Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 17
Exploring Promising Therapies for Non-Alcoholic Fatty Liver Disease: A ClinicalTrials.gov Analysis
Authors Hegazi OE ![]() , Alalalmeh SO
, Alalalmeh SO ![]() , Shahwan M, Jairoun AA, Alourfi MM, Bokhari GA, Alkhattabi A, Alsharif S, Aljehani MA, Alsabban AM, Almtrafi M, Zakri YA, AlMahmoud A, Alghamdi KM, Ashour AM
, Shahwan M, Jairoun AA, Alourfi MM, Bokhari GA, Alkhattabi A, Alsharif S, Aljehani MA, Alsabban AM, Almtrafi M, Zakri YA, AlMahmoud A, Alghamdi KM, Ashour AM ![]() , Alorfi NM
, Alorfi NM ![]()
Received 16 November 2023
Accepted for publication 11 January 2024
Published 2 February 2024 Volume 2024:17 Pages 545—561
DOI https://doi.org/10.2147/DMSO.S448476
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Antonio Brunetti
Omar E Hegazi,1,2 Samer O Alalalmeh,1,2 Moyad Shahwan,1,2 Ammar Abdulrahman Jairoun,3,4 Mansour M Alourfi,5,6 Ghfran Abdulrahman Bokhari,6 Abdullah Alkhattabi,6 Saeed Alsharif,7 Mohannad Abdulrahman Aljehani,8 Abdulmalik Mohammed Alsabban,9 Mohammad Almtrafi,9 Ysear Abdulaziz Zakri,9 Abdullah AlMahmoud,10 Khalid Mohammed Alghamdi,10 Ahmed M Ashour,11 Nasser M Alorfi11
1Center of Medical and Bio-Allied Health Sciences Research, Ajman University, Ajman, United Arab Emirates; 2Department of Clinical Sciences, College of Pharmacy and Health Sciences, Ajman University, Ajman, United Arab Emirates; 3Health and Safety Department, Dubai, United Arab Emirates; 4School of Pharmaceutical Sciences, Universiti Sains Malaysia, Pulau Pinang, Malaysia; 5Internal medicine Department, King Faisal Medical City for Southern Region, Abha, Saudi Arabia; 6Department of gastroenterology, East Jeddah hospital, Jeddah, Saudi Arabia; 7Gastroenterology Department, Armed force Hospital of southern region, Khamis Mushait, Saudi Arabia; 8Division of Gastroenterology, Department of Medicine, King Faisal Specialist Hospital and Research Centre, Jeddah, Saudi Arabia; 9Gastroenterology Section, Department of Medicine, King Abdulaziz Medical City, Jeddah, Saudi Arabia; 10Gastroenterology Section, Internal Medicine Department, King Fahad Hospital, Jeddah, Saudi Arabia; 11Department of Pharmacology and Toxicology, College of Pharmacy, Umm Al-Qura University, Makkah, Saudi Arabia
Correspondence: Nasser M Alorfi, Department of Pharmacology and Toxicology, College of Pharmacy, Umm Al-Qura University, Makkah, Saudi Arabia, Email [email protected]
Background: Non-alcoholic fatty liver disease (NAFLD) is a common disease and has been increasing in recent years. To date, no FDA-approved drug specifically targets NAFLD.
Methods: The terms “Non-alcoholic Fatty Liver Disease” and “NAFLD” were used in a search of ClinicalTrials.gov on August 24, 2023. Two evaluators independently examined the trials using predetermined eligibility criteria. Studies had to be interventional, NAFLD focused, in Phase IV, and completed to be eligible for this review.
Results: The ClinicalTrials.gov database was searched for trials examining pharmacotherapeutics in NAFLD. The search revealed 1364 trials, with 31 meeting the inclusion criteria. Out of these, 19 were finalized for evaluation. The dominant intervention model was Parallel. The most prevalent studies were in Korea (26.3%) and China (21.1%). The most common intervention was metformin (12.1%), with others like Exenatide and Pioglitazone accounting for 9.1%.
Conclusion: Therapeutics used to manage NAFLD are limited. However, various medications offer potential benefits. Further investigations are definitely warranted.
Keywords: NAFLD, hepatology, clinical trials, therapeutics, metabolic disorder
Introduction
Non-alcoholic fatty liver disease (NAFLD) is a common disease today, reflecting the increasing rates of obesity, metabolic syndrome, and type 2 diabetes mellitus (T2DM).1,2 The pathophysiology of NAFLD includes multifaceted interactions between insulin resistance, abnormal lipid homeostasis, oxidative stress, and inflammation.3,4 While non-pharmacological interventions, especially dietary and weight loss strategies, are the foundational management techniques for NAFLD, the persistence and adherence to such measures remain a challenge.5
Several promising therapeutic agents such as Peroxisome proliferator-activated receptor agonists, Farnesoid X receptor agonists, Glucagon-like peptide-1 (GLP-1) receptor agonists, and sodium-glucose cotransporter 2 (SGLT2) inhibitors are undergoing further analysis for their potential efficacy to counteract NAFLD progression. They work by modulating insulin sensitivity, rectifying lipid metabolism, abating hepatic inflammation, and reducing the risk of fibrosis and cirrhosis.6–8 Current management emphasizes lifestyle modification including weight management. For instance, the Mediterranean diet, abundant in whole foods and beneficial fats, has shown promise in ameliorating hepatic lipid content and insulin dynamics in NAFLD individuals.9,10
Clinical trial databases, with ClinicalTrials.gov leading the cohort, serve as indispensable repositories for gauging the efficacy and safety of innovative interventions.11 As of today, ClinicalTrials.gov alone encompasses a large range of clinical trials. Despite the growing amount of literature highlighting the potential of pharmacological interventions for NAFLD, the methodical assessment of clinical trials assessing these remedies is conspicuously lacking. Although ClinicalTrials.gov serves as an invaluable corpus of such trials, a dedicated review encapsulating the role of pharmacotherapeutics within the NAFLD therapeutic landscape is still awaited.
Methodological Framework and Research Design
Search Strategy and Inclusion Criteria
On August 24, 2023, a thorough search of ClinicalTrials.gov was conducted using the keywords “Non-alcoholic Fatty Liver Disease” and “NAFLD”. Two evaluators reviewed the trials using established eligibility standards to ensure objectivity. To qualify, studies needed to focus predominantly on NAFLD and be interventional, in addition to being in Phase IV and being concluded.
Results
The preliminary search of the ClinicalTrials.gov database yielded 1364 trials. These were subsequently screened and filtered. Exclusion criteria were applied, eliminating trials that were incomplete (n = 762), non-interventional (n = 98), or outside of phase IV (n = 473). Initially, 31 studies met the inclusion parameters for our review. Upon further examination, 12 trials were excluded due to their inadequate focus on NAFLD. Thus, a total of 19 clinical trials were finalized for evaluation. The stepwise selection methodology is graphically represented in Figure 1, detailing the approach used to discern the pertinent clinical trials for this study.
