Back to Journals » International Journal of General Medicine » Volume 18
Exploring Clinical and Imaging Differences in COVID-19: an Observational Approach to the IFITM3 rs12252 Polymorphism
Authors Mitrea A ![]() , Mitroi AF
, Mitroi AF ![]() , Opariuc-Dan C, Constantin AA
, Opariuc-Dan C, Constantin AA ![]() , Dantes E
, Dantes E
Received 22 December 2024
Accepted for publication 28 March 2025
Published 10 April 2025 Volume 2025:18 Pages 2077—2091
DOI https://doi.org/10.2147/IJGM.S512160
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Adriana Mitrea,1,2 Anca-Florentina Mitroi,3,4 Cristian Opariuc-Dan,5 Ancuta-Alina Constantin,6,7 Elena Dantes8,9
1Doctoral School of Medicine, “Ovidius” University of Constanta, Constanta, Romania; 2Department of Pulmonology, “Sf. Apostol Andrei” Emergency Clinical County Hospital of Constanta, Constanta, Romania; 3Pathology Department, “Sf. Apostol Andrei” Emergency Clinical County Hospital of Constanta, Constanta, Romania; 4CEDMOG Center, “Ovidius” University of Constanta, Constanta, Romania; 5Faculty of Law and Administrative Science, “Ovidius” University of Constanta, Constanta, Romania; 6Department of Cardio-Thoracic Pathology, “Carol Davila” University of Medicine and Pharmacy, Bucharest, Romania; 7Department of Cardio-Thoracic Pathology, Institute of Pneumology “Marius Nasta”, Bucharest, Romania; 8Faculty of Medicine, ‘Ovidius’ University of Constanta, Constanta, Romania; 9 1st Pneumology Department, Clinical Hospital of Pneumophtisiology, Constanta, Romania
Correspondence: Anca-Florentina Mitroi, Pathology Department, “Sf. Apostol Andrei” Emergency Clinical County Hospital of Constanta, 145 Tomis Blv, Constanta, Romania, Email [email protected]
Purpose: The severity of COVID-19 infections varies among individuals, prompting research into factors that may influence outcomes. Numerous studies have investigated the conditions that influence the intensity of illness caused by COVID-19. These factors include the Interferon-Induced Transmembrane Protein 3 (IFITM3) rs12252 polymorphism. We investigate whether the polymorphism rs12252 plays a role within our population and observe the differences in other parameters between the mild and severe forms of the disease.
Patients and Methods: The observational study examining the IFTIM3 rs12252 polymorphism based on the level of COVID-19 severity and differences between inflammatory markers. The study included 51 participants, with 31 severe and 20 mild cases.
Results: The average age of participants was 54 years, and 16.1% of patients with severe symptoms were diagnosed with the AG genotype. Patients showing serious symptoms had significantly higher ESR, CRP, Fibrinogen, LDH, and D-dimer levels than those with mild symptoms.
Conclusion: This study discovered a notable correlation between the G allele of IFITM3 rs12252, inflammatory markers, CT scan score, and COVID-19 severity.
Keywords: COVID-19, IFITM3 protein, inflammatory markers, genotype
Introduction
COVID-19 is an infectious disease caused by the novel coronavirus, SARS-CoV-2, which was first identified in December 2019 in Wuhan, China.1 The disease quickly spread worldwide, leading to the ongoing global pandemic. The clinical symptoms of COVID-19 range from mild respiratory issues to severe complications, including pneumonia, acute respiratory distress syndrome (ARDS), and multi-organ failure.2 Epidemiologically, COVID-19 has affected millions globally, with varying severity depending on factors such as age, underlying health conditions, and genetic predispositions.3
Interferon-induced transmembrane proteins (IFITMs) represent a family of small transmembrane proteins that modulate key cellular processes by limiting the intracellular entry of various enveloped viruses.4–10 The human IFITM locus contains four functional genes IFITM 1, IFITM 2, IFITM 3, and IFITM 5, and is located on chromosome 11.11 IFITM 1, 2, and 3 activated in response to stimulation by type I and II interferons and act as the first line of defense against invading pathogens.12–14 IFITM3 restricts viral fusion by amplifying the structural stiffness of endosomal membranes and accelerates the conveyance of endosomal cargo for degradation into the lysosome, decreasing the fusion rate of the viral endosome.15,16
The scientific literature on COVID-19 includes studies suggesting that IFITM3 blocks fusion with the endosomal membrane, thereby inhibiting the endocytosis of SARS-CoV-2 and the dissemination of coronaviruses including other Ribonucleic Acid (RNA) viral agents with an envelope such as Ebola, influenza and dengue virus.17–20 In the influenza virus, rs12252 (NC_000011.10:q.320772A>G) increases resistance to the disease by upregulating the expression of the IFITM3 protein.21 This observation led to the premise that genetic variation (A>G) could affect resistance to SARS-CoV-2 by impairing IFITM3 expression.22
Versions of the IFITM3 gene, especially the G alleles of a single nucleotide polymorphism (SNP) rs12252, have been frequently linked to altered immune response and heightened vulnerability to viral infections, including severe forms of COVID-19.15,23–27 The frequency of alleles varies according to population. This variability might clarify the reason why certain groups increased susceptibility to severe forms of COVID-19. It is not certain that individuals with the GG genotype are more vulnerable to severe forms of the disease and mortality than individuals with the AG or AA genotype.28
While genetic polymorphisms, including the IFITM3 rs12252 polymorphism, may play a significant role in determining COVID-19 severity, it is also essential to consider the broader context of other factors that contribute to disease outcomes. Age has consistently been shown to be a major determinant of disease severity, with older adults being at a higher risk of developing severe symptoms.29 Comorbidities such as cardiovascular diseases, diabetes, and obesity have also been identified as key risk factors for poor prognosis.30
Several factors contribute to an individual’s susceptibility to more severe forms of COVID-19. In this context, we sought to investigate the potential role of the rs12252 genetic variant in our population, and to explore how this mutation may influence disease severity, particularly by examining differences in clinical, imaging, and laboratory parameters between mild and severe COVID-19 cases.
