")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
Exploring Female Relatives of Patients with Hemophilia’ Awareness, Attitudes, and Understanding Towards Genetic Testing
Authors Zhao H, Geng WJ, Wu RH, Li ZZ
Received 6 November 2023
Accepted for publication 31 January 2024
Published 16 February 2024 Volume 2024:17 Pages 711—721
DOI https://doi.org/10.2147/JMDH.S430984
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Hua Zhao,1 Wen-Jing Geng,2 Rui-Hong Wu,3 Zhen-Zhen Li3
1College of Nursing, Shanxi University of Chinese Medicine, Jinzhong, Shanxi, People’s Republic of China; 2Nursing Department, Third Hospital of Shanxi Medical University, Shanxi Bethune Hospital, Shanxi Academy of Medical Sciences, Tongji Shanxi Hospital, Taiyuan, Shanxi, People’s Republic of China; 3Department of Hematology, the Second Hospital of Shanxi Medical University, Taiyuan, Shanxi, People’s Republic of China
Correspondence: Hua Zhao, College of Nursing, Shanxi University of Chinese Medicine, Jinzhong, Shanxi, 030619, People’s Republic of China, Tel +86 13903465019, Email [email protected]
Purpose: A better understanding of the factors that influence engagement is needed to provide a reference for conducting genetic testing in female relatives of patients with hemophilia (PWH). We therefore determined the perceptions and understanding of genetic testing among female relatives of PWH in China.
Methods: We carried out a qualitative study using in-depth, semi-structured interviews with 11 female relatives of PWH in Shanxi Province, China. The resulting data were analyzed using thematic analyses.
Results: This study extracted four topics: uncertainty about carrier genetic status; limited understanding of genetic testing; coexistence of positive and negative coping; and multi-aspect demands.
Conclusion: Healthcare professionals should provide personalized and multidimensional health education and comprehensive decision-making support to female relatives of PWH, to enhance their motivation and willingness to undergo genetic testing. It is also important to actively improve relevant policies, strengthen the genetic testing service system, and promote the popularization of genetic testing in female relatives of PWH.
Keywords: hemophilia, female, genetic testing, attitudes, qualitative study
A Letter to the Editor has been published for this article.
Introduction
Hemophilia is an X-linked recessive genetic bleeding disorder caused by a deficiency or decrease in the activity of coagulation factor VIII or IX. Hemophilia can be divided into hemophilia A (HA) and hemophilia B (HB), and can be severe (factor level <1 IU/dL), moderate (1–5 IU/dL), or mild (5–40 IU/dL), depending on the clotting factor concentration.1 An annual global survey 2022 by The World Federation of Hemophilia (WFH) reported 257,146 patients with hemophilia (PWH) in 125 countries. HA and HB comprise 81.26% (208,957/257,146) to 16.41% (42,203/257,146) of PWH, with the remaining 2.33% (5,986/257,146) attributed to hemophilia of type unknown or type not reported.2 The reported prevalence of hemophilia was 2.73–3.09 per 100,000 population in China, with approximately 120,000 PWH, with approximately 40,000 cases currently registered.3,4 Shanxi Province in northern China covers an area of 156,700 km2, with a population of 34.91 million, and is considered to be an underdeveloped province. The Shanxi Hemophilia Treatment Center (HTC) was established in 2009, and a multidisciplinary team was subsequently developed. The HTC is responsible for managing the medical records of PWH, including the collection and reporting of information related to diagnosis, treatment, nursing care, education, and access to coagulation factors. A total of 902 PWH have been registered thus far.
The main clinical characteristic of hemophilia is bleeding (spontaneous or after trauma) into major joints such as the ankles, knees and elbows, while some patients with severe hemophilia may also have intracranial or internal organ bleeds.5 The treatment of hemophilia is based on replacement therapy with coagulation factor products. However, PWH in developing countries face many challenges and barriers to obtaining adequate treatment, and may thus suffer from different degrees of chronic damage to the musculoskeletal system, resulting in severe handicaps and even death.6,7 Other complications, such as the development of inhibitory antibodies, further increase the complexity and costs of managing the disease.8 Available data from medium- and high-income countries show life-expectancy disadvantages of people with HA and HB of 30% and 24%, respectively, compared with the rest of the population, with a much greater disadvantage in countries with more limited access to treatments for hemophilia.9 These findings suggest that, in addition to its clinical burden, hemophilia also places a significant economic burden on healthcare payers, patients/caregivers, and society.10
Hemophilia is usually inherited, with up to 30% of babies with hemophilia having no family history of the disorder, while the remaining 70% are born into families where hemophilia has been diagnosed.11 Most affected patients are males, who inherit an affected X-chromosome from their mother, while females with a factor VIII or factor IX pathogenic variant are referred to as obligate hemophilia carriers. Obligate hemophilia carriers can be identified as having a hemophilia gene based on an analysis of their family history, and include any biological daughter of a father with hemophilia, any biological mother of a child with hemophilia who also has at least one other family member with hemophilia or who is a known carrier of hemophilia, and any biological mother of two or more children with hemophilia. Potential hemophilia carriers include any biological daughter, sister, mother, maternal grandmother, aunt, niece, or female cousin of a carrier of hemophilia, and any biological mother of a child with hemophilia but no known family history of hemophilia or carriers of hemophilia.1 Every PWH may thus have five female relatives who are potential carriers.11 Carriers are often perceived to have no bleeding symptoms; however some carriers of hemophilia are now known to experience bleeding problems, including joint hemorrhages similar to males, as well as experiencing female-specific problems, such as prolonged or heavy menstrual bleeding. The study showed that carriers may have an increased bleeding risk, more doctor visits, and greater health-related costs than females without the affected gene. However, health issues of carriers are often only discovered later in life, such as during pregnancy, and they are often not aware of their reproductive risks and choices or their potential bleeding risks, and are often overlooked and underdiagnosed.12–14 The earlier diagnosis of carriers may reduce the incidence rate of hemophilia, and help to decrease carriers’ health issues and associated costs.15,16
