Back to Journals » Nursing: Research and Reviews » Volume 12
Exploring Challenges Faced by Nurses on Provision of Hormonal Contraceptives to Women on Antiretroviral Therapy in Selected Healthcare Facilities in Lilongwe District, Malawi
Authors Mkwinda E, Thombozi E, Botha J, Chilinda I, Mandala E, Chipeta M ![]()
Received 24 February 2022
Accepted for publication 8 August 2022
Published 16 August 2022 Volume 2022:12 Pages 147—157
DOI https://doi.org/10.2147/NRR.S363871
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Natasha Hodgkinson
Esmie Mkwinda,1 Enalla Thombozi,2 Janet Botha,2 Idesi Chilinda,2 Edna Mandala,2 Mep Chipeta3
1Nursing Department, Saint John of God College of Health Sciences, Mzuzu, Malawi; 2Community and Mental Health Department, Kamuzu University of Health Sciences, Lilongwe, Malawi; 3Department of Nursing and Midwifery, Mzuzu University, Mzuzu, Malawi
Correspondence: Esmie Mkwinda, Saint John of God College of Health Sciences, P. O. Box 744, Mzuzu, Malawi, Tel +265999672324, Email [email protected]
Background: Malawi is a low-income country with a high maternal mortality rate, unmet need for family planning and high reports (41%) of unintended pregnancies. Women on Antiretroviral Therapy (ART) continued to experience unintended pregnancies after using hormonal contraceptives provided by nurses in the family planning clinics. However, the unintended pregnancies could affect the sexual and reproductive health of women and decisions of nurses on contraceptive provision to women on ART.
Objective: The purpose of the study was to explore challenges faced by nurses in the provision of hormonal contraceptives to women on ART in selected clinics in Lilongwe, Malawi.
Methods: A qualitative approach using an explorative design was used in this study. Eight (8) participants were selected purposefully from five public family planning clinics in Lilongwe. They were interviewed individually using a semi-structured interview guide. Data were analyzed using a content analysis guide.
Results: Three themes emerged from the data and these were as follows: limited knowledge of nurses; inadequate resources and inadequate support. Results revealed that nurses had limited knowledge of contraceptives to provide to women on ART due to lack of ART content in the contraceptive training which they had. They also lacked clinical and human resources and adequate time to teach clients which affected provision of the right hormonal contraceptives to women on ART. Furthermore, they needed support in the form of supervision, reference materials and integration of ART and contraceptive provision services.
Conclusion: The challenges that nurses faced had an influence on the provision of contraceptives to women on ART. The study recommends that nurses should be trained on the provision of contraceptives to women on ART and be provided with the required resources and support for proper care to be achieved. Furthermore, there is a need for clear guidelines on hormonal contraceptives that women on ART could get and the integration of ART and family planning services.
Keywords: antiretroviral therapy, hormonal contraceptives, unintended pregnancies, nurses, challenges
Introduction
Unintended pregnancies for women living with HIV, especially in developing countries, remain a major global health concern since this could affect their sexual and reproductive health and concomitant risk of mother-to-child transmission of HIV infection.1,2 Contraceptive use has been noted as a cost-effective intervention for preventing both maternal to child transmission of HIV and maternal morbidity and mortality from unintended pregnancies.2 Despite the benefit, a Malawian study reported that contraceptive use was poor among HIV-infected men and women with an unmet need of 27%.3,4 Another Malawian study noted that the total fertility rate is 4.4 births per woman and 41% of pregnancies are unintended, increasing the risk of vertical transmission of HIV, HIV-related maternal morbidity and mental health problems.5 Furthermore, it is argued that hormonal contraceptives (HC) are one of the most commonly used methods of family planning world-wide even among women on ART.6 However, the provision of HCs to women on ART requires the knowledge of providers in both ART and contraceptives to avoid drug interactions that would render contraceptives ineffective and, subsequently, lead to unintended pregnancies.7,8
Malawi, one of the countries in sub-Saharan Africa where the study took place is among the top 16 countries with a high maternal mortality rate of 439 per 100,000 live births which could have been averted if family planning needs were met.1,9 In addition, women living with HIV and AIDS are often of reproductive age, who desire effective contraceptive options to prevent unwanted pregnancies.10 However, it is noted that the efficacy of some contraceptives is reduced if women are on certain ART regimes, thus predisposing these women to unintended pregnancies.11,12 Furthermore, it is noted that nevirapine-based ART and efavirenz reduce the efficacy of oral contraceptives and depot medroxyprogesterone acetate, thereby increasing the risk of unintended pregnancies in women.13,14 Several studies conducted in Malawi found that most HIV-positive women on ART did not desire future fertility although there was inadequate contraceptive use with high rates of unintended and mistimed pregnancies.2,15 This is a clear indication of missed opportunities for the prevention of unintended pregnancies and maternal mortality in Malawi, and the need for knowledgeable providers.
