Back to Journals » Risk Management and Healthcare Policy » Volume 15
Exploring Enablers and Barriers to Utilize Printed Information, Education, and Communication Materials Among Healthcare Providers of North Shoa Zone, Oromia, Ethiopia
Received 29 January 2022
Accepted for publication 28 June 2022
Published 5 July 2022 Volume 2022:15 Pages 1303—1313
DOI https://doi.org/10.2147/RMHP.S360417
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Haiyan Qu
Tinsae Abeya Geleta, Berhanu Senbeta Deriba
Department of Public Health, College of Health Sciences, Salale University, Fitche, Ethiopia
Correspondence: Tinsae Abeya Geleta, Email [email protected]
Background: Information, education, and communication (IEC) materials have paramount relevance in primary health care which mainly focused on disease prevention and control. They are a cost-effective approach for achieving better health outcomes in all clinical and public health interventions. This study aimed to explore enablers and barriers to utilize printed IEC materials among healthcare providers of North Shoa Zone, Oromia, Ethiopia, 2020.
Methods: A descriptive, qualitative study was conducted from December 1, 2020, to December 30, 2020, among health care providers. A judgmental sampling technique was used and 20 key informants were recruited considering their educational level, professional categories, working units, work experience, and types of health facilities. The data were collected by using a semi-structured interview guide. The transcribed data were uploaded into ATLAS. ti version 7.5.18 software. Then, the inductive process of thematic analysis was employed and the data were coded, categorized, and thematized. Direct quotations were presented with a thick description of the findings.
Results: The findings of the study were discussed under four themes of enablers and four themes of barriers. The four themes of enablers were availability of printed IEC materials, distribution of printed IEC material, perceived usefulness of printed IEC materials, and support from the non-government organization. The four themes of barriers were printed IEC materials-related factors, patients related factors, health care provider’s related factors, and government-related factors.
Conclusion: In this study, we found that the utilization of IEC materials was influenced by a number of facilitators and barriers. Thus, all concerned bodies need to give due attention to IEC materials and work towards the improvement of the quality of IEC materials, provide training for health care providers, work to increase the availability of IEC materials, and distribute them to the health facilities.
Keywords: IEC materials, utilization, health care providers, Ethiopia
Introduction
Many low and middle-income countries including Ethiopia are suffering from the double burden of communicable and non-communicable diseases.1,2 The majority of these can be due to behavioral factors which cannot be overcome by taking medication and call for the need for health education at the individual, group, and community level.3,4 It was recognized as the most essential component of primary health care to reach the goal of “health for all”.5 Patient education is a critical idea that helps to enhance the quality of care at lower costs and encourages people to establish preventive behaviors, take precautions to avoid health problems, and improve their self-care.6,7
For effective communication and to bring the desired behavioral change health communicators have to be guided by health learning materials such as printed materials, audio, and audiovisuals.8 Printed materials such as posters, leaflets, flipcharts, can be found in a variety of places such as hospitals, public libraries, grocery stores, fire stations, schools, drug stores, local health departments, and online.9
A number of negative outcomes occur due to ineffective communication and inappropriate utilization of health learning materials. For instance, About 40–80% of the medical information provided by healthcare practitioners is quickly forgotten.10 Furthermore, patients remember as little as 20% of the information given to them during a 5-minute consultation, and nearly half of what they remember is incorrect.11
Health learning materials have been recognized as one of the practicable and cost-effective approaches that can be used in addressing a wide range of determinants of health, risk factors and to achieving better health outcomes in all clinical and public health interventions.12,13 Health learning materials are commonly thought to be an effective technique of achieving fundamental health education and promotion objectives such as raising public awareness, the quick reach of information, counteracting rumors/doubts and misconceptions, providing detailed facts, improving skills, communicating risks, supplementing messages presented verbally during interpersonal communications, reminding for key messages, increasing retention, encouraging the target audience, increasing self-efficacy, building trust, assisting community sensitization and mobilization and reducing costs, and ultimately bringing the desired behavioral change14–16 For instance, evidence showed that providing additional text information after consultations can increase retention by up to 50%17 which implies the relevance of health learning materials for effective communication. Thus, health practitioners are recommended to employ health learning materials as their primary teaching.8,18,19 This study was aimed to explore enablers and barriers to printed information education and communication material utilization among health care providers in the north Shoa zone. The findings from this study have input for Governmental and non-governmental organizations and health professionals. Indeed, it also serves as a baseline for other researchers study conducted studies on the related topic.
