Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Exploring Barriers and Facilitators to Early Rehabilitation in Post-Stroke Hand Dysfunction: A Qualitative Study
Authors Qin X, Zou Q, He Y, Liu L, Zhao C
Received 10 April 2025
Accepted for publication 18 July 2025
Published 31 July 2025 Volume 2025:18 Pages 4469—4480
DOI https://doi.org/10.2147/JMDH.S533560
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Krzysztof Laudanski
Xiaohuan Qin,1,2,* Qinhan Zou,3,* Yanan He,4 Lang Liu,5 Chunyan Zhao2
1School of Medicine, Tongji University, Shanghai, 200092, People’s Republic of China; 2Nursing Department, Shanghai East Hospital, School of Medicine, Tongji University, Shanghai, 200120, People’s Republic of China; 3Nursing Department, Shanghai Key Laboratory of Maternal Fetal Medicine, Shanghai Institute of Maternal-Fetal Medicine and Gynecologic Oncology, Shanghai First Maternity and Infant Hospital, School of Medicine, Tongji University, Shanghai, 200092, People’s Republic of China; 4Department of Respiratory and Critical Care Medicine, Shanghai East Hospital, School of Medicine, Tongji University, Shanghai, 200120, People’s Republic of China; 5Center of Gallbladder Disease, Shanghai East Hospital, School of Medicine, Tongji University, Shanghai, 200120, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Chunyan Zhao, Nursing Department, Shanghai East Hospital, School of Medicine, Tongji University, 150 Jimo Road, Shanghai, 200120, People’s Republic of China, Email [email protected]
Background: Early rehabilitation can improve limb function and enhance quality of life for patients with hand dysfunction following a stroke. Currently, there is a lack of research exploring the factors that facilitate or hinder the participation of patients with hand dysfunction in early rehabilitation. Exploring these factors is crucial for the formulation of strategies aimed at boosting patients’ motivation towards early rehabilitation and cultivating their proactive engagement.
Aim: This study aimed to explore the barriers and facilitators to early rehabilitation in post-stroke hand dysfunction.
Methods: This is a descriptive qualitative study. 15 patients with post-stroke hand dysfunction were selected using the purposive sampling method. Data were collected through semi-structured, face-to-face, in-depth interviews conducted at a tertiary hospital in Shanghai, China, between March and April 2024. The data were coded using NVivo software and analyzed via Braun and Clarke’s reflective thematic approach.
Results: Four themes were identified, encompassing eight sub-themes: (1) gaining benefits from early treatments, (2) active participation of individuals and their families, (3) a low level of perceived self-efficacy, and (4) unmet medical needs.
Conclusion: The likelihood of patients with hand dysfunction following a stroke participating in early rehabilitation treatments is influenced by numerous factors. Intervention strategies can be tailored around these factors and may include educating patients and their families about stroke and early rehabilitation, training healthcare professionals (HCPs) to enhance their skills, providing professional support to patients after discharge and optimizing health insurance policies.
Keywords: stroke, hand dysfunction, early rehabilitation treatments, barriers, facilitators, qualitative study
Introduction
Stroke is a sudden event involving bleeding or blockages in blood vessels, leading to disturbances in local blood circulation. It is most prevalent among the elderly and includes types such as ischemic strokes, intracranial hemorrhage, and subarachnoid hemorrhage.1 Approximately 87% of strokes are ischemic. In China, the annual incidence rate of stroke among people over the age of 40 is approximately 500 cases per 100,000 people, which is higher than the global average.2 Furthermore, the incidence rate of stroke doubles every ten years after the age of 60.3 This extremely high incidence rate has placed a huge burden on the medical system. Although patients receive timely therapy after an acute episode, approximately 75% experience motor dysfunction in the limbs, particularly in the distal upper limb (eg, hand dysfunction).4 Early rehabilitation treatment has been proven to be effective for stroke patients hand dysfunction.5 Patients who receive early, continuous, professional, and systematic rehabilitation are likely to recover more quickly.6,7
Exercise rehabilitation is the primary treatment for stroke patients in the early rehabilitation phase. Exercise rehabilitation encompasses a variety of techniques, including bilateral training, repetitive task training, constraint-induced movement therapy, electrical stimulation, and robotic therapy, among others.8 It has been specially designed to restore damaged muscles and enhance overall physical capability, helping patients to regain their ability to perform daily activities. Additionally, it plays a significant role in reducing the recurrence rate of cardiovascular diseases and preventing mortality.9 Throughout the physical exercise regimen, patients develop the ability to refine and optimize their motor, sensory, and cognitive functions through carefully administered, repetitive, goal-focused, progressive, task-specific, and context-specific training.10 Compared with late rehabilitation, early rehabilitation can significantly improve patients’ ability to improve self-care and daily activities, as well as restore neurological function.11 Therefore, HCPs should promote the active involvement of stroke patients with hand dysfunction in early rehabilitation.
Currently, the compliance rate of stroke patients with the early rehabilitation post-discharge remains relatively low. In other countries, this rate ranges from 28% to 68.6%.12–14 In China, however, it is even lower, ranging from 18% to 37%.15 Therefore, there is an urgent need for research aimed at increasing stroke patients’ enthusiasm for early rehabilitation and encouraging their participation. At present, there is a paucity of research concerning the factors that influence rehabilitation behaviors in stroke patients with hand dysfunction. The identified factors include age, gender, history of stroke, residential location, stigma, effective communication, and cost.16–20 Qualitative research enables researchers to gain a deeper understanding of patients’experiences and insights during their rehabilitation process. This is a crucial step in developing personalised intervention measures to improve treatment compliance. However, there is still a lack of qualitative research into the factors affecting hand dysfunction in stroke patients during early rehabilitation in China.
This study aimed to explore the factors influencing the participation of stroke patients with hand dysfunction in early rehabilitation after discharge. A qualitative research method21 was used to gain insight into the rehabilitation experiences of these patients. This approach can capture more information that cannot be obtained through quantitative research methods.