Furthermore, another study found that ART regimens containing protease inhibitors and non-nucleoside reverse transcriptase inhibitors may decrease the area under the curve levels of steroids released by HCs, while others do not, which leads to unintended pregnancies in some women.16 In Malawi, HCs are provided to both HIV infected and uninfected women, mostly by nurses and other health care workers using family planning guidelines which indicate that HIV-infected women could use any hormonal contraceptives without restriction.17,18 In addition, the World Health Organization (WHO) reviewed guidelines, indicating that women taking nucleoside reverse transcriptase inhibitor ART can use all hormonal contraceptive methods without restriction, and women using protease inhibitors like ritonavir can generally use hormonal contraceptives.19 Furthermore, the WHO Consolidated Guidelines on Sexual and Reproductive Health and Rights of Women Living with HIV recommend specific contraceptive methods for women on several ARTs in consideration to HIV stage and encourage that women be counselled on reproductive health and their rights.20
However, the Malawi ART guidelines indicate that some hormonal methods such as the pill and implants may be less effective with ARTs and encourage the use of depo provera contraceptive which is slightly less effective in preventing pregnancy and the use of dual protection to prevent HIV transmission.21 Although anecdotal clinic records at Bwaila, Area 18, Kawale, Mitundu and Area 25 family planning clinics, show that most women on ART are given depo provera as a contraceptive method, some clients continue to get other methods like implants since ART and family planning guidelines and services are not yet integrated. This could be one of the challenges for the nurses providing the services. Thus, there is an urgency of knowing and addressing the challenges of nurses providing the services in Malawi to reduce unintended pregnancies and maternal death.
The main interest in the current provision of hormonal contraceptives to women on ART is to prevent unintended pregnancies. However, women on ART in Malawi continue to experience unintended pregnancies despite consistent use of hormonal contraceptives.2 A study conducted in Malawi, South Africa and Uganda indicated that high rates of unmet contraceptive need and unplanned pregnancies have been reported among HIV-positive women even with the integration of HIV and contraceptive services.22 The Malawi government’s effort and policies are geared towards providing hormonal contraceptives to all women regardless of their HIV status. HCs are mostly provided by nurses at the family planning clinics and by the Health Surveillance Assistants in the communities using family planning guidelines. Unintended pregnancies have affected the government’s efforts and quality of lives for women on ART. Contraceptive access tailored to the needs of HIV-positive women and their ART regime is possible if guidelines and services could be integrated.17,19
Assurance is needed for HIV-positive women who want child spacing or to prevent pregnancy so that the efficacy of their HC will not be altered by concomitant use of ARVs.6 It is vital to know the challenges that nurses face in family planning clinics for proper contraceptive provision to women on ART. This paper reports the challenges faced by nurses on the provision of HCs to women on ART in selected healthcare facilities in Lilongwe, Malawi.
Materials and Methods
Study Design
The study used a qualitative approach employing explorative design to collect information on the challenges faced by nurses in the provision of HCs to women on ART in selected health facilities in Lilongwe. Qualitative research is dynamic and attempts to capture experiences in the context of those experiencing them.23 As such, a qualitative approach was the most suitable research method to carry out this study and gain an in-depth understanding of the phenomenon.
Study Setting and Sample
The study was conducted at five public health family planning clinics in Lilongwe district in the central part of Malawi in July 2018. These clinics were Bwaila District hospital family planning clinic, Kawale Health centre family planning clinic, Area 18 Health Centre family planning clinic, Area 25 Health Centre family planning clinic and Mitundu Rural Hospital family planning clinic. The study sites were selected for the following reasons: all of them were within Lilongwe and were the major health centres where family planning services were provided during the time of study. The sites were also utilized for teaching of nursing students in family planning and represented government care delivery in Malawi. Furthermore, the sites have an increased influx of clients from both urban and rural Lilongwe.
A purposive sampling technique was used to identify the sites and recruit participants who consented to take part in the study, subject to data saturation. In addition, snowball sampling was also used to recruit some participants who met the inclusion criteria. Participants met the following inclusion criteria: age 18 years or above, all nurses at the five family planning clinics, a minimum of three months of providing the services and had been trained in the provision of HCs. The sample size was determined by data saturation, meaning that the data of some interviewees reappeared and no new themes appeared while analyzing the data. The final sample size was eight (8) participants who met the inclusion criteria from a total population of 24 nurses. The target population for the study from the five sites was as follows: Bwaila N = 5, Kawale N = 5, Area 18 N = 5, Area 25 N = 5 and Mitundu N = 4.
Ethical Considerations
The study was approved by the College of Medicine Research and Ethics Committee (COMREC) (now known as Kamuzu University Research and Ethics Committee) (Approval number: P.03/16/1912) and permission was sought from Lilongwe District Health Office and management of the five sites. The study was conducted in accordance with the Declaration of Helsinki. Before the interviews, the interviewees were informed in detail regarding the purpose, methods, content and confidentiality of the study. The analysis of the results and the writing of the paper were coded and carried out anonymously. Written informed consent forms were signed by all interviewees after agreeing to participate in the study voluntarily and that responses would be published anonymously in a scientific journal.
