Back to Journals » Nature and Science of Sleep » Volume 17

Exploring Causal Pathways to Sleep Quality in Young Adults Using a Multimodal Data-Driven Causal Discovery Analysis
Authors Xiao X ![]() , Wang Y, Dong D, Wang W, Li Z, Guo Y
, Wang Y, Dong D, Wang W, Li Z, Guo Y ![]()
Received 6 July 2025
Accepted for publication 20 September 2025
Published 14 October 2025 Volume 2025:17 Pages 2681—2698
DOI https://doi.org/10.2147/NSS.S550127
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Xiong Xiao,1,2,* Yulin Wang,3,* Debo Dong,3 Wei Wang,1,2 Zhangyong Li,2 Yiqun Guo1,2
1School of Life Health Information Science and Engineering, Chongqing University of Posts and Telecommunications, Chongqing, People’s Republic of China; 2Chongqing Engineering Research Center of Medical Electronics and Information Technology, Chongqing University of Posts and Telecommunications, Chongqing, People’s Republic of China; 3Faculty of Psychology, Southwest University, Chongqing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zhangyong Li, School of Life Health Information Science and Engineering, Chongqing University of Posts and Telecommunications, No. 2, Chongwen Road, Nanan District, Chongqing, People’s Republic of China, Email [email protected] Yiqun Guo, School of Life Health Information Science and Engineering, Chongqing University of Posts and Telecommunications, No. 2, Chongwen Road, Nanan District, Chongqing, People’s Republic of China, Email [email protected]
Purpose: Poor sleep quality is prevalent across the population and may significantly impact both physical and mental health. However, our understanding of the complex mechanisms underlying poor sleep quality is still incomplete, particularly regarding the various contributing factors. To address this, we utilized a data-driven causal discovery analysis (CDA) approach to explore causal pathways of sleep quality.
Patients and Methods: We relied on a large sample of healthy young adults from the Human Connectome Project (HCP; n = 1206 [54% female, 56% unmarried/non-cohabiting]) to explore causal pathways of sleep quality. We first used exploratory factor analysis to cluster 122 broad phenotypic variables into 21 factors and computed the functional connectivity of 13 resting-state brain networks. Then, using Greedy Fast Causal Inference (GFCI), we simultaneously integrated the obtained phenotypic factors, brain network connectivity, and sleep quality into the causal discovery analysis and ultimately constructed a causal model.
Results: The model proposes a hierarchical structure with causal effects propagating through complex interactions across multiple domains, ultimately linked to changes in sleep quality. Our causal model identified three phenotypic factors (negative affect, somaticism, and delay discounting) as directly linked to sleep quality. In addition, we examined causal models of sleep quality across gender (male and female) and relationship status (unmarried/non-cohabiting and married/cohabiting) and found some demographic-specific pathways.
Conclusion: Our data-driven model reveals complex mechanisms by which factors from different domains influence sleep quality and highlights several key factors that influence sleep quality, which may have important implications for the development of sleep theories and the improvement of sleep quality.
Keywords: sleep quality, causal discovery analysis, resting-state fMRI, negative affect, somaticism, delay discounting
Introduction
Sleep is a critical human function that profoundly correlates with physical health, mood, cognitive functions, social life, and quality of work.1–4 Adequate sleep enhances attention, memory, positive mood, and work performance, while also reducing disease risk.3,5 Conversely, poor sleep quality is associated with fatigue, daytime dysfunction, impaired immunity, and increased risks for cardiovascular, metabolic, and mental health disorders, such as anxiety and depression.2–4,6,7 Despite its importance, sleep problems are highly prevalent. For example, in the United States, one-third of adults experience sleep deprivation,8 and more than 60% of college students are considered poor sleepers.3 Therefore, identifying the factors that affect sleep quality and incorporating them into future interventions is crucial.
Sleep is a tightly regulated neurophysiological process involving the ascending reticular activating system, key brain regions such as the hypothalamus and brainstem, and multiple neurotransmitters, which together govern the cycling between non-rapid eye movement (NREM) and rapid eye movement (REM) sleep.9–12 Neuroimaging evidence further links sleep quality to neural activity in frontal, parietal, and temporal cortical regions.13 Nonetheless, it remains unclear whether poor sleep quality is a cause or a consequence of brain dysfunction.13,14 Beyond these neural mechanisms, sleep is regulated by interactions between biological, psychological, and other factors. Theoretical models, such as Blake et al’s multilevel framework, emphasize that these biopsychosocial factors do not operate in isolation but collectively shape sleep through their interactions.2 Given the complex, multi-systemic regulation of sleep, focusing solely on single factors (eg, stress, alcohol consumption)2,15 may overlook other critical elements and their interactions and synergies, thereby potentially limiting a comprehensive understanding of the mechanisms influencing sleep quality.
Currently, there is no consensus on how sleep problems develop and which factors play a decisive role in maintaining them. In recent years, research on the causal relationships of sleep has grown, particularly through Mendelian Randomization (MR) which uses genetic signals from genome-wide association studies to explore links between sleep traits and disease outcomes. However, MR has limitations, especially regarding pleiotropism, where a single gene may affect multiple traits, potentially skewing results. Additionally, MR often assumes a linear relationship between exposure and disease outcome, and ignoring nonlinearity may lead to false negatives. To date, only one MR study has considered both linear and non-linear associations when exploring the causal relationships between sleep phenotypes and disease outcomes.16 Moreover, much research on sleep has focused on its effects on mood and cognition.2,4 As a result, there remains a lack of in-depth exploration of the causal mechanisms behind sleep problems and the key factors that influence their development. Causal models typically represent causal relationships in the data graphically. As the number of variables increases, the space of potential causal models may also expand, making it difficult to determine which potential causal model best fits the observed data. As a machine learning technique for learning causal models from data, causal discovery analysis (CDA) can identify the causal structures that best fit the data.17 In order to understand this issue, we adopted a data-driven CDA to comprehensively analyze and explore the complex phenotypes related to sleep quality in order to construct comprehensive models containing clear causal pathways. This will help us elucidate how multiple domains and factors work together in leading to differences in sleep quality, and provide a scientific basis for developing more precise and effective interventions.
Although there are emerging studies that reveal unique sleep patterns in men and women, including sleep quality, duration, etc.,8,18 the reasons for gender differences in sleep behaviors are unclear and not well researched. At all stages of life, women typically have poorer sleep quality and are more susceptible to factors than men.8,19 Historically, biomedical research has underrepresented women’s sleep studies, mainly due to the assumption that findings from male subjects are universally applicable.8 In addition, most sleep research tends to view sleep as an individual behavior and ignores its social context. Ignoring the social aspects of sleep not only calls into question the ecological validity of these findings, but also has important consequences for sleep-focused interventions.20 Sleep can be conceptualized as a basic “attachment behavior” and the presence of secure attachment facilitates sleep health.21 Therefore, it is important to consider the causal variability that contributes to sleep problems across relationship status. Embracing technological advances and evidence-based practices makes it important to understand these differences in gender and relationship status as healthcare moves toward greater personalization.
To address these limitations, we draw on two relevant frameworks with overlapping insights and mutual reinforcement in key aspects. The Research Domain Criteria (RDoC) framework, developed by the US National Institute of Mental Health, moves beyond traditional diagnostic categories to focus on transdiagnostic functional domains (eg, Cognitive Systems, Negative Valence Systems) underlying psychopathology.22,23 It emphasizes multidimensional assessments of core biobehavioral mechanisms and advocates for multivariate models that integrate growing knowledge of how multiple functional domains interact to contribute to psychopathology. Meanwhile, Blake et al’s multilevel model elucidates how biological (eg, neurochemistry, brain circuits), psychological (eg, worry), and social (eg, social withdrawal) factors interact to shape insomnia,2 highlighting systemic cross-domain interplay. Integrating these frameworks allows for capturing both the biopsychosocial mechanisms and cross-diagnostic functional domains of sleep problems, providing a holistic theoretical foundation. Accordingly, we systematically incorporated a broad range of biopsychosocial phenotypes and large-scale brain network functional characteristics from HCP data to capture as many potential sleep-related domains as possible. Our objective is to identify core factors associated with sleep quality. Guided by this theoretical framework, we hypothesize that sleep quality is influenced by the interplay of multi-level factors (social, psychological, biological, and neurological) with complex associations across these domains.
In this study, we aimed to construct a causal model related to sleep quality. We initially downscaled the extensive phenotypic measures for a large community sample using exploratory factor analysis and computed the functional connectivity within the subjects’ resting-state brain networks. Subsequently, we applied CDA to the obtained phenotypic factors, brain network connectivity, and sleep quality. In this way, we successfully built an integrated multimodal causal model that reveals the causal pathways of brain connectivity and phenotypic factors on sleep quality. In addition, we examined and compared the causal models of sleep quality in groups of different gender (male and female) and different relationship status (unmarried/non-cohabiting and married/cohabiting). Our study may provide valuable insights into the specific mechanisms linking brain network connectivity and phenotypic factors to sleep quality in the general young population.
Materials and Methods
Subjects
We used the data from the Human Connectome Project WU-Minn1200 Subjects Data Release (n = 1206, age range: 22–37 years, 54% females, 44% married/cohabiting), comprising healthy young adults with no clinical diagnoses of psychiatric or neurological disorders.24 All subjects provided written informed consent and all procedures were approved by the University of Washington Institutional Review Board (IRB # 201204036). This secondary analysis of the Human Connectome Project (HCP) dataset was approved by the Ethics Committee of Chongqing University of Posts and Telecommunications (protocol code: No. 2024028). This study included subjects who completed least two runs of rfMRI data (phenotypic n = 1206, resting-state fMRI n = 1096, final n = 1090). The demographic characteristics of the subjects are presented in Table 1. We estimated missing values using multiple imputation method implemented with the “mice” package in R software,25 version 4.3.2. Specifically, binary variables were imputed using logistic regression, multinomial variables using polytomous regression, and continuous variables using random forests. Five independent imputed datasets were generated and subsequently analyzed, with final estimates pooled according to Rubin’s rules.