Methods
Study Design
This qualitative study employed phenomenological methods, consisting of conducting individualized, semi-structured interviews to gain an in-depth understanding of the experiences of patients with hand dysfunction following stroke during the early rehabilitation phase at a tertiary hospital in Shanghai, China. Descriptive phenomenological methods were used to explore the experience of stroke-induced hand dysfunction during rehabilitation treatment, including physical exercise, dietary interventions, social activities, and communication with HCPs. This approach facilitates a profound understanding of patients’ perceptions and awareness of their rehabilitation experiences, as well as revealing their actual needs.22 Descriptive phenomenology requires the researcher to suspend all personal knowledge and biases, adopt an open-minded approach, and describe the phenomena without any preconceptions.23
Participants and Recruitment
Participants were recruited from East Hospital Affiliated with Tongji University, China, through purposive sampling from March 2024 to April 2024. Inclusion criteria of participants who were: (1) diagnosed with stroke using CT and MRI scans, according to the criteria of the Guidelines for the Diagnosis and Treatment of Acute Ischemic Stroke in China (2018) and Guidelines for the Diagnosis and Treatment of Cerebral Hemorrhage in China (2019);24,25 2) they were undergoing rehabilitation after their first stroke within six months; (3) their limbs were dysfunctional, and their Brunstrom stage was between I and V; (4) they volunteered and provided written informed consent to participate in this study; and (5) they were aged 18 years or older. Exclusion criteria for participants in this study included suffering from other systemic complications, critical illness, language and communication disorders, cognitive disorders, or psychiatric disorders. We used the maximum variance sampling method to gain a deeper understanding of stroke patients’ thoughts during the rehabilitation process. The sampling was based on a maximum variance of participant’ characteristics (eg, age, gender, education and insurance).26,27 The potential participants were contacted via telephone. Prior to the interview, participants were informed of the purpose, methodology, benefits, and risks of the study. 15 stroke patients with hand dysfunction agreed to take part in the study and signed an informed consent. After completing interviews with these 15 patients, we confirmed that data saturation was reached and no new insights emerged.
Data Collection
The data collection phase took place from March 2024 to April 2024. We collected data through face-to-face, in-depth, semi-structured interviews. The interview guide was initially generated by the study’s purpose, literature review, researcher’s experience and expert consultation. Then the interview guide (see Table 1) was refined through three pilot interviews, which were not included in the final analysis.
 |
Table 1 Interview Guide |
Prior to the study, the research team comprised nurses with extensive experience in stroke care and qualitative methodology. The interviews took place in a quiet room within the hospital, ensuring privacy and minimizing distractions. During the interview, the researcher flexibly adjusted the order and method of the questions according to the interview guide and participants’ responses. Although the interview questions were semi-structured, participants were encouraged to express any new insights during the interview. Interviews were audio-recorded, and the participants’ body movements and facial expressions were observed and recorded. Data collection continued until saturation was reached. The average interview duration was 30 minutes, ranging from 25 to 37 minutes. A total of 15 participants were interviewed, each participating in one interview only. To ensure accuracy, the transcripts were confirmed by the participants at the end of the interviews. To protect privacy, participants were coded from N1 to N15.
Data Analysis
The interviews were transcribed within 24 hours and analyzed using NVivo 12.0 software, with non-verbal behaviors integrated into the written transcriptions. The two researchers independently conducted a thorough thematic analysis by employing Braun and Clarke’s reflective thematic analysis approach.28 Thematic analysis, which involves the systematic identification, analysis, and interpretation of patterns or themes within the data, provides comprehensive insights into the factors contributing to the inadequate participation in early rehabilitation behaviors among patients with post-stroke hand dysfunction (see Table 2). To enhance the reliability of data coding and minimize potential biases in data interpretation, we engaged in discussions with the research team.
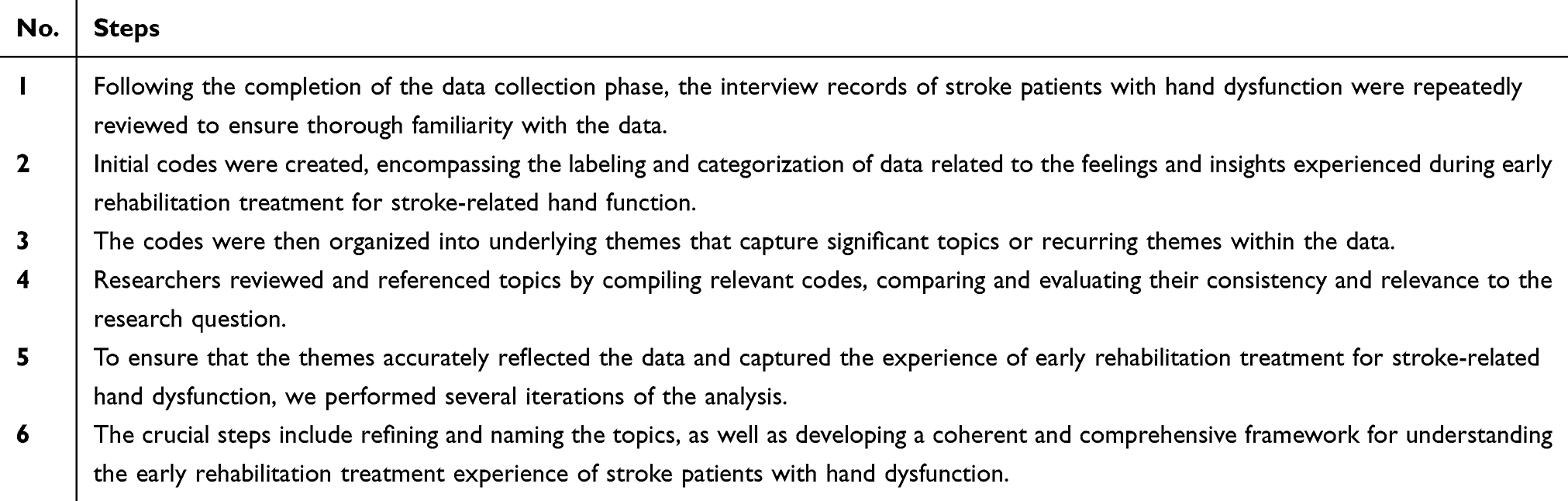 |
Table 2 Braun and Clarke’s Reflective Thematic Analysis |
Ethical Considerations
Ethical approval was granted by the Medical Ethics Committee of Shanghai East Hospital, affiliated with Tongji University (Approval number: [2022] Review No. (186)). Prior to this study, all participants were informed about the study’s purposes, methodologies and the format of interviews. After obtaining their consent, all participants signed a written informed consent. Additionally, they were informed that they could withdraw form this study at any time. They were also assured that their participation would not affect their ordinary care. Their identities were encoded to ensure privacy, and the data was used only for this study with their consent.
