Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Exploring Goals and Functional Changes in Reablement for People with Fractures and People with Dizziness and Balance Problems
Authors Licina S ![]() , Kjeken I, Førland O
, Kjeken I, Førland O ![]() , Langeland E, Tuntland H
, Langeland E, Tuntland H ![]()
Received 11 May 2023
Accepted for publication 28 June 2023
Published 15 August 2023 Volume 2023:16 Pages 2323—2337
DOI https://doi.org/10.2147/JMDH.S417883
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Selma Licina,1 Ingvild Kjeken,1 Oddvar Førland,2 Eva Langeland,3 Hanne Tuntland1,4
1Department of Occupational Therapy, Prosthetics and Orthotics, OsloMet - Oslo Metropolitan University, Oslo, Norway; 2Centre for Care Research Western Norway, Western Norway University of Applied Sciences, Bergen, Norway; 3Department of Health and Caring Sciences, Western Norway University of Applied Sciences, Bergen, Norway; 4Department of Health and Functioning, Western Norway University of Applied Sciences, Bergen, Norway
Correspondence: Hanne Tuntland, Tel +47 55587839, Email [email protected]
Background: Although older people often have challenges with fractures and dizziness/balance problems, knowledge concerning the impact of reablement of people with these conditions is limited.
Aim: To explore functional changes in reablement for older home-dwelling people with fractures and dizziness/balance problems regarding 1) occupational performance and satisfaction with performance, 2) physical function and 3) health-related quality of life, and 4) which occupations they prioritize as rehabilitation goals.
Material and Methods: The sample is derived from a nationwide clinically controlled trial in Norway consisting of 149 participants with fractures and 113 with dizziness/balance problems who participated in a four to 10-week reablement program. Data were collected at baseline and at 10-week, 6-month, and 12-month follow-up and were analyzed with paired t-tests and analysis of covariance. Occupational priorities were categorized into sub-areas of occupation.
Results: Both groups had significant short-, mid-, and long-term improvements in occupational performance and satisfaction with performance. Except for balance from baseline to 12-month follow-up, the fracture group showed significant improvements in physical function and health-related quality of life at all follow-ups. The results varied more in the group with dizziness/balance problems in physical function and health-related quality of life. Functional mobility was the highest prioritized occupational sub-area in both groups.
Conclusion: The findings of this study provide extended knowledge about goals and functional changes in people with fractures and dizziness/balance problems following a reablement program.
Significance: Tailoring and individual adjustments according to diagnosis may be important in person-centered care in reablement.
Keywords: activities of daily living, Canadian occupational performance measure, diagnosis, occupation, health related quality of life, physical function, rehabilitation
Introduction
A rapidly aging population presents several socioeconomic and demographic challenges which raise concerns related to whether current healthcare services, welfare provision and economic growth are sustainable.1,2 As a solution, several western countries have evaluated and implemented reablement.3–5
In an international Delphi study by Metzelthin et al, reablement was defined as an intensive, person-centred, inclusive and holistic approach provided by an interdisciplinary team in the client’s home or local community. It is intended for everyone who can benefit from the service, irrespective of diagnosis, age, capacity or setting. Furthermore, the definition describes reablement as a goal-oriented intervention that focuses on increasing clients’ independence in daily activities.4 Additionally, reablement takes place in the client’s home or community and emphasizes enabling participation in meaningful occupations perceived as important by the client. Moreover, the intervention aims to develop health services in a more sustainable direction, reducing the need for long-term care and related costs.4
Despite a growing evidence base on reablement internationally, it is uncertain which clients receive the greatest benefit.6 Previous research of reablement has explored which occupations are frequently prioritised as rehabilitation goals by people receiving reablement7,8 and examined its effectiveness on independence in daily activities,9–11 physical function11–14 and health-related quality of life.11,15,16 However, this previous research is irrespective of diagnosis. Fractures and dizziness/balance problems are amongst the most common conditions in the older population17–20 and are a growing public health concern.21,22 Norway is a high-incidence country when it comes to osteoporotic fractures, especially hip fractures, with among the highest rates in the world.23 Hip fractures are associated with substantial functional decline and long-term institutionalization,24 as well as increased mortality and morbidity,25 and functional recovery depends on both surgical variables26 and level of frailty.27 Other fracture types such as osteoporotic vertebral fractures and upper extremity fractures, are also severe and linked to higher mortality.28 Recovery in upper extremity functioning in activities of daily living (ADLs), balance and gait, and instrumental ADL and lower extremity ADL functioning after a hip fracture, can take from several months to one year,21 and some individuals with poor premorbid health do not fully recover.24 Furthermore, dizziness and balance problems are serious and frequent symptoms among older people as well, causing a significantly higher risk of accidental falls and consequent injuries.22 For older people, falls are the main cause for hospital admission and accidental death,22 and the annual prevalence of severe dizziness that interferes with everyday functioning is 50% for people over 80 years old.29 Despite that dizziness and balance problems represent challenges in everyday life with managing and participating in daily activities,11,19,21,29,30 evidence regarding the outcomes of reablement for these two conditions is limited but is needed in order to tailor reablement to the individual’s needs.
In general, there is a paucity of studies examining reablement related to specific diagnostic groups. A few studies contribute to knowledge around the implementation, optimization and outcomes of reablement for people with dementia.31,32 The studies show that reablement is beneficial to individuals with dementia and their relatives31 and re-engages and promotes participation in everyday activities for the person with dementia.32 Another study that used the same sample as this study, found that diagnosis is a significant predictor of outcomes in reablement, where fractures predicted significantly better outcomes compared to dizziness/balance problems.30
Knowledge regarding the outcomes of reablement for people with fractures and dizziness/balance problems may be of importance for multidisciplinary healthcare working with reablement to achieve expertise and provide evidence-based intervention within an interdisciplinary team, with special consideration given to goal-setting and to design interventions that meet the individual’s needs. Although it is already known that having fractures predicts significantly better outcomes compared to dizziness/balance problems in reablement,30 it was in our interest to explore in more depth goals and functional changes in these two groups over a one-year period, in terms of implications for practice. Thus, the main purpose of this study was to explore goals and functional changes of reablement for older home-dwelling people with fractures and dizziness/balance problems regarding 1) occupational performance and satisfaction, 2) physical function and 3) health-related quality of life, and 4) which occupations they prioritize as rehabilitation goals.