Methods
Study Design, Setting, and Period
A descriptive qualitative study was conducted from 1 to 30 Dec 2020 in the North Shoa zone, Oromia region, Ethiopia. The North shoa zone has a total area of 10,322.48 Km square with 138.66 population density. The zone has 13 rural districts and two town administrations. Fiche town, the capital of the zone is located 112 km away from Addis Ababa, the capital city of Ethiopia, in the North direction. The zone has sixty-four health centers and five public hospitals (two general and three primarily hospitals) that provide health care services for the community. In this study, we have included three hospitals (Fitche general hospital, Kuyu general hospital, and Gudo Meskel primarily hospital) and three health centers (Fitche number one health center, Kuyu health center, and Muketuri health center).
Sampling Approaches and Population
A judgmental sampling technique was employed to recruit key informants. The authors judged to include diversified key informants in order to elicit rich ideas and insight into the issue considering some factors such as their educational level, professional types, Working facilities and units, and work experiences. Accordingly, a total of 20 key informants (10 from hospitals, 8 from health centers, and 2 from zonal and woredas bureau) participated in the study. Of the 20 key informants; 8 were Nurses, 5 public health, 3 medical doctors, and 4 midwives. The key informants were recruited from different working units such as the maternal and child health care unit, outpatient department (OPD), and chronic follow-up units. The recruitment was conducted 7 day/s back before the actual date of interviews. The date, site, and time of interviews were decided after discussion with the key informants considering their workload and convenience for interviews. Before starting the interview, the participants were informed of the objectives and significance of the study. Then written consent was obtained to precede the interview. After obtaining permission from the health facility leaders, the interview was conducted in the health facility’s free room and restricted personal movement area.
Data Collection
The data were collected by using a semi-structured interview guide. The interview guide was developed after reviewing relevant literatures and considering the objective of the study.20–22 The guide was first prepared in English and translated into local languages Afan Oromo and Amharic. The interview guide contains A) Background characteristics of the respondents, B) awareness, and utilization of health learning materials, and C) Barriers related to health learning materials utilization such as government and policy-related factors, health facility-related factors, and health professional-related factors. The guide has open-ended questions which were sequenced from general to specific. The main questions were followed by probing questions for further exploration. The voices of the key informants were recorded using a voice recorder. Indeed, field notes were taken on core points and non-verbal communications. The interviews were conducted by the principal investigator. Rapport was conducted before starting the interviews. KIIs were conducted averagely for 30 minutes.
Data Analysis
First, the audio recorded data were transcribed verbatim and then translated from local languages into English. The translated data were uploaded into Atlas.ti version 7.5.18 software for data management and analysis. The researcher used an inductive approach of thematic analysis to identify a set of key themes that captured the different perspectives and sentiments revealed by participants. Before the actual coding began, the investigators read and reread all the transcripts several times to become familiar with the data. The transcripts were read by the principal investigator and qualitative experts before the actual coding began in order to identify important topics and create a code book. To improve inter-coder reliability, the coders each used the code book independently and disparities in coding were solved by discussion. After that, a final edition of the code book was developed. Then, each transcript was coded line by line by principal investigators and qualitative expert. Codes were collated into meaningful groups to identify categories and major themes. For each theme and category, the coded transcripts were further analyzed and summarized in narratives. As findings, direct quotations were supplied alongside the detailed explanation.
Trustworthiness
Interview guides were evaluated by qualitative experts from Salale University. Before the actual data collection, the interview guide was pre-tested on two participants at Sandafa Bake hospital. Then, the tool was modified based on the pre-test findings.
The methodology section clearly stated the general research procedure, study setting, and study participant characteristics in order to maintain transferability. Between each question, probing interview techniques were employed to better understand the barriers related to IEC material utilization. The interviews were recorded using a tape recorder, and field notes were taken by the data collector. Finally, the thick description was done.
Various strategies were utilized to maintain conformability. Self-reflection and bracketing were the first techniques used by the researchers. The study’s lead investigator is a public health specialist with a master’s degree in health promotion and behavior. In addition, the principal investigators have extensive qualitative research experience. In order to properly address the research question, this experience and specialty were essential.