Genetic testing is the only way to confirm that a woman has hemophilia (or is a symptomatic or asymptomatic carrier), and can allow more accurate guidance on scientific pregnancy preparations and fertility assessments for hemophilia family members.17,18 WFH guidelines for the management of hemophilia, 3rd edition, recommend that all obligate carriers of hemophilia and “at-risk” female relatives of PWH or potential carriers of hemophilia receive genetic counselling about their risk of being a carrier, and that genetic testing should be offered for previously identified genetic variants of the F8 or F9 gene.1 Furthermore, the Core Information about Health Education for the Prevention and Treatment of Hemophilia issued by the National Health Commission of China advocated that high-risk groups should receive genetic counseling, genetic testing, and prenatal diagnosis before pregnancy and parturition.19 Genetic testing should thus be promoted vigorously to improve the health, wellbeing, and quality of life for hemophilia families. The Knowledge, Attitude, and Practice (KAP) theory is a theoretical model for changes in human health-related behaviors.20 KAP suggests that improving understanding of diseases, developing positive attitudes, and forming healthy practices are three continuous processes of health education, and that individuals with positive attitudes are more motivated to implement practices and obtain better results.21 Although the knowledge and attitude of female relatives of PWH is likely to influence comprehensive genetic testing,22–24 there have been few reports on the knowledge of and attitudes towards genetic testing in female relatives of PWH in China, and insufficient importance is attached to studies in this field. Obtaining a better understanding of the knowledge and attitudes of female relatives of PWH towards genetic testing could thus provide information to support the design and development of genetic counseling services, and facilitate the implementation of genetic testing plans for female relatives of PWH.
Materials and Methods
Study Design
This qualitative study examined the awareness of genetic testing and attitudes towards participating in such testing among 11 female relatives of PWH from Shanxi HTC (Taiyuan, China), based on semi-structured interviews.
Target Population and Sampling
We employed the purposive sampling method in conjunction with a maximum variation sampling to select female relatives of PWH. The number of interviewees was determined based on the study objectives and input from key informants, ensuring that no new themes emerged. Data saturation was achieved after interviewing the 11th participant. All interviewees met the following criteria: female relative with a genetic connection with a PWH; age ≥ 18 years; normal linguistic expression and communication competence; and signed an informed consent form and participated in this study in a voluntary manner. The exclusion criteria were: subject diagnosed with severe psychological health problems or emotional disorders, such as anxiety, depression, psychosis, or bipolar disorder; and subject had hearing, communication, or cognitive impairments.
Study Protocol
A research team developed the interview protocol guided by the consolidated criteria for reporting of qualitative research (COREQ)25 and informed by a literature review and insights from the research team. The research team consisted of one physician, one coagulation-laboratory-testing specialist, one psychological counselor, three hemophilia nurses, and one research assistant. All researchers directly involved in data collection and analysis were well-experienced in qualitative interviewing and/or thematic analysis. The researchers formulated the interview outline with the following questions: (a) How do you perceive your identity as a female relative of a PWH? (b) Have you heard of genetic testing for female relatives of PWH? What are your attitudes about it? (c) What effects do you think genetic testing would have on your life? (d) What suggestions and expectations do you have for the development of genetic testing for female relatives of PWH? The question sequence was not fixed, and could be adjusted according to actual situations while answering the questions of the interviewees.
Data Collection
Before starting the interview, the researcher explained the objectives, significance, and confidentiality principle to the interviewees, and informed them that the interview process would be simultaneously audiotaped. Written consent and permission for audio recording were obtained from each participant. The interview format was a one-on-one in-depth interview, with the location and time determined by the interviewee. The interviews were conducted in an open-ended atmosphere, so that the interviewees could communicate in a relaxed state with maximum trust. During the interview process, researchers encouraged the interviewees to express their real thoughts and feelings by adopting interviewing techniques such as questioning, listening, responding, making detailed inquiries, and repeating, while observing and recording the interviewees’ body movements, facial expressions, tones, and other non-verbal behaviors. As a method of participant validation, the interviewer outlined the main points after the interview.26 The entire interview lasted from 30 min to 1 h. Data were collected over a 3-month period, due to the impact of the COVID-19 pandemic. The interviewees were thanked for their time at the end of each interview and were reminded that they would be called upon for further clarification if needed. No interviewees dropped out of the study.
Data Analysis
The recordings of the interviews were transcribed and analyzed by the research team within 24 h of the completion of each interview, using Nvivo 12 software. Two researchers respectively and independently read the corresponding data and stored backups. The research team then analyzed the data using the Braun and Clarke thematic analysis method,27 with the following steps: (a) being familiar with the data, (b) generating initial codes, (c) finding topics, (d) reviewing topics, (e) defining and naming topics, and (f) generating reports. Finally, the research team returned the corresponding results to the interviewees. If new data were obtained during the data-verification process, these new data were integrated into the existing data to reflect the interviewees’ real thoughts on the interview questions. The data were continuously assessed and evaluated for meaning and completeness to ensure their dependability. Confirmability was achieved by the classification of coding into categories, and major categories were discussed together among all researchers. One researcher with expertise in conducting qualitative studies supervised and audited the whole process.
