Back to Journals » Clinical Interventions in Aging » Volume 18
Exploring Population Characteristics and Recruitment Challenges in Older People Experiencing Falls at Home without Hospitalization or with an Emergency Department Visit: Insights from the RISING-DOM Experience
Authors Bouzid W ![]() , Tavassoli N, Berbon C, Qassemi S, Vaysset S, Poly M, Bounes V, Shourick J, Nourhashémi F
, Tavassoli N, Berbon C, Qassemi S, Vaysset S, Poly M, Bounes V, Shourick J, Nourhashémi F
Received 9 June 2023
Accepted for publication 5 September 2023
Published 1 December 2023 Volume 2023:18 Pages 1995—2008
DOI https://doi.org/10.2147/CIA.S421053
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Wafa Bouzid,1,2 Neda Tavassoli,1 Caroline Berbon,1 Soraya Qassemi,1 Sandrine Vaysset,1 Magali Poly,1 Vincent Bounes,3 Jason Shourick,4,5 Fati Nourhashémi1,5
1Geriatric Medicine Unit (Gérontopole), University of Toulouse Hospital Center, Toulouse, France; 2Regional Health Agency of Occitanie, Toulouse, 31000, France; 3Emergency Medicine Unit, University of Toulouse Hospital Center, Toulouse, France; 4Research Methodology Support Unit (USMR), Clinical Epidemiology and Public Health Department, University of Toulouse Hospital Center, Toulouse, France; 5CERPOP, UMR 1295, INSERM – University of Toulouse III, Toulouse, France
Correspondence: Wafa Bouzid, La Cité de la Santé - Équipe Régionale Vieillissement et Prévention de la Dépendance Hôpital La Grave, Place Lange, TSA 60033, Toulouse Cedex 9, 31059, France, Tel +33 5 61 77 83 79, Fax +33 5 61 77 64 75, Email [email protected]
Background: An increasing number of falls among community-living older adults are reported in emergency calls. Data on evidence of appropriate fall prevention interventions are limited and challenges in recruiting this population in randomized trials are acknowledged.
Purpose: The main aim of this study was to provide demographic data, circumstance and fall-related outcomes of the population in the RISING-DOM study [Impact d’une évaluation des facteurs de RISque de chute et d’une prise en charge personnalisée, sur la mortalité et l’institutionnalisation, après INtervention du SAMU chez la personne âGée à DOMicile], a multicenter, randomized interventional trial involving community-dwelling older adults who have experienced a fall at home and were not hospitalized. Additionally, the challenges of remote recruitment in this population were discussed.
Patients and Methods: Participants were identified through the Occitania Emergency Observatory database. Participant recruitment and data collection were performed through telephone interviews (October 2019-March 2022). Additionally, a sample survey of Emergency Medical Services calls was carried out.
Results: Out of the 1151 individuals screened, a total of 951 participants were included in the trial follow-up, resulting in an acceptance rate of 82.62%. The screening delay was extended due to the COVID-19 pandemic. Recruiting difficulties were mainly related to identifying potential participants, unavailable contact information and unreachability. Participants’ mean age was 84.1 years, 65.8% were women, and 44.3% lived alone. Pain was the most frequent outcome (53%). In the previous year, 73.5% of participants reported experiencing a fall, with 66.7% of those falls requiring assistance from Emergency Medical Services (EMS). Nearly, 40% did not take proactive steps to prevent future falls and walking aids (79.8%) were the most common preventive action.
Conclusion: Indicators of a high-risk group of falls have been identified underscoring the need for appropriate fall interventions in the target population. Challenges of large sampling for randomized fall prevention trials were provided.
Trial Registration: Clinicaltrials.gov identifier: NCT04132544. Registration date: 18/10/2019. https://www.clinicaltrials.gov/ct2/show/NCT04132544?term=rising-dom&draw=2&rank=1.
Keywords: fall prevention in community-living older adults, Emergency Medical Service, descriptive analysis, recruitment of older people for fall-related clinical trial
Introduction
Falls in older people are a major public health issue leading to death, functional decline and an increased need for institutionalization1 and cause substantial burden worldwide.2 Despite a considerable number of falls leading to Emergency Medical Services (EMS) calls for assistance, it is concerning that approximately half of older people involved in such incidents are not conveyed to the hospital or are swiftly discharged from Emergency Departments (ED) without a thorough assessment of the underlying factors contributing to the fall and the provision of appropriate fall referrals.3,4 This highlights the potential gaps in the current healthcare system’s response to fall-related incidents among older individuals. In addition, this group has been specifically identified as a vulnerable population that faces a high risk of future falls and mortality, as well as an increased likelihood of utilizing health services in an unplanned manner, such as through frequent health care contact, ED visits, and hospital admissions.3,5–9 Therefore, this population represents an interesting target for delivering appropriate fall prevention interventions.6,9,10 Even though, there is an emerging evidence that personalized multifactorial fall prevention programs are successful in decreasing fall rate,11–15 results in particular from randomized controlled trials are mixed12,16 and evidence of implementing appropriate fall prevention interventions in community-dwelling is limited.17 In addition, the recruitment of older people in fall prevention trials and strategies is a critical step and could result in limiting data on assessing their effectiveness.18–20
The RISING-DOM study has been conducted in Southwest France since 2019. It is a multicenter, randomized interventional trial that specifically targets the community-dwelling population that experienced a fall at home who were not hospitalized or hospitalized for less than 24 hours. The aim was to assess the effectiveness of an individualized multidimensional intervention introduced by geriatric nurses.21
At present, the inclusion phase has been completed, and the follow-up phase is currently in progress with a scheduled end date in April 2024. The main objective of the present work is to provide an initial overview of the demographic characteristics of the target population and the circumstances related to falls. Moreover, the challenges associated with remote recruitment in this particular population were discussed.
Materials and Methods
Study Population and Data Collection
The RISING-DOM study involved 12 investigator sites located in the Occitania region of Southwest France (population of 6,053,548 aged 41.8 years old on average and 30% aged over 60 years old).22 The sampling targeted individuals aged 70 and over, living at home and 45 minutes at most from an investigator center, who had fallen at home with EMS intervention, who were not hospitalized or hospitalized for less than 24 hours and who (or their close relatives or legal representative) are able to give telephone information. Due to the logistical constraints associated with the nurse intervention in the “intervention group” being conducted at the participant’s home, it was not possible to include older individuals who lived a considerable distance from the investigator site.
