Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Exploring Impact of Multidisciplinary Care on Patient Activation in Saudi Rheumatoid Arthritis Patients: A Cross-Sectional Survey—Extended Results from the COPARA National Project
Authors Almalag HM ![]() , Al Juffali L
, Al Juffali L ![]() , Alshehri MM, Altokhais NA, Aljanobi GA
, Alshehri MM, Altokhais NA, Aljanobi GA ![]() , El Dessougi MI, AlHarthi A
, El Dessougi MI, AlHarthi A ![]() , Attar SM, Bahlas SM, Alfurayj AS, Alazmi MS, Asiri AM
, Attar SM, Bahlas SM, Alfurayj AS, Alazmi MS, Asiri AM ![]() , AlOmair MM, Omair MA
, AlOmair MM, Omair MA ![]()
Received 16 September 2023
Accepted for publication 2 November 2023
Published 14 November 2023 Volume 2023:16 Pages 3455—3463
DOI https://doi.org/10.2147/JMDH.S436826
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Haya M Almalag,1 Lobna Al Juffali,1 Maha M Alshehri,2 Nouf A Altokhais,2 Ghada A Aljanobi,3 Maha I El Dessougi,4 Amal AlHarthi,4 Suzan M Attar,5 Sami M Bahlas,5 Abdullah S Alfurayj,6 Mansour S Alazmi,7 Alhussain M Asiri,8 Mohammed M AlOmair,8 Mohammed A Omair9
1Department of Clinical Pharmacy, College of Pharmacy, King Saud University, Riyadh, Saudi Arabia; 2College of Pharmacy, King Saud University, Riyadh, Saudi Arabia; 3Rheumatology Unit, Department of Medicine, Johns Hopkins Aramco Healthcare, Dhahran, Saudi Arabia; 4Rheumatology Unit, Department of Medicine, Security Forces Hospital, Riyadh, Saudi Arabia; 5Rheumatology Unit, Department of Medicine, King Abdulaziz University, Jeddah, Saudi Arabia; 6Rheumatology Unit, Department of Medicine, Buraidah Central Hospital, Buraidah, Saudi Arabia; 7Rheumatology Unit, Department of Medicine, Prince Mohammed Medical City, Sakaka-Aljouf, Saudi Arabia; 8Rheumatology Unit, Department of Medicine, Aseer Central Hospital, Abha, Saudi Arabia; 9Rheumatology Unit, Department of Medicine, King Saud University, Riyadh, Saudi Arabia
Correspondence: Haya M Almalag, Department of Clinical Pharmacy, College of Pharmacy, King Saud University, Riyadh, Saudi Arabia, Email [email protected]
Introduction: Multidisciplinary setting in healthcare provide positive patient outcomes.
Objective: To evaluate the impact of specialized rheumatology clinics (multidisciplinary settings) on the activation and engagement of rheumatoid arthritis (RA) patients.
Material and Methods: This cross-sectional survey assessed patient activation using the patient activation measure-13. Participants attending Specialized Rheumatology Clinics (SRC multidisciplinary clinics) were compared with age- and sex-matched patients attending Standard of Care (SOC). The study was observational in nature, assessing several demographic and therapeutic options and their relation to the clinical setting and patient activation.
Results: This study included 117 SRC matched RA patients with 117 SOC. The majority of the included patients were female (n=211, 90.2%), > 40 years of age (n=177, 75.6%), and had intermediate-to-high education (n=147, 62.8%). Patients in the SRC were also more likely to have activation levels 3 and 4 with an odds ratio of 3.194 (95% confidence interval [CI] 1.835– 5.562, p< 0.001). In addition, SRC participants were more likely to be in levels 3 and 4 activation, even after adjustment for confounding variables, with an adjusted odds ratio of 2.401 (95% CI 1.121– 4.758, p=0.012) and 2.175 (95% CI 1.127– 4.196, p=0.020), respectively.
Conclusion: Establishing SRC for RA patients seems to have a positive impact on patient activation and engagement and adds to the previously explored benefits of multidisciplinary care in chronic disease management.