Ethics
This study was approved by the ethics review committee of the Second Hospital of Shanxi Medical University (Shanxi, China; Approval No. [2022] YX No. [102]), and written informed consent was obtained from all interviewees. The study conformed to the Declaration of Helsinki.28 In this study, the researchers had no relationship with the interviewees. The interviewees had the right to withdraw from the study at any time, and their participation in the study would not influence their treatment and nursing care. Their anonymity and confidentiality were ensured throughout the study.
Results
A total of 11 female relatives of PWH (F1–F11) from eight hemophilia families, defined as known (4/8) and without family history (sporadic, 4/8), were included. Nine female relatives were from families with HA and two from families with HB. There were five obligate and six potential carriers. The demographic characteristics are shown in Table 1.
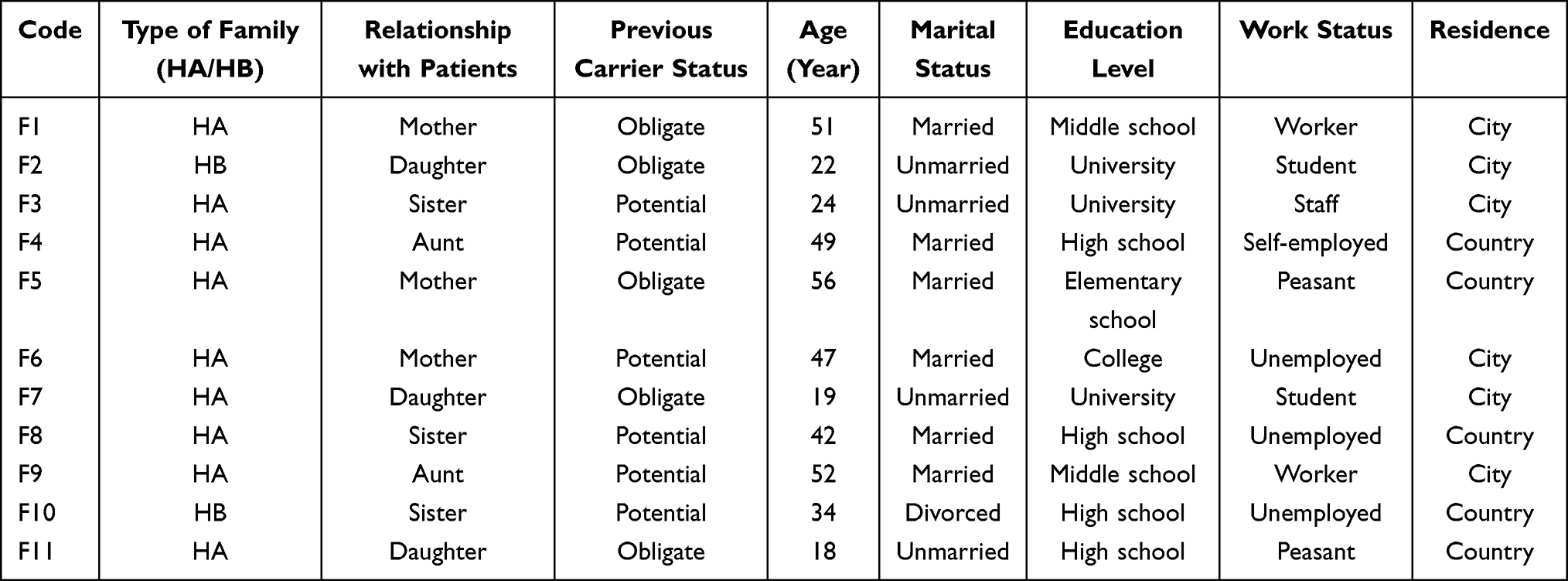 |
Table 1 Demographic Characteristics of Female Relatives of PWH (N = 11) |
Topic 1: Uncertainty About Carrier Genetic Status
Of the 11 interviewees, 10 individuals indicated that they were aware of hemophilia being a hereditary disease, while one expressed complete unawareness of its hereditary nature (F5). Only three interviewees were able to fully explain the genetic inheritance pattern of hemophilia, four could describe obligate carriers but were unsure about potential carriers, and the remaining four interviewees had no understanding of the genetic inheritance pattern of hemophilia. None of the 11 interviewees had undergone genetic testing, resulting in a lack of genetic information. Three individuals were aware of their status as obligate carriers, while eight were uncertain about the possibility of being carriers.
Uncertainty was also experienced as a “lack of identity”, which falls under person-centered issues of uncertainty.29 For female relatives of PWH, a significant part of their identity was undefined, and receiving a diagnosis would allow them to regaining their missing identity and join an identifiable group of people with the same known condition, such as access to support groups and the ability to qualify for participation in research: “I and my family eager to join a peer group, but my uncertain status made it difficult to find” (F3).Concerning the feelings of uncertainty about their genetic carrier status, one participant spoke about “the burden of passing the gene on to the offspring” and the fear associated with it: “I have been informed that I am a carrier of hemophilia, yet I am uncertain about this assertion. I am hesitant about the prospect of marriage, as I worry about the potential difficulties it may bring for my future children. I am uncertain if my family will blame me for this”. She also pointed out: “I will not complain about my father, as I have witnessed the immense suffering he has endured. It is a hereditary disease, and all I can say is that our fate has been unfortunate (F2)”.