Data presented in this study include pre-randomization data collected through the screening process that was extended to 30 months (October 2019 to April 2022) due to the COVID-19 pandemic. The methodology employed was previously outlined in the study protocol.21 Briefly, when a fall happened, EMS personnel provided a study information sheet to the fallers and notified them of the possibility of being contacted for potential study inclusion. Participants were then identified by Associate Research Coordinators (CRA) from the Occitania Emergency Observatory (ORU-Occitania) database.
Once identified, the CRA contacted individuals to check their eligibility and collected a set of data including age, gender, time and location of the fall, the activity being performed at the time of the fall, person who gave the alert, the fall circumstances, severity and consequences (Figure 1).
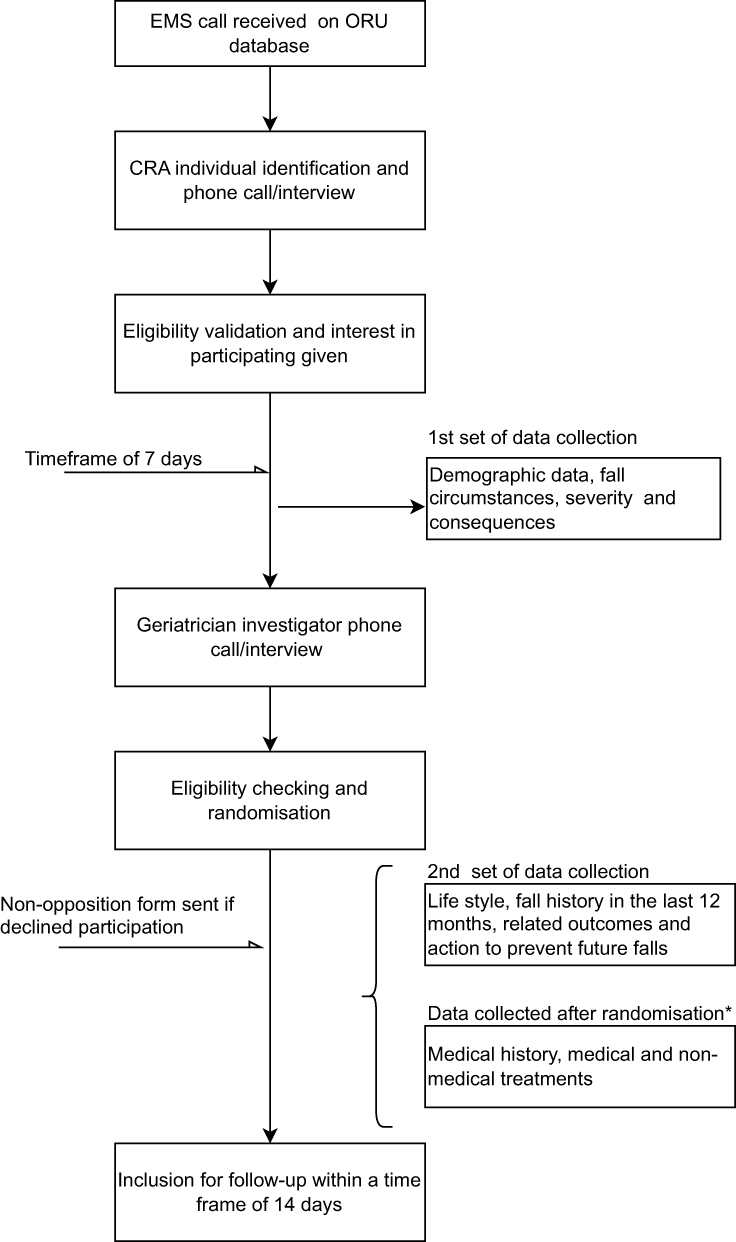 |
Figure 1 Flowchart for participant recruitment and data collection. Abbreviations: EMS, Emergency Medical Service; ORU database, Emergency Observatory database; CRA, Clinical Research Associate. Note: *Post-randomization data not available at this stage of the study and not included in the present analysis. |
Within 7 days, the geriatrician investigators contacted eligible individuals to obtain their oral consent and collect a second set of data including information on their lifestyle and data on fall history in the last 12 months (number and fall frequency, related outcomes such as injury, the ability to self-lift and the use of medical resources and actions taken to prevent future falls following a fall in the last 12 months). Furthermore, data regarding the refusal to participate, based on the individual providing it, has been collected. Additional data on participant medical history and medical and non-medical treatments were also collected after randomization. The participant follow-up started promptly upon completion of the inclusion process within a maximum timeframe of 14 days and for a minimum follow-up duration of 24 months. The maximum follow-up period will be 54 months for the first subjects included. This timeframe allows for the evaluation of the intervention’s effects over a sustained duration, providing valuable insights into its long-term efficacy and long-lasting effects.
As the clinical trial is currently ongoing, only pre-randomized data are available and were analyzed in this study. In order to get a more accurate representation of the study population and minimize selection bias, this analysis incorporated data from all older adults who underwent screening, irrespective of their inclusion or withdrawal from the RISING-DOM follow-up. Additionally, non-opposition forms were sent to screened individuals who declined to participate in the study, to inform them about the use of their data for descriptive purpose.
Furthermore, in order to identify potential barriers related to the identification of older people with falls from EMS dispatch records, we conducted a follow-up of the flow of these calls within the Haute Garonne department (229,567 inhabitants, a mean age of 38.5 years and 13.4% of the population is aged 60 years or older)22 over a discontinuous period of 3 months i.e January 2020, June 2020 and March 2021 where screening was continuously performed. This area was selected as it represents the most populous department in the Occitania region. During this follow-up, the collected data included information on the number of received calls, the number of calls meeting the inclusion/exclusion criteria, the number of discarded cases, and the reasons for their rejection, such as incomplete or unavailable contact details, technical issues with the older person’s phone usage, hearing problems, or cases that did not meet the inclusion criteria (patients residing in nursing homes, post-fall deaths, hospitalizations exceeding 24 hours, falls that occurred outside the home, patients living more than 45 minutes away from the investigator site, etc.). Later on, data regarding the number of refusals to participate, the number of individuals accepting to be contacted by the geriatrician investigator for potential participation, as well as the reasons for refusing to participate, were collected.