Rigor
Four criteria were used to ensure research rigor: credibility, transferability, dependability, and confirmability.29 Credibility was ensured through researcher triangulation and confirmed the data with the participants. Dependability and confirmability of the study were ensured by two external qualitative research experts, who reviewed the decision leads, findings, and conclusions. The researchers enhanced the transferability of the findings by providing detailed descriptions of the study’s background, purpose, methods, and analysis process, employing open-ended questions, and encouraging participants to express their ideas freely.
Results
In total, 15 participants completed this study. and their basic characteristics are presented in Table 3. The age of participants ranged from 53–69 years (average of 59.6 years), and included eight female (53.3%) and seven male stroke survivors (46.7%). 80% of participants had an ischemic stroke, 13.3% had an intracranial hemorrhage and 6.7% had a subarachnoid hemorrhage.
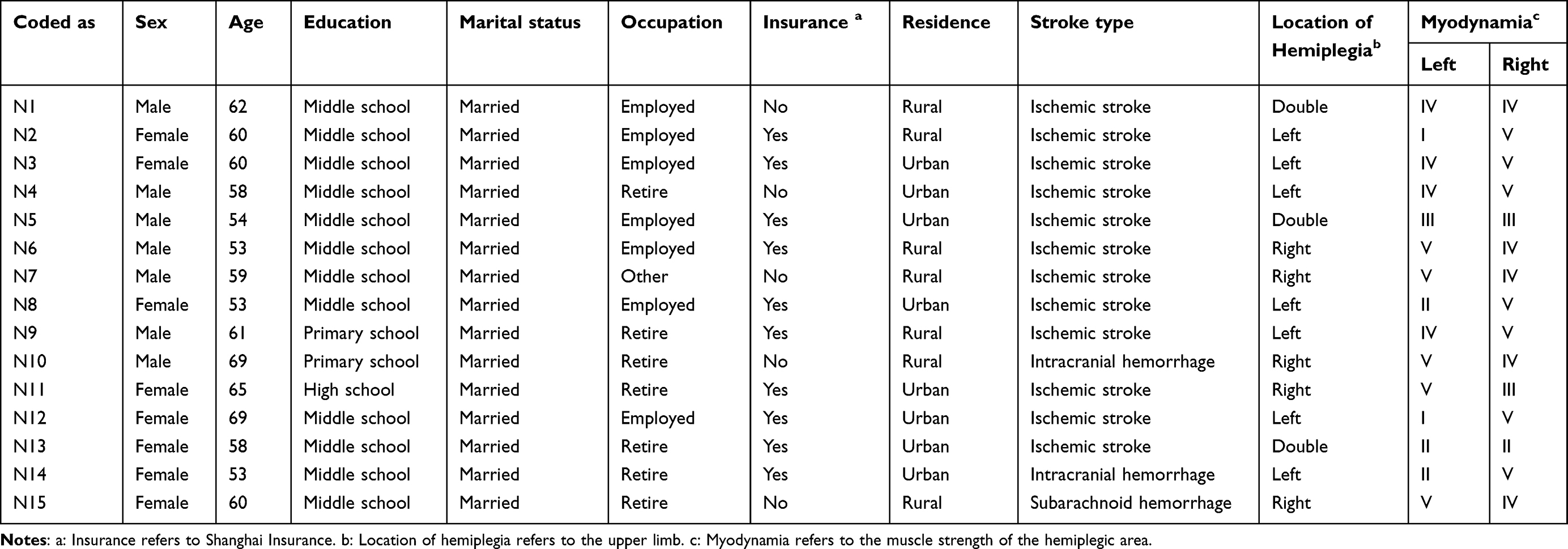 |
Table 3 Demographic Characteristics of 15 Patients |
We identified the facilitators and barriers that affect the participation of stroke patients with hand dysfunction in rehabilitation therapy. These factors were categorized into four themes and nine sub-themes: Facilitators: 1) gaining benefits from early treatments; 2) active participation of individuals and their families; and Barriers: 3) a low level of perceived self-efficacy; 4) unmet medical needs (see Figure 1).
