Back to Journals » Integrated Pharmacy Research and Practice » Volume 9
Exploratory Findings of Prescribing Unlicensed and Off-Label Medicines Among Children and Neonates
Authors Shakeel S, Iffat W ![]() , Nesar S, Zaidi H, Jamshed S
, Nesar S, Zaidi H, Jamshed S ![]()
Received 15 September 2019
Accepted for publication 28 November 2019
Published 5 February 2020 Volume 2020:9 Pages 33—39
DOI https://doi.org/10.2147/IPRP.S231134
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Jonathan Ling
Sadia Shakeel,1,2 Wajiha Iffat,2 Shagufta Nesar,3 Hina Zaidi,3 Shazia Jamshed4,5
1Discipline of Social and Administrative Pharmacy, School of Pharmaceutical Sciences, University Sains Malaysia, Penang, Malaysia; 2Faculty of Pharmaceutical Sciences, Dow University of Health Sciences, Karachi, Pakistan; 3Faculty of Pharmacy, Hamdard University, Karachi, Pakistan; 4Department of Pharmacy Practice, Kulliyyah of Pharmacy, International Islamic University Malaysia, Kuantan, Pahang, Malaysia; 5Qualitative Research-Methodological Applications in Health Sciences Research Group, Kulliyyah of Pharmacy, International Islamic University Malaysia, Kuantan, Pahang, Malaysia
Correspondence: Shazia Jamshed
Pharmacy Practice, Kulliyyah of Pharmacy, Indera Mahkota Campus, Kuantan 25200, Pahang, Malaysia
Email [email protected]
Objective: A cross-sectional study was carried out to evaluate the practice of unlicensed and off-label drug prescribing/dispensing in children and neonates by physicians and clinical pharmacists in the metropolitan city of Karachi.
Methods: The study was conducted for the duration of 5 months – November 2018 to March 2019 – in different clinics and tertiary care hospitals of Karachi, Pakistan. Respondents were interviewed by our researchers using 30 items questionnaire. Descriptive statistics were used to evaluate the answers of respondents to survey items. Pearson correlation and independent sample t-test were employed to recognize the association between the responses of participants and independent variables. P values less than 0.05 were considered statistically significant.
Results: A total of 421 questionnaires were completed by physicians and clinical pharmacists. The mean age of the study participants was 49.5 years. Around 98% of pharmacists and 93.5% of physicians were well conversant with the definition of unlicensed and off-label drugs. Around 68% of physicians and 77% of pharmacists reported that they were more concerned about the efficacy of such drugs as compared to that of licensed medicines in children. The most frequent off-label categories observed in the study were dose (65.21%) and indication (17.52%). A vast majority (> 80%) thought that approving new drugs by regulatory authorities will drop the occurrence of medication errors due to incorrect dosing. The British National Formulary (BNF) for children was used as the best reliable source of information among respondents.
Conclusion: The present study highlighted the common practice of unlicensed and off-label drug prescribing in pediatrics; however, respondents showed their concern towards decreasing such practice and are likely to welcome initiatives intended to assure medication safety in children.
Keywords: unlicensed drug and off-label prescribing, physicians, clinical pharmacists, Pakistan
Introduction
Pediatric prescribing is always challenging for health care professionals due to diverse responses in pharmacokinetics, insufficient evidence-based prescribing and inadequate research studies conducted among this vulnerable population, leading to compromised effectiveness and/or safety of drug.1 Food and Drug Dosage and European Union for pediatric pharmacotherapy have taken several steps to overcome these challenges in preceding two decades; however, neonates yet exposed to unlicensed and off-label drug (UOLD) prescriptions. Pakistan follows both the Food and Drug Dosage guidelines and European Union Regulation on Medicinal Products for Pediatric Use (Regulation n° 1901/2006) implemented in 2007.2
Unlicensed drug prescribing is the practice of prescribing a drug in the absence of product license, whereas off-label drug prescribing means prescribing the drug for specifications (in terms of age group, dosage, route of drug administration or particular indication) other than those that are mentioned on the label of the product license.3 The scarcity of controlled clinical trials in neonates, limited financial support of local governments, and lack of interest of industries (owing to less generation of revenue and efforts required for formulating drugs for the pediatric population) are the key whys and wherefores for the common prescribing practice of UOLD in children and neonates.4 Inappropriate UOLD usage may be the reason for serious adverse drug reactions (ADRs) as observed in previous research.5 The probability of ADRs has amplified twofold in neonates since their body is physiologically immature.6,7 Therefore, it is imperative to study this issue in the context of Pakistan and the current research is an attempt to explore the knowledge and prescribing/dispensing practices of physicians and clinical pharmacists regarding UOLD in Karachi, Pakistan.