Statistical Analysis
Descriptive analysis was performed with categorical variables given as count and percentage and continuous variables as mean standard deviation and range. Additionally, for fall consequences and preventive measures already taken in the past year, we quantified intersections and presented them in an UpSet plot. To evaluate the presence of selection bias, we also compared randomized and non-randomized participants using the T-test or Wilcoxon test for continuous variables depending on the normality of the distribution and the Chi2 square test for categorical variables. A p value under 5% was considered significant. Due to the exploratory nature of comparison in this mainly descriptive study, we did not perform adjustment for the multiplicity of tests.
Results
Participant Recruitment
On an expected recruitment goal of 1190 participants, a total of 1151 people were screened and 952 included in the RISING-DOM follow-up, resulting in an acceptance rate of 82.62%. Out of the 1151 individuals screened, 527 consents were given by the individuals themselves, and 424 consents were given by the family or legal representative. There were no significant differences in participation decline (p = 0.107) whether it was given by the older adults (8.2%) or their family/legal representatives (11.1%).
The survey of EMS calls in the Haute Garonne department indicated a total of 5472 calls during the three investigated months, out of which 3673 were excluded due to unavailable contact information, protocol exclusion criteria and unreachability (Figure 2). The remaining 1799 individuals were contacted by the CRA. Out of those, 125 were found to be eligible, and ultimately, 96 individuals were enrolled in the trial’s follow-up. Furthermore, all of the individuals contacted by the CRA reported that they had not received any information about the study from the EMS staff, or they could not recall receiving such information.
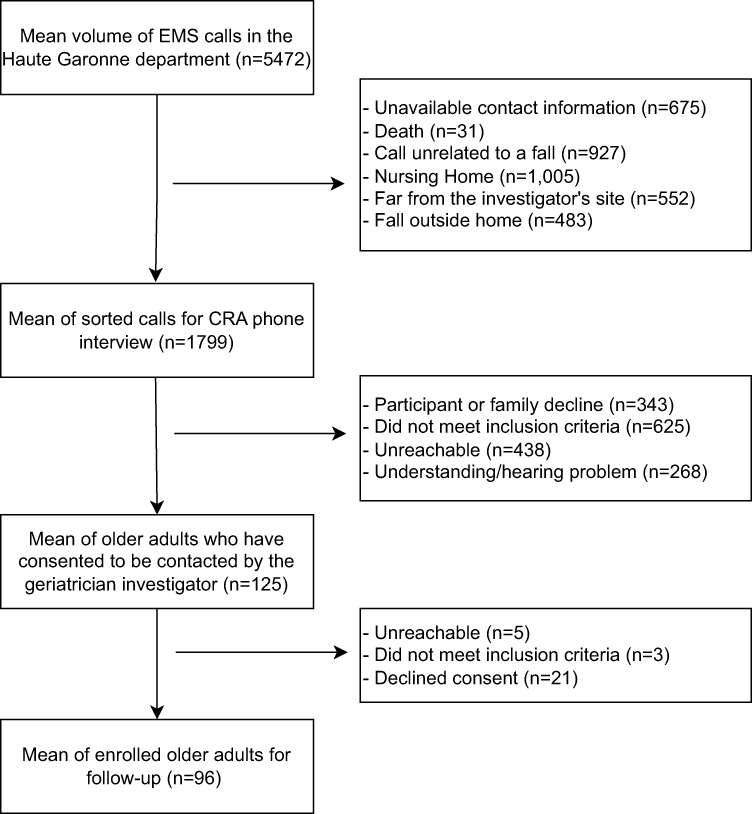 |
Figure 2 Screening flowchart of EMS mean calls recorded in the Haute Garonne department for three-month period (January 2020, June 2020, and March 2021). Abbreviations: EMS, Emergency Medical Service; CRA, Clinical Research Associate. |
Population Characteristics and Fall Circumstances