Topic 2: Limited Understanding of Genetic Testing
The interviews revealed that the interviewees lacked professional channels to obtain information. Among the 11 interviewees, four stated that they had never known about genetic testing, while seven said that, although they had heard of genetic testing, they did not understand its specific significance. The interviews indicated that the seven interviewees’ knowledge mainly came from hematologists (3/7), other patients and female relatives of PWH (2/7), and from self-exploration (2/7): “I had never heard of this term of ‘genetic testing’ before this interview” (F5). “I’ve heard of genetic testing, but I don’t know about it” (F10). “I heard it from another patient, but he just mentioned it, and I didn’t learn about it further” (F4). “I’ve searched some knowledge about it (genetic testing) on the Internet by myself, but I still don’t know how to participate in it” (F3). “When I went to the Obstetrics and Gynecology Department after becoming pregnant and mentioned that there were hemophilia patients in my family, the doctor there seemed unaware of whether I was a carrier, did not suggest genetic testing, and did not provide any advice on reproductive risks and choices, only suggesting that I consult the hematology department (F10)”.
These interviewees lacked knowledge of or lacked confidence in understanding genetic testing, which usually led to them being hesitant or unsure about the significance of their testing results. Regardless of their level of education, the interviewees all mentioned a lack of relevant knowledge when asked about the significance of testing results and the possible sources of disease risks.
Topic 3: Coexistence of Positive and Negative Coping
Hold Favorable Attitudes Toward Genetic Testing
Most female relatives of PWH showed positive attitudes towards genetic testing. They believed developments in genetic testing technology would improve medical standards and the quality of life of female relatives of PWH, and would represent a positive action to reduce the prevalence of defective offspring: “I support the application of this technology, as we could take more appropriate actions only if we understand the causes of disease and potential risks” (F11). “Although the Doctor assured me that I was a obligate carrier. But I have no symptoms, and apart from my father, none of our ancestors have had the disease. So I’m still not convinced I have a problem. I want to check and make sure” (F7); “I haven’t got married and given birth to babies yet, and as my younger brother is a hemophiliac, I want to check whether I’m a carrier of pathogenic genes, so that I could make corresponding plans early, and I don’t want my children to be affected (F3)”.
Genetic Testing-Related Concerns and Worries
Technology Concerns
Some interviewees expressed various uncertainties about genetic testing. “Is it safe to participate in the screening?” “Will I catch other diseases?” “I really don’t want to have any disease” (F4). Privacy concerns affected their decision-making: “Will you keep the (screening) results confidential for us?” (F1).The accuracy of the screening results was also of great concern to the interviewees: What’s the accuracy rate of the screening?” (F6).
Economic Pressure
Hemophilia imposes a significant burden on affected families,30,31 and the cost of genetic testing may be a barrier to implementing screening. Most interviewees indicated that the cost of screening would be a constraint affecting their decision to participate in genetic testing: “Now, the most disturbing thing is that I can’t go to work because I have to look after my son, and thus lost my source of income, having no money to support myself to participate in genetic testing. (F6)”.
Genetic testing in families with hemophilia is currently not included in medical insurance in Shanxi Province, and screening usually has a relatively high cost, suggesting that these factors could serve as potential barriers and limit its use. “Could this expense be reimbursed by medical insurance?” “The financial conditions of our family can’t afford it” (F8).
Concern About Genetic Testing Results
Recent developments in carrier testing may have increased the psychological burden on female relatives of PWH. Female relatives of PWH are well aware of the suffering associated with long-term coexistence with this disease, resulting in fear and a guilty conscience, involving concern that the pathogenic genes may be passed to their next generation, and blaming themselves for affecting their children’s future employment, marriage, childbearing choices, and social activities. One participant talked about her feelings about being a carrier: “Previously, I would console myself by thinking that if my child were to fall ill, it could be due to a genetic mutation. However, I know that genetic testing might reveal that I am the culprit. Just the thought of it makes me incredibly sad and disrupts my peace of mind. (F6)”.
During the interview, some interviewees indicated that they were willing to undergo genetic testing and understood that genetic testing had certain positive values for themselves and their families, but they still had concerns. They expected to receive good results from the screening, but also worried about receiving bad results, and this ambivalence eroded their decision on whether to continue participating in genetic testing: “I worry that bad genetic information would increase my child’s psychological burden and anxiety” (F9); “I expect to receive a screening report indicating no potential health risks, but I’m also in fear of getting poor results that would affect my child’s future growth and bring about one disaster after another to our family (with anxiety). (F10)”.
Topic 4: Multi-Aspect Demands
Professional Information Support
Cognition is the premise and foundation of actions; obtaining relevant knowledge about genetic testing through professional channels can improve the recognition, acceptance, and action of families with hemophilia concerning genetic testing, to facilitate screening. Most interviewees stated that they were information seekers but had little knowledge about genetic testing, and hoped that professional medical institutions would provide databases and resource navigations for genetic testing information, to emphasize the value of screening: “I suggest that medical workers should organize popular science lectures on genetic testing in a regular manner, and also post all the relevant knowledge about genetic testing on the Internet, such as on WeChat official accounts and other platforms. (F11)”.