Materials and Methods
Study Design and Setting
The study was conducted for 5 months – from November 2018 to March 2019. Physicians and clinical pharmacists working in different clinics and tertiary care hospitals in Karachi were recruited.
Sampling Technique
The sample size was calculated by using Raosoft sample size calculator using the following formula:



N = population size; r = fraction of responses; n = sample size; E = confidence interval; c = confidence level; Z(c/100) = critical value for the confidence level.
Since the exact number of physicians and pharmacists practicing in Karachi is not known, the population size was considered N = 2000. Using a confidence level of 95% the minimum sample size was estimated to be n = 323 with 5% margin error. A snowball sampling approach was adopted.
Study Tool
A 30 items questionnaire was adapted from previous studies8,9 to evaluate the prescribing/dispensing practice of respondents and their perception about UOLD. Along with the demographic information the questionnaire consisted of 4 sections.
- The first section contains 10 questions inquiring about their knowledge of UOLD, their concerns about its safety and efficacy, and the likelihood of ADRs when using UOLD.
- The second part consists of 10 questions evaluating their current practice of prescribing/dispensing UOLD, reasons for prescribing/dispensing UOLD, their choice of information sources, and explores their suggestions for reducing such prescribing.
- The third part consist of 5 questions concerning their practice of requesting informed, written/verbal consent from parents or guardians before prescribing/dispensing/administering UOLD to a child.
- The fourth part consist of 5 questions inquiring whether the respondents are willing to participate in conducting clinical trials on children.
The questionnaire was subjected to face validity and content validity and sent to 5 experts. A pilot study was conducted with 20 physicians and clinical pharmacists to ascertain the reliability coefficient. Cronbach alpha was computed to be 0.72.
Data Collection and Analysis
In terms of tool processing, interviewer-administered questionnaires were used to assemble information from respondents. The responses collected were entered into the Statistical Package for Social Sciences (SPSS 20.0, Chicago, IL) for descriptive and inferential analysis. Pearson correlation and independent sample t-test were employed to recognize the association between the responses of participants and independent variables. P values less than 0.05 were considered statistically significant.
Statement of Consent
Verbal consent was obtained from the participants prior to recording their answers. The research reflects insignificant risk/harm to subjects and involves no intercedes for which written approval is usually necessary.
Ethical Approval
Earlier consent was taken from the different heads of departments in the hospitals and clinics before initiating the investigation. It was assured that the identification of the respondents and their working hospitals and clinics will not be revealed and will be kept anonymous. The questionnaires were circulated to the respondents subsequent to clarifying them the motivation behind the study.
Results
In the current research, 250 physicians (pediatricians [168], and general physicians, [82], and 200 clinical pharmacists belonging to different clinics and tertiary care hospitals of Karachi were interviewed; 21 physicians and 8 pharmacists did not agree to participate after initial contact and were excluded. Finally, a total of 421 completed questionnaires were included in the research. Among them, 229 and 192 were physicians and clinical pharmacists, respectively. The overall response rate was 93.5%. A total of 58.2% male and 41.8% female clinical pharmacists and 63.4% male and 36.6% females participated. More than half (61.9%) were rendering their services in public sector hospitals. The mean age of the study participants was 49.5 years with 51.5% having an experience of 10–15 years. For detailed demographics please refer to Table 1.