Materials and Methods
Design and Participants
In this study, we use a longitudinal pretest-posttest design. The sample is a subsample derived from a nationwide clinically controlled study that aimed to assess the effects of reablement in Norway.11 The larger study was commissioned by the Norwegian Directorate of Health and consisted of 828 participants from 47 municipalities in Norway.11 Recruitment of participants took place from 1 April 2014 to 1 July 2015 through local study coordinators in each municipality, who were responsible for controlling the inclusion criteria. Home-dwelling people over the age of 18 who understood Norwegian and who had recently experienced a functional decline were eligible. People who needed institution-based rehabilitation, nursing home placement, were terminally ill or had cognitive impairments were excluded from the study. The 828 participants were distributed to either an intervention group that received a four to 10-week reablement program (n = 707) or to a control group receiving standard health care services (n = 121). The average age of the intervention group was 78 years.11
Because there were few participants in the control groups for fractures and for dizziness/balance problems (19 and 12 participants, respectively), we considered this sample too small to serve as control groups. Hence, the subsample selected in this study consisted of the 149 participants with fractures and 113 participants with dizziness/balance problems from the intervention group. Data were collected at baseline, 10-week, 6-month, and 12-month follow-up.11 Data from baseline and the three follow-ups were used to examine the short-, mid-, and long-term functional changes. The trial was approved by the Regional Committee for Medical and Health Research Ethics for Western Norway (REK West, 2014/57) and registered at ClinicalTrials.gov (24 October 2014, identifier: NCT02273934). Informed consent was provided, and all participants received information about the study’s purposes and the right to withdraw from the study.11 The procedures were conducted in accordance with the principles stated in the Declaration of Helsinki.33
Intervention
Reablement
Tailoring the intervention to the individual is an essential principle in reablement.11 The content of the reablement therefore varied among the participants, although the general features were the same.11
The municipalities’ average reablement period was 5.7 weeks.11 Throughout the reablement period, an integrated, multidisciplinary team worked together with the participant towards shared goals. The team provided intensive intervention with repeated home visits to guide and encourage participants to independently perform their daily occupations, gain confidence and relearn skills.11
The composition of the multidisciplinary teams varied across municipalities, with auxiliary nurses, physiotherapists, occupational therapists and nurses being the most frequent professions that took part in the rehabilitation in the participants’ homes.11 More details regarding the intervention can be found in the published clinical controlled trial11 or protocol.34
Data Collection
Participants’ sociodemographic characteristics (age, gender, living status and educational level), motivation for rehabilitation (1–10 point scale where 10 is highest) and major health challenges (fracture and dizziness/balance problems) were collected at baseline. Data from three different outcome measurements were included to capture the various outcomes of reablement. Data collection lasted from April 2014 until December 2015.11
Primary Outcomes
To provide a good foundation for the reablement intervention, the Canadian Occupational Performance Measure (COPM) was used as a part of the baseline assessment.11 The primary outcomes in the study were measured with COPM, which is a generic and person-centered assessment tool,35 used to describe and measure the participant’s self-perception of occupational performance (COPM-P) and satisfaction with performance (COPM-S).11 The COPM addresses three areas of occupational performance, involving self-care, productivity and leisure.35 For this reason, the reablement intervention may have included cognitive, physical, psychological and social components.11 It starts with a semi-structured interview, where the participant describes self-perceived occupational performance and satisfaction with performance over time in the nine following occupational sub-areas: personal care, functional mobility, community management (self-care), paid/unpaid work, household management play/school/education (productivity), quiet recreation, active recreation and socialization (leisure).35 The participants described which occupations were important but challenging to perform and then rated the occupations’ importance on a 10-point scale, where 10 indicates high importance. At the end of the interview, the participants could prioritize up to five of the most important occupational goals of personal importance and rate their COPM-P and COPM-S on a 10-point scale, where 10 reflects the best performance and highest satisfaction.35 These goals were included in their rehabilitation plan.11 The psychometric properties of the Norwegian version of COPM have been found to be good in older home-dwelling people receiving reablement.36 The individual minimal important change in COPM-P and COPM-S has been estimated at 3.0 and 3.2 points, respectively.36
Secondary Outcomes
The Short Physical Performance Battery (SPPB) is a screening test for functional mobility37 and was applied to determine physical function.11 The SPPB is designed to identify people at risk of functional decline and consists of the following three subtests: a standing balance test, a walking test for four meters at a regular pace, and a test of five repetitions of rising from a chair and sitting down rapidly. The length of time (seconds) spent on each subtest is reported and converted into points.37 A score of 0–4 points can be achieved in each subtest, where 4 points correspond to the best function. The different subtest scores are then added together, giving a total score ranging from 0–12 points.37 A change of 1.0 point in SPPB total score is considered a meaningful change.38 The four-meter walking test was used to calculate the preferred gait speed of the participants. A gait speed of > 1.0 meters per second (m/s) was reported as normal, and a gait speed of 0.6–1.0 m/s was considered as an initial functional decline.39 If the gait speed was < 0.6 m/s, it was interpreted as an indication of frailty that could lead to possible consequences such as falls, functional disability and hospitalization.39 The threshold for a meaningful change in gait speed is 0.1 m/s.40 A systematic review including individual studies conducted on older home-dwelling people concluded that SPPB shows adequate validity, reliability and responsiveness.41
Health-related quality of life (HRQoL) was measured with the European Quality of Life Scale (EQ-5D), which consists of two parts: the EQ-5D-5L index and the EQ-5D Visual Analogue Scale (VAS).42 The EQ-5D-5L index is a questionnaire comprising the following five domains: mobility, personal care, usual activities, pain/discomfort and anxiety/depression. The five domains are scored on an ordinal scale of 1–5 (1 = no problems, 5 = severe problems). EQ-5D (VAS) indicates how the participants evaluated their current health status (health today) on a scale of 0–100, where a higher score reflects a better health status.42 A structured review consisting of individual studies that included older adults concluded that there is satisfactory evidence regarding EQ-5D and its reliability, validity and responsiveness.43
Statistical Analysis
Descriptive statistics of the sample’s sociodemographic and clinical characteristics at baseline are reported as means and standard deviations or as frequency counts and percentages. Independent t-tests, Mann–Whitney U-tests and the chi-square test for proportions were used to explore differences between the two groups at baseline. The probability values are reported two-tailed and considered statistically significant at p < 0.05.
Paired t-tests were performed to analyze changes in mean scores in each group in COPM-P, COPM-S, physical function and health-related quality of life, from baseline to 10-week, baseline to 6-month, and baseline to 12-month follow-up. The strength of changes (effect sizes) was reported with Cohen’s d and mean differences with 95% confidence interval (CI). According to Cohen’s guidelines, d = 0.2 is considered a small effect, d = 0.5 a medium effect and d = 0.8 a large effect size.44
One-way between-group analyses of covariance (ANCOVA) was conducted to explore differences between the two groups in COPM-P and COPM-S scores at 10-week, 6-month, and 12-month follow-up while adjusting for confounders such as baseline scores of COPM-P, COPM-S, motivation, gait speed, SPPB total score, EQ-5D health today, age and gender.
Participants’ prioritized occupations were categorized into the nine sub-areas of occupations in the COPM form.35 Items addressing issues other than occupations were excluded from the analysis to better align the goals with occupational performance. The numbers of occupational priorities in each group were reported with frequency counts, percentages and means.
No power calculations have been conducted in this sub-sample. The main study conducted power calculations to determine the required sample size.11 A statistician was involved in these analyses. Due to frail participants, the estimates showed a need for at least 400 participants in the intervention group and 107 participants in the control group.11 Based on these estimates, the numbers of participants in the control groups for fractures (19) and dizziness/balance problems (12) were too small to be included in the analyses conducted in this study.
