Back to Journals » Journal of Inflammation Research » Volume 17
Exploring Interleukin-10 Levels in Diabetes Patients with and without Oral Diseases: A Systematic Review
Authors Novianti Y ![]() , Nur’aeny N
, Nur’aeny N ![]()
Received 20 November 2023
Accepted for publication 23 January 2024
Published 31 January 2024 Volume 2024:17 Pages 541—552
DOI https://doi.org/10.2147/JIR.S449546
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Tara Strutt
Yessy Novianti,1 Nanan Nur’aeny2
1Oral Medicine Residency Program, Faculty of Dentistry, Universitas Padjadjaran, Bandung, Indonesia; 2Oral Medicine Department, Faculty of Dentistry, Universitas Padjadjaran, Bandung, Indonesia
Correspondence: Yessy Novianti, Faculty of Dentistry, Universitas Padjadjaran, Jalan Sekeloa Selatan I, Bandung, 40132, Indonesia, Tel +6281368429045, Email [email protected]
Aim: Interleukin-10 (IL-10) is a cytokine that plays an important role in the progression of diabetes mellitus (DM). Oral diseases were more common in diabetics than in non-diabetics. The aim of this review is to identify IL-10 levels in diabetic patients with and without oral diseases.
Methods: A systematic review was conducted based on the PRISMA guidelines. Three databases (PubMed, Cochrane Library, and Science Direct) were used to search for articles up to November 2023 for studies on the measurement of IL-10 in diabetics with and without oral disease. The criteria were limited to human studies and full-text in English only. The outcome was the value of IL-10. The study was quality-graded using the Risk of Bias Assessment Tool for Non-randomized Studies (RoBANS).
Results: There were eleven articles that met the eligibility criteria for analysis. Four articles discovered higher IL-10 levels, while seven articles discovered lower IL-10 levels in diabetes patients with oral diseases compared with each control group.
Conclusion: Most studies showed lower IL-10 levels in diabetic patients with oral diseases compared with the control group.
Keywords: anti-inflammatory, candidiasis, cytokine, insulin resistance, periodontitis
Introduction
Diabetes mellitus (DM) is a chronic metabolic disorder marked by elevated blood glucose levels due to insufficient insulin production, impaired insulin function, or both.1,2 It is a global health concern with a rising prevalence.3,4 According to the International Diabetes Federation (IDF) Annual Report 2022, an estimated 540 million people worldwide are affected by diabetes, with the number expected to rise in the future.5 Diabetes can be broadly classified into two types: type 1 and type 2.2,6–12 Type 1 diabetes (T1D) is an autoimmune condition where the immune system attacks and destroys insulin-producing beta cells in the pancreas.2,11,13 Type 2 diabetes (T2D) is marked by insulin resistance, where the body’s cells do not respond effectively to insulin, and insufficient insulin production.10,11,14,15 The complications of diabetes are diverse and affect various organ systems, including the cardiovascular system, kidneys, eyes, and oral cavity.1,16,17
Oral health is a vital component of overall health, and people with diabetes are more susceptible to oral diseases.18,19 Diabetes is known to cause oral complications, including periodontal disease, xerostomia (dry mouth), an increased risk of infections, delayed wound healing, and other oral diseases.3,16,18–24 It is essential to comprehend and tackle oral health in diabetic patients. Poor oral health can exacerbate complications related to diabetes and vice versa, creating a bidirectional relationship.18,19 Periodontal disease has been linked to increased insulin resistance and uncontrolled glycemic.25 Furthermore, oral infections may contribute to systemic inflammation, which could affect the management of diabetes.7,9,16 Investigating the relationship between DM, oral health, and immune responses, such as IL-10 levels, can provide valuable knowledge on how these conditions are interrelated and guide holistic approaches to patient care.
Interleukin-10 (IL-10) is a cytokine, a signaling molecule that is fundamental for regulating the immune system.26 It is known for its anti-inflammatory properties and is produced by various immune cells, including macrophages and T cells.27 IL-10 has a crucial function in prohibiting excessive immune reactions and preventing prolonged inflammation and tissue damage.28,29 In the context of DM and related complications, IL-10 may play a role in modulating immune responses that could impact oral health.30 The imbalance of IL-10 levels has been linked to inflammatory conditions. Exploring their role in the context of DM and oral diseases can provide insights into the associated immune mechanisms.30–33 Investigation of IL-10 levels in diabetic patients with oral diseases is relevant not only for understanding the immunological aspects of the disease but also for exploring potential therapeutic targets that may help in managing both DM and oral health issues.30
The aim of this systematic review is to clarify the relationship between IL-10 levels and oral diseases in patients with DM. This may include considerations for healthcare providers in managing the oral health of patients with DM, highlighting areas for preventive strategies or interventions based on IL-10 levels. In addition, the review’s objective is to identify gaps in the existing literature and suggest directions for future research to guide the scientific community in addressing open-ended issues and understanding the interplay between DM, IL-10, and oral health.