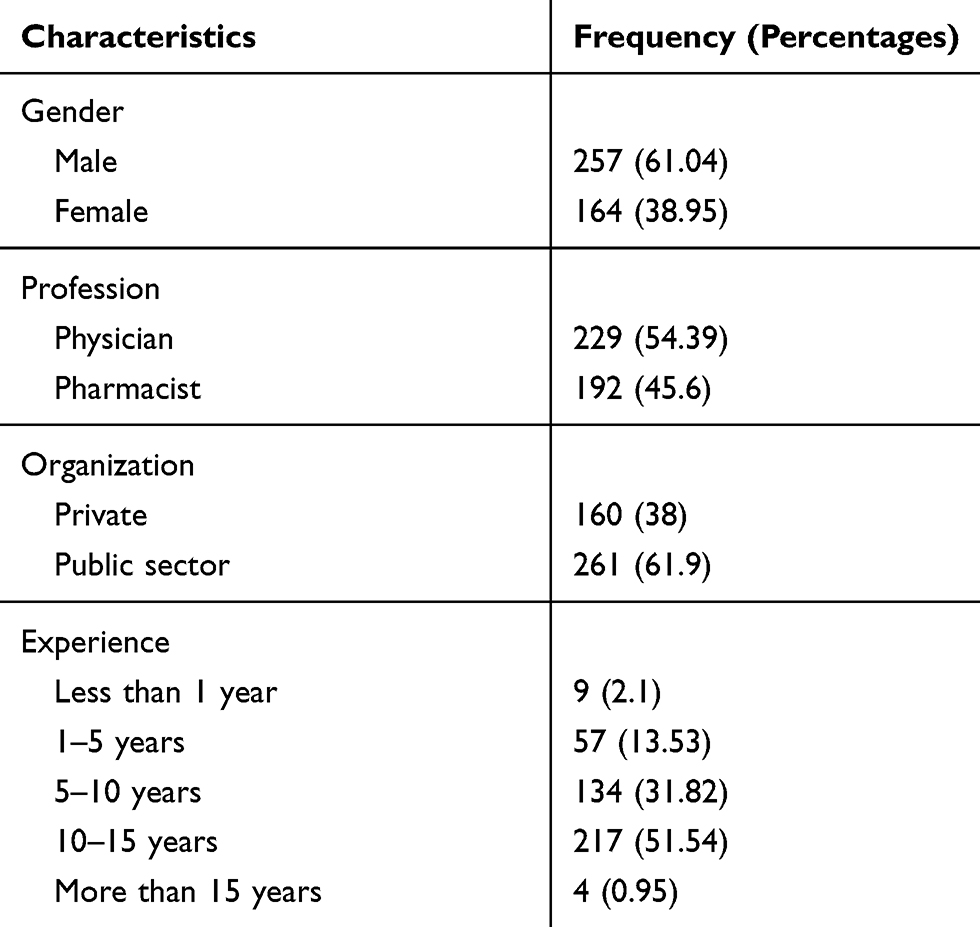 |
Table 1 Characteristics of Study Population |
Around 98% of pharmacists and 93.5% of physicians were well conversant with the definition of UOLD and around half of them had heard about the use of UOLD during their graduate studies. However, the knowledge of UOLD was found to be statistically significant with their profession and pharmacists were more well-informed as compared to the physicians (p = 0.001). On inquiring about the safety of UOLD, 35.7% of physicians and 44.6% of pharmacists considered UOLD as safe if prescribed with appropriate scientific support (Figure 1). Figure 2 illustrats the respondents’ opinions towards the common age group of children and neonates for prescribing UOLD. Around 56.2% of pharmacists and 49.5% of physicians deemed that children from 2 to 11 years, whereas 31.5% of pharmacists and 24.39% of physicians considered infants from 1 to 23 months, are most likely to receive UOLD. The male respondents were more likely to prescribe or dispense the UOLD in the age range of 2–11 years (p=0.001).