All statistical analyses were performed using IBM SPSS version 27.45
Results
A flow diagram of participants in each group is outlined in Figure 1. Dropout rates at 10-week, 6-month, and 12-month follow-up were 10.7%, 4.7% and 39.6% respectively in the fracture group and 18.6%, 5.3% and 35.4% respectively in the dizziness/balance problems group. The most prominent reason for dropout was that the study was terminated before many participants completed the 12-month follow-up. Other reasons for dropout were poor health, death, placement in a temporary or permanent care facility or because they could no longer bear to participate.
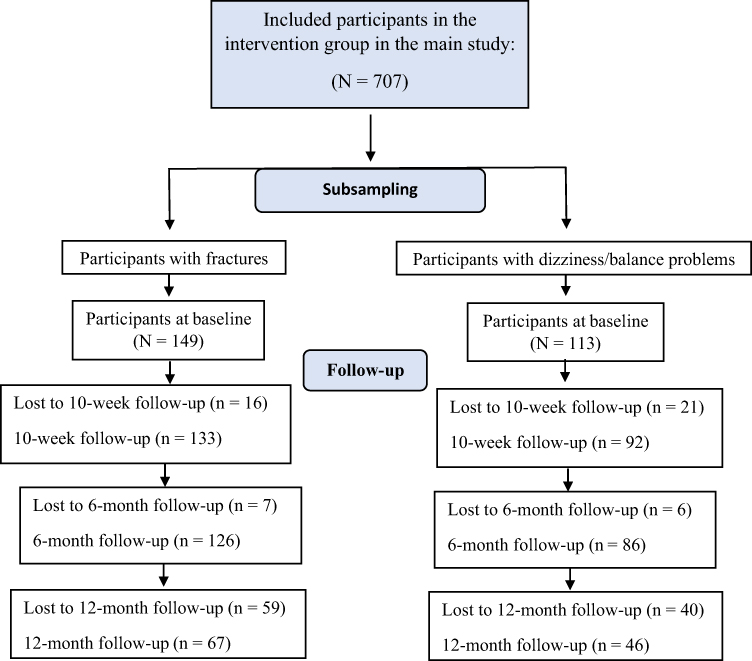 |
Figure 1 Flow chart of the participants at three follow-ups. |
The fracture group consisted of participants from 34 municipalities and the dizziness/balance problems group of participants from 27 municipalities. The baseline characteristics are presented separately for each group in Table 1. The average age (SD) of the fracture group and the dizziness/balance problems group was 80 (9.2) and 79 (11.4) years, respectively, indicating a sample of mostly older people. The majority of the sample was female, but this number was significantly higher in the fracture group (p = < 0.001). According to the SPPB-manual,39 the mean gait speed of this sample (0.46 m/s) indicated a frail sample.
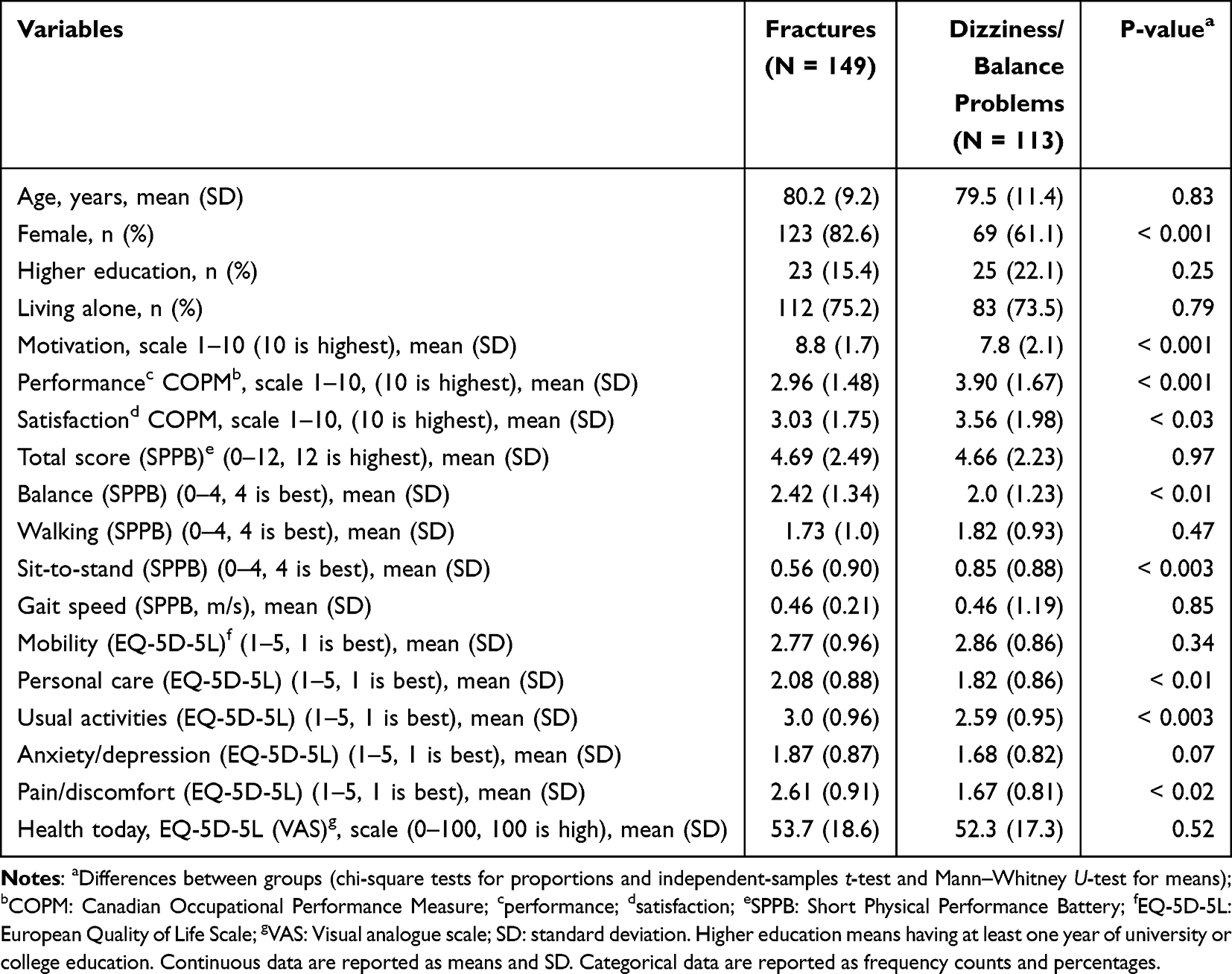 |
Table 1 Participant Characteristics at Baseline |
Participants with dizziness/balance problems had a significantly better baseline score than the fracture group on COPM-P score (p = < 0.001), COPM-S score (p = < 0.03) and SPPB sit-to-stand (p = < 0.003), whereas participants in the fracture group were slightly more motivated (p = 0.001) and had more pain/discomfort (p = < 0.02) than the group with dizziness/balance problems. They also had a significantly better score than the dizziness/balance problems group on balance (p = < 0.01), personal care (p = < 0.01) and usual activities (p = < 0.003).
