Back to Journals » Risk Management and Healthcare Policy » Volume 16
Exploring the Challenges for Universal Health Coverage: A Call to Africa by AfroPHC
Authors Moosa S ![]()
Received 9 October 2022
Accepted for publication 22 September 2023
Published 27 September 2023 Volume 2023:16 Pages 1999—2017
DOI https://doi.org/10.2147/RMHP.S392454
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Kent Rondeau
Shabir Moosa1,2
1African Forum for Primary Health Care, Johannesburg, South Africa; 2Department of Family Medicine and Primary Care, University of Witwatersrand, Johannesburg, South Africa
Correspondence: Shabir Moosa, African Forum for Primary Health Care, 5 Westway Road, Fourways, Johannesburg, 2191, South Africa, Tel +27824466825, Email [email protected]
Abstract: The primary health care (PHC) system in Africa faces many challenges AND opportunities. To date, human resources for health in PHC are grossly insufficient in number, often inefficiently and inequitably distributed, lacking adequate training for delivering fully responsive and comprehensive frontline care and are treated inequitably within the health system. There has been a lack of solidarity among key role players in healthcare to create adequate PHC funding in Africa. Resources do not appropriately or adequately reach the frontline PHC service platform due to outdated service delivery and payment models. Patients experience PHC as numbers in a queue, with poor comprehensiveness, continuity, and coordination. Health workers are also treated like numbers in a bureaucracy that fragments and undermines training and service for integrated care around patient and population needs. However, opportunities abound with global PHC milestones, increasing political will for investment in PHC, and proven mechanisms for achieving a stronger workforce such as community health workers, clinical task-sharing, and the integration of family doctors into PHC. The African Forum for PHC (AfroPHC) has a vision for PHC and UHC that is team-based with skills mix appropriate to Africa, including family doctors, family nurse practitioners, clinical officers, community health workers and others that are empowered to take care of an empaneled population in high-quality people centred PHC. AfroPHC is making a call on stakeholders to develop and implement a regional forward-looking plan to 1) build robust PHC systems, 2) train, recruit and maintain a sufficient frontline PHC workforce, and 3) support PHC with appropriate financing. This can all come together easily in a nationally defined PHC contract using risk-adjusted blended capitation payment to decentralised PHC teams empanelled to enrolled populations, coordinated by district health services and easily administered at national or sub-national level for empowered public and private providers.
Keywords: PHC workforce, PHC financing, PHC systems, PHC teamwork, PHC blended capitation, empanelment
Introduction
The African population suffers from the challenges of high disease burden and public and private health systems that are divided, with poorly managed resources, governance, and accountability. Almost one in ten people incur catastrophic health expenditure and fifteen million people are driven to poverty annually due to out-of-pocket expenditure.1 There are also many opportunities in Africa to deliver on PHC/UHC with the economic growth trajectory in Africa, the demographic dividend of a youthful Africa, well-trained and competent health professionals, the indigenous traditional healthcare network, a strong civil society, a developed private sector, the innovation ecosystem, and health system strengthening efforts in response to COVID-19.1
There have been important milestones on the global journey to PHC/UHC.2 The World Health Report (2008) on PHC speaks of (i) the need for PHC to be central to universal health coverage (UHC); (ii) the need for service delivery reforms that re-organize health services around people’s needs; (iii) the need for integrating public health actions with primary care; and (iv) the need for leadership reforms (where governments act as custodians of the entire health system, including the private sector and not just of the public service).3 The Astana Declaration (2018) set out several operational levers including models of care that prioritize primary care and public health functions, as well as engagement with private providers in new purchasing and payment systems.4 The World Bank Report (2021) “Walk the Talk: reimagining Primary Health Care after COVID-19” suggests four structural shifts: from low to high-quality PHC, from fragmentation to person-centred integration, from inequity to fairness and integration, and from fragility to resilience.5
The African Forum for Primary Health Care (AfroPHC) brings together the leadership of ALL health workers and activists at the coalface of primary health care (PHC) in Africa to be a voice for change, allow sharing of resources, and provide support towards the PHC team for UHC in Africa. [Box 1] Our experience of primary health care (PHC) is of patients who are treated as numbers in a queue, with poor comprehensiveness, continuity, and coordination. Health workers are also treated like numbers in a bureaucracy that fragments and undermines integrated care around patient and population needs. [Box 2] AfroPHC has had a series of interactive workshop with PHC frontline staff from 2020 exploring policy issues for PHC in Africa. This evolved into a “Call to Africa” that was supported financially by the Primary Healthcare Performance Initiative (PHCPI) in 2022 to engage in wider consultations, including an in-person workshop of the AfroPHC Executive and Advisory Boards, before launching. The AfroPHC Call to Africa to build effective primary health care teams for universal health coverage in Africa focuses on three issues in exploring the policy challenges for Universal Health Coverage: PHC Systems PHC Workforce, and PHC Financing.
 |
Box 1 More About AfroPHC |
 |
Box 2 Members of AfroPHC |
PHC Systems
AfroPHC embraces the Bio-Psycho-Social-Spiritual Approach for PHC
Many professional members of the PHC team are integrating principles of primary health care and primary care within their discipline, with many shared values across disciplines. Family medicine, the specialist discipline of generalist primary care, has principles that are increasingly shared among other professions and medical disciplines. Healthcare workers trained in family medicine are expertly able to deliver person- and family-centered care that addresses patient’s problems with a bio-psycho-social-spiritual approach. [Box 3] In Africa PHC service delivery is expected to be personalised, comprehensive, continuous, and coordinated just like the global standard.6 Personalisation comes with the several tools for patient- and family-centred care that matter to generalists across the world and that are still implemented by African family physicians, family nurse practitioners and others, under difficult circumstances in some spaces. Knowledge and practice of good consultation skills is essential for the delivery of patient centred care with shared decision-making in delivering care. Comprehensiveness can be achieved by ensuring that as many of the patients’ needs are met in any one of their encounters with first contact care. Continuity means that repeated episodes of care are perceived by patients as continuous, whether personally, informationally or by continuity of management by a team. Coordination is about the PHC team as a unit ensuring that referrals within and especially beyond the team are coordinated around the patient’s bio-psycho-social-spiritual needs.7
 |
Box 3 Family Medicine |
AfroPHC envisions Comprehensive Person-, Family- and People-Centred PHC
Low- and middle-income countries risk over-simplifying primary care and primary health care.3 Whilst PHC is a broader concept than primary care (PC), good-quality primary care services need to be better understood and structured to achieve PHC. This must make use of primary care as defined in the three levers of PHC from WHO/UNICEF’s Operational Framework for PHC.9 It must also utilize primary care services as the cornerstone of frontline PHC service delivery and the principal tool of governments’ provision of first contact health care for their populations. PHC service includes illness prevention, health promotion, treatment, rehabilitation, and palliation. Common conditions are easily complicated by growing multimorbidity, unhealthy choices fuelled by the commercial determinants of health, psychosocial and spiritual issues. Such unique person-centred care with strong humanism is best delivered within a wider spectrum of care in the context of family, work, community, environment, and information. While a systematic review has shown that most patients in Sub-Saharan Africa view PHC positively, our experience is that African patients are no longer happy to be treated as numbers in a large faceless PHC system where relationships are neither existent nor supported.10 Unsafe and ineffective primary care increases morbidity and preventable mortality, leading to increased use of hospital and specialist resources, especially in private health care. Traditional-indigenous health and self-care are important constructs for engagement by PHC in Africa.3,11 There is a growing interest in OneHealth with climate change, where human health (especially PHC) is seen as intertwined with the health of other living things and the environment as a whole.12 Africans, especially the poor, are struggling with climate change and air pollution, affecting their health and safety in a variety of ways. The WONCA Course on Planetary Health is an important free resource for PHC workers for community care and advocacy, starting at a local level and in small ways.
