. Stener-Victorin E, Deng Q. Epigenetic inheritance of polycystic ovary syndrome: challenges and opportunities for treatment. Nat Rev Endocrinol. 2021;17(9):521–533. doi:10.1038/s41574-021-00517-x
43. Kent J, Dodson WC, Kunselman A, et al. Gestational weight gain in women with polycystic ovary syndrome: a controlled study. J Clin Endocrinol Metab. 2018;103(11):4315–4323. doi:10.1210/jc.2017-02764
44. Tata B, Mimouni NEH, Barbotin AL, et al. Elevated prenatal anti-Müllerian hormone reprograms the fetus and induces polycystic ovary syndrome in adulthood. Nat Med. 2018;24(6):834–846. doi:10.1038/s41591-018-0035-5
45. Maliqueo M, Lara HE, Sánchez F, et al. Placental steroidogenesis in pregnant women with polycystic ovary syndrome. Eur J Obstet Gynecol Reprod Biol. 2013;166(2):151–155. doi:10.1016/j.ejogrb.2012.10.015
46. Maliqueo M, Sundström Poromaa I, Vanky E, et al. Placental STAT3 signaling is activated in women with polycystic ovary syndrome. Hum Reprod. 2015;30(3):692–700. doi:10.1093/humrep/deu351
47. Gautam R, Prambil AM, Patel AK, et al. Emerging pollutants in etiology and pathophysiology of polycystic ovary syndrome. Reprod Toxicol. 2024;123:108515. doi:10.1016/j.reprotox.2023.108515
48. Barker DJ, Osmond C, Law CM. The intrauterine and early postnatal origins of cardiovascular disease and chronic bronchitis. J Epidemiol Community Health. 1989;43(3):237–240. doi:10.1136/jech.43.3.237
49. Barrett ES, Hoeger KM, Sathyanarayana S, et al. Anogenital distance in newborn daughters of women with polycystic ovary syndrome indicates fetal testosterone exposure. J Dev Orig Health Dis. 2018;9(3):307–314. doi:10.1017/s2040174417001118
50. Risal S, Pei Y, Lu H, et al. Prenatal androgen exposure and transgenerational susceptibility to polycystic ovary syndrome. Nat Med. 2019;25(12):1894–1904. doi:10.1038/s41591-019-0666-1
51. Mimouni NEH, Paiva I, Barbotin AL, et al. Polycystic ovary syndrome is transmitted via a transgenerational epigenetic process. Cell Metab. 2021;33(3):513–530.e8. doi:10.1016/j.cmet.2021.01.004
52. Chen X, Koivuaho E, Piltonen TT, et al. Association of maternal polycystic ovary syndrome or anovulatory infertility with obesity and diabetes in offspring: a population-based cohort study. Hum Reprod. 2021;36(8):2345–2357. doi:10.1093/humrep/deab112
53. Risal S, Li C, Luo Q, et al. Transgenerational transmission of reproductive and metabolic dysfunction in the male progeny of polycystic ovary syndrome. Cell Rep Med. 2023;4(5):101035. doi:10.1016/j.xcrm.2023.101035
54. Lambertini L, Saul SR, Copperman AB, et al. Intrauterine reprogramming of the polycystic ovary syndrome: evidence from a pilot study of cord blood global methylation analysis. Front Endocrinol. 2017;8:352. doi:10.3389/fendo.2017.00352
55. Risal S, Manti M, Lu H, et al. Prenatal androgen exposure causes a sexually dimorphic transgenerational increase in offspring susceptibility to anxiety disorders. Transl Psychiatry. 2021;11(1):45. doi:10.1038/s41398-020-01183-9
56. Dubey P, Thakur B, Rodriguez S, et al. A systematic review and meta-analysis of the association between maternal polycystic ovary syndrome and neuropsychiatric disorders in children. Transl Psychiatry. 2021;11(1):569. doi:10.1038/s41398-021-01699-8
57. Helvaci N, Yildiz BO. Polycystic ovary syndrome as a metabolic disease. Nat Rev Endocrinol. 2025;21(4):230–244. doi:10.1038/s41574-024-01057-w
58. Cassar S, Misso ML, Hopkins WG, et al. Insulin resistance in polycystic ovary syndrome: a systematic review and meta-analysis of euglycaemic–hyperinsulinaemic clamp studies. Hum Reprod. 2016;31(11):2619–2631. doi:10.1093/humrep/dew243
59. Tosi F, Bonora E, Moghetti P. Insulin resistance in a large cohort of women with polycystic ovary syndrome: comparison between euglycaemic–hyperinsulinaemic clamp and surrogate indexes. Hum Reprod. 2017;32(12):2515–2521. doi:10.1093/humrep/dex308