While several studies have previously reported on the association between SNPs in the IFITM3 gene and COVID-19 severity, the specific role of the rs12252 polymorphism in COVID-19, particularly within Romanian Caucasian populations, remains unclear. This study aims to fill this gap by investigating the impact of the IFITM3 rs12252 polymorphism on the severity of COVID-19 in a cohort of 51 patients, using a combination of clinical, imaging, and laboratory data. Our findings provide a unique perspective on the role of this genetic variant, particularly in a population that has not been extensively studied in the context of COVID-19.
Multiple factors contribute to an individual’s vulnerability to advancing to more serious forms of COVID-19. Therefore, we wanted to investigate whether the gene mutation rs12252 plays a role within our population and observe the differences in other parameters between the mild and severe forms of the disease.
Material and Methods
Study Design
Our research is an observational study in which we analyzed blood samples from 51 patients. This study aimed to assess if a relationship exists between allele G of SNP rs12252 of the IFITM3 gene and the acuteness of COVID-19 symptoms in the Romanian citizens. We compared the frequency of the G allele in severe COVID-19 patients (31 cases) and mild patients (20 cases).
The blood samples were analyzed at the “Center for Research and Development for Morphological and Genetic Studies in Malignant Pathology (CEDMOG)” in Constanța. Other parameters were collected after the patient’s hospitalization at the Department of Pulmonology Constanta County Clinical Emergency Hospital “St. Apostol Andrei” and the Clinical Hospital of Pneumophtisiology Constanta.
The acceptance criteria were patients over 18 years of age (in Romania, persons over 18 are considered adults) who showed a positive result for SARS-CoV-2 in a Polymerase Chain Reaction (PCR) test.
Ethical Approval
The institutional ethics committee (“Universitatea Ovidius Constanța”, Romania, no. DCI CEDMOG 02/12.01.2022) approved this analysis. The principles of the Declaration of Helsinki were duly respected.
All patients included in the study were fully informed about the purpose of the research. Informed consent was obtained from each participant prior to their involvement in the study, ensuring they understood the study objectives and the nature of their participation. Each patient provided consent to contribute to this research. It is important to note that participants did not receive any benefits or face any secondary consequences from their participation, which was entirely voluntary and without coercion.
Data Collection
All examinations were performed in the same imaging laboratory and analyzed by the same technician. The Total Severity Score Computer Tomography (TSS) proposed by Li et al was used to quantify lung involvement. This score classifies COVID-19 cases into three categories based on lung damage: mild (TSS 0–9 points), moderate (TSS 10–17 points), and severe (TSS 18–25 points), following the international scoring system.27
In the context of this study, COVID-19 severity was categorized based on imaging criteria and clinical symptoms. Mild cases were defined as patients who experienced mild symptoms, such as fever, fatigue, or cough, without the need for hospitalization. These patients did not present with signs of severe respiratory distress or other critical complications. Severe cases were defined based on the presence of more pronounced symptoms, including significant respiratory distress, hypoxia, and the need for supplemental oxygen or mechanical ventilation, as well as findings of extensive lung involvement on chest CT imaging. By using both clinical and imaging data, we aimed to capture a more comprehensive picture of disease severity, which is particularly important when studying genetic factors like the rs12252 polymorphism.
Blood samples were taken from all patients on admission and before discharge, including: erythrocyte sedimentation rate (ESR); fibrinogen; D-dimer; lactate dehydrogenase (LDH); C-reactive protein (CRP). All samples were collected from fasting venous blood.
Sample Screening for SARS-CoV-2 Positivity Using PCR
To ensure accurate patient classification, all samples were screened for SARS-CoV-2 positivity using a PCR-based diagnostic test. Nasopharyngeal swabs were collected from all participants and processed according to standard operating procedures. All patients included in this study were confirmed to be SARS-CoV-2 positive through PCR testing.
Genotyping
Genomic Deoxyribonucleic acid (DNA) was isolated from peripheral blood collected in ethylenediaminetetraacetic acid (EDTA) vacuum vials using the PureLink Genomic DNA Mini Kit (Invitrogen,ThermoScientific, USA) according to the manufacturer`s protocol. Quantifying of DNA samples was done with NanoDrop One™ Spectrophotometer (Thermo Fisher Scientific, USA) and a ratio of ultraviolet absorbance A260/A280 = 1.7–2.0, and A260/A230 > 2 was evaluated as acceptable.
SNPs polymorphisms of IFTIM3 (rs12252, A/G) were genotyped by a real-time Polymerase Chain reaction (PCR) experiments with ready to use TaqMan® Genotyping Master Mix (Applied Biosystems) and the 40 X TaqMan® SNP Genotyping Assay (Applied Biosystems), that incorporates sequence-specific forward and reverse primers to amplify the sequence of interest and two TaqMan minor groove binder probes with nonfluorescent quenchers: VIC -marked probe is attached to the 5´ end of the Allele 1 and FAM-marked probe is attached to the 5´ end of the Allele 2 (Table 1). The DNA concentration was adjusted to range from 1 to 10 ng per 10 μL of Reverse Transcription Polymerase Chain Reaction (RT-PCR). Practically, every RT-PCR consists of 5 μL TaqMan Genotyping Master Mix (2✕), 0.5 μL of TaqMan Genotyping Assay Mix (20✕), and 4.5 μL DNA. Real time PCR experiments were performed with a 7500 Fast Real-Time System (Applied Biosystems) using the following conditions: polymerase activation at 95°C for 10 min, denaturation at 95°C for 15s, and annealing/extension at 60°C for 1 min. The last two steps, were repeated 40 times, according to previous describing protocol.31,32 Data analysis and genotyping was accomplished with the 7500 Fast Real-Time PCR Software, version 2.3. The genotyping assays are described in Table 1.
 |
Table 1 VIC/FAM Sequences of Single Nucleotide Polymorphism (SNP) Genotyping Assays |
Statistical Analysis
All study data were evaluated with IBM SPSS Statistics 25 and illustrated using Microsoft Office Excel/Word 2021. To assess normality, the Shapiro–Wilk Test was performed on the quantitative variables and reported as averages along with standard deviations or medians with interquartile ranges. Quantitative variables with normal distribution was assessed across groups using Welch`s T-Test (considering an inequality of variances between groups according to Levene`s Tests). Error plots with 95% confidence intervals for means were created to illustrate the comparisons.