Preparation of Interview Questions
The interview guide was prepared in English using the objectives of the study. One central question was “Explain the challenges that you face when providing hormonal contraceptives to women on ART?” Probing and follow-up questions were used to enhance the responses, and reflection was used to improve clarity (see Appendix 1). Field notes were used to verify issues that arose during data collection. The data collection tool also comprised demographic profile of participants.
Pre-Test of Data Collection Tool
The semi-structured interview guide was pre-tested at Lumbadzi Health Centre family planning clinic in Dowa District in the Central Region. Four individual participants were used to adapt the tool accordingly and increase its credibility. The results from the pilot study were not included in the main study.
Data Collection
Data were collected through dialogue using in-depth, individual face-to-face, semi-structured open-ended questions with all nurses. This allowed participants to express themselves fully regarding their experiences on the phenomenon. The information given by the participants was audio-taped, observations on non-verbal cues were made and field notes were used to verify issues during data collection. Data collection took place from 16th July to 25th July 2018 and interviews lasted 45–60 minutes each. Independent data collectors facilitated the dialogue sessions in a quiet room within the facility premises to avoid bias. A non-threatening environment allowed participants to open up and give rich information.
Methodological Rigor
For the study to be more credible and dependable, the researchers applied trustworthiness principles.23 Credibility was achieved by pilot testing of data collection tools and prolonged engagement with data during collection of 45–60 minutes and during analysis to have an in-depth understanding. Audio recorded data and member checking also ensured credibility and confirmability where researchers returned to participants to validate the findings. Transferability was achieved by triangulation of the study sites to obtain multiple views of participants. Dependability was achieved by using the same main question in all the individual interviews to maintain consistency of data findings. Furthermore, authenticity and confirmability were achieved by using participant’s quotes when presenting the study findings and provide a dense description of research methodology.
Data Analysis
The principles of thematic analysis using content method were applied to analyze data. This approach systematically sorted and compared items in order to summarize information.24 The interviewers and another researcher analyzed data within 24 hours of the interview concurrently with data collection. Data saturation was reached after interviewing eight participants and no new information emerged. The first step was to transcribe verbatim the interviews after listening to the voice recordings. The next step was to verify the transcriptions by re-reading the transcribed data to obtain a general sense of the content. This step was followed by identifying content that pertained to the phenomena under study to formulate meanings from significant statements. The significant contents were then sorted into themes and sub-themes that reflected challenges of nurses. Thereafter, careful reading through the entire field notes and observations were made, clustering together similar information and identifying themes based on the content list. Finally, themes and subthemes were grouped according to their content, and validation of findings was done by returning to participants to compare the results.
Results
Demographic Characteristics of Participants
A total of eight (8) participants were selected from a population of 24 nurses from the five clinics that were purposefully selected. One (1) participant was from Kawale health centre, two (2) were from Area 25 health centre and another two (2) from Mitundu Rural hospital, one (1) was from area 18 health centre and two (2) were from Bwaila district hospital, respectively. Of these, six (6) were females and two (2) were males. Baseline characteristics consisted of the following areas: age, sex, nursing cadre, period spent as a provider and type of family planning training attended.
The results indicated that four (4) participants’ ages ranged from 41 to 50, three (3) of them ranged from 31 to 40 years and one (1) participant had the age range between 26 and 30 years, respectively. This showed that most nurses working in family planning care have age ranges between 31 and 50 years.
Participants also stated their cadre which showed their level of nursing training. Six (6) participants were enrolled nurses showing that they have a certificate in nursing and two (2) participants were registered nursed showing that they either had a diploma or degree in nursing. Participants were asked on the type of family planning training that they had. Five (5) participants indicated that they attended an in-service training for five days, while three (3) got trained as they worked in the clinic. In addition, two (2) participants had ART included in their training, while six (6) did not have that component.
Themes That Emerged
The study findings depict nurses’ challenges in the provision of hormonal contraceptives to women on ART in Lilongwe district in Malawi which was the main theme of the study. The following three sub-themes emerged from the study: limited knowledge of nurses, need for resources and inadequate support. Details of the main theme, subthemes and categories that emerged from the study are shown in Table 1.