 |
Figure 1 Respondents’ belief towards the safety of unlicensed and off-label drug use in children. |
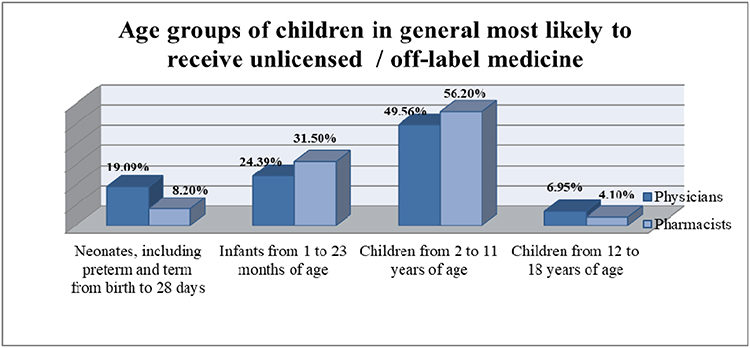 |
Figure 2 Respondents’ opinion towards the most common age group of children and neonates for prescribing unlicensed and off-label drugs. |
Around 68% of physicians and 77% of pharmacists revealed that they are lot more concerned about the efficacy of UOLD than for licensed medicines in children. Though their concerns about the efficacy was significantly related to their profession and pharmacists were found to be more concerned (p=0.023). In current research, more than 52% of physicians and around 67% of pharmacists felt that incorrect use of UOLD increased the probability of ADRs when compared to licensed medicines. Figure 3 illustrates the respondents’ suggestions for reducing the use of UOLD in children. Both physicians (49%) and pharmacists (56%) considered that there is a need to make new drug formulations for children.
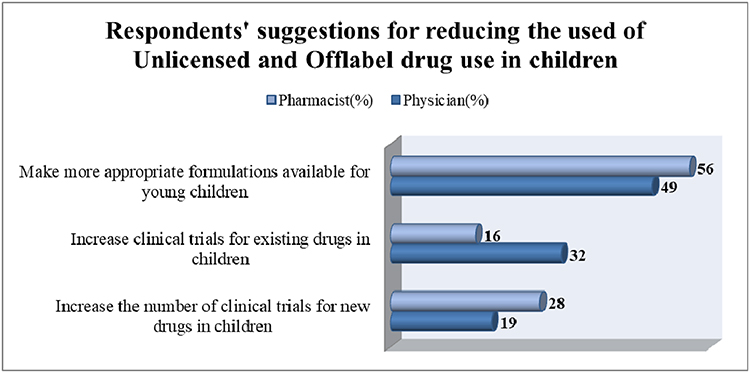 |
Figure 3 Respondents’ suggestions for reducing the use of unlicensed and off-label drugs in children. |
It was alarming that only 23% of physicians and 47% of pharmacists informed parents or guardians when an UOLD had been dispensed/prescribed for a child. Their practice of notifying was significantly associated with gender and female respondents were more likely to inform parents or guardians when UOLD has been prescribed for a child (p = 0.0001). Physicians (18%) and pharmacists (27%) reported to request informed consent from parents earlier than prescribing or dispensing UOLD. It was interesting to observe that 45% of physicians place the onus on pharmacists and 70% of pharmacists claimed physicians to be accountable for notifying parents about treatment with UOLD. Around 40% of physicians and 63% of pharmacists thought that it would unreasonably alarm parents if they will be notified that their child is receiving UOLD. This perception of respondents was significantly related with their organization and respondents rendering their services in private sector hospitals or clinics were more likely to consider the response of parents when using UOLD (p = 0.003).
About 34% of physicians and 51% of pharmacists reported that commonly used medicines following UOLD criteria must go through clinical trials in children having the indication(s) in questioning for their approval in children. Physicians (41%) and pharmacists (77%) stated that manufacturers should be enforced to investigate all new drugs (with a perspective for pediatric usage) in children having the indication(s) in interrogation, as an integral component of the drug development process. More than 50% of physicians and more than 62% of pharmacists were willing to be actively involved in conducting clinical trials in children. Yet, their inclination towards participation was significantly associated with their profession and pharmacists were more likely to involved in clinical trials (p = 0.0001). In the present research, around 90% of physicians and 98% of pharmacists claimed to check doses of medicines twice if a calculation was necessary for determining the dose to be given. Around 80% of physicians and 89% of pharmacists thought that approving new drugs by regulatory authorities for pediatric usage will reduce the occurrence of medication errors due to incorrect dosing. Pharmacists were observed to be more enthusiastic about licensing more medicines for use in children (p = 0.0001). The most frequent off-label categories observed in the current study were dose (65.21%) and indication (17.52%). Other detected off-label categories were; age-group (13.48%), indication-dose (7.93%), age group-dose (3. 72%), indication-dosage form (1.94%), age group-dosage form (1.03%), dosage form (0.72%), dosage form-dose (0.63%), age group-indication (0.26%), age group-indication-dose (0.21%), and age group-dosage form-dose (0.21%). Figure 4 illustrated the respondents’ reliable sources of information for prescribing. Both physicians (34%) and pharmacists (47%) used the British National Formulary (BNF) for children as the most trustworthy source of information.