The Mann–Whitney U-Test tested quantitative variables with non-parametric distribution among the groups. Comparisons were presented using box-plots, where values below the 1st quartile – 1.5*interquartile range or above the 3rd quartile + 1.5*interquartile range are considered outliers and shown as circles in the graph, while values that are below the 1st quartile −3*interquartile range or above the 3rd quartile + 3*interquartile range are considered extreme outliers and represented as asterisks symbols in the graph.
Qualitative variables were expressed as counts or expressed as percentages, and evaluated between groups Fisher’s Exact Test. A one-sided Fisher’s Exact Test was used to test the association between the COVID-19 form and the IFTIM3 genotype. Implementation of a Firth’s Bias-Reduced Logistic Regression model was made using the logistf package in R software (The R Project for Statistical Computing, version 4.4.0). The model calculated the odds of having severe COVID-19 symptoms in patients with heterogenous genotype vs homogenous genotype, while taking care of the perfect separation issue. Effect of genotype in the prediction was estimated as an odds ratio with 95% confidence interval along with the significance value. A risk ratio with a 95% confidence interval was calculated to estimate the risk of severe COVID-19 disease in patients with heterozygous genotypes compared to homozygous genotypes, and the significance of the risk ratio was estimated based on the confidence interval obtained. The threshold for the significance level was set at α = 0.05 for all tests.
Results
In this study, we aimed to explore the relationship between clinical characteristics, laboratory parameters, and the IFITM3 rs12252 polymorphism in COVID-19 patients with varying symptom severities. The analysis focused on evaluating general patient characteristics, inflammatory biomarker levels, and genetic predispositions to identify potential contributors to disease severity. These findings offer valuable insights into how clinical, laboratory, and genetic factors interplay in the progression of COVID-19, highlighting both key differences between mild and severe cases and the potential role of the IFITM3 rs12252 polymorphism in influencing outcomes. Prior to evaluating the genetic profile, we assessed the patients` general characteristics and compared the values of inflammatory biomarkers. Patient`s characteristics are shown in Table 2 and Figures 1–4.
 |
Table 2 Characteristics of the Analyzed Groups |
 |
Figure 1 Comparison of patients’ age according to COVID-19 form. |
 |
Figure 2 Distribution of the patients according to gender and COVID-19 form. |
 |
Figure 3 Comparison of patients’ BMI according to COVID-19 form. |
 |
Figure 4 Distribution of the patients according to IFTIM3 genotype and COVID-19 form. |
51 patients were analyzed: 20 patients (39.2%) with mild symptoms of COVID-19 and 31 patients (60.8%) with severe symptoms of COVID-19. The median age was 54 years (IQR = 47–66), and patients with severe symptoms had a significantly higher age (median = 62, IQR = 50–69) in comparison to those with mild symptoms (median = 46.5, IQR = 30.2–52.2) (p<0.001) (Figure 1). 45.1% (n=23) of the patients were men, being significantly more frequent in severe symptoms group (64.5%; n=20) than in the mild symptoms group (15%; n=3) (p=0.001) (Figure 2). Median Body Mass Index (BMI) was 27.5 kg/m2 (IQR = 24.2–30), patients with severe symptoms having a significantly higher value of BMI (median = 28.9, IQR = 27.7–32) in comparison to patients with mild symptoms (median = 25.1, IQR = 23.9–26.2) (p<0.001) (Figure 3). 9.8% (n=5) of the patients had a heterozygous genotype (AG), and 46 had a homozygous genotype (AA). Table 3 and Table 4 present the distribution of patients based on disease severity and sex, as well as disease severity and IFITM3 genotype (homozygous or heterozygous).
 |
Table 3 Distribution of the Patients According to Gender and COVID-19 Form |
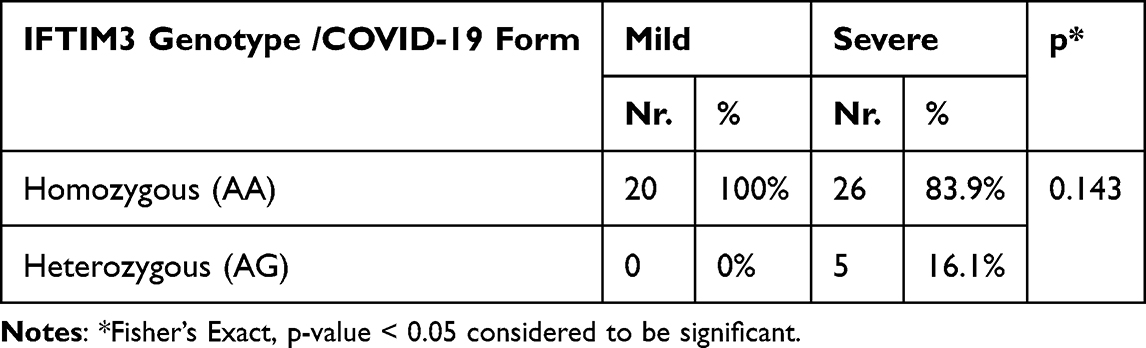 |
Table 4 Distribution of the Patients According to IFTIM3 Genotype and COVID-19 Form |
Considering the assumption that patients with severe symptoms of COVID-19 might be more associated with a heterozygous genotype, the application of a 1-sided Fisher’s Exact Test reveals a tendency toward statistical significance (p=0.072), in the direction of patients with severe symptoms having a higher frequency of heterozygous genotype (16.1%; n=5) in comparison to patients with mild symptoms (0%) (Figure 4). Using a Firth’s Bias-Reduced Logistic Regression model (because of the perfect separation issue), proves that patients with AG genotype have an increased odds of having severe symptoms of COVID-19 (OR = 2.141, 95% C.I.: −0.126–7.039, p=0.067), however the confidence interval and the associated p-value show the same result as in the existence of a tendency towards statistical significance, in this case in the direction of an increased odds of severe COVID-19. Calculation of a risk ratio in this situation showed a significantly higher risk of severe symptoms in the case of patients with heterozygous genotype (AG) (RR = 1.7692, 95% C.I.: 1.3731–2.2796, p<0.001) in comparison to patients with homozygous genotype (AA). Table 5 contains the severity score from the computed tomography examination and the corresponding genotype observed. We observe that the heterozygous form was found exclusively in severe cases of the disease, with pulmonary involvement showing a CT score above 18.