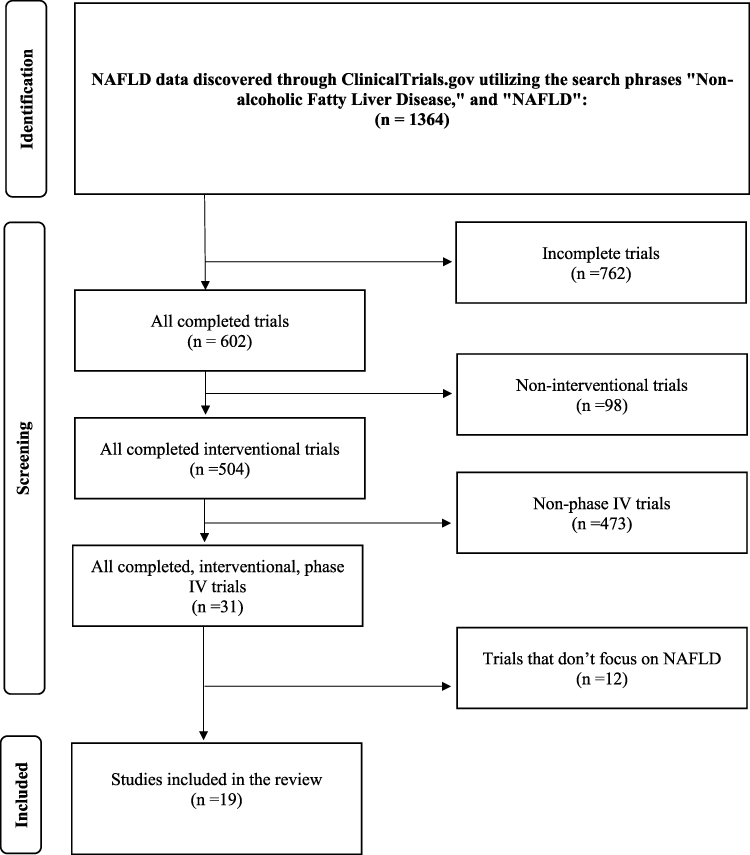 |
Figure 1 Flow diagram of trial selection process. |
Characteristics of Included Studies
Table 1 shows the description of the clinical trials studied. Most studies (89.5%) were randomized, while 10.5% were non-applicable regarding allocation. The primary intervention model used was Parallel (84.2%), followed by Single Group (10.5%) and Crossover (5.3%).
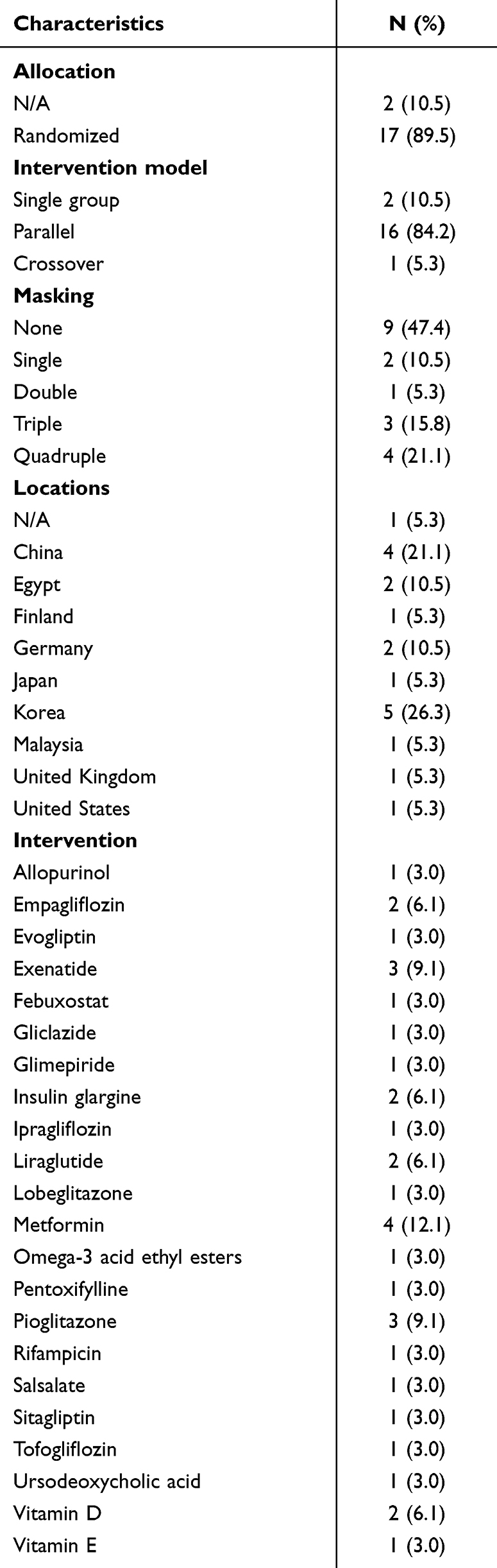 |
Table 1 Trial Characteristics |
In terms of masking, nearly half (47.4%) had no masking, and the remaining studies employed Single (10.5%), Double (5.3%), Triple (15.8%), or Quadruple (21.1%) masking techniques. Geographically, Korea was the most common location for these studies, hosting just over one quarter (26.3%). China followed with 21.1%, and other countries, including Egypt and Germany, ranged from 5.3% to 10.5% of the studies.
Various interventions were used, with metformin being the most prevalent (12.1%). Other interventions such as Exenatide and Pioglitazone were used in 9.1% of the trials, and a diversity of other treatments appeared in 3.0% to 6.1% of the studies. Further details can be found in Table 2.
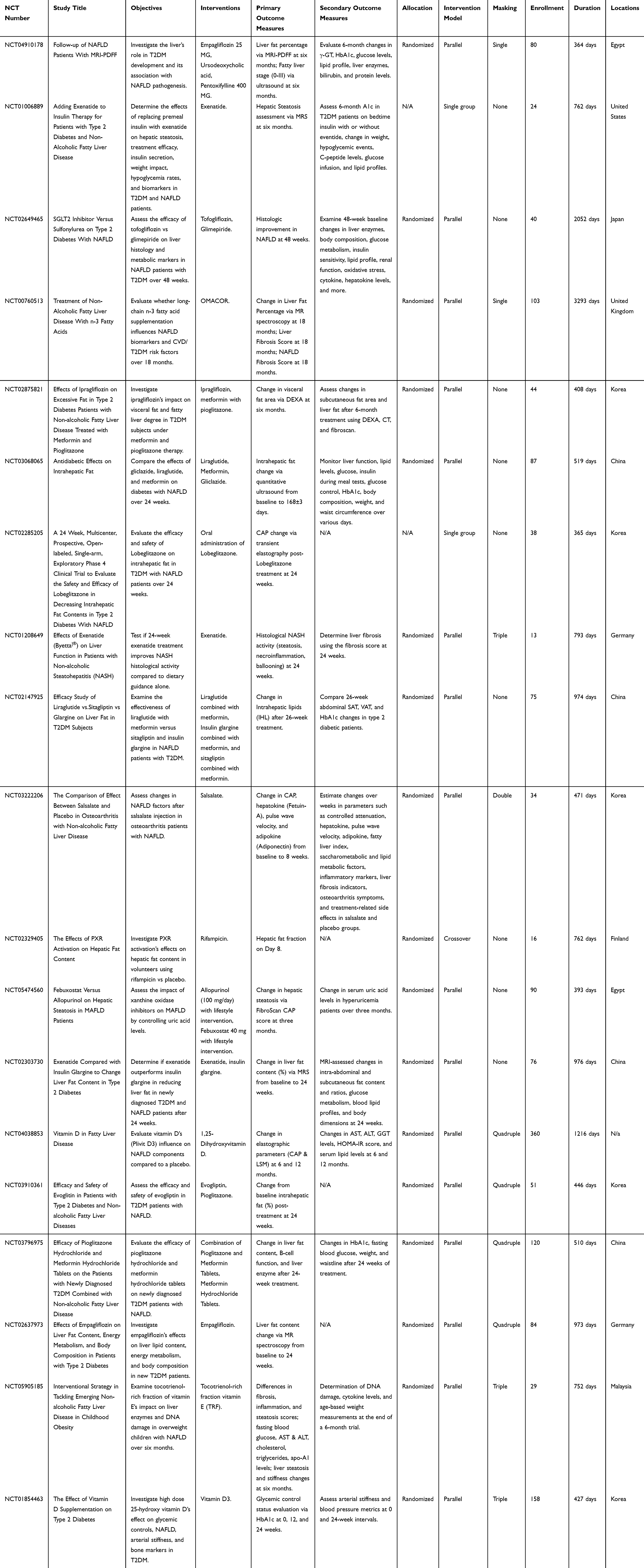 |
Table 2 Overview of the Clinical Trials |
Pharmacological Treatment and Management Strategies
Allopurinol
Allopurinol, a xanthine oxidase inhibitor, is used mainly for hyperuricemia and gout. Other indications include cardiovascular and kidney diseases.12,13 Allopurinol exerts its therapeutic effect by inhibiting xanthine oxidase, a critical enzyme in the metabolic pathway that transforms hypoxanthine into xanthine and subsequently into uric acid.13 Through this inhibition, allopurinol not only effectively lowers serum uric acid concentrations but also diminishes the production of reactive oxygen species.14,15
Elevated serum uric acid levels correlate independently with a heightened severity of hepatic steatosis and fibrosis.16–18 The underlying pathophysiological mechanisms that might bridge hyperuricemia with NAFLD include insulin resistance and oxidative stress.19 Notably, one specific trial incorporated allopurinol to evaluate the impact of xanthine oxidase inhibitors on MAFLD by regulating uric acid concentrations.