AfroPHC wants Integrated PHC Priorities
Strong person-, family- and community-oriented PHC must have priority health programmes that are integrated within the care that is provided to each person in a personalised manner. This can work very well in PHC teams that are themselves integrated to work on that premise, embrace task-sharing and supporting each other in a range of skills suitable to the country’s full human resources, both public and private, and designed to cater to empanelled populations universally across the country. Important priorities in the burden of disease across Africa must be part of both the training and service by integrated PHC teams: communicable diseases, non-communicable diseases, mother-child and women's health, violence and trauma, mental health and a range of national/regional priorities. Ultimately, the PHC team should be able to understand the demographics and epidemiology of their local empanelled populations and incorporate these priorities into strong community-oriented primary care.
AfroPHC wants Strengthened Rehabilitation and Palliation in PHC
Most communities in Africans are denied access to rehabilitation and palliation services, with poor understanding of disability issues as well as death and dying, centralised services, skills shortages, spending largely out of pocket and poor policy. Populations needing these services are hidden and experience more significant barriers to care, eg, lack of transport. This population is also more vulnerable to social determinants of health. Cost-effective community-based rehabilitation and palliation services require service delivery reform with strong emphasis on accountability to this vulnerable population and performance management. Decentralising services to community level, including task-sharing with mid-level rehabilitation and palliation workers in team-based care supervised by rehabilitation and palliation professionals, peer parent facilitators – home care, innovative assistive device management and social empowerment by CHWs, as an add-on to a set of community practices, can strengthen rehabilitation and palliative service coverage in PHC for UHC.
AfroPHC wants Oral Health Integrated into PHC
In Africa, there are independently functioning dental and medical care systems with inequity and missed opportunities to provide services. The integration of oral health into PHC systems can reduce the burden of oral disease and improve access to oral health care, especially for the disadvantaged and under-served communities. It should include risk assessment, oral health evaluation, preventive intervention, communication, and oral health education. This is important as there is a strong biological relationship between what occurs in the mouth and the rest of the body. Many vulnerable population groups with untreated oral disease often obtain medical care but not oral health care, especially in emergency settings. Integration can also reduce the cost of oral health care. This can be achieved by integrated team-based service delivery models that include appropriate task-shifting to a range of PHC team members and oral health care practitioners, using population-based models of care. This must include dentist supervision. Whilst the populations for oral health care teams may have to be larger than those for the medical/clinical core team the prerogative of oral health care needs to be embedded into all community practices, especially with CHW work on environmental and societal factors that impact on oral health as practiced in Brazil.13,14
AfroPHC wants Improved Access to Medicines and Investigations in PHC
Medicines and investigations are an important component and cost of PHC, besides the workforce. It is of vital importance that pharmacists are incorporated into PHC and supervise and support teams that cover multiple PHC facilities and mid-level pharmacy staff who can then improve the quality of management of medicines as well as reduce the burden of pharmacy management on the non-pharmacy workforce. Laboratory technicians are quite prevalent across Africa. This cadre can be enhanced with the use of more point-of-care testing devices, better training, and stronger quality assurance at PHC level for patient safety. The increasing technological advance of devices, the value of simple tests in local and important clinical decision-making, eg, antibiotic prescription and the increasing value of such interventions make this a compelling proposition for African PHC. This includes a range of investigations that technology has made more accessible and amenable to be placed in PHC, eg, point-of-care ultrasound and digital radiology.
AfroPHC wants Improved Coordination of Referrals
Coordination of care, specifically managing referrals from primary to other levels of care, is a vital component of high-quality PHC and is best done by postgraduate-trained family doctors placed in PHC. They will be able to manage referrals as gatekeepers, doing what is possible in the PHC setting and then referring appropriately to other specialists and services. This coordination function operates with other key elements of first contact PHC – management continuity and service comprehensiveness to achieve higher quality care. Global work done on trained family doctors placed in PHC shows that this type of care can achieve fewer and more appropriate referrals, fewer re-admissions, and lower overall costs of care. This placement can also allow well-trained generalist expertise to negotiate the engagement of various other specialties into PHC based on medical need and in a targeted manner to achieve better results at a lower cost.6,15,16
AfroPHC wants Health in All Policies (HiAP) for Robust PHC
The Africa Health Agenda International Conference (AHAIC) Commission makes important recommendations to re-orientate African health systems to prioritise and strengthen PHC as the foundation for UHC. [Box 4] It recommends a “Health in All Policies” approach by national government as an integrating and developmental public health approach to decentralised government. The “Health in All Policies” approach brings together various stakeholders whose contributions are critical to ensuring a functional, effective, and efficient PHC system, including the providers of utilities (potable water, electricity and waste, information, and security management). AHAIC suggested PHC delivery be implemented by using flexible models of non-hierarchical multidisciplinary teams of clinical and non-clinical staff to provide integrated care to defined empanelled populations.1
 |
Box 4 AHAIC Recommendations |
AfroPHC wants to build the District Health System
The district health system has been promoted across Africa. However, planning of health service delivery in some African countries is conducted at a ministry level, in most cases with local managers, health workers and communities just receiving what was concluded without their involvement. Most district managers utilise the top-down approach rather than focusing it on the patient in what must be a bottom-up approach led by the PHC team in their daily encounters. Complexity is a way of thinking, in which system structures are interconnected with non-linear multi-directional interactions that the system evolves with. Complexity theory supports “emergent” behavior from the ground up, which mostly cannot be predicted using deterministic models. PHC should be seen as a complex adaptive system and supported with a clear purpose, values and simple operating principles to drive it in the right direction.17 Policy proposals for UHC contracting for PHC indicate that healthcare workers can be agents of change with a few principled operational drivers set out by policymakers for action at district level to drive appropriate and responsive PHC.18 Some governments in Africa, eg, Rwanda, Kenya, Sierra Leone and Nigeria, are already embracing this bottom-up approach where policymakers are able to step back and give PHC providers space to do what they are trained to do. We see the role of District Health System as coordinating empowered PHC providers working as PHC teams at both facility and community levels.19
AfroPHC wants to Empanel Defined Populations to a Defined Team
The World Health Organization (WHO) considers empanelment as a foundational component of PHC. It is about assigning populations to facilities/PHC teams with a responsibility of understanding their assigned population and to deliver coordinated PHC to them. Empanelment allows PHC to move from reactive care, oriented around facility visits by patients, to proactive care that leverages the PHC team’s potential to improve population health. It allows a relationship to be built between the population and their providers.20 Small defined populations cared for by a team with an appropriate mix of healthcare workers and delivered in a comprehensive, continuous, coordinated manner can be the complex adaptive system that could deliver better PHC and health for all in Africa.7 While global panels average 1500, there are some countries where it is larger, eg, Brazil with 3500 cared for by a doctor, nurse and set of CHWs. Africa has the experience to explore larger panels for a PHC team eg, the Chiawelo Community Practice with 10,000 to 30,000 people. [Box 5] There is a need to define and standardize PHC facilities and human resource nomenclature across Africa as teamwork should involve all healthcare workers. From here, appropriate population panels to PHC team mixes can be defined in ratios appropriate to each country’s human resources (including private sector providers). However, this must be built in layers, starting with the clinical core of community health workers, family nurse practitioners, clinical officers, and family doctor.
 |
Box 5 Chiawelo Community Practice |
AfroPHC wants to develop Community-Oriented Primary Care for Africa
A culture of distributed leadership and clinical accountability can be created to improve PHC team cohesion and thereby ensure quality of care for populations in Africa. This can be realised in a decentralised model of PHC team practice, dubbed “community practice”. This is based on experience with PHC teams in Africa, eg, the Chiawelo Community Practice. In this model CHWs serve defined sections of an enrolled population of 30000 strongly linked to clinicians at a local clinic where care is provided in patient- and family-centred manner by a PHC team with a mix of skills including a doctor, clinical associate, nurses, and community health workers. This link involving individual, facility, community and self-care is enhanced by stakeholder engagement and targeted health promotion based on data collected from the enrolled population. Panel sizes of enrolled populations can be larger than the global averages. The Chiawelo Community Practice reveals that 30000 per core clinical PHC team of a family doctor, family nurse practitioners, clinical officers, and community health workers can work as a point of departure. However, we propose 10000 per core PHC team across Africa as an aspirational target for 2050. PHC team configurations for various ancillary disciplines can also vary across Africa, taking pathophysiological processes, social determinants of health, available human resources, and the skills mix (including ancillary health professions) needed into account [Box 6].