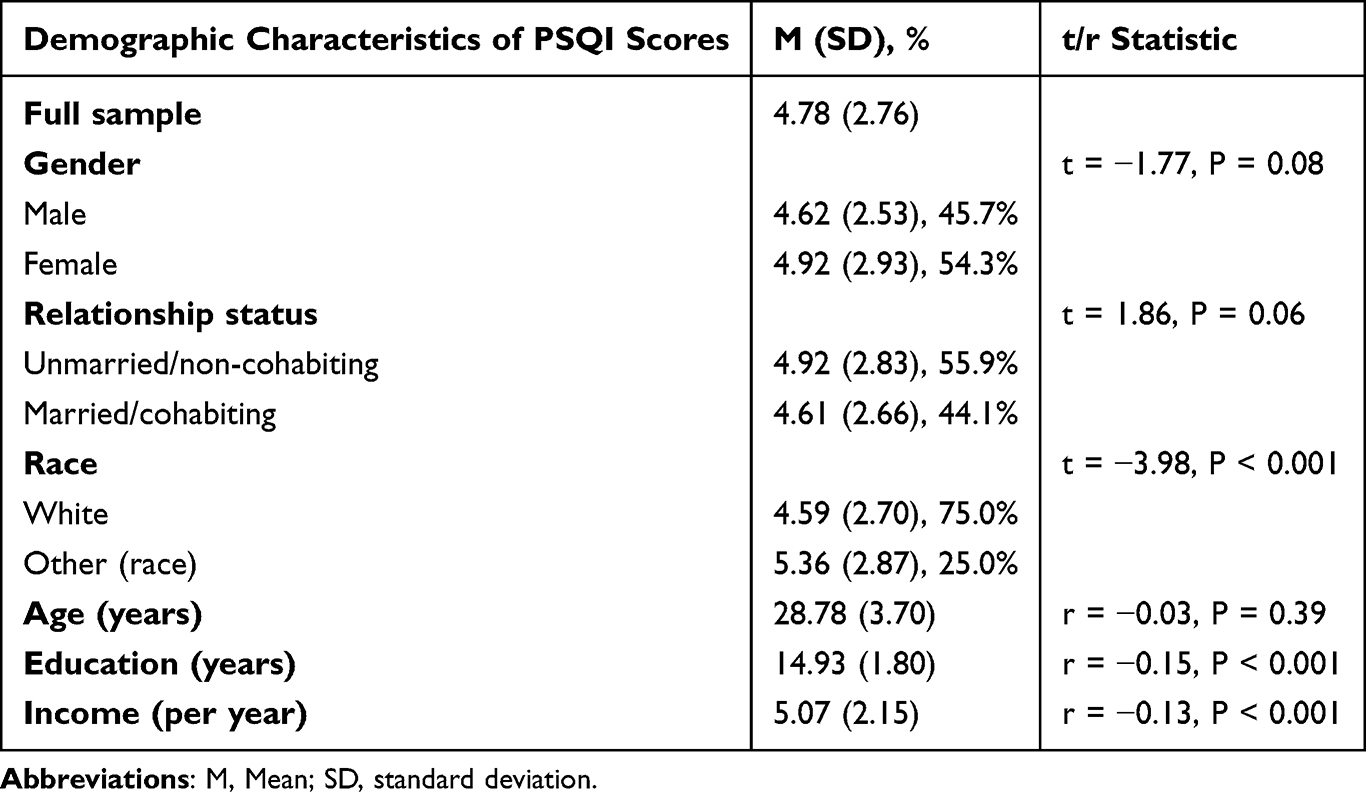 |
Table 1 Demographic Characteristics of Participants (N = 1090) |
Outcome Measure
Subjects’ sleep quality was assessed using the Pittsburgh Sleep Quality Index (PSQI).26 PSQI is a self-assessment questionnaire used to assess sleep quality and disturbance over a 1-month time interval. PSQI comprises nineteen individual items, which are aggregated into seven “component” scores: (1) subjective sleep quality; (2) sleep latency; (3) sleep efficiency; (4) sleep duration; (5) sleep disturbance; (6) use of sleep medications; and (7) daytime dysfunction. These items are rated on a four-point Likert scale according to the frequency or severity of the problem. Each item is rated on a scale of 0 to 3 (eg, 0 = Not during the past month, 1 = Less than once a week, 2 = Once or twice a week, 3 = 3 or more times a week). The sum of the component scores yields a total PSQI score ranging from 0 to 21, with higher scores indicating poorer sleep quality. The tool developers26 suggested a threshold of 5, meaning that an overall PSQI score greater than 5 indicates poor subjective sleep quality. Notably, 344 of the 1090 participants (31.6% of the current sample) had a total PSQI score higher than 5. See Table 1 for more specific information.
Behavioral and Self-Report Measures
The HCP dataset encompasses an extensive range of self-report, diagnostic, and behavioral measures evaluating various domains, including emotion, cognition, social functioning, psychiatric disorders, and personality traits. To ensure comprehensive coverage of phenotypic characteristics, we included as many available sleep-related metrics as possible from the HCP dataset as possible. Our inclusive approach encompasses behavioral task data collected within the scanner environment, but excludes fMRI measurements of brain activation related to the task. We utilize summary scores, rather than item-level or subordinate scores, encapsulating the task constructs of our interest.27 For example, for the N-Back task, which assesses working memory capacity, we included accuracy as well as average of median reaction time for the 2-back task and the 0-back task across all conditions. For domains that provide both age/gender-adjusted and unadjusted scores, we only include unadjusted scores. Ultimately, we included 122 measures (see Supplemental Materials for details and rationale for inclusion).
Exploratory Factor Analysis
We conducted exploratory factor analysis (EFA) to downscale the screened HCP phenotype data (122 measures in total). EFA was performed using the “Psych” package and “GPArotation” package for R (version 4.3.2),28,29 where factors were extracted using the maximum likelihood method and subsequently rotated using the “direct Oblimin” method. The maximum likelihood method estimates model parameters by maximizing the likelihood function of observed data, demonstrating good reliability and robustness, even in cases where distributional assumptions are violated.30,31 Oblimin rotation is a diagonal rotation method that accommodates correlated factors. We used Monte Carlo permutation analysis (parallel analysis)32 to determine the optimal number of factors to be extracted from the factor analysis. Only measures with loadings greater than or equal to 0.30 were considered to contribute to the factor, which is a commonly accepted threshold in factor analysis.33
MRI Scanning and Preprocessing
MRI scanning was performed using a customized 3T Siemens Connectome Skyra with a standard 32-channel Siemens receiver head coil and a body transmission coil. Structural images (T1-weighted and T2-weighted) were preprocessed to correct for gradient non-linearities, readout distortions, bias field distortions, and aligned to the MNI space template. For detailed preprocessing steps, see.34 During resting-state fMRI scanning, all subjects were instructed to relax, keep their eyes open, keep awake and not think of anything in particular. The resting-state fMRI data were preprocessed by correcting spatial distortions, realigning for motion, registering to the structural images, normalizing to MNI space. fMRI data were then high-pass filtered, denoised using ICA-FIX, and regressed out for the artifact components and 24 motion regressors. For detailed information on the preprocessing pipeline see.34 The final ICA-FIX denoised version of the fMRI data was downloaded and used for the next brain network analysis.
fMRI Network Connectivity
Eighty-four percent of subjects completed four rs-fMRI scans within two days, totaling 58 minutes and 12 seconds of rs-fMRI data. Our rfMRI network connectivity analysis only included subjects who completed at least two rfMRI acquisitions (90% of total subjects). We used the set of 300 regions of interest (ROIs) and associated network assignments described by Green’s team as nodes of the whole-brain functional network,35 which was further augmented with additional nodes for subcortical and cerebellar structures based on the Power 264 atlas.36 This parcellation used a set of functionally defined spherical ROIs in volumetric space, and employed the Infomap algorithm to compute network assignments for each ROI. Specifically, we partitioned the 300 ROIs into functional connections within 13 resting-state brain networks. For each network, we calculated pairwise Pearson correlations between every pair of parcels. Within each network, we then averaged these correlations to derive summary statistics of connectivity.37–40 The final 13 networks obtained include default mode network, cingulo-opercular network, dorsal attention network, frontoparietal network, ventral attention network, somatomotor lateral network, somatomotor dorsal network, salience network, auditory network, medial temporal lobe network, parieto-medial network, visual network, and reward network.
Greedy Fast Causal Inference
The Greedy Fast Causal Inference (GFCI) algorithm41 is a graph search methodology for inferring causal structures. It adeptly integrates greedy strategies with constraint satisfaction techniques, enabling the algorithm to efficiently and relatively accurately identify causal relationships between variables, even in the presence of unmeasured confounding factors. This capability provides valuable insights into the underlying causal structure.17 The GFCI makes causal inferences in two steps. In its initial phase, the GFCI employs the Fast Greedy Equivalence Search (FGES) algorithm42 to explore potential causal models, minimizing a penalized likelihood score like the Bayesian Information Criterion (BIC).43 FGES iteratively adjusts edges, maximizing model fit. Initially, it assumes that there are no unmeasured common causes, which allows for a preliminary assessment of causal relationships among the measured variables. In the second phase, GFCI drops this assumption and conducts a series of conditional independence tests. These tests iteratively excluded causal relationships for which conditional independence was implied and remained unconfirmed by the data. We provide an additional example of how constraint-based causal inference works in Figure 1. The output of the GFCI algorithm results in a partial ancestral graph (PAG), which is able to encode the presence of causal relationships, uncertain relationships, and unmeasured confounding variables. For the generated PAG, the variables are represented as nodes in the graph. The type and direction of the edge connecting two nodes specify the nature of the modeled causal relationship.41,44,45 Figure 2 lists the possible edge types in the PAG and their corresponding meanings.