Changes in the One-Year Period
Changes in Occupational Performance and Satisfaction with Performance
Both groups had significant improvements in COPM-P and COPM-S from baseline to 10-week, baseline to 6-month, and baseline to 12-month follow-up (p = < 0.001 at all follow-ups) (Table 2). Figure 2 illustrates the trend in COPM-P and COPM-S sum scores in the two groups over time. The largest improvements were in both groups from baseline to 10 weeks follow-up. For both groups the COPM-P and COPM-S scores were higher at 12 months follow-up than at baseline, shoving the durability of the improvements. However, the improvements in the fracture group were more stable over time. The results show that there were significant differences between the groups in occupational performance (COPM-P) and in satisfaction with performance (COPM-S) in favor of the fracture group (Table 3), at 10-week, 6-month, and 12-month follow-up.
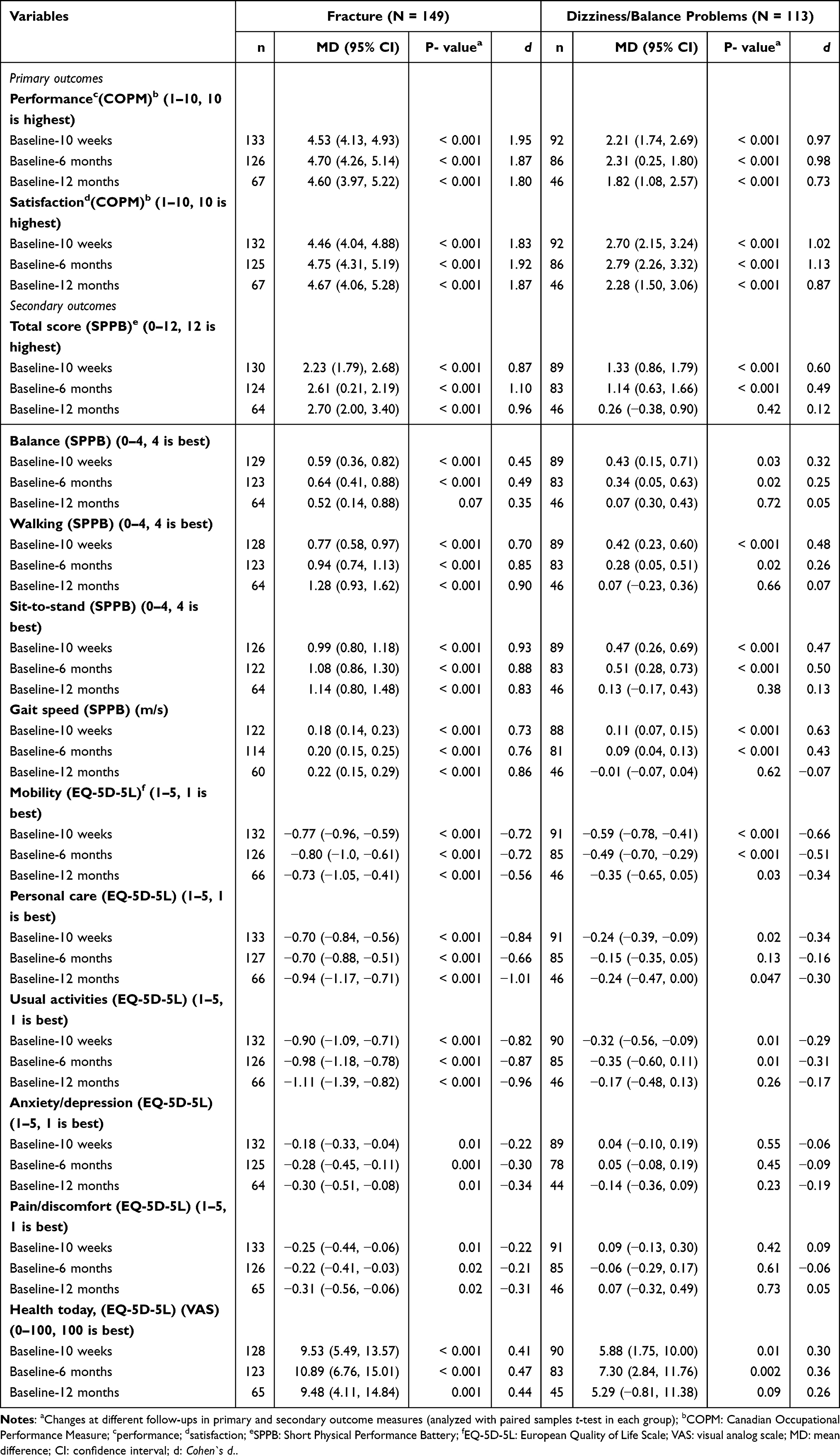 |
Table 2 Description of Changes in Mean Difference Scores in Primary and Secondary Outcome Measures from Baseline to 10-Week, Baseline to 6-Month, and Baseline to 12-Month Follow-Up in the Fracture Group and the Dizziness/Balance Problems Group, Respectively |
 |
Table 3 Description of Group Differences of COPM-P and COPM-S at 10-Week, 6-Month, and 12-Month Follow-Up, Estimated by ANCOVA |
 |
Figure 2 Changes in sum scores in occupational performance (to the left) and satisfaction with performance (to the right) in the fracture (N = 149) and dizziness/balance problem (N = 113) group over time assessed with the Canadian Occupational Performance Measure (COPM). |
In accordance with the threshold for a clinically important change in COPM-P (3.0 points) and COPM-S (3.2 points),36 the fracture group had clinically important changes at all follow-ups in both COPM-P and COPM-S, whereas there were no clinically important changes in COPM-P or COPM-S in the dizziness/balance problems group (see Table 2).
Changes in Physical Function in the Two Groups
In general, both groups had significant improvements in the SPPB subtests total score, balance, walking, sit-to-stand, and gait speed (see Table 2 for more details). However, the fracture group had better improvements in mean differences in all SPPB subtests at all follow-ups compared to the dizziness/balance problems group.
The fracture group had meaningful changes in SPPB total score and gait speed at all follow-ups. The dizziness/balance problems group only had meaningful changes from baseline to 10-week and 6-month follow-up in the SPPB total score and from baseline to 10-week follow-up in gait speed (Table 2).
Changes in Health-Related Quality of Life in Each Group
In general, both groups had significant improvements in the dimension’s mobility, personal care, usual activities and health today in health-related quality of life (EQ-5D-5L). Only the fracture group had significant improvements in the dimension’s anxiety/depression and pain/discomfort. Compared to the dizziness/balance problems group, the fracture group had larger improvements in mean differences in all EQ-5D-5L dimensions at all follow-ups (see Table 2 for more details).