Participant demographic characteristics are given in Table 1. The mean age of the population was 84.1 (sd 6.9) with 48.9% (N = 563) were aged between 80 and 89 years old. The majority of the participants were women (65.8%, N = 757). Approximately 55.7% (N = 574) lived with a partner or family while 44.3% (N = 456) lived alone.
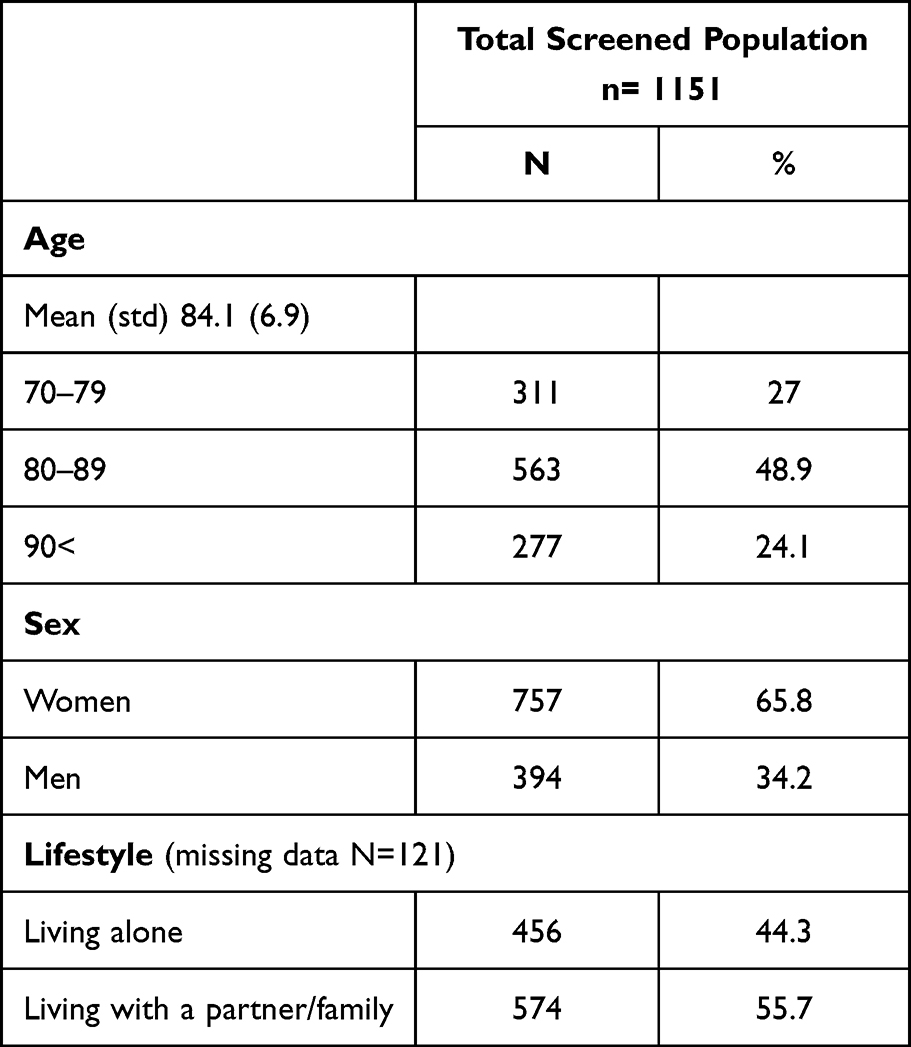 |
Table 1 Demographic Characteristics of the 1151 Screened Older People Who Experienced a Fall at Home with No Hospitalization or with Hospitalization Less Than 24 Hours |
Fall characteristics, including the time, location, activity being performed and circumstances, are presented in Table 2. Walking was the most frequently reported activity prior to or during the fall (41.2%), followed by positional changes such as transfers, getting up, sitting down and bending over (35.3%). The majority of falls occurred in the bedroom (28.8%), followed by the living room (20.4%) and the immediate surroundings of the home (14.5%). Fall-related injuries are distributed as follows: 39.3% resulted in no physical-reported injury, 38.1% were minor injuries (hematoma, wound without stitching) and 22.6% were moderate injuries (including injuries with deep wounds requiring stitches and fracture). The main reported fall consequence was pain (53%), followed by no fall consequence (31.5%), activity restriction (26.7%) and fear of falling (23.7%).
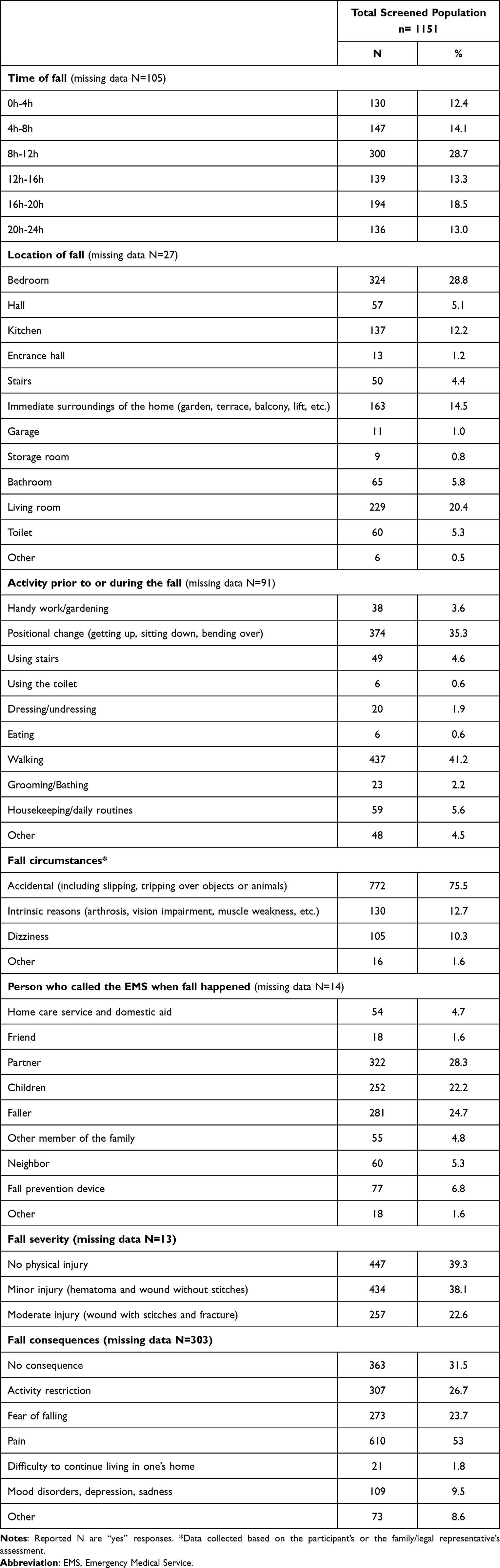 |
Table 2 Fall Characteristics of the 1151 Screened Older People Who Experienced a Fall at Home with No Hospitalization or with Hospitalization Less Than 24 Hours |
Previous Fall History, Frequency and Induced Outcomes
A total of 73.5% (N = 709) of the screened participants reported at least one fall in the year prior screening (Table 3). Among them 18.1% and 18.4% recount 2 and 3 falls, respectively and at the extreme end 3.1% of individuals described more than 20 falls. Of those who fell, 57.7% sustained an injury as a result of a fall with 66.7% of falls resulting in EMS assistance, 61.1% in ED visits, 51.3% in referring doctor visits and 11.4% in hospitalization. After falling, approximately 17.5% of individuals reported being able to lift themselves up while roughly 26.7% remained on the floor for more than an hour.