Keywords: patient activation, multidisciplinary care, rheumatoid arthritis
Introduction
In healthcare, multidisciplinary teamwork has been adopted for high-quality disease management. A multidisciplinary team is a group of diverse clinicians who communicate with each other to care for a specific group of patients.1 Pharmacists and other healthcare providers are integral parts of this team, and multidisciplinary settings have been documented to improve patient outcomes.2 The role of multidisciplinary care has been defined in multiple settings including cancer, COVID-19, and geriatric ambulatory care.1–4 However, until this report was written, the role of multidisciplinary care in rheumatology had rarely been explored. Rheumatoid arthritis (RA) is chronic complex illness and RA patients can benefit from such collaborative work.
Considering the success of care provided by a multidisciplinary team, there is a guarantee of advancement in the management of rheumatic illnesses. Patients with inflammatory conditions require appropriate drug management to reduce disease progression and improve their quality of life. A specialized rheumatology clinic was established at the study center in 2017. This setting has the advantage of involving multiple disciplines other than well-known nursing and physician collaboration.5 They include clinical pharmacists, dietitians, ultrasound specialists, nurses, and social workers. As an example of interaction in this team-based setting, the clinical pharmacist can provide advice for medication use and adherence and contribute to the prescribing physician in the choice and dosing of anti-rheumatic medications. Another key role is the management of coexisting diseases in rheumatic patients, which commonly include diabetes, hypertension, dyslipidemia, and bronchial asthma.6 In addition, all team members spent time with the patient and involved in discussion with the patient on their care and wellbeing.
With the shift of healthcare management to patient centered approach, the impact of patient activation on therapy is highly expected.7 Patient activation is a parameter that captures patient engagement in his or her therapy. This parameter was first quantified by patient activation measure 22 by Hibbard in 2004.8 It was then reduced to PAM-13 to facilitate ease of application.9 Since its development, the 13 item tool was extensively used in research and was correlated with positive patient reported outcomes in several settings.10–13 The first study that highlighted the impact of clinical setting and patient activation was our research team, in the published paper by Al juffali, et al, recently in 2022.14 Given the limitation of borderline significance due to the inadequate recruitment related to the COVID-19 pandemic, the research team decided to recruit more participants with clinical setting as a major comparison for this work, and hence the aim of this project. The project is part of the Compliance and Patient Activation in Rheumatoid Arthritis (COPARA) study. This is a large multicenter cohort study involving more than 1000 adult patients with confirmed rheumatoid arthritis.
Materials and Methods
Study Design
This study was part of a national survey on patient activation, compliance, and RA in Saudi Arabia.14,15 This study was a cross-sectional comparison between patients in specialized rheumatology clinics (SRC) and age- and sex-matched patients attending the standard of care setting (SOC). The Compliance and Patient Activation in Rheumatoid Arthritis (COPARA) project is observational in nature and guided by the STrengthening of Observational Studies in Epidemiology (STROBE) checklist.16
Settings
This study included participants with confirmed RA diagnoses across multiple Saudi centers. Participants attending the SRC at King Saud University Medical City (previously known as King Khalid University Hospital) in Riyadh were compared with age- and sex-matched participants attending other SOC throughout the kingdom. The SOC centers included the following: Security Forces Hospital, Riyadh; King Abdulaziz University Hospital, Jeddah; Prince Mohammed Medical City, Al-Jouf; Qatif Central Hospital, Qatif; Buraidah Central Hospital, Buraidah; Aseer Central Hospital, Abha; and the Charitable Association for Rheumatic Diseases database. All centers are government tertiary referral centers (free healthcare system), except for the charitable association, which provides support to patients with rheumatic diseases across the kingdom. SRC is a multidisciplinary setting where patients are examined by several health care providers. First, the patient is attended to by a physician, who then refers the patient to a clinical pharmacist, and then to a social worker. Patients will get a joint ultrasound taken, if needed. The patient visits and referrals are facilitated and coordinated by the nursing staff of the SRC. For patients receiving SOC, the patient is attended to by a physician only. The SRC setting application depends on feasibility per institution setting, thus it was only applied in KSUMC.
Participants
All adult participants attending SRC or SOC with a confirmed RA diagnosis were included. The RA diagnosis in all involved centers was based on the American College of Rheumatology 2010 diagnostic criteria.17 Participants younger than 18 years of age or those unable to answer the survey questions owing to mental incapability were excluded. Recruitment in all centers began in November 2019 and continued until 2021, with plans resumed in 2023 with the inclusion of other rheumatic disorders and amendment of the IRB. A predesigned online form was sent to the participants after obtaining electronic consent, either during clinic visits or through phone, in which numbers were obtained from the Charitable Association for Rheumatic Diseases database. A member of the research team was available during the survey to assess technical difficulties.
