Back to Journals » Journal of Hepatocellular Carcinoma » Volume 9
Expert Insights on Current Treatments for Hepatocellular Carcinoma: Clinical and Molecular Approaches and Bottlenecks to Progress
Authors Shannon AH, Ruff SM, Pawlik TM ![]()
Received 20 September 2022
Accepted for publication 18 November 2022
Published 7 December 2022 Volume 2022:9 Pages 1247—1261
DOI https://doi.org/10.2147/JHC.S383922
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr David Gerber
Alexander H Shannon, Samantha M Ruff, Timothy M Pawlik
Department of Surgery, Division of Surgical Oncology, The Ohio State University Wexner Medical Center, Columbus, OH, USA
Correspondence: Timothy M Pawlik, Department of Surgery, The Urban Meyer III and Shelley Meyer Chair for Cancer Research, Professor of Surgery, Oncology, Health Services Management and Policy, The Ohio State University, Wexner Medical Center, 395 W. 12th Ave., Suite 670, Columbus, OH, USA, Tel +1 614 293 8701, Fax +1 614 293 4063, Email [email protected]
Abstract: Hepatocellular carcinoma (HCC) is a primary liver tumor that typically occurs in the setting of chronic liver disease/cirrhosis. Treatment modalities for HCC have evolved and given the variety of treatment options, a multi-disciplinary approach requiring input from surgical, medical, and radiation oncology, hepatology, and interventional radiology is necessary. Multiple advances have been made over the last decade regarding treatment of HCC, especially advanced disease. Resection and transplantation remain as cornerstone curative-intent treatment options. For patients who are not candidates for curative-intent therapy, exciting progress has been made in molecular and cellular approaches to systemic therapy for HCC including immunotherapies and tyrosine kinase inhibitors. Although the prognosis for advanced HCC remains poor, the armamentarium of therapies has increased, and valuable years of life can be gained with these therapies. While the main therapeutic modality for early-stage disease remains resection, multimodal immunotherapy has emerged as first-line treatment for advanced disease. We herein review different clinical and molecular treatment modalities related to the treatment of HCC, as well as provide insights into future directions for HCC treatment. We highlight how research and progress are needed to move into a new era of molecular and cellular treatments.
Keywords: hepatocellular carcinoma, current treatments
Introduction
Hepatocellular carcinoma (HCC) is a primary liver tumor that typically occurs in the setting of chronic liver disease/cirrhosis. Responsible for most liver cancer diagnoses and deaths, HCC generally has a poor prognosis with a five-year survival of 20–40%, especially among patients with advanced disease.1,2 Risk factors for HCC include hepatitis B virus (HBV), hepatitis C virus (HCV), non-alcoholic fatty liver disease (NAFLD), alcoholic cirrhosis, tobacco use, and inherited disorders such as hemochromatosis, Wilson’s disease, and alpha-1 antitrypsin deficiency.3
Treatment modalities for HCC have evolved and given the variety of treatment options, a multi-disciplinary approach requiring input from surgical, medical, and radiation oncology, hepatology, and interventional radiology is necessary. Determining the best treatment option is challenging given the frequent presence of underlying liver cirrhosis/fibrosis, burden and extent of disease, and different etiologies of HCC.4 Resection is a common curative-intent treatment option for HCC; however, many patients are not eligible due to advanced stage or inadequate functional liver reserve (FLR). Other options for HCC – depending on extent of tumor burden and underlying liver disease – including transplantation, thermal ablation, and locoregional and systemic therapies. We herein review the latest treatments for HCC and discuss barriers to progress in the field. In particular, a literature review was performed of data published on HCC between 2018 and 2022 using google.com, Google Scholar, and PubMed database.