Materials and Methods
Protocol and Eligibility Criteria
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were followed in the conduct of this systematic review. PICO components included a population, a problem (human patients with all types of diabetes), an intervention (measuring interleukin 10), a comparison (people with and without oral disease), and an outcome (the results of the intervention). The authors agreed not to distinguish the source of the IL-10 measurement sample, whether blood, saliva, or gingival sulcus fluid were all included. The inclusion criteria included articles published in the last 3 years, available full-text, human studies, English-language publications, articles addressing the interleukin-10 level in diabetic patients with oral diseases, and no age, sex, or racial limitations. As there were no systematic reviews of publications from the preceding three years, we made the decision to compile studies from 2020 to 2023. The exclusion criteria were articles irrelevant to the topic, duplication, literature/systematic reviews, case reports, incomplete manuscripts, and non-English language.
Information Sources and Search Strategy
The electronic article search was conducted using three databases, such as PubMed, Cochrane Library, and Science Direct. The keywords used were “interleukin-10” [MeSH terms] AND “oral complication of diabetes mellitus” [MeSH terms] OR “oral disease” [MeSH terms] OR “oral candidiasis” [MeSH terms] OR “gingivitis” [MeSH terms] OR “periodontitis” [MeSH terms] OR “oral ulcer” [MeSH terms] OR “oral lichen planus” [MeSH terms] OR “geographic tongue” [MeSH terms] OR “sialosis” [MeSH terms] OR “oral lesions” [text word] OR “oral cancer” [MeSH terms] OR “dental caries” [MeSH terms] OR “xerostomia” [MeSH terms] OR “burning mouth syndrome” [MeSH terms] OR “dysgeusia” [MeSH terms]. The PRISMA flowchart is shown below (Figure 1).
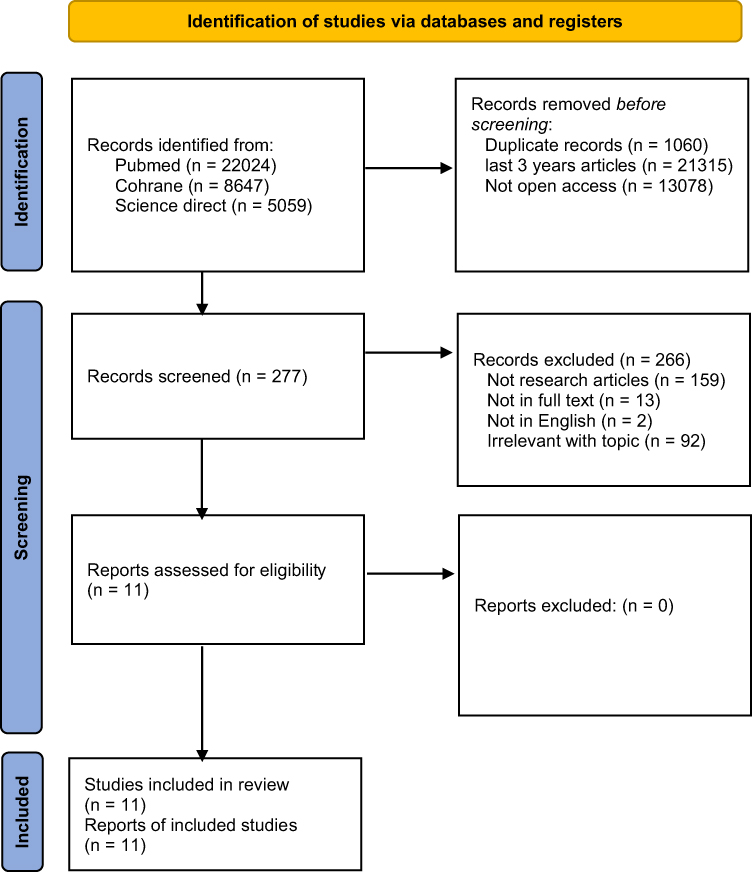 |
Figure 1 The PRISMA flow diagram of the article search and selection process. |
Study Records and Data Items
The selection of articles was carried out by YN. The relevant data were extracted, and the important information was selected by the authors (NN and YN). The data extracted from the full-text articles includes researcher, country, aim, population, type of DM, oral diseases, sample and method, result, and conclusion, as shown in Table 1. The main study outcome was IL-10 levels in humans. The final recommendation in this study was modified after the authors, NN and YN, discussed the extracted data. Discussions and decisions are made according to the differences of opinion in order to reach a mutually acceptable conclusion. There is no difference in the determination of the articles to be reviewed, the extracted data, or the assessment of the risk of bias.