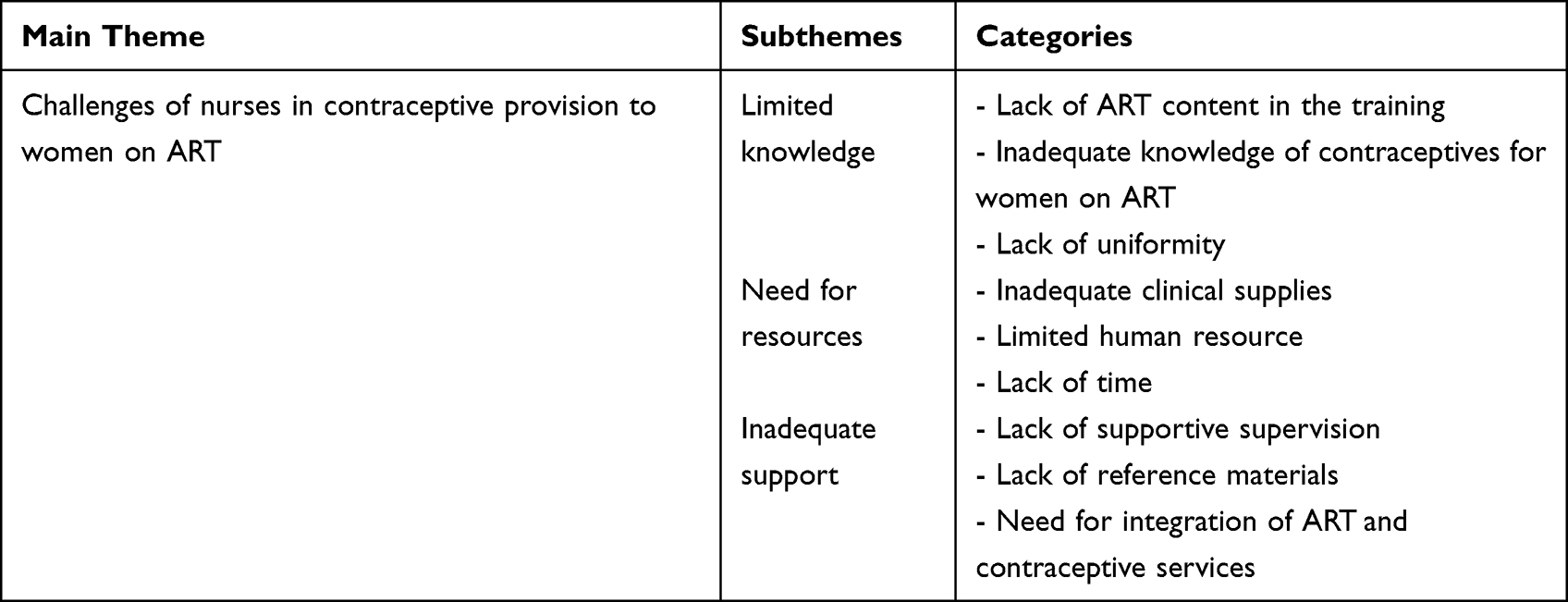 |
Table 1 Themes and Subthemes and Categories That Emerged |
Sub-Theme 1: Limited Knowledge
The findings highlighted that the majority of participants had inadequate knowledge on the HC methods for women on ART. The following three (3) categories emerged under this theme, and these were as follows: Lack of ART content in the contraceptive training, inadequate knowledge of contraceptive methods for women on ART and lack of uniformity in contraceptive and care provision to women on ART.
Lack of ART Content in the Contraceptive Training
Participants indicated that they were trained on provision of contraceptives to all women in general and not to women on ART which created a knowledge gap that affected their role and the outcome of clients who were on ART. The findings indicated that the training content lacked ART component which affected their knowledge. Participants also stated that they could benefit from being trained in both ART and contraceptives and the following excerpt attests to the above statements:
I was trained in family planning and all contraceptives … but not ART so there is a gap in knowledge since we also get clients that are on ART and want contraceptives, we treat them the same way. (Participant 003)
Another participant had this to say:
We need both trainings to function properly and have adequate knowledge. (Participant 006)
Another participant expressed the need for training in this manner:
I heard that some contraceptives interact with ART and cause contraceptives to lose efficacy … but I don’t know which ones. We need to be trained. (Participant 001)
Inadequate Knowledge of Contraceptive Methods for Women on ART
Participants cited how their clients who were also on ART came back with unintended pregnancies after consistently using the hormonal methods which they gave. This made them realize that efficacy of some contraceptives is reduced by ART, and they lacked knowledge on this. One participant stated as follows:
We were surprised that women were coming back with unintended pregnancies after using the methods we gave them consistently … especially implants. (Participant 004)
Another participant said:
we realized that ART reduces efficacy of some methods. (Participant 007)
Another participant felt sad that the methods given to the clients did not assist the women in this narrative:
It was very sad for women to have unintended pregnancies while using our methods … we realized that the methods given are not effective anymore for women on ART. (Participant 002)
In addition, participants expressed their realization of reduced efficacy of some contraceptives and need for training to improve their knowledge. Another participant narrated as follows:
I realized that we need knowledge on contraceptives that efficacy is not reduced by ART … when unintended pregnancies continued.. (Participant 004)
Another participant explained the need for training as follows:
I heard that nurses working in ART clinics and others get trained on specific contraceptives to give these women such as depo provera … my client got pregnant while using depo provera method consistently … we really need knowledge. (Participant 008)
Lack of Uniformity
Participants noted that they lacked uniformity in the methods that they provided and wished for consistency in the methods that they provide. The following excerpt illustrates this:
We need to be consistent in our practice … especially for women on ART …. (Participant 002)
some give all hormonal methods, some only depo provera while some give implants or pills … we lack uniformity I would say. (Participant 005)
Besides the need for uniformity in the methods provided to women on ART, participants indicated that the essential assessment of the women on ART is not uniform. One participant had this to say:
At this clinic no one collects subjective data and physical examinations are not done … I feel that it is not necessary … our records do not require that …. (Participant 003)
Another participant said the following:
… but for women on ART, I don’t know what we are supposed to be doing. (Participant 007)
Another participant explained the reasons for not assessing the clients on ART as follows:
May be ART assessments are being done … but I doubt … most of us do not do that … this could be looked at as discrimination. (Participant 001)
Another participant also explained the following:
We were told that HIV testing is not mandatory … I have to respect women’s rights … I do not consider HIV or ART when providing contraceptive methods …. (Participant 007)
One participant narrated as follows:
I take it that HIV care is provided in the ART clinic … I treat them as normal clients. (P 005)
Sub-Theme 2: Need for Resources
Under this sub-theme, three (3) categories emerged and these were inadequate clinical resources, limited human resources and lack of time.