 |
Table 5 Distribution of the Patients According to Total Severity Score Computer Tomography (TSS) Value and IFTIM3 Genotype |
Laboratory parameters were compared between patients grouped according to the form of COVID-19 symptoms, as shown in Table 6 and Figures 5–10. The results show that patients with severe symptoms had higher values for Erythrocyte Sedimentation Rate (ESR) (mean = 50.58 ± 21.51 vs mean = 16.11 ± 8.63, p<0.001), fibrinogen (mean = 4.8 ± 1.79 vs mean = 3.27 ± 0.77, p=0.001), C-reactive protein (CRP) (median = 76.8, IQR = 34–130 vs median = 4.2, IQR = 0.75–8.5), Lactate Dehydrogenase (LDH) (median = 428, IQR = 297–660 vs median = 202, IQR = 161.5–215.5, p<0.001) and Total Computer Tomography lung severity -SLCT (median = 19, IQR = 17–21 vs median = 4, IQR = 3–5) compared to patients with mild symptoms of COVID-19, while the values of D-dimer did not differ significantly between the groups (p=0.332).
 |
Table 6 Comparison of Laboratory Parameters According to Clinical Presentation of COVID-19 |
 |
Figure 5 Comparison of patients’ ESR value according to COVID-19 form. |
 |
Figure 6 Comparison of patients’ fibrinogen value according to COVID-19 form. |
 |
Figure 7 Comparison of patients’ CRP value according to COVID-19 form. |
 |
Figure 8 Comparison of patients’ LDH value according to COVID-19 form. |
 |
Figure 9 Comparison of patients’ D-dimer value according to COVID-19 form. |
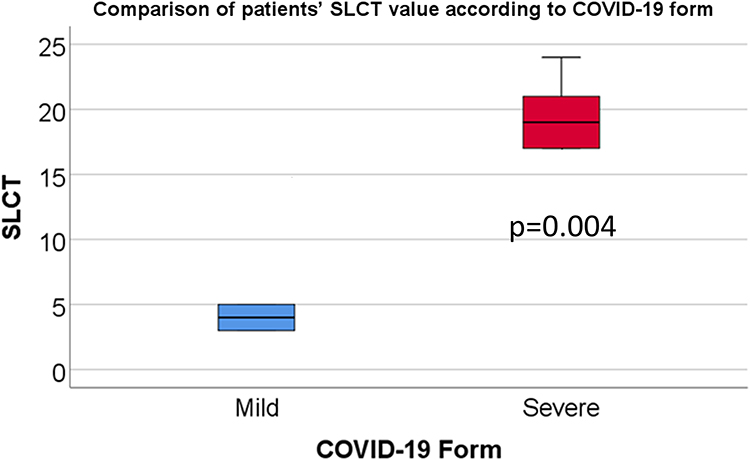 |
Figure 10 Comparison of patients’ SLCT value according to COVID-19 form. |
Discussion
A different response to viral infections can be observed among individuals, which is influenced by genetic variations of certain molecules involved in cellular entry. The severity may possibly be linked to single-nucleotide polymorphisms (SNPs), as these proteins play a crucial role in the penetration of SARS-CoV-2 into host cells and in the host’s immune response to this virus.
Our results are consistent with the findings from the existing literature.33–38 The G allele of SNP rs12252 in the IFITM3 gene has a frequency of 0.01 to 0.05 in Caucasians. This allele is correlated with higher seriousness of the condition, including COVID-19, and is less common in Caucasians compared to Africans, Americans and Asians.34
Although the allele reflects a reduced prevalence in the general population, 9.8% of the patients studied had a heterozygous genotype (AG). Moreover, all of them were patients with severe COVID-19. It is of utmost importance to mention that the G allele is rare, and its homozygosity was not identified in our study. Several studies have reported that certain polymorphisms in the IFITM3 gene, including the heterozygous genotype (AG), may be linked to altered immune responses, which can influence the severity of viral infections, including COVID-19. Specifically, a study by Chu et al demonstrated that the presence of the rs12252-C allele in the IFITM3 gene (often found in the heterozygous genotype) was associated with an increased risk of severe disease in COVID-19 patients.39 Additionally, Zhang et al found that individuals with the AG genotype exhibited a more pronounced immune response, which might contribute to heightened inflammation and, consequently, more severe symptoms of COVID-19.40
Based on three meta-analyses, the IFITM3 rs12252 gene polymorphism was found to be correlated with a higher susceptibility and severity of COVID-19.37–41 A study conducted in hospitalized COVID-19 patients in Beijing, China, detected a meaningful connection between homozygosity for the IFITM3-rs12252 allele and increased severity of COVID-19 and mortality.40 The frequency of homozygosity for IFITM3-rs12252 was similar in individuals with mild illness as in the general population. Moreover, this allele was linked to an increased likelihood of hospitalization within a cohort of COVID-19 patients in Spain.30
In our study, patients with the heterozygous AG genotype were associated with increased illness severity and lung injury, as well as in a meta-analysis by Valentina Pecoraro et al.37 However, this correlation was not observed in an Egyptian study by Sara M. Elessawy et al, which found a correlation with mortality risk, and in another study by Cuesta-Llavona E. et al which found an association between the interferon-induced transmembrane protein 3 gene (IFITM3) rs34481144 /rs12252 haplotypes and a higher risk of hospitalization.42,43
We found that age was an essential factor, with patients with more severe disease manifestations tending to be older. These outcomes are supported by similar studies that have found a tie between age and severe forms of the disease. The Centers for Disease Control and Prevention (CDC) pointed out that the elderly patients are predisposed to remain symptom-free when infected with COVID-19, but face an increased likelihood of hospitalization or cessation of life if diagnosed with the disease.44,45 In addition, both virologists and clinicians acknowledge that older adults tend to be more susceptible to COVID-19, with a strong correlation between patient age and the presence of symptoms and comorbidities.46–49
In our study, men had more serious manifestations of the disease in contrast to women, 64.5% (n=20) versus 35.5% (n=11). Epidemiologic data suggest that SARS-CoV-2 infections tend to be more severe in men than in women, leading to a higher percentage of COVID-19 related deaths and transfer to intensive care despite similar infection rates.50 Research undertaken by Gholami Melika et al, found that males showed a great tendency to have the IFITM3 rs12252 GG and AG variants and experienced a higher mortality rate compared to females.51 Several hypotheses have been proposed to explain the underlying pathophysiologic mechanisms behind this trend.52–58 One prominent hypothesis is the role of sex hormones, particularly estrogens, which are believed to provide a protective effect against viral infections in women. Estrogens have been shown to enhance immune responses, promoting the activity of immune cells such as T lymphocytes and dendritic