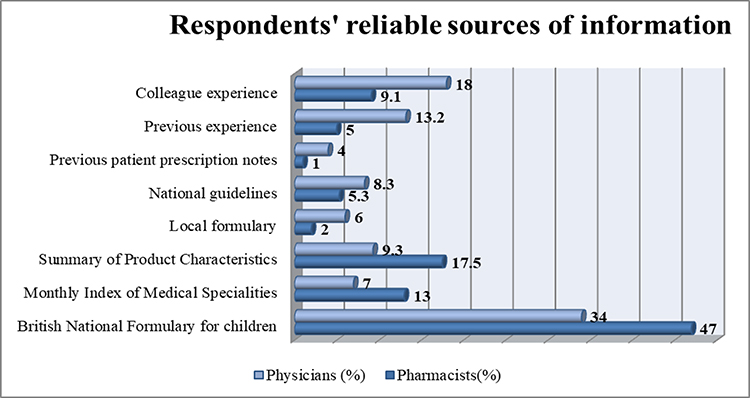 |
Figure 4 Respondents’ reliable sources of information for prescribing in children. |
Discussion
The findings of this research reported worthy knowledge of UOLD among both pharmacists and physicians, as they were found to be well conversant with the definition of UOLD from their graduate studies. Other studies specified similar reasons for awareness of UOLD among health care professionals, indicating post‐graduate and undergraduate teaching and practice as the key reasons.8–10 Another study reported that respondents showed their understanding by using the phrases; off-label (58.6%) and unlicensed (82.9%) prescribing, and the most commonly mentioned reason for such prescribing was the scarcity of evidence-based literature available for this vulnerable group of population.10 Studies revealed that the lack of synchronization among the available evidence-based research, the data presented to doctors, and its usage in clinical practice, makes the off-label therapies common among children.11 The current research highlighted that UOLD are safe if prescribed rationally.
In the current study, around half of the respondents believed that children from 2 to 11 years are most likely to receive UOLD. The male respondents were more likely to prescribe or dispense the UOLD in the age duration of 2–11 years. Off-label utilization of medications displays a wider and increasingly complex issue in preterm and full-term neonates, babies and in children smaller than 2 years of age. Another study revealed that most pharmacists dispensed off‐label medicines intended for infants whose age is between 1 to 23 months.10 Unlicensed drug use is found be high in 0 to 1-year-olds Dutch children, and off-label drug use is at its peak amongst 12- to 16-year-olds Dutch children.12 It was worthy to observe that majority of respondents reported their uneasiness towards the efficacy of UOLD and felt that an inappropriate use of UOLD increases the likelihood of ADRs as compared to licensed medicines. Though their concerns about the efficacy was significantly related with their profession and pharmacist were found to be more concerned, other studies also revealed respondents concerns as regards the safety and efficacy of off-label prescribing for children.10,13 Therapeutic innovations has contributed substantially in improving the neonate survival rate over recent decades; however, short or long term adverse consequences from the irrational consumption cannot be predicted.13
The selection of the correct medicine and accurate doses for treating neonates is a complex task owing to the inadequate prevailing information on pharmacodynamics, pharmacokinetics development, and dose determination in terms of neonates, in association with the inadequacy of clinical trials in children.14,15 In this study, the majority of respondents emphasized a need for developing more appropriate formulations for young children. In another study, the physicians emphasized attaching legible and concise labels on such products which are used as UOLDs and considered it to be a significant approach; nevertheless, other health care professionals characterized further new appropriate drug preparations accessible for pediatrics as the best method to shorten off label prescribing.10 Health care professionals are lawfully bounded to notify patients about the risks involved in using UOLDs. The fact that there is an absence of data available for off-label use ought to be considered a possibility of hazard for the patient. Henceforth, physicians ought to observe lawful measures that expect them “to obtain informed consent from a person before performing a test or stating a treatment – particularly a treatment that involves some uncertainty”.11 It ought to follow then that physicians and pharmacists be required to educate patients regarding off-label use, however this does not appear to be the situation. In the current research only a small percentage of respondents (23% of physicians and 47% of pharmacists) informed parents or guardians and requested informed