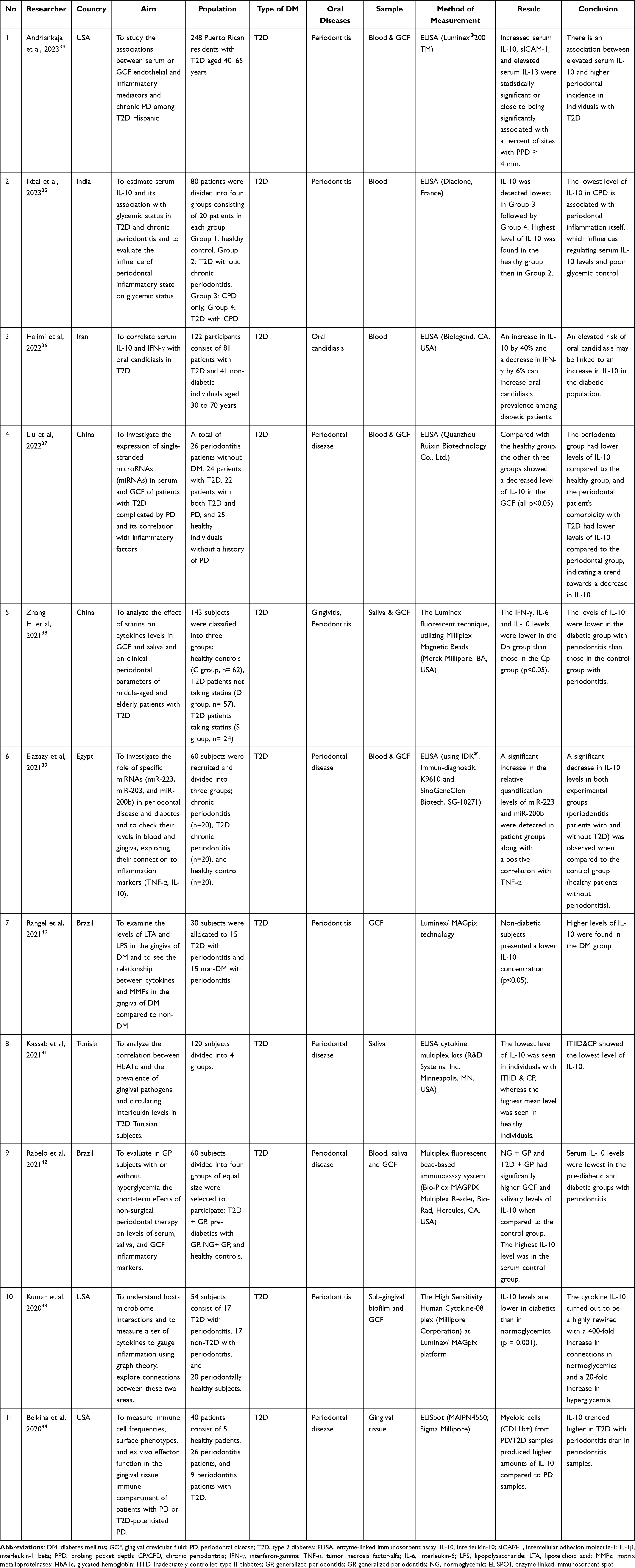 |
Table 1 Characteristics of the Reviewed Studies |
Risk of Bias in Individual Studies
The potential for bias was assessed using the Risk of Bias Assessment Tool for Non-randomized Studies (RoBANS) by YN and NN. The six domains of RoBANS consisted of participant selection, confounding variables, measurement of exposure or intervention, blinding of outcome assessment, incomplete outcome data, and selective reporting. Each assessment item is a question with a score of 1 for the answer “yes” or “available”, and 0 for the answer “no” or “not available”. The total score is the sum of the answers to all six questions; it might vary from 0 to 6. The evaluation parameters were: the risk of bias is high or the quality of the article is low if the total score is between 0 and 2, and the risk of bias is low or the quality of the article is high if the total score is between 3 and 6.
Results
The search of the database yielded a total of 35,730 articles. 22,024 articles were identified using keywords from the PubMed database, 8647 from the Cochrane Library, and 5059 from Science Direct. The screening process, including database filters and inclusion criteria, resulted in a total of 277 articles. 266 articles were excluded due to not being research studies, not being in full text, non-English, and irrelevant to the topic. A total of 11 articles were at the end of the screening stage. These articles were then evaluated for their eligibility using risk-of-bias tools and subjected to a qualitative review. Figure 1 depicts a flowchart of the article search and selection process in this review.
Table 1 summarizes the characteristics of the studies reviewed based on the year of publication. The USA34,43,44 conducted three of the articles, with one each from India,35 Iran,36 China (two articles),37,38 Egypt,39 Tunisia,41 and Brazil (two articles).40,42 The research participant count in each article ranges from 15 to 248 diabetic patients, resulting in a total of 801 diabetic patients, both with and without oral diseases. The study involved 253 control participants, ranging from 5 to 62 individuals per article. The review encompasses eleven articles, out of which ten examined interleukin-10 levels in diabetic patients with periodontitis as an oral disease, while the remaining article evaluated interleukin-10 levels in diabetic patients with oral candidiasis.