Diagnosis and Staging
To fully understand treatment options, it is important to review how HCC is diagnosed and staged, which can guide treatment decisions. HCC can be diagnosed as an incidental lesion in an asymptomatic patient or can be detected at an advanced stage. Advanced disease usually presents with vague symptoms such as anorexia, weight loss, malaise, and right upper quadrant pain; the physical exam may reveal jaundice or hepatomegaly. Imaging with multi-phase CT scan or MRI utilizing the LI-RADs classification system is a key to work-up of patients with suspected HCC. HCC is characterized by arterial hypervascularity and rapid wash out in the portal venous phase.5 Imaging characteristics are often pathognomonic; however, biopsy is sometimes required for diagnosis. Serum alpha-fetoprotein (AFP) is serum marker often used relatively to HCC, however it is neither sensitive nor specific and cannot be used reliably to rule in or out HCC.6 Complete staging workup should also include a CT chest, viral serologies, and assessment of liver function as part of the initial work up.7 Liver function has traditionally been assessed using the Child-Turcotte-Pugh classification, although the Model for End-Stage Liver Disease (MELD) and the new Albumin-Bilirubin grade (ALBI) score are now often more commonly used.8–10 The ALBI score assessing liver function using objective values related to bilirubin and albumin; the ALBI score has been validated and eliminates the use of more subjective measures, like ascites and encephalopathy in Child-Turcotte-Pugh score.9
There are a wide range of HCC staging systems, including the American Joint Committee on Cancer (AJCC)/Union for International Cancer Control (UICC), the Cancer of the Liver Italian Program (CLIP) score, and BCLC system.11,12 The AJCC/UICC is based on pathological findings and utilizes Tumor, Node, Metastasis (TNM) classification; AJCC/UICC staging does not incorporate histologic grade or cirrhosis.13 In contrast, the CLIP system utilizes tumor morphology, serum AFP, and presence/absence of portal vein thrombosis, as well as the severity of cirrhosis to determine prognosis; CLIP can be applied to patients undergoing surgery, as well as individuals who are treated with transarterial chemoembolization (TACE).14
The most often used staging system is likely the BCLC, which was just updated in 2022.15 The BCLC estimates prognosis, as well as provides specific treatment recommendations relative to tumor burden, liver function, and Eastern Cooperative Oncology Group (ECOG)-performance status; the BCLC guidelines can change based on individual factors and response to first-line therapy.15 The BCLC categorizes patients into one of five categories: Very early stage (0), Early stage (A), Intermediate stage (B), Advanced stage (C), and Terminal stage (D) (Figure 1). BCLC-0 may be candidates for resection, liver transplantation or ablation.16 Similarly, early stage (BCLC-A) includes patients with single or less than 3 nodules all less than 3 cm who have preserved liver function based on portal pressure and bilirubin, as well as performance status; BCLC-A patients benefit from resection, ablation, or transplant. Patients with advanced BCLC-C stage disease are characterized as having preserved liver function but portal invasion with or without extrahepatic spread and poor performance status; these patients are generally treated with systemic therapy. Terminal stage (BCLC-D) patients with end stage liver disease and poor performance status typically are only candidates for best supportive care.
 |
Figure 1 Barcelona Clinic Liver Cancer (BCLC) staging, treatment strategy, and prognosis in 2022. Reproduced from Reig M, Forner A, Rimola J, et al. BCLC strategy for prognosis prediction and treatment recommendation: the 2022 update. J Hepatol. 2022;76(3):681–693. © 2021 European Association for the Study of the Liver. Published by Elsevier B.V. All rights reserved.15 Abbreviations: AFP, alpha-fetoprotein; ALBI, albumin-bilirubin; BSC, best supportive care; ECOG-PS, Eastern Cooperative Oncology Group-performance status; LT, liver transplantation; MELD, model for end stage liver disease; TACE, transarterial chemoembolization. |
There has been debate about BCLC recommendations for intermediate stage (BCLC-B), defined as multinodular disease without vascular invasion or extrahepatic spread with preserved liver function and performance status. The current treatment recommendations for this group of patients range from liver transplant using “extended liver transplant criteria” beyond the Milan Criteria versus TACE for individuals who are not transplant candidates or systemic therapy for patients who are not TACE candidates.15,17,18 Notably absent from this treatment algorithm is surgical resection presumably due to belief that multinodular disease assumes a prohibitive prognosis following resection. Evidence suggests, however, surgical that resection can indeed be an option for select patients with intermediate stage BCLC-B disease and may provide better survival outcomes versus TACE.19–26 In one review, Kim et al compared surgical resection ± intraoperative ablation versus TACE among patients with intermediate stage HCC and preserved liver function.21 The authors reported that overall survival (OS) and progression-free survival (PFS) were longer among patients who underwent resection + ablation versus TACE (OS 88.6 vs 56.2 months and PFS 18.4 vs 15.3 months, respectively).21 As such, BCLC recommendations for intermediate stage HCC may not be applicable for all patients with BCLC-B disease.