The other technique was peer debriefing, which was carried out by a qualitative specialist from Salale University’s Department of Public Health and focused mostly on qualitative data coding and analysis. Last but not least, there was prolonged involvement. Staying in the research location for a long time resulted in sustained involvement. The principal investigator confirmed the points mentioned in the KIIs throughout this time. At the end of each interview, the investigators summarized all sections and invited the key informants to whether the summaries were fit with their own ideas which contribute to member checking. In addition, we attempted to improve the quality of this study through a variety of methods, including obtaining an ethical letter from the Salale University ethical review community, an approval letter from the North Shoa Health Bureau, and permission letters from all selected health facilities. The data was collected until ideal saturation and then analyzed by qualitative experts using qualitative data analysis protocols.
Ethical Approval and Participants’ Consent
Ethical clearance was obtained from the Ethical Review Committee of Salale University. A letter of support was obtained from the North Showa Zone health office, as well as official permission from the selected hospitals and health centers. After explaining the aim and benefits of the study, the participants signed a permission form to indicate their desire to participate. In addition, permission to audio-record conversations was obtained before data collection. The respondents were informed that they had the right to refuse or terminate the interview at any time. We have anonymized all quotes and names in this manuscript. All participants have provided written consent to publish anonymised quotes. The responders’ information was kept private.
Results
Background Characteristic of the Participants
There were a total of 20 participants in this study. Half of the participants were in the age groups of 31 to 35 years. A majority of them were first degree in terms of educational status and had work experiences of greater than 5 years (Table 1).
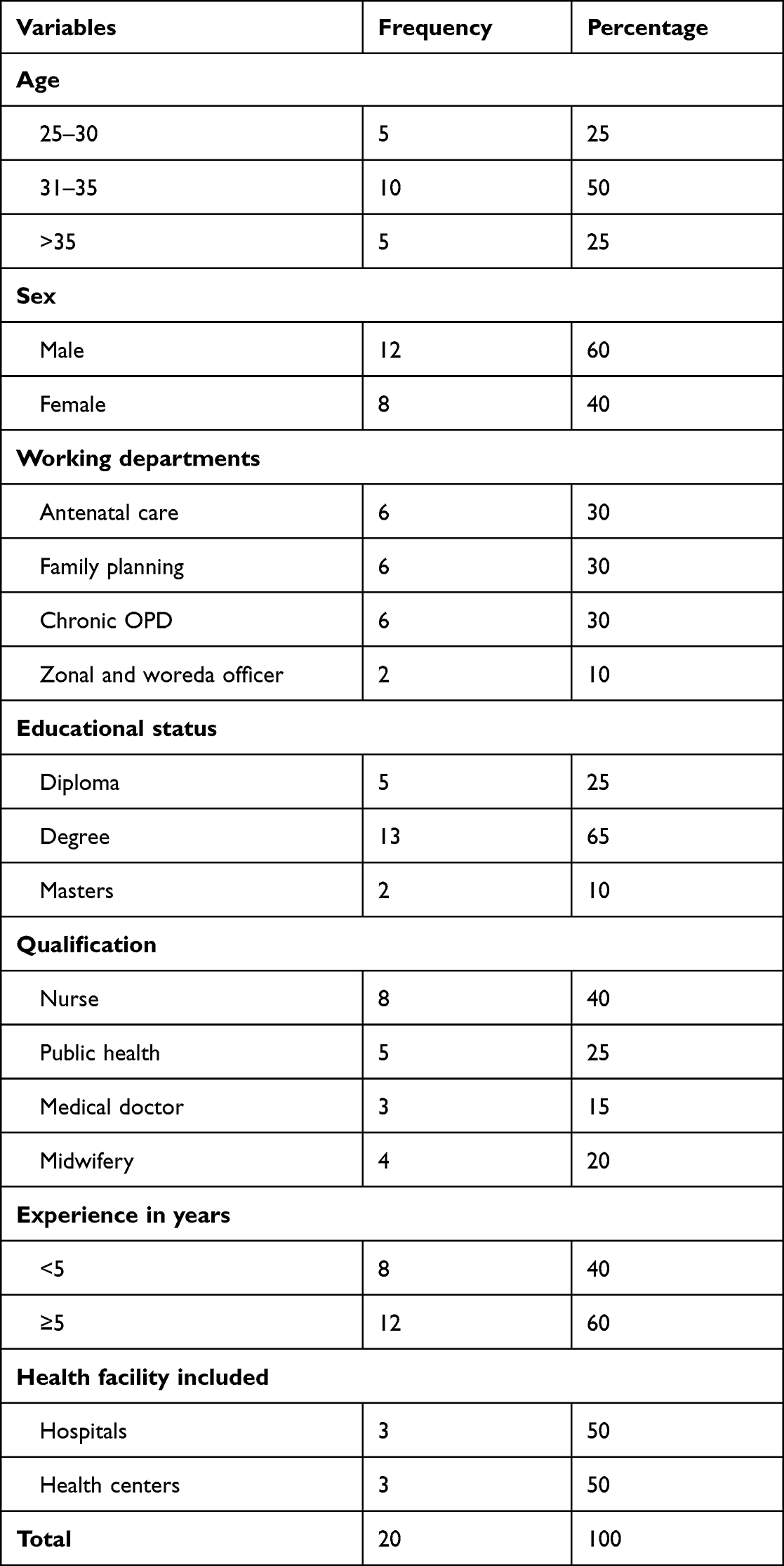 |
Table 1 Sociodemographic Characteristics of the Study Participants to Explore Enablers and Barriers to Printed Information Education and Communication Material Utilization Among Health Care Providers in the North Shoa Zone |
Enablers to Utilize printed IEC Materials
The findings of this study were discussed under four major themes: Availability of health learning materials, distribution of printed IEC materials, perceived usefulness of printed IEC materials, and support from the non-government organization.
Availability of printed IEC Materials
The participants respond to different information education and communication materials utilized at the North Shoa zone health facility. Accordingly, posters, flipcharts, brochures, leaflets, cards, charts, and books are the commonly utilized IEC materials in the North Shoa health facility. An interviewee said that:
During the counseling service in the ANC room, I frequently use flip charts. When I give service at the youth health service area a lot of interesting posters available and I utilized them. (32 years old, women, KII participants)
The other interviewee also said that:
At our health center, we frequently used printed IEC materials such as cards, posters, brochures, leaflets, and protocol charts. (30 years old male, KII participants)
Distribution of printed IEC Materials