Inadequate Clinical Supplies
Participants indicated that they had inadequate clinical supplies in their clinics to assist the women which negatively impacted the quality of care provided. The specific items mentioned by participants included availability of all contraceptive methods and space for client assessments. One participant gave the following narrative:
There is need for the availability of all contraceptives at all times … women on ART might require specific contraceptives which need to be available ….I give what is available since some methods are not available at times. (Participant 002)
Another participant expressed the need in this excerpt:
I cannot return the women because of ART methods that they are on, I give what I have at the time. (Participant 007)
Another participant expressed that their clinic relies on donated items for some methods and the need was expressed as follows:
Some contraceptives are only available when donated … I cannot rely on them especially for women on ART … I give what is available at the time … We need all the methods at all times to carter for women on ART …. (Participant 004)
In addition to clinical resources, participants observed the need for adequate space to perform client assessment. This was expressed by one participant as follows:
Space is not adequate for our practice … its hard to even provide privacy … there’s no space to examine clients ….it would be hard to care for those on ART. (Participant 006)
Limited Human Resource
Besides the challenge of clinical resources, participants shared that their clinics had limited human resources such that most clinics were being manned by one or two nurses most of the times which affected the quality of care delivered. One participant had this to say:
I work alone in the clinic most of the times … I need to finish the queue in good time …. (Participant 004)
In addition, another participant narrated:
You are alone for all these women … sometimes it’s just the two of you at the clinic against a lot of clients … and you do not waste time asking many questions. (Participant 008)
Lack of Time
The participants also highlighted the challenge of inadequate time for providing proper services due to long queues. This is what one participant stated:
There’s no time to practice what I know … I work to manage the queue and asking about HIV and ART would delay us more …. (Participant 003)
Another participant expressed the need for time as follows:
It is hard to ask each client about ART and HIV, it would need more time and you will need follow-up questions … you want to see other clients and finish the queue. Women on ART need more time and care (Participant 002)
Furthermore, another participant stated the following:
It would take time to assess clients on ART, you have to advice them each time … the queues are long and you would be wasting time, nurses at ART clinic can continue looking after these clients there (Participant 003)
Sub-Theme 3: Inadequate Support
Even though participants provided the services to clients in the clinics, inadequate support had a negative influence on the care that was provided. The following three (3) categories emerged under this sub-theme: lack of supportive supervision, lack of reference materials with ART component and the need for integration of ART and family planning services.