When hemophiliacs and their family members were confused about relevant information regarding genetic testing, their confidence and motivation to participate were reduced: “Which hospital is capable of carrying out genetic testing? What’s the specific screening procedure? Does it need to draw blood? We don’t know anything about it, and of course our interest is not high. (F7)”.
Medical Service Guarantees
Having an accurate understanding of the demands for information of female relatives of PWH regarding genetic testing could promote full implementation of genetic testing projects and provide guidance for the development of genetic testing services.32 During interviews, the interviewees voiced their demands for genetic testing services. At present, many hospitals in China do not have outpatient services for genetic testing and do not possess the capacity for genetic testing. Samples need to be sent to third-party institutions to conduct testing, and the results are then uploaded in higher-level hospitals or testing institutions for further diagnosis, thus lengthening the screening cycle and leading the screened participant to generate negative emotions: “How long would it take to get the results? The waiting process is really painful” (F3). The nearer that the medical institution is to home, ie, the greater the geographic accessibility, the more positive the health behaviors.33,34 “I hope we could participate in screening in a local institution, so that we don’t have to travel back and forth very far” (F9). “As for the genetic testing results, I hope to have face-to-face consultations with medical workers and get their authoritative analysis and guidance” (F11).
Discussion
The National Health Commission of China requires efforts to be made to prevent and control birth defects. This includes guiding the public in enhancing their health literacy and actively seeking services, with the goal of reducing the incidence of hemophilia.35 WFH emphasized the need for continued efforts to increase knowledge and awareness, to ensure that girls and women with bleeding disorders received a correct and timely diagnosis, as well as proper access to care.36 The conceptual core of the Knowledge, Attitude, Belief and Practice model is the cascade of knowledge, beliefs, and behaviors.37 Information and knowledge provide the basis for establishing positive attitudes, which are in turn the driving force for behavioral modification. The current study showed that awareness of genetic testing among female relatives of PWH was still insufficient and incomplete, indicating inadequate relevant knowledge about genetic testing, and some interviewees also expressed demands for obtaining genetic testing information. Providing multi-channel health education to improve the cognitive level of female relatives of PWH is thus a concern of genetic testing.
The interviews revealed that female relatives of PWH were more receptive to inquiries about their family history compared with directly discussing genetic testing. The WFH recommends that, for obligate carriers of hemophilia and “at-risk” female relatives of PWH or potential carriers of hemophilia, a detailed family pedigree should be included to support the genetic testing referral.1 Genetic counselling for female relatives of PWH is an essential requirement prior to genetic testing, to ensure that the individuals fully understand the testing procedure, the benefits and limitations of the test, and the possible consequences of the test results.38 Healthcare providers can thus conduct health education in stages; staff at the HTC can begin to educate individuals on the natural history of hemophilia, establish their family tree/pedigree, and perform risk assessments related to the inheritance of hemophilia, and on this basis, can then facilitate genetic testing, help them to process and integrate genetic information, and discuss relevant reproductive options. Notably however, we have to be aware that genetic testing raises ethical and cultural concerns, especially with regard to the communication of information and test results during childhood. Healthcare professionals and families should consider whether such information should be disclosed, and if so, how, when, and by whom. These decisions should be informed by the readiness of an underage girl to manage the information about her potential hemophilia status, including factors such as her age, emotional maturity, and level of understanding and interest in the information. The WFH recommends that formal genetic testing should be offered to potential carriers when they are mature enough to understand the consequences of the diagnosis and give consent.1 However, discussions should include the affected children, not just their parents, given that children often have a good understanding of their status and can work with the physician if properly informed and educated.
Studies have shown that enhancing visual effects could improve people’s understanding of screening information.39 Hospitals should therefore make full use of digital media to record popular science videos and distribute promotional and educational brochures. They could also invite experts in this field, as well as patients or their family members with experience in genetic testing, to share their experiences or take similar actions, to help female relatives of PWH by enhancing their understanding of genetic testing and risk awareness. In addition to obtaining information about genetic testing, comprehensive care teams also need to be provided with as much information as possible about the physical, psychological, emotional, an economic dimensions of hemophilia carriers, in terms that female relatives of PWH can understand.
The results of this study showed that perceptions of and attitudes to hemophilia in female relatives of PWH, including complications, drug treatment, heredity, marriage, childbearing risks, and other risks of hemophilia, indicated a strong motivation for a change in their attitudes and behaviors towards genetic testing. Female relatives would be more willing to undergo genetic testing if they could fully recognize the possible dangers of the disease, especially in terms of the health of the next generation. Some researchers use used the term “genetic responsibility” to describe this specific situation and the feeling of being responsible for the health of others.40,41 In addition, when families with hemophilia are overly aware of the dangers of the disease but still fail to adjust their attitudes, excessive concerns about life, marriage, and childbearing of future generations lead to negative emotions such as self-accusation, fear, and depression.42,43 Sheridan et al44 found that the most common reasons for guilt among mothers of children with hemophilia included putting their child through pain during infusions and passing on the affected X chromosome. Our results found that female relatives of PWH were concerned about financial, physical, and psychological burdens related to the stress, tension, and anxiety that they experienced as caregivers and carriers, faced with challenges. Guiding female relatives of PWH to correctly understand the severity of the disease, without causing excessive panic, requires healthcare professionals to provide individualized and multi-dimensional health education, as well as comprehensive and effective decisional support to these individuals, to help them understand the disease and its inheritance, and improve the awareness of genetic testing among high-risk carriers, to enhance their motivation and willingness to change attitudes and behaviors towards genetic testing.