Table 2 and Figure 2 present the findings of the risk of bias evaluation conducted to determine the quality of the selected articles. The results of the risk assessment of bias indicate that all eleven articles had a low risk of bias, thus indicating the high quality of the studies. Domain selection of participants (item 1), confounding variables (item 2), and measurement exposure (item 3) achieved a score of 100%. This score was excellent, as all articles met the expected criteria. All participants adhered to the research protocol and successfully completed it. The domain with the lowest percentage score was the incomplete outcome data domain (item 5), which received a score of 0% because all articles did not mention missing outcome data. The blinding of outcome assessment (item 4) had a percentage score of 9.1% because only one article stated explicit blinding methodology in the article’s research protocol. The selective outcome reporting (item 6) received a score of 90.9%; this score was deemed satisfactory, as only one out of eleven articles in these domains failed to meet the criteria.
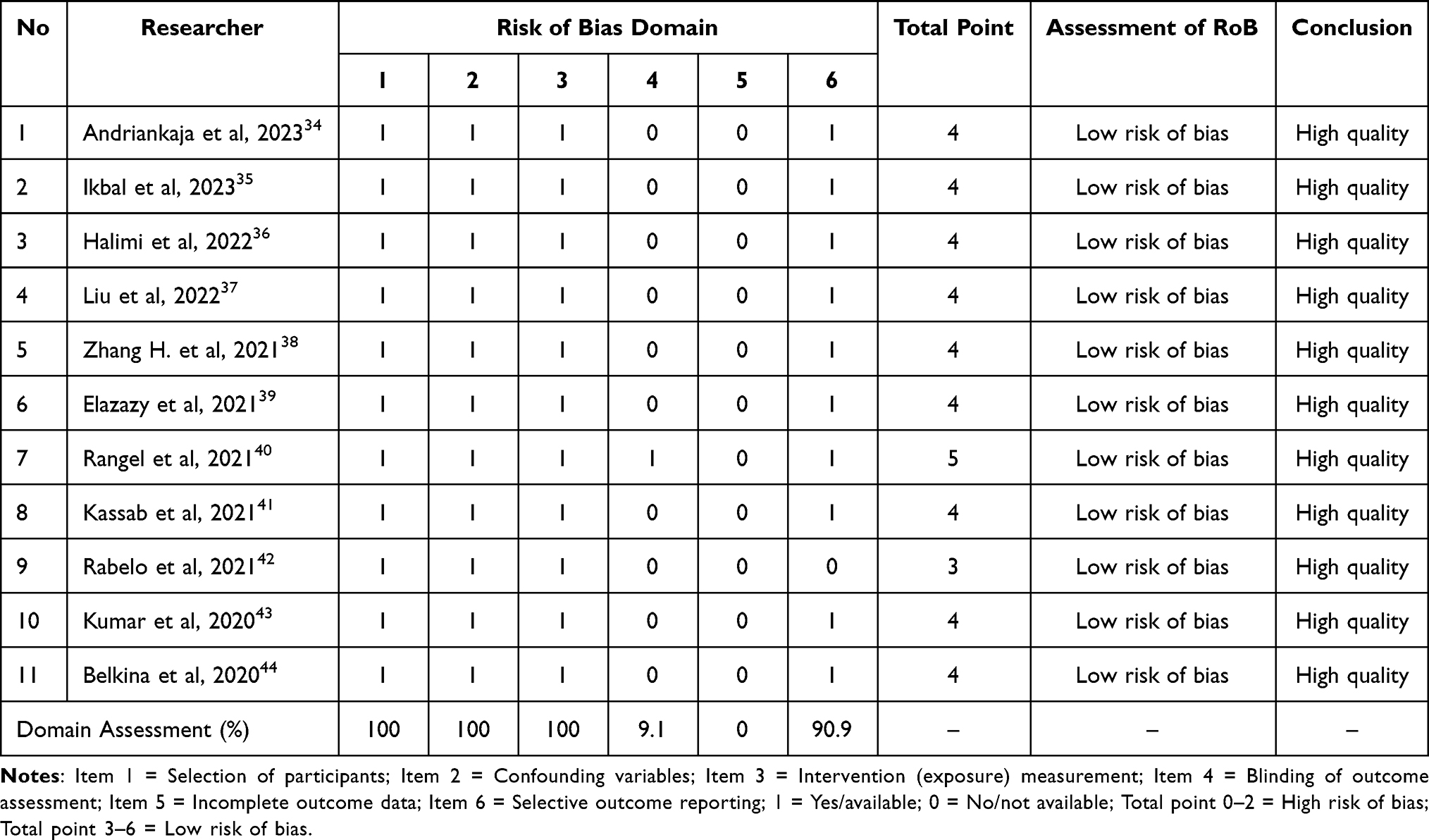 |
Table 2 Risk of Bias Assessment (RoB) |
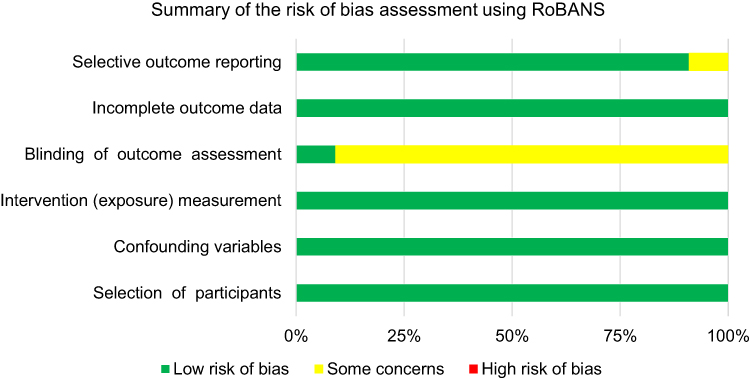 |
Figure 2 Author assessment of each RoBANS domain for the included articles. Green denotes a low risk of bias, yellow denotes an unclear risk, and red denotes a high risk. The six domains are “participant selection, confounding variables, measurement of exposure, blinding of the outcome, incomplete outcome data, and selective outcome reporting”. |
Discussion
DM is a systemic condition characterized by hyperglycemia resulting from defects in insulin secretion, insulin action, or both.1,7,8,45 DM patients had a significantly higher prevalence of oral diseases compared to non-DM patients.10 These manifestations refer to symptoms or conditions in the mouth that arise due to the underlying disease. Changes in immune system function can influence the appearance of oral diseases in DM patients.11,46 The oral diseases commonly seen in diabetic patients include geographic tongue, oral candidiasis, dental caries, sialosis, oral cancer, oral ulcer, gingivitis and periodontitis, oral lichen planus/lichenoid mucositis, xerostomia, burning mouth syndrome, and dysgeusia.7,8,10,11,19,24,46–49