Treatments for Early and Intermediate HCC
Surgical Resection
Hepatic resection is an option for patients with early-stage HCC disease. Many patients are not candidates for resection, however, due to underlying liver dysfunction or locally advanced disease. Patients best suited for resection are generally individuals who have a solitary tumor without evidence of vascular invasion and have adequate hepatic reserve based with an adequate FLR. Patients with an inadequate FLR (ie, <20% for noncirrhotics and <35–40% for cirrhotics) may require portal vein embolization prior to resection to induce hypertrophy of the FL. Resection is associated with a 5-year survival of 40–60%, depending on stage of disease; 5-year recurrence can be high (>70%) due to the underlying chronic inflammation of the liver that alters the immune environment.27,28 While some surgeons have advocated for anatomic resection for HCC, other data have suggested that nonanatomic resection had comparable risk of recurrence and prognosis as long as an adequate margin was achieved.29,30 To this point, data from meta-analyses and prospective studies note that anatomic hepatectomy, when feasible given tumor size, multinodular disease, and involvement of surrounding structures was associated with lower recurrence and better long-term outcomes, especially for tumors with microvascular invasion.31–35
Liver Transplant
Liver transplant is therapeutic option for individuals with early-stage HCC that offers the best chance for optimal long-term outcomes. The determination of liver transplant vs resection is complex, requiring balancing of many factors such as underlying liver function, presence of portal hypertension, performance status, and tumor characteristics. Traditionally, the Milan Criteria, defined as a solitary lesion <5 cm or three separate lesions <3 cm without vascular invasion or distant metastases, was used to determine if a patient is a transplant candidate.36 Transplantation of HCC has been associated with 5- and 10-year survival of 70% and 50%, respectively; 5-year recurrence has been reported to be 10–15%.4 Unfortunately, organs are scarce and many patients with HCC progress on the wait list.
In an attempt to expand the number of patients eligible for transplantation, “extended liver transplant criteria” (ie, UCSF criteria, “up-to-seven”) have been adopted at many centers.17,18 The UCSF exception criteria are used to assess patients with HCC for liver transplant who have solitary tumor <6.5 cm, patients with 3 or fewer nodules with largest <4.5 cm or having a total diameter less than 8.5 cm without vascular invasion.37 Other surgeons have suggested using alpha fetoprotein level and uptake on PET-CT scans to help select patients with advanced HCC who may or may not be appropriate candidates for transplantation.38 In addition, neoadjuvant therapy has been proposed as a possible means to reduce tumor burden to fit Milan Criteria.39
Ablation
Ablation involves inducing tumor necrosis either with thermal energy or cryoablation to the lesion. Radiofrequency ablation (RFA) and microwave ablation (MWA) are two forms of thermal ablation. MWA has replaced RFA at many institutions due to the lack of a heat sink effect, as well as its speed and ease compared with RFA. Generally, ablation is applicable for single tumors that are <3–4 cm. Currently, the BCLC staging update in 2022 recommends ablation for very early stage (BCLC-0) who are not candidates for liver transplant and early stage (BCLC-A) patients who have increased portal pressure or bilirubin and contraindications to liver transplant.15
Embolization
Given that most of the blood supply to liver tumors is derived from the hepatic artery, embolization naturally evolved as a therapeutic modality for intermediate to large size HCC (5–7 cm) that is unresectable and not amenable to ablation techniques. By eliminating the blood supply to the lesion, tumor ischemia results followed by cell death. TACE uses embolization and adds concentrated chemotherapy to augment the effect of the therapy. Relative/absolute contraindications to TACE or embolization include absent or reduced portal vein flow and decompensated cirrhosis. The BCLC 2022 update describes TACE as therapeutic options for certain intermediate stage (BCLC-B) tumors, defined as multinodular tumors with preserved liver function among patients with good/fair performance status. The staging system divides BCLC-B into three subgroups: patients with well-defined HCC nodules who may be candidates for transplant via extended criteria, patients with well-defined nodules and preserved portal flow, who may be candidates for TACE, and patients with diffuse infiltrative extensive bilateral liver involvement, who may be candidates for systemic therapy.15,17,18 Radioembolization is a potential alternative to TACE, which uses intraarterial injection of 90-Y labeled microspheres to induce tumor necrosis. In one study comparing TACE with radioembolization, there was a longer time to tumor progression in radioembolization group with similar response rates and overall survival.40
Treatments for Advanced HCC
For many years, patients with advanced HCC, such as portal invasion and/or extrahepatic spread, had very few treatment options. Cirrhotic patients often would not tolerate chemotherapy and if chemotherapy was given, it was thought to be less efficacious in cirrhotics.41 The SHARP trial in 2008 demonstrated improved survival with sorafenib versus placebo/best supportive care.42 Sorafenib (Nexavar) is an inhibitor of tyrosine kinase receptors of vascular endothelial growth factors (VEGF) and platelet-derived growth factor receptor-beta (PDGFR-B), both of which have been implicated in the pathogenesis of HCC.43,44 Lenvatinib, another VEGF and PDGFR-B inhibitor, emerged as non-inferior to sorafenib, and has been used in patients intolerant of sorafenib.45 As a result of the SHARP trial, sorafenib became the standard treatment for patients with advanced HCC, especially in the United States. However, follow-up studies noted markedly lower survival rates than initially reported in the SHARP trial and demonstrated that the benefit of sorafenib was greater in patients with hepatitis C as the underlying etiology of HCC versus other etiologies.46–48 The side effect profiles of sorafenib and Lenvatinib were also significant. More recently, researchers have identified more efficacious systemic therapies for patients with advanced HCC (Table 1).