Variables
Pre-designed Google Forms collected the following variables: demographic characteristics, socioeconomic characteristics, and medication received. The primary outcome variable was patient activation, which was assessed using the Arabic version of the PAM-13. The research team was aware that the participants attended rheumatology clinics at King Saud University Medical City, where ambulatory multidisciplinary care is provided.
Data Source and Measurements
A predesigned Google Form was developed to gather the required information. For assessing patient activation and engagement, PAM-13 survey was used. A license to use the survey was obtained (number: 1570198456–1601820856). The PAM-13 was originally developed as a 22-item survey, which was then reduced to a 13-item survey.8,9 The measure consists of 13-Likert scale items (five point Likert scale), in which participants rate their experiences. The items are then summed to produce a score from 0 to 100 with higher scores indicating better activation. The total score can be categorized into four levels (levels 1, 2, 3, and 4), in which levels 3 and 4 represent higher activation; level 1 is a total score of <47; level 2, 47.1 to 55.1; level 3, 55.2 to 67.0; and level 4, 67.1 or above. The items of patient activation depend on several elements that affect behavior. Level 1 (represented by PAM1 and PAM2 items), covers the patient’s belief that their role is important. Level 2 (represented by PAM3-8 items) covers the patient knowledge and confidence to act. Level 3 (represented by PA9-11, reflects the ability to take action) and finally level 4 (PAM12 and 13) indicating staying on course and taking action even under stress (Supplementary Material 1 for behavior classification base on PAM level).
Bias
Consecutive patients across multiple centers were recruited for this study. Only the patients with complete data were included in the analysis. In addition, to eliminate confounders, the SRC participants were matched with similar participants from the SOC. The matching was performed according to age and sex.
Quantitative Variables and Statistical Methods
Data were coded and entered into the statistical analysis software IBM SPSS Statistics for Windows, Version 28.0. (Armonk, NY, USA).18 Categorical variables were presented as numbers and percentages. Differences between categorical variables were assessed using the chi-squared test. Binary logistic regression was used to predict the effect of different demographics on the activation levels of 3 or 4. In addition, the odds of being in SRC versus SOC were predicted using binary logistic regression.
Ethical Considerations
The study protocol was approved by the institutional review board of King Saud University (IRB number: E-19-4364). All participants agreed to be included in the study and provided electronic consent. No identifiers were collected to ensure anonymity of the survey data. All the participants provided electronic consent and voluntarily agreed to participate in the study. No identifiable patient data was used, thereby guaranteeing complete patient confidentiality. The study complied with the ethical guidelines of the Declaration of Helsinki.
Results
The ongoing COPARA study has recruited up to 1438 patients. A total of 117 participants from the SRC setting were matched with 117 participants from the larger cohort of 1438 patients with confirmed RA diagnosis. The majority of the included patients were female (n=211, 90.2%), >40 years of age (n=177, 75.6%), and had intermediate-to-high education (n=147, 62.8%). The majority did not smoke (n=218, 93.2%) and had a low-to-intermediate income (n=189, 80.8%). Most participants did not work (n=164, 70.1%), lived with their family (n=225, 96.2%), and approximately half did not have other comorbidities (n=128, 54.7%) (Table 1). Regarding the characteristics of participants with RA, the majority had established RA (n=212, 90.6%) and were using conventional synthetic disease-modifying anti-rheumatic drugs (csDMARDs) (n=158, 67.5%). In terms of patient activation, most participants had activation levels of 3 and 4 (n=145, 62.0%). Baseline demographics and disease characteristics are presented in Table 1.