Most of the key informants mentioned the health learning materials were distributed to different areas both in and out of health facilities. Accordingly, the antenatal care room, family planning room, delivery room, emergency room, and youth service are the most frequently mentioned areas. One of the KII participants said that:
Most of the time, printed IEC materials are distributed at family planning and antenatal care units. For instance, I regularly access posters and flipcharts related to antenatal care services, which enhance the utilization of health learning materials. (36 years old, male, KII participants)
The other interviewee also said that:
Currently, the government and non-government focus areas are MCH, so different printed IEC materials are easily distributed for family planning and antenatal care unity. As a result, health care providers who work in family planning and ANC frequently access and practice the materials. (42 years old, female, KII participants)
Perceived Usefulness of Printed IEC Materials
Findings pointed out that health care providers’ perception has an influence on health learning materials utilization. The majority of respondents stated that health learning materials have paramount relevance to delivering health information, increasing health service utilization, reducing medical errors, serving as a guideline, obtaining updated information, and serving as a reference. An interviewee said that:
Information education and communication materials are important to deliver health education, reduce medical errors, serve as a guideline, and also provide updated information. (32 years old, male, KII participants)
The other interviewee also said that:
Information education and communication materials have a variety of advantages. For instance, it is critical to provide health information and increase healthcare utilization. The community preferred to learn through observation. (32-year-old male, KII participants)
Support from a Non-Government Organization
The other theme that emerged as enablers to utilize printed IEC was the availability of strong support from the non-government organization. Most of the KII participants were said that different printed IEC materials were available easily at antenatal care and family planning due to support from the different non-government organizations and routine supervision from the donated organization. An interviewee said that:
Most of the time, the IEC materials I utilized in this room (antenatal care) were donated by non-government organizations …. MCH department does not need any support from the government; all materials are available from non-government organizations. (35 years old, female, KII participant)
The other interviewee also said that:
A lot of printed IEC materials supplied by different NGOs. Different health education providing materials are available in this family planning room and I frequently used the materials for counseling the clients. (37 years old, female, KII participants)
Barriers to Utilize Printed IEC Materials
Barriers to utilize health learning materials were explored and categorized under four major areas as follows (Table 2)
 |
Table 2 Themes and Categories Emerged from Qualitative Data Analysis as Barriers to Utilize Printed IEC Materials |
Theme One: Printed IEC Materials-Related Factors
Findings obtained from key informants indicated that language barriers, lack of appropriate health learning materials, and unavailability of health learning materials diminished their utilization.