Lack of Supportive Supervision
Participants indicated that they lacked supportive supervision which affected care provision to all women and especially those on ART. This was expressed by one participant in the following excerpt:
No one monitors what we do in these clinics and no one cares … we need supportive supervision to help us provide proper care and be mentored. (Participant 006)
Another participant expressed this challenge in the following statement:
I need supervision by those that have more knowledge at least in both ART and contraceptives … our current supervisors just check if we are on duty … I fail to ask because they also lack knowledge …. (Participant 003)
Lack of Reference Materials
Lack of reference materials was mentioned as something which negatively affected their care provisions. This was illustrated in the following excerpt:
I cannot remember everything that I was taught at the workshop, I wish that our clinic should have books to refer to. (Participant 002)
Another participant mentioned the lack of reference materials such as guidelines and books to refer to and this was expressed as follows:
There are no guidelines, we need reference materials, … job aids or even small booklets to refer to. (P007)
Another participant added the following:
Most books at this clinic lack the ART content … we need such reference materials with ART content. (P 005)
Another participant mentioned the need for reference materials with recommended methods. This was narrated as follows:
We need books and reference materials with recommendations for methods that we should give to women on ART. (P004)
Need of Integration of ART and Family Planning Services
Participants also expressed the need of integrating ART and family planning services that would improve services provided to women on ART. One participant said the following:
There is also need to integrate family planning and ART services for the benefit of women on ART, they spend more time visiting the clinics than to get all services at one clinic by the same providers. (Participant 008)
Another participant felt that integration of ART and family planning services would improve ART knowledge of nurses. This was explained as follows:
The solution is to integrate family planning and ART services to improve the knowledge of nurses … they will be forced to train us in both … this will benefit clients on ART as well. (Participant 007)
Another participant felt that integration of ART and family planning services would force the Ministry to develop guidelines. This was expressed as follows:
Integration will force the ministry of health to develop integrated guidelines for ART provision and contraceptives and that will help us in provision of these services. (Participant 002)
Discussion
The study findings revealed that the participants lacked knowledge in both ART and hormonal contraceptives since they were not trained which affected the provision of the right contraceptives and the prevention of unwanted pregnancies in women on ART. The findings support existing literature of a study conducted in South Africa which found that lack of training, affected providers’ knowledge which influenced the counseling and methods provided to clients.25 The need of nurses to be trained in both ART and hormonal contraceptives is consistent with other published studies,26 who also state that knowledge in both areas would be important in the provision of proper contraceptives that would prevent unintended pregnancies. In addition, a study conducted in Malawi found that the shortage of trained providers was one of the barriers to the provision of family planning in ART clinics.15
Our study also revealed a lack of clinical, limited time and human resources which affected the way care was provided to family planning clients. Lack of clinical resources, such as contraceptives, affected the continuity of contraceptive provision, especially for women on ART who are at risk of unintended pregnancies. Consistent with the current study, limited human resources, limited time to counsel clients and lack of private space were some of the challenges affecting contraceptive provision in HIV care in Malawi.15 The findings illustrate the importance of the availability of contraceptive methods to all women at all times, including those on ART. Women should be provided with appropriate information and counseling so that they make informed choices.26
Nurses perceived that lack of supportive supervision negatively affected their role although it was viewed as an important strategy in mentoring and improving their knowledge. It could therefore be argued that there is a need for supportive supervision so that nurses perceive their role as one that makes an important contribution. This also reflects a lack of supportive professional relationship between the supervisors and nurses. It is noted that lack of supportive supervision affects the performance of health workers since it has been said to be a key determinant of service quality that strengthens the health system in low-income countries.27,28 In addition, supportive supervision strategy helps to reduce programme barriers and achieve the desired objectives.29
Unique to our study, nurses perceived that integration of family planning into ART care would support them in improving their knowledge and outcome of women on ART. In addition, other studies found that integration of family planning into HIV care reduced unintended pregnancies and the unmet need for contraception.30 A study conducted in Uganda showed that the integration of HIV care and family planning is critical in preventing contraceptive failure and vertical transmission of HIV.31 Integration of contraceptive and ART services has been noted as a beneficial intervention that provides women with knowledgeable providers that provide contraceptives that do not interact with ART.32 In addition, integration of services is a successful strategy to ensure the best outcomes for women on ART.33 Furthermore, several studies conducted in Malawi agree that integration of services improves both coverage, access to other services and improves knowledge of staff members.15,34
Limitations of the Study
The results of this study should be interpreted with caution since only five family planning care facilities were sampled in one district in Malawi; as such, the results should be transferred with caution.
Conclusions and Recommendations
The findings of the study highlight the challenges faced by nurses on the provision of hormonal contraceptives to women on ART in selected clinics in Lilongwe, Malawi. The study showed that, although nurses provided contraceptives to women on ART, they were not trained and lacked knowledge. They felt that supportive supervision, guidelines and integration of family planning and ART services would benefit them to provide proper services and prevent unintended pregnancies.
The researchers added that training institutions should take an active role in supporting nurses through provision of reference materials and knowledge sharing sessions so that up-to-date information is shared in the clinical area for the benefit of clients and their students. They also recommended integration of contraceptive services into HIV care which would support nurses to improve knowledge and ensure that better services are provided to women on ART which they also recommended.
The challenge of inadequate clinical and human resource was mentioned by participants as vital for proper service delivery to clients in the prevention of unintended pregnancies. Although the participants were from different settings, common challenges emerged, highlighting the consistency of experiences of family planning nurses. The study noted that it was crucial to deal with the challenges faced by participants in order to prevent unintended pregnancies in women on ART and prevent concomitant risk of mother-to-child transmission of HIV infection.
To this end, management of the facilities and departments should work with nurses on the staffing needs and address them. Furthermore, management and nurses need to ensure that clinical resources such as contraceptives of all types are available at all times for women to have their choice according to their needs. Nurses should be encouraged to conduct counseling on contraceptive methods and other sexual and reproductive health measures to clients in order to prevent concomitant transmission of HIV and promote their health. Other studies have indicated that strengthening competencies and skills of health managers of health systems is important in filling the gap in managerial, knowledge and capacity building of the whole organization.35
The study was conducted in selected clinics in Lilongwe, Malawi, and the findings presented here are only for nurses from these settings. Therefore, there is a need for larger-scale studies to explore the challenges faced by family planning clients on ART in Malawi and include more health facilities.