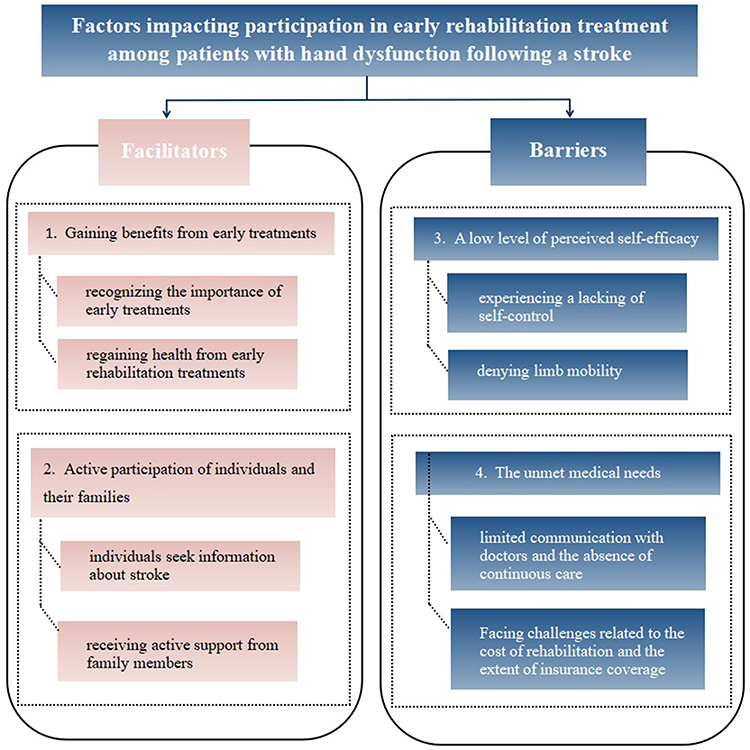 |
Figure 1 Themes and sub-themes. |
Theme 1: Gaining Benefits from Early Treatments
Sub-Theme 1: Recognizing the Importance of Early Treatments
For individuals who receive immediate treatment, their condition tends to be mild and often does not necessitate surgery. Patients who delay seeking medical attention for more than six hours following a stroke typically experience more significant impairments in hand function. They recognized that the prognosis of a stroke is intimately linked to the timeliness of treatment.
Due to the timely treatment, I did not undergo surgery. I began to recall and understand the process of stroke and realized the importance of time. (N7)
On Saturday night, I experienced palpitations and numbness in my hands. Mistakenly attributing these symptoms to fatigue, I took some medication and retired to bed early. It was only the following day, when the numbness in my hands persisted, that my family rushed me to the hospital. The doctor informed me that I had missed the window for thrombolytic therapy. I deeply regret not seeking immediate medical attention. (N5)
Sub-Theme 2: Regaining Health from Early Rehabilitation Treatments
Four patients maintained a positive outlook towards rehabilitation and embracing a healthy lifestyle, reporting that they had altered their detrimental habits and were on the road to recovery.
Following the stroke, my balance significantly deteriorated, causing me to easily lose stability while walking. However, after a month of dedicated rehabilitation training, I regained enough confidence and strength to take solo strolls around the neighborhood after dinner”. (N2)
Previously, I indulged in excessive drinking and neglected physical exercise. During my hospitalization, my doctor strongly encouraged me to engage actively in rehabilitation. As a result, I have quit drinking and have adopted a regular exercise regimen. Consequently, I feel healthier than ever before. (N13)
Theme 2: Active Participation of Individuals and Their Families
Sub-Theme 3: Individuals Seek Information About Stroke
Most patients are preoccupied with obtaining treatment information during the recovery period following a stroke. This includes understanding the nature of a stroke, its underlying causes, the quickest path to recovery, and the likelihood of recurrence. They tend to adhere to the recommendations of their healthcare professionals and also seek additional information through various platforms such as TikTok and Baidu.
“Doctors are professionals who are well-versed in my medical condition. When they recommended rehabilitation, I agreed without hesitation, bolstered by their positive reassurance, which instilled in me a sense of security”. (N14)
“Although I am advanced in years, I also enjoy engaging with platforms like TikTok and Baidu. Since my illness, I have frequently explored popular science videos on these platforms to gather information about stroke treatment, finding them to be immensely beneficial in my journey to recovery”. (N9)
Sub-Theme 4: Receiving Active Support from Family Members
Continuous care following discharge is crucial for expediting recovery, and its successful implementation is heavily dependent on family support, which includes both financial and emotional dimensions. This study revealed that patients who receive substantial family support exhibit a pronounced propensity towards actively participating in rehabilitation activities.
“Life after the stroke was extraordinarily challenging. I found it unbearable to experience my body as beyond my control. There was a period when I was reluctant to venture outdoors. However, my family reached out to friends, neighbors, and others to visit me, and their encouragement played a pivotal role in restoring my confidence in life”. (N8)
“My son diligently monitors my diet, and under his vigilant supervision, I have become accustomed to a low-sodium, low-fat dietary regimen. My daughter-in-law has enlisted the assistance of a nanny to manage the household chores, thereby enabling my wife to focus exclusively on my rehabilitation. Whenever I grow weary of exercising and contemplate abandoning my efforts, my family consistently provides comfort and encouragement, motivating me to persevere and try again”. (N13)
Theme 3: A Low Level of Perceived Self-Efficacy
Sub-Theme 5: Experiencing a Lack of Self-Control
Home-based rehabilitation encompassed the development of healthy eating habits. However, participants reported struggling with self-control in maintaining these dietary practices.
“I am able to adhere to a low-oil diet, but I find it challenging to tolerate a low-salt diet as it diminishes my appetite. Furthermore, I follow my doctor’s advice regarding exercise. The intense sweating resulting from physical activity leads to a decrease in salt levels in my body, necessitating the consumption of salty foods to replenish energy reserves”. (N15)
Sub-Theme 6: Denying of Limb Mobility
Patients were aware that their ability to walk was impaired due to a limb disorder following the stroke. They recognized their abnormality and consequently curtailed their daily activities to minimize the risk of injury, such as falling.
The doctor advised me to increase my walking, but with the abnormality in my left side, I find it challenging to walk unassisted. I can only manage to walk more with the support of my son holding me up. (N4)
Theme 4: Unmet Medical Needs
Sub-Theme 7: Limited Communication with Doctors and the Absence of Continuous Care
Participants reported that during their hospitalization, they observed their doctors to be extremely busy, with the majority of interactions confined to morning rounds. This limited communication can result in delayed comprehension of disease-related knowledge and treatment information for patients.
During the morning rounds, the doctor provided an explanation of my condition to me and my family. However, due to the high patient volume in the ward, the doctors have a restricted amount of time available for individual patient communication. (N6)
Although the doctor conveyed the treatment information during the ward rounds, I was unable to recall or comprehend it fully. When I attempted to seek further clarification from the doctor, the nurse informed me that he was unavailable as he was attending to surgical duties. (N11)
During hospitalization, patients reported more frequent interactions with nurses. They expressed gratitude for the nursing care and health guidance received, while also voicing concerns about the lack of continuous care following discharge.