The process of wound healing and tissue repair in DM patients involves cytokines.50 One of the anti-inflammatory cytokines that plays an important role in the regulation of immune response and inflammation is interleukin (IL)-10. IL-10 was initially discovered by Mosmann et al in 1989.27 It functions as a crucial anti-inflammatory cytokine by acting as a negative regulator of the immune response to microbial antigens.27 IL-10 effectively prevents excessive inflammation during the course of infection and is produced in response to pro-inflammatory signals by immune cells, including T cells, B cells, macrophages, and dendritic cells.26,27
Inflammation plays a key role in the development of diabetic complications.51 Inflammation is a mechanism activated in response to harmful conditions to maintain homeostasis and tissue integrity.52 Chronic activation of the inflammatory response triggers collaterally injurious effects. Hyperglycemia and oxidative stress are the drivers of tissue damage in individuals with DM.17 Impaired immune response and higher susceptibility to infection play an important role in the development of DM complications, including oral diseases in DM patients.16 This review explored the IL-10 level as an anti-inflammatory mediator in diabetic patients with and without oral diseases.
Table 1 shows that the studies were conducted in type 2 diabetes populations in the USA,34,43,44 India,35 Iran,36 China,37,38 Egypt,39 Brazil,40,42 and Tunisia.41 The most observed DM-related oral diseases were periodontitis, with 10 articles, and one article discussed oral candidiasis. Samples taken to check IL-10 were generally from blood, saliva, gingival crevicular fluid (GCF), and gingival tissue.
Four of the eleven studies that were reviewed regarding IL-10 and oral diseases in diabetic individuals came to the conclusion that those patients had higher levels of IL-10. This is supported by four articles by the following researchers: Andriankaja et al,34 Halimi et al,36 Rangel et al,40 and Belkina et al.44 An article conducted by Halimi et al36 discussed IL-10 levels related to oral candidiasis as DM-related oral diseases, while three other articles discussed IL-10 levels related to periodontitis in DM patients.