60. Diamanti-Kandarakis E, Dunaif A. Insulin resistance and the polycystic ovary syndrome revisited: an update on mechanisms and implications. Endocr Rev. 2012;33(6):981–1030. doi:10.1210/er.2011-1034
61. Zhao H, Zhang J, Cheng X, et al. Insulin resistance in polycystic ovary syndrome across various tissues: an updated review of pathogenesis, evaluation, and treatment. J Ovarian Res. 2023;16(1):9. doi:10.1186/s13048-022-01091-0
62. Angelidi AM, Filippaios A, Mantzoros CS. Severe insulin resistance syndromes. J Clin Invest. 2021;131(4). doi:10.1172/jci142245
63. Lungu AO, Zadeh ES, Goodling A, et al. Insulin resistance is a sufficient basis for hyperandrogenism in lipodystrophic women with polycystic ovarian syndrome. J Clin Endocrinol Metab. 2012;97(2):563–567. doi:10.1210/jc.2011-1896
64. Malek R, Chong AY, Lupsa BC, et al. Treatment of type B insulin resistance: a novel approach to reduce insulin receptor autoantibodies. J Clin Endocrinol Metab. 2010;95(8):3641–3647. doi:10.1210/jc.2010-0167
65. Bayona A, Martínez-Vaello V, Zamora J, et al. Prevalence of PCOS and related hyperandrogenic traits in premenopausal women with type 1 diabetes: a systematic review and meta-analysis. Hum Reprod Update. 2022;28(4):501–517. doi:10.1093/humupd/dmac011
66. Ruddenklau A, Campbell RE. Neuroendocrine impairments of polycystic ovary syndrome. Endocrinology. 2019;160(10):2230–2242. doi:10.1210/en.2019-00428
67. Moore AM. Impaired steroid hormone feedback in polycystic ovary syndrome: evidence from preclinical models for abnormalities within central circuits controlling fertility. Clin Endocrinol. 2022;97(2):199–207. doi:10.1111/cen.14711
68. Garg A, Patel B, Abbara A, et al. Treatments targeting neuroendocrine dysfunction in polycystic ovary syndrome (PCOS). Clin Endocrinol. 2022;97(2):156–164. doi:10.1111/cen.14704
69. Cimino I, Casoni F, Liu X, et al. Novel role for anti-Müllerian hormone in the regulation of GnRH neuron excitability and hormone secretion. Nat Commun. 2016;7:10055. doi:10.1038/ncomms10055
70. Dewailly D, Barbotin AL, Dumont A, et al. Role of anti-Müllerian hormone in the pathogenesis of polycystic ovary syndrome. Front Endocrinol. 2020;11:641. doi:10.3389/fendo.2020.00641
71. Franks S, Stark J, Hardy K. Follicle dynamics and anovulation in polycystic ovary syndrome. Hum Reprod Update. 2008;14(4):367–378. doi:10.1093/humupd/dmn015
72. Barber TM, Golding SJ, Alvey C, et al. Global adiposity rather than abnormal regional fat distribution characterizes women with polycystic ovary syndrome. J Clin Endocrinol Metab. 2008;93(3):999–1004. doi:10.1210/jc.2007-2117
73. Mannerås-Holm L, Leonhardt H, Kullberg J, et al. Adipose tissue has aberrant morphology and function in PCOS: enlarged adipocytes and low serum adiponectin, but not circulating sex steroids, are strongly associated with insulin resistance. J Clin Endocrinol Metab. 2011;96(2):E304–E311. doi:10.1210/jc.2010-1290
74. Ezeh U, Chen IY, Chen YH, et al. Adipocyte expression of glucose transporter 1 and 4 in PCOS: relationship to insulin-mediated and non-insulin-mediated whole-body glucose uptake. Clin Endocrinol. 2019;90(4):542–552. doi:10.1111/cen.13931
75. Ezeh U, Arzumanyan Z, Lizneva D, et al. Alterations in plasma non-esterified fatty acid kinetics and relationship with insulin resistance in polycystic ovary syndrome. Hum Reprod. 2019;34(2):335–344. doi:10.1093/humrep/dey356
76. Ezeh U, Chen IY, Chen YH, et al. Adipocyte insulin resistance in PCOS: relationship with GLUT4 expression and whole-body glucose disposal and β-cell function. J Clin Endocrinol Metab. 2020;105(7):e2408–e2420. doi:10.1210/clinem/dgaa235
77. Dumesic DA, Phan JD, Leung KL, et al. Adipose insulin resistance in normal-weight women with polycystic ovary syndrome. J Clin Endocrinol Metab. 2019;104(6):2171–2183. doi:10.1210/jc.2018-02086