Empagliflozin
Empagliflozin, an SGLT2 inhibitor, is predominantly used to manage type 2 diabetes. Its mechanism of action involves inhibiting the SGLT2 protein within the proximal tubules of the kidneys, which in turn facilitates the excretion of glucose via the urine. This results in a notable reduction of blood glucose concentrations.20 Empagliflozin is used also for weight reduction, decreased blood pressure, and enhancements in cardiovascular health outcomes.21
The intricate relationship between T2DM and NAFLD has been conclusively identified. NAFLD is currently acknowledged as the hepatic representation of the metabolic syndrome.22 Given the proven efficacy of SGLT2 inhibitors in managing T2DM, there is’ growing interest in their potential applicability in NAFLD therapy.23,24 Empirical evidence from studies on empagliflozin indicates that its administration is linked to a substantial reduction in hepatic fat accumulation and improved liver enzyme in people with T2DM.25 Moreover, Empagliflozin’s potential to exert anti-inflammatory and antifibrotic effects is a subject of ongoing research. Preliminary findings are pointing toward encouraging results.26 Notably, two clinical trials incorporated empagliflozin to report its influence on liver lipid content, energy metabolism, and overall body composition in recently diagnosed T2DM patients.
Evogliptin
Evogliptin, a dipeptidyl peptidase-4 (DPP-4) inhibitor, is predominantly used for managing T2DM by augmenting insulin secretion and reducing glucagon secretion.27 Research has suggested that DPP-4 inhibitors could have therapeutic implications in NAFLD due to their influence on hepatic lipid metabolism and their inherent anti-inflammatory attributes.28 In preclinical models, Evogliptin has demonstrated notable benefits by mitigating hepatic steatosis, inflammation, and fibrosis.29 One trial incorporated Evogliptin to evaluate its efficacy and safety for T2DM patients concurrently diagnosed with NAFLD.
Exenatide
Exenatide, a GLP-1 receptor agonist, is commonly prescribed for managing T2DM. Its mechanism of action involves enhancing insulin release, curbing glucagon secretion, and decelerating gastric emptying.30,31 Within the realm of NAFLD, Exenatide, alongside other GLP-1 agonists, has attracted attention due to its potential benefits: promoting weight reduction, heightening insulin sensitivity, and exhibiting hepatoprotective properties.32,33 Notably, the weight reduction achieved via exenatide might indirectly confer advantages to NAFLD patients, considering the pronounced link between obesity and the onset of NAFLD.33
Three trials integrated exenatide into their experimental designs with varied objectives. One aimed to assess the outcomes of substituting premeal insulin with exenatide in terms of hepatic steatosis, therapeutic efficacy, insulin secretion, weight modulation, rates of hypoglycemia, and pertinent biomarkers in patients with T2DM and NAFLD. Another sought to evaluate whether a 24-week Exenatide regimen ameliorates histological activity in NASH compared to dietary guidance alone. The last delved into the comparative efficacy of exenatide and insulin glargine in diminishing liver fat in patients newly diagnosed with T2DM and NAFLD over 24 weeks.
Febuxostat
Febuxostat, a non-purine selective xanthine oxidase inhibitor, is mainly prescribed for managing hyperuricemia in patients with gout.34 Numerous studies have underscored the potential influence of uric acid on the pathogenesis of NAFLD, pinpointing oxidative stress as a pivotal mechanism.14,15 Emerging evidence indicates that Febuxostat has the potential to counteract oxidative stress, reduce lipid accumulation in the liver, and alleviate inflammation; factors that are fundamental to the onset and progression of NAFLD.35 One trial incorporated Febuxostat in its design, aiming to evaluate the effects of xanthine oxidase inhibitors on MAFLD through the modulation of uric acid levels.
Gliclazide
Gliclazide is an oral sulfonylurea antidiabetic agent that stimulates insulin secretion from the pancreatic beta cells by binding to specific receptors on these cells, causing ATP-sensitive potassium channels to close.36,37
Intriguingly, research has shed light on gliclazide’s potential for mitigating liver steatosis and inflammation, especially as evidenced in rodent models.38 Key mechanisms that have been posited include enhancing insulin sensitivity, promoting antioxidant actions, and modulating the release of proinflammatory cytokines.39–41 In a singular trial, gliclazide was incorporated to compare its effects with those of liraglutide and metformin, specifically addressing diabetes concomitant with NAFLD over 24 weeks.
Glimepiride
Glimepiride is an oral medication often used for treating T2DM. It operates similarly to gliclazide, enhancing insulin release from the pancreas by specifically interacting with the sulfonylurea receptor. This interaction leads to the shutting down of ATP-sensitive potassium channels.42 Notably, glimepiride exhibits a range of additional effects, including significant anti-inflammatory and antioxidative properties. Emerging research suggests that glimepiride may also protect the liver. This potential benefit is primarily due to its ability to reduce oxidative stress and inflammation, key factors in the development of NAFLD.43 Moreover, glimepiride’s role in improving blood sugar control and increasing insulin sensitivity could indirectly help in alleviating NAFLD.44 In one study, the effectiveness of glimepiride was compared to that of tofogliflozin, focusing on their effects on liver health and metabolic indicators in NAFLD patients with T2DM over a period of 48 weeks.
Insulin Glargine
Insulin glargine, a long-acting insulin, is used for DM. Its relevance in NAFLD is notable, as it may counteract fat buildup in the liver by improving blood sugar control.45–47 While there is’ a theory that exogenous insulin administration might intensify hepatic steatosis,48 insulin glargine, through its potential to enhance glycemic control and reduce glycemic variability, might counteract these adverse effects.49,50 This aspect was investigated in two studies: one compared the efficacy of liraglutide with metformin against that of sitagliptin and insulin glargine, for treating T2DM patients with NAFLD. The other study evaluated whether exenatide is more effective than insulin glargine in reducing liver fat in newly diagnosed T2DM and NAFLD patients over 24 weeks.
Ipragliflozin
Ipragliflozin, part of the SGLT2 inhibitor medication class, is noted for its promising effects on liver steatosis and fibrosis.51,52 Extensive studies indicate that Ipragliflozin can reduce liver fat, improve liver enzyme levels, and potentially reduce signs of liver fibrosis.52–54 These positive effects are thought to stem from several mechanisms, such as weight reduction, increased insulin sensitivity, and direct anti-inflammatory effects on the liver.53,55 One trial incorporated Ipragliflozin to investigate its impact on visceral fat and the extent of fatty liver in T2DM patients undergoing metformin and pioglitazone treatment.
Liraglutide
Liraglutide, a GLP-1 receptor agonist similar to Exenatide, has garnered attention in the study of NAFLD. The LEAN trial highlighted its effectiveness, demonstrating liraglutide’s ability to resolve non-alcoholic steatohepatitis more effectively than a placebo, without worsening fibrosis.56 The positive effects of liraglutide in patients with NAFLD/NASH may be attributed to various factors including weight loss promotion, reduction in liver fat accumulation, anti-inflammatory properties, and possible direct antifibrotic effects.57–61 Two trials incorporated liraglutide into their study design with distinct objectives. One trial sought to compare the effects of gliclazide, liraglutide, and metformin on diabetes patients afflicted by NAFLD over 24 weeks. Another aimed to compare the efficacy of combining liraglutide with metformin with the effectiveness of sitagliptin and insulin glargine, specifically targeting NAFLD patients diagnosed with T2DM.