Occupational Priorities
In COPM interviews at baseline, the fracture group prioritized a total of 610 issues, of which 587 (96.2%) were occupation-based. On average, there were 3.9 occupation-based rehabilitation goals per participant with fractures. The participants with dizziness/balance problems prioritized a total of 425 issues, of which 386 (90.8%) were occupation-based. On average, there were 3.4 occupation-based rehabilitation goals per participant with dizziness/balance problems. The unclassifiable items in both groups were mainly related to body functions, such as improving endurance, balance, functional strength or getting rid of dizziness (data not shown). The distribution of prioritized occupations into the nine COPM sub-areas in each group is illustrated in Figure 3.
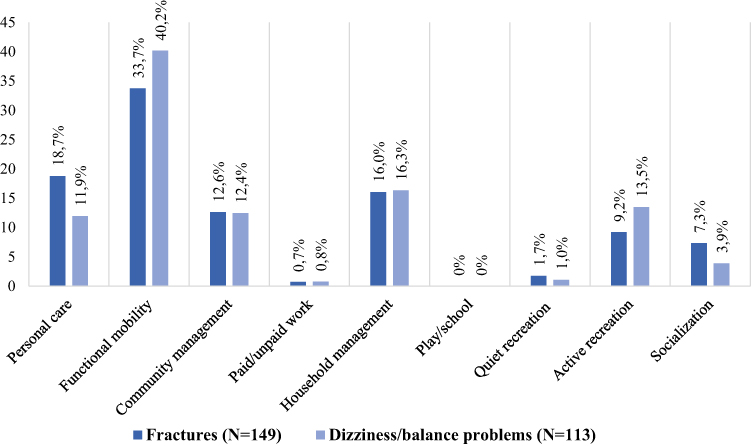 |
Figure 3 Percentages of occupations prioritized in the fracture group (dark blue columns, n = 587) and the dizziness/balance problems group (light blue columns, n = 386), respectively, in each of the nine sub-areas assessed with the Canadian Occupational Performance Measure (COPM). |
In both groups, the most frequent rehabilitation goal was to improve functional mobility with a distribution of 33.7% of the total occupation prioritized in the fracture group (n = 587) and 40.2% in the group with dizziness/balance problems (n = 386). However, the groups vary in their second and third most frequently prioritized occupations. Personal care and household management were the second and third most frequently prioritized sub-areas of occupations in the fracture group. Furthermore, household management was the second most frequently prioritized sub-area of occupations, followed by active recreation, in the dizziness/balance problems group (more details are shown in Figure 3).
Discussion
Occupational Performance and Satisfaction with Performance
The main aim of this study was to explore goals and functional changes in reablement for older home-dwelling people with fractures and dizziness and balance problems. The results show that although the dizziness/balance problems group had better scores in occupational performance (COPM-P) and satisfaction with performance (COPM-S) at baseline, the fracture group had the best scores at 10 weeks, 6 months and 12 months follow-up. The dizziness/balance problems group had some decline in mean sum scores in COPM-P and COPM-S from 6 months to 12 months, but the results in the fracture group were stable in a one-year perspective. The results from the secondary between-groups analyses which was adjusted for confounding variables, indicate significant differences in progress/improvement between the groups, in both COPM-P and COPM-S, in favor of the fracture group at all follow-ups. This was expected, as the medical conditions in the two groups are vastly different. A possible explanation for this finding may be that spontaneous improvements are expected due to the fracture healing process.46
Dizziness/balance problems are often used to describe a comprehensive set of perceptions and symptoms,47 and the underlying cause is complex and multi-factorial in the elderly.22 Changes in any aspect of the balance system, including those of sensory, visual, vestibular, neurologic, and muscular origin, can cause dizziness and imbalance. The functionality of all these parts deteriorates with age.22 Thus, recovery from dizziness and balance problems may generally be more complex than recovery from fractures. There are several other possible explanations for why the dizziness/balance problems group had less progression than the fracture group. First, fear of falling often occurs due to dizziness/balance problems48,49 and may lead to limitations in performance of everyday activities, reduced mobility, functional impairment and loss of self-confidence.18,48,49 Fear of falling is generally shown to be associated with poorer rehabilitation outcomes.50 Second, older people’s experiences with reablement show that they feel more secure when health professionals are present while they perform their everyday occupations at home.51 For such reasons, participants with dizziness/balance problems may not have felt comfortable enough to perform and practice their daily occupations alone, resulting in inactivity and less progress. Furthermore, data on whether the participants experienced fear of falling, whether they had fallen before or the causes of fracture and dizziness/balance problems, were not collected in this study. This type of data could have given such possible explanations more value.
However, it is important to note that the results show that both groups had statistically significant short-, mid-, and long-term improvements in COPM-P and COPM-S compared with baseline. These findings are consistent with three systematic reviews which found some evidence for improved independence in daily activities because of reablement.9,10,52 However, the findings in the reviews are irrespective of diagnosis. Furthermore, comparisons of this study’s results with previous research should be interpreted with caution as the length, intensity, and content of reablement intervention may vary between studies and countries, making comparisons less reliable.4,5 The results from Tuntland et al8 are more comparable with the findings in this study because they used similar outcome measures (COPM-P and COPM-S) and because long-term improvements in COPM-P and COPM-S were found. It should be mentioned that this study examined the effect of reablement compared to usual care regardless of the participants’ diagnosis.8
Unlike the fracture group, the dizziness/balance problems group showed no clinically important changes in COPM-P or COPM-S although they had statistically significant short-, mid-, and long-term improvements in COPM-P and COPM-S. Reablement is known for the principle of tailoring the intervention to the individual and for being a person-centered intervention.4 Nevertheless, reablement is considered to be a “one size fits all” intervention due to its general features.53 A general feature of reablement is, according to Metzelthin et al, its inclusive approach irrespective of diagnosis.4 The findings in this study concerning clinically important changes imply that diagnosis has an impact on the outcomes of reablement, and that the clinical importance of reablement outcomes for the dizziness and balance problem group should be questioned. There are still unanswered questions regarding the most advantageous components of reablement,6 and to our knowledge, there is no evidence indicating which elements in reablement are most beneficial to various diagnoses. As discussed elsewhere, individual adjustments according to diagnosis may be important and necessary within reablement.30 The dizziness and balance problem group may have needed closer follow-up from a physical therapist in order to build fundamental balance skills to improve performance of everyday activities. Although reablement is based on multidisciplinary collaboration, different professions may be more or less important for different diagnoses.