 |
Box 6 Strategy for Defining PHC Teams per Panel |
AfroPHC wants to “Rural Proof” Rural and Marginalised Urban Health
Africa is still largely rural. The Blueprint for Rural Health urges governments to act on several fronts. The ideas are applicable in both rural areas and marginalised urban settings in an Africa that are grappling with rapid and poorly managed urbanisation. Governments should ensure that resources are available and conveniently accessible to all sections of the population, irrespective of their socio-economic situation. PHC in marginalised areas should be predicated on fit-for-purpose community infrastructure. Education, employment, housing, clean water, sanitation, good roads, and sustainable energy are essential to this. Communities should be empowered – in all spheres of life - to identify and solve their local health care challenges. Policies should be assessed in terms of their impact on vulnerable communities to mitigate any deleterious effects of these in marginalised areas. Government should strengthen intersectoral collaboration and coordination among various departments and work towards developing a unified policy to promote health and resilience among vulnerable groups. The Blueprint for Rural Health also informs human resource development. It advises that the health workforce be systematically supported and planned with a stepladder progression of skills attainment and certification of the PHC team. Students undertaking health science courses should also have marginalised immersion that reflects the significance and importance of practice in hard-to-reach areas. Educational institutions must orient their training, research, and service provision to prioritise the under-served population living in marginalised areas.23 Decentralised training platforms and distance-based training can cater to all members of the PHC team. Nigeria and Ethiopia offer examples of such training schemes.24–26
AfroPHC wants Women to get Extra Consideration in PHC
It is important to consider women in PHC for UHC, both as users and providers. Many women interact with PHC as users, with many finding themselves suited to provide care in PHC. There are serious limitations to women’s participation in PHC as both users and providers, especially with gender-based violence and sexual harassment, plus the lack of safe avenues for reporting these. Female users also must contend with inaccessible facilities, lack of financial and cultural independence, greater health burdens, home obligations, cultural-community norms, and a reluctance to be attended to by male healthcare workers. Female providers also must contend with salary gaps and male-dominated leadership in some countries.
AfroPHC wants Youth to get Extra Consideration in PHC
It is important to consider youth in PHC for UHC, both as users and providers. With a youthful Africa, it is important to address their needs. The WHO vision for PHC in the 21st century includes the importance of managing youth.17 Youthful professional students and providers are an important source of inspiration for AfroPHC. The organisation is actively developing youth activities to support PHC and UHC by involving youthful leaders in the governance of AfroPHC so that they can drive its agenda far into the future. The youth can build a strong community of practice in creating the foundations of PHC and UHC in Africa.27
AfroPHC wants e-Health Accessible, Interoperable, and Patient- and User-Friendly
COVID-19 has brought e-health to the fore for all of us, especially in PHC. e-Health is a vital part of the solution to bring quality PHC and UHC to scale across Africa. However, solutions are not well contextualised for both provider and user. Solutions need to always be focused on patients and the population, and therefore must take into consideration end-user capacity. This is both in terms of skills and ability to integrate e-health into poorly capacitated and busy African PHC settings. There is a great opportunity to utilise e-health with growing internet connectivity and mobile phone usage, growing use of digital tools and the evolution of electronic medical records in high disease burden African settings. A combination of innovative and tech-enabled solutions could, over time, help to re-imagine an African PHC system that is tailored to patient pathways. These would ideally seamlessly integrate brick-and-mortar and remote Point-of-Care solutions to provide continuous, integrated, and preventative care, especially for long-term conditions, among team members and between different levels of care. E-health can increase efficiencies to reduce unnecessary in-person visits, optimise facility workflow processes and reduce access barriers for clients. It can also streamline and coordinate supply chains, workforce, and facility costs, thus increasing availability and quality of PHC services. E-Health can also be integrated with professional education to build the capacity of the health workforce. AfroPHC does not endorse single national digital health systems, but rather advocates for strong nationally regulated systems that integrate multiple solutions with interoperability and make for seamless PHC service provision across Africa.28–30 This can help the continent to leapfrog the world.
AfroPHC wants to build Community Engagement and Social Participation
AfroPHC strongly supports community engagement and social participation for UHC and recognises the role of CHWs in the African PHC team, as set out in WHO’s Handbook on social participation for UHC.31 UHC may not translate into adequate PHC if social participation is not addressed. Participation by communities, as an empowered voice with agency, is vital to get behind this call. There needs to be an enabling environment for participation where power dynamics are addressed to create equal conditions for participation. Representatives need to be considered legitimate and able to represent. The engagement between government, communities and civil society needs to be recalibrated to create a level playing field for frank discussion and policy influence. Legal frameworks should be created for participation, especially on decentralization. Long-term sustainability of participatory spaces can only happen if they are adequately funded so that people stay engaged, results are visible, and a culture of participation is created.31 We intend to engage communities using these principles whenever we can, from building AfroPHC Chapters in our countries to building best practice community-oriented primary care around our own practices.
AfroPHC wants to build Quality into PHC
Improving access has come at the cost of quality. There is a need for major reform to achieve quality and UHC offers the opportunity. Quality PHC can best be provided by a suitable trained workforce with the multi professional perspectives of family doctors, family nurse practitioners, midwives, clinical officers, community health workers, oral health care workers, pharmacists, laboratory technicians, physiotherapist, occupational therapists, social workers, and administrative staff as well. However, the priority for quality improvement is empowering healthcare providers and the enhancement of teamwork by the array of professionals available. Africa should avoid a siloed training and practice medical model of PHC service delivery in UHC initiatives, especially among clinicians. There is culture of territoriality in healthcare with entrenched silos, which could derail a renewed focus on the patient, teamwork and interprofessionalism. There is a need to develop and understand professional identity and to then articulate the role, space, and contribution of each cadre in a PHC team as colleagues. Multidisciplinary teamwork in PHC goes beyond care providers – The PHC team needs to liaise with other disciplines and various networks, eg, education, civil works, water, power supply, security, environment, trade, and community-based institutions, in line with the Health in All Policies policy described earlier.27,32
AfroPHC wants to manage Effectiveness
What gets measured gets done. It is unfortunate that a 2022 scoping review on Strengthening the Health System as a Strategy to Achieving a Universal Health Coverage in Underprivileged Communities in Africa shows little evidence for PHC teams empanelled to populations to be able to achieve UHC.33 This is despite a consensus amongst PHC workers that this concept does deliver better health care and outcomes in line with UHC. The Primary Health Care Performance Initiatives (PHCPI) 38 Core Indicators and resulting Vital Signs Profile, inspired by the PHCPI Conceptual Framework (2017) have further inspired the various indicators in the WHO’s PHC Measurement Framework (2022). These tools, based on the 14 levers of the Astana Operational framework, can support the improvement of service coverage, financial risk protection and ultimately the health of patients and populations in Africa. These are particularly pertinent to the PHC workforce, models of care, engagement with private providers and purchasing and payment systems. Whilst Tier 1 indicators (including the Global Indicators) are more feasible to collect, Tier 2 indicators, deemed desirable and needing testing, speak more compellingly to issues that could test the value of PHC teams empanelled to populations. These are specifically processes and outputs of PHC. There are useful examples in both. On the process, useful examples of indicators include experience of an empanelment system in models of care; multidisciplinary team-based service delivery in organization and facility management; and collaboration between facility-based and community-based service providers. In outputs, there are access indicators collected. However, there needs to be more work on useful indicators on quality of care, eg, people’s perception of health system and services; admissions for ambulatory care-sensitive conditions; prescribing patterns for antibiotics; and provider caseload.34,35 These can be expanded upon with testing of revalidated tools that can be more widely scaled across Africa. The indicators can be incorporated into WHO measures of UHC across Africa. We need to focus on key indicators such as out-of-pocket expenditure and catastrophic expenditure to provide a much more sensitive measure of service coverage, as opposed to the current narrow programmatic-type measures available. This would truly underpin WHO strategic goals in Africa of rethinking and repivoting health service delivery with a focus on service integration, community involvement, private sector engagement and enhancing resilience.36
AfroPHC is working with various partners to develop and strengthen practice- and population-based research networks across Africa. We are committed to mobilising PHC workers across Africa to create teams around empanelled populations as sentinel sites across Africa, to share best practices and to show evidence of how effective we can be at both practice and population level once empowered to deliver quality PHC as a team. We also consider the PHCPI’s PHC Progression Model as a way to develop country AfroPHC Chapters and engage with stakeholders around these objectives.37
PHC Workforce
AfroPHC wants to strengthen Human Resources for PHC
Africa has the most severe health personnel shortages, with the need predicted to reach 6.1 million by 2030 out of the anticipated global health care worker need of 14.5 million required for UHC and to achieve the Sustainable Development Goals (SDGs). Africa had an average of 1.30 health workers per 1000 people in 2015, significantly less than the 4.5 needed to meet the SDGs.1 With this shortfall, the focus of the health system becomes more curative with professionals working in curative spaces like hospitals (often serving the elite) and primary care (usually for marginalised communities) regarded simplistically.3 This distortion in the distribution of human resources compounds the problem of poor quality primary care with the growth in hospitals and a private sector that both perversely neglect PHC needs.