Lobeglitazone
Lobeglitazone is a member of the thiazolidinedione family, known for enhancing insulin sensitivity.62 These medications work by activating the peroxisome proliferator-activated receptor gamma, leading to improved insulin response in peripheral tissues.63 Research indicates that Lobeglitazone may reduce liver fat, improve the histological characteristics of NASH, and potentially have antifibrotic effects.64,65 One study was conducted to evaluate the effectiveness and safety of Lobeglitazone in reducing intrahepatic fat in patients with T2DM patients and NAFLD over 24 weeks.
Metformin
Metformin, a biguanide antihyperglycemic agent, is widely used to treat T2DM, mainly by reducing liver glucose production and increasing muscle insulin sensitivity.66 Its potential effectiveness in managing NAFLD has become a subject of interest. However, research outcomes have been inconsistent; while some studies suggest benefits like reduced liver enzymes and liver fat, others find its effects comparable to those of lifestyle changes in terms of improving liver health.67,68 Recent clinical trials have further explored its efficacy, including its use in combination with other treatments like ipragliflozin, pioglitazone, liraglutide, gliclazide, sitagliptin, and insulin glargine, in patients with coexisting T2DM and NAFLD.
Omega-3 Acid Ethyl Esters (OMACOR)
In the field of molecular biochemistry, Omega-3 acid ethyl esters, which are derived from longer-chain omega-3 fatty acids like eicosapentaenoic acid and docosahexaenoic acid, have been recognized for their heart-protective properties.69,70 Recently, there has’ been growing interest in these fatty acids within the scope of NAFLD, largely due to their reported anti-inflammatory, antioxidative, and lipid-modulating effects.5,71 In a trial, Omega-3 acid ethyl esters were incorporated to discern the influence of long-chain n-3 fatty acid supplementation on NAFLD biomarkers and the risk factors associated with cardiovascular disease and T2DM over an 18-month span.
Pentoxifylline
Pentoxifylline, a drug derived from methylxanthine, is primarily used to treat intermittent claudication resulting from peripheral artery disease.72 Its possible role in treating NAFLD arises from its significant anti-inflammatory and antifibrotic properties. A key mechanism of pentoxifylline involves inhibiting tumor necrosis factor-alpha (TNF-α), a critical cytokine involved in inflammation and the progression of NAFLD. Various clinical studies have assessed its effectiveness in patients with NAFLD/NASH, with initial results highlighting its potential benefits, particularly in reducing liver enzymes and indicators of liver damage. Additionally.73 One trial incorporated pentoxifylline to examine the liver’s contribution to the onset of T2DM and its correlation with the pathogenesis of NAFLD.
Pioglitazone
Pioglitazone, a key drug in the thiazolidinedione class, primarily acts as an insulin sensitizer by targeting the peroxisome proliferator-activated receptor gamma.74 The drug helps reduce liver steatosis and inflammation, possibly due to improved insulin sensitivity, reduced inflammation in fat tissue, and altered lipid metabolism.75 Recent studies also highlight its potential in managing NAFLD by reducing liver fat and inflammation, attributed to enhanced insulin sensitivity and adjustments in lipid metabolism.76 Despite its efficacy in improving NAFLD, particularly in diabetic patients, caution is necessary due to side effects like weight gain and the risks of bone fractures and bladder cancer, underscoring the need for a balanced risk-to-benefit assessment.8,77 Three clinical trials involving pioglitazone were conducted with distinct goals: assessing ipragliflozin’s impact on visceral fat in T2DM patients on metformin and pioglitazone; evaluating the efficacy and safety of evogliptin in T2DM patients with NAFLD, and examining the effectiveness of pioglitazone hydrochloride and metformin hydrochloride combination therapy in newly diagnosed T2DM patients with NAFLD symptoms.
Rifampicin
Rifampicin is primarily recognized as a potent antibiotic targeting Mycobacterium tuberculosis. Intriguingly, it also is a robust inducer of the liver’s cytochrome P450 system.78 Its connection to NAFLD is primarily underscored by its influence on bile acid metabolism and its potential therapeutic role in alleviating pruritus, a symptom often associated with liver diseases, including primary biliary cholangitis.79 While direct evidence advocating for rifampicin’s application in NAFLD remains scarce, its ability to regulate bile acid transport and synthesis might indirectly affect the disease’s progression. However, the use of rifampicin for NAFLD must be judiciously considered due to its potent antibiotic nature and the possible hepatotoxic repercussions, particularly with extended usage.80 One trial incorporated rifampicin to discern the effects of PXR activation on hepatic fat content by comparing rifampicin with a placebo in volunteers.
Salsalate
Salsalate, a derivative of salicylate that does not contain acetyl groups, is primarily known for its anti-inflammatory properties.81 Recently, it has attracted attention for its potential use in treating metabolic disorders, especially due to its ability to reduce inflammation, a key aspect in conditions like T2DM and NAFLD.82,83 NAFLD is characterized by chronic, low-level inflammation, and targeting this aspect of the disease could offer significant therapeutic benefits. Studies have shown that salsalate can improve insulin sensitivity and glucose control in people with T2DM. Its effects on NAFLD are believed to stem from its ability to inhibit the nuclear factor-kappa B pathways, leading to a decrease in the release of proinflammatory cytokines from the liver.84 In one trial, salsalate was included in a treatment plan for patients with osteoarthritis who also had NAFLD, to observe changes in NAFLD indicators following its administration.
Sitagliptin
Sitagliptin, a type of DPP-4 inhibitor, plays a crucial role in treating T2DM.85 Its primary mechanism involves prolonging the action of incretin hormones, which leads to increased insulin production and decreased glucagon release, thereby achieving a balanced metabolic effect.86 Recently, the use of DPP-4 inhibitors like sitagliptin has shown promise in treating NAFLD, especially in patients with both T2DM and NAFLD. Studies indicate that sitagliptin can significantly improve liver function and reduce liver fat, as evidenced by advanced imaging methods such as magnetic resonance spectroscopy.87 The drug works by reducing cell death in liver cells, decreasing fat production in the liver, and managing oxidative stress and related inflammation.88 In one clinical trial, researchers explored the effectiveness of combining sitagliptin with insulin glargine for treating NAFLD in T2DM patients, comparing it to the combination of liraglutide and metformin.
Tofogliflozin
Tofogliflozin, a key SGLT2 inhibitor, is mainly used to treat T2DM.89 It works by blocking SGLT2 in the kidney’s proximal tubules. This action significantly lowers glucose reabsorption in the kidneys, leading to increased glucose excretion in urine and improved blood sugar control.90 Recent studies also highlight the potential benefits of SGLT2 inhibitors for treating NAFLD.23 These benefits are thought to arise from reduced visceral fat, lower hepatic glucose production, increased fat oxidation, and decreased fat synthesis in the liver.91–93 Specific research on tofogliflozin has shown its ability to reduce liver fat and improve indicators of liver damage in patients with both NAFLD and T2DM.94 One trial compared tofogliflozin with glimepiride, focusing on their effects on liver histology and metabolic markers in NAFLD patients with T2DM over a 48-week period.
Ursodeoxycholic Acid (UDCA)
Ursodeoxycholic acid (UDCA) is a naturally occurring bile acid that is traditionally used to treat primary biliary cholangitis.94 Due to its cytoprotective, immunomodulatory, and anti-apoptotic properties, there is growing interest in exploring its use in treating other liver diseases, such NAFLD.95,96 Preliminary studies have posited that UDCA may improve liver function and reduce liver cell damage in NAFLD by stabilizing cell membranes, reducing harmful bile acids, and protecting against oxidative stress.97 One trial incorporated UDCA to understand the hepatic role in the onset of T2DM and its interrelation with NAFLD pathogenesis.
Vitamin E
Vitamin E, recognized for its robust fat-soluble antioxidant qualities, is of interest to researchers due to its possible role in addressing NAFLD and its more advanced form, NASH.98 The antioxidant effects of Vitamin E show promise in potentially decelerating or reversing the progression of these conditions. However, it is’ important to approach its use with caution. Certain studies have highlighted possible adverse effects associated with prolonged consumption, such as an increased risk of overall mortality, hemorrhagic stroke, and a greater likelihood of prostate cancer in men, particularly when used in therapeutic doses.98,99 One trial studied the impact of a tocotrienol-rich fraction of vitamin E on liver enzymes and DNA damage in overweight children with NAFLD over a span of 6 months.