Acknowledgments
The authors acknowledge with gratitude the Norwegian government for financial support through Kamuzu College of Nursing (now known as Kamuzu University of Health Sciences), the management and staff of the five research sites and also the study participants.
Author Contributions
All authors contributed towards the following: conception and design of the study, data collection, analysis and interpretation, identification of the journal and revising the paper and agree to be accountable for all aspects of the work. At the time of the study, Kamuzu College of Nursing was a constituent college of University of Malawi and College of Medicine was also a constituent college of University of Malawi which have now merged and are called Kamuzu University of Health Sciences. College of Medicine Research and Ethics Committee was the approval body that was used for all health-related research under the University of Malawi which approved this study.
Disclosure
Mrs Enalla Thombozi reports grants from NORHED, during the conduct of the study. The authors declare that they have no other conflicts of interest in this work.
References
1. Habte D, Namasasu J. Family planning use among women living with HIV: knowing HIV positive status helps – results from a national survey. Reprod Health. 2015;12(1):1. doi:10.1186/s12978-015-0035-6
2. Haddad LB, Feldacker C, Jamieson DJ, et al. Pregnancy prevention and condom use practices among HIV-infected women on antiretroviral therapy seeking family planning in Lilongwe, Malawi. PLoS One. 2015;10(3):e0121039. doi:10.1371/journal.pone.0121039
3. Haddad LB, Tang JH, Krashin J, et al. Factors associated with condom use among men and women living with HIV in Lilongwe, Malawi: a cross-sectional study. BMJ Sex Reprod Health. 2018;44(1):1–2. doi:10.1136/bmjsrh-2017-101825
4. Odland ML, Vallner O, Toch-Marquardt M, Darj E. Women do not utilise family planning according to their needs in Southern Malawi: a cross-sectional survey. Int J Environ Res Public Health. 2021;18(8):4072. doi:10.3390/ijerph18084072
5. Tweya H, Feldacker C, Gugsa S, Phiri S. Contraceptive use and pregnancy rates among women receiving antiretroviral therapy in Malawi: a retrospective cohort study. Reprod Health. 2018;15(1):1–6. doi:10.1186/s12978-017-0440-0
6. Thurman AR, Anderson S, Doncel GF. Effects of hormonal contraception on antiretroviral drug metabolism, pharmacokinetics and pharmacodynamics. Am J Reprod Immunol. 2014;71(6):523–530. doi:10.1111/aji.12210
7. Ministry of Health, Malawi. Malawi health sector strategic plan 2011 – 2016: moving towards equity and quality. Lilongwe: government printers; 2011. Available from: http://www.healthdatacollaborative.org.
8. Mersha AG, Erku DA, Belachew SA, Ayele AA, Gebresillassie BM, Abegaz TM. Contraceptive use among HIV-positive and negative women: implication to end unintended pregnancy. Contracept Reproduct Med. 2019;4(1):1–8. doi:10.1186/s40834-019-0084-2
9. Trends in maternal mortality. US Agency for International development; 2021. Available from: https://www.usaid.gov.
10. Nance N, Ralph L, Padian N, et al. Unintended pregnancy and subsequent postpartum long-acting reversible contraceptive use in Zimbabwe. BMC Womens Health. 2018;18(1):1–8. doi:10.1186/s12905-018-0668-z
11. Robinson JA, Jamshidi R, Burke AE. Contraception for the HIV-positive woman: a review of interactions between hormonal contraception and antiretroviral therapy. Infect Dis Obstet Gynecol. 2012;2012:1–15. doi:10.1155/2012/890160
12. Gujo AB, Kare AP. Utilization of long-acting reversible contraceptives and associated factors among reproductive age women attending governmental health institutions for family planning services in Wondo Genet District, Sidama, National Regional State, Southern Ethiopia. Health Serv Res Manag Epidemiol. 2021;8:23333928211002401. doi:10.1177/23333928211002401
13. Sharma M, Walmsley SL. Contraceptive options for HIV‐positive women: making evidence‐based, patient‐centred decisions. HIV Med. 2015;16(6):329–336. doi:10.1111/hiv.12221
14. Nanda K, Stuart GS, Robinson J, Gray AL, Tepper NK, Gaffield ME. Drug interactions between hormonal contraceptives and antiretrovirals. AIDS. 2017;31(7):917. doi:10.1097/QAD.0000000000001392
15. Caplan MR, Phiri K, Parent J, Phoya A, Schooley A, Hoffman RM. Provider perspectives on barriers to reproductive health services for HIV-infected clients in Central Malawi. Clin Obstet Gynecol Reprod Med. 2018;4(1). doi:10.15761/COGRM.1000208
16. El-Ibiary SY, Cocohoba JM. Effects of HIV antiretrovirals on the pharmacokinetics of hormonal contraceptives. Eur J Contracept Reprod Health Care. 2008;13(2):123–132. doi:10.1080/13625180701829952
17. World Health Organization. Hormonal contraceptive methods for women at high risk of HIV and living with HIV. 2014 guidance statement. Available from: www.who.int/reproductivehealth/topics/family_planning.