During the interview, most female relatives of PWH reported using emotion-focused coping strategies, such as acceptance and emotional support from family and friends or self-care strategies, to cope with stress. Some obligate carriers expressed feelings of calmness or acceptance, while potential carriers expressed fear and concern, especially when they already had experience of hemophilia in their relatives. This range of feelings indicates that the feelings of obligate carriers may differ from those of potential carriers, and that their needs and feelings might also be affected by their family history. As a consequence, information and counseling might need to be adapted to these specific situations to make sure that all the individual’s feelings and needs are appropriately addressed. Some findings indicated a strong need for understandable, clear, and basic information regarding the modes of inheritance and the inheritance patterns of pathogenic variants, in order to prevent blame and negative feelings; it might thus be important to explain that these inheritance patterns cannot be influenced and no one is to blame for anything.45 McClaren et al46 thus identified bringing genetic diseases “into the worlds” of the general public, who largely viewed it as the domain of small groups of affected families, as a key challenge in the successful implementation of carrier screening programs. Hughes and Phelps47 showed that “different people want different things at different stages in their life and throughout their genetic journey”, and proposed a model of support consisting of multiple elements, including social events, a 24 h phone line, a chat forum, and a central professional and peer-led organizing body.
This study found that privacy, expense, and a fear of positive results affected the choice of female relatives of PWH regarding participation in genetic testing, consistent with the findings of Punt et al and Chaigneau et al23,48 These results suggest that when conducting genetic testing, it is necessary to ensure the security of the genetic information for the whole family,49 and relevant departments should improve personal privacy protection policies, strengthen the awareness of medical safety precautions among medical workers, and eliminate the concerns of hemophiliac families about the inappropriate use of their genetic information. Professional medical and nursing teams should be organized to expand specialist training and assessment in genetics, improve genetic testing techniques, and report the interpretation ability of medical workers, to provide comprehensive and systematic genetic guidance and prompt high-risk groups to overcome their fear and negative emotions. Regarding testing costs, the government should encourage relevant institutions to facilitate the continuous advancement of biotechnology for genetic testing, reduce the costs of screening, and improve the validity and reliability of screening results, as well as coordinating multiple organizations to jointly provide social support, form a social-assistance system led by the government with the participation of forces from all walks of life, and expand the supply coverage of health services for genetic testing in families with hemophilia, thereby reducing the resistance of families with hemophiliacs. In addition, it is necessary to provide more needs-oriented health education and to help female relatives of PWH to understand the relationship between costs and outcomes. An earlier diagnosis may help reduce their health issues and associated costs.
Study Limitations
To the best of our knowledge, this is the first study to explore the attitudes of female relatives of PWH towards genetic testing in China, including in-depth insights into a broad spectrum of different perspectives, life situations, feelings, and opinions of this specific target group. The results of this study provide a basis for future research in related fields. However the study also had some limitations. First, we only considered genetic testing from the perspective of female relatives of PWH, which may have resulted in some bias. Second, the study was conducted at a single HTC in China, and further studies are needed covering wider geographic areas, especially rural areas, to better serve female relatives of PWH.
Conclusion
This study aimed to gain deeper insights into the experiences and perceptions of female relatives of PWH, particularly regarding genetic testing. We discovered that the knowledge and attitudes of these relatives towards genetic testing significantly influenced their testing behaviors. Furthermore, hemophilia had profound negative impacts on the psychological well-being and overall quality of life of these individuals; however, their unique experiences and needs were often overlooked. The results suggest that, although female relatives of PWH generally have a positive attitude towards genetic testing, they lack the necessary knowledge and decision-making support, resulting in conflicts and a strong desire for information. They seek decision-making support led by healthcare professionals. These finding underscore the need to develop and implement patient and family education programs and decision support measures in China, guided by healthcare professionals and tailored to the clinical context. Medical practitioners should thus respond appropriately to enhance the literacy of female relatives of PWH regarding genetic testing, thereby improving their engagement in screening activities. Moreover, medical institutions should invest in specialized training for healthcare professionals, emphasizing confidentiality awareness and proficiency in genetic testing, to ensure accurate and secure screening outcomes. It is also crucial for society at large to prioritize the well-being of female relatives of PWH. The government should allocate increased funding for genetic testing in this population and refine the genetic testing service system to enhance its accessibility and uptake. Furthermore, understanding the emotions, coping mechanisms, and support requirements of female relatives is essential and beneficial. We therefore recommend providing psychological support and establishing peer groups for these individuals, as well as exploring and strengthening the involvement of nurses in genetic testing initiatives.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the declaration of Helsinki. This study was approved by the ethics review committee of the Second Hospital of Shanxi Medical University (Shanxi, China; Approval No. [2022] YX No. [102]), and written informed consent was obtained from all interviewees. Consent included the publication of their anonymized responses. The informed consent obtained from participants included consent to publish identifying details in Table 1.