I am immensely grateful to the nurses for the exceptional nursing care they provided, including administering injections, dispensing medication, and offering valuable health guidance. During my hospital stay, I developed a significant reliance on the nurses, appreciating the convenience of being able to consult them at any time. However, upon discharge, the reality of no longer having regular access to this level of care for frequent consultations became apparent. (N10)
Sub-Theme 8: Facing Challenges to the Cost of Rehabilitation Treatment and the Extent of Insurance Coverage
Participants reported that the duration of rehabilitation treatment and financial constraints negatively impacted their motivation to engage in rehabilitation. Notably, patients without Shanghai medical insurance and those residing in remote areas demonstrated poorer adherence to rehabilitation practices.
“As non-local individuals, our journey to Shanghai for medical care has resulted in substantial financial burdens, with the matter of reimbursement remaining unsettled. The duration of rehabilitation treatment is extensive and accompanied by considerable costs. We lack Shanghai medical insurance, which not only complicates the reimbursement process but also renders us unable to bear the remaining out-of-pocket expenses”. (N7)
I was aware that attending a hospital rehabilitation center or a dedicated rehabilitation hospital would be beneficial for my physical recovery. However, the distance presented significant challenges. Additionally, I am concerned about the costs of undergoing rehabilitation away from home (N15)
Discussion
By conducting interviews with stroke patients suffering from hand dysfunction post-discharge, this study aimed to gain a deeper understanding of the Chinese patients’ experiences and insights regarding their early rehabilitation treatment. The study showed that patients who were female, older, had a history of stroke, lacked hospital social counseling services, lived in remote areas and had lower incomes were less likely to receive rehabilitation.18,19 Our findings are consistent with previous studies in which participants reported cost and transportation as significant factors in reducing the need for rehabilitation.
Our study indicated that patients who recognize the importance of early treatments and regain health through early rehabilitation treatments were more likely to adhere these treatments. Those who received health education during the early rehabilitation tended to have more confidence in the entire process. Coupled with the support from the family and financial assistance, this enabled the patient to smoothly transition from bad habits to beneficial ones. Furthermore, it encourages patients to adopt effective self-management strategies, which are crucial for in improving stroke patients’ survival rates and promoting their recovery.30 Kamal et al developed a rehabilitation treatment strategy for stroke patients that combined exercise and medication, delivered via video courses.31 This approach enhanced patients’ self-efficacy, improved treatment compliance and reduced the incidence of disability and mortality.
This study identified factors that influenced patients’ active participation in rehabilitation activities, key among them being active support from their families. Family members proactively share household chores, manage the patient’s diet, and engage in physical activities with the patient, fostering an environment that encourages active adherence to post-stroke rehabilitation treatments. Social isolation, characterized by a sense of disconnection from others, is frequently observed among stroke patients. They tend to avoid contacting friends and engaging in social activities in order to avoid comments from friends about their condition following their stroke.31 Mendes et al’s research emphasised the importance of support from others, such as close friends or neighbors, improving the living conditions of stroke patients.32 The study found that patients tend to protect their self-esteem by reducing their social activites. Encouraging patients to communicate with friends and neighbours and providing them with positive family support will significantly help to alleviate their social isolation. Consequently, this study recommends that HCPs should mobilize the patient’s social network, encompassing family support, friend assistance et.al aid. This approach will enhance patients’ confidence and facilitate their transition back to a normal life.
Through in-depth patient interviews, we learned that patients with low levels health self-efficacy exhibited limited engagement in rehabilitation therapies. Perceived self-efficacy refers to an individual’s ability to assess their own conditions and engage in health-promoting behaviors by utilizing available medical resources.33 In our interviews, patients often eat a high-salt diet to satisfy their taste preferences and to compensate for salt loss due to physical activity. This behavior indicates lower levels of self-efficacy, characterized by a lack of control over personal behavior and a deficiency in health knowledge pertaining to stroke. Our results align with the findings of Buster et al34 indicating that kidney transplant patients exhibit a deficient perception of health self-efficacy, and a low level of self-efficacy is strongly associated with reduced treatment adherence. Participants in this study predominantly possessed a low level of education. Research demonstrated that good education can enhance people’s comprehension of the disease, facilitating the adoption of preventive measures and the utilization of treatment resources and information.35 Simultaneously, stroke patients interviewed expressed that they find walking challenging and harbor concerns about potential injury if they engage in physical exercise. Our findings align with those reported by Arvidsson et al36 indicating that stroke patients exhibit reduced activity levels due to impaired balance and a fear of falling. Evidence shows that physical active rehabilitation, both in the early or mid-term stages of stroke, can help patients recover and adjust to daily life as soon as possible, which includes the use of necessary supportive devices, such as walking aids.9,37 Therefore, this study suggests that HCPs elucidate the necessity of exercise rehabilitation to patients and their families, and also assess patients’ levels of healthy self-efficacy. Targeted interventions are designed according to the patient’s level of disease knowledge and self-control. Utilize external support to motivate patients to comply with treatment guidelines, including encouragement from HCPs and their families.
When discussing the participants’ rehabilitation journeys, it was found that those who actively sought rehabilitation treatment information about rehabilitation treatments exhibited a higher level of engagement in their rehabilitation therapies. For example, patients who sought such information on platforms like TikTok and Baidu were more likely to actively engage in their therapy, often motivated by the success stories of rehabilitation that they had encountered. Some participants also reported a sense of security stemming from receiving treatment information and experiencing positive interactions with doctors. Our findings are consistent with those of Yang et al38 who found that patients actively seek relevant information and gain a sense of security through various channels after lung cancer surgery, including the Internet and consultations with professional doctors. Providing appropriate information has been shown to motivate patients to engage in therapy, encourage participatory behaviour and alleviate anxiety.39 Similarly, family caregivers also need access to accurate rehabilitation information.40 HCPs should attend to the informational needs of both patients and family caregivers, disseminating treatment information through various channels, including hospital public accounts, hotline consultation services, timely follow-ups, and community linkage services.