Environmental-related causes, gait/balance disorders or weakness, dizziness/vertigo or difficulties in transferring are among the most frequently reported causes of falls in older people.54,55 To tailor the reablement intervention to individuals with dizziness/balance problems, it may be important for the multidisciplinary reablement team to assess the risk of falls. In addition, it is important to talk about how fear of falling may affect individuals’ self-confidence to independently perform daily occupations and to facilitate possible needs.47,48 Individuals should be informed about the significance of certain environmental modifications, such as bathroom grab rails and stairwell banisters, and of avoiding loose carpets or unnecessary inventory.55 Practicing different transferring situations, such as getting in and out of bed or the shower, may also help the individual feel more secure and able to live independently in their own home.54 Adjustments with mobility aids are another option that could be considered. Given that people with dizziness/balance problems tend to avoid activity due to fear of falling,49 environmental modifications, adjustments with walking aids, and practicing transferring or receiving support from family may be of importance for older people with dizziness/balance problems to improve occupational performance, physical function, increase activity levels and to feel more secure. Some of these assumptions are supported by Arvidsson et al, who found that people with dizziness and balance problems experience that walking aids provide physical support and increased self-confidence to participate and manage everyday life.48 It is conceivable that such adjustments may diminish possible inactivity among participants with dizziness/balance problems in periods without health professionals present. It should be mentioned that these previous studies have not been conducted on a reablement intervention.47–49,54,55 Nevertheless, some of these points may be relevant in a reablement setting for people with dizziness and balance problems to benefit optimally from a reablement program.
Physical Function
In accordance with results from other studies on reablement irrespective of diagnosis, both groups improved their physical function from baseline to 10-week and from baseline to 6-month follow-up.11,13,14,56 Significant improvements in all SPPB dimensions from baseline to 12-month follow-up were only seen in the fracture group. These results imply that the participants with dizziness/balance problems benefit more from reablement in the short- and mid-term, while the fracture group benefits in the short-, mid-, and long-term regarding physical function. Pain and loss of bone and muscle strength caused by a fracture can have a profound impact on an individual’s physical function in terms of decreased mobility and occupational performance.19 Compared to the dizziness/balance problem group, the fracture group had significantly more pain/discomfort at baseline. A possible explanation for the progress in physical function in the fracture group may therefore be pain reduction related to the fracture healing.
Compared to the dizziness/balance problems group, the clinical meaningful changes in COPM and SPPB were better in the fracture group. One possible implication of these findings is that participants with dizziness/balance problems require repeated periods of reablement or a more extended reablement period than the main study’s average reablement period of 5.7 weeks in order to gain more long-term progress.11
Health-Related Quality of Life
The results imply that both groups had improvements in health-related quality of life. However, the fracture group had significantly better progression in all EQ-5D domains at all follow-ups compared to the dizziness/balance challenge group. Several studies have shown similar tendencies in reablement improving health-related quality of life,11,15,16 but the results are inconsistent. Unlike the clinical controlled trial of Langeland et al,11 this study which used a sample deriving from the Langeland trial found improvements in health-related quality of life in anxiety/depression and pain/discomfort in the fracture group. Fractures are shown to be associated with increased pain57,58 and can cause depression and postoperative anxiety due to fear of re-fracture.59 Thus, it is conceivable that the fracture group had improvements in pain/discomfort due to the fracture healing, and that gradually gaining more confidence and feeling more secure in managing their daily activities made them less anxious.
Prioritized Occupations
The results provide insight into which occupations the two groups prioritized as their rehabilitation goals. Occupations prioritized in the two groups varied to some extent. However, functional mobility was the most important occupational sub-area for both groups. These findings replicate the findings of Tuntland et al, who found significant associations between diagnosis and occupational priorities and that functional mobility is an important occupational area prioritized regardless of diagnosis.7
Previous research of reablement has found that personal care has been a second or third priority of older people,7,8 which corresponds with the importance of personal care in the fracture group. Interestingly, personal care is not among the most frequently prioritized occupational sub-areas in the dizziness/balance problems group, as it was ranked fifth, which is a finding that differs from previous studies of reablement.7,8 A possible interpretation of this finding is that shoulder or hip fractures can cause movement restrictions and pain. Thus, it can lead to occupational limitations in personal care to a greater extent than having dizziness/balance problems. Additionally, it could be that the dizziness and balance problems group are not hindered in personal care anymore, as they already have found compensatory methods to reduce their imbalance and dizziness by sitting while dressing and therefore have not prioritized personal care.
Occupational challenges related to functional mobility were expected to be most important to participants in both groups, since their low baseline scores in gait speed indicated a fragile sample. Mobility in terms of low gait speed is associated with challenges regarding Activities of Daily Living (ADL) and Instrumental Activities of Daily Living (IADL).60 Maintaining mobility is vital for managing IADL and participating in various social occupations, given that mobility involves essential functions such as walking and climbing stairs.61 Additionally, it contributes to increased well-being among older people.61 Hence, participants may have considered mobility important in order to master other types of occupations in self-care, productivity and leisure, and thus frequently prioritized functional mobility. The findings in this study support the findings of Tuntland et al,7 which highlights the importance of assessing, evaluating and facilitating functional mobility challenges, since it is a highly prominent occupational sub-area among older people with fractures and dizziness/balance problems.
The results also indicate that participants are allowed to choose a wide range of rehabilitation goals in a Norwegian reablement setting. The wide range of rehabilitation goals is most likely due to the context of reablement, which takes place in the individual’s natural environment and provides a broad range of occupational options. Another explanation could be that COPM allows participants to prioritize occupations of personal importance as rehabilitation goals.62 It is essential that reablement continues to be a person-centered intervention, enabling participants to prioritize rehabilitation goals perceived as meaningful. Such practice opens for tailoring and adjusting reablement intervention to the individual’s needs, regardless of whether they are related to physical, mental, cognitive or social aspects.7
Strengths and Limitations
A strength of this study is that the outcomes of reablement for people with fractures and people with dizziness/balance problems were examined at baseline and at three different follow-ups. This has resulted in findings that show changes over time in the two groups. Additionally, the participants were a diverse group from various municipalities in Norway, which may enhance the generalizability of the results. However, this study is limited by a lack of control groups and a relatively small sample size. Another limitation is that some participants were prevented from completing the 12 months follow up, due to the short data collection period. Furthermore, this study has merged participants with dizziness problems and participants with balance problems into one group. This choice was made because these symptoms often occur together among the older population due to changes in the vestibular system as a result of ageing processes. This is a limitation in this study as it is known that imbalance can occur without dizziness and vice versa. Moreover, no causal conclusions can be drawn regarding whether the reablement itself has led to the improvements in the two groups, nor any firm conclusion can be drawn concerning the clinical implications of the findings. Thus, generalizations should be made with caution.
Conclusion
An important finding in this study is that both people with fractures and people with dizziness/balance problems improved in terms of occupational performance and satisfaction with performance, physical function and health-related quality of life. However, participants with fractures seem to improve more than participants with dizziness/balance problems. Although functional mobility was the highest prioritized occupational sub-area in both groups, it was found diversity in their other priorities. The findings indicate that reablement needs to be tailored to the individual’s diagnosis to ensure optimal progression. Future research should explore how reablement may be tailored according to diagnosis, and how this may affect the outcomes of reablement.
Data Sharing Statement
All data is included in this article and no further data will be available.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study used a subsample derived from a larger study funded by the Norwegian Directorate of Health.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Indicators OE, Hagvísar OE. Health at a glance 2019: OECD indicators. Paris: OECD Publishing; 2019.