Acknowledgments
We thank the Female Relatives of Patients with Hemophilia, their families, and the clinical personnel who participated in this study. We thank International Science Editing for editing a draft of this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study has been conducted through a project grant from the Scientific Research Foundation for Doctoral Programs of Shanxi University of Chinese Medicine, grant no.: 2020BK16; 2023 Shanxi Provincial Philosophy and Social Science Planning Project, grant no.: 2023YJ100; Shanxi provincial colleges and universities general teaching reform and innovation project, grant no.: J20230894.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Srivastava A, Santagostino E, Dougall A, et al. WFH Guidelines for the Management of Hemophilia, 3rd edition. Haemophilia. 2020;Suppl 26(S6):1–158. doi:10.1111/hae.14046
2. World Federation of Hemophilia. Report on the Annual Global Survey 2022. Montreal, Canada: WFH; 2023.
3. Zhang L, Dai XY. Clinical research progress of hemophilia gene therapy. J Clin Hematol. 2022;35(07):464–468. doi:10.13201/j.issn.1004-2806.2022.07.003
4. Xue F, Dai J, Chen LX, et al. Report on diagnosis and treatment of hemophilia in China 2023[J]. J Diagnostics Concepts Practice. 2023;22(02):89–115. doi:10.16150/j.1671-2870.2023.02.001
5. Berntorp E, Fischer K, Hart DP, et al. Haemophilia. Nat Rev Dis Primers. 2021;7(1):45. doi:10.1038/s41572-021-00278-x
6. Ndoumba-Mintya A, Diallo YL, Tayou TC, Mbanya DN. Optimizing Haemophilia Care in Resource-Limited Countries: current Challenges and Future Prospects. J Blood Med. 2023;14:141–146. doi:10.2147/JBM.S291536
7. Mannucci PM. Hemophilia therapy: the future has begun. Haematologica. 2020;105(3):545–553. doi:10.3324/haematol.2019.232132
8. Walsh CE, Jiménez-Yuste V, Auerswald G, Grancha S. The burden of inhibitors in haemophilia patients. Thromb Haemost. 2016;116 Suppl 1:S10–S17. doi:10.1160/TH16-01-0049
9. Quintana paris L. Foundations of hemophilia and epidemiology. Blood Coagul Fibrinolysis. 2023;34(S1):S35–S36. doi:10.1097/MBC.0000000000001222
10. Chen SL. Economic costs of hemophilia and the impact of prophylactic treatment on patient management. Am J Manag Care. 2016;22(5 Suppl):s126–s133.
11. Street AM, Ljung R, Lavery SA. Management of carriers and babies with haemophilia. Haemophilia. 2008;14(Suppl 3):181–187. doi:10.1111/j.1365-2516.2008.01721.x
12. Hermans C, Krumb E, Rotellini D, Pierce GF. The under-evaluated impacts of the therapeutic revolution of hemophilia on women and girls. J Thromb Haemost. 2023. doi:10.1016/j.jtha.2023.12.027
13. Zhang W, Li K, Poon MC, et al. Women and girls with haemophilia: a retrospective cohort study in China. Haemophilia. 2023;29(2):578–590. doi:10.1111/hae.14740
14. Xing S, Batt K, Kuharic M, et al. Evaluation of clinical characteristics, health care resource utilization, and cost outcomes of hemophilia A carriers and noncarriers in the United States: a real-world comparative analysis. J Manag Care Spec Pharm. 2023;29(6):626–634. doi:10.18553/jmcp.2023.29.6.626
15. d’Oiron R, O’Brien S, James AH. Women and girls with haemophilia: lessons learned. Haemophilia. 2021;27(Suppl 3):75–81. doi:10.1111/hae.14094
16. Kulkarni R. Improving care and treatment options for women and girls with bleeding disorders. Eur J Haematol. 2015;95(suppl 81):2–10. doi:10.1111/ejh.12580
17. Women and girls with hemophilia - eLearning Platform. Available from: https://elearning.wfh.org/elearning-centres/women-and-girls-with-hemophilia/?.
18. Dardik R, Janczar S, Lalezari S, et al. Four Decades of Carrier Detection and Prenatal Diagnosis in Hemophilia A: historical Overview, State of the Art and Future Directions. Int J Mol Sci. 2023;24(14):11846. doi:10.3390/ijms241411846
19. Notice of the General Office of the National Health Commission on the Publicity Day of 2022 (National Health Office No.66,2022); 2022.