Vitamin D
Vitamin D impacts cellular growth, immune function, and inflammation reduction, suggesting its involvement in the development and progression of NAFLD.100–102 Epidemiological data reveal an inverse correlation between vitamin D levels and NAFLD prevalence, with deficiencies more prevalent in NAFLD patients.103,104 This vitamin has shown the potential to inhibit NAFLD progression through anti-inflammatory antifibrotic effects and to improve insulin sensitivity.105 Rodent studies further support these findings, indicating that vitamin D supplementation reduces liver steatosis and inflammation.106–108 Two trials explored Vitamin D’s influence on NAFLD and its related metabolic parameters in T2DM patients.
Discussion
An exploration of the therapeutic potential of various agents in managing NAFLD indicates the multifaceted nature of the disease and its intricate interconnections with other metabolic disorders, especially T2DM. This complexity is aptly mirrored in the multitude of therapeutic agents being considered.
Thiazolidinediones like Lobeglitazone and Pioglitazone have traditionally been harnessed for their insulin-sensitizing capacities.61,73 Their potential utility in NAFLD hinges on enhancing insulin sensitivity in peripheral tissues, consequently diminishing liver fat accumulation and ameliorating histological indicators of the disease.62,75 Nevertheless, caution is imperative with pioglitazone, given the associated risks of bone fractures, weight gain, and potential long-term safety concerns.76
Metformin is a cornerstone for T2DM management in the same metabolic milieu, and its implications for NAFLD management cannot be sidelined.65 However, its efficacy is contested, with some studies highlighting its potential advantages in liver aminotransferase reduction and hepatic steatosis mitigation, and others debating its superiority over lifestyle modifications.67
A noteworthy entry into this therapeutic spectrum is the Omega-3 acid ethyl esters or OMACOR. These derivatives, notably eicosapentaenoic acid and docosahexaenoic acid, bring cardioprotective capabilities.69 Their burgeoning role in NAFLD is rooted in their anti-inflammatory, lipid-regulating, and antioxidative attributes, elucidating their potential as a therapeutic adjunct.7,70
Agents like Pentoxifylline and Salsalate, despite their primary roles in managing peripheral artery disease and inflammation, respectively, have demonstrated potential benefits in NAFLD due to their anti-inflammatory properties. Their therapeutic impact, especially that of pentoxifylline, can be attributed to their potential to suppress vital inflammatory cytokines, such as TNF-α, which are pivotal in NAFLD progression.71,83
While rifampicin’s primary role as a potent antibiotic is widely acknowledged, its implications for NAFLD hinge on its influence on bile acid metabolism and potential therapeutic role in alleviating pruritus, a symptom often associated with liver diseases.78 However, it must be prescribed with caution due to possible hepatotoxic repercussions.79
DPP-4 inhibitors like Sitagliptin and SGLT2 inhibitors such as Tofogliflozin showcase the intertwined pathophysiology of NAFLD and T2DM, underscoring the potential benefits these antidiabetic agents might confer on hepatic steatosis and inflammation.84,88
Moreover, traditional agents like UDCA and vitamins like Vitamin E and Vitamin D underscore the multifactorial therapeutic approach to NAFLD. While UDCA’s hepatoprotective and anti-apoptotic properties offer therapeutic possibilities, Vitamin E’s antioxidant prowess suggests potential therapeutic benefits. Still, the latter must be approached cautiously, given the potential risks associated with high doses.96,97 Vitamin D, on the other hand, bridges the realm of bone health with cellular growth, immune function, and inflammation, suggesting an intricate role in NAFLD’s development and progression.101
Future Directions
As NAFLD research and therapy advance, it is’ evident that a multifaceted approach is crucial. Personalized treatments rooted in genomic and metabolic profiling appear to be the way forward, while long-term studies remain vital to establish the safety and efficacy of new agents. Understanding NAFLD’s molecular foundations can lead to novel therapeutic targets, potentially offering more effective treatments. Given the disease’s multifactorial nature, there is’ potential for combining various therapeutic agents and merging them with lifestyle modifications.
Conclusion
Since NAFLD has become a major health concern, more clinical trials and different pharmacological approaches are required to counteract the potential side effects associated with the disease. Agents like Thiazolidinediones, Metformin, Omega-3 acid ethyl esters, and DPP-4 inhibitors, among others, highlight the diverse approaches toward NAFLD management. At the same time, each agent presents potential therapeutic benefits but has associated risks and limitations. Further investigations are definitely warranted.
Data Sharing Statement
All data are contained within the article.
Disclosure
The authors declare no conflicts of interest.
References
1. Maurice J, Manousou P. Non-alcoholic fatty liver disease. Clin Med. 2018;18(3):245–250. doi:10.7861/clinmedicine.18-3-245
2. Shahwan M, Jairoun AA, Alaila RFF, et al. Relation of erythrocyte sedimentation rate, glycemic parameters and lipid profile for the prediction of major adverse cardiovascular events: a single-center, cross-sectional study in Palestine. Obes Med. 2023;43:100513. doi:10.1016/j.obmed.2023.100513
3. Marchisello S, Di Pino A, Scicali R, et al. Pathophysiological, molecular and therapeutic issues of nonalcoholic fatty liver disease: an overview. Int J Mol Sci. 2019;20(8):1948. doi:10.3390/ijms20081948
4. Role of insulin resistance in nonalcoholic fatty liver disease | The Journal of Clinical Endocrinology & Metabolism | Oxford Academic. Available from: https://academic.oup.com/jcem/article/91/12/4753/2656230.
5. Hegazi OE, Alalalmeh SO, Alnuaimi GRH, et al. NAFLD and nutraceuticals: a review of completed Phase III and IV clinical trials. Front Med. 2023;1:10.
6. Attia SL, Softic S, Mouzaki M. Evolving Role for Pharmacotherapy in NAFLD/NASH. Clin Transl Sci. 2021;14(1):11. doi:10.1111/CTS.12839
7. Pouwels S, Sakran N, Graham Y, et al. Non-alcoholic fatty liver disease (NAFLD): a review of pathophysiology, clinical management and effects of weight loss. BMC Endocr Disord. 2022;22(1):63. doi:10.1186/s12902-022-00980-1
8. Mantovani A, Dalbeni A. Treatments for NAFLD: state of Art. Int J Mol Sci. 2021;22(5):2350. doi:10.3390/ijms22052350
9. Mascaró CM, Bouzas C, Tur JA. Association between Non-Alcoholic Fatty Liver Disease and mediterranean lifestyle: a systematic Review. Nutrients. 2022;15(1):14. doi:10.3390/NU14010049
10. The impact of intermittent fasting on non-alcoholic fatty liver disease in older adults: a review of clinicaltrials.gov registry: diabetes, metabolic syndrome and obesity. Available from: https://www.tandfonline.com/doi/abs/10.2147/DMSO.S430740.