In the interviews, participants expressed that limited communication with doctors and the absence of continuous care negatively impacted their motivation to participate in rehabilitation therapy. In the actual clinical settings, doctors often have demanding schedules and are frequently involved in surgeries after morning rounds. Consequently, the issue of restricted communication between patients and doctors becomes notably prominent. Vital communication and access to accurate information between patients and their physicians have been demonstrated to diminish anxiety, foster a sense of security, and enhance adherence.38,39 As is widely recognised, rehabilitation forms part of long-term care, and successful collaboration between patients and HCPs is crucial.41 The participants expressed concerns regarding the accessibility of ongoing services post-discharge and the challenges in obtaining timely medical services due to physical disabilities, travel difficulties, and other impediments. These findings align with previous research,42 indicating that access and continuity of care are pivotal factors influencing patients’ continued engagement in rehabilitation treatment. The rehabilitation treatment team, which consists of doctors, nurses, community health care workers, psychologists, and other professionals, inherently depends on effective multi-member collaboration. Consequently, cultivating a three-dimensional partnership between hospitals, communities, and families is crucial for guaranteeing patients’ access to continuous and comprehensive care.
During the interviews, the patients conveyed that the extended duration of rehabilitation treatment entails considerable costs. In particular, participants in this study who lacked Shanghai insurance reported being unable to bear the costs. The treatment of stroke can be expensive, with costs including nursing expenses during hospitalisation and long-term rehabilitation after discharge.43 Research conducted by Xu et al44 supported the findings of this study, which found that stroke patients were bored with the financial pressure of the rehabilitation therapy. Rural residents, confronted with higher hospital copayments for coverage, are more than twice as likely as urban residents to discontinue treatment.45 Since our research subjects were from stroke patients in Shanghai, China, it is important to note that the medical insurance policy in Shanghai is unique (medical insurance from other regions are not applicable in Shanghai). Consequently, despite the relative abundance of medical resources in Shanghai, these resources are not distributed equitably.35 Therefore, the Chinese government must strengthen the integration of medical insurance policies, expand coverage and maximise public participation. This will ensure that patients obtain the benefits of medical insurance in cities with abundant resources.
Study Limitations
This study has three potential limitations. Firstly, the participants in this study had hand dysfunction but did not experience communication difficulties. As a result, the findings may not be generalizable to the rehabilitation experiences of patients with severe stroke. Secondly, the geographical location of the interviews and the unique aspects of Shanghai’s medical insurance system, along with its abundant medical resources, may limit the generalizability of the findings to other regions or populations. Future research should involve multiple regions and a more diverse array of participants to gain a comprehensive understanding of the factors influencing the participation of stroke patients with hand dysfunction in rehabilitation across different settings. Thirdly, this study focused on the experiences of stroke patients undergoing rehabilitation within the initial six months following disease onset. Given that full recovery can be an extended process, future research should investigate the challenges encountered by stroke patients beyond the six-month mark.
Conclusions
This descriptive study aimed to enrich the existing literature on rehabilitation care for stroke-induced hand dysfunction by providing in-depth insights into the experiences of stroke patients undergoing rehabilitation therapy. The insights gained from this study will refine the management strategies of HCPs and encourage greater patient engagement in rehabilitation, addressing the issue of low compliance with rehabilitation treatment for stroke-induced hand dysfunction prevalent in China. Investigating the factors that affect early rehabilitation behavior in stroke patients is essential for creating targeted rehabilitation interventions and services tailored to stroke survivors.
Data Sharing Statement
The data that support the findings of this study are available on request from the corresponding author.
The data are not publicly available due to privacy or ethical restrictions.
Ethics Approval and Consent to Participate
This study was approved by the institutional review board at the East Hospital Affiliated to Tongji University (Approval number: [2022] Review No. (186)). The procedures used in this study adhere to the tenets of the Declaration of Helsinki. Informed consent was obtained from all individual participants included in the study.
Acknowledgments
The authors would like to thank the staff at the East Hospital Affiliated to Tongji University, who facilitated this study, and all the participants who participated in the study.
Author Contributions
XQ and CZ designed the study. Material preparation and data collection were performed by XQ and QZ. Data analysis was performed by XQ, QZ, YH, LL and CZ, CZ and QZ interpreted the results and drafted the paper. XQ and YH received salary support from scientific clinical research project of the East Hospital Affiliated to Tongji University. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the articlehas been submitted; and agree to be accountable for all aspects of the work.
Consent for Publication
All patients provided written informed consent.
Funding
Shanghai East Hospital Angel Program and Young Nurses Growth Program (DFTS-2255);Sailing talents program of Shanghai East Hospital (Grant No. DFYY-YH19); and General Project of Shanghai Pudong New Area Health Commission (Grant No. PW2019A-44).
Disclosure
The authors declare no competing interests.