 |
Figure 1 Figure 1 illustrates a constraint-based causal discovery algorithm, showing four possible causal relationships among variables X, Y, and Z. From left to right, the figures are (a–d). (a) A collider graph is displayed where X causes Z, Z causes Y, and X and Y have a causal relationship. (b) The edges between X and Z and between Z and Y are reversed, so now Y causes X. (c) Shows a scenario where both X and Y cause Z, but X and Y are not related. In this structure, X and Z are dependent, Y and Z are dependent, but X and Y are independent. However, when conditioning on Z, it becomes a common cause for X and Y, making them dependent on each other. GFCI uses observations from conditional Independence tests to determine the direction of causal relationships. This allows for distinguishing whether the data is generated by (a) or one of the other three figures, as these four graphs exhibit different conditional dependencies. |
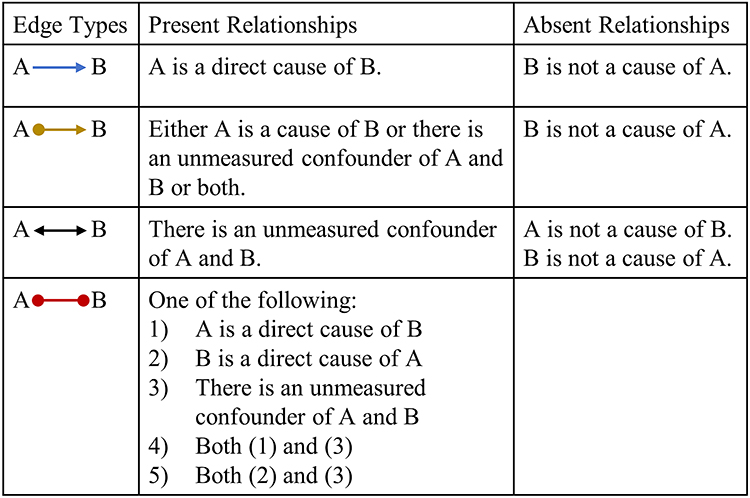 |
Figure 2 Types of edges. |
We implemented the GFCI algorithm using the Tetrad software version 7.6.6, with the following model parameters: a BIC score, which was set to a default penalty discount value of 2, was used to evaluate the penalized likelihood; a Fisher Z test value, with an alpha threshold set at the default of 0.01, served to perform the conditional independence tests; and a maximum graph degree limit of 100. To ensure the stability of causality, we performed 1000 bootstrap iterations on 90% of the samples to adequately estimate the distribution of the statistics. Within each iteration, we applied the same GFCI algorithm to analyze the data. Subsequently, we summarized the proportions of all potential relationships after aggregating the results of 1000 iterations, including the frequency of various edges and edge types.
SEM: Effect Size Estimation
To uncover the effect sizes of causal pathways in the model, we fitted standardized effect sizes by constructing a structural equation model (SEM) for the output of the GFCI using R’s “lavaan” software package.46 The statistical power of each model was also assessed (see Supplemental Materials).
Results
Exploratory Factor Analysis: Dimensionality Reduction Decomposition of the Phenotypic Measures
According to the Kaiser-Meyer-Olkin test (KMO) and Bartlett’s Test of Sphericity,47 our phenotypic data had a good fit (KMO = 0.87, P < 0.001), which was well suited for Exploratory factor analysis (EFA) that was used to downscale the screened complete HCP phenotype data. Based on the results of the Monte Carlo simulation, we categorized the 122 phenotypic variables into 21 factors that together accounted for 46% of the common variance (see Figure 3). The EFA model fit indices indicated good factor separation (RMSEA= 0.04, Tucker-Lewis Index = 0.85). These 21 factors cover five domains: (1) Cognitive domain includes Crystalized IQ, Delay Discounting, Fluid Cognition, Gambling Task Reaction Time, Language Task Performance, Memory Performance, Processing Speed and Visuospatial Processing; (2) Physiological domain includes Blood Pressure and Somaticism; (3) Negative valence domain include Externalizing, Internalizing and Negative Affect; (4) Behavioral domain includes Alcohol Use, Cigarette Use, Drug Use, Hyperactivity and Unconscientiousness/Inattention; (5) Social domain includes Openness, Social Support/ Positive Affect and Social Withdrawal. Factor correlations were presented in Supplemental Materials (Figure S1).
 |
Figure 3 Permutation-based test for eigenvalue significance (Monte Carlo permutation analysis). |
GFCI: Using Causal Discovery Analysis to Explore Causal Pathways of Sleep Quality
We constructed a causal model related to sleep quality using the Greedy Fast Causal Inference (GFCI) algorithm. The GFCI outputs are shown in Figure 4, depicting the causal relationships among 21 extracted factors, 13 predefined resting-state brain network connectivity, and sleep quality. Structural equation modeling (SEM) was then employed to assess model fit and effect sizes, and revealed that the model fit was good (RMSEA = 0.05; Comparative Fit Index (CFI) = 0.91) and all paths were significant (p < 0.05). The results of the stability analysis are presented in the Supplemental Materials (Figures S2–S6).
 |
Figure 4 Greedy Fast Causal Inference (GFCI) was applied to simultaneously integrate phenotypic factors, brain network connectivity, and sleep quality into a causal discovery model of sleep quality. The variables are represented in different colors to distinguish their types. The weights of the normalized edges are displayed next to each edge in text form, with only the explicitly pointed edges labeled. The structural equation model (SEM) demonstrated good fit (RMSEA = 0.05; CFI = 0.91), and all paths were significant (p < 0.05). See the Supplemental Materials for factor correlations and additional data. |
Our causal model reveals the complex interactions between brain network connectivity, behavioral phenotypes and sleep quality, and highlights some key causal pathways linked to sleep quality (see Figure 4). We identified three critical phenotypic factors that are directly related to sleep quality: somaticism (effect size (ES) = 0.31), delay discounting (ES = −0.17), and negative affect (ES = 0.18). Notably, elevated somaticism is associated with a decline in sleep quality, while factors such as high internalization problems and cigarette consumption may contribute to heightened somaticism. In our model, the delay discounting factor takes the area under the curve (AUC) as its indicator, with higher AUC values representing lower discount rates. Our findings reveal that high discount rates are directly linked to poor sleep quality, with low crystallized IQ and high cigarette use associated with increased delay discount rates. Furthermore, both high alcohol use and low language task performance are crucially indirectly related to elevating somaticism and increasing delay discount rates. High negative affect emerges as another pivotal factor that is directly related to poor sleep quality. We also identified a trigger for negative affect, namely high somaticism. In addition, reduced connectivity within the frontoparietal network is associated with decreased performance on language tasks, and decreased connectivity within the ventral attention network is linked to increased drinking, with both pathways ultimately and indirectly associated with impaired sleep quality. Overall, our causal analysis reveals complex pathways in which multi-domain and multi-modal factors are directly and indirectly linked to sleep quality, which contributes to the understanding of the mechanisms underlying the emergence of sleep problems.
Causal Models of Sleep Quality Across Gender and Relationship Status
Although the independent samples t-test did not reveal significant differences in PSQI total scores for gender (t = −1.77, P = 0.08) or relationship status (t = 1.86, P = 0.06), there are emerging studies that reveal their potentially unique effects on sleep.8,18,21 We further constructed causal models tailored to different gender and relationship status in order to explore the demographic characteristics and unique patterns of sleep. For the causal models of gender, we found that the models were well-fitted (Male model: RMSEA = 0.06, CFI = 0.88, with all paths significant at p < 0.001; Female model: RMSEA = 0.07, CFI = 0.84, with all paths significant at p < 0.001), and for explicitly pointing edges, 16 identical paths and 60 different paths were found in the male and female models (see Figure 5). In particular, somaticism and delay discounting emerge as common factors directly linked to sleep quality in both male and female models, whereas male sleep quality is also directly associated with negative affect. And Poor sleep quality in women is linked to externalizing problems. Furthermore, in females, social withdrawal is directly associated with somaticism, whereas in males, somaticism tends to be linked to social withdrawal. And for females, substance use (such as drug and cigarette consumption) has a direct association with delay discounting. In contrast, among males, the use of substances like alcohol affects social factors, such as social withdrawal and social support/positive affect, which subsequently associated with the emergence of negative affect.
 |
Figure 5 Causal models of sleep quality across gender are presented, with the left and right panels showing the models for males and females, respectively. Both models fit well. For the male model: RMSEA = 0.06, CFI = 0.88, with all paths significant (p < 0.001). For the female model: RMSEA = 0.07, CFI = 0.84, with all paths significant (p < 0.001). |
For the causal models of relationship status, we found goodness-of-fit indices for the both models (Unmarried/Non-cohabiting model: RMSEA = 0.06, CFI = 0.90, with all paths significant at p < 0.001; Married/Cohabiting model: RMSEA = 0.05, CFI = 0.90, with all paths significant at p < 0.01), and for explicitly directed edges, 13 identical paths and 75 different paths were found between unmarried/non-cohabiting and married/cohabiting populations (see Figure 6). In particular, somaticism and delay discounting emerged as common factors directly linked to sleep quality across both relationship status, whereas the sleep quality of married/cohabiting individuals is also directly associated with negative affect. Moreover, within the married/cohabiting group, hyperactivity problem is linked to somaticism, while in the unmarried/non-cohabiting group, somaticism tends to be associated with hyperactivity. Additionally, crystallized IQ is indirectly linked to delay discounting in married/cohabiting individuals, whereas for unmarried/non-cohabiting individuals, crystallized IQ has a direct association with delay discounting.