 |
Table 1 Summary of Select Trials for the Treatment of Advanced HCC |
Immunotherapy for Advanced HCC
Atezolizumab and Bevacizumab
Over time, the treatment paradigm for advanced HCC has shifted from sorafenib as first-line treatment to newer immunotherapies. Immunotherapy for advanced HCC initially involved single agent therapy. For example, monotherapy with nivolumab, a PD-L1 inhibitor, was demonstrated not to improve OS or PFS compared with sorafenib in the CheckMate 040 study published in 2022.49 Consequently, attention shifted to the use of multiple agents to address tumor heterogeneity. To this end, Lee et al investigated the use of Atezolizumab (Atezo) with and without bevacizumab (Bev) among patients with unresectable HCC not previously treated with systemic therapy.50 Atezo is a PD-L1 inhibitor, while bevacizumab inhibits VEGF. In this study, combination therapy was associated with a longer progression-free survival versus atezolizumab alone.50
The landmark Phase III multi-center global IMbrave 150 trial compared Atezo-Bev versus sorafenib among patients with unresectable HCC; primary outcomes included overall survival (OS) and progression-free survival (PFS). Five hundred one patients were randomized to either the Atezo-Bev or sorafenib treatment arms. Inclusion criteria were unresectable disease and preserved liver function defined as Child-Pugh class A, no prior systemic treatment for HCC, and treatment of esophageal varices if present on endoscopy within the last 6 months. One year OS was 67.2% among patients treated with Atezo-Bev versus 54.6% among patients treated with sorafenib; median PFS was 6.8 months and 4.3 months for Atezo-Bev and sorafenib, respectively.51 An interim update of the IMbrave 150 trial demonstrated continued improvement in OS and PFS among patients treated with Atezo-Bev versus sorafenib.52 The incidence of adverse events in the two groups was largely comparable, however individuals treated with Atezo-Bev experienced a higher incidence of hypertension, transaminitis, and proteinuria; diarrhea was more common in the sorafenib group. Upper gastrointestinal bleeding is the most serious potential adverse effect of Atezo-Bev. As such, patients required an upper endoscopy with intervention for any esophageal varices prior to enrollment; untreated or severe esophageal varices were a contraindication to Atezo-Bev use. Given that only with patients who had preserved liver function (Childs-Pugh A) were included in the trial, the effects of Atezo-Bev remain unclear among patients with worse liver function. Atezo-Bev is also contraindicated for patients who recur after liver transplantation, due to risk of allograft rejection with the use of these agents, as well as a relative contraindication in patients with severe autoimmune disorders or arterial hypertension.53,54
Patient reported outcomes after therapy with either drug demonstrated that patients treated with Atezo-Bev had better reported quality of life, overall function, and disease symptoms compared with individuals treated with sorafenib.55 A recent systematic review confirmed these findings and the United States Food and Drug Administration (FDA) approved Atez-Bev as first-line therapy for unresectable HCC on May 29, 2020 (Figure 2).56,57 In turn, the updated BCLC staging algorithm recommends consideration of Atezo-Bev for patients with BCLC-C, defined by vascular invasion or extrahepatic spread.15,53 In fact, both the BCLC and the American Society of Clinical Oncology (ASCO) recommend Atezo-Bev as first-line treatment for advanced HCC.15,58
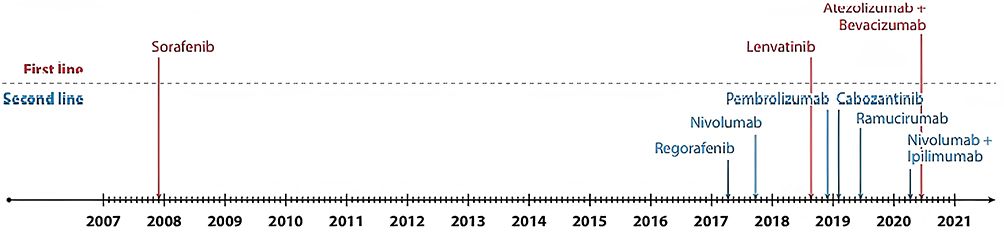 |
Figure 2 Timeline of United States Food and Drug Administration approvals for the systemic treatment of hepatocellular carcinoma. Used with permission of Annual Review, Inc., from Hepatocellular Carcinoma Immunotherapy, Sperandio RC, Pestana RC, Miyamura BV, Kaseb AO, Volume 73, 2022; permission conveyed through Copyright Clearance Center, Inc.59 |
The combination of bevacizumab and sintilimab, another anti-PD-1 monoclonal antibody, has also been studied in a Chinese cohort of patients with HCC, who had a high prevalence of hepatitis B. The ORIENT-32 clinical trial compared sintilimab plus IBI305, a bevacizumab biosimilar, to sorafenib as first-line therapy for patients with unresectable hepatitis B related HCC. The primary outcomes were median OS and PFS both of which were significantly longer in the sintilimab plus IBI305 group.60 This data is encouraging for patients with hepatitis B related HCC.