consent from parents prior to prescribing or dispensing UOLD to a child. The higher ratio of pharmacists might be due to the fact that pharmacists are more involved in patient counseling and education compared to physicians. Furthermore, the pharmacists are uniquely trained to offer appropriate guidance to patients in their choices of suitable pharmacotherapy. Both groups of respondents in the research put the onus of accountability on the other for notifying parents about treatment with UOLDs. Other studies also described similar attitudes of health care professionals, as the majority agreed that at the time a medication was prescribed in an off-label way, the information ought to be disclosed to guardians. Be that as it may, the rate revealed for such practice remains low.16–18
Clinical trials are necessary to decide the efficiency and safety of drugs in children. Whenever new medications are presented for licensing in the USA, the Food and Drug Administration requires the manufacturing company to provide additional data with respect to the utilization of medications in the pediatric populace, and if appropriate, to legitimize explanations for not doing pediatric studies.4 In the current research, respondents reported that all medications used in an unlicensed or off-label manner must undergo clinical trials in children having the indication(s) in question. Thus they would be authoritatively able to prescribe such drugs and drug manufacturers ought to scrutinize all new drugs used on children as a primary factor of the drug development. A majority in the current research expressed their willingness to be part of clinical trials in children. Yet, their inclination towards participation was significantly associated with their profession and pharmacist were more likely to involved in clinical trials (p = 0.0001). Other studies also reported similar findings, that their participants were eager to contribute to clinical trials in children. However, their inclination for their own children to participate in clinical trials was related to a decline in a child’s wellbeing status and benefits associated with the clinical investigation.17,18 The majority claimed to check drug doses twice and believed that approving newer drugs by regulatory authorities for pediatrics will decrease the rate of medication errors relating to incorrect dosing. A study from Jordan reported that the majority claimed to check the calculations of doses of medications twice to dispense off-label medicines and likewise, recognized the need to inform parents whenever an off-label medicine was suggested for their children.16 The most frequent off-label categories observed in the current study were dose and indication. Surprisingly another study conducted in Pakistan reported a similar pattern of the most frequently prescribed off-label categories, i.e., indication and dose.19 Other studies reported that prescriptions being dispensed as off‐label were for younger children, compared to the age that the drug was recommended for use in children, and highlighted age as the common category of off‐label drug use.10,16,18 Both physicians and pharmacists used the BNF for children as the most trustworthy source of information. Another study reported that the BNF was the generally referred to source of information for pediatric prescribing, whereas the Summary of Product Characteristics (SPC) and local formularies were the minimum utilized sources; no respondent acknowledged the use of the available pediatric formulary.9
This study reported an increase in UOLD prescribing by physicians in pediatrics; however, respondents demonstrated their concern towards declining such practice. The findings of our study are supported by another study from Pakistan displaying a similar trend of elevated prescribing of UOLD in clinical settings.19 UOLD use is an international challenging issue which was not investigated earlier in Pakistan. Policies need to be enacted and executed by health regulatory authorities to avoid the complications associated with inappropriate prescribing in pediatrics.