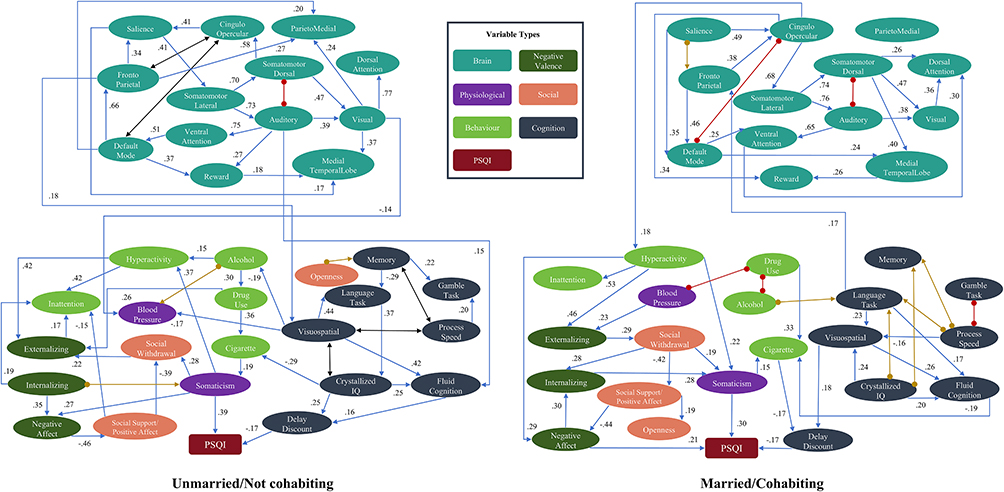 |
Figure 6 Causal models of sleep quality across relationship status are shown, with the left panel representing the unmarried/non-cohabiting group and the right panel the married/cohabiting group. Both models fit well. For the unmarried/non-cohabiting model: RMSEA = 0.06, CFI = 0.90, with all paths significant (p < 0.001). For the married/cohabiting model: RMSEA = 0.05, CLI = 0.900, with all paths significant (p < 0.01). |
Discussion
Previous studies on the causal mechanisms of sleep quality are limited, and the underlying pathways remain unclear. Here, we used a data-driven approach to construct a multi-modal, multilevel causal model integrating brain networks, phenotypic factors, and sleep quality. While our findings are exploratory and should be considered hypothesis-generating rather than confirmatory, they provide important insights into the causal architecture of sleep. The model elucidates specific pathways through which brain and behavioral factors influence sleep in young adults. Furthermore, stratified analyses by gender and relationship status revealed distinct causal pathways that may underlie demographic differences in sleep. These results advance understanding of the determinants of poor sleep and offer a theoretical foundation for targeted interventions.
Our analyses revealed three key factors directly linked to sleep quality: negative affect, somaticism, and delay discounting. Many studies have demonstrated the link between negative affect and sleep and have shown that all types of negative affect appear to be detrimental to sleep and considered to be major predictors of poor sleep quality.1,7 Our model clearly depicts a direct association between negative affect and poor sleep quality. According to previous studies, negative affect may be linked to sleep through multiple mechanisms. On the one hand, certain negative affect may activate the hypothalamic-pituitary-adrenal (HPA) axis, resulting in physiological responses such as increased cortisol secretion, heart rate, respiratory rate, and muscle tension,48 which disrupt normal sleep.49 On the other hand, persistent negative emotions may be associated with individuals experiencing cognitive activities such as rumination and worrying before bedtime, which may be linked to the perception of heightened psychological stress that can be associated with disruptions in sleep onset and sleep maintenance.50 Our model also suggests that negative affect is linked to problems within internalizing and social factors, which is consistent with existing research.51,52 It is noteworthy that negative emotions are directly associated low social support/positive affect, which in turn may spread and be linked to social withdrawal. These results suggest a potential mechanism of emotional contagion whereby emotional states between individuals can permeate and influence each other through social interactions.1,53
Our causal model indicated that somatization, which is the expression of psychological distress as physical symptoms (eg, persistent pain, fatigue, or other discomfort),54,55 is another factor directly linked to poor sleep quality. In individuals with generally good overall sleep quality, the moderate effect size (ES = 0.31) suggests that even mild somatic symptoms may disrupt sleep regulatory mechanisms, positioning somatization as a critical target for early intervention. Unlike in clinical samples, where comorbidities often obscure the specific impact of somatic symptoms,56,57 otherwise healthy individuals experiencing somatization may excessively focus on minor bodily discomforts or changes, especially during nighttime rest. This heightened interoceptive awareness can trigger or exacerbate difficulties falling asleep and increased arousal, thereby impairing both sleep initiation and maintenance and ultimately being linked to reduced sleep quality.58,59 Moreover, somatization is often accompanied by high levels of anxiety, depressed mood and rumination,58,60 and these mood states have been shown to be strongly associated with poor sleep quality.61 Our model also found another pathway by which somaticism is indirectly linked to sleep quality through negative affect. Furthermore, we identified several factors associated with somatization, including high cigarette use and high internalizing. Studies show a positive correlation between nicotine abuse and the somatization index.62 Additionally, individuals with internalizing issues are more likely to experience negative life events frequently, and these negative experiences may be linked to the development of functional somatic symptoms.63,64 And internalizing issues encompass psychological stress, depression and anxiety, with prolonged psychological stress and depression being recognized as significant triggers for somatization disorder.65
An interesting finding of our study is that steep delay discounting that refers to people’s preference for immediate small rewards over delayed but larger ones is associated with poor sleep quality. A previous study also used the HCP dataset reported an association between delayed discounting and sleep, but failed to clarify the direction of the relationship.66 Our results extend this work by demonstrating that delay discounting may precede and predict poorer sleep. This contrasts with many existing studies, which typically treat sleep deficiency as a contributor to impulsive decision-making, particularly in sleep-deprived populations.67 The discrepancy may stem from our focus on healthy adults. In this group, mild sleep disturbances are more likely to reflect voluntary behavioral choices influenced by delay discounting, rather than arising from impaired cognitive control. Importantly, this pattern may challenge the traditional theories, which typically positions cognitive function as a consequence of sleep disruption.68 Instead, our findings suggest that delay discounting, a key cognitive trait, functions as an antecedent. Resisting the temptation to obtain a reward immediately requires the activation of self-control processing, and individuals with high rates of delay discounting typically perform poorly in self-regulation and impulse control.69 Our results suggest that the possible roles of high discounting in contributing to poor sleep quality may be due to the formation and maintenance of unhealthy sleep habits (eg, delay bedtime, irregular sleep times, and excitatory activities prior to bedtime) resulting from poor self-control. Unhealthy behaviors such as irregular sleep schedules, nighttime cell phone use, and gaming before bedtime have been proved to be associated with excessive delayed discounting,70 and all contribute to poor sleep quality.71,72 With a modest effect size (ES = −0.17, comparable to that of negative affect), delay discounting may still be linked to influences on sleep regulation in otherwise healthy individuals. This finding points to a possible role for delay discounting in early intervention strategies and adds to the emerging evidence that cognitive traits may play a meaningful role in sleep regulation, complementing more established sleep models. Additionally, our findings underscore the association between delay discounting and both crystallized IQ and cigarette use. Lower crystallized IQ may impair the ability to forecast long-term consequences,73,74 while substance use disrupts dopamine-mediated reward processing and diminishes inhibitory control, thereby reinforcing preference for immediate rewards.75,76
Our causal model reveals pathways through which brain networks are related to behavioral phenotypes, whereby reduced connectivity of the frontoparietal network is linked to a decline in language task performance, while reduced connectivity in the ventral attention network (VAN) is associated with increased alcohol consumption, with both pathways ultimately linked to decreased sleep quality. Studies have identified a potential association between the frontoparietal network and language, with the left inferior frontal gyrus supporting syntactic processing (eg, grammar construction and complex sentence comprehension) and parietal regions aiding spatial attention and contextual language interpretation.77,78 Consequently, decreased connectivity within the frontoparietal network may be linked to difficulties and poorer performance on language tasks. Additionally, numerous studies have shown an association between VAN and excessive alcohol consumption.79 The VAN is one of the core neural systems in response inhibition, and deficits in response inhibition may be linked to difficulties in suppressing impulsive behaviors in individuals, thus being associated with difficulties in resisting or exacerbating substance use.79 Furthermore, the VAN plays a crucial role in regulating sudden emotional responses and maintaining goal-directed behaviors, and its dysfunction may lead to affective dysregulation and executive dysfunction,80 which may further elevate the risk of alcohol abuse.81
In addition, our causal models of sleep quality for males and females revealed both identical and gender-specific pathways. Somaticism and delay discounting were found to be directly linked to sleep quality in both genders, suggesting these factors may have a certain robustness. However, the sleep quality of women is not directly associated with the negative affect factor compared to men. In the HCP dataset, there was no significant difference in negative affect scores between the two genders (t = 0.47, P = 0.64). Although women of all age groups reported more subjective sleep problems,82–84 numerous studies consistently indicate that healthy women generally have better objective sleep quality than men.84–87 Existing research generally suggests that women experience more sleep problems than men,88,89 but this may be related to more severe insomnia problems in women,90 not just sleep quality itself. At the same time, due to physiological reasons such as pregnancy and menstrual cycles, women are more affected by hormones like ovarian steroids, which may make their sleep responses to negative emotions more complex and uncertain.84,91–94 Based on our causal model, women may alleviate the association between negative emotions and sleep quality through internalizing mechanisms. Furthermore, poor sleep quality in women can alsobe linked to externalizing problems. Sleep plays a crucial role in the neural mechanisms of emotion regulation and emotion expression.95 Women may be more susceptible to the negative effects of poor sleep and may be more emotionally affected,96–98 which may be linked to externalizing problems.99 Additionally, in women, social withdrawal is directly associated with somaticism, while somaticism is linked to social withdrawal in men. Women are generally more inclined to engage in social interactions and express their emotions.100 When women withdraw from social activities, the lack of emotional communication may be linked to emotional suppression and psychological stress, which may subsequently be associated with somatic symptoms.101,102 In contrast, men have traditionally been encouraged to repress their emotions and experiences of distress.103 As a result, when men experience somatization issues, they are often reluctant to show psychological and physical vulnerability.104,105 Various discomforting symptoms may be linked to their reducing or avoiding social activities, thus contributing to social withdrawal.106,107 Finally, substance use for females (eg, drugs, smoking) is associated with delay discounting. In males, substance use is linked to social factors like social withdrawal and social support/positive affect, which in turn are associated with negative affect. Research has shown that women often develop dependence more rapidly than men following the initiation of substance use and they find it harder to quit.108,109 Substances such as cocaine and nicotine can affect neurotransmitter systems, including dopamine, which are closely tied to the processing of immediate rewards and decision-making.110–113 Subsequent reductions in the use of these substances may also be linked to withdrawal symptoms,114–116 thereby further influencing women’s delay discounting rates. However, substance use is linked to social factors like social withdrawal and social support/positive affect in males, which in turn are associated with negative affect. Studies have indicated that alcohol consumption negatively impacts the anterior cingulate cortex, with particularly pronounced effects observed in men.117,118 Impairment of the anterior cingulate cortex can diminish inhibitory control, potentially associated with social withdrawal,102,119 which in turn may provoke issues such as negative emotions.102,120,121
We also analyzed causal models of sleep quality for relationship status (unmarried/non-cohabiting and married/cohabiting). Somaticism and delay discounting are robust factors directly linked to sleep quality in both relationship status. Compared to unmarried/non-cohabiting individuals, the sleep quality of married/cohabiting individuals is additionally directly associated with negative affect. In the HCP dataset, the unmarried/non-cohabiting group showed higher levels of negative affect (t = 2.19, P < 0.05) compared to the married/cohabiting group. Unmarried/non-cohabiting individuals may be more likely to experience isolation in times of difficulty,122 while also lacking the positive impact of a stable partner relationship,123 which could contribute to higher levels of negative emotions.124,125 However, they may have developed specific coping mechanisms (eg, reduced social interactions) that provide temporary relief from poor sleep quality. Future research could consider relationship status as a moderating variable to verify and discuss the impact of negative emotions on sleep quality. Additionally, within the married/cohabiting groups, hyperactivity is linked to somaticism, while somaticism tends to be associated with hyperactivity problems in the unmarried/non-cohabiting group. Studies have shown that individuals with anxiety symptoms and hyperactivity problems are at risk for functional somatic symptoms.126,127 Furthermore, in general, married/cohabiting groups show higher sensitivity and concern for physical changes and family dynamics,128,129 and hyperactivity symptoms may amplify their perception of changes in the external environment,130 which also triggers higher levels of anxiety, stress, and consequently somatic problems.103,131,132 In contrast, unmarried/non-cohabiting individuals tend to face challenges alone, lacking external emotional support and social resources.122,133 In the presence of somatic problems, they may alleviate or express psychological discomfort and physical uneasiness through hyperactive behaviors.134,135 Moreover, crystallized IQ is indirectly linked to delay discounting in married/cohabiting individuals, but has a direct association with delay discounting in the unmarried/non-cohabiting group. Delay discounting is typically associated with crystallized intelligence.136,137 Married/cohabiting individuals often navigate a shared decision-making environment, making it more likely that they will consult with their partners,138 which may result in the effects of crystallized intelligence on their decision-making being more indirect. Conversely, unmarried/non-cohabiting individuals may be more inclined to make independent decisions,139 meaning that existing knowledge and experience may be related to their delay discounting.