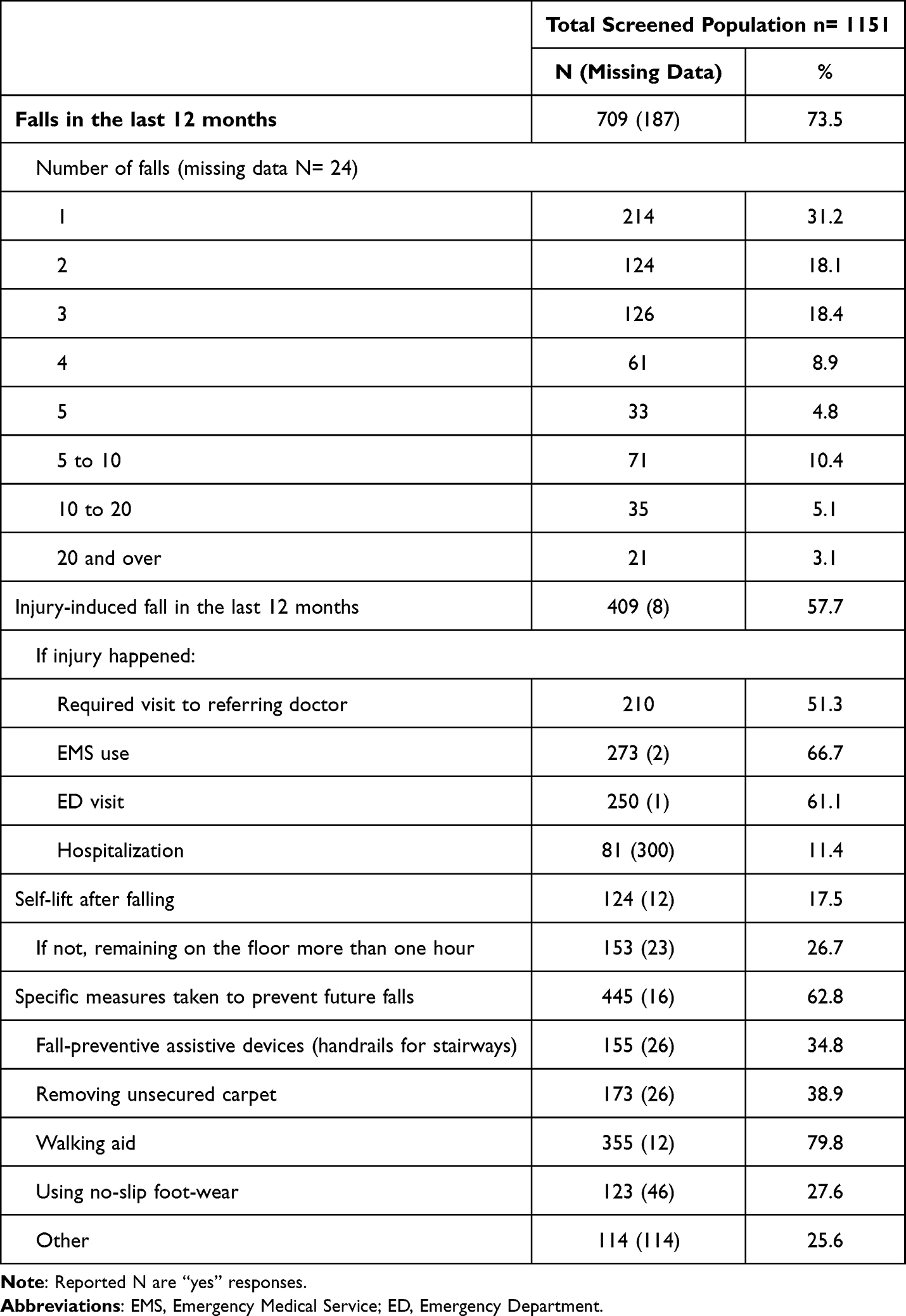 |
Table 3 Previous Fall History and Related Consequences |
More than half (60%) of the individuals with a history of falls took proactive steps to prevent future falls. The most frequently reported measure was the utilization of walking aids which accounted for 79.8% of cases. Removing unsecured carpet was the second measure at 38.9%, followed by wearing proper non-slip shoes or slippers at 27.6%. An analysis of the data using an UpSet plot revealed that in 8.5% (N = 38) of cases, measures were taken simultaneously including the installation of fall-preventive assistive devices, removal of unsecured carpet and use of walking aids (Figure 3).
 |
Figure 3 UpSet plot analysis of fall prevention strategies adopted by individuals with a history of falls. |
The comparison of randomized and non-randomized participants to check the presence of selection bias showed that no considerable differences in demographic characteristics such as age, sex or lifestyle as well as the injury severity and fall outcomes were found. However, a significant difference (p=0.022) was found in the variable “number of falls in the last 12 months =1” (Supplementary Data 1).
Discussion
Challenges associated with enrolling older people in randomized trials are acknowledged, and recruitment could be the first critical step in fall prevention trials.18,20 Providing feedback on our recruitment experience is of interest, especially as the used methodologies of recruitment and interventions are implemented outside the hospital setting and target a population for which limited data are available.5,6,9
Participants Screening and Enrollment: The RISING-DOM Experience
In the RISING-DOM study, we faced recruitment challenges at various stages. First, our investigation on the sample of EMS calls revealed that a substantial portion of calls were deemed ineligible for inclusion due to protocol exclusion criteria (such as living in nursing homes, falls outside home, living far from the investigator sites) and other constraints such as the absence of contact information. This point emphasizes the challenge of identifying our target population, even when applying keyword filters as they are often drowned out within the important flow of EMS calls. Although we have not assessed the EMS call profile of the other participating centers, our investigation teams have frequently reported a problem with a small number of eligible individuals and a lack in patient contact information. This issue could be attributed, in part, to misreporting by the EMS staff, which is sometimes influenced by challenges in hearing and speech during the telephone medical interview.
The second challenging point was the recruitment of the target population by telephone that could result in a laborious process, particularly when the investigator team must make multiple attempts to reach the individual, in addition to known problems in older adults enrollment such as hearing impairments and decreased comprehension of the study design.23 Moreover, some older adults or their relatives were uncomfortable with the calls as they feared they might be related to fraudulent information or commercial purposes. According to the study protocol,21 EMS staff had to deliver study information during home interventions for falls. However, our results reveal that, despite establishing a strong partnership, the intended information delivery did not take place. Our experience showed that once a trusted relationship with the “would-be participants” or their family had been established, the rate of achieving enrollment was important (82.62%). Nevertheless, we believe that effective collaboration from the EMS staff would have had a positive impact on the acceptance of participation and increase in screening opportunities. It would be of interest to investigate and address the barriers preventing EMS providers from actively participating in the dissemination of study information and their potential involvement in providing fall prevention guidelines. Barmentloo et al18 emphasized that changing the mindset and routines of healthcare professionals is among one of the significant barriers to be addressed in screening older fallers.