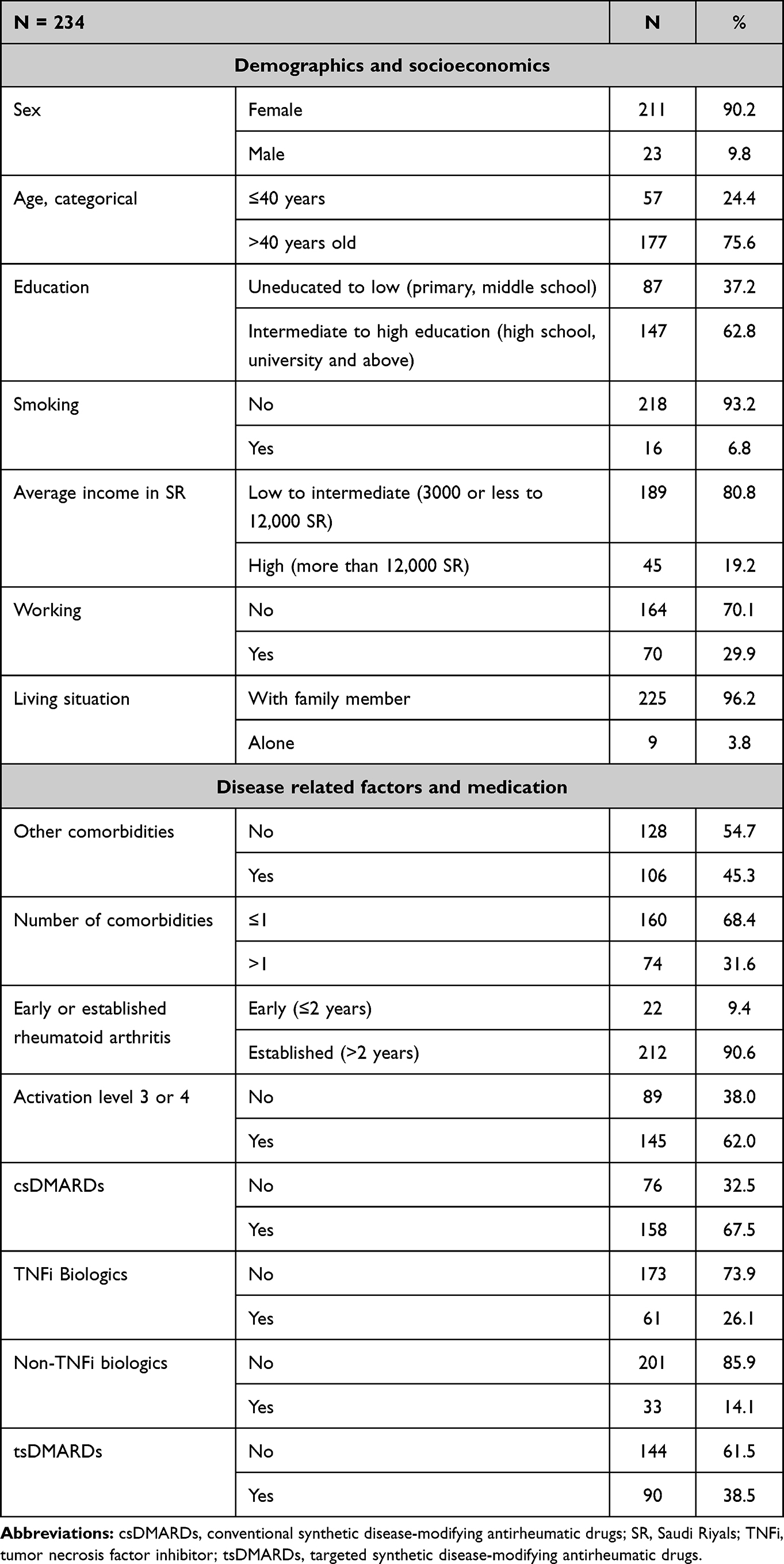 |
Table 1 Demographical Characteristics of Participants |
Demographic factors that were commonly seen in participants attending SRC were their nonsmoking status (odds ratio [OR] 0.059, 95% confidence interval [CI] 0.008–0.452, p=0.006) and fewer comorbidities (OR 0.447, 95% CI 0.253–0.788, p=0.005) with established RA (OR 11.856, 95% CI 2.703–52.001, p=0.001). SRC patients were also more likely to have activation levels 3 and 4 (OR 3.194, 95% CI 1.835–5.562, p<0.001). Patients were also less likely to be using csDMARDs (OR 0.295, 95% CI 0.165–0.530, p<0.001) and more likely to be on targeted synthetic disease-modifying anti-rheumatic drugs (tsDMARDs) (OR 1.929, 95% CI 1.129–3.290, p=0.016) (Table 2).