78. Echiburu B, Pérez-Bravo F, Galgani JE, et al. Enlarged adipocytes in subcutaneous adipose tissue associated with hyperandrogenism and visceral adipose tissue volume in women with polycystic ovary syndrome. Steroids. 2018;130:15–21. doi:10.1016/j.steroids.2017.12.009
79. Blouin K, Nadeau M, Perreault M, et al. Effects of androgens on adipocyte differentiation and adipose tissue explant metabolism in men and women. Clin Endocrinol. 2010;72(2):176–188. doi:10.1111/j.1365-2265.2009.03645.x
80. Chazenbalk G, Singh P, Irge D, et al. Androgens inhibit adipogenesis during human adipose stem cell commitment to preadipocyte formation. Steroids. 2013;78(9):920–926. doi:10.1016/j.steroids.2013.05.001
81. Dumesic DA, Padmanabhan V, Chazenbalk GD, et al. Polycystic ovary syndrome as a plausible evolutionary outcome of metabolic adaptation. Reprod Biol Endocrinol. 2022;20(1):12. doi:10.1186/s12958-021-00878-y
82. O’Reilly MW, Kempegowda P, Walsh M, et al. AKR1C3-mediated adipose androgen generation drives lipotoxicity in women with polycystic ovary syndrome. J Clin Endocrinol Metab. 2017;102(9):3327–3339. doi:10.1210/jc.2017-00947
83. Livadas S, Pappas C, Karachalios A, et al. Prevalence and impact of hyperandrogenemia in 1,218 women with polycystic ovary syndrome. Endocrine. 2014;47(2):631–638. doi:10.1007/s12020-014-0200-7
84. Huang A, Brennan K, Azziz R. Prevalence of hyperandrogenemia in polycystic ovary syndrome diagnosed by the National Institutes of Health 1990 criteria. Fertil Steril. 2010;93(6):1938–1941. doi:10.1016/j.fertnstert.2008.12.138
85. Rosenfield RL, Ehrmann DA. The pathogenesis of polycystic ovary syndrome: the hypothesis of PCOS as functional ovarian hyperandrogenism revisited. Endocr Rev. 2016;37(5):467–520. doi:10.1210/er.2015-1104
86. Sanchez-Garrido MA, Tena-Sempere M. Metabolic dysfunction in polycystic ovary syndrome: pathogenic role of androgen excess and potential therapeutic strategies. Mol Metab. 2020;35:100937. doi:10.1016/j.molmet.2020.01.001
87. Huang ZH, Manickam B, Ryvkin V, et al. PCOS is associated with increased CD11c expression and crown-like structures in adipose tissue and increased central abdominal fat depots independent of obesity. J Clin Endocrinol Metab. 2013;98(1):E17–E24. doi:10.1210/jc.2012-2697
88. Sadeghi HM, Adeli I, Calina D, et al. Polycystic ovary syndrome: a comprehensive review of pathogenesis, management, and drug repurposing. Int J Mol Sci. 2022;23(2):Article583. doi:10.3390/ijms23020583
89. Bhattacharya K, Dey R, Sen D, et al. Polycystic ovary syndrome and its management: in view of oxidative stress. Biomol Concepts. 2024;15(1):Article38. doi:10.1515/bmc-2022-0038
90. Lewis RD, Narayanaswamy AK, Farewell D, et al. Complement activation in polycystic ovary syndrome occurs in the postprandial and fasted state and is influenced by obesity and insulin sensitivity. Clin Endocrinol. 2021;94(1):74–84. doi:10.1111/cen.14322
91. Butler AE, Moin ASM, Sathyapalan T, et al. Components of the complement cascade differ in polycystic ovary syndrome. Int J Mol Sci. 2022;23(20):12232. doi:10.3390/ijms232012232
92. Butler AE, Moin ASM, Sathyapalan T, et al. Complement dysregulation in obese versus nonobese polycystic ovary syndrome patients. Cells. 2023;12(15):2002. doi:10.3390/cells12152002
93. Zhou H, Hong Y, Diao F, et al. Guidelines for diagnosis and treatment of polycystic ovary syndrome with integrated traditional Chinese and Western medicine (2024 edition). J Tradit Chin Med. 2025;66(6):649–656. doi:10.13288/j.11-2166/r.2025.06.017
94. Li J, Feng L, Feng X, et al. Study on the combination law of TCM four-diagnostic information in polycystic ovary syndrome based on principal component and cluster analysis. World Sci Technol Mod Tradit Chin Med. 2024;26(2):437–443.