The third major challenge faced was the overlap of participant screening with the COVID-19 pandemic. Initially, screening was disrupted due to the lock-down and restrictions on visits to the homes of older people and then slowed down as healthcare professionals at the study sites were focused on managing the health crisis. However, the remote screening and conducting the trial outside the hospital were a good opportunity to avoid an extended interruption of the trial. In response to the health crisis, remote screening and clinical trials with decentralized design have gained increased popularity.24
The involvement of family members or legal representatives in the consent process seems to not have a significant impact on the participation of older adults in the study. Comparison of randomized and non-randomized characteristics showed a significant difference in participants with only one fall suggesting a possible denial and under-estimation of the risk of falling. This issue has been previously reported as a barrier to participation in fall prevention interventions.25
Beyond all the barriers cited above, conducting the trial in the participant’s own house was one of the appreciated aspects of the study that potentially impacted the decision of the older persons and their families to participate.
Population and Fall Characteristics
Our findings showed that the general demographic characteristics of the target population (mean age, sex differences in fall rates) and fall traits (main home fall locations, timing and main activities prior to falling) are comparable with what has been documented in previous studies on community-dwelling older adults and for home falls.26–29
For example, as previously reported,26,29,30 walking was the most frequently cited activity prior to falls (47.3%) and most falls happened in the morning (28.7%) in commonly used rooms (bedroom, living room and kitchen). In addition, our finding is consistent with existing literature which suggests that falls typically result in no physical injuries or minor injuries, such as grazes and bruises and that a small range (10 to 15%) resulted in serious injuries.31–33 Moderate injuries were reported in only 22.6% of cases showing that falls at home resulted mainly in no physical injury or minor injuries.
Apart from described fall characteristics, it is worth noting that our population sample shares the features of a high-risk fall group. For example, the main reported outcomes here were pain and, to a lesser extent, fear of falling and restriction of activities. These fall-induced outcomes have been recognized as predictors of future falls and can lead to negative health outcomes.27,34–36 For instance, results from a systematic review investigating pain as a risk for falls in community-dwelling showed that older adults who experience pain are more likely to have fallen in the past year and experience a higher risk of future falls compared to those without pain.27
Moreover, we found that about three quarters of individuals in our cohort indicated having a fall history in the past 12 months which is relatively high compared to reported rates (25.6%–53%),26,28,32,37 which could be explained by over-estimation due to self-reporting. Our finding suggests that our sample study population is at increased risk of repeated falls as previous investigations showed that older people who experienced previous falls are at increased risk of recurrence and EMS use.38–40 This was especially outlined in older adults aged over 80 years and living alone with complaints of dizziness and other symptoms.41 Data on medical history and medical treatments are not available yet in our analysis but the mean age of our sample (84.1) and the proportion of those living alone (44%) are indicators of vulnerability. Studies have suggested that living alone can significantly increase the risk of falling,42 with some authors estimating that the risk can be 1.2 to 3.1 times higher.43 In this sense, Choi et al44 recommended that fall prevention programs should focus specifically on individuals living in isolation as they may have limited access to medical resources and are more likely to require hospitalization after a fall.
More than half of the respondents who had experienced a fall reported taking specific measures to prevent future falls, indicating that about 40% had not taken any action. Furthermore, the use of walking aids was the only engaged action in most cases. We did not explore whether this action was taken on the participant’s own initiative or based on professional guidance. According to a survey on Californian older people with a history of fall, it was stated that professional recommendations on fall prevention-related lifestyle or living condition changes were not consistently given to these patients.45 In our study, given that most interventions only included walking aids, it is likely that most participants would not have benefited from proper medical guidance. Walking aids could indeed represent fall risk factors and appropriate instructions on their proper use in terms of adequate and safe gait patterns are recommended.46,47
Based on our results, our findings highlight the potential need to improve guidance in this high-risk population to receive proper post-fall/fall-preventive advices. Qin et al45 suggested that future interventions should further involve health care professionals, especially primary care physicians. In our cohort, out of the 417 older people who experienced a fall causing an injury in the past 12 months, only 81 underwent long-term hospitalization but more than half resulted in referring doctor visits and EMS use. This further suggests that our population sample is unlikely to be given fall prevention guidance during their hospital stay and their main healthcare sources are primary physicians and EMS personnel.
Limitation and Strength
This study provides information about a group of older people who represent a priority for fall prevention.6 Screening from the ORU database ensures maximizing the representation of the target population (not only those attending the hospital or with geriatric history or only those attending community-based settings who could be most robust). In addition, we have successfully built up a substantial sample size from different areas, thereby maximizing the external validity of the study. The weakness of our study lies in the fact that it is mostly based on self-reported data and could result in miss-reporting and lack of accuracy. Study shortcomings may arise from potential selection bias in participant recruitment such as low recruitment rates among individuals who have not called for EMS assistance after falling or those who use personal medical alarms which do not provide identifiable contact information.
Conclusion
The screening and recruitment of a significant number of participants, despite the various challenges, supports the effectiveness of remote screening of community-dwelling individuals who have experienced a fall and its usefulness in the epidemic context. Preliminary capture of the target population revealed that our sample shares characteristics of a high risk of fall group in need of guidance to prevent future falls. The RISING-DOM intervention should state to what extent the designed multidimensional prevention program could be effective and applicable to the community-living older adults.
Data Sharing Statement
The data that support the findings are available from the corresponding author Wafa Bouzid ([email protected]) upon reasonable request.
Ethics Declarations
As far as the RISING-DOM trial falls under the category of studies with minimal risk and does not entail any additional risks beyond those encountered in everyday life, oral consent was deemed sufficient. Furthermore, since recruitment was conducted remotely, it is more convenient to have verbal consent rather than written consent. The collection of verbal consent, as well as the tools employed to inform potential participants, have received approval from the ethics committee “Committee for the Protection of Persons and Competent Authority” (CPP of Ile de France VII, 05 December 2018).
Prior to enrollment, all participants received the informed consent form by email or postal mail. The investigator delivered then all the necessary information about the study and collected oral consent according to the study design. The investigator filled out a consent form in the source file, explicitly indicating that the consent was obtained orally via phone, specifying the date and time of the phone call and providing their signature. This completed form is then archived among the study documents, and a copy is sent to the participant by email or postal mail. In addition, a non-opposition approval form was sent to all screened participants, whether they were later included or withdrawn from the RISING-DOM follow-up to inform them about the use of their data for descriptive purpose. The study was conducted in accordance with the Declaration of Helsinki.