cells, which may contribute to a stronger defense against SARS-CoV-2 in women.52 In contrast, testosterone, the primary male sex hormone, may exacerbate inflammation and promote more severe immune responses, which could result in worse clinical outcomes in men.53–57 Another hypothesis revolves around genetic factors, particularly the X chromosome, which contains many immune-related genes. Since women have two X chromosomes, they may benefit from a more robust immune response due to the presence of a second, potentially protective X chromosome. Men, with only one X chromosome, may lack this compensatory effect, leading to a weaker immune response to infections like COVID-19.58 Finally, immune system differences between men and women, such as a generally more pronounced inflammatory response in men, may play a role in determining disease severity. Men tend to exhibit higher levels of pro-inflammatory cytokines, which can contribute to more severe symptoms and complications, including acute respiratory distress syndrome (ARDS).59,60
Body mass index and inflammatory markers are also predictors of a greater chance of severe disease and more severe lung involvement, as seen on computed tomography. Numerous studies and meta-analyses in the literature have found an enhanced susceptibility to serious illness in patients with elevated body mass index. Nevertheless, the fundamental mechanisms remain incompletely understood.61–66
C-reactive protein (CRP) is an important marker for assessing lung involvement, with elevated levels being associated with poor prognosis, admission to intensive care, and increased mortality. Similarly, higher lactate dehydrogenase (LDH) activity correlates with disease progression and severity, while elevated fibrinogen levels are accompanied by more critical forms of COVID-19 and poorer treatment outcomes.67–69 LDH, a non-specific indicator of tissue damage, enters the bloodstream and has been related to disease progression and higher severity of Computed Tomography (CT) in patients infected with SARS-CoV- 2.70
Our study provides novel insights into the role of the IFITM3 rs12252 polymorphism in COVID-19 severity, particularly within a Romanian Caucasian population. Previous studies have reported on similar associations in other populations, but to our knowledge, this is the first study to examine this polymorphism in such a cohort. Additionally, the integration of clinical, imaging (chest CT scans), and laboratory data in the classification of COVID-19 severity offers a more comprehensive analysis of the impact of this genetic variant. These findings contribute to a better understanding of how the IFITM3 gene may influence COVID-19 outcomes in populations with different genetic and environmental backgrounds.
Limitations
The main limitation of this study is the restricted sample size, possibly reducing the generalizability and statistical power to detect significant associations. In addition, the study population consists exclusively of Caucasian individuals from a single geographic region, which further limits the generalizability of the results to other ethnic and geographic populations. This study also did not consider other genetic variants that interact with the SNP rs12252, and could potentially influence the severity of COVID-19.
As a result of the small participant count and the limited study design (observational study), the association between the severity of COVID-19 and existence of IFITM3 rs12252 phenotype cannot be demonstrated only on this data, future studies with large sample sizes and experimental design being necessary to prove this observed hypothesis.
Conclusion
COVID-19 is a highly contagious disease displaying symptoms that vary in intensity, covering a spectrum from asymptomatic cases to severe forms of the disease and death. Therefore, it is crucial to elucidate the mechanisms of action and the factors that determine the harshness of the disease in order to ensure prompt and appropriate therapy, develop effective vaccines to prevent intense forms of the condition, and reduce the number of deaths and severe cases among patients.
We found a possible correlation within the severity of COVID-19 infection, AG genotypes of IFITM3 rs12252 and clinical parameters. Large-scale investigations remain necessary to validate our conclusions. The implementation of a Firth’s Bias-Reduced Logistic Regression model provided valuable insights into the association between genotype and the severity of COVID-19 symptoms. Our findings suggest that patients with the AG genotype are more likely to experience severe COVID-19 symptoms, with an odds ratio of 2.141 (95% C.I.: −0.126–7.039, p=0.067). While the results indicate a trend toward statistical significance, further studies with larger sample sizes are needed to confirm these findings and better understand the underlying mechanisms. Additionally, future research could explore the role of other genetic and environmental factors in determining COVID-19 severity.
Genetic variations in the immune system are thought to profoundly impact the response to therapy and prognosis for individuals with SARS-CoV-2 virus infection, and they are increasingly recognized as poor prognostic factors. This requires the early identification of patients predisposed to severe manifestations and the search for appropriate therapeutic elements. Further research is needed to replicate these findings in more extensive, diverse populations and to investigate the underlying biological mechanisms.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of Universitatea Ovidius Constanța, Romania, no. DCI CEDMOG 02/12.01.2022.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patient(s) to publish this paper.
Acknowledgments
We thank the Doctoral School of Medicine for the funding and Research and Development Center for Morphological and Genetic Study in Malignant Pathology- CEDMOG Constanta for their collaboration and the conduct of the study. We are grateful to Dr. Andrei Condurache for his skilled advice on biostatistical analysis.