Language Barriers
The first category that emerged under material-related factors was language barriers. Most of the KIIs raised language problems as a major factor. The majority of the participants said that the IEC materials were prepared in federal and national languages. One of the participants said that:
Most of the IEC materials are prepared in federal and international languages. The majority of our clients are Afan Oromo speakers, making it extremely difficult to use that material for this community. (30 years old, male, KII)
The other interviewee also said that:
Language barriers are the most significant impediment to effectively utilizing IEC material. The majority of the printed IEC material is prepared in federal and international languages. The majority of our clients and health professionals are not fluent in the federal language. (28 years old, women, KII participants)
Lack of Appropriate Printed IEC Materials
The other category that has emerged under this theme is the lack of appropriate materials. Most of the study participants said the lack of appropriate materials for different departments was the major factor in not utilizing IEC materials. The majority of the participants said the printed IEC materials were prepared for specific departments only.
Most of the IEC material supplied by the zonal health office is focused on HIV/AIDS and family planning only. (30 years old, male, KII participant)
The magnitude of the problems is not high, but sometimes the lack of appropriated printed IEC materials is the main problem of not utilizing IEC materials. (32 years old, male, KII participant)
Theme Two: Patients-Related Factors
Patient Lack of Interest to Learn from IEC Materials
A patient’s lack of interest in learning from IEC materials is one category that has emerged under the patient-related factors theme. According to KII participants, the main reasons for not using IEC materials are a lack of interest by both educated and uneducated clients/patients, lack of interest to learn from printed IEC materials, and time constraints to attend health education sections. One of the interviewees said:
People who are educated are more concerned with service than with health education, and they do not want to learn health information from flipcharts … Uneducated people are more interested in learning from IEC materials. (42 years old, women, KII participants)
The other interviewee also said that:
It is difficult to claim that all clients are eager to learn from IEC materials. The majority of those who attend formally educated clients are less eager to learn from IEC material due to time constraints. (31 years old male, KII participants)
In contrast, some of the KII participants said that some groups of clients/patients were more interested in learning from the IEC materials.
Especially in the youth health service area, young people prefer to learn from printed IEC such as brochures and posters. (32 years old, women, KII participants)
Theme Three: Health Care Providers-Related Factors
Work Overload
The job burden is one of the categories that has emerged from the health professional-related factors. The KII participants raise different factors for not utilizing IEC materials related to job burdens. Accordingly, the shortage of health professionals, delivering service in different rooms, and lack of time are the main factors in not utilizing IEC materials. An interviewee said that:
In our health facility, most of the health care providers have not utilized IEC materials due to job burden, but in another area, it is related to negligence. (42 years old, women, KII participant)
Some health professionals regarded IEC material utilization as an additional workload and ignored it. In my opinion, IEC material utilization reduces job burden. (28 years old, male, KII participant)
Lack of Knowledge and Training About Printed IEC Materials
In the interviews conducted with health professionals, it was identified that lack of knowledge and training can contribute to printed IEC materials not being used. The main reasons given by the interviewees were a lack of knowledge about the importance of IEC materials and a lack of training about printed IEC materials.
The KII participants said that:
In my opinion, failing to use printed IEC material was due to a lack of training and knowledge about the importance of IEC material. It is preferable if the government provides guidance on the IEC’s material importance. (32 years old, women, KII participants)
In fact, poor use of printed health learning materials is associated with a lack of training; for example, STIs/STDs are not treated by all health professionals; trained professionals are required to understand what is found on the charts. (36 years old, male, KII participants)
Attitude Towards Printed IEC Materials
Under this theme, the other category that emerged was the attitude towards printed IEC materials. Most of the KII participants said that the majority of the health professionals perceived the utilization of printed IEC material as an unnecessary activity, an additional job, perceived as useless for the clients, and a neglected issue by the care providers.