Increased IL-10 in DM patients with periodontitis may weaken their immune response, worsening infectious inflammation in both conditions. Elevated IL-10 in periodontitis can hinder pro-inflammatory cytokine production, impacting disease progression. The elevated plasma/serum IL-10 was observed more frequently in individuals with T2D, showing hyper-inflammatory states.34,40,44
IL-10 impacts the immune cells involved in fungal defense, increasing the risk of fungal infections.36 Research conducted by Halimi et al revealed elevated IL-10 levels among diabetic patients with oral candidiasis as compared to healthy individuals.36 This association indicates that the immune system in diabetic individuals is more vulnerable to chronic diseases, possibly due to the inhibitory effects of IL-10 on fungal defense, leading to the progression of chronic diseases.36
Seven out of eleven studies concluded that IL-10 levels in DM patients with oral diseases (periodontitis) were lower than IL-10 levels in the control group.35,37–39,41–43 The reduced IL-10 levels in periodontitis patients might explain the altered immune response.28 IL-10 may play a pivotal role in regulating the immune response in T2D patients with periodontitis.27,30 The relationship between IL-10 and oral diseases in diabetes mellitus patients revealed a complex interplay between immune regulation and disease progression.30 Deficiency in IL-10 expression can increase the inflammatory response to microbes and lead to the development of autoimmune diseases. Increased levels of IL-10 can trigger apoptosis in response to infection. In addition, increased IL-10 signaling can inhibit the production of pro-inflammatory cytokines and modulate immune function by preventing the maturation of macrophages and dendritic cells, thereby limiting co-stimulation, antigen presentation, and chemokine secretion capacity.31
The review’s limitations include the possibility that relevant articles meeting the review’s aims may have been missed in the database search or that full papers do not exist. This review provides basic data and can serve as a starting point for further research on immunotherapy as a potential therapy for DM patients with oral manifestations, targeting IL-10 modulation. New research opportunities related to the value of IL-10 in DM patients with oral diseases including xerostomia, geographic tongue, dental caries, sialosis, oral ulcer, oral lichen planus, dysgeusia, and burning mouth syndrome are unlikely to have been conducted, and there are no publications related to these results.
Conclusion
This review presents conflicting findings on the levels of IL-10 in diabetic patients with oral diseases. Four studies suggest higher IL-10 levels in these patients compared to the control group, while seven studies indicate the opposite, that IL-10 levels are lower. It is important to note that IL-10 levels can vary among diabetic patients, with or without oral disease, and may present as either lower or higher.
Acknowledgments
The authors would like to express their sincere appreciation to Dr. Ahmedz Widiasta (a pediatric nephrology specialist) for his invaluable and outstanding contribution to the review process. The authors gratefully acknowledge funding support from the directorate of research and community service at Universitas Padjadjaran.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Alam S, Hasan MK, Neaz S, Hussain N, Hossain MF, Rahman T. Diabetes mellitus: insights from epidemiology, biochemistry, risk factors, diagnosis, complications and comprehensive management. Diabetology. 2021;2(2):36–50. doi:10.3390/diabetology2020004
2. Loscalzo J, Kasper DL, Longo DL, Fauci AS, Hauser SL, Jameson JL. Harrison’s Principles of Internal Medicine.
3. Al Shihi N, Al Rawahi A, Al Jahdhami R. Oral health knowledge, attitudes, and practices of individuals with diabetes mellitus in the Sultanate of Oman. Dubai Diabetes Endocrinol J. 2023;29(1):33–41. doi:10.1159/000529684
4. Indrahadi D, Wardana A, Pierewan AC. The prevalence of diabetes mellitus and relationship with socioeconomic status in the Indonesian population. J Gizi Klin Indones. 2021;17(3):103–112. doi:10.22146/ijcn.55003
5. IDF. Diabetes around the world in 2021. IDF Diabetes Atlas Report 2022; 2022. Available from: https://diabetesatlas.org/.
6. ElSayed NA, Aleppo G, Aroda VR, et al; ADA. Classification and diagnosis of diabetes: standards of care in diabetes — 2023. Diabetes Care. 2023;46(1):19–40. doi:10.2337/dc23-S002
7. Glick M, Greenberg M, Lockhart P, et al. Burket’s Oral Medicine. Vol. 4.
8. Ongole R, P BN. Textbook of Oral Medicine, Oral Diagnosis and Oral Radiology.
9. Neville BW, Damm DD, Allen CM, Chi AC. Color Atlas of Oral and Maxillofacial Diseases. Elsevier Inc.; 2019.
10. Ghom AG, Ghom SA. Textbook of Oral Medicine.
11. Miller C, Rhodus NL, Treister NS, Stoopler ET, Kerr AR. Little and Falace’s Dental Management of the Medically Compromised Patient. Elsevier Health Sciences; 2018; doi:10.1016/B978-0-323-28745-6.00026-0
12. Melmed S, Koenig RJ, Auchus RJ, Rosen CJ, Goldfine AB. Williams Textbook of Endocrinology.
13. Arthur C, Guyton MD, John E, Hall PD. Textbook of Medical Physiology. Elsevier; 2006.
14. Khin PP, Lee JH, Sook JH. Pancreatic beta-cell dysfunction in type 2 diabetes. Eur J Inflamm. 2023;21:1–13. doi:10.1177/1721727X231154152