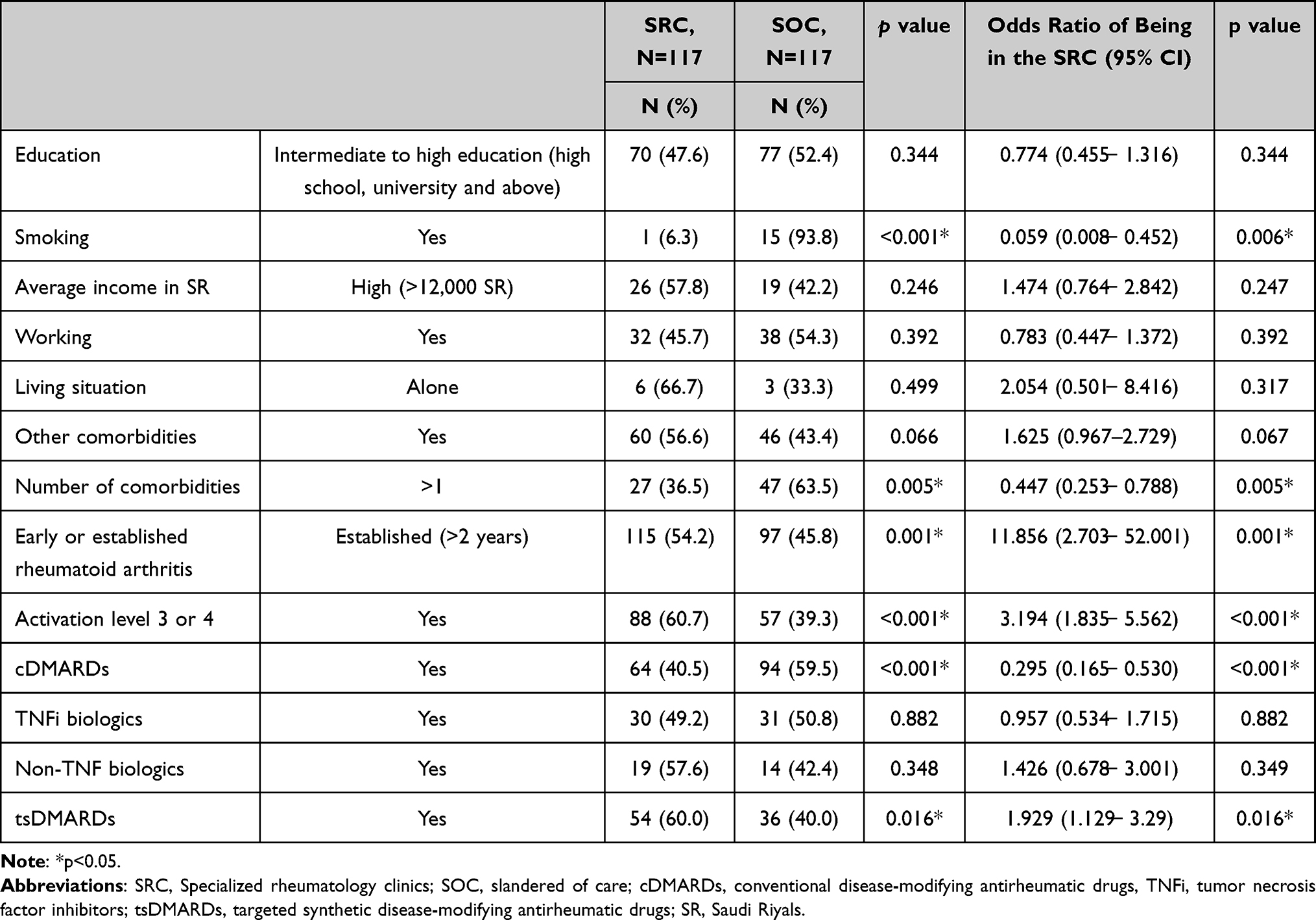 |
Table 2 Demographics and Patient Characteristics of Participants in SRC with p value of Difference from SOC |
Figure 1 illustrates the difference in patient activation levels between the two types of clinics. In the SRC setting, the majority of patients were categorized at activation levels 3 and 4, while in the SOC setting, patients were predominantly at activation level 2. To evaluate the items of patient activation, the SRC participants had a higher agreement with responses related to activation levels 1 and 2, indicating that they agreed more on the items related to the patient role and had sufficient confidence and knowledge to act (Figure 2). However, in terms of higher levels of activation (levels 3 and 4), the SRC and SOC groups were very similar to each other (Figure 3).