11. Alalalmeh SO, Hegazi OE, Shahwan M, et al. Amphetamines in child medicine: a review of ClinicalTrials.gov. Front Pharmacol. 2023:14. doi:10.3389/fphar.2023.1280562
12. Struthers A, Shearer F. Allopurinol: novel indications in cardiovascular disease. Heart Br Card Soc. 2012;98:1543–1545. doi:10.1136/heartjnl-2012-302249
13. Goicoechea M, de Vinuesa SG, Verdalles U, et al. Effect of allopurinol in chronic kidney disease progression and cardiovascular risk. Clin J Am Soc Nephrol CJASN. 2010;5:1388–1393. doi:10.2215/CJN.01580210
14. Kang S-M, Lim S, Song H, et al. Allopurinol modulates reactive oxygen species generation and Ca2+ overload in ischemia-reperfused heart and hypoxia-reoxygenated cardiomyocytes. Eur J Pharmacol. 2006;535:212–219. doi:10.1016/j.ejphar.2006.01.013
15. Lanaspa MA, Sanchez-Lozada LG, Choi Y-J, et al. Uric acid induces hepatic steatosis by generation of mitochondrial oxidative stress. J Biol Chem. 2012;287:40732–40744. doi:10.1074/jbc.M112.399899
16. Petta S, Cammà C, Cabibi D, Di Marco V, Craxì A. Hyperuricemia is associated with histological liver damage in patients with non-alcoholic fatty liver disease. Aliment Pharmacol Ther. 2011;34:757–766. doi:10.1111/j.1365-2036.2011.04788.x
17. Yang C, Yang S, Xu W, Zhang J, Fu W, Feng C. Association between the hyperuricemia and nonalcoholic fatty liver disease risk in a Chinese population: a retrospective cohort study. PLoS One. 2017;
18. Liu Z, Wang Q, Huang H, Wang X, Xu C. Association between serum uric acid levels and long-term mortality of metabolic dysfunction-associated fatty liver disease: a nationwide cohort study. Diabetol Metab Syndr. 2023;15:27. doi:10.1186/s13098-023-00997-z
19. Toledo-Ibelles P, Gutiérrez-Vidal R, Calixto-Tlacomulco S, Delgado-Coello B, Mas-Oliva J. Hepatic accumulation of hypoxanthine: a link between hyperuricemia and nonalcoholic fatty liver disease. Arch Med Res. 2021;52:692–702. doi:10.1016/j.arcmed.2021.04.005
20. Ndibalema AR, Kabuye D, Wen S, Li L, Li X, Fan Q. Empagliflozin protects against proximal renal tubular cell injury induced by high glucose via regulation of hypoxia-inducible factor 1-alpha. Diabetes Metab Syndr Obes Targets Ther. 2020;13:1953–1967. doi:10.2147/DMSO.S243170
21. Fitchett D, Zinman B, Wanner C, et al. Heart failure outcomes with empagliflozin in patients with type 2 diabetes at high cardiovascular risk: results of the EMPA-REG OUTCOME® trial. Eur Heart J. 2016;37:1526–1534. doi:10.1093/eurheartj/ehv728
22. Zarghamravanbakhsh P, Frenkel M, Poretsky L. Metabolic causes and consequences of nonalcoholic fatty liver disease (NAFLD). Metab Open. 2021;12:100149. doi:10.1016/j.metop.2021.100149
23. Androutsakos T, Nasiri-Ansari N, Bakasis A-D, et al. SGLT-2 Inhibitors in NAFLD: expanding their role beyond diabetes and cardioprotection. Int J Mol Sci. 2022;23:3107. doi:10.3390/ijms23063107
24. Wei Q, Xu X, Guo L, Li J, Li L. Effect of SGLT2 Inhibitors on Type 2 diabetes mellitus with non-alcoholic fatty liver disease: a meta-analysis of randomized controlled trials. Front Endocrinol. 2021;12:635556. doi:10.3389/fendo.2021.635556
25. Scheen AJ. Effect of sodium-glucose cotransporter type 2 inhibitors on liver fat in patients with type 2 diabetes: hepatic beyond cardiovascular and renal protection? Ann Transl Med. 2018;6:S68–S68. doi:10.21037/atm.2018.10.39
26. Hussein NA, Abdel Gawad HS, Maklad HM, EL-Fakharany EM, Aly RG, Samy DM. Empagliflozin inhibits autophagy and mitigates airway inflammation and remodelling in mice with ovalbumin-induced allergic asthma. Eur J Pharmacol. 2023;950:175701. doi:10.1016/j.ejphar.2023.175701
27. Bajaj S, Aiwale A, Trailokya A, Sharma A. Clinical evidence of evogliptin plus metformin in management of type 2 diabetes mellitus. J Assoc Physicians India. 2021;69:25–29.
28. Sharma A, Virmani T, Sharma A, et al. Potential effect of DPP-4 inhibitors towards hepatic diseases and associated glucose intolerance. Diabetes Metab Syndr Obes Targets Ther. 2022;15:1845–1864. doi:10.2147/DMSO.S369712
29. Wang Z, Park H, Bae EJ. Efficacy of evogliptin and cenicriviroc against nonalcoholic steatohepatitis in mice: a comparative study. Korean J Physiol Pharmacol off J Korean Physiol Soc Korean Soc Pharmacol. 2019;23:459–466. doi:10.4196/kjpp.2019.23.6.459
30. Nakatani Y, Maeda M, Matsumura M, et al. Effect of GLP-1 receptor agonist on gastrointestinal tract motility and residue rates as evaluated by capsule endoscopy. Diabetes Metab. 2017;43:430–437. doi:10.1016/j.diabet.2017.05.009
31. Meloni AR, DeYoung MB, Lowe C, Parkes DG. GLP-1 receptor activated insulin secretion from pancreatic β-cells: mechanism and glucose dependence. Diabetes Obes Metab. 2013;15:15–27. doi:10.1111/j.1463-1326.2012.01663.x
32. Sofogianni A, Filippidis A, Chrysavgis L, Tziomalos K, Cholongitas E. Glucagon-like peptide-1 receptor agonists in non-alcoholic fatty liver disease: an update. World J Hepatol. 2020;12:493–505. doi:10.4254/wjh.v12.i8.493
33. Nevola R, Epifani R, Imbriani S, et al. GLP-1 receptor agonists in non-alcoholic fatty liver disease: current evidence and future perspectives. Int J Mol Sci. 2023;24:1703. doi:10.3390/ijms24021703
34. Schumacher HR. Febuxostat: a non-purine, selective inhibitor of xanthine oxidase for the management of hyperuricaemia in patients with gout. Expert Opin Investig Drugs. 2005;14:893–903. doi:10.1517/13543784.14.7.893
35. Kakimoto M, Fujii M, Sato I, et al. Antioxidant action of xanthine oxidase inhibitor febuxostat protects the liver and blood vasculature in SHRSP5/Dmcr rats. J Appl Biomed. 2023;21:80–90. doi:10.32725/jab.2023.009
36. Campbell DB, Lavielle R, Nathan C. The mode of action and clinical pharmacology of gliclazide: a review. Diabet Res Clin Pract. 1991;14(Suppl 2):S21–36. doi:10.1016/0168-8227(91)90005-x
37. van Haeften TW, Veneman TF, Gerich JE, van der Veen EA. Influence of gliclazide on glucose-stimulated insulin release in man. Metabolism. 1991;40:751–755. doi:10.1016/0026-0495(91)90096-F
38. Ren J, Wang X, Yee C, Gorrell MD, McLennan SV, Twigg SM. Sitagliptin is more effective than gliclazide in preventing pro-fibrotic and pro-inflammatory changes in a rodent model of diet-induced non-alcoholic fatty liver disease. Molecules. 2022;27:727. doi:10.3390/molecules27030727
39. Ma A, Kamp M, Bird D, Howlett V, Cameron DP. The effects of long term gliclazide administration on insulin secretion and insulin sensitivity. Aust N Z J Med. 1989;19:44–50. doi:10.1111/j.1445-5994.1989.tb01674.x
40. Sena CM, Louro T, Matafome P, Nunes E, Monteiro P, Seiça R. Antioxidant and vascular effects of gliclazide in type 2 diabetic rats fed high-fat diet. Physiol Res. 2009;58:203–209. doi:10.33549/physiolres.931480
41. de Araújo AA, de Morais HB, de Medeiros CACX, et al. Gliclazide reduced oxidative stress, inflammation, and bone loss in an experimental periodontal disease model. J Appl Oral Sci. 2019;27:e20180211. doi:10.1590/1678-7757-2018-0211
42. Proks P, Reimann F, Green N, Gribble F, Ashcroft F. Sulfonylurea stimulation of insulin secretion. Diabetes. 2002;51(Suppl 3):S368–376. doi:10.2337/diabetes.51.2007.s368
43. Hepatoprotective activity of glimepiride by inducing Ccl4 hepatotoxicity. PharmaTutor. Available from: https://www.pharmatutor.org/articles/hepatoprotective-activity-of-glimepiride-by-inducing-ccl4-hepatotoxicity.