15. Kumar V, Abbas AK, Aster. JC. Robbins Basic Pathology. Vol. 4.
16. Verhulst MJL, Loos BG, Gerdes VEA, Teeuw WJ. Evaluating all potential oral complications of diabetes mellitus. Front Endocrinol. 2019;10(FEB). doi:10.3389/fendo.2019.00056
17. Rayego-Mateos S, Morgado-Pascual JL, Opazo-Ríos L, et al. Pathogenic pathways and therapeutic approaches targeting inflammation in diabetic nephropathy. Int J Mol Sci. 2020;21(11):1–43. doi:10.3390/ijms21113798
18. Kapila YL. Oral health’s inextricable connection to systemic health: special populations bring to bear multimodal relationships and factors connecting periodontal disease to systemic diseases and conditions. Periodontology 2000. 2021;87(1):11–16. doi:10.1111/prd.12398
19. Borgnakke WS, Poudel P. Diabetes and oral health: summary of current scientific evidence for why transdisciplinary collaboration is needed. Front Dent Med. 2021;2(1–13). doi:10.3389/fdmed.2021.709831
20. Homagarani YM, Adlparvar K, Teimuri S, Tarrahi MJ, Nilchian F. The effect of diabetes mellitus on oral health-related quality of life: a systematic review and meta-analysis study. Front Public Health. 2023;11:1112008. doi:10.3389/fpubh.2023.1112008
21. Kane SF. The effects of oral health on systemic health. Acad Gen Dent. 2017;65(6):30–34.
22. Kumari S, Gnanasundaram N. Oral manifestations in diabetes mellitus ‑ a review. J Indian Acad Oral Med Radiol. 2021;33(4):352–356. doi:10.4103/jiaomr.jiaomr
23. Rohani B. Oral manifestations in patients with diabetes mellitus. World J Diabetes. 2019;10(9):485–489. doi:10.4239/wjd.v10.i9.485
24. Indurkar MS, Maurya AS, Indurkar S. Oral manifestations of diabetes. Clin Diabetes. 2016;34(1):54–57. doi:10.2337/diaclin.34.1.54
25. Duarte PM, Neto JBC, Casati MZ, Sallum EA, Nociti FH. Diabetes modulates gene expression in the gingival tissues of patients with chronic periodontitis. Oral Dis. 2007;13(6):594–599. doi:10.1111/j.1601-0825.2006.01348.x
26. Saraiva M, Vieira P, Garra AO. Biology and therapeutic potential of interleukin-10. J Exp Med. 2019;216(1):1–19. doi:10.1084/jem.20181961
27. Ma X. Regulation of Cytokine Gene Expression in Immunity and Diseases. Springer Nature; 2016.
28. Scully C. Oral and Maxillofacial Medicine. Elsevier; 2013; doi:10.1111/j.1601-0825.2008.01461.x
29. Slavin AJ, Maron R, Weiner HL. Mucosal administration of IL-10 enhances oral tolerance in autoimmune encephalomyelitis and diabetes. Int Immunol. 2001;13(6):825–833. doi:10.1093/intimm/13.6.825
30. Lu J, Liu J, Li L, Lan Y, Liang Y. Cytokines in type 1 diabetes: mechanisms of action and immunotherapeutic targets. Clin Transl Immunol. 2020;9(3):1–17. doi:10.1002/cti2.1122
31. Iyer SS, Cheng G. Role of interleukin 10 transcriptional regulation in inflammation and autoimmune disease. Crit Rev Immunol. 2013;32(1):23–63. doi:10.1615/CritRevImmunol.v32.i1.30
32. Berbudi A, Rahmadika N, Tjahjadi AI, Ruslami R. Type 2 diabetes and its impact on the immune system. Curr Diabetes Rev. 2020;16(5):442–449. doi:10.2174/1573399815666191024085838
33. Xu A, Zhu W, Li T, et al. Interleukin-10 gene transfer into insulin-producing β cells protects against diabetes in non-obese diabetic mice. Mol Med Rep. 2015;12(3):3881–3889. doi:10.3892/mmr.2015.3809
34. Andriankaja OM, Adatorwovor R, Kantarci A, Hasturk H, Shaddox L, Levine MA. Periodontal disease, local and systemic inflammation in Puerto Ricans with type 2 diabetes mellitus. Biomedicines. 2023;11(10):1–15. doi:10.3390/biomedicines11102770
35. Ikbal SKA, Gupta S, Tiwari V, Dhinsa G, Verma N. Association of serum interleukin-10 level with glycemic status to predict glycemic alteration with periodontitis: a cross-sectional, observational study. Contemp Clin Dent. 2023;8:11–19. doi:10.4103/ccd.ccd
36. Halimi A, Mortazavi N, Memarian A, Zahedi M, Niknejad F, Sohrabi A. The relation between serum levels of interleukin 10 and interferon ‑ gamma with oral candidiasis in type 2 diabetes mellitus patients. BMC Endocr Disord. 2022;22(1):1–6. doi:10.1186/s12902-022-01217-x
37. Liu L, Xiao Z, Ding W, et al. Relationship between microRNA expression and inflammatory factors in patients with both type 2 diabetes mellitus and periodontal disease. Am J Transl Res. 2022;14(9):6627–6637.