 |
Figure 1 Differences in patient activation levels stratified by clinic type. Abbreviations: SOR, Standard of care; SRC, Specialized rheumatology clinics. |
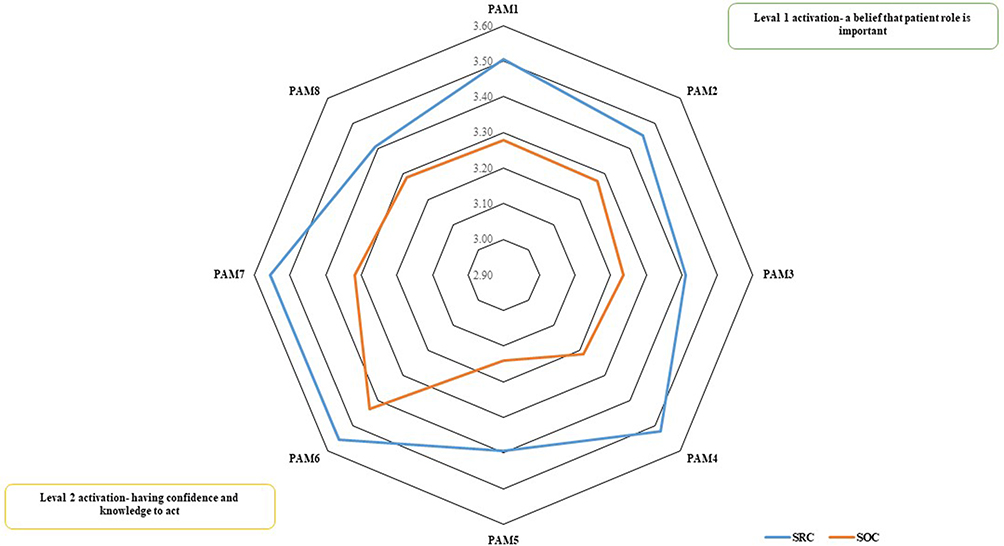 |
Figure 2 Activation levels (items of level 1 and level 2) and average of participants agreement according to clinic type as specialized rheumatology clinics (SRC) or standard of care (SOC). |
 |
Figure 3 Activation levels (items of level 3 and level 4) and average of participants agreement according to clinic type as specialized rheumatology clinics (SRC) or standard of care (SOC). |
Participants with level 2 activation were less likely to be in the SRC group (OR 0.186, 95% CI 0.092–0.380, p<0.001). This remained the same even after adjusting for confounding variables (adjusted odds ratio [AOR] 1.405, 95% CI 0.572–3.455, p=0.458). Patients with activation level 3 were more likely to be in SRC setting (OR 1.763, 95% CI 1.004–3.097, p=0.048), and the significance of this association was higher after adjustment (AOR 2.401, 1.121–4.758. p=0.012). Similarly, SRC patients with activation level 4 had increased odds of being in the SRC setting (OR 1.978, 95% CI 1.129–3.495, p=0.017), and the significance of this association was increased after adjustment (AOR 2.175, 95% CI 1.127–4.196, p=0.020) (Table 3).
 |
Table 3 Activation Level per Clinic with Unadjusted and Adjusted Odds Ratio |
Discussion
Patient activation measures are associated with positive patient reported outcomes in multiple clinical and non-clinical settings.10–13 Generally, in Saudi Arabia, patient activation was explored and was higher than other populations in different countries.14 In the current work, participants who received multidisciplinary care showed better activation. A limited number of confounding variables were also included. Although patients showed significant level 4 activation, some elements of their behavior still required improvement, which needs to be addressed in qualitative studies. Additionally, the impact of the unique culture of the population needs to be explored. Participants attending the SRC had sufficient knowledge and confidence to act and believed that the patient’s role was important. However, it should be noted that there was inconsistency within the activation levels 3 or 4 items, despite the participants having an overall level 3 or 4 activation score. This finding highlights that there is still considerable work to be done in empowering patients to take charge of their own health management.