2. World Health Organization. World Report of Ageing and Health. World Health Organization; 2015.
3. Aspinal F, Glasby J, Rostgaard T, Tuntland H, Westendorp RGJ. New horizons: reablement - supporting older people towards Independence. Age Ageing. 2016;45(5):574–578. doi:10.1093/ageing/afw094
4. Metzelthin SF, Rostgaard T, Parsons M, Burton E. Development of an internationally accepted definition of reablement: a Delphi study. Ageing Soc. 2020;1–16. doi:10.1017/S0144686X20000999
5. Rostgaard T, Parsons J, Tuntland H. Reablement in Long-Term Care for Older People. International Perspectives and Future Directions. Policy Press; 2023.
6. Ryburn B, Wells Y, Foreman P. Enabling Independence: restorative approaches to home care provision for frail older adults. Health Soc Care Community. 2009;17(3):225–234. doi:10.1111/j.1365-2524.2008.00809.x
7. Tuntland H, Kjeken I, Folkestad B, Førland O, Langeland E. Everyday occupations prioritised by older adults participating in reablement. A cross-sectional study. Scand J Occup Ther. 2020;27(4):248–258. doi:10.1080/11038128.2019.1604800
8. Tuntland H, Aaslund MK, Espehaug B, Forland O, Kjeken I. Reablement in community-dwelling older adults: a randomised controlled trial. BMC Geriatr. 2015;15:145. doi:10.1186/s12877-015-0142-9
9. Whitehead PJ, Worthington EJ, Parry RH, Walker MF, Drummond AE. Interventions to reduce dependency in personal activities of daily living in community dwelling adults who use homecare services: a systematic review. Clin Rehabil. 2015;29(11):1064–1076. doi:10.1177/0269215514564894
10. Sims-Gould J, Tong CE, Wallis-Mayer L, Ashe MC. Reablement, reactivation, rehabilitation and restorative interventions with older adults in receipt of home care: a systematic review. J Am Med Dir Assoc. 2017;18(8):653–663. doi:10.1016/j.jamda.2016.12.070
11. Langeland E, Tuntland H, Folkestad B, Førland O, Jacobsen FF, Kjeken I. A multicenter investigation of reablement in Norway: a clinical controlled trial. BMC Geriatr. 2019;19(1):29. doi:10.1186/s12877-019-1038-x
12. Lewin G, Vandermeulen S. A non-randomised controlled trial of the Home Independence Program (Hip): an Australian restorative programme for older home-care clients. Health Soc Care Community. 2010;18(1):91–99. doi:10.1111/j.1365-2524.2009.00878.x
13. Parsons J, Sheridan N, Rouse P, Robinson E, Connolly M. A randomized controlled trial to determine the effect of a model of restorative home care on physical function and social support among older people. Arch Phys Med Rehabil. 2013;94(6):1015–1022. doi:10.1016/j.apmr.2013.02.003
14. Tinetti ME, Baker D, Gallo WT, Nanda A, Charpentier P, O’Leary J. Evaluation of restorative care vs usual care for older adults receiving an acute episode of home care. JAMA. 2002;287(16):2098–2105. doi:10.1001/jama.287.16.2098
15. Pettersson C, Iwarsson S. Evidence-based interventions involving occupational therapists are needed in re-ablement for older community-living people: a systematic review. Br J Occup. 2017;80(5):273–285. doi:10.1177/0308022617691537
16. Tessier A, Beaulieu M-D, McGinn CA, Latulippe R. Effectiveness of reablement: a systematic review. Healthc Policy. 2016;11(4):49–59. doi:10.12927/hcpol.2016.24594
17. Lin HW, Bhattacharyya N. Balance disorders in the elderly: epidemiology and functional impact. Laryngoscope. 2012;122(8):1858–1861. doi:10.1002/lary.23376
18. Lindell E, Kollén L, Johansson M, et al. Dizziness and its association with walking speed and falls efficacy among older men and women in an urban population. Aging Clin Exp Res. 2020;32(6):1049–1056. doi:10.1007/s40520-019-01303-6
19. Stanghelle B, Bentzen H, Giangregorio L, Pripp AH, Bergland A. Associations between health-related quality of life, physical function and pain in older women with osteoporosis and vertebral fracture. BMC Geriatr. 2019;19(1):298. doi:10.1186/s12877-019-1268-y
20. Eckert T, Kampe K, Kohler M, et al. Correlates of fear of falling and falls efficacy in geriatric patients recovering from Hip/pelvic fracture. Clin Rehabil. 2020;34(3):416–425. doi:10.1177/0269215519891233
21. Fosse RM, Ambugo EA, Moger TA, Hagen TP, Tjerbo T. Does rehabilitation setting influence risk of institutionalization? A register-based study of Hip fracture patients in Oslo, Norway. BMC Health Serv Res. 2021;21(1):1–678. doi:10.1186/s12913-021-06703-x
22. Iwasaki S, Yamasoba T. Dizziness and imbalance in the elderly: age-related decline in the vestibular system. Aging Dis. 2015;6(1):38–47. doi:10.14336/AD.2014.0128
23. Dahl C, Madsen C, Omsland TK, et al. The association of cold ambient temperature with fracture risk and mortality: national data from Norway—a Norwegian epidemiologic osteoporosis studies (NOREPOS) study. J Bone Miner Res. 2022;37(8):1527–1536. doi:10.1002/jbmr.4628
24. Beaupre LA, Binder EF, Cameron ID, et al. Maximising functional recovery following Hip fracture in frail seniors. Best Pract Res Clin Rheumatol. 2014;27(6):771–788. doi:10.1016/j.berh.2014.01.001
25. Haentjens P, Lamraski G, Boonen S. Costs and consequences of Hip fracture occurrence in old age: an economic perspective. Disabil Rehabil. 2005;27(18–19):1129–1141. doi:10.1080/09638280500055529
26. Amata OO, Ridolo EE, Costantino VV, et al. Maximizing rehabilitation outcomes in geriatric Hip fracture patients: the impact of surgical variables. Acta Biomed Ateneo Parmense. 2023;94:2.
27. Amata OO, Panella LL, Incorvaia CC, et al. Role of frailty in functional recovery after Hip fracture, the variable impact in restoring autonomy. Acta Biomed Ateneo Parmense. 2022;92:6.
28. Somersalo A, Paloneva J, Kautiainen H, Lönnroos E, Heinänen M, Kiviranta I. Increased mortality after upper extremity fracture requiring inpatient care. Acta Orthop. 2015;86(5):533–557. doi:10.3109/17453674.2015.1043833
29. Cao Z, Zhu C, Zhou Y, et al. Risk factors related balance disorder for patients with dizziness/vertigo. BMC Neurol. 2021;21(1):186. doi:10.1186/s12883-021-02188-7
30. Tuntland H, Kjeken I, Langeland E, et al. Predictors of outcomes following reablement in community-dwelling older adults. Clin Interv Aging. 2017;12:55–63. doi:10.2147/CIA.S125762
31. Clemson L, Laver K, Rahja M, et al. Implementing a reablement intervention, “care of people with dementia in their environments (COPE)”: a hybrid implementation-effectiveness study. Gerontologist. 2020;2020:1.