References
1. Saini V, Guada L, Yavagal DR. Global epidemiology of stroke and access to acute ischemic stroke interventions. Neurology. 2021;97(20 Suppl 2):S6–S16. doi:10.1212/WNL.0000000000012781
2. Zhao D, Liu J, Wang M, Zhang X, Zhou M. Epidemiology of cardiovascular disease in China: current features and implications. Nat Rev Cardiol. 2019;16(4):203–212. doi:10.1038/s41569-018-0119-4
3. Tu W, Zhao Z, Yin P, et al. Estimated Burden of Stroke in China in 2020. JAMA Netw Open. 2023;6(3):e231455. doi:10.1001/jamanetworkopen.2023.1455
4. Niama ND, Lejeune T, Detrembleur C, et al. Effectiveness of a self-rehabilitation program to improve upper-extremity function after stroke in developing countries: a randomized controlled trial. Ann Phys Rehabil Med. 2021;64(1):101413. doi:10.1016/j.rehab.2020.03.017
5. Bernhardt J, Godecke E, Johnson L, et al. Early rehabilitation after stroke. Curr Opin Neurol. 2017;30(1):48–54. doi:10.1016/j.rehab.2020.03.017
6. Huang J, Zuo J, Tang X, et al. Early Rehabilitation and Nursing Intervention (ERNI) accelerates the recovery of patients with ischemic stroke. Neurologist. 2023;28(6):409–412. doi:10.1097/NRL.0000000000000515
7. Li Z, Zhang X, Wang K, Wen J. Effects of early mobilization after acute stroke: a meta-analysis of randomized control trials. J Stroke Cerebrovasc Dis. 2018;27(5):1326–1337. doi:10.1016/j.jstrokecerebrovasdis.2017.12.021
8. Langhorne P, Coupar F, Pollock A. Motor recovery after stroke: a systematic review. Lancet Neurol. 2009;8(8):741–754. doi:10.1016/S1474-4422(09)70150-4
9. Lee KE, Choi M, Jeoung B. Effectiveness of rehabilitation exercise in improving physical function of stroke patients: a systematic review. Int J Environ Res Public Health. 2022;19(19). doi:10.3390/ijerph191912739
10. Kwakkel G, Stinear C, Essers B, et al. Motor rehabilitation after stroke: European Stroke Organisation (ESO) consensus-based definition and guiding framework. Eur Stroke J. 2023;8(4):880–894. doi:10.1177/23969873231191304
11. Wei X, Sun S, Zhang M, et al. A systematic review and meta-analysis of clinical efficacy of early and late rehabilitation interventions for ischemic stroke. BMC Neurol. 2024;24(1):91. doi:10.1177/23969873231191304
12. Cheiloudaki E, Alexopoulos EC. Adherence to Treatment in Stroke Patients. Int J Environ Res Public Health. 2019;16(2):196. doi:10.3390/ijerph16020196
13. Mahmood A, Solomon JM, English C, et al. Measurement of adherence to home-based exercises among community-dwelling stroke survivors in India. Physiother Res Int. 2020;25(2):e1827. doi:10.1002/pri.1827
14. Gunnes M, Indredavik B, Langhammer B, et al. Associations between adherence to the physical activity and exercise program applied in the LAST study and functional recovery after stroke. Arch Phys Med Rehabil. 2019;100(12):2251–2259. doi:10.1016/j.apmr.2019.04.023
15. Dong X, Jing R, Duan Y. Research status of rehabilitation training compliance and its influencing factors in stroke patients. J Yanan Univ. 2023;21(01):85–88. doi:10.19893/j.cnki.ydyxb.2022-0231
16. Zheng Z, Song R, Zhao Y, et al. An investigation of the level of stigma and the factors influencing it in the rehabilitation of young and middle-aged stroke patients-a cross-sectional study. BMC Neurol. 2023;23(1):139. doi:10.1186/s12883-023-03189-4
17. Yan Q, Wang X, Zhang Y, Zhang H, Zhao L. Analysis of influencing factors of rehabilitation treatment effect in patients with first-episode stroke. Am J Transl Res. 2021;13(12):14046–14056.
18. Unrath M, Kalic M, Berger K. Who receives rehabilitation after stroke?: data from the quality assurance project “Stroke Register Northwest Germany”. Dtsch Arztebl Int. 2013;110(7):101–107. doi:10.3238/arztebl.2013.0101
19. Labberton AS, Barra M, Rønning OM, et al. Patient and service factors associated with referral and admission to inpatient rehabilitation after the acute phase of stroke in Australia and Norway. BMC Health Serv Res. 2019;19(1):871. doi:10.1186/s12913-019-4713-x
20. Simpson DB, Jose K, English C, et al. “Factors influencing sedentary time and physical activity early after stroke: a qualitative study”. Disabil Rehabil. 2022;44(14):3501–3509. doi:10.1080/09638288.2020.1867656
21. Noble H, Smith J. Qualitative data analysis: a practical example. Evid Based Nurs. 2014;17(1):2–3. doi:10.1136/eb-2013-101603
22. Sundler AJ, Lindberg E, Nilsson C, Palmér L. Qualitative thematic analysis based on descriptive phenomenology. Nurs Open. 2019;6(3):733–739. doi:10.1002/nop2.275
23. Sorsa MA, Kiikkala I, Åstedt-Kurki P. Bracketing as a skill in conducting unstructured qualitative interviews. Nurse Res. 2015;22(4):8–12. doi:10.7748/nr.22.4.8.e1317
24. Liu L, Chen W, Zhou H, et al. Chinese Stroke Association guidelines for clinical management of cerebrovascular disorders: executive summary and 2019 update of clinical management of ischaemic cerebrovascular diseases. Stroke Vasc Neurol. 2020;5(2):159–176. doi:10.1136/svn-2020-000378
25. Dong Y, Guo Z-N, Li Q, et al. Chinese Stroke Association guidelines for clinical management of cerebrovascular disorders: executive summary and 2019 update of clinical management of spontaneous subarachnoid haemorrhage. Stroke Vasc Neurol. 2019;4(4):176–181. doi:10.1136/svn-2019-000296