Models of multidisciplinary care in rheumatology have been discussed previously.19 Multidisciplinary care for RA patients has been advocated in international guidelines for management excellence.20 It provides an opportunity for comprehensive disease management and may positively impact patient-reported outcomes such as quality of life.21 The ideal multidisciplinary care setting varies across institutions and strongly depends on the facilities and resources available in each setting.19 Being linked to an academic institution, the study site had the advantage of developing a multidisciplinary care model. It also provides an ideal location for student training with the best available models of care. The primary goal of the multidisciplinary care model is to provide optimal patient management.20 The availability of this option for patients with chronic conditions is highly important, especially with rapid advances in therapeutic options. In previously published literature, the model was linked to patient satisfaction but never to activation and engagement.22
The patient attending SRC had a documented belief that the patient’s role was important, had the confidence to act, was able to take action, and could stay on course even under stress. Having all these characteristics will enable patients to achieve better disease control by increasing adherence and reducing disease activity.23 In terms of cost, a multidisciplinary setting may increase the economic burden owing to the number of individuals involved. By contrast, multidisciplinary approaches may provide economic benefits.24 It should be emphasized that multidisciplinary care may differ across institutions, and a direct economic evaluation is needed.
To our knowledge, this is the first study to address patient activation from a multidisciplinary care perspective. While our previous work touched upon this topic, it was not the primary objective. The limitations were its cross-sectional nature, possible unknown confounders, and limited number of participants. Additionally, implementing multidisciplinary care is not an easy task; it requires human power and resources that may not be easily available in all the centers involved.
In conclusion, the SRC model showed better patient activation after assessment by PAM-13. These findings could provide pilot evidence on how multidisciplinary care might impact not only disease management but also patient activation and engagement. However, SRC are not cost-effective. Hence, economic evaluation of the use of these clinics over a long term is warranted.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are not publicly available but are available from the corresponding author upon reasonable request.
Ethics Approval
The study protocol was approved by the institutional review board of King Saud University (IRB number: E-19-4364).
Informed Consent
Participants provided electronic consent and agreed to participate voluntarily.
Acknowledgment
The authors would like to thank the Charitable Association for Rheumatic Diseases, patients, and coordinators who helped complete this study. The authors would like to thank Researchers Supporting Project number (RSP2023R209), King Saud University, Riyadh, Saudi Arabia, for funding this project.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Taberna M, Gil Moncayo F, Jané-Salas E, et al. The multidisciplinary team (MDT) approach and quality of care. Front Oncol. 2020;10(85). doi:10.3389/fonc.2020.00085
2. Wagner EH. The role of patient care teams in chronic disease management. BMJ. 2000;320(7234):569–572. doi:10.1136/bmj.320.7234.569
3. Baldwin L-M, Inui TS, Stenkamp S. The effect of coordinated, multidisciplinary ambulatory care on service use, charges, quality of care and patient satisfaction in the elderly. J Community Health. 1993;18(2):95–108. doi:10.1007/BF01324418
4. Coffey JD, Christopherson LA, Glasgow AE, et al. Implementation of a multisite, interdisciplinary remote patient monitoring program for ambulatory management of patients with COVID-19. Npj Digit Med. 2021;4(1):123. doi:10.1038/s41746-021-00490-9
5. Apantaku G, Aguiar M, Kaal KJ, Munro S, Teo M, Harrison M. Understanding multidisciplinary care for people with rheumatic disease in British Columbia, Canada, through patients, nurses and physicians voices: a qualitative policy evaluation. BMC Health Serv Res. 2021;21(1):1148. doi:10.1186/s12913-021-07138-0