Our study integrated indicators traditionally scattered across emotional, cognitive, physiological, and other domains into a single causal model, identifying three factors directly associated with sleep quality. This provides empirical support for the theoretical framework of hierarchical biopsychosocial interactions emphasized by Blake et al.2 Notably, positioning delay discounting as a precursor of poor sleep rather than a result challenges the conventional view that sleep deficiency is the primary driver of impulsive decision-making,67,68 expanding understanding of sleep regulation in healthy populations. The study reveals that altered connectivity within brain networks indirectly influences sleep through behavioral phenotypes, adding neurobiological depth to these theories. It both validates the RDoC framework’s focus on cross-dimensional links between neural circuits and behavior and highlights the hierarchical system (from neural activity to behavioral expression) often overlooked by traditional sleep models.22,23 Furthermore, the moderating roles of gender and relationship status underscore the need to refine theories by incorporating demographic-specific pathways, aligning with RDoC’s advocacy for dimensional, context-sensitive mechanisms over universal models. Collectively, our study uncovers the intricate causal mechanisms influencing sleep quality and identifies key causal pathways. It deepens understanding of sleep disorder etiology, enriches theoretical frameworks, advances knowledge of sleep regulatory mechanisms, and provides a theoretical basis for targeted sleep interventions. For instance, targeting the regulation of negative emotions may be more effective in improving sleep quality than interventions that promote positive emotions. In the era of popularization of mobile electronics and online entertainment, it may be crucial to adopt effective guidance methods or techniques to change sleep-related decisions and reduce various undesirable temptations. Reducing or prohibiting substance use is important for alleviating a variety of problems as well as improving sleep.
However, this study has several limitations. First, the HCP dataset is cross-sectional and does not capture temporal dynamics, limiting our understanding of long-term changes. Although the GFCI algorithm is suitable for such data, it can only infer static associations. Future studies should employ longitudinal methods, such as Granger Causality Testing, to more accurately model the temporal evolution of sleep problems. Second, although GFCI accounts for unobserved confounders, key variables may still be missing. Factors such as genetic predispositions (eg, circadian rhythm genes), lifestyle behaviors (eg, physical activity), and environmental exposures (eg, light, noise) could simultaneously influence sleep and cognitive or emotional phenotypes, potentially biasing causal inferences. Third, sleep quality was assessed solely via the PSQI, a self-reported measure that may not fully align with objective sleep architecture. Future research should incorporate objective metrics, such as polysomnography, to validate and extend these findings. Finally, the sample consisted primarily of healthy young adults not suffering from sleep disorders, limiting the generalizability of our findings to clinical populations or older adults, who may exhibit distinct neurobiological, cognitive, or psychosocial profiles.140,141 Future work should systematically collect multimodal phenotypic and neuroimaging data from individuals with sleep disorders or older populations, applying causal discovery methods to build population-specific models and advance personalized sleep interventions.
Conclusion
In conclusion, we have for the first time applied a data-driven CDA approach to construct a causal model of sleep quality across resting-state brain function networks and multiple behavioral phenotypes related to sleep quality. We identified the following key findings: (a) high delay discount rates, somaticism, and negative affect are three key factors directly linked to reduced sleep quality; (b) the reduced connectivity within the frontoparietal and ventral attention networks indirectly reduces sleep quality by modulating behavioral phenotypes; (c) gender and relationship status moderate some of the causal pathways of sleep quality. This study visualizes the complexity of sleep models and reveals unique causal mechanisms across gender and relationship status, providing valuable insight into the mechanisms underlying poor sleep quality and helping to develop more effective interventions. In particular, our causally-driven model can be used as a base model to further integrate more domains and variables related to sleep quality, thus creating a more comprehensive and integrated multimodal sleep model.
Data Sharing Statement
The data utilized in this study are available for download from the Human Connectome Project (www.humanconnectome.org/). Users must agree to data use terms for the HCP before being allowed access to the data and ConnectomeDB, details are provided at https://www.humanconnectome.org/study/hcp-young-adult/data-use-terms. Factor loadings and factor nomenclature from the analysis of standardized variables are available upon request to the corresponding author. The Codes that support the findings of this study are available from the corresponding author upon reasonable request.
Ethical Approval Statement
This study was performed using publicly available datasets from Human Connectome Project (HCP) Young Adult. Human data acquisition for the HCP was approved by the Institutional Review Board (IRB) of the University of Washington in St. Louis (IRB # 201204036; Title: “Mapping the Human Connectome: Structure, Function, and Heritability”), and all open access data were deidentified. In addition, the present study received approval from the Human Ethics Committee of Chongqing University of Posts and Telecommunications (protocol code: No. 2024028) and adheres to the ethical guidelines outlined in the Declaration of Helsinki.
Acknowledgment
Data were provided by the Human Connectome Project, WU-Minn Consortium (Principal Investigators: David Van Essen and Kamil Ugurbil; 1U54MH091657) funded by the 16 NIH Institutes and Centers that support the NIH Blueprint for Neuroscience Research; and by the McDonnell Center for Systems Neuroscience at Washington University. We thank Eric Rawls from the University of Minnesota, USA, for his invaluable help with the methodology and for reviewing and editing the first draft of the paper.
Author Contributions
Xiong Xiao: Formal analysis, Methodology, Writing - original draft, Writing - review & editing; Yulin Wang: Methodology, Writing - original draft, Writing - review & editing; Debo Dong: Conceptualization, Writing - review & editing; Wei Wang: Conceptualization, Writing - review & editing; Zhangyong Li: Funding acquisition, Project administration, Conceptualization, Writing - review & editing; Yiqun Guo: Funding acquisition, Project administration, Conceptualization, Supervision, Methodology, Writing - original draft, Writing - review & editing. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation; all authors took part in drafting, revising or critically reviewing the article; all authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by the National Natural Science Foundation of China (32000777, 82202247, 32300861, 62171073, 62311530103), the Scientific research Funds of Chongqing University of Posts and Telecommunications (E010A2018130), and the National Natural Science Foundation of Chongqing (CSTB2022NSCQ-MSX0511).
Disclosure
The authors assert that they have no competing financial or personal interests.
References
1. Ben Simon E, Vallat R, Barnes CM, Walker MP. Sleep loss and the socio-emotional brain. Trends Cognit Sci. 2020;24(6):435–450. doi:10.1016/j.tics.2020.02.003
2. Blake MJ, Trinder JA, Allen NB. Mechanisms underlying the association between insomnia, anxiety, and depression in adolescence: implications for behavioral sleep interventions. Clin Psychol Rev. 2018;63:25–40. doi:10.1016/j.cpr.2018.05.006
3. Alamir YA, Zullig KJ, Kristjansson AL, Wen S, Misra R, Montgomery-Downs H. A theoretical model of college students’ sleep quality and health-related quality of life. J Behav Med. 2022;45(6):925–934. doi:10.1007/s10865-022-00348-9
4. Palmer CA, Bower JL, Cho KW, et al. Sleep loss and emotion: a systematic review and meta-analysis of over 50 years of experimental research. Psychol Bull. 2024;150(4):440–463. doi:10.1037/bul0000410
5. Forrester N. How better sleep can improve productivity. Nature. 2023;619(7970):659–661. doi:10.1038/d41586-023-02307-z
6. Young TB, Peppard PE, Gottlieb DJ. Epidemiology of obstructive sleep apnea: a population health perspective. Am J Respir Crit Care Med. 2002;165(9):1217–1239.