18. United States Agency for International Development (USAID) Technical brief: Hormonal contraception and HIV. Advancing sexual and Reproductive health worldwide through research, policy analysis and public education; 2012. Available from: www.guttmacher.org.
19. World Health Organization. Family planning: a handbook for providers; 2018. Available from: www.fphandbook.org.
20. World Health Organization. Consolidated guideline on sexual and reproductive health and rights of women living with HIV. Available from: www.who.int/reproductivehealth.
21. Ministry of Health, Malawi. Clinical management of HIV in children and adults. 2019 Policy update: addendum to the 4th Edition of Malawi integrated guidelines and standard operation procedures for clinical HIV services. Lilongwe: Government Printers; 2018.
22. Imbuki K, Shaffer DN, Sinei SK, Todd CS, Stibich MA. Factors influencing contraceptive choice and discontinuation among HIV-positive women in Kericho, Kenya. Afr J Reprod Health. 2010;14(4):103–114.
23. Polit DF, Beck CT. Nursing Research: Generating and Assessing Evidence for Nursing Practice. Lippincott Williams & Wilkins; 2008.
24. Grove SK, Burns N, Gray J. The Practice of Nursing Research: Appraisal, Synthesis, and Generation of Evidence. Elsevier Health Sciences; 2012.
25. Lince-Deroche N, Hendrickson C, Moolla A, Kgowedi S, Mulongo M. Provider perspectives on contraceptive service delivery: findings from a qualitative study in Johannesburg, South Africa. BMC Health Serv Res. 2020;20(1):1. doi:10.1186/s12913-020-4900-9
26. Patel RC, Bukusi EA, Baeten JM. Current and future contraceptive options for women living with HIV. Expert Opin Pharmacother. 2018;19(1):1–2. doi:10.1080/14656566.2017.1378345
27. Purity M, Eilish M, Ogenna U, Honorati M, Henry M. The impact of supportive supervision on the implementation of HRM processes; a mixed-methods study in Tanzania. Health Syst Policy Res. 2017;4(1). doi:10.21767/2254-9137.100066
28. Avortri GS, Nabukalu JB, Nabyonga-Orem J. Supportive supervision to improve service delivery in low-income countries: is there a conceptual problem or a strategy problem? BMJ Glob Health. 2019;4(Suppl 9):e001151. doi:10.1136/bmjgh-2018-001151
29. Adetiloye O. The use of integrated supportive supervision (ISS) visits to strengthen family planning service delivery in two selected states of Nigeria. Texila Intl J Public Health. 2017;5(4). doi:10.21522/TIJPH.2013.05.04.Art052
30. Newmann SJ, Zakaras JM, Tao AR, et al. Integrating family planning into HIV care in western Kenya: HIV care providers’ perspectives and experiences one year following integration. AIDS Care. 2016;28(2):209–213. doi:10.1080/09540121.2015.1080791
31. Scarsi KK, Darin KM, Nakalema S, et al. Unintended pregnancies observed with combined use of the levonorgestrel contraceptive implant and efavirenz-based antiretroviral therapy: a three-arm pharmacokinetic evaluation over 48 weeks. Clin Infect Dis. 2016;62(6):675–682. doi:10.1093/cid/civ1001
32. Harrington EK, Newmann SJ, Onono M, et al. Fertility intentions and interest in integrated family planning services among women living with HIV in Nyanza Province, Kenya: a qualitative study. Infect Dis Obstet Gynecol. 2012;2012:1–8. doi:10.1155/2012/809682
33. Patel RC, Morroni C, Scarsi KK, Sripipatana T, Kiarie J, Cohen CR. Concomitant contraceptive implant and efavirenz use in women living with HIV: perspectives on current evidence and policy implications for family planning and HIV treatment guidelines. J Int AIDS Soc. 2017;20(1):21396. doi:10.7448/IAS.20.1.21396
34. Phiri S, Feldacker C, Chaweza T, et al. Integrating reproductive health services into HIV care: strategies for successful implementation in a low-resource HIV clinic in Lilongwe, Malawi. J Fam Plann Reprod Health Care. 2016;42(1):17–23. doi:10.1136/jfprhc-2013-100816
35. Ravaghi H, Beyranvand T, Mannion R, Alijanzadeh M, Aryankhesal A, Belorgeot VD. Effectiveness of training and educational programs for hospital managers: a systematic review. Health Serv Manag Res. 2021;34(2):113–126. doi:10.1177/0951484820971460
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.