As AfroPHC came together, we realised that the definition of the PHC workforce is lacking with non-standardised nomenclature, training, qualifications, pay and career prospects across the continent. Primary care providers within many low-middle income countries (LMICs) struggle with the poor definition of PHC services resulting in difficulty measuring the financial and human resource allocations to PHC. Many countries do not have statutory standards of care to be expected at the different levels of care, including the PHC level. Health services, especially the primary care service delivery platform lacks definition and ringfenced resources. The number of family doctors, family nurse practitioners, clinical officers, community health workers and other members of the PHC team available in the country is often not easily or reliably available. This is further exacerbated because governments do not take their stewardship role over the private sector very seriously and have not created systems to measure the total number of professionals across the country, with planning based on just public health service “shortages”. There is a need to clearly define the spaces of primary health care, including the human resources required to service it in a standardised way across Africa. This will lay the basis for strengthening human resources for PHC and UHC in Africa.22
AfroPHC wants to build the Team with Role-Sharing and Collaborative, Supportive Supervision
We acknowledge various cadres – family nurse practitioners, midwives, dental therapists, pharmacy assistants, laboratory technicians and community health practitioners – who serve as the backbone of PHC service delivery across the continent. Their neglect is clear with a growing service burden on them without the required competence, resources, and support. Rather than looking for some ubiquitous “mid-level” worker to “solve all” problems we propose the adoption of the language of interdisciplinary and interprofessional teams, as mentioned in Astana, for enhanced health outcomes. There will always be professions but trans professional collaboration (TPC) can enhance a deliberate exchange of knowledge and skills aimed at meeting complex healthcare needs. Role-sharing is important in current PHC service delivery with the shortage of all health professional cadres. However, siloed task-sharing is not the same as teamwork, where everyone should be focused as a team on holistic person-centred care. Role-sharing should not be about “replacing” or “substituting” any health professional. It is about extending the reach of the PHC team considering the limited resources. PHC teamwork is best achieved in an integrated and flexible mix of skills with supportive supervision. Role-sharing can be achieved through PHC teamwork and collaboration among many disciplines and should not be resisted by professional turfs. Instead, there should be cooperation to extend the range of services/tasks possible by the PHC team in an accountable manner, eg, allowing advanced nurse practitioners and clinical officers to prescribe based on their education so that the team becomes fit for “purpose” in an efficient manner. The skill mix will create resilience with flexibility.
Service packages are not usually defined by a written document but rather by the mix of professionals and resources available at practice level. Whilst nurses, midwives, clinical officers, family doctors and community health workers are all core to integrated PHC service delivery in Africa, all healthcare professionals (including pharmacy, laboratory, mental, rehabilitation, oral health, etc.) and other stakeholders (patients, administrative staff, community, traditional services, local leaders, etc.) need to be part of the PHC team in an interprofessional team-based approach that balances curative and preventive care. This can only be achieved by adequate human resource planning and integration, upscaled workforce training and education, appropriate credentialing and regulations, plus by incorporating aspects of support and supervision. For the protection of patients and to ensure quality care outcomes, role-sharing should be subject to appropriate education and training in new skills. It should also be backed by supportive supervision, mentoring, monitoring and evaluation.
AfroPHC wants to build Distributed Leadership
Professional turf wars continue globally, and in Africa. The sources of conflict include role boundary issues, scope of practice and accountability.38 The increasingly globalized and digital nature of work in the future is not in fixed roles, teams, and spaces, and would require practical changes in PHC.39–41 A critical role in this regard is leadership. It is crucial to train PHC teams on the need to embrace such roles at the undergraduate level. Leadership is often portrayed as an entitled position, usually of authority and power. However, all PHC members must be trained to understand that occupation of a formal leadership role is not a requirement to be a leader.37,38 True leadership for teamwork should support various team roles in relation to tasks. Team members as “leaders” should look and listen to the team dynamic, reinforce the value of each role, help set boundaries and attempt to fill gaps in the team where needed skills are not available. This leadership role should assiduously seek to understand unique ideas and motivations, both in relation to the initial team objectives, and then weave each of these into an overall bigger vision for the team.37 True leadership should also actively seek to empower others to be leaders, building on strengths, helping overcome weakness and seeing in teammates the things that the teammates themselves may not see – possibilities.41 This enhances team motivation and cohesion much stronger, thus reflecting the wise words of Aristotle that “the whole is greater than the sum of its parts”.
AfroPHC wants to build Clinical Governance
True leadership should recognise and defer to clinical knowledge and the need for clinical governance in the PHC team.42 Clinical governance practiced in Africa, with low income and resource constraints, needs to be more contextually relevant, with managers and professional members of the facility working synergistically to address the many quality-hampering gaps, such as the lack of enabling health law, financing-mix, lack of infrastructure of water, sanitation, electricity, etc. An example is the 12-Pillar Clinical Governance programme in Nigeria43 The hierarchy of clinical knowledge, especially with medical training, needs to be acknowledged and respected.
PHC teamwork and distributed leadership will not work if the PHC team is not held clinically accountable. Post-graduate-trained family doctors, dentists and other professionals can ensure broad clinical accountability and specifically prevent inappropriate referrals. They need to be acknowledged for their ability to improve clinical quality across the spectrum of care from clinic to community, and not just in hospitals41 In addition, an enhanced role in more decentralised primary care settings to support clinical governance could strengthen the competencies of family nurse practitioners and other healthcare providers and create effective and efficient PHC teams. We advocate that mechanisms be in place to ensure that all cadres respect and keep to their clinical competence levels for the safety of patients under their care and referring to the next higher cadre as appropriate in a timely manner.