Tremelimumab and Durvalumab
The 2022 BCLC guidelines state Atezo-Bev should be first-line treatment for advanced HCC (BCLC-C); however, combination therapy with tremelimumab plus durvalumab has also emerged as an alternative approach. Tremelimumab is an anti-cytotoxic T-lymphocyte associate protein 4 (CTLA-4) monoclonal antibody and durvalumab is an anti PD-L1 monoclonal antibody. The phase III HIMALAYA trial was presented at the American Society of Clinical Oncology in March 2022. These data included over 1000 patients with Child-Pugh class A cirrhosis, no prior systemic therapy, and unresectable disease. Patients treated with single priming dose tremelimumab and interval durvalumab had a significant improvement in OS and objective response rate (ORR) compared with sorafenib (OS 16.4 vs 13.3 months and ORR 20 vs 5%, respectively).61 The HIMALAYA trial demonstrated that durvalumab monotherapy was non-inferior to sorafenib in terms of median OS (16.6 vs 13.8 months); durvalumab had a higher objective response rate (17 vs 5%) and a better side effect profile with a lower discontinuation of therapy (4 vs 11%).61 Patients treated with durvalumab monotherapy versus tremelimumab plus durvalumab had similar median OS (16.4 vs 16.6 months), however combination therapy was associated with better survival at 3-years.61 The safety profile of tremelimumab and durvalumab was assessed in a phase I/II trial by Kelley et al.62 In this study, tremelimumab or durvalumab monotherapy alone had similar toxicity profiles; however, ORR and OS were better among patients with tremelimumab plus durvalumab. The main adverse events associated with combination therapy included pruritis and rash, as well as transaminitis. Of note, only patients with preserved liver function and good performance status were included in these studies. Importantly, the OS benefit of tremelimumab plus durvalumab was not as pronounced among patients with hepatitis C related HCC. Despite these limitations, tremelimumab plus durvalumab may be an acceptable alternative for patients with unresectable HCC who are not candidates for Atezo-Bev.
Ramucirumab
Ramucirumab is another immunotherapy approach to HCC, which has been used especially in the setting of sorafenib or other immunotherapy failures. Ramucirumab is a recombinant monoclonal antibody of the immunoglobulin G class (IgG) and blocks the receptor for VEGFR-2. In a small trial of 42 patients, there was an objective response rate of 10% and median OS was 12 months.63 Unfortunately, there have been no studies directly comparing ramucirumab to sorafenib and therefore it has largely been used as second-line therapy.
Although currently only indicated in patients who have failed sorafenib, the benefit of ramucirumab has been demonstrated in several patient populations, such as those with high alpha feto-protein (AFP) levels. For example, in one study, median survival of patients with AFP levels >400 ng/mL was 7.8 months among individuals treated with ramucirumab versus only 4.2 months for placebo.64 In the REACH-2 trial, 300 patients with progression on sorafenib who had AFP >400 ng/mL were randomized to ramucirumab or placebo. Patients treated with ramucirumab had better OS and objective response rate.65 The side effect profile was generally tolerable with fatigue, abdominal pain, hypertension, and lower extremity edema being the most commonly reported symptoms. Consequently, the FDA approved ramucirumab as second-line therapy for HCC with progression after sorafenib in the setting of an AFP > 400 ng/mL at initial diagnosis (Figure 2).
Nivolumab and Ipilimumab
Nivolumab monotherapy has been demonstrated to improve outcomes of patients with advanced HCC.49,66 Combination immunotherapy with multiple agents such as nivolumab and ipilimumab has also been investigated. Nivolumab is a human monoclonal antibody that targets PD-1, whereas ipilimumab is an inhibitor of CTLA-4. The CheckMate 040 trial compared nivolumab plus ipilimumab combination therapy versus nivolumab monotherapy among 148 Child-Pugh A patients with advanced HCC who were previously treated with sorafenib. Combination therapy demonstrated an objective response rate of 32% versus just 14% among patients treated with nivolumab monotherapy. Median OS was 22.2 months in the combination group; there were, however, more adverse side effects including rash, adrenal insufficiency, hypothyroidism, or thyroiditis.67 Based on the results of this trial, the FDA approved combination therapy with nivolumab plus ipilimumab for treatment of advanced HCC for patients who had progressed on sorafenib (Figure 2). Unfortunately, no data are currently available relative to combination therapy after initial immunotherapy such as Atezo-Bev.