Funding
This research was funded by “Doctoral School of Ovidius University of Constanta Research”.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zhu N, Zhang D, Wang W. et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. New Engl J Med. 2020;382(8):727–733. doi:10.1056/NEJMoa2001017
2. Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China. JAMA. 2020;323(13):1239–1242. doi:10.1001/jama.2020.2648
3. Guan WJ, Ni ZS, Hu Y, et al. Clinical Characteristics of Coronavirus Disease 2019 in China. New Engl J Med. 2020;382(18):1708–1720. doi:10.1056/NEJMoa2002032
4. Liao Y, Goraya MU, Yuan X, Zhang B, Chiu SH, Chen JL. Functional Involvement of Interferon-Inducible Transmembrane Proteins in Antiviral Immunity. Front Microbiol. 2019;10:1097. doi:10.3389/fmicb.2019.01097
5. Siegrist F, Ebeling M, Ulrich C. The small interferon-induced transmembrane Genes and proteins. J Interferon Cytokine Res. 2011;31(1):1.
6. Meischel T, Fritzlar S, Villalon-Letelier F, et al. IFITM Proteins That Restrict the Early Stages of Respiratory Virus Infection Do Not Influence Late-Stage Replication. J Virol. 2021;95(20):e0083721. doi:10.1128/JVI.00837-21
7. Bailey CC, Zhong G, Huang IC, Farzan M. IFITM-Family Proteins: the Cell’s First Line of Antiviral Defense. Annu Rev Virol. 2014;1:261–283. doi:10.1146/annurev-virology-031413-085537
8. Shi G, Schwartz O, Compton AA. More than meets the I: the diverse antiviral and cellular functions of interferon-induced transmembrane proteins. Retrovirology. 2017;14(1):53. doi:10.1186/s12977-017-0377-y
9. Diamond MS, Farzan M. The broad-spectrum antiviral functions of IFIT and IFITM proteins. Nat Rev Immunol. 2013;13(1):46–57. doi:10.1038/nri3344
10. Friedlová N, Zavadil Kokáš F, Hupp TR, Vojtěšek B, Nekulová M. IFITM protein regulation and functions: far beyond the fight against viruses. Front Immunol. 2022;13:1042368. doi:10.3389/fimmu.2022.1042368
11. Schönfelder K, Breuckmann K, Elsner C, et al. The influence of IFITM3 polymorphisms on susceptibility to SARS-CoV-2 infection and severity of COVID-19. Cytokine. 2021;142:155492. doi:10.1016/j.cyto.2021.155492
12. Wang J, Luo Y, Katiyar H, Liang C, Liu Q. The Antiviral Activity of Interferon-Induced Transmembrane Proteins and Virus Evasion Strategies. Viruses. 2024;16(734):734. doi:10.3390/v16050734
13. Lee LJ, Robinson ME, Ma N, et al. IFITM3 functions as a PIP3 scaffold to amplify PI3K signaling in B cells. Nature. 2020;588(7838):491–497. doi:10.1038/s41586-020-2884-6
14. Spence JS, He R, Hoffmann HH, et al. IFITM3 directly engages and shuttles incoming virus particles to lysosomes. Nat Chem Biol. 2019;15(3):259–268. doi:10.1038/s41589-018-0213-2
15. Shi G, Kenney AD, Kudryashova E, et al. Opposing activities of IFITM proteins in SARS-CoV-2 infection. EMBO J. 2021;40(3):e106501.
16. Brass AL, Huang IC, Benita Y, et al. The IFITM proteins mediate cellular resistance to influenza A H1N1 virus, West Nile virus, and dengue virus. Cell. 2009;139(7):1243–1254. doi:10.1016/j.cell.2009.12.017
17. Everitt AR, Clare S, Pertel T, et al. IFITM3 restricts the morbidity and mortality associated with influenza. Nature. 2012;484(7395):519–523. doi:10.1038/nature10921
18. Huang IC, Bailey CC, Weyer JL, et al. Distinct patterns of IFITM-mediated restriction of filoviruses, SARS coronavirus, and influenza A virus. PLoS Pathog. 2011;7:1.
19. National Library Medicine. Reference SNP (rs) Report. Available from: https://www.ncbi.nlm.nih.gov/snp/rs12252.
20. Eisfeld AJ, Kawaoka Y. Calculated risk: a new single-nucleotide polymorphism linked to severe influenza disease. Nat Med. 2017;23(8):911–912. doi:10.1038/nm.4383
21. Lee N, Cao B, Ke C, et al. IFITM3, TLR3, and CD55 Gene SNPs and Cumulative Genetic Risks for Severe Outcomes in Chinese Patients with H7N9/H1N1pdm09 Influenza. J Infect Dis. 2017;216(1):97–104. doi:10.1093/infdis/jix235
22. Kim YC, Jeong BH. Ethnic variation in risk genotypes based on single nucleotide polymorphisms (SNPs) of the interferon-inducible transmembrane 3 (IFITM3) gene, a susceptibility factor for pandemic 2009 h1N1 influenza A virus. Immunogenetics. 2020;72(9–10):447–453. doi:10.1007/s00251-020-01188-0
23. Zhang Y, Qin L, Zhao Y, et al. Interferon-induced transmembrane protein 3 genetic variant rs12252-C associated with disease severity in coronavirus disease 2019. J Infect Dis. 2020;222(1):34–37. doi:10.1093/infdis/jiaa224
24. Gómez J, Albaiceta GM, Cuesta-Llavona E, et al. The interferon-induced transmembrane protein 3 gene (IFITM3) rs12252 C variant is associated with COVID-19. Cytokine. 2021;137:155354. doi:10.1016/j.cyto.2020.155354
25. Grujičić D, Mirkov L, Banković D, et al. Homozygous-Recessive Characteristics as a Biomarker of Predisposition for COVID-19. Clin Nurs Res. 2023;32(3):589–600. doi:10.1177/10547738221147754
26. Mohammed FS, Farooqi YN, Mohammed S. The Interferon-Induced Transmembrane Protein 3-rs12252 Allele May Predict COVID-19 Severity Among Ethnic Minorities. Frontiers in Genetics. 2021;12:692254. doi:10.3389/fgene.2021.692254
27. Li K, Fang Y, Li W, et al. CT image visual quantitative evaluation and clinical classification of coronavirus disease (COVID-19). Eur Radiol. 2020;8(8):4407–4416. doi:10.1007/s00330-020-06817-6
28. Romero SK, Reissig D, Petereit-Haack G, Schmauder S, Nienhaus A, Seidler A. The isolated effect of age on the risk of COVID-19 severe outcomes: a systematic review with meta-analysis. BMJ Glob Health. 2021;6(12):1.