The KII participants said that:
Most health professionals preferred mobile (soft copy) IEC material overprinted IEC material or hard copy of books and leaflets. Failure to use printed IEC material is associated with health professionals’ negligence. (27 years old, women, KII participants)
The reason health professionals do not utilize printed IEC material is related to a lack of interest and ignorance. (36 years old, male, KII participants)
Theme Four: Government-Related Factors
The fourth theme identified under barriers to using printed IEC materials was poor government concerns about printed IEC materials. Finally most of KIIs participants mention lack of training on IEC materials, lack of regular auditing (weak service quality control), health facilities being poorly concerned, poor supervision, poor integration with NGOs, and a shortage of IEC materials, which were associated with IEC materials, not utilization. Interviewees said that:
IEC material utilization is primarily poor when it comes to health care facilities. Health facilities regularly collect medical equipment, but they do not collect IEC materials for health education. (40-year-old male, KII participant)
The main problem with not utilizing IEC materials is related to poor supervision of health professionals and a lack of auditing. (36 years old, male, KII participant)
The other interviewee also said that:
Most of the time printed IEC material was dumped at the store and wasted without utilization. The main factors for this wastage are due to lack of need assessment and follow-up by the concerned body (federal minister of health). (37 years old, women, KII participant)
Discussion
The study aimed to explore enablers and barriers to utilize printed IEC materials among healthcare providers of North Shoa Zone, Oromia, Ethiopia. In this study, eight themes: availability of printed IEC materials, distribution of printed IEC material, perceived usefulness of printed IEC materials, and support from non-government organization themes were emerged as enablers to utilize printed IEC materials and also printed IEC materials related factors, patients related factors, health care provider’s related factors, and government-related factors were emerged as barriers to utilize printed IEC materials.
This study identified that posters, flipcharts, brochures, leaflets, cards, charts, and books were commonly utilized printed IEC material in the study area. This implies that most professions at the hospital in North Shoa used posters, flipcharts, brochures, and leaflets regularly. This finding was in line with the previous study conducted in the Jimma zone.20 The previous study showed that posters, leaflets, and brochures were the common printed materials practice in the Jimma zone. This study finding revealed that most health professionals utilized printed IEC material at antenatal care room, family planning room, delivery room, emergency room, and youth service area. This finding indicated that the majority of the professionals utilized printed IEC material in the maternal and child health area. This finding was contradicted with the previous study conducted in Saudi Arabia. The majority of the clients read printed IEC material at the patient waiting area.23 To improve the utilization area or to involve all professionals, the health facility and health education focal person should work on the availing IEC material at each department, and patient waiting areas and routine supervision should be important.
This study finding shows that the language barrier and lack of appropriated IEC materials were the main factors for not utilizing IEC materials. This finding implies that the lack of appropriate IEC materials for different OPD and wards and lack of local language prepared printed IEC materials in the health facility are the main factors for not utilizing IEC materials by health professionals. This finding was in line with the studies conducted in different areas.24–27 In the study area, the majority of the local community and health professionals’ first language is Afan Oromo, therefore it is better if it is prepared in the local language to teach and learn from the materials. In Ethiopia, the majority of the IEC materials are prepared by the federal minister of health. The minister should consider the local language during developing IEC materials and also prepare different messages for different OPD and wards to deliver different messages to the clients.
The other factor identified in this study was the patient’s lack of interest in learning from printed IEC materials. This finding indicated that clients visiting health facilities for different services were less interested in learning from the printed IEC materials due to their giving more intention to the service other than health education. This finding was in line with the previous study conducted in Saudi Arabia.23 The previous study revealed that patients preferred direct contact with healthcare providers. According to health promotion science, printed IEC materials such as posters and flipcharts were important for providing health information to both uneducated and educated people regardless of educational status, but uneducated people preferred pictures and educated people preferred written messages such as leaflets and brochures most of the time. Our study finding indicated that majority of the health professional were used posters and flipchart.