Pembrolizumab
Pembrolizumab is another anti-PD-1 monoclonal antibody that has been studied in HCC patients post sorafenib treatment. The KEYNOTE-240 randomized 413 patients with advanced HCC, Child-Pugh class A cirrhosis, who had been previously treated with sorafenib.66 In this trial, patients were randomized to take pembrolizumab or placebo. Median OS was 14 months for patients treated with pembrolizumab versus 10.6 months for patient receiving placebo; PFS was 3 and 2.8 months, respectively.66 The objective response rate was markedly better among patient treated with pembrolizumab (18.3%) versus placebo (4.4%). Grade 3 or higher adverse events occurred in 52.7% of patients in the pembrolizumab group. The most common adverse effect was transaminitis and hyperbilirubinemia. Other major toxicities reported with pembrolizumab use include myocarditis, anemia, rash, colitis, diarrhea, and endocrinopathies. The FDA granted approval for pembrolizumab monotherapy for patients previously treated with sorafenib; however, pembrolizumab has not been endorsed in most European society recommendations due to no difference in OS or PFS.68
Avelumab
Like pembrolizumab, avelumab is another monoclonal antibody that targets PD-1. Avelumab has shown promise in the treatment of other malignancies such as Merkel cell carcinoma, urothelial carcinoma, and renal cell carcinoma.69–71 Lee et al reported data from a single center study that examined tumor response after administration of avelumab among patients with Child-Pugh A cirrhosis and unresectable HCC who had been previously treated with sorafenib. The objective response rate was 10%; TTP and OS were 4.4 and 14.2 months, respectively. The authors concluded that avelumab had moderate efficacy and was safe for use in this patient population.72 A second small study from Japan demonstrated similar efficacy of avelumab in combination with axitinib, a tyrosine kinase inhibitor of VEGFR1-3, as first-line therapy for advanced HCC.73 Although these trials show promise, avelumab has not been approved by the FDA for use in the treatment of HCC. As such, avelumab has not been included in any current HCC treatment algorithms.
Current Systemic Therapies for Advanced HCC
In addition to immunotherapy, systemic therapies have evolved over the decade.
Cabozantinib
Cabozantinib is an inhibitor of multiple tyrosine kinases including VEGFR1-3, hepatocyte growth factor/c-MET.74 The 2022 BCLC guidelines note that cabozantinib is appropriate as second-line therapy for BCLC-C advanced HCC after progression of disease on sorafenib. The phase III CELESTIAL trial assessed 707 patients with advanced HCC who had progressed on sorafenib treatment. Patients were randomized to receive cabozantinib monotherapy or placebo. Median OS for cabozantinib and placebo was 10.2 vs 8 months, respectively; progression-free survival was 5.2 vs 1.9 months, respectively.75 Cabozantinib was associated with more side effects, including hand and foot syndrome, diarrhea, transaminitis, and fatigue.75 The FDA granted approval for cabozantinib as second-line therapy in January 2019 (Figure 2). The patient profile for treatment with cabozantinib included only individuals with preserved liver function and performance status.
Cabozantinib has been shown to be effective in the treatment of multiple solid organ tumors, such as renal cell carcinoma and prostate cancer, in conjunction with immune checkpoint inhibitors.76–78 Accordingly, the role of cabozantinib combination therapy in advanced HCC has been investigated. The COSMIC-312 trial, published in 2022, compared the effectiveness of cabozantinib plus atezolizumab versus sorafenib for advanced HCC not amenable to curative-intent treatment or locoregional therapy. Preliminary data demonstrated that primary PFS was longer among patients treated with cabozantinib plus atezolizumab versus sorafenib (6.8 vs 4.2 months); median OS was, however, not significantly different on interim analysis. Overall, the combination therapy with cabozantinib plus atezolizumab improved PFS versus sorafenib, however there was no difference in OS. As such, prior to recommending atezolizumab as therapy, this combination therapy warrants additional study and is not part of 2022 BCLC treatment algorithm.
Lenvatinib
Lenvatinib is an inhibitor of VEGFR1-3 and FGFR1-4, PDGFR-alpha, RET, and KIT. Multiple studies have demonstrated its effectiveness among patients with unresectable advanced HCC who are not eligible for local therapy.45,79 The REFLECT trial compared lenvatinib versus sorafenib among patients with unresectable HCC. The primary end point was median OS, which was 13.6 months and 12.3 months for patients treated with lenvatinib and sorafenib, respectively. The objective response rate and median time to progression were better among patients treated with lenvatinib. Side effect profile was generally tolerable with hypertension, hand and foot syndrome, proteinuria, dysphonia, and diarrhea being the most commonly reported. As a result, lenvatinib was approved for use in the United States in August 2018 and is currently recommended as first-line therapy for patients who are not eligible or cannot tolerate Atezo-Bev or tremelimumab plus durvalumab.