29. Heid CA, Stevens J, Livak KJ, Williams PM. Real time quantitative PCR. Genome Res. 1996;6(10):986–994. doi:10.1101/gr.6.10.986
30. Chatterjee S, L.v N, Sharma M, et al. Association of COVID-19 with Comorbidities: an Update. ACS Pharmacol Transl Sci. 2023;6(3):334–354. doi:10.1021/acsptsci.2c00181
31. Mitroi AF, Leopa N, Dumitru E, et al. Association of TCF7L2, CASC8 and GREM1 polymorphism in Patients with Colorectal Cancer and Type II Diabetes Mellitus. Genes. 2022;13(8):1297. doi:10.3390/genes13081297
32. Mitroi AF, Leopa N, Dumitru E, et al. TCF7L2, CASC8 and GREM1 Polymorphism and Colorectal Cancer in South-Eastern Romanian Population. Medicine. 2023;102(7):e33056. doi:10.1097/MD.0000000000033056
33. Coperchini F, Chiovato L, Ricci G, Croce L, Magri F, Rotondi M. The cytokine storm in COVID-19: further advances in our understanding the role of specific chemokines involved. Cytokine Growth Factor Rev. 2021;58:82–91. doi:10.1016/j.cytogfr.2020.12.005
34. Alghamdi J, Alaamery M, Barhoumi T, et al. Interferon-induced transmembrane protein-3 genetic variant rs12252 is associated with COVID-19 mortality. Genomics. 2021;113(4):1733–1741. doi:10.1016/j.ygeno.2021.04.002
35. Čiučiulkaitė I, Siffert W, Elsner C, et al. Influence of the Single Nucleotide Polymorphisms rs12252 and rs34481144 in IFITM3 on the Antibody Response after Vaccination against COVID-19. Vaccines. 2023;11(7):1257. doi:10.3390/vaccines11071257
36. Hashemi SMA, Thijssen M, Hosseini SY, Tabarraei A, Pourkarim MR, Sarvari J. Human gene polymorphisms and their possible impact on the clinical outcome of SARS-CoV-2 infection. Arch Virol. 2021;166(8):2089–2108. doi:10.1007/s00705-021-05070-6
37. Pecoraro V, Cuccorese M, Trenti T. Genetic polymorphisms of ACE1, ACE2, IFTM3, TMPRSS2 and TNFα genes associated with susceptibility and severity of SARS-CoV-2 infection: a systematic review and meta-analysis. Clin Exp Med. 2023;23(7):3251–3264. doi:10.1007/s10238-023-01038-9
38. Kajal G, Gaganpreet Kaur Tejal P, Indranil B, Banerjee I. Systematic review and meta-analysis of human genetic variants contributing to COVID-19 susceptibility and severity. Gene. 2022;844:146790. doi:10.1016/j.gene.2022.146790
39. Chu H, J.f.w C, Yuen TTT, et al. SARS-CoV-2 infects human monocytic cells through ACE2 and TMPRSS2, and is inhibited by a clinically proven protease inhibitor. Nature Microbiology. 2020;5:1413–1422.
40. Zhang Y, Chen M, Guo L, et al. The association between IFITM3 gene polymorphisms and severity of COVID-19 infection. Front Immunol. 2021;12:691731.
41. Yapeng L, Lanlan W, Lanye H, Jiahui S, Nanyang L. Interferon-induced transmembrane protein 3 gene polymorphisms are associated with COVID-19 susceptibility and severity: a meta-analysis. J Infect. 2022;84(6):825–833. doi:10.1016/j.jinf.2022.04.029
42. Elessawy SM, Shehab A, Dina A, Soliman A, Eldeeb MA, SaraI IT. Interferon-Induced Transmembrane Protein-3 Rs12252-G Variant Increases COVID-19 Mortality Potential in Egyptian Population. Viral Immunology. 2024;37(4):186–193. doi:10.1089/vim.2024.0015
43. Cuesta-Llavona E, Albaiceta GM, Garcia-Clemente M, et al. Association between the interferon-induced transmembrane protein 3 gene (IFITM3) rs34481144 / rs12252 haplotypes and COVID-19. Virological Science. 2021;2:100016. doi:10.1016/j.crviro.2021.100016
44. Das KM, Singh R, Subramanya S, et al. Serum biochemical parameters as a surrogate marker for chest computed tomography in children with COVID-19. Future Virol. 2021;16(9):601–609. doi:10.2217/fvl-2021-0118
45. CDC UC for DC and P. Older adults and COVID-19. Available from: https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/older-adults.html.
46. Liu K, Chen Y, Lin R, Han K. Clinical features of COVID-19 in elderly patients: a comparison with young and middle-aged patients. J Infect. 2020;80:3–7.
47. CDC UC for DC and P. Symptoms of Coronavirus. Available form: https://www.cdc.gov/coronavirus/2019-ncov/symptoms-testing/symptoms.html.
48. CNN. Seniors with Covid-19 show unusual symptoms, doctors say. Available from: https://edition.cnn.com/2020/04/23/health/seniors-elderly-coronavirus-symptoms-wellness-partner/index.html.
49. WHO. Coronavirus Disease (COVID-19) Outbreak - Statement - Older People are at Highest Risk From COVID-19, but All Must Act to Prevent Community Spread; 2020.