95. Mohammed S, Sundaram V, Adidam Venkata CR, et al. Polycystic ovary rat model exposure to 150-kHz intermediate frequency: hypothalamic–pituitary–ovarian axis at receptor, cellular, tissue, and hormone levels. J Ovarian Res. 2021;14(1):173. doi:10.1186/s13048-021-00914-w
96. Miao M, Peng M, Yan X. Effect of total flavonoids of Cuscuta chinensis on letrozole-induced polycystic ovary syndrome in rats. Chin J Exp Prescr. 2019;25(16):17–23. doi:10.13422/j.cnki.syfjx.20191607
97. Zuo L, Hai Y, Zhang R, et al. Therapeutic potential of icariin in rats with letrozole and high-fat diet–induced polycystic ovary syndrome. Eur J Pharmacol. 2023;953:175825. doi:10.1016/j.ejphar.2023.175825
98. Li L, Xiao Y, Zhou J, et al. Effects of berberine on glucolipid metabolism in dehydroepiandrosterone-induced insulin-resistant PCOS rats. Heliyon. 2024;10(2):e24338. doi:10.1016/j.heliyon.2024.e24338
99. Fadilah F, Ermanto B, Bowolaksono A, et al. Prediction of the signaling pathway in polycystic ovary syndrome using an integrated bioinformatics approach. Gynecol Obstet Invest. 2024;89(6):485–511. doi:10.1159/000539228
100. Yang JP, Ullah A, Su YN, et al. Glycyrrhizin ameliorates impaired glucose metabolism and ovarian dysfunction in a polycystic ovary syndrome mouse model. Biol Reprod. 2023;109(1):83–96. doi:10.1093/biolre/ioad048
101. Otoo A, Czika A, Lamptey J, et al. Emodin improves glucose metabolism and ovarian function in PCOS mice via the HMGB1/TLR4/NF-κB pathway. Reproduction. 2023;166(5):323–336. doi:10.1530/REP-22-0449
102. Huang Q, Li Y, Chen Z, et al. Bushenhuoluo Decoction improves polycystic ovary syndrome by regulating exosomal miR-30a-5p/SOCS3/mTOR/NLRP3 signaling–mediated autophagy and pyroptosis. J Ovarian Res. 2024;17(1):29. doi:10.1186/s13048-024-01355-x
103. Kicińska AM, Maksym RB, Zabielska-Kaczorowska MA, et al. Immunological and metabolic causes of infertility in polycystic ovary syndrome. Biomedicines. 2023;11(6):1567. doi:10.3390/biomedicines11061567
104. Wang Y, Du Z, Zhang X, et al. Effects of Hippophae rhamnoides flavonoids on polycystic ovary syndrome in rats by regulating the TLR4/NF-κB pathway. Food Ind Sci Technol. 2024;45(16):340–347. doi:10.13386/j.issn1002-0306.2023060221
105. Motta AB. Polycystic ovary syndrome and oxidative stress: natural treatments. Curr Med Chem. 2025;32(8):1457–1468. doi:10.2174/0109298673270372231130071320
106. Wu Y, Yang X, Hu Y, et al. Moringa oleifera leaf supplementation relieves oxidative stress and regulates intestinal flora to ameliorate polycystic ovary syndrome in letrozole-induced rats. Food Sci Nutr. 2023;11(9):5137–5156. doi:10.1002/fsn3.3473
107. Zhao H, Chen R, Zheng D, et al. Modified Banxia Xiexin Decoction ameliorates polycystic ovary syndrome with insulin resistance by regulating intestinal microbiota. Front Cell Infect Microbiol. 2022;12:854796. doi:10.3389/fcimb.2022.854796
108. Huang W, Jin Y, Jiang L, et al. Radiomics optimizing the evaluation of endometrial receptivity in women with unexplained recurrent pregnancy loss. Front Endocrinol. 2023;14:1181058. doi:10.3389/fendo.2023.1181058