44. Kabadi MU, Kabadi UM. Effects of glimepiride on insulin secretion and sensitivity in patients with recently diagnosed type 2 diabetes mellitus. Clin Ther. 2004;26:63–69. doi:10.1016/s0149-2918(04)90006-9
45. Talamantes S, Lisjak M, Gilglioni EH, Llamoza-Torres CJ, Ramos-Molina B, Gurzov EN. Non-alcoholic fatty liver disease and diabetes mellitus as growing aetiologies of hepatocellular carcinoma. JHEP Rep. 2023;5:100811. doi:10.1016/j.jhepr.2023.100811
46. Zhang AMY, Wellberg EA, Kopp JL, Johnson JD. Hyperinsulinemia in obesity, inflammation, and cancer. Diabetes Metab J. 2021;45:285–311. doi:10.4093/dmj.2020.0250
47. Paschos P, Paletas K. Non alcoholic fatty liver disease and metabolic syndrome. Hippokratia. 2009;13:9–19.
48. Richard J, Lingvay I. Hepatic steatosis and Type 2 diabetes: current and future treatment considerations. Expert Rev Cardiovasc Ther. 2011;9:321–328. doi:10.1586/erc.11.15
49. Colosimo S, Tan GD, Petroni ML, Marchesini G, Tomlinson JW. Improved glycaemic control in patients with type 2 diabetes has a beneficial impact on NAFLD, independent of change in BMI or glucose lowering agent. Nutr Metab Cardiovasc Dis. 2023;33:640–648. doi:10.1016/j.numecd.2022.12.010
50. Guo W, Tian W, Lin L, Xu X. Liraglutide or insulin glargine treatments improves hepatic fat in obese patients with type 2 diabetes and nonalcoholic fatty liver disease in twenty-six weeks: a randomized placebo-controlled trial. Diabet Res Clin Pract. 2020;170:108487. doi:10.1016/j.diabres.2020.108487
51. Morishita A, Tadokoro T, Fujihara S, et al. Ipragliflozin attenuates non-alcoholic steatohepatitis development in an animal model. PLoS One. 2022;17:e0261310. doi:10.1371/journal.pone.0261310
52. Suga T, Sato K, Ohyama T, et al. Ipragliflozin-induced improvement of liver steatosis in obese mice may involve sirtuin signaling. World J Hepatol. 2020;12:350–362. doi:10.4254/wjh.v12.i7.350
53. Seko Y, Sumida Y, Tanaka S, et al. Effect of sodium glucose cotransporter 2 inhibitor on liver function tests in Japanese patients with non-alcoholic fatty liver disease and type 2 diabetes mellitus. Hepatol Res off J Jpn Soc Hepatol. 2017;47:1072–1078. doi:10.1111/hepr.12834
54. Yanai H, Hakoshima M, Katsuyama H. The possible mechanisms for improvement of liver function due to sodium-glucose cotransporter-2 inhibitors. J Clin Med Res. 2019;11:769–772. doi:10.14740/jocmr4019
55. Komiya C, Tsuchiya K, Shiba K, et al. Ipragliflozin improves hepatic steatosis in obese mice and liver dysfunction in type 2 diabetic patients irrespective of body weight reduction. PLoS One. 2016;11:e0151511. doi:10.1371/journal.pone.0151511
56. Dufour J-F, Caussy C, Loomba R. Combination therapy for non-alcoholic steatohepatitis: rationale, opportunities and challenges. Gut. 2020;69:1877–1884. doi:10.1136/gutjnl-2019-319104
57. Yang F, Luo X, Li J, et al. Application of glucagon-like peptide-1 receptor antagonists in fibrotic diseases. Biomed Pharmacother. 2022;152:113236. doi:10.1016/j.biopha.2022.113236
58. Bendotti G, Montefusco L, Lunati ME, et al. The anti-inflammatory and immunological properties of GLP-1 Receptor Agonists. Pharmacol Res. 2022;182:106320. doi:10.1016/j.phrs.2022.106320
59. Fang Y, Ji L, Zhu C, et al. Liraglutide Alleviates Hepatic Steatosis by Activating the TFEB-Regulated Autophagy-Lysosomal Pathway. Front Cell Dev Biol. 2020;8:602574. doi:10.3389/fcell.2020.602574
60. Tølbøl KS, Kristiansen MN, Hansen HH, et al. Metabolic and hepatic effects of liraglutide, obeticholic acid and elafibranor in diet-induced obese mouse models of biopsy-confirmed nonalcoholic steatohepatitis. World J Gastroenterol. 2018;24:179–194. doi:10.3748/wjg.v24.i2.179
61. Alorfi NM, Alshehri FS. Usage of glucagon-like peptide-1 for obesity in children Updated Review of Clinicaltrials Gov. J Multidiscip Healthc. 2023;16:2179–2187. doi:10.2147/JMDH.S419245
62. Blackman SM, Cooke DW. Diabetes. In: Lennarz WJ, Lane MD editors, Encycl Biol Chem.
63. Bailey CJ. Thiazolidinediones. In: InxPharm: The Comprehensive Pharmacology Reference. Elsevier; 2015. doi10.1016/B978-0-12-801238-3.10867-0
64. Shinzato T, Ohya Y, Nakamoto M, Ishida A, Takishita S. Beneficial effects of pioglitazone on left ventricular hypertrophy in genetically hypertensive rats. Hypertens Res. 2007;30:863–873. doi:10.1291/hypres.30.863
65. Chang E, Park C, Park SW. Role of thiazolidinediones, insulin sensitizers, in non‐alcoholic fatty liver disease. J Diabetes Investig. 2013;4:517–524. doi:10.1111/jdi.12107
66. Nasri H, Rafieian-Kopaei M. Metformin: current knowledge. J Res Med Sci Off J Isfahan Univ Med Sci. 2014;19:658–664.
67. Bhatt HB, Smith RJ. Fatty liver disease in diabetes mellitus. Hepatobiliary Surg Nutr. 2015;4:10108. doi:10.3978/j.issn.2304-3881.2015.01.03
68. Huang K-H, Lee C-H, Cheng Y-D, et al. Correlation between long-term use of metformin and incidence of NAFLD among patients with type 2 diabetes mellitus: a real-world cohort study. Front Endocrinol. 2022;2:13.
69. Innes JK, Calder PC. Marine Omega-3 (N-3) Fatty Acids for Cardiovascular Health: an Update for 2020. Int J Mol Sci. 2020;21:1362. doi:10.3390/ijms21041362
70. Oscarsson J, Hurt-Camejo E. Omega-3 fatty acids eicosapentaenoic acid and docosahexaenoic acid and their mechanisms of action on apolipoprotein B-containing lipoproteins in humans: a review. Lipids Health Dis. 2017;16:149. doi:10.1186/s12944-017-0541-3
71. Oscarsson J, Önnerhag K, Risérus U, et al. Effects of free omega-3 carboxylic acids and fenofibrate on liver fat content in patients with hypertriglyceridemia and non-alcoholic fatty liver disease: a double-blind, randomized, placebo-controlled study. J Clin Lipidol. 2018;12:1390–1403.e4. doi:10.1016/J.JACL.2018.08.003
72. Pentoxifylline - StatPearls - NCBI Bookshelf. Available from: https://www.ncbi.nlm.nih.gov/books/NBK559096/.
73. Du J, Ma -Y-Y, Yu C-H, Li Y-M. Effects of pentoxifylline on nonalcoholic fatty liver disease: a meta-analysis. WJG. 2014;20:569–577. doi:10.3748/wjg.v20.i2.569
74. Chiarelli F, Marzio DD. Peroxisome proliferator-activated receptor-γ agonists and diabetes: current evidence and future perspectives. Vasc Health Risk Manag. 2008;4:297–304.