20. Bettinghaus EP. Health promotion and the knowledge-attitude-behavior continuum. Prev Med. 1986;15(5):475–491. doi:10.1016/0091-7435(86)90025-3
21. Zheng S, Zhao L, Ju N, et al. Relationship between oral health-related knowledge, attitudes, practice, self-rated oral health and oral health-related quality of life among Chinese college students: a structural equation modeling approach. BMC Oral Health. 2021;21(1):99. doi:10.1186/s12903-021-01419-0
22. Boardman FK, Hale R, Gohel R, Young PJ. Preventing lives affected by hemophilia: a mixed methods study of the views of adults with hemophilia and their families toward genetic screening. Mol Genet Genomic Med. 2019;7(5):e618. doi:10.1002/mgg3.618
23. Punt MC, Aalders TH, Bloemenkamp KWM, et al. The experiences and attitudes of hemophilia carriers around pregnancy: a qualitative systematic review. J Thromb Haemost. 2020;18:1626–1636. doi:10.1111/jth.14825
24. Babington-Ashaye A, Diop S, Geissbuhler A, de Moerloose P. Unravelling the knowledge, beliefs, behaviours and concerns of Persons with Haemophilia and their carriers in Senegal. Haemophilia. 2020;26(5):840–846. doi:10.1111/hae.14040
25. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
26. Birt L, Scott S, Cavers D, et al. Member Checking: a Tool to Enhance Trustworthiness or Merely a Nod to Validation? Qual Health Res. 2016;26(13):1802–1811. doi:10.1177/1049732316654870
27. Braun V, Clarke V. Using Thematic Analysis in Psychology. Qual Res Psychol. 2006;3:77–101. doi:10.1191/1478088706qp063oa
28. World Medical Association. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194. doi:10.1001/jama.2013.281053
29. Han PKJ, Umstead KL, Bernhardt BA, et al. A taxonomy of medical uncertainties in clinical genome sequencing. Genet Med. 2017;19(8):918–925. doi:10.1038/gim.2016.212
30. Huang Z, Nicholas S, Yang Y, et al. Medical costs and hospital utilization for hemophilia A and B urban inpatients in China: a national cross-sectional study. BMC Health Serv Res. 2022;22(1):230. doi:10.1186/s12913-022-07626-x
31. Chen Y, Cheng SJ, Thornhill T, et al. Health care costs and resource use of managing hemophilia A: a targeted literature review. J Manag Care Spec Pharm. 2023;29(6):647–658. doi:10.18553/jmcp.2023.29.6.647
32. Rysst Gustafsson S, Eriksson I. Quality indicators in telephone nursing - An integrative review. Nurs Open. 2021;8(3):1301–1313. doi:10.1002/nop2.747
33. Jin M, Liu L, Tong D, et al. Evaluating the Spatial Accessibility and Distribution Balance of Multi-Level Medical Service Facilities. Int J Environ Res Public Health. 2019;16(7):1150. doi:10.3390/ijerph16071150
34. Vanderlaan J, Edwards JA, Dunlop A. Geospatial variation in caesarean delivery. Nurs Open. 2020;7(2):627–633. doi:10.1002/nop2.433
35. Yang R. Reflections on diagnosis and treatment of hemophilia in China. Chine J Thrombosis Hemostasis. 2022;28(5):1135–1138. doi:10.3969/j.issn.1009-6213.2022.05.001
36. Medical and Scientific Advisory Council (MASAC) of the National Hemophilia Foundation (NHF). MASAC Document 264 - MASAC Recommendations Regarding Diagnosis and Management of Inherited Bleeding Disorders in Girls and Women with Personal and Family History of Bleeding; 2023.
37. Qu B, Hou Q, Men X, et al. Research and application of KABP nursing model in cardiac rehabilitation of patients with acute myocardial infarction after PCI. Am J Transl Res. 2021;13(4):3022–3033.
38. Gomez K, Laffan M, Keeney S, et al. Recommendations for the clinical interpretation of genetic variants and presentation of results to patients with inherited bleeding disorders. A UK Haemophilia Centre Doctors’ Organisation Good Practice Paper. Haemophilia. 2019;25(1):116–126. doi:10.1111/hae.13637
39. Walters R, Leslie SJ, Polson R, et al. Establishing the efficacy of interventions to improve health literacy and health behaviours: a systematic review. BMC Public Health. 2020;20(1):1040. doi:10.1186/s12889-020-08991-0
40. Hallowell N. Doing the right thing: genetic risk and responsibility. Sociol Health Illn. 1999;21:597–621. doi:10.1111/1467-9566.00175
41. Grant AM, Teijlingen ERV, Forrest-Keenan K, et al. Does breast cancer genetic counselling meet women’s expectations? A qualitative study. Crit Public Health. 2006;16:281–293. doi:10.1080/09581590601089038
42. James CA, Hadley DW, Holtzman NA, Winkelstein JA. How does the mode of inheritance of a genetic condition influence families? A study of guilt, blame, stigma, and understanding of inheritance and reproductive risks in families with X-linked and autosomal recessive diseases. Genet Med. 2006;8(4):234–242. doi:10.1097/01.gim.0000215177.28010.6e
43. Negri L, Buzzi A, Aru AB, et al. Perceived well-being and mental health in haemophilia. Psychol Health Med. 2020;25(9):1062–1072. doi:10.1080/13548506.2020.1717556
44. Sheridan N, Thompson B, Lichten L, et al. The emotional experience of mothers of children with haemophilia: maternal guilt, effective coping strategies and resilience within the haemophilia community. Haemophilia. 2023;29(2):513–520. doi:10.1111/hae.14746
45. Fisher CL, Maloney E, Glogowski E, et al. Talking about familial breast cancer risk: topics and strategies to enhance mother-daughter interactions. Qual Health Res. 2014;24(4):517–535. doi:10.1177/1049732314524638
46. McClaren BJ, Delatycki MB, Collins V, et al. ‘It is not in my world’: an exploration of attitudes and influences associated with cystic fibrosis carrier screening. Eur J Hum Genet. 2008;16(4):435–444. doi:10.1038/sj.ejhg.5201965
47. Hughes L, Phelps C. ”The bigger the network the bigger the bowl of cherries.”: exploring the acceptability of, and preferences for, an ongoing support network for known BRCA 1 and BRCA 2 mutation carriers. J Genet Couns. 2010;19(5):487–496. doi:10.1007/s10897-010-9300-6
48. Chaigneau M, Botros M, Grabell J, et al. Challenges and knowledge gaps facing hemophilia carriers today: perspectives from patients and health care providers. Res Pract Thromb Haemost. 2022;6(6):e12783. doi:10.1002/rth2.12783
49. Torres-Ortuño A. Hemophilia carriers: quality of life and management at different life stages. Blood Coagul Fibrinolysis. 2020;31(1S):S12–S14. doi:10.1097/MBC.0000000000000988
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.