7. Pressman SD, Jenkins BN, Kraft-Feil TL, Rasmussen H, Scheier MF. The whole is not the sum of its parts: specific types of positive affect influence sleep differentially. Emotion. 2017;17(5):778–793. doi:10.1037/emo0000256
8. Lok R, Qian J, Chellappa SL. Sex differences in sleep, circadian rhythms, and metabolism: implications for precision medicine. Sleep Med Rev. 2024;75:101926. doi:10.1016/j.smrv.2024.101926
9. Liu D, Dan Y. A motor theory of sleep-wake control: arousal-action circuit. Annu Rev Neurosci. 2019;42:27–46. doi:10.1146/annurev-neuro-080317-061813
10. Yaffe K, Falvey CM, Hoang T. Connections between sleep and cognition in older adults. Lancet Neurol. 2014;13(10):1017–1028. doi:10.1016/s1474-4422(14)70172-3
11. Tamaki M, Wang Z, Barnes-Diana T, et al. Complementary contributions of non-REM and REM sleep to visual learning. Nat Neurosci. 2020;23(9):1150–1156. doi:10.1038/s41593-020-0666-y
12. Morris CJ, Aeschbach D, Scheer FA. Circadian system, sleep and endocrinology. Mol Cell Endocrinol. 2012;349(1):91–104. doi:10.1016/j.mce.2011.09.003
13. Sexton CE, Storsve AB, Walhovd KB, Johansen-Berg H, Fjell AM. Poor sleep quality is associated with increased cortical atrophy in community-dwelling adults. Neurology. 2014;83(11):967–973. doi:10.1212/WNL.0000000000000774
14. Smevik H, Habli S, Saksvik SB, et al. Poorer sleep health is associated with altered brain activation during cognitive control processing in healthy adults. Cereb Cortex. 2023;33(11):7100–7119. doi:10.1093/cercor/bhad024
15. Hasler BP, Schulz CT, Pedersen SL. Sleep-related predictors of risk for alcohol use and related problems in adolescents and young adults. Alcohol Res. 2024;44(1):02. doi:10.35946/arcr.v44.1.02
16. Henry A, Katsoulis M, Masi S, et al. The relationship between sleep duration, cognition and dementia: a Mendelian randomization study. Int J Epidemiol. 2019;48(3):849–860. doi:10.1093/ije/dyz071
17. Spirtes P, Glymour C, Scheines R. Causation, Prediction, and Search. The MIT Press; 2001.
18. Ohayon MM, Reynolds CF, Dauvilliers Y. Excessive sleep duration and quality of life. Ann Neurol. 2013;73(6):785–794. doi:10.1002/ana.23818
19. Vitiello MV, Larsen LH, Moe KE. Age-related sleep change: gender and estrogen effects on the subjective–objective sleep quality relationships of healthy, noncomplaining older men and women. J Psychosom Res. 2004;56(5):503–510. doi:10.1016/S0022-3999(04)00023-6
20. Buysse DJ, Ancoli-Israel S, Edinger JD, Lichstein KL, Morin CM. Recommendations for a standard research assessment of insomnia. Sleep. 2006;29(9):1155–1173. doi:10.1093/sleep/29.9.1155
21. Adams GC, Stoops MA, Skomro RP. Sleep tight: exploring the relationship between sleep and attachment style across the life span. Sleep Med Rev. 2014;18(6):495–507. doi:10.1016/j.smrv.2014.03.002
22. Cuthbert BN, Insel TR. Toward the future of psychiatric diagnosis: the seven pillars of RDoC. BMC Med. 2013;11:126. doi:10.1186/1741-7015-11-126
23. Cuthbert BN, Kozak MJ. Constructing constructs for psychopathology: the NIMH research domain criteria. J Abnorm Psychol. 2013;122(3):928–937. doi:10.1037/a0034028
24. Van Essen DC, Ugurbil K, Auerbach E, et al. The human connectome project: a data acquisition perspective. Neuroimage. 2012;62(4):2222–2231. doi:10.1016/j.neuroimage.2012.02.018
25. van Buuren S, Groothuis-Oudshoorn K. mice: multivariate imputation by chained equations in R. J Stat Softw. 2011;45(3):1–67. doi:10.18637/jss.v045.i03
26. Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. doi:10.1016/0165-1781(89)90047-4
27. Smith SM, Nichols TE, Vidaurre D, et al. A positive-negative mode of population covariation links brain connectivity, demographics and behavior. Nat Neurosci. 2015;18(11):1565–1567. doi:10.1038/nn.4125
28. Bernaards CA, Jennrich RI. Gradient projection algorithms and software for arbitrary rotation criteria in factor analysis. Educ Psychol Meas. 2005;65(5):676–696. doi:10.1177/0013164404272507
29. Revelle W. psych: procedures for personality and psychological research. 2017.
30. Fuller EL, Hemmerle WJ. Robustness of the maximum-likelihood estimation procedure in factor analysis. Psychometrika. 1966;31(2):255–266. doi:10.1007/bf02289512
31. Muthen B, Kaplan D. A comparison of some methodologies for the factor analysis of non-normal Likert variables: a note on the size of the model. Br J Math Stat Psychol. 1992;45(1):19–30. doi:10.1111/j.2044-8317.1992.tb00975.x
32. Horn JL. A rationale and test for the number of factors in factor analysis. Psychometrika. 1965;30(2):179–185. doi:10.1007/BF02289447
33. Rawls E, Kummerfeld E, Zilverstand A. An integrated multimodal model of alcohol use disorder generated by data-driven causal discovery analysis. Commun Biol. 2021;4(1):435. doi:10.1038/s42003-021-01955-z
34. Glasser MF, Sotiropoulos SN, Wilson JA, et al. The minimal preprocessing pipelines for the Human Connectome Project. Neuroimage. 2013;80:105–124. doi:10.1016/j.neuroimage.2013.04.127
35. Seitzman BA, Gratton C, Marek S, et al. A set of functionally-defined brain regions with improved representation of the subcortex and cerebellum. Neuroimage. 2020;206:116290. doi:10.1016/j.neuroimage.2019.116290
36. Power JD, Cohen AL, Nelson SM, et al. Functional network organization of the human brain. Neuron. 2011;72(4):665–678. doi:10.1016/j.neuron.2011.09.006
37. Hagler DJ, Hatton S, Cornejo MD, et al. Image processing and analysis methods for the adolescent brain cognitive development study. Neuroimage. 2019;202:116091. doi:10.1016/j.neuroimage.2019.116091
38. Mamah D, Barch DM, Repovš G. Resting state functional connectivity of five neural networks in bipolar disorder and schizophrenia. J Affect Disord. 2013;150(2):601–609. doi:10.1016/j.jad.2013.01.051
39. Repovs G, Csernansky JG, Barch DM. Brain network connectivity in individuals with schizophrenia and their siblings. Biol Psychiatry. 2011;69(10):967–973. doi:10.1016/j.biopsych.2010.11.009
40. Van Dijk KR, Hedden T, Venkataraman A, Evans KC, Lazar SW, Buckner RL. Intrinsic functional connectivity as a tool for human connectomics: theory, properties, and optimization. J Neurophysiol. 2010;103(1):297–321. doi:10.1152/jn.00783.2009
41. Ogarrio JM, Spirtes P, Ramsey J. A hybrid causal search algorithm for latent variable models. JMLR Workshop Conf Proc. 2016;52:368–379.
42. Ramsey J, Glymour M, Sanchez-Romero R, Glymour C. A million variables and more: the Fast Greedy Equivalence Search algorithm for learning high-dimensional graphical causal models, with an application to functional magnetic resonance images. Int J Data Sci Anal. 2017;3(2):121–129. doi:10.1007/s41060-016-0032-z
43. Schwarz G. Estimating the dimension of a model. Ann Stat. 1978;6(2):461–464.
44. Ramsey J. Scaling up Greedy equivalence search for continuous variables. ArXiv, abs/1507.07749. 2015.
45. Chickering DM. Optimal structure identification with greedy search. J Mach Learn Res. 2003;3:507–554. doi:10.1162/153244303321897717
46. Rosseel Y. lavaan: an R Package for Structural Equation Modeling. J Stat Softw. 2012;48(2):1–36. doi:10.18637/jss.v048.i02
47. Dziuban CD, Shirkey EC. When is a correlation matrix appropriate for factor analysis? Some decision rules. Psychol Bull. 1974;81(6):358–361. doi:10.1037/h0036316
48. Kemeny ME. The psychobiology of stress. Curr Dir Psychol Sci. 2003;12:124–129.
49. Zhaoyang R, Scott SB, Smyth JM, Kang JE, Sliwinski MJ. Emotional responses to stressors in everyday life predict long-term trajectories of depressive symptoms. Ann Behav Med. 2020;54(6):402–412. doi:10.1093/abm/kaz057
50. Clancy F, Prestwich A, Caperon L, Tsipa A, O’Connor DB. The association between worry and rumination with sleep in non-clinical populations: a systematic review and meta-analysis. Health Psychol Rev. 2020;14(4):427–448. doi:10.1080/17437199.2019.1700819
51. Kirchner L, Kube T, Berg M, et al. Social expectations in depression. Nat Rev Psychol. 2025;4(1):20–34. doi:10.1038/s44159-024-00386-x
52. Naragon-Gainey K, McMahon TP, Park J. The contributions of affective traits and emotion regulation to internalizing disorders: current state of the literature and measurement challenges. Am Psychol. 2018;73(9):1175–1186. doi:10.1037/amp0000371
53. Yu H, Gao X, Shen B, Hu Y, Zhou X. A levels-of-analysis framework for studying social emotions. Nat Rev Psychol. 2024;3(3):198–213. doi:10.1038/s44159-024-00285-1