109. Liu YC, Wang JW, Li J, et al. Mechanism of cryptotanshinone in improving endocrine and metabolic functions in the endometrium of PCOS rats. J Ethnopharmacol. 2024;319(Pt 3):117346. doi:10.1016/j.jep.2023.117346
110. Ribeiro MP, Lemos C, Leal C, et al. Reproductive prognosis factors in women with infertility and polycystic ovary syndrome undergoing in vitro fertilization techniques. JBRA Assist Reprod. 2025. doi:10.5935/1518-0557.20250040
111. Song N, Yuan M. Factors affecting the efficacy of Jinkui Shenqi Pill in treating kidney-yang deficiency PCOS and construction of a prediction model. Hebei Tradit Chin Med. 2025;47(9):1443–1449.
112. Lu Q, Zhou Y, Yang B, et al. Clinical study of Ziyu prescription in treating polycystic ovary syndrome with kidney deficiency. J Nanjing Univ Tradit Chin Med. 2025;9:1224–1231. doi:10.14148/j.issn.1672-0482.2025.1224
113. Wu J, Li L, Hu Y. Effect of Bushen Zhuyun decoction on sex hormones and ovarian microenvironment in infertile women with PCOS. J Tradit Chin Med. 2025;53(9):75–79. doi:10.19664/j.cnki.1002-2392.250191
114. Dai Y, He B, Yang S, et al. Effects of Jianpi Huatan decoction on Treg/Th17 balance in PCOS with spleen deficiency and phlegm-dampness. Chin J Clin Pharmacol Ther. 2025;30(9):1153–1164.
115. Xin X, Zhang J, Dong L, et al. Effect of electroacupuncture on assisted reproductive outcomes and follicular fluid exosomal lncRNA in obese PCOS patients. Acta TCM Sinica. 2025;40(7):1377–1383. doi:10.16368/j.issn.1674-8999.2025.07.221
116. Liu Y, Liao B, Zhang X, et al. Efficacy of Ren Du Tong Tiao acupuncture for hyperandrogenic PCOS with kidney-yin deficiency and fire hyperactivity. Chin Acupunct Moxibustion. 2025;45(8):1078–1082. doi:10.13703/j.0255-2930.20240612-0003
117. Wu J, Zhang S, Tang L, et al. Acupoint injection improves glucose metabolism in PCOS with kidney deficiency and blood stasis. World Sci Technol Mod Tradit Chin Med. 2025;27(7):1982–1989.
118. Xu Q, Zhong F. Warming-needle moxibustion with midnight–noon ebb-flow acupuncture plus Bushen Huayu decoction in PCOS with kidney deficiency and blood stasis. J Gansu Univ Tradit Chin Med. 2025;1–6.
119. Li X, Sun X, Zhong W, et al. Effect of Huanglian Wendan decoction combined with acupuncture on polycystic ovary syndrome. Lab Med Clin. 2025;22(17):2357–2361.
120. Wang N, Liu L, Huang Y, et al. Acupuncture combined with Cangfu Daotan pill for PCOS with spleen deficiency and phlegm-dampness: a study based on intestinal flora. J Clin Acupunct Moxibustion. 2025;41(5):16–21. doi:10.19917/j.cnki.1005-0779.025086
121. Zhou J, Zhang H, Wang X. Effect of modified phlegm-regulating decoction plus Baduanjin on insulin resistance in polycystic ovary syndrome. Liaoning J Tradit Chin Med. 2025;52(8):103–108. doi:10.13192/j.issn.1000-1719.2025.08.026
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Evolving PCOS Management: From Symptom Control to Phenotype-Targeted Therapy
Wang T, Zhang T, Wang J, Lu T
Diabetes, Metabolic Syndrome and Obesity 2026, 19:560296
Published Date: 4 February 2026