This study revealed that health professional-related factors (lack of knowledge about printed IEC materials, lack of refreshment training on printed IEC materials and job burdens of health care providers) were the other factors that hinder the utilization of printed IEC materials. This finding implies that health professionals’ lack of refreshment training on printed IEC materials, as well as the professional’s job burden, were the primary reasons for not using printed IEC materials. This finding was in line with the previous study conducted in Saudi Arabia.22 The previous study findings revealed that the nursing professionals were less concerned about behavioral change communication due to a lack of refreshment training and the need to give priority to acute disease. Another study conducted in Texas discovered that job burdens were the primary cause of poor health promotion practice.28
Finally, this study discovered that a lack of government concern for IEC materials is another factor impeding the use of IEC materials among health professionals. This finding suggests that the government is unconcerned about printed IEC material preparation, distribution, and utilization, as well as providing refresher training on IEC materials to health care providers. This finding was in line with the study conducted previously at the Jimma zone.20 This finding was contradicted the Ethiopian minister of health policy direction,
Information, Education, and Communication of Health shall be given the appropriate importance to enhance health awareness and to propagate the important concepts and practices of self-responsibility in health.29
Conclusion and Recommendation
Generally, this study identified material-related factors, patients’ related factors, health professional-related factors, and government-related factors were identified as factors that hinder the utilization of printed IEC materials. Therefore, to increase utilization of IEC materials effort will be needed from the minister of health, Oromia health bureau, zonal health bureau, health facility, and health professional. The public health professional especially health promotion and health behavioral experts should work on the advocacy of IEC materials to improve the government’s poor concerns. The federal government should avail printed IEC material regularly and should consider local language during preparing IEC material. Additional regional governments should provide training focusing on the importance of IEC material utilization. Zonal health bureau and health facility should establish strong linkage on IEC material distribution and collection. The non-government organization should concede the local language during preparing IEC materials and should focus on capacity building.
Data Sharing Statement
The data sets used and analyzed during the current study are available from the corresponding author on a reasonable request.
Ethics and Consent Statement
The study conforms with the principles outlined in the Declaration of Helsinki.30 Ethical clearance was obtained from the Ethical Review Committee of Salale University. A letter of support was obtained from the North Showa Zone health bureau, as well as official permission from the selected hospital. After explaining the study’s aim, the respondent signed a permission form to indicate his or her desire to participate. The respondents were informed that they had the right to refuse or terminate the interview at any time. We have anonymized all quotes and names in this manuscript. All participants have provided written consent to publish anonymised quotes. The responders’ information was kept private.
Acknowledgments
First of all, we would like to praise our God for His help in each step of our life and this development of the proposal. Next, we thank the Salale University Research and Community Service Coordinator’s Office for arranging this opportunity. Finally, we acknowledge the health facilities from which the data were collected and the study participants for their cooperation.
Author Contributions
All authors made a significant contribution to the conception, study design, execution, and acquisition of data, analysis, and interpretation. All authors were involved in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The Salale University supported this research work. The sponsors had no role in study design, data collection, analysis, decision to publish, or manuscript preparation.
Disclosure
The authors declare that they have no conflicts of interest in relation to this work.
References
1. Boutayeb A. The double burden of communicable and non-communicable diseases in developing countries. Trans R Soc Trop Med Hyg. 2006;100(3):191–199. doi:10.1016/j.trstmh.2005.07.021
2. Bygbjerg IC. Double burden of noncommunicable and infectious diseases in developing countries. Science. 2012;337(6101):1499–1501. doi:10.1126/science.1223466
3. Israel BA, Checkoway B, Schulz A, Zimmerman M. Health education and community empowerment: conceptualizing and measuring perceptions of individual, organizational, and community control. Heal Educ Behav. 1994;21(2):149–170.
4. McAlister AL, Perry CL, Parcel GS, Read M, McDevitt-Murphy M, Ward K. How individuals, environments, and health behaviors interact. Health Behav Health Educ. 2008;39(2):91–94. doi:10.1080/19325037.2008.10599020
5. WHO-Unicef. Alma-Ata primary health care. In:
6. Hoffmann T, Worrall L. Designing effective written health education materials: considerations for health professionals. Disabil Rehabil. 2004;26(19):1166–1173. doi:10.1080/09638280410001724816
7. Griffin J, McKenna K, Tooth L. Written health education materials: making them more effective. Aust Occup Ther J. 2003;50(3):170–177.