32. Rahja M, Culph J, Clemson L, Day S, Laver K. A second chance: experiences and outcomes of people with dementia and their families participating in a dementia reablement program. Brain Impairm. 2020;1–12. doi:10.1017/BrImp.2019.34
33. World Medical Association. World medical association declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194. doi:10.1001/jama.2013.281053
34. Langeland E, Tuntland H, Forland O, et al. Study protocol for a multicenter investigation of reablement in Norway. BMC Geriatr. 2015;15. doi:10.1186/s12877-015-0115-z
35. Law M, Baptiste S, Carswell A, McColl MA, Polatajko H, Pollock N. COPM. Canadian Occupational Performance Measure (Norwegian Version).
36. Tuntland H, Aaslund MK, Langeland E, Espehaug B, Kjeken I. Psychometric properties of the Canadian occupational performance measure in home-dwelling older adults. J Multidiscip Healthc. 2016;9:411–423. doi:10.2147/jmdh.S113727
37. Guralnik J, Simonsick E, Ferrucci L, et al. A short physical performance battery assessing lower extremity function: association with self-reported disability and prediction of mortality and nursing home admission. J Gerontol. 1994;49:M85–94. doi:10.1093/geronj/49.2.M85
38. Perera S, Mody SH, Woodman RC, Studenski SA. Meaningful change and responsiveness in common physical performance measures in older adults. J Am Geriatr Soc. 2006;54(5):743–749. doi:10.1111/j.1532-5415.2006.00701.x
39. Bergh S, Lyshol H, Selbæk G, Strand BH, Taraldsen K, Thingstad P. Short physical performance battery (SPPB). Available from: https://www.legeforeningen.no/contentassets/870420284b7d4cb98100191ff93e7983/sppb.pdf.
40. Chui K, Hood E, Klima D. Meaningful change in walking speed. Top Geriatr Rehabil. 2012;28(2):97–103. doi:10.1097/TGR.0b013e3182510195
41. Freiberger E, de Vreede P, Schoene D, et al. Performance-based physical function in older community-dwelling persons: a systematic review of instruments. Age Ageing. 2012;41(6):712–721. doi:10.1093/ageing/afs099
42. The EuroQol Group. EuroQol - a new facility for the measurement of health-related quality of life. Health Policy (New York). 1990;16(3):199–208. doi:10.1016/0168-8510(90)90421-9
43. Haywood KL, Garratt AM, Fitzpatrick R. Quality of life in older people: a structured review of generic self-assessed health instruments. Qual Life Res. 2005;14(7):1651–1668. doi:10.1007/s11136-005-1743-0
44. Cohen J. Statistical Power Analysis for the Behavioral Sciences.
45. IBM Corporation. SPSS for Windows, Version 27. IBM Corporation; 2020.
46. Clark D, Nakamura M, Miclau T, Marcucio R. Effects of aging on fracture healing. Curr Osteoporos Rep. 2017;15(6):601–608. doi:10.1007/s11914-017-0413-9
47. Desai MH, McKinnon BJ. Balance and Dizziness Disorders in the Elderly: a Review. Curr Otorhinolaryngol Rep. 2020;8(2):198–207. doi:10.1007/s40136-020-00281-y
48. Arvidsson LM, Forsberg A, Appelros P, Anderzén-Carlsson A. ”I can manage the challenge” - a qualitative study describing experiences of living with balance limitations after first-ever stroke. Int J Qual Stud Health Well-Being. 2021;16(1):1857044. doi:10.1080/17482631.2020.1857044
49. Kollén L, Hörder H, Möller C, Frändin K. Physical functioning in older persons with dizziness: a population-based study. Aging Clin Exp Res. 2017;29(2):197–205. doi:10.1007/s40520-016-0567-9
50. Pfeiffer K, Kampe K, Klenk J, et al. Effects of an intervention to reduce fear of falling and increase physical activity during Hip and pelvic fracture rehabilitation. Age Ageing. 2020;49(5):771–778. doi:10.1093/ageing/afaa050
51. Hjelle KM, Tuntland H, Førland O, Alvsvåg H. Driving forces for home-based reablement; a qualitative study of older adults’ experiences. Health Soc Care Community. 2017;25(5):1581–1589. doi:10.1111/hsc.12324
52. Cochrane A, Furlong M, McGilloway S, Molloy DW, Stevenson M, Donnelly M. Time-limited home-care reablement services for maintaining and improving the functional Independence of older adults. Cochrane Database Syst Rev. 2016;10:Cd010825. doi:10.1002/14651858.CD010825.pub2
53. Legg L, Gladman J, Drummond A, Davidson A. A systematic review of the evidence on home care reablement services. Clin Rehabil. 2016;30(8):741–749. doi:10.1177/0269215515603220
54. Lindell E, Karlsson T, Kollén L, Johansson M, Finizia C. Benign paroxysmal positional vertigo and vestibular impairment among older adults with dizziness. Laryngoscope Investig Otolaryngol. 2021;6(3):488–495. doi:10.1002/lio2.566
55. Rubenstein LZ. Falls in older people: epidemiology, risk factors and strategies for prevention. Age Ageing. 2006;35(suppl–2):ii37–ii41. doi:10.1093/ageing/afl084
56. Lewin G, De San Miguel K, Knuiman M, et al. A randomised controlled trial of the home independence program, an Australian restorative home-care programme for older adults. Health Soc Care Community. 2013;21(1):69–78. doi:10.1111/j.1365-2524.2012.01088.x
57. Hallberg I, Bachrach-Lindström M, Hammerby S, Toss G, Ek A-C. Health-related quality of life after vertebral or Hip fracture: a seven-year follow-up study. BMC Musculoskelet Disord. 2009;10(1):135. doi:10.1186/1471-2474-10-135
58. Gjertsen J-E, Baste V, Fevang JM, Furnes O, Engesæter LB. Quality of life following Hip fractures: results from the Norwegian Hip fracture register. BMC Musculoskelet Disord. 2016;17(1):265. doi:10.1186/s12891-016-1111-y
59. Yoo JI, Lee YK, Koo KH, Park YJ, Ha Y-C. Concerns for older adult patients with acute hip fracture. Yonsei Med J. 2018;59(10):1240–1244. doi:10.3349/ymj.2018.59.10.1240
60. Wang DXM, Yao J, Zirek Y, Reijnierse EM, Maier AB. Muscle mass, strength, and physical performance predicting activities of daily living: a meta-analysis. J Cachexia Sarcopenia Muscle. 2020;11(1):3–25. doi:10.1002/jcsm.12502
61. Satariano W, Guralnik J, Jackson R, Marottoli R, Phelan E, Prohaska T. Mobility and aging: new directions for public health action. Am J Public Health. 2012;102:1508–1515. doi:10.2105/AJPH.2011.300631
62. Enemark AL, Rasmussen B, Christensen JR. Enhancing a client-centred practice with the Canadian occupational performance measure. Occup Ther Int. 2018;2018:5956301. doi:10.1155/2018/5956301
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.