AfroPHC wants Professionalized Community Health Workers
Community health workers (CHWs) and the many equivalent cadres across Africa are an essential part of the PHC team and need to be respected otherwise UHC may not translate into adequate PHC. [Box 7] Participation by communities, as an empowered voice with agency, is vital.31 CHWs need to be professionalised by defining their training, employment, and fair remuneration, among other things. They perform important educational and support tasks for rural and marginalised communities in Africa. They embed a whole of society approach that embraces meaningful engagement across sectors (education, agriculture, environment, financial, etc.) to identify innovative and sustainable solutions tackling preventive, promotive, predictive, and curative health areas. However, they should not be seen as substitute professionals but rather extend their reach as a part of the PHC team. They are essential in balancing the bio-medical focus of health professionals and to engender community engagement by the PHC team. CHWs, as part of the holistic interdisciplinary team can improve reach, reduce inequity, and provide a good return on investment, not only through their impact on community health but as a job creation mechanism across a country. It is recommended that CHWs be professionalized and remunerated in all countries in Africa as they form an integral part of the health ecosystem.44 [Box 8]
 |
Box 7 Nomenclature for CHWs, Including TBAs |
 |
Box 8 Two Sides of the Same Coin |
The effective use of CHWs is evident in case studies from Nigeria, Ethiopia, and Rwanda.46 Career progression of CHWs including prioritizing them as recruits for higher levels of professional training can create professional retention in rural and marginalized communities.47
AfroPHC wants Human Resources Better Managed
Human resource management for PHC is critical. The shortage of human resources in Africa compared to the rest of the world is compounded in African PHC, with professional resources drawn into hospitals located in urban centres and often linked to private practice. Weak African human resource for health (HRH) leadership and governance compounds the challenges of PHC workers, resulting in poor remuneration, poor facilities-working conditions, high workload-overwork-burnout, all of which contribute to poor quality of health care. Other challenges include the development of curricula that have ignored the reality of the African context, poor harnessing of the multidisciplinary team, a lack of supportive supervision and mentoring, migration, inefficient use of the available workforce, weak leadership, staff demotivation from lack of appreciation and poor work–life balance.48,49 Documents such as the Kampala Declaration and Agenda for Global Action mention, inter alia, the retention of an effective, responsive and equitably distributed health workforce and scaling up health worker education and training using a needs-based skill mix. Critical success factors for scaling up include political commitment and good governance; workforce planning (with relevant skills mix); and creation of an enabling environment.48,49
A useful framework on how to manage human resources better is depicted in the working lifespan framework from WHO: Entry (Preparing the Workforce with planning, education, and recruitment), Workforce (Enhancing worker performance with Supervision, Compensation, Systems Support and Lifelong Learning) and Exit (Managing attrition with migration, career choice, health and safety and retirement). All this is expected to lead to Workforce Performance (availability, competence, responsiveness and productivity).48,50,51 The WHO AFRO Regional Road Map for Scaling Up the Health Workforce by 2025 offers useful insights on scaling up with proposals for investments in harmonised health systems, with national registries and HRH information systems, to support and track the development and efficiency of the PHC workforce.52 Each PHC team member should be working within the full scope of their capabilities in versatile resilient teams, and supported further by a wider regional team through collaboration. The Blueprint for Rural Health provides useful insights for PHC workforce management. Successful recruitment requires inter-sectoral investment in training and career progression in PHC, thus creating a desirable workplace and thereby creating and incentivizing a pool of workers to make a longer-term commitment to a rural area. These initiatives can be successful in attracting and retaining young health professionals to remote and marginalised areas.23
AfroPHC wants Human Resources Better Developed
All team members must be educated in the core competencies to deliver UHC. Focused education of all healthcare professionals for PHC service delivery should be intensified. In addition, all professionals should be trained inter-professionally together in different levels of comprehensive family and community care rather than just in narrow fragmented task-shifting or in the artificial environment of central academic institutions. This will enable the entire PHC team, well trained in the principles of family medicine and generalist PHC, to deliver high-quality bio-psycho-social-spiritual personal healthcare. This must be practiced to a scope that is most efficient for each country.53 Curricula used to educate the health workforce should be reviewed to integrate key competency areas such as clinical prevention, disease management, soft skills (eg, emotional intelligence), entrepreneurship, digital literacy, population health, research, leadership, and management. This approach must be integrated into the basic training, undergraduate, and postgraduate training and continuing professional development. Africa needs to upscale and train more PHC workers to a higher level to ensure a more capable and competent workforce able to provide the needed level of care Some mid-level professional cadres need to be created who will work in partnership with professions, not to serve as substitutes but rather to extend their reach.
Collaboration between all the various cadres of the PHC team in Africa (including CHWs) with lifelong learning will offer better options at scaled up training than offering training en-masse as a once-off exercise. In an AfroPHC workshop, PHC clinicians from Africa shared lessons from the training of family doctors, family nurse practitioners and clinical officers. Some useful lessons were the alignment of training (programmatic learning outcomes informing curriculum content, assessment and educational approach) with resources, and the roles and responsibilities in the health system. An experiential and co-constructivist adult learning approach was considered central to decentralised training centres, workplace-based learning and online support. Liaising with specialists in regional hospitals to create decentralised training platforms can enhance gatekeeping for secondary care and related costs. This onsite training can be further enhanced by online and/or blended learning approaches. The Family Medicine Diploma in Nigeria supported by the Postgraduate Medical College of Nigeria offers a useful template.25 AfroPHC is building a core curriculum for online modular clinical family medicine and PHC training of family doctors, family nurse practitioners and clinical officers. [Box 9] A key challenge is the commonality within Africa around nomenclature of PHC cadres as well as training. Professional credentialing authorities need to come together across Africa to work on this. Training of clinical trainers and national (and even regional) licensing examinations are useful opportunities. We advocate for educational frameworks for PHC in Africa. Governments should invest in research and innovation including creating dedicated domestic funds for building research capacity, offering grants and fellowships, together with the dissemination and utilization of research findings to inform PHC training, practice, and policy. [Box 10]
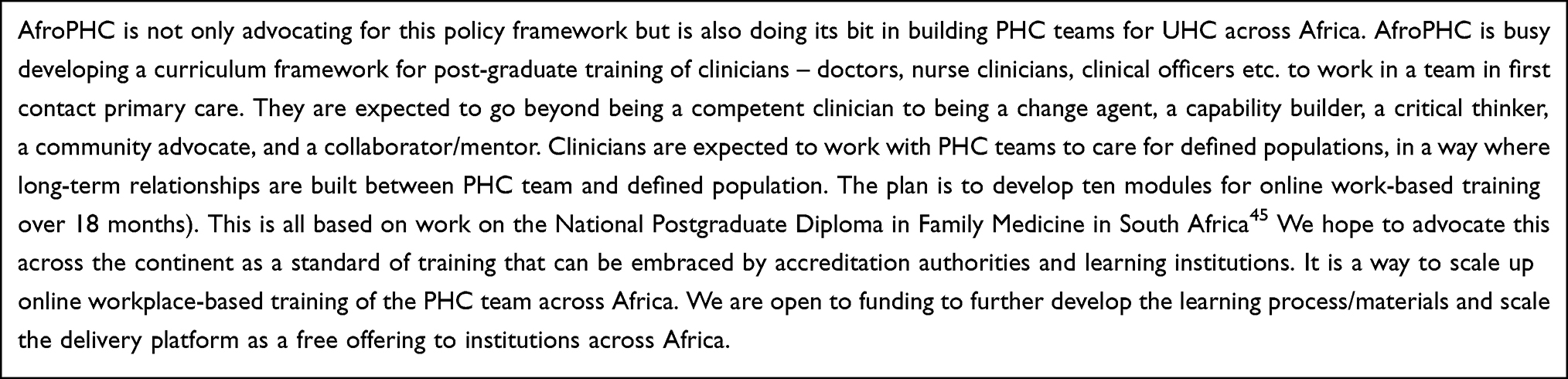 |
Box 9 AfroPHC Diploma in Family Medicine |
 |
Box 10 AfroPHC Research |
AfroPHC wants PHC Workers Protected
Health is on one of the most hazardous sectors for workers, with daily exposure to dangerous diseases, chronic low back pain and poor mental health. Workers in PHC are more at risk due to high patient load, wider exposure, and isolated work dynamics, and the resulting poor access to occupational health services. The PHC workforce in Africa is struggling with urban-rural inequities, fragmented and poor organisation of PHC, poor resourcing of PHC, disempowerment, poor working conditions and challenging community contexts. COVID 19 exposed the vulnerability of PHC workers poor health workforce management, hazardous working conditions, occupationally acquired COVID-19, mental health challenges, etc. Policies for healthier and safer workplaces are part of global commitments to UHC. Such policies will improve quality of care, build resilience and stimulate retention of the healthcare workforce. All this starts with political commitment, and WHO provides excellent resources. Governments need to adopt a bottom-up approach to organisation of PHC by empowering the PHC team, and communities being served, to protect PHC workers. PHC workers working as a multi-disciplinary team can protect each other better.54
PHC Financing
AfroPHC wants Political and Funding Action for PHC as an Investment
The progress on PHC/UHC in Africa is variable. The African Union should be congratulated on its efforts with Agenda 2063, the New Public Health Order and various UHC policies in Africa, with some focus on PHC.55 However, the implementation of PHC/UHC is challenged, not only by factors outside our control but more importantly by factors within our control. Health should not just be viewed as an expense but as an investment and an opportunity for job creation, with resulting economic growth from improvements in both the quantity and quality of human capital.56,57 Government (and AU) commitments on PHC often seem like rhetoric. The Abuja Declaration of 2001, committing AU countries to dedicate at least 15% of their annual budget to enhance sustainable financing of health, has been poorly implemented with only two of the 54 in Africa achieving this.58 The Lancet Report on Financing for PHC (2022) reveals that average GDP per capita PHC expenditure of just $3 (0.4%) is being spent by low-income countries (LICs) on PHC, with out-of-pocket expenditure at $8, room for efficient taxation to create pooled funds. The Lancet Report on Financing for PHC (2022) reveals that low-income countries (LICs) allocate an average of just $3 (0.4%) of GDP per capita on PHC, with out-of-pocket expenditure at $8. The report identified key challenges such as lack of a clear definition of PHC and financing of PHC across Low-Middle Income Countries (LMICs).59 LMICs spend less than 1% of their GDP on PHC compared to the 2% allocation in HICs. Ultimately, the decision to prioritise and invest in PHC is political. However, there are other diverse and creative ways of mobilising funds.