75. Al-Muzafar HM, Alshehri FS, Amin KA. The role of pioglitazone in antioxidant, anti-inflammatory, and insulin sensitivity in a high fat-carbohydrate diet-induced rat model of insulin resistance. Braz J Med Biol Res. 2021;54:e10782. doi:10.1590/1414-431X2020e10782
76. Wang Z, Du H, Zhao Y, et al. Response to pioglitazone in non-alcoholic fatty liver disease patients with vs. without type 2 diabetes: a meta-analysis of randomized controlled trials. Front Endocrinol. 2023;14:1111430. doi:10.3389/fendo.2023.1111430
77. Spence JD, Viscoli CM, Inzucchi SE, et al. Pioglitazone therapy in patients with stroke and prediabetes. JAMA Neurol. 2019;76:526–535. doi:10.1001/jamaneurol.2019.0079
78. Chen J, Raymond K. Roles of rifampicin in drug-drug interactions: underlying molecular mechanisms involving the nuclear pregnane X receptor. Ann Clin Microbiol Antimicrob. 2006;5:3. doi:10.1186/1476-0711-5-3
79. Gregorio GV, Ball CS, Mowat AP, Mieli-Vergani G. Effect of rifampicin in the treatment of pruritus in hepatic cholestasis. Arch Dis Child. 1993;69:141–143.
80. Huang J-H, Zhang C, Zhang D-G, Li L, Chen X, Xu D-X. Rifampicin-induced hepatic lipid accumulation: association with Up-regulation of peroxisome proliferator-activated receptor γ in mouse liver. PLoS One. 2016;11:e0165787. doi:10.1371/journal.pone.0165787
81. Aronson JK, editor. Salsalate. In: Meylers Side Eff. Drugs Sixt. Oxford: Elsevier; 2016:302–303. doi:10.1016/B978-0-444-53717-1.01431-1
82. Henao-Mejia J, Elinav E, Jin C, et al. Inflammasome-mediated dysbiosis regulates progression of NAFLD and obesity. Nature. 2012;482:179–185. doi:10.1038/nature10809
83. Li J, Chen C, Zhang W, Bi J, Yang G, Li E. Salsalate reverses metabolic disorders in a mouse model of non-alcoholic fatty liver disease through AMPK activation and caspase-6 activity inhibition. Basic Clin Pharmacol Toxicol. 2021;128:394–409. doi:10.1111/bcpt.13535
84. Hüttl M, Markova I, Miklánková D, et al. Hypolipidemic and insulin sensitizing effects of salsalate beyond suppressing inflammation in a prediabetic rat model. Front Pharmacol. 2023;2:14.
85. Pathak R, Bridgeman MB. Dipeptidyl Peptidase-4 (DPP-4) Inhibitors In the Management of Diabetes. Pharm Ther. 2010;35:509–513.
86. Kim JH. Effects of Sitagliptin on insulin and glucagon levels in type 2 diabetes mellitus. Diabetes Metab J. 2015;39:304–306. doi:10.4093/dmj.2015.39.4.304
87. Kongmalai T, Srinonprasert V, Anothaisintawee T, et al. New anti-diabetic agents for the treatment of non-alcoholic fatty liver disease: a systematic review and network meta-analysis of randomized controlled trials. Front Endocrinol. 2023;14:1182037. doi:10.3389/fendo.2023.1182037
88. Cao Q, Xu D, Chen Y, et al. Sitagliptin reduces endothelial dysfunction and apoptosis induced by high-fat diet and palmitate in thoracic aortas and endothelial cells via ROS-ER stress-CHOP pathway. Front Pharmacol. 2021;12:670389. doi:10.3389/fphar.2021.670389
89. Katakami N, Mita T, Yoshii H, et al. Effect of tofogliflozin on arterial stiffness in patients with type 2 diabetes: prespecified sub-analysis of the prospective, randomized, open-label, parallel-group comparative UTOPIA trial. Cardiovasc Diabetol. 2021;20:4. doi:10.1186/s12933-020-01206-1
90. Novikov A, Vallon V. SGLT2 inhibition in the diabetic kidney – an update. Curr Opin Nephrol Hypertens. 2016;25:50–58. doi:10.1097/MNH.0000000000000187
91. Qureshi K, Abrams GA. Metabolic liver disease of obesity and role of adipose tissue in the pathogenesis of nonalcoholic fatty liver disease. WJG. 2007;13:3540–3553. doi:10.3748/wjg.v13.i26.3540
92. van der Kooy K, Leenen R, Seidell JC, Deurenberg P, Visser M. Abdominal diameters as indicators of visceral fat: comparison between magnetic resonance imaging and anthropometry. Br J Nutr. 1993;70:47–58. doi:10.1079/bjn19930104
93. Zhang E, Zhao Y, Hu H. Impact of sodium glucose cotransporter 2 inhibitors on nonalcoholic fatty liver disease complicated by diabetes mellitus. Hepatol Commun. 2021;5:736–748. doi:10.1002/hep4.1611
94. Bica I-C, Stoica RA, Salmen T, et al. The effects of sodium-glucose cotransporter 2-inhibitors on steatosis and fibrosis in patients with non-alcoholic fatty liver disease or steatohepatitis and type 2 diabetes: a systematic review of randomized controlled trials. Medicina. 2023;59:1136. doi:10.3390/medicina59061136
95. Bodge M, Cumpston A. Chapter 2 - pharmacology of drugs used in hematopoietic cell transplantation. In: Bashir Q, Hamadani M, editors. Hematop Cell Transplant. Elsevier; 2019:19–35. doi:10.1016/B978-0-323-56802-9.00002-X
96. Ursodeoxycholic acid induces apoptosis in hepatocellular carcinoma xenografts in mice - PMC. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4579883/.
97. Nadinskaia M, Maevskaya M, Ivashkin V, et al. Ursodeoxycholic acid as a means of preventing atherosclerosis, steatosis and liver fibrosis in patients with nonalcoholic fatty liver disease. World J Gastroenterol. 2021;27:959–975. doi:10.3748/wjg.v27.i10.959
98. Hadi HE, Vettor R, Rossato M. Vitamin E as a treatment for nonalcoholic fatty liver disease: reality or myth? Antioxid. 2018;7:12. doi:10.3390/ANTIOX7010012
99. Arroyave-Ospina JC, Wu Z, Geng Y, Moshage H. Role of oxidative stress in the pathogenesis of non-alcoholic fatty liver disease: implications for prevention and therapy. Antioxid. 2021;10:174. doi:10.3390/ANTIOX10020174
100. Umar M, Sastry KS, Chouchane AI. Role of vitamin D beyond the skeletal function: a review of the molecular and clinical studies. Int J Mol Sci. 2018. doi:10.3390/ijms19061618
101. Aranow C. Vitamin D and the Immune System. J Investig Med off Publ Am Fed Clin Res. 2011;59:881–886.
102. Office of Dietary Supplements - Vitamin D. Available from: https://ods.od.nih.gov/factsheets/VitaminD-HealthProfessional/.
103. Wang X, Li W, Zhang Y, Yang Y, Qin G. Association between vitamin D and non-alcoholic fatty liver disease/non-alcoholic steatohepatitis: results from a meta-analysis. Int J Clin Exp Med. 2015;3:8.
104. Alimentary pharmacology & therapeutics. Pharmacology Journal. Wiley Online Library. Available from: https://onlinelibrary.wiley.com/doi/10.1111/apt.12377.
105. Aggeletopoulou I, Thomopoulos K, Mouzaki A, Triantos C. Vitamin D–VDR novel anti-inflammatory molecules—new insights into their effects on liver diseases. Int J Mol Sci. 2022;23:8465. doi:10.3390/ijms23158465
106. Lim H, Lee H, Lim Y. Effect of vitamin D3 supplementation on hepatic lipid dysregulation associated with autophagy regulatory AMPK/Akt-mTOR signaling in type 2 diabetic mice. Exp Biol Med. 2021;246:1139. doi:10.1177/1535370220987524
107. Barchetta I, Cimini FA, Cavallo MG. Vitamin D and Metabolic Dysfunction-Associated Fatty Liver Disease (MAFLD): an Update. Nutrients. 2020;12:1–14. doi:10.3390/NU12113302
108. Eliades M, Spyrou E. Vitamin D: a new player in non-alcoholic fatty liver disease? WJG. 2015;21:1718–1727. doi:10.3748/wjg.v21.i6.1718
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.