8. Leep Hunderfund AN, Bartleson JD. Patient education in neurology. Neurol Clin. 2010;28(2):517–536. doi:10.1016/j.ncl.2009.11.002
9. Shieh C, Hosei B. Printed health information materials: evaluation of readability and suitability. J Community Health Nurs. 2008;25(2):73–90. doi:10.1080/07370010802017083
10. Kessels RPC. Patients’ memory for medical information. JRSM. 2003;96(5):219–222. doi:10.1258/jrsm.96.5.219
11. Neeman N, Isaac T, Leveille S, et al. Improving doctor-patient communication in the outpatient setting using a facilitation tool: a preliminary study. Int J Qual Heal Care. 2012;24(4):357–364. doi:10.1093/intqhc/mzr081
12. McGinnis JM. Communication for better health. Public Health Rep. 1990;105(3):217–218.
13. Waisbord S, Larson H. Why invest in communication for immunization. Evidence Lessons Learned. 2015;15(6):28–312.
14. Best JA, Cameron R. Health behavior and health promotion. Am J Heal Promot. 1986;1(2):48–57. doi:10.4278/0890-1171-1.2.48
15. Giguère A, Légaré F, Grimshaw J, et al. Printed educational materials: effects on professional practice and healthcare outcomes. Cochrane Database Syst Rev. 2012; 4. doi:10.1002/14651858.CD004398.pub3
16. Bero LA, Grilli R, Grimshaw JM, Harvey E, Oxman AD, Thomson MA. Getting research findings into practice: closing the gap between research and practice: an overview of systematic reviews of interventions to promote the implementation of research findings. BMJ. 1998;317(7156):465–468. doi:10.1136/bmj.317.7156.465
17. Khan S, Karuppaiah K, Bajwa A. The influence of process and patient factors on the recall of consent information in mentally competent patients undergoing surgery for neck of femur fractures. Ann R Coll Surg Engl. 2012;94(5):308–312. doi:10.1308/003588412X13171221591970
18. Gal I, Prigat A. Why organizations continue to create patient information leaflets with readability and usability problems: an exploratory study. Health Educ Res. 2005;20(4):485–493. doi:10.1093/her/cyh009
19. Demir SG, Bulut H, Dal Ü. Student’s experience with developing patient education materials. Procedia. 2009;1(1):2828–2831. doi:10.1016/j.sbspro.2009.01.503
20. Birhanu Z, Godesso A, Challi Jira SM. Assessment of production and distribution of printed Information Education Communication (IEC) materials in Ethiopia and utilization in the case of Jimma assessment of production and distribution of printed information education communication (IEC) MA. Ethiopian J Health Sci. 2011;21:77–83.
21. Reeve K, Byrd T, Quill BE. Health promotion attitudes and practices of Texas nurse practitioners. J Am Acad Nurse Pract. 2004;16(3):125–133. doi:10.1111/j.1745-7599.2004.tb00383.x
22. Aldossary A, Barriball L, While A. The perceived health promotion practice of nurses in Saudi Arabia. Health Promot Int. 2013;28(3):431–441. doi:10.1093/heapro/das027
23. Haji A. Patients ’ utilisation and perception of the quality of printed health education materials in primary health care: a cross- - sectional study. BJGP Open. 2019;3(4):4–11.
24. Foster DR, Rhoney DH, Walroth TA, Buening NR, Foster DR, Sood R. Readability of printed patient information for epileptic patients RESULTS. J Burn Care Res. 2015;36(6):641–650. doi:10.1097/BCR.0000000000000191
25. Ho EY, Tran H, Chesla CA. Assessing the cultural in culturally sensitive printed patient-education materials for Chinese Americans with type 2 diabetes assessing the cultural in culturally sensitive printed patient-education materials for Chinese Americans with type 2 diabetes. Health commun. 2014;30:37–41.
26. Buller MK, Bettinghaus E, Buller DB, Liu X, Fluharty L. Perceived availability of culturally and demographically diverse photographs for Health Education Materials, Colorado, 2010. Preve Chronic Dis. 2015;12:1–3.
27. Jawad M, Halla H, Amani M, Al O. Health education materials for Arab patients: content and design preferences. Med Princ Pract. 2013;22(4):411–414. doi:10.1159/000346276
28. Reeve K, Byrd T, Quill BE. Health promotion attitudes and practices of texas nurse practitioners. J Am Acad Nurse Pract. 2020;1995:125–133.
29. FDRMOH. Transitional Government of EthiopiaThe National Population Policy of Ethiopia; 1993.
30. WMA. Declaration of Helsinki World Medical Association declaration of Helsinki. Bull World Heal Organ. 2001;79:1975.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.