Recent research has focused on the use of lenvatinib and pembrolizumab, an anti PD-L1 inhibitor. In one multicenter study, 104 patients with unresectable advanced HCC were treated with lenvatinib and pembrolizumab to determine safety and tolerability, as well as response rate.80 Preliminary data demonstrated the safety of this combination and the future potential, although the use has yet to be embraced by any treatment guidelines.80
Regorafenib
Regorafenib is another tyrosine kinase inhibitor that has been added to treatment algorithms for advanced HCC who have had disease progression on sorafenib. Regorafenib inhibits VEGFR1-3, as well as multiple other kinase receptors such as PDGFRB, KIT, RET, and RAF-1. The phase III RESOURCE trial investigated patients with advanced HCC who had progression on sorafenib and were subsequently placed either on regorafenib or placebo. The RESOURCE trial included only patients with Child-Pugh A cirrhosis, good performance status, and only individuals who had been treated with at least 20 days of sorafenib. Median OS was higher among patients treated with regorafenib versus placebo (10.6 vs 7.8 months, respectively); regorafenib was well tolerated with few adverse events.81 Similar to other drugs, rash, hyperbilirubinemia, hand and foot syndrome, anemia, proteinuria, abdominal pain, and diarrhea were common side effects. Consequently, the FDA approved its use in 2017 as second-line therapy for patients who have received sorafenib or Lenvatinib (Figure 2). Regorafenib is now part of the American Society of Clinical Oncology (ASCO) and BCLC guidelines for treatment of HCC.15,58
Apatinib and Donafenib
Apatinib is a VEGFR-2 inhibitor that has been used to treat advanced gastric cancer.82 A phase III clinical trial from China examined the use of apatinib among patients with advanced HCC who had been treated with systemic therapy.83 Median OS was longer among patients treated with apatinib versus placebo (8.7 vs 6.8 months, respectively) and the tolerability profile associated with apatinib was acceptable.83 Of note, patients in this study had a particularly high prevalence of hepatitis B. A second nonrandomized study assessed objective response rate among patients with unresectable disease treated with apatinib in combination with camrelizumab, an anti PD-1 monoclonal antibody. The objective response rate was 34.3% and 12-month survival was 74.7%; the combination of apatinib and camrelizumab was generally well tolerated.84 Apatinib was approved for use as second-line therapy in China after failure or progression with sorafenib or chemotherapy with oxaliplatin. Apatinib is not currently available or approved in the United States or Europe.
Donafenib, a novel multi-kinase inhibitor derived from sorafenib, has been approved in China but not in the United States or Europe. A phase III clinical trial randomized patients with unresectable or metastatic HCC without prior treatment to receive donafenib or sorafenib and then assessed OS.85 Median OS was longer among patients treated with donafenib versus sorafenib (12.1 vs 10.3 months respectively); however, there was no difference in the objective response rate (4.6% vs 2.7%) or median PFS (3.7 vs, 3.6 months). Donafenib was well tolerated and had an acceptable safety profile. In turn, the authors proposed donafenib use as first-line therapy for patients with unresectable HCC in lieu of sorafenib.85
Emerging Therapies
While much progress has been made, multiple areas of research continue to emerge. For example, neoadjuvant therapy to treat patients with advanced HCC has been a topic of growing interest. While there are no standard recommendations for neoadjuvant therapy, nivolumab and ipilimumab have proven efficacy as neoadjuvant therapy for a host of several cancers such as melanoma, bladder cancer, urothelial cancer, and non-small cell lung cancer.86–89 The PRIME-HCC is an ongoing phase IB clinical trial that is examining ipilimumab plus nivolumab in the neoadjuvant setting for early-stage HCC prior to liver resection.90 While the results of this study are pending, hopefully the data will help delineate the role of neoadjuvant therapy in the perioperative management of resectable HCC.
Another potential agent that is a candidate for neoadjuvant therapy is dovitinib. Dovitinib is a tyrosine kinase that inhibits multiple angiogenesis pathways similar to sorafenib and lenvatinib. A recent Phase II trial of 24 patients with early and intermediate stage HCC (BCLC grade 0, A-B) were treated with neoadjuvant therapy oral dovitinib followed by locoregional therapy; objective response rates, TTP, and OS were assessed.91 Overall results were favorable with an objective response rate of 48%, TTP of 16.8 months, and OS of 34.8 months. Tolerance of dovitinib had a wide range, resulting in dose adjustment or discontinuation in many cases. There are currently several trials investigating neoadjuvant therapy for resectable disease including neoadjuvant cabozantinib and nivolumab (NCT03299946), neoadjuvant and adjuvant pembrolizumab (NCT03337841), and neoadjuvant ipilimumab and nivolumab (NCT03222076, NCT03682276).