26. Redish J. Doing research in the real world. Tech Communication. 2005;52(3):376–377.
27. Patton MQ. Enhancing the quality and credibility of qualitative analysis. Health Services Res. 1999;34(5):1189–1208.
28. Braun V, Clarke V. Toward good practice in thematic analysis: avoiding common problems and be(com)ing a knowing researcher. Int J Transgend Health. 2023;24(1):1–6. doi:10.1080/26895269.2022.2129597
29. Guba EG, Lincoln YS. Epistemological and methodological bases of naturalistic inquiry. Ectj-Educ Comm Technol J. 1982;30(4):233–252. doi:10.1007/BF02765185
30. Sun Y, Liu C, Zhang N, et al. Effect of self-management of stroke patients on rehabilitation based on patient-reported outcome. Front Neurosci. 2022;16:929646. doi:10.3389/fnins.2022.929646
31. Kamal AK, Khoja A, Usmani B, et al. Translating knowledge for action against stroke--using 5-minute videos for stroke survivors and caregivers to improve post-stroke outcomes: study protocol for a randomized controlled trial (Movies4Stroke). Trials. 2016;17:52. doi:10.1186/s13063-016-1175-x
32. Mendes PC, Greenwood N, Jones F. “A proof of life” through transition from hospital to home after a stroke in a Portuguese setting - a multi-perspective, longitudinal qualitative study. Int J Qual Stud Health Well-Being. 2023;18(1):2238986. doi:10.1080/17482631.2023.2238986
33. Prochaska JO, Velicer WF. The transtheoretical model of health behavior change. Am J Health Promot. 1997;12(1):38–48. doi:10.4278/0890-1171-12.1.38
34. Buster S, Ozsaker E. Locus of control, self-efficacy perception and treatment adherence in kidney transplant patients. Transpl Immunol. 2022;75:101723. doi:10.1016/j.trim.2022.101723
35. Yang S, Wang D, Li C, Wang C, Wang M. Medical treatment behaviour of the elderly population in shanghai: group features and influencing factor analysis. Int J Environ Res Public Health. 2021;18(8). doi:10.3390/ijerph18084108
36. Arvidsson LM, Forsberg A, Appelros P, Anderzén-Carlsson A. “I can manage the challenge” - a qualitative study describing experiences of living with balance limitations after first-ever stroke. Int J Qual Stud Health Well-Being. 2021;16(1):1857044. doi:10.1080/17482631.2020.1857044
37. Billinger SA, Coughenour E, Mackay-Lyons MJ, Ivey FM. Reduced cardiorespiratory fitness after stroke: biological consequences and exercise-induced adaptations. Stroke Res Treat. 2012;959120. doi:10.1155/2012/959120
38. Yang Y, Chen X, Pan X, et al. The unmet needs of patients in the early rehabilitation stage after lung cancer surgery: a qualitative study based on Maslow’s hierarchy of needs theory. Support Care Cancer. 2023;31(12):677. doi:10.1007/s00520-023-08129-z
39. Oh J, Kim JA. Information-seeking behavior and information needs in patients with amyotrophic lateral sclerosis: analyzing an online patient community. Comput Inform Nurs. 2017;35(7):345–351. doi:10.1097/CIN.0000000000000333
40. Merati-Fashi F, Dalvandi A, Parsa YZ. Stroke survivors and their family caregivers’ experiences of health information seeking: a qualitative study. Int J Community Based Nurs Midwifery. 2022;10(4):269–278. doi:10.30476/IJCBNM.2022.94489.1997
41. Aadal L, Angel S, Dreyer P, Langhorn L, Pedersen BB. Nursing roles and functions in the inpatient neurorehabilitation of stroke patients: a literature review. J Neurosci Nurs. 2013;45(3):158–170. doi:10.1097/JNN.0b013e31828a3fda
42. Meadmore KL, Hallewell E, Freeman C, Hughes A. Factors affecting rehabilitation and use of upper limb after stroke: views from healthcare professionals and stroke survivors. Top Stroke Rehabil. 2019;26(2):94–100. doi:10.1080/10749357.2018.1544845
43. Rochmah TN, Rahmawati IT, Dahlui M, Budiarto W, Bilqis N. Economic burden of stroke disease: a systematic review. Int J Environ Res Public Health. 2021;18(14):7552. doi:10.3390/ijerph18147552
44. Xu L, Dong Q, Jin A, et al. Experience of financial toxicity and coping strategies in young and middle-aged patients with stroke: a qualitative study. BMC Health Serv Res. 2024;24(1):94. doi:10.1186/s12913-023-10457-z
45. Jian W, Chan KY, Reidpath DD, Xu L. China’s rural-urban care gap shrank for chronic disease patients, but inequities persist. Health Aff. 2010;29(12):2189–2196. doi:10.1377/hlthaff.2009.0989
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Barriers and Facilitators to Successful Intensive Adherence Counseling in Rural Northern Uganda: An Exploratory Interview with HIV-Positive Clients Using the COM-B Framework
Beja H, Daisy N, Edek MT, Kobusinge V, Akaki O, Owachgiu IO, Udho S
HIV/AIDS - Research and Palliative Care 2022, 14:553-563
Published Date: 21 November 2022
Barriers and Facilitators to Utilization of Community Drug Distribution Points Among People Living with HIV in Bushenyi District, South-Western Uganda: A Qualitative Study
Oyet D, Niyonzima V, Akol G, Onyait E, Twinomugisha D, Kawala Wambera D, Wakida EK, Obua C
HIV/AIDS - Research and Palliative Care 2023, 15:633-640
Published Date: 16 October 2023
Planning for Hospital Discharge for Older Adults in Uganda: A Qualitative Study Among Healthcare Providers Using the COM-B Framework
Owokuhaisa J, Schwartz JI, Wiens MO, Musinguzi P, Rukundo GZ
Journal of Multidisciplinary Healthcare 2023, 16:3235-3248
Published Date: 2 November 2023
Exploring Factors Affecting Acceptance of Fecal Microbiota Transplantation for Patients with Recurrent Urinary Tract Infections: a Descriptive Qualitative Study
Liu H, Wei Y, Xu Z, Lin H, Zhao Y, Wang S, Gao F, Feng N, Wolfe AJ, Liu F
Patient Preference and Adherence 2024, 18:1257-1269
Published Date: 17 June 2024
Identification of Facilitators and Barriers to Functional Ability in Elderly Stroke Patients: A Descriptive Qualitative Study
Zhang W, Ma R, Tao X, Wang A
Journal of Multidisciplinary Healthcare 2025, 18:1007-1019
Published Date: 21 February 2025