54. Edition F. Diagnostic and statistical manual of mental disorders. Am Psychiatr Assoc. 2013;21(21):591–643.
55. Ionescu CG, Popa-Velea O, Mihăilescu AI, Talaşman AA, Bădărău IA. Somatic symptoms and sleep disorders: a literature review of their relationship, comorbidities and treatment. Healthcare. 2021;9(9):1128. doi:10.3390/healthcare9091128
56. Fu X, Zhang F, Huang M, Zhang L, Guo W. Editorial: brain and somatization symptoms in psychiatric disorders, volume II. Front Psychiatry. 2022;13:881245. doi:10.3389/fpsyt.2022.881245
57. Kılınçarslan MG, Ocak Ö, Şahin EM. The impact of neuropsychiatric burden on Restless Legs Syndrome (RLS) disease severity. Sleep Med. 2025;126:82–87. doi:10.1016/j.sleep.2024.12.004
58. Albinni B, de Zambotti M, Iacovides S, Baker FC, King CD. The complexities of the sleep-pain relationship in adolescents: a critical review. Sleep Med Rev. 2023;67:101715. doi:10.1016/j.smrv.2022.101715
59. Zhang J, Lam SP, Li SX, et al. Insomnia, sleep quality, pain, and somatic symptoms: sex differences and shared genetic components. Pain. 2012;153(3):666–673. doi:10.1016/j.pain.2011.12.003
60. Walentynowicz M, Raes F, Van Diest I, Van den Bergh O. The specificity of health-related autobiographical memories in patients with somatic symptom disorder. Psychosom Med. 2017;79(1):43–49. doi:10.1097/psy.0000000000000357
61. Lund HG, Reider BD, Whiting AB, Prichard JR. Sleep patterns and predictors of disturbed sleep in a large population of college students. J Adolesc Health. 2010;46(2):124–132. doi:10.1016/j.jadohealth.2009.06.016
62. Feussner O, Rehnisch C, Rabkow N, Watzke S. Somatization symptoms-prevalence and risk, stress and resilience factors among medical and dental students at a mid-sized German university. PeerJ. 2022;10:e13803. doi:10.7717/peerj.13803
63. Bonvanie IJ, Janssens KA, Rosmalen JG, Oldehinkel AJ. Life events and functional somatic symptoms: a population study in older adolescents. Br J Psychol. 2017;108(2):318–333. doi:10.1111/bjop.12198
64. Henson-García M, Weerakoon SM, Duncan C, et al. Assessing the prevalence rates of internalizing symptomatology among multiracial adolescents in the United States: a systematic review. Child Psychiatry Human Dev. 2023;2023:1–4. doi:10.1007/s10578-023-01636-4
65. Schnabel K, Petzke TM, Witthöft M. The emotion regulation process in somatic symptom disorders and related conditions - A systematic narrative review. Clinic Psychol Rev. 2022;97:102196. doi:10.1016/j.cpr.2022.102196
66. Curtis BJ, Williams PG, Anderson JS. Objective cognitive functioning in self-reported habitual short sleepers not reporting daytime dysfunction: examination of impulsivity via delay discounting. Sleep. 2018;41(9):zsy115. doi:10.1093/sleep/zsy115
67. Lim JYL, Killgore WDS, Bennett D, Drummond SPA. The impact of sleep loss on decision making: opening the cognitive black box. Sleep Med Rev. 2025;82:102114. doi:10.1016/j.smrv.2025.102114
68. Walker MP. The role of sleep in cognition and emotion. Ann N Y Acad Sci. 2009;1156:168–197. doi:10.1111/j.1749-6632.2009.04416.x
69. Peters J, Büchel C. The neural mechanisms of inter-temporal decision-making: understanding variability. Trends Cognit Sci. 2011;15(5):227–239. doi:10.1016/j.tics.2011.03.002
70. Massar SAA, Chee MWL. Sleep and delay discounting: is insufficient sleep a cause or a manifestation of short-sighted choice? Sleep. 2019;42(4):zsz005. doi:10.1093/sleep/zsz005
71. King DL, Gradisar M, Drummond A, et al. The impact of prolonged violent video-gaming on adolescent sleep: an experimental study. J Sleep Res. 2013;22(2):137–143. doi:10.1111/j.1365-2869.2012.01060.x
72. Munezawa T, Kaneita Y, Osaki Y, et al. The association between use of mobile phones after lights out and sleep disturbances among Japanese adolescents: a nationwide cross-sectional survey. Sleep. 2011;34(8):1013–1020. doi:10.5665/sleep.1152
73. Shamosh NA, Gray JR. Delay discounting and intelligence: a meta-analysis. Intelligence. 2008;36(4):289–305. doi:10.1016/j.intell.2007.09.004
74. Hirsh JB, Morisano D, Peterson JB. Delay discounting: interactions between personality and cognitive ability. J Res Personality. 2008;42(6):1646–1650. doi:10.1016/j.jrp.2008.07.005
75. Robles E, Huang BE, Simpson PM, McMillan DE. Delay discounting, impulsiveness, and addiction severity in opioid-dependent patients. J Subst Abuse Treat. 2011;41(4):354–362. doi:10.1016/j.jsat.2011.05.003
76. Hildebrandt MK, Dieterich R, Endrass T. Neural correlates of inhibitory control in relation to the degree of substance use and substance-related problems – a systematic review and perspective. Neurosci Biobehav Rev. 2021;128:1–11. doi:10.1016/j.neubiorev.2021.06.011
77. Bzdok D, Hartwigsen G, Reid A, Laird AR, Fox PT, Eickhoff SB. Left inferior parietal lobe engagement in social cognition and language. Neurosci Biobehav Rev. 2016;68:319–334. doi:10.1016/j.neubiorev.2016.02.024
78. Stockert A, Wawrzyniak M, Klingbeil J, et al. Dynamics of language reorganization after left temporo-parietal and frontal stroke. Brain. 2020;143(3):844–861. doi:10.1093/brain/awaa023
79. Qiu Z, Wang J. Altered neural activities during response inhibition in adults with addiction: a voxel-wise meta-analysis. Psychol Med. 2021;51(3):387–399. doi:10.1017/s0033291721000362
80. Viviani R. Emotion regulation, attention to emotion, and the ventral attentional network. Front Hum Neurosci. 2013;7:746. doi:10.3389/fnhum.2013.00746
81. Tessner KD, Hill SY. Neural circuitry associated with risk for alcohol use disorders. Neuropsychol Rev. 2010;20(1):1–20. doi:10.1007/s11065-009-9111-4
82. Groeger JA, Zijlstra FR, Dijk DJ. Sleep quantity, sleep difficulties and their perceived consequences in a representative sample of some 2000 British adults. J Sleep Res. 2004;13(4):359–371. doi:10.1111/j.1365-2869.2004.00418.x
83. Zhang B, Wing YK. Sex differences in insomnia: a meta-analysis. Sleep. 2006;29(1):85–93. doi:10.1093/sleep/29.1.85
84. Dorsey A, de Lecea L, Jennings KJ. Neurobiological and hormonal mechanisms regulating women’s sleep. Front Neurosci. 2020;14:625397. doi:10.3389/fnins.2020.625397
85. Ohayon MM, Carskadon MA, Guilleminault C, Vitiello MV. Meta-analysis of quantitative sleep parameters from childhood to old age in healthy individuals: developing normative sleep values across the human lifespan. Sleep. 2004;27(7):1255–1273. doi:10.1093/sleep/27.7.1255
86. Redline S, Kirchner HL, Quan SF, Gottlieb DJ, Kapur V, Newman A. The effects of age, sex, ethnicity, and sleep-disordered breathing on sleep architecture. Arch Intern Med. 2004;164(4):406–418. doi:10.1001/archinte.164.4.406
87. Goel N, Kim H, Lao RP. Gender differences in polysomnographic sleep in young healthy sleepers. Chronobiol Int. 2005;22(5):905–915. doi:10.1080/07420520500263235
88. Mong JA, Baker FC, Mahoney MM, et al. Sleep, rhythms, and the endocrine brain: influence of sex and gonadal hormones. J Neurosci. 2011;31(45):16107–16116. doi:10.1523/jneurosci.4175-11.2011
89. van de Straat V, Bracke P. How well does Europe sleep? A cross-national study of sleep problems in European older adults. Int J Public Health. 2015;60(6):643–650. doi:10.1007/s00038-015-0682-y
90. Suh S, Cho N, Zhang J. Sex differences in insomnia: from epidemiology and etiology to intervention. Curr Psychiatry Rep. 2018;20(9):69. doi:10.1007/s11920-018-0940-9
91. Camhi SL, Morgan WJ, Pernisco N, Quan SF. Factors affecting sleep disturbances in children and adolescents. Sleep Med. 2000;1(2):117–123. doi:10.1016/s1389-9457(99)00005-2
92. Johnson EO, Roth T, Schultz L, Breslau N. Epidemiology of DSM-IV insomnia in adolescence: lifetime prevalence, chronicity, and an emergent gender difference. Pediatrics. 2006;117(2):e247–56. doi:10.1542/peds.2004-2629
93. Morssinkhof MWL, van Wylick DW, Priester-Vink S, et al. Associations between sex hormones, sleep problems and depression: a systematic review. Neurosci Biobehav Rev. 2020;118:669–680. doi:10.1016/j.neubiorev.2020.08.006
94. Harrington YA, Parisi JM, Duan D, Rojo-Wissar DM, Holingue C, Spira AP. Sex hormones, sleep, and memory: interrelationships across the adult female lifespan. Front Aging Neurosci. 2022;14:800278. doi:10.3389/fnagi.2022.800278
95. Gujar N, McDonald SA, Nishida M, Walker MP. A role for REM sleep in recalibrating the sensitivity of the human brain to specific emotions. Cereb Cortex. 2011;21(1):115–123. doi:10.1093/cercor/bhq064
96. Meers J, Stout-Aguilar J, Nowakowski S. Chapter 3 - Sex differences in sleep health. In: Grandner MA, editor. Sleep and Health. Academic Press; 2019:21–29.