A final exciting area of focus is vaccines for HCC. The HepaVac-101 is a phase I/II multicenter single arm trial assessing a novel vaccine for HCC. The study assessed 22 patients with early or intermediate HCC and suitable HLA haplotype; patients were given nine intradermal injections of the vaccine, which consisted of multi-peptide antigens identified on human HCC tissue and an RNA-based immunostimulator. Primary end points were safety, tolerability, and antigen specific T-cell responses. The results were promising with a good safety profile; there was an immune response against HLA class I (37%) and HLA class II (53%) tumor peptides.92 While promising, the results need to be validated in a larger clinical setting.
Challenges to Progress
Despite the progress over the last decade with immunotherapy and systemic treatments, there are still many challenges related to the treatment of patients with advanced HCC. The underlying cause of HCC varies among populations, with NASH and alcohol as leading causes in the US, whereas HBV and HCV are more common in eastern Asia (Figure 3). Given the differing populations, studies from one part of the world may not be applicable to another.
 |
Figure 3 The incidence of hepatocellular carcinoma according to geographical area and etiology. Reproduced from Reig M, Forner A, Rimola J, et al. BCLC strategy for prognosis prediction and treatment recommendation: the 2022 update. J Hepatol. 2022;76(3):681–693. © 2021 European Association for the Study of the Liver. Published by Elsevier B.V. All rights reserved.15 Abbreviations: HBV, hepatitis B virus; HCV, hepatitis C virus; NASH, non-alcoholic steatohepatitis; ASR, age-standardized incidence rate. |
Another challenge is that virtual all studies only include patients with Child-Pugh A cirrhosis with preserved functional status. In turn, the results of many trials can be difficult to extrapolate to individuals with Child-Pugh B/C cirrhosis or individuals with poor functional status. The guidelines relative to systemic therapy and immunotherapies, including tyrosine kinase inhibitors, are less clear for patients with cirrhosis or poor performance status. For example, nivolumab may not be safe in patients with Child-Pugh B patients. The CELESTIAL trial retrospectively reviewed patients with Child-Pugh B cirrhosis and did note modest efficacy and safety of cabozantinib in this population.93,94
An additional challenge to progress in the treatment of advanced HCC involves health disparities. Certain racial or ethnic groups such as African or Asian/pacific Americans are disproportionately affected by HCC and African Americans are generally diagnosed at more advanced stages than other racial/ethnic groups.95 Additionally, multiple studies have noted that race/ethnicity and socioeconomic status affect access to care.96,97 Complicating matters further are the exorbitant cost of these therapies that can serve as additional barriers to access.98 Addressing issues of cost and disparities in access to treatment will be crucial to ensure equitable care for patients with HCC.
One challenge in the systemic treatment of HCC is the development of therapeutic resistance. HCC is characterized by genetic heterogeneity and a diverse tumor microenvironment, which contributes to failure of treatment; as a result, HCC has historically been chemotherapy-refractory.99 Resistance to sorafenib is well documented and its mechanism continues to be elucidated.100,101 Tumor heterogeneity poses a grave challenge to the development of novel therapies for HCC and may contribute to resistance to newer therapies.
Expert Opinion
Treatment modalities for HCC have evolved over the last decade with many more options available than a decade ago. While surgical resection and transplantation remain the main treatment paradigms for early and intermediate stage disease, patients with advanced HCC have fewer options and a poorer prognosis. HCC is a complex disease with a varying underlying pathogenesis related to different etiologies such as hepatitis viral infection, alcohol, and NASH cirrhosis. Each underlying etiology may drive heterogeneous changes at the molecular level causing differing tumor genotypes, as well as different tumor microenvironments. Guidelines such as the 2022 BCLC staging and treatment algorithm can help direct clinical decision-making, especially for patients with advanced stage disease.
More recently, immunotherapy has emerged as a primary treatment option for patients with advanced HCC. In particular, atezo/bev has demonstrated benefit as a first-line therapy, which now has replaced sorafenib as the main treatment option. While there is considerable excitement about immunotherapy, it is unclear whether all patients with advanced disease will benefit from immunotherapy given the heterogeneity associated with HCC tumors. In this regard, biomarkers may play a role in predicting which patients may benefit from certain therapies. Alpha fetoprotein (AFP