Acknowledgments
The Authors wish to thank the Occitania Emergency Observatory for providing EMS data, in particular A. Broens. The Authors express their gratitude to all the geriatrician investigators, emergency physicians, referring doctors, nurses, pharmacists and clinical research associates who contributed to this study. They are also grateful to Dr C. Lafont, Dr C. Faisant, Dr B. Abdeljalil, Dr O. Azema and E. Moulis for their precious help in participant inclusion, P. Cassan for data management assistance and C. Dedieu for handling regulatory issues.
Funding
This study was supported by a grant from the French Ministry of Health (Programme de recherche sur la performance du système des soins; PREPS 2017, PREPS-17–0357).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Rubenstein LZ. Falls in older people: epidemiology, risk factors and strategies for prevention. Age Ageing. 2006;35(Suppl 2):ii37–ii41. doi:10.1093/ageing/afl084
2. James SL, Lucchesi LR, Bisignano C, et al. The global burden of falls: global, regional and national estimates of morbidity and mortality from the Global Burden of Disease Study 2017. Inj Prev. 2020;26(Supp 1):i3–i11. doi:10.1136/injuryprev-2019-043286
3. Mikolaizak AS, Simpson PM, Tiedemann A, Lord SR, Close JCT. Systematic review of non-transportation rates and outcomes for older people who have fallen after ambulance service call-out. Australas J Ageing. 2013;32(3):147–157. doi:10.1111/ajag.12023
4. Close JCT, Halter M, Elrick A, Brain G, Swift CG. Falls in the older population: a pilot study to assess those attended by London ambulance service but not taken to A&E. Age Ageing. 2002;31(6):488–489. doi:10.1093/ageing/31.6.488
5. Logan PA, Coupland CAC, Gladman JRF, et al. Community falls prevention for people who call an emergency ambulance after a fall: randomised controlled trial. BMJ. 2010;340:c2102. doi:10.1136/bmj.c2102
6. Snooks HA, Halter M, Close JCT, Cheung WY, Moore F, Roberts SE. Emergency care of older people who fall: a missed opportunity. Qual Saf Health Care. 2006;15(6):390–392. doi:10.1136/qshc.2006.018697
7. Gray JT, Walker A. Avoiding admissions from the ambulance service: a review of elderly patients with falls and patients with breathing difficulties seen by emergency care practitioners in South Yorkshire. Emerg Med J. 2008;25(3):168–171. doi:10.1136/emj.2007.050732
8. Vilke GM, Sardar W, Fisher R, Dunford JD, Chan TC. Follow-up of elderly patients who refuse transport after accessing 9-1-1. Prehosp Emerg Care. 2002;6(4):391–395. doi:10.1080/10903120290938003
9. Tiedemann A, Mikolaizak AS, Sherrington C, Segin K, Lord SR, Close JCT. Older fallers attended to by an ambulance but not transported to hospital: a vulnerable population at high risk of future falls. Aust N Z J Public Health. 2013;37(2):179–185. doi:10.1111/1753-6405.12037
10. Bonner M, Capsey M, Batey J. A paramedic’s role in reducing number of falls and fall-related emergency service use by over 65s: a systematic review. Br Paramed J. 2021;6(1):46–52. doi:10.29045/14784726.2021.6.6.1.46
11. Boright LE, Arena SK, Wilson CM, McCloy L. The effect of individualized fall prevention programs on community-dwelling older adults: a scoping review. Cureus. 2022;14(3):e23713. doi:10.7759/cureus.23713
12. Gates S, Fisher JD, Cooke MW, Carter YH, Lamb SE Multifactorial assessment and targeted intervention for preventing falls and injuries among older people in community and emergency care settings: systematic review and meta-analysis. Centre for Reviews and Dissemination (UK); 2008. Available from: https://www.ncbi.nlm.nih.gov/books/NBK74943/.
13. Gillespie LD, Robertson MC, Gillespie WJ, et al. Interventions for preventing falls in older people living in the community. Cochrane Database Syst Rev. 2012;2012(9):CD007146. doi:10.1002/14651858.CD007146.pub3
14. Hopewell S, Adedire O, Copsey BJ, et al. Multifactorial and multiple component interventions for preventing falls in older people living in the community. Cochrane Database Syst Rev. 2018;7(7):CD012221. doi:10.1002/14651858.CD012221.pub2
15. Montero-Odasso M, van der Velde N, Martin FC, et al. World guidelines for falls prevention and management for older adults: a global initiative. Age Ageing. 2022;51(9):afac205. doi:10.1093/ageing/afac205
16. Ganz DA, Latham NK, Solomon CG. Prevention of falls in community-dwelling older adults. N Engl J Med. 2020;382(8):734–743. doi:10.1056/NEJMcp1903252
17. Guirguis-Blake JM, Michael YL, Perdue LA, Coppola EL, Beil TL, Thompson JH Interventions to prevent falls in community-dwelling older adults: a systematic review for the U.S. preventive services task force. Agency for Healthcare Research and Quality (US); 2018. Available from: http://www.ncbi.nlm.nih.gov/books/NBK525700/.
18. Barmentloo LM, Dontje ML, Koopman MY, et al. Barriers and facilitators for screening older adults on fall risk in a hospital setting: perspectives from patients and healthcare professionals. Int J Environ Res Public Health. 2020;17(5):1461. doi:10.3390/ijerph17051461
19. Fernandes JB, Fernandes SB, Almeida AS, Vareta DA, Miller CA. Older adults’ perceived barriers to participation in a falls prevention strategy. J Pers Med. 2021;11(6):450. doi:10.3390/jpm11060450
20. Wilding MJ, Seegert L, Rupcic S, Griffin M, Kachnowski S, Parasuraman S. Falling short: recruiting elderly individuals for a fall study. Ageing Res Rev. 2013;12(2):552–560. doi:10.1016/j.arr.2012.12.002
21. Bouzid W, Tavassoli N, Berbon C, et al. Impact of a personalised care plan for the elderly calling emergency medical services after a fall at home: the RISING-DOM multi-centre randomised controlled trial protocol. BMC Geriatr. 2022;22(1):182. doi:10.1186/s12877-022-02850-w
22. INSEE - Institut national de la statistiques et des études économiques [The National Institute of Statistics and Economic Studies]; February 27, 2023 Available from: https://www.insee.fr/fr/accueil.