97. Liang J, Qian C. Gender differences in the effects of sleep deprivation on emotional reactivity. Chin Gen Pract. 2019;23:861–865. doi:10.12114/j.issn.1007-9572.2019.00.450
98. Baglioni C, Spiegelhalder K, Lombardo C, Riemann D. Sleep and emotions: a focus on insomnia. Sleep Med Rev. 2010;14(4):227–238. doi:10.1016/j.smrv.2009.10.007
99. Brissette I, Cohen S. The contribution of individual differences in hostility to the associations between daily interpersonal conflict, affect, and sleep. Pers Soc Psychol Bull. 2002;28:1265–1274. doi:10.1177/01461672022812011
100. Turton S, Campbell C. Tend and befriend versus fight or flight: gender differences in behavioral response to stress among university students. J Appl Biobehav Res. 2005;10(4):209–232. doi:10.1111/j.1751-9861.2005.tb00013.x
101. Malagón-Amor Á, Martín-López LM, Córcoles D, et al. Family features of social withdrawal syndrome (Hikikomori). Front Psychiatry. 2020;11:138. doi:10.3389/fpsyt.2020.00138
102. Porcelli S, Van Der Wee N, van der Werff S, et al. Social brain, social dysfunction and social withdrawal. Neurosci Biobehav Rev. 2019;97:10–33. doi:10.1016/j.neubiorev.2018.09.012
103. Giacobo RS, Jané MC, Bonillo A, Arrufat FJ, Araujo E. ADHD and functional somatic symptoms: structural equations of a conceptual model. Child Adolesc Ment Health. 2014;19(2):83–89. doi:10.1111/camh.12026
104. Mahalik JR, Burns SM, Syzdek M. Masculinity and perceived normative health behaviors as predictors of men’s health behaviors. Soc Sci Med. 2007;64(11):2201–2209. doi:10.1016/j.socscimed.2007.02.035
105. Schrock D, Schwalbe M. Men, masculinity, and manhood acts. Annu Rev Sociol. 2009;35(1):277–295. doi:10.1146/annurev-soc-070308-115933
106. Weeks JW, Rodebaugh TL, Heimberg RG, Norton PJ, Jakatdar TA. “To Avoid Evaluation, Withdraw”: fears of evaluation and depressive cognitions lead to social anxiety and submissive withdrawal. Cognitive Ther Res. 2009;33(4):375–389. doi:10.1007/s10608-008-9203-0
107. Sette S, Pecora G, Laghi F, Coplan RJ. Motivations for social withdrawal, mental health, and well-being in emerging adulthood: a person-oriented approach. Behav Sci. 2023;13(12):977. doi:10.3390/bs13120977
108. Becker JB, Hu M. Sex differences in drug abuse. Front Neuroendocrinol. 2008;29(1):36–47. doi:10.1016/j.yfrne.2007.07.003
109. Hernandez-Avila CA, Rounsaville BJ, Kranzler HR. Opioid-, cannabis- and alcohol-dependent women show more rapid progression to substance abuse treatment. Drug Alcohol Depend. 2004;74(3):265–272. doi:10.1016/j.drugalcdep.2004.02.001
110. Pine A, Shiner T, Seymour B, Dolan RJ. Dopamine, time, and impulsivity in humans. J Neurosci. 2010;30(26):8888–8896. doi:10.1523/jneurosci.6028-09.2010
111. Diergaarde L, Pattij T, Poortvliet I, et al. Impulsive choice and impulsive action predict vulnerability to distinct stages of nicotine seeking in rats. Biol Psychiatry. 2008;63(3):301–308. doi:10.1016/j.biopsych.2007.07.011
112. Rogers RD, Everitt BJ, Baldacchino A, et al. Dissociable deficits in the decision-making cognition of chronic amphetamine abusers, opiate abusers, patients with focal damage to prefrontal cortex, and tryptophan-depleted normal volunteers: evidence for monoaminergic mechanisms. Neuropsychopharmacology. 1999;20(4):322–339. doi:10.1016/s0893-133x(98)00091-8
113. Wise RA, Robble MA. Dopamine and addiction. Annu Rev Psychol. 2020;71(1):79–106.
114. Bickel WK, Odum AL, Madden GJ. Impulsivity and cigarette smoking: delay discounting in current, never, and ex-smokers. Psychopharmacology. 1999;146(4):447–454. doi:10.1007/pl00005490
115. Martini F, Fregna L, Bosia M, Perrozzi G, Cavallaro R. Substance-Related Disorders. In: Cavallaro R, Colombo C, editors. Fundamentals of Psychiatry for Health Care Professionals. Springer International Publishing; 2022:263–295.
116. Bahji A, Stephenson C, Tyo R, Hawken ER, Seitz DP. Prevalence of cannabis withdrawal symptoms among people with regular or dependent use of cannabinoids: a systematic review and meta-analysis. JAMA Network Open. 2020;3(4):e202370. doi:10.1001/jamanetworkopen.2020.2370
117. Flores-Bonilla A, Richardson HN. Sex differences in the neurobiology of alcohol use disorder. Alcohol Res. 2020;40(2):04. doi:10.35946/arcr.v40.2.04
118. Morris VL, Owens MM, Syan SK, et al. Associations between drinking and cortical thickness in younger adult drinkers: findings from the human connectome project. Alcohol Clin Exp Res. 2019;43(9):1918–1927. doi:10.1111/acer.14147
119. Blair RJ. The amygdala and ventromedial prefrontal cortex in morality and psychopathy. Trends Cognit Sci. 2007;11(9):387–392. doi:10.1016/j.tics.2007.07.003
120. Grav S, Hellzèn O, Romild U, Stordal E. Association between social support and depression in the general population: the HUNT study, a cross-sectional survey. J Clin Nurs. 2012;21(1–2):111–120. doi:10.1111/j.1365-2702.2011.03868.x
121. Jolly PM, Kong DT, Kim KY. Social support at work: an integrative review. J Organ Behav. 2021;42(2):229–251. doi:10.1002/job.2485
122. Ayalon L, Shiovitz-Ezra S, Palgi Y. Associations of loneliness in older married men and women. Aging Mental Health. 2013;17(1):33–39. doi:10.1080/13607863.2012.702725
123. Umberson D, Montez JK. Social relationships and health: a flashpoint for health policy. J Health Soc Behav. 2010;51(Suppl):S54–66. doi:10.1177/0022146510383501
124. Gellman MD. Behavioral Medicine. In: Gellman MD, editor. Encyclopedia of Behavioral Medicine. Springer International Publishing; 2020:223–226.
125. Luo Q, Shao R. The positive and negative emotion functions related to loneliness: a systematic review of behavioural and neuroimaging studies. Psychoradiology. 2023;3:kkad029. doi:10.1093/psyrad/kkad029
126. Cho SC, Kim BN, Kim JW, et al. Full syndrome and subthreshold attention-deficit/hyperactivity disorder in a Korean community sample: comorbidity and temperament findings. Eur Child Adolesc Psychiatry. 2009;18(7):447–457. doi:10.1007/s00787-009-0755-7
127. Holmberg K, Hjern A. Health complaints in children with attention-deficit/hyperactivity disorder. Acta Paediatr. 2006;95(6):664–670. doi:10.1080/08035250600717121
128. Legenbauer T, Vocks S, Schäfer C, et al. Preference for attractiveness and thinness in a partner: influence of internalization of the thin ideal and shape/weight dissatisfaction in heterosexual women, heterosexual men, lesbians, and gay men. Body Image. 2009;6(3):228–234. doi:10.1016/j.bodyim.2009.04.002
129. Robles TF, Slatcher RB, Trombello JM, McGinn MM. Marital quality and health: a meta-analytic review. Psychol Bull. 2014;140(1):140–187. doi:10.1037/a0031859
130. Panagiotidi M, Overton PG, Stafford T. The relationship between ADHD traits and sensory sensitivity in the general population. Compr Psychiatry. 2018;80:179–185. doi:10.1016/j.comppsych.2017.10.008
131. Beck JE. A developmental perspective on functional somatic symptoms. J Pediatr Psychol. 2008;33(5):547–562. doi:10.1093/jpepsy/jsm113
132. Chrousos GP. Stress and disorders of the stress system. Nat Rev Endocrinol. 2009;5(7):374–381. doi:10.1038/nrendo.2009.106
133. Adamczyk K. An investigation of loneliness and perceived social support among single and partnered young adults. Curr Psychol. 2016;35(4):674–689. doi:10.1007/s12144-015-9337-7
134. Shaw P, Stringaris A, Nigg J, Leibenluft E. Emotion dysregulation in attention deficit hyperactivity disorder. Am J Psychiatry. 2014;171(3):276–293. doi:10.1176/appi.ajp.2013.13070966
135. Beheshti A, Chavanon ML, Christiansen H. Emotion dysregulation in adults with attention deficit hyperactivity disorder: a meta-analysis. BMC Psychiatry. 2020;20(1):120. doi:10.1186/s12888-020-2442-7
136. Shamosh NA, Deyoung CG, Green AE, et al. Individual differences in delay discounting: relation to intelligence, working memory, and anterior prefrontal cortex. Psychol Sci. 2008;19(9):904–911. doi:10.1111/j.1467-9280.2008.02175.x
137. Zaval L, Li Y, Johnson EJ, Weber EU. Chapter 8 - complementary contributions of fluid and crystallized intelligence to decision making across the life span. In: Hess TM, Strough J, Löckenhoff CE, editors. Aging and Decision Making. Academic Press; 2015:149–168.
138. Su C, Zhou KZ, Zhou N, Li JJ. Harmonizing conflict in husband–wife purchase decision making: perceived fairness and spousal influence dynamics. J Acad Mark Sci. 2008;36(3):378–394. doi:10.1007/s11747-007-0079-4
139. DePaulo BM, Morris WL. TARGET ARTICLE: singles in society and in science. Psychol Inq. 2005;16(2–3):57–83. doi:10.1080/1047840X.2005.9682918
140. Mander BA, Winer JR, Walker MP. Sleep and human aging. Neuron. 2017;94(1):19–36. doi:10.1016/j.neuron.2017.02.004
141. Insel T, Cuthbert B, Garvey M, et al. Research domain criteria (RDoC): toward a new classification framework for research on mental disorders. Am J Psychiatry. 2010;167(7):748–751. doi:10.1176/appi.ajp.2010.09091379
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.