Conclusion
UOLD prescribing/dispensing practice in pediatrics is well examined. Respondents emphasized that there is a need to develop evidence-based formulations for younger children and increase clinical trials in children and neonates to minimize such prescribing trends. Policies should be developed to scrutinize off-label prescribing that compromises patient safety or represents an irresponsible use of medication.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hill P. Off licence and off label prescribing in children: litigation fears for physicians. Arch Dis Child. 2005;90(1):17–18. doi:10.1136/adc.2004.058867
2. Walton SM, Schumock GT, Lee KV, et al. Prioritizing future research on off label prescribing: results of a quantitative evaluation. Pharmacother. 2008;28(12):1443–1452. doi:10.1592/phco.28.12.1443
3. Balan S, Hassali M, Mak V. Awareness, knowledge and views of off‐label prescribing in children: a systematic review. Br J Clin Pharmacol. 2015;80(6):1269–1280. doi:10.1111/bcp.12750
4. LindellOsuagwu L, Korhonen M, Saano S, et al. Off‐label and unlicensed drug prescribing in three paediatric wards in Finland and review of the international literature. J Clin Pharm Ther. 2009;34(3):277–287. doi:10.1111/j.1365-2710.2008.01005.x
5. Mazhar F, Shamim S, Malhi SM. Drug utilization evaluation of antiepileptics in three selected multidisciplinary teaching hospitals of Pakistan. Int J Pharm Pharm Sci. 2014;6(5):59–66.
6. Lindell Osuagwu L, Hakkarainen M, Sepponen K, et al. Prescribing for off label use and unauthorized medicines in three paediatric wards in Finland, the status before and after the European Union Paediatric Regulation. J Clin Pharm Ther. 2014;39(2):144–153. doi:10.1111/jcpt.12119
7. Silva D, Ansotegui I, Morais-Almeida M. Off-label prescribing for allergic diseases in children. W Aller Org J. 2014;7(1):1.
8. Marchetti F, Bua J, Ventura A, et al. The awareness among paediatricians of off-label prescribing in children: a survey of Italian hospitals. Eur J Clin Pharmacol. 2007;63(1):81–85. doi:10.1007/s00228-006-0223-y
9. Ekins Daukes S, Helms PJ, Taylor MW, et al. Off label prescribing to children: attitudes and experience of general practitioners. Br J Clin Pharmacol. 2005;60(2):145–149. doi:10.1111/j.1365-2125.2005.02397.x
10. Mukattash T, Hawwa AF, Trew K, et al. Healthcare professional experiences and attitudes on unlicensed/off-label paediatric prescribing and paediatric clinical trials. Eur J Clin Pharmacol. 2011;67(5):449–461. doi:10.1007/s00228-010-0978-z
11. Pandolfini C, Bonati M. A literature review on off-label drug use in children. Eur J Ped. 2005;164(9):552–558.
12. Schirm E, Tobi H, de Jong-van den Berg LTW. Risk factors for unlicensed and off-label drug use in children outside the hospital. Ped. 2003;111(2):291–295. doi:10.1542/peds.111.2.291
13. De Souza AS, Dos Santos DB, LC R, et al. Off-label use and harmful potential of drugs in a NICU in Brazil: a descriptive study. BMCPediatr. 2016;16(1):13.
14. Allegaert K, Anker JN. Adverse drug reactions in neonates and infants: a population tailored approach is needed. Br J Clin Pharmacol. 2015;80(4):788–795. doi:10.1111/bcp.12430
15. Porta A, Esposito S, Menson E, et al. Off-label antibiotic use in children in three European countries. Eur J Clin Pharmacol. 2010;66(9):919–927. doi:10.1007/s00228-010-0842-1
16. Mukattash TL, Alzoubi KH, Abuirjie AM, et al. Perceptions and attitudes towards off-label dispensing for pediatric patients, a study of hospital based pharmacists in Jordan. Saudi Pharm J. 2018;26(1):20–24. doi:10.1016/j.jsps.2017.11.004
17. Mukattash T, Millership J, Collier P, et al. Public awareness and views on unlicensed use of medicines in children. Br J Clin Pharmacol. 2008;66:838–845. doi:10.1111/j.1365-2125.2008.03290.x
18. McLay JS, Tanaka M, Ekins‐Daukes S, et al. A prospective questionnaire assessment of attitudes and experiences of off label prescribing among hospital based paediatricians. Arch Dis Child. 2006;91:584–587. doi:10.1136/adc.2005.081828
19. Aamir M, Khan JA, Shakeel F, et al. Unlicensed and off-label use of drugs in pediatric surgical units at tertiary care hospitals of Pakistan. Int J Clin Pharm. 2017;39:860. doi:10.1007/s11096-017-0485-8
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.