23. Kelsey JL, O’Brien LA, Grisso JA, Hoffman S. Issues in carrying out epidemiologic research in the elderly. Am J Epidemiol. 1989;130(5):857–866. doi:10.1093/oxfordjournals.aje.a115418
24. Loucks TL, Tyson C, Dorr D, et al. Clinical research during the COVID-19 pandemic: the role of virtual visits and digital approaches. J Clin Transl Sci. 2021;5(1):e102. doi:10.1017/cts.2021.19
25. Bunn F, Dickinson A, Barnett-Page E, Mcinnes E, Horton K. A systematic review of older people’s perceptions of facilitators and barriers to participation in falls-prevention interventions. Ageing Soc. 2008;28(4):449–472. doi:10.1017/S0144686X07006861
26. Berg WP, Alessio HM, Mills EM, Tong C. Circumstances and consequences of falls in independent community-dwelling older adults. Age Ageing. 1997;26(4):261–268. doi:10.1093/ageing/26.4.261
27. Stubbs B, Binnekade T, Eggermont L, Sepehry AA, Patchay S, Schofield P. Pain and the risk for falls in community-dwelling older adults: systematic review and meta-analysis. Arch Phys Med Rehabil. 2014;95(1):175–187.e9. doi:10.1016/j.apmr.2013.08.241
28. Zhang L, Ding Z, Qiu L, Li A. Falls and risk factors of falls for urban and rural community-dwelling older adults in China. BMC Geriatr. 2019;19(1):379. doi:10.1186/s12877-019-1391-9
29. Stevens JA, Mahoney JE, Ehrenreich H. Circumstances and outcomes of falls among high risk community-dwelling older adults. Inj Epidemiol. 2014;1(5). doi:10.1186/2197-1714-1-5
30. Sanders KM, Lim K, Stuart AL, et al. Diversity in fall characteristics hampers effective prevention: the precipitants, the environment, the fall and the injury. Osteoporos Int. 2017;28(10):3005–3015. doi:10.1007/s00198-017-4145-6
31. Resnick B, Junlapeeya P. Falls in a community of older adults: findings and implications for practice. Appl Nurs Res. 2004;17(2):81–91. doi:10.1016/j.apnr.2004.03.004
32. Milat AJ, Watson WL, Monger C, Barr M, Giffin M, Reid M. Prevalence, circumstances and consequences of falls among community-dwelling older people: results of the 2009 NSW Falls Prevention Baseline Survey. N S W Public Health Bull. 2011;22(3–4):43–48. doi:10.1071/NB10065
33. Campbell AJ, Borrie MJ, Spears GF, Jackson SL, Brown JS, Fitzgerald JL. Circumstances and consequences of falls experienced by a community population 70 years and over during a prospective study. Age Ageing. 1990;19(2):136–141. doi:10.1093/ageing/19.2.136
34. Hill KD. Fear of falling: a hidden burden with or without a history of falls. Evid Based Nurs. 2019;22(1):21. doi:10.1136/eb-2018-102978
35. Makino K, Makizako H, Doi T, et al. Impact of fear of falling and fall history on disability incidence among older adults: prospective cohort study. Int J Geriatr Psychiatry. 2018;33(4):658–662. doi:10.1002/gps.4837
36. Cai Y, Leveille SG, Shi L, Chen P, You T, Newman AB. Chronic pain and risk of injurious Falls in community-dwelling older adults. J Gerontol a Biol Sci Med Sci. 2021;76(9):e179–e186. doi:10.1093/gerona/glaa249
37. Torres MJ, Pédrono G, Rigou A, Carcaillon-Bentata L, Beltzer N. Identifying profiles of people aged 65 and over who fall at home and associated falling-induced injuries: the French ChuPADom study. Injury. 2022;53(7):2511–2518. doi:10.1016/j.injury.2022.02.021
38. Mikolaizak AS, Harvey L, Toson B, et al. Linking health service utilisation and mortality data-unravelling what happens after fall-related paramedic care. Age Ageing. 2022;51(1):afab254. doi:10.1093/ageing/afab254
39. Simpson PM, Bendall JC, Tiedemann A, Lord SR, Close JCT. Epidemiology of emergency medical service responses to older people who have fallen: a prospective cohort study. Prehosp Emerg Care. 2014;18(2):185–194. doi:10.3109/10903127.2013.856504
40. Simpson PM, Bendall JC, Toson B, Tiedemann A, Lord SR, Close JCT. Predictors of nontransport of older fallers who receive ambulance care. Prehosp Emerg Care. 2014;18(3):342–349. doi:10.3109/10903127.2013.864355
41. Pratt NL, Ramsay EN, Kalisch Ellett LM, Nguyen TA, Barratt JD, Roughead EE. Association between use of multiple psychoactive medicines and hospitalization for falls: retrospective analysis of a large healthcare claim database. Drug Saf. 2014;37(7):529–535. doi:10.1007/s40264-014-0179-2
42. Xu Q, Ou X, Li J. The risk of falls among the aging population: a systematic review and meta-analysis. Front Public Health. 2022;10. doi:10.3389/fpubh.2022.902599
43. Kwan MMS, Close JCT, Wong AKW, Lord SR. Falls incidence, risk factors, and consequences in Chinese older people: a systematic review. J Am Geriatr Soc. 2011;59(3):536–543. doi:10.1111/j.1532-5415.2010.03286.x
44. Choi NG, Choi BY, DiNitto DM, Marti CN, Kunik ME. Fall-related emergency department visits and hospitalizations among community-dwelling older adults: examination of health problems and injury characteristics. BMC Geriatr. 2019;19(1):303. doi:10.1186/s12877-019-1329-2
45. Qin Z, Baccaglini L. Distribution, determinants, and prevention of falls among the elderly in the 2011–2012 California Health Interview Survey. Public Health Rep. 2016;131(2):331–339. doi:10.1177/003335491613100217
46. Deandrea S, Lucenteforte E, Bravi F, Foschi R, La Vecchia C, Negri E. Risk factors for falls in community-dwelling older people: a systematic review and meta-analysis. Epidemiology. 2010;21(5):658–668. doi:10.1097/EDE.0b013e3181e89905
47. Roman de Mettelinge T, Cambier D. Understanding the relationship between walking aids and falls in older adults: a prospective cohort study. J Geriatr Phys Ther. 2015;38(3):127–132. doi:10.1519/JPT.0000000000000031
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.