AfroPHC wants Global Solidarity Action on PHC Funding Pools
The reflection on global inequity by Anyangwe (2007) has shown that while sub-Saharan Africa only accounts for 11% of the world’s population it bears over 24% of the global disease burden. The region is home to only 3% of the global health workforce and spends less than 1% of the world’s financial resources on health. This has worsened materially in the last 15 years.60 The Lancet Global Health Commission (2022) on financing primary health care found that government PHC spending by High-Income Countries (HICs) was $840 compared to $3 per capita in Low-Income Countries (LICs), mostly in Africa and on human resources. This means that HICs spend 280 times more than LICs on PHC.59 As of 2019 global health spending stood at about $7.5 trillion per year. Furthermore, to achieve PHC targets globally requires $200 billion (2.6% of $7.5T). To achieve more comprehensive UHC targets requires an additional $170 billion more (2.3% of $7.5T). Global social solidarity contributions of just 4.9% of the world’s health expenditure can take the world forward dramatically and bring the wealth of health to the poorest, especially in Africa.61 Global “aid donors” spend $6 per capita in LICs (twice that of governments) but are invariably fragmenting and distorting the local health system.59 Selective PHC, viz. the GOBI FFF and HIV-AIDS programmes, driven by international agencies seeking low-cost results, has resulted in poor social solidarity, greater fragmentation of PHC and the growing power of hospitals/specialism with poor quality PHC, especially in Africa.62 The 30 by 2030 campaign advocates for donors to allocate 30% of their funds to integrated PHC.63
AfroPHC wants Pooled Funds Managed with Strategic Purchasing
As mentioned previously, the Lancet Global Health Commission (2022) on financing primary health care shows out-of-pocket expenditure at $8 per capita, that is mostly spent on medicines. It advocates for stronger social solidarity using single funding pools with innovative and progressive taxation strategies and mandatory social/community insurance.59 Rwanda, Ghana and Kenya are cited as examples of growing social solidarity. Countries, like Nigeria, have also expanded this pool through innovative policies, like ring-fencing for health “sin-taxes” (“sugar tax” 2022) and allocating specific proportions of the consolidated federation accounts).64 Contributions to this pool from donors can address not only inequities but also reduce fragmentation of funding and integrate service delivery. Line-item budget systems make services unresponsive to the populations served, as accountability is usually to the budget holder, often more centrally. WHO asserts that strategic purchasing must prioritise PHC as the engine for UHC as it reflects the right priorities and remains the most cost-effective way to address comprehensive needs close to people’s home and communities. Strategic purchasing, in line with global PHC thinking, is about separating public providers from the Ministry of Health and empowering them. In addition, it is about introducing private providers into the equation, where possible, and enabling government to play a strong leadership and coordinating role across a regulated and integrated health provider system.22 The Lancet Global Health Commission (2022) advocates for strategic purchasing to improve efficiency in the management of funds. Private health services are a threat to public services in many LMICs as they grow exponentially with populations disaffected with public services. In addition, they contribute to the drawing out human resources into the private sector, in an environment of weak regulatory and enforcement culture. Reversing this can be extremely difficult. Nevertheless, strategic purchasing offers a great opportunity if governments can get ahead of the curve, to draw the private sector into this more regulated environment, provided governments embrace a systems approach with less bureaucracy and a greater focus on simple outcomes.22
AfroPHC wants Reform on PHC Payment with Blended Capitation
Strategic purchasing, with the global best practice payment reforms of blended capitation not only empowers decentralised units of care but also allows the private sector to enter regulated UHC systems. Blended capitation, that is mostly risk-adjusted capitation with some fee-for-service and performance payment, is a global best practice.22 Current line-item budgetary systems are unresponsive to users. Whilst fee-for-service is more responsive, it can easily be abused by providers. Mixed or blended capitation payment allows empanelment of populations. A dominantly per capita payment system is better suited to the complex bio-psycho-social-spiritual nature of PHC than fee-for-service payments.22 Important elements of PHC service are difficult to re-imburse in a fee-for-service system, eg, teamwork, community work, group work or health promotion. Adjustments in capitation rates can target equity, eg, risk groups, multi-morbidity, rurality, or socio-economic status better over time with enrollee data. Nationally defined mixed or blended capitation contracts offer a great opportunity for PHC where enrollees can regularly vote with their feet and change providers.22
Simple National Contracting
Many critics will consider this framework a long and incoherent wish list. This can all come together into a simple and practical national PHC contracting system. An example is the National Health Insurance PHC Capitation Framework, as developed for the National Treasury of South Africa. Community practices defined by population and an appropriate mix of skills, including family doctors, using numbers that are in line with the country’s human resources of public and private providers can be set up quite easily across the country. A nationally defined PHC contract using risk-adjusted blended capitation can be easily administered at national or sub-national level for both public and private providers. They should be coordinated by the district health services to provide services to the full population, especially marginalised communities, in a manner that is regulated and respectful of the abilities of PHC teams (which include professionals) to be able to manage resources from appropriate payment systems, be resilient to emergencies and progressively adjust the care to the needs of the populations served [https://profmoosa.com/summary-of-proposed-nhi-capitation-contract-design/].
Conclusion
AfroPHC’s adopted vision of African PHC service delivery under Universal Health Coverage (UHC) is that it should be comprehensive, accessible, of high quality, responsive to local needs, be in partnership with communities and delivered by strong teamwork that has adequate training and supportive supervision. We see ourselves practicing in community practices as a PHC team with skills mix appropriate to Africa, including family doctors, family nurse practitioners, clinical officers, community health workers and others that are empowered to take care of an empaneled population in high-quality people centred PHC.