38. Zhang H, Zhang Y, Chen X, Li J, Zhang Z, Yu H. Effects of statins on cytokines levels in gingival crevicular fluid and saliva and on clinical periodontal parameters of middle-aged and elderly patients with type 2 diabetes mellitus. PLoS One. 2021;16:1–18. doi:10.1371/journal.pone.0244806
39. Elazazy O, Amr K, Abd El Fattah A, Abouzaid M. Evaluation of serum and gingival crevicular fluid microRNA-223, microRNA-203 and microRNA-200b expression in chronic periodontitis patients with and without diabetes type 2. Arch Oral Biol. 2021;121:104949. doi:10.1016/j.archoralbio.2020.104949
40. Rangel TP, Reis AA, Caponi L, et al. Subgingival endotoxin and lipoteichoic acid modulate cytokine production in diabetic subjects: a Case–control Study. Oral Dis. 2021;27(5):1325–1333. doi:10.1111/odi.13661
41. Kassab A, Ayed Y, Elsayed SA, et al. Glycated hemoglobin influence on periodontal status, pathogens and salivary interleukins in type II diabetic Tunisian subjects with chronic periodontitis. J Dent Sci. 2021;16(2):614–620. doi:10.1016/j.jds.2020.09.018
42. de Sousa Rabelo M, Gomes GH, Foz AM, et al. Short-term effect of non-surgical periodontal treatment on local and systemic cytokine levels: role of hyperglycemia. Cytokine. 2021;138:155360. doi:10.1016/j.cyto.2020.155360
43. Kumar PS, Monteiro MF, Dabdoub SM, et al. Subgingival host-microbial interactions in hyperglycemic individuals. J Dent Res. 2020;99(6):650–657. doi:10.1177/0022034520906842
44. Belkina AC, Azer M, Lee JJ, et al. Single-cell analysis of the periodontal immune niche in type 2 diabetes. J Dent Res. 2020;99(7):855–862. doi:10.1177/0022034520912188
45. Chinaarkatakul K, Loakhajorn K. Diabetes mellitus: a leading cause of death worldwide. Int J Curr Sci Res Rev. 2023;06(08):5640–5646. doi:10.47191/ijcsrr/V6-i8-31
46. de la Rosa García E, Mondragón Padilla A, Aranda Romo S, Bustamante Ramírez MA. Oral mucosa symptoms, signs and lesions, in end stage renal disease and non-end stage renal disease diabetic patients. Med Oral Patol Oral Cir Bucal. 2006;11(6):E467–E673.
47. Elad S, Zadik Y, Caton JG, Epstein JB. Oral mucosal changes associated with primary diseases in other body systems. Periodontol 2000. 2019;80(1):28–48. doi:10.1111/prd.12265
48. Sanjeeta N, Sivapathasundharam B, Nandini DB. Oral lesions and periodontal status in diabetics and non ‑ diabetics: a hospital based study. J Oral Maxillofac Pathol. 2022;26(419):1–6. doi:10.4103/jomfp.jomfp
49. Miguel Á, Ramos-Garcia P. State of evidence on oral health problems in diabetic patients: a critical review of the literature. J Clin Med Rev. 2021;10(22):5383.
50. Sun J, Chen T, Zhao B, et al. Acceleration of oral wound healing under diabetes mellitus conditions using bioadhesive hydrogel. ACS Appl Mater Interfaces Against. 2023;15(1):416–431. doi:10.1021/acsami.2c17424
51. Tsalamandris S, Antonopoulos AS, Oikonomou E, et al. The role of inflammation in diabetes: current concepts and future perspectives. Eur Cardiol Rev. 2019;14(1):50–59. doi:10.15420/ecr.2018.33.1
52. Lontchi-Yimagou E, Sobngwi E, Matsha TE, Kengne AP. Diabetes mellitus and inflammation. Curr Diab Rep. 2013;13(3):435–444. doi:10.1007/s11892-013-0375-y
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Serum Uric Acid to High‑density Lipoprotein Cholesterol Ratio is Associated with Visceral Fat in Patients with Type 2 Diabetes
Sun H, Su H, Zheng R, Liu C, Wang Y, Fang C
Diabetes, Metabolic Syndrome and Obesity 2023, 16:959-967
Published Date: 4 April 2023
Association Between Thymosin β4 and Coronary Arterial Lesions in Children with Kawasaki Disease
Wu J, Yang P, Zhang J, Chen Z, Wei Y, Su Y, Yi Q
Journal of Inflammation Research 2025, 18:8755-8765
Published Date: 3 July 2025
Clinical Outcomes and Complications of Basal, Bolus, and Combination Insulin Regimens in Type 2 Diabetes Mellitus: Evidence from Published Case Reports
Natsir RM, Halimah E, Diantini A, Levita J
Diabetes, Metabolic Syndrome and Obesity 2025, 18:3215-3236
Published Date: 3 September 2025