50. Twitchell D, Christensen M, Hackett G, Morgentaler A, Saad F, Pastuszack WA. Examining Male Predominance of Severe COVID-19 Outcomes: a Systematic Review. Androgens: Clinical Research and Therapeutics. 2022;3(1):41–53. doi:10.1089/andro.2022.0006
51. Gholami M, Sakhaee F, Sotoodehnejadnematalahi F, et al. Increased risk of COVID-19 mortality rate in IFITM3 rs6598045 G allele carriers infected by SARS-CoV-2 delta variant. Hum Genomics. 2022;16(1):60. doi:10.1186/s40246-022-00434-8
52. Financial Express. Coronavirus pandemic: elderly more vulnerable to the disease; here’s what doctors have to say. Available from: https://www.financialexpress.com/lifestyle/health/coronavirus-pandemic-elderly-more-vulnerable-to-the-disease-heres-what-doctors-have-to-say/1938699.
53. Costea DO, Serbanescu L, Badiu D, et al. Pain Management in the Right Iliac Fossa During the COVID-19 Pandemic. J Mind Med Sci. 2022;9(1):162–167. doi:10.22543/7674.91.P162167
54. Lassi ZS, Ana A, Das JK, et al. A systematic review and meta-analysis of data on pregnant women with confirmed COVID-19: clinical presentation, and pregnancy and perinatal outcomes based on COVID-19 severity. J Glob Health. 2021;11:05018. doi:10.7189/jogh.11.05018
55. Goren A, Vaño-Galván S, Wambier CG, et al. A preliminary observation: male pattern hair loss among hospitalized COVID-19 patients in Spain - A potential clue to the role of androgens in COVID-19 severity. J Cosmet Dermatol. 2020;19(7):1545–1547. doi:10.1111/jocd.13443
56. Wambier CG, Goren A. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection is likely to be androgen mediated. J Am Acad Dermatol. 2020;83(1):308–309. doi:10.1016/j.jaad.2020.04.032
57. Rowland SP, O’Brien B. Screening for low testosterone is needed for early identification and treatment of men at high risk of mortality from Covid-19. Crit Care. 2020;24(1):367. doi:10.1186/s13054-020-03086-z
58. Feng Z, Liao M, Zhang L. Sex differences in disease: sex chromosome and immunity. J Transl Med. 2024;22(1):1150. doi:10.1186/s12967-024-05990-2
59. Del Valle DM, Kim-Schulze S, Huang HH, et al. An inflammatory cytokine signature predicts COVID-19 severity and survival. Nat Med. 2020;26(10):1636–1643. doi:10.1038/s41591-020-1051-9
60. Zamfir V, Stanci IV, Mitrea A, et al. Is the Severity of SARS CoV2 Infection Dependent on the Patient’s Gender? ARS Medica Tomitana. 2021;27(2):78–82.
61. Yang Y, Wang L, Liu J, Fu S, Zhou L, Wang Y. Obesity or increased body mass index and the risk of severe outcomes in patients with COVID-19: a protocol for systematic review and meta-analysis. Medicine. 2022;101(1):e28499. doi:10.1097/MD.0000000000028499
62. Yang J, Hu J, Zhu C. Obesity aggravates COVID‐19: a systematic review and meta‐analysis. J Med Virol. 2021;93(1):257–261. doi:10.1002/jmv.26237
63. Cai Q, Chen F, Wang T, et al. Obesity and COVID-19 severity in a designated hospital in Shenzhen, China. Diabetes Care. 2020;43(7):1392–1398. doi:10.2337/dc20-0576
64. Du YB, Lv Y, Zha WT, Zhou N, Hong XO. Association of Body mass index (BMI) with Critical COVID-19 and in-hospital mortality: a dose-response meta-analysis. Metabolism-Clinical and Experimental. 2021;117:e154373. doi:10.1016/j.metabol.2020.154373
65. Kalligeros M, Shehadeh F, Mylona EK, et al. Association of obesity with disease severity among patients with coronavirus disease 2019. Obesity. 2020;28(7):1200–1204. doi:10.1002/oby.22859
66. Földi M, Farkas N, Kiss S, et al. Obesity is a risk factor for developing critical condition in COVID‐19 patients: a systematic review and meta‐analysis. Obes Rev. 2020;21(10):e13095. doi:10.1111/obr.13095
67. Rashid PMA, Salih GF. The significance of IFITM3 polymorphism in COVID-19 asymptomatic and ICU admission Kurdish patients. Cytokine. 2023;171:e156349.
68. Mitrea A, Postolache P, Man MA, et al. The profile of serum inflammatory biomarkers in patients with SARS-CoV-2 infection: how well do they reflect the presence of pulmonary involvement? Orvosi Hetilap. 2023;164(41):1607–1615. doi:10.1556/650.2023.32880
69. Zhu Y, Cao X, Tao G, et al. The lymph index: a potential hematological parameter for viral infection. Int J Infect Dis. 2013;17(7):e490–e493. doi:10.1016/j.ijid.2012.12.002
70. Wu MY, Yao L, Wang Y, et al. Clinical evaluation of potential usefulness of serum lactate dehydrogenase (LDH) in 2019 novel coronavirus (COVID-19) pneumonia. Respir Res. 2020;21(1):e171. doi:10.1186/s12931-020-01427-8
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Diagnostic Value of Inflammatory Markers (CRP, IL6, CRP/IL6, CRP/L, LCR) for Assessing the Severity of COVID-19 Symptoms Based on the MEWS and Predicting the Risk of Mortality

Wolszczak-Biedrzycka B, Dorf J, Milewska A, Łukaszyk M, Naumnik W, Kosidło JW, Dymicka-Piekarska V
Journal of Inflammation Research 2023, 16:2173-2188
Published Date: 22 May 2023
Altered Liver Enzyme Markers in Patients with Asymptomatic, and Mild Omicron Infection: A Retrospective Study
Cao X, Xie YL, Yi JY, Liu ZL, Han M, Duan JH, Gao Q, Mu H, Zhou CL
Journal of Inflammation Research 2024, 17:6875-6885
Published Date: 30 September 2024