Primary health care has been considered the most equitable, effective, efficient, and cost-effective approach to achieving UHC. AfroPHC calls on Africa to empower and build an effective PHC team to achieve PHC and UHC in Africa by 1) building robust PHC systems, 2) educating, recruiting, and maintaining a sufficient frontline PHC workforce and 3) supporting PHC with finances. [Box 11]
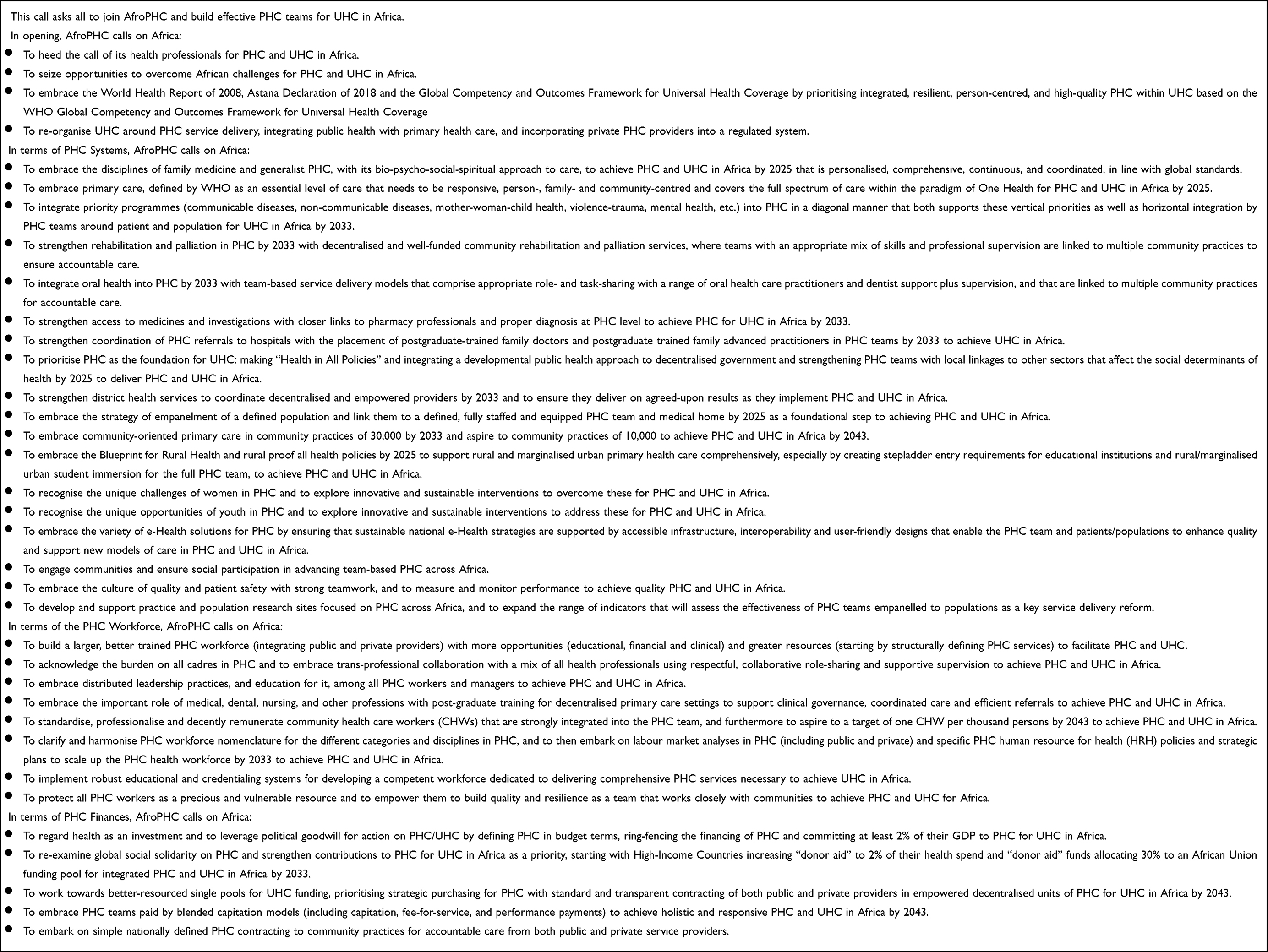 |
Box 11 A Call to Africa |
PHC systems must be based on a high-quality bio-psycho-social-spiritual approach for PHC that is comprehensive, coordinated and integrated person-, family- and community-centred. It must integrate PHC priorities and Health in All Policies. It must be based on empanelling of defined populations to a specific PHC team using community-oriented primary care. It must be supported by interoperable e-Health and a strong DHS to coordinate public and private providers.
Educating, recruiting, and maintaining a sufficient frontline PHC workforce must include a complete workforce of locally trained family doctors, family nurse practitioners, medical officers, clinical officers, nurses, professionalised CHWs and other cadres and allied health care professionals, to ensure delivery of high-quality PHC. This workforce must involve role-sharing with supportive supervision; distributed leadership; clinical governance by accountable clinicians; and an integrated human resource development and management plan suitable for PHC.
Supporting PHC with finances must be political and sustained action that considers PHC an investment; a fight for global solidarity action on PHC funding pools; and better management of PHC across Africa with strategic purchasing and payment reforms using blended capitation.
We, as the African Forum for Primary Health Care (AfroPHC), commit to educating and empowering providers and their communities at the frontline to support this goal in any way we can, including building AfroPHC Chapters at country level as a forum for PHC and UHC in Africa.
AfroPHC calls on Africa to commit to making this plan a reality and building effective PHC teams for UHC in Africa. AfroPHC commits to mobilising PHC workers across Africa to create teams around empanelled populations as sentinel sites across Africa to share best practices and to show evidence of how effective we can be at both practice and population level, if we are empowered to deliver quality PHC as a team.
Acknowledgments
This work has been the product of extensive consultations within the AfroPHC network, especially the AfroPHC Executive and Advisory Boards.
Funding
The AfroPHC process of further consultation resulting in this article was funded by PHC Performance Initiative, Award Number: PHC-CSO-04 and Wits Health Consortium.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Barasa E, Solange H, Fenny Ama P, et al. The state of universal health coverage in Africa.
2. International Conference on Primary Health Care. Alma Ata Declaration. Alma Ata; 1978.
3. World Health Organisation. The world health report 2008: primary health care–now more than ever. Geneva; 2008.
4. Global Conference on Primary Health Care. Declaration of Astana. Astana; 2018 October.
5. Barış E, Silverman R, Wang H, Zhao F, Pate MA. WALKING the TALK Reimagining Primary Health Care After COVID-19. World Bank Publications; 2022.
6. Starfield B, Shi L, Macinko J. Contribution of primary care to health systems and health. Milbank Q. 2005;83(3):457–502. doi:10.1111/j.1468-0009.2005.00409.x
7. Moosa S. Community-oriented primary care for National Health Insurance in South Africa. Afr J Prm Health Care Fam Med. 2021;13(1):3243.
8. African Forum for Primary Health Care. AfroPHC [Internet]. Website. [cited December 4, 2021]. Available from: https://afrophc.org/.
9. Word Health Organization and the United Nations Childrens Fund (UNICEF). Operational framework for primary health care transforming vision into action. 2020.
10. Ogaji DS, Giles S, Daker-White G, Bower P. Systematic review of patients’ views on the quality of primary health care in sub-Saharan Africa. SAGE Open Med. 2015;3:2050312115608338. doi:10.1177/2050312115608338
11. Campbell-Hall V, Petersen I, Bhana A, Mjadu S, Hosegood V, Flisher AJ. Collaboration between traditional practitioners and primary health care staff in South Africa: developing a workable partnership for community mental health services. Transcult Psychiatry. 2010;47(4):610–628. doi:10.1177/1363461510383459
12. German Constituency. Integration of the one health approach into the work of the global fund to fight AIDS, TB and malaria [Internet]. Available from: https://www.oie.int/fileadmin/Home/eng/Media_Center/docs/pdf/Tripartite_2017.pdf.
13. Pucca GA
14. Wang T, Mathur MR, Schmidt H. Universal health coverage, oral health, equity and personal responsibility. Bull World Health Organ. 2020;98(10):719–721. doi:10.2471/BLT.19.247288
15. Starfield B. Primary care: an increasingly important contributor to effectiveness, equity, and efficiency of health services. SESPAS report 2012. Gac Sanit. 2012;26(5):25–31. doi:10.1016/j.gaceta.2011.10.009
16. Macinko J, Starfield B, Erinosho T. The impact of primary healthcare on population health in low- and middle-income countries. J Ambul Care Manage. 2009;32(2):150–171. doi:10.1097/JAC.0b013e3181994221
17. Sturmberg JP, Martin CM. Complexity and health - Yesterday’s traditions, tomorrow’s future. J Eval Clin Pract. 2009;15:543–548. doi:10.1111/j.1365-2753.2009.01163.x
18. Moosa S Summary of proposed NHI capitation contract design [Internet]. Post; 2019 [cited 2021 Dec 4]. Available from: https://profmoosa.com/summary-of-proposed-nhi-capitation-contract-design/.