6. Taylor PC, Atzeni F, Balsa A, Gossec L, Müller-Ladner U, Pope J. The key comorbidities in patients with rheumatoid arthritis: a narrative review. J Clin Med. 2021;10(3):509. doi:10.3390/jcm10030509
7. Rutten GEHM, Van Vugt H, de Koning E. Person-centered diabetes care and patient activation in people with type 2 diabetes. BMJ Open Diabetes Res Care. 2020;8(2):e001926. doi:10.1136/bmjdrc-2020-001926
8. Hibbard JH, Stockard J, Mahoney ER, Tusler M. Development of the patient activation measure (PAM): conceptualizing and measuring activation in patients and consumers. Health Serv Res. 2004;39(4 Pt 1):1005–1026. doi:10.1111/j.1475-6773.2004.00269.x
9. Hibbard JH, Mahoney ER, Stockard J, Tusler M. Development and testing of a short form of the patient activation measure. Health Serv Res. 2005;40(6 Pt 1):1918–1930. doi:10.1111/j.1475-6773.2005.00438.x
10. Harvey L, Fowles J, Xi M, Terry P. When activation changes, what else changes? The relationship between change in patient activation measure (PAM) and employees’ health status and health behaviors. Patient Educ Couns. 2012;88(2):338–343. doi:10.1016/j.pec.2012.02.005
11. Jones B, Hunt A, Hewlett S, Harcourt D, Dures E. Rheumatology patients’ perceptions of patient activation and the Patient Activation Measure: a qualitative interview study. Musculoskeletal Care. 2022;20(1):74–85. doi:10.1002/msc.1555
12. Ngooi B, Packer T, Kephart G, et al. Validation of the patient activation measure (PAM-13) among adults with cardiac conditions in Singapore. ?quality Life Res. 2017;26(4):1071–1080. doi:10.1007/s11136-016-1412-5
13. McCabe PJ, Stuart-Mullen LG, McLeod CJ, et al. Patient activation for self-management is associated with health status in patients with atrial fibrillation. Patient Prefer Adherence. 2018;12:1907–1916. doi:10.2147/PPA.S172970
14. Al Juffali L, Almalag HM, Alswyan N, et al. The Patient activation measure in patients with rheumatoid arthritis: a systematic review and cross-sectional interview-based survey. Patient Prefer Adherence. 2022;16:2845–2865. doi:10.2147/PPA.S379197
15. Omair MA, Alshehri MM, Altokhais NA, et al. Exploring factors influencing medication compliance in Saudi rheumatoid arthritis patients: a nationwide cross-sectional survey - results from the COPARA study. Patient Prefer Adherence. 2022;16:1105–1114. doi:10.2147/PPA.S363477
16. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol. 2008;61(4):344–349. doi:10.1016/j.jclinepi.2007.11.008
17. Aletaha D, Neogi T, Silman AJ, et al. 2010 Rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum. 2010;62(9):2569–2581. doi:10.1002/art.27584
18. Corp IBM. IBM SPSS Statistics for Windows, Version 28.0. Armonk, NY: IBM Corp; 2013.
19. Bearne LM, Byrne A-M, Segrave H, White CM. Multidisciplinary team care for people with rheumatoid arthritis: a systematic review and meta-analysis. Rheumatol Int. 2016;36(3):311–324. doi:10.1007/s00296-015-3380-4
20. National Institute for Health and Care Excellence. Rheumatoid Arthritis in Adults: Diagnosis and Management. London: National Institute for Health and Care Excellence (NICE); 2018. Available from Https://Www.Ncbi.Nlm.Nih.Gov/Books/NBK519103/.
21. Vliet Vlieland TPM, Hazes JMW. Efficacy of multidisciplinary team care programs in rheumatoid arthritis. Semin Arthritis Rheum. 1997;27(2):110–122. doi:10.1016/S0049-0172(97)80011-X
22. Will KK, Johnson ML, Lamb G. Team-based care and patient satisfaction in the hospital setting: a systematic review. J Patient Cent Res Rev. 2019;29(6):158–171. doi:10.17294/2330-0698.1695
23. Hibbard JH, Greene J, Sacks RM, Overton V, Parrotta C. Improving population health management strategies: identifying patients who are more likely to be users of avoidable costly care and those more likely to develop a new chronic disease. Heal Serv Res. 2017;52(4):1297–1309. doi:10.1111/1475-6773.12545
24. Hall J, Julia Kaal K, Lee J, Duncan R, Tsao N, Harrison M. Patient satisfaction and costs of multidisciplinary models of care in rheumatology: a review of the recent literature. Curr Rheumatol Rep. 2018;20(4):19. doi:10.1007/s11926-018-0727-3
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.