19. Strategic Purchasing Africa Resource Centre. Strategic purchasing Africa resource centre [Internet]. [cited December 4, 2021]. Available from: https://sparc.africa/.
20. Joint Learning Network for Universal Health Coverage (JLN). Empanelment: a foundational component of primary health care. 2019.
21. Moosa S. Community-oriented primary care for National Health Insurance in South Africa. Afr J Prim Health Care Fam Med. 2022;14(1). doi:10.4102/phcfm.v14i1.3243
22. Moosa S. Provider perspectives on financing primary health care for universal health coverage. Lancet Glob Health. 2022;10(5):e609–10. doi:10.1016/S2214-109X(22)00173-5
23. Wonca Rural Health. Blueprint for rural health.
24. Okwor T Community health worker programme in Nigeria.
25. Postgraduate Medical College of Nigeria. Diploma in family medicine programme [Internet]. [cited July 20, 2022]. Available from: https://npmcn.edu.ng/diploma-in-family-medicine-programme/.
26. Abimbola S, Okoli U, Olubajo O, Abdullahi MJ, Pate MA. The Midwives service scheme in Nigeria. PLoS Med. 2012;9(5):e1001211. doi:10.1371/journal.pmed.1001211
27. Kruk M, Pate M. The Lancet Global Health Commission on High Quality Health Systems 1 year on: progress on a global imperative. Lancet. 2020;8(1):e30–e32.
28. National Department of Health. National digital health strategy for South Africa 2019–2024; 2019.
29. Mbunge E, Batani J, Gaobotse G, Muchemwa B. Virtual healthcare services and digital health technologies deployed during coronavirus disease 2019 (COVID-19) pandemic in South Africa: a systematic review. Glob Health J. 2022;6(2):102–113. doi:10.1016/j.glohj.2022.03.001
30. Pagliari C. Digital health and primary care: past, pandemic and prospects. J Glob Health. 2021;11:1–9. doi:10.7189/jogh.11.01005
31. Handbook on social participation for universal health coverage [Internet]. Geneva; 2021. Available from: http://socialparticipationhandbook.info/Register.
32. Kruk ME, Gage AD, Arsenault C, et al. High-quality health systems in the sustainable development goals era: time for a revolution. Lancet Glob Health. 2018;6(11):e1196–252. doi:10.1016/S2214-109X(18)30386-3
33. Jaca A, Malinga T, Iwu-Jaja CJ, et al. Strengthening the health system as a strategy to achieving a universal health coverage in underprivileged communities in Africa: a scoping review. Environ Health Res. 2022;19(1):587.
34. Veillard J, Cowling K, Bitton A, et al. Better measurement for performance improvement in low- and middle-income countries: the Primary Health Care Performance Initiative (PHCPI) experience of conceptual framework development and indicator selection. Milbank Q. 2017;95(4):836–883. doi:10.1111/1468-0009.12301
35. World Health Organization. Primary health care measurement framework and indicators: monitoring health systems through a primary health care lens; 2022.
36. World Health Organization Africa. Tracking universal health coverage in the WHO African Region, 2022; 2022.
37. Chreim S, Williams BE, Janz L, Dastmalchian A. Change agency in a primary health care context: the case of distributed leadership. Health Care Manage Rev. 2010;35(2):187–199. doi:10.1097/HMR.0b013e3181c8b1f8
38. Brown J, Lewis L, Ellis K, Stewart M, Freeman TR, Kasperski MJ. Conflict on interprofessional primary health care teams can it be resolved? J Interprof Care. 2011;25(1):4–10. doi:10.3109/13561820.2010.497750
39. Macnaughton K, Chreim S, Bourgeault IL. Role construction and boundaries in interprofessional primary health care teams: a qualitative study. BMC Health Serv Res. 2013;13(486):1–13. doi:10.1186/1472-6963-13-486
40. Chreim S, Langley A, Comeau-Vallée M, Huq JL, Reay T. Leadership as boundary work in healthcare teams. Leadership. 2013;9(2):201–228. doi:10.1177/1742715012468781
41. Moosa S. Family doctor leadership in African primary health care. Afr J Prim Health Care Fam Med. 2021;13(1):1–2. doi:10.4102/phcfm.v13i1.3198
42. Angood P, Birk S. The value of physician leadership. Physician Educ J. 2014;40(3):6–22.
43. Ana J. Clinical governance in Nigerian hospitals: Nigerian Medical Association leads. Afr Health. 2014;36(2):5–7.
44. Ballard M, Alban R, Nandini V, et al. Compensation models for community health workers: comparison of legal frameworks across five countries Carey Westgate Community Health Impact Coalition. J Glob Health. 2021. doi:10.21203/rs.3.rs-36222/v1
45. Mash R, Malan Z, von Pressentin K, Blitz J. Strengthening primary health care through primary care doctors: the design of a new national Postgraduate Diploma in Family Medicine. S Afr Fam Pract. 2015;6190:1–5.
46. Olaniran A, Madaj B, Bar-Zev S, van den Broek N. The roles of community health workers who provide maternal and newborn health services: case studies from Africa and Asia. BMJ Glob Health. 2019;4(4):e001388. doi:10.1136/bmjgh-2019-001388
47. Malhotra B, Dasgupta U, Basu G; World Health Organization. Regional Office for South-East Asia. Improving Retention of Health Workers in Rural and Remote Areas: Case Studies from WHO South-East Asia Region; 2020:231.
48. World Health Organisation. The world health report 2006: working together for health. Geneva; 2006.
49. Global health observatory [Internet]. [cited April 7, 2022]. Available from: https://www.who.int/data/gho.
50. First Global Forum on Human Resources for Health. The Kampala declaration and agenda for global action. Kampala; 2008.
51. Crisp N, Cantab KM. A global perspective on the education and training of primary care and public health professionals. Lond J Prim Care. 2012;4(2):116–119. doi:10.1080/17571472.2012.11493347
52. World Health Organisation Regional Office for Africa. Regional road map for scaling up the health workforce by 2025; 2012.
53. World Health Organization. Global competency and outcomes framework for universal health coverage; 2022.
54. World Health Organization. CARING FOR THOSE WHO CARE Guide for the development and implementation of occupational health and safety programmes for health workers; 2022.
55. African Union. Africa agenda 2063 [Internet]. Webpage. [cited December 5, 2021]. Available from: https://au.int/agenda2063.
56. Horton R, Araujo EC, Bhorat H, et al. Final report of the expert group to the high-level commission on health employment and economic growth. World Health Organization [Internet]; 2016:84. Available from: http://apps.who.int/iris/bitstream/10665/250040/1/9789241511285-eng.pdf?ua=1.
57. World Health Organisation. Working for health and growth: investing in the health workforce. Report of the high-level commission on health employment and economic growth. Geneva; 2016.
58. World Health Organisation. The Abuja declaration: ten years on. Geneva; 2011.
59. Hanson K, Brikci N, Erlangga D, et al. The Lancet Global Health Commission on financing primary health care: putting people at the centre. Lancet Globl Health. 2022;10(5):e715–72. doi:10.1016/S2214-109X(22)00005-5
60. Anyangwe SCE, Mtonga C. Inequities in the global health workforce: the greatest impediment to health in Sub-Saharan Africa. Int J Environ Res Public Health. 2007;4:93–100. doi:10.3390/ijerph2007040002
61. World Health Organization. Primary health care on the road to universal health coverage: 2019 monitoring report: executive summary. Geneva; 2019.
62. Rifkin SB, Rifkin SB. Health for all and primary health care, 1978–2018: a historical perspective on policies and programs over 40 years. Oxford Research Encyclopedia of Global Public Health; 2018.
63. De Maeseneer J, Li D, Palsdottir B, et al. Universal health coverage and primary health care: the 30 by 2030 campaign. Bull World Health Organ. 2020;98(11):812–814. doi:10.2471/BLT.19.245670
64. How does BHCPF, Nigeria’s healthcare programme, work? ONE [Internet]. [cited July 31, 2022]. Available from: https://www.one.org/africa/blog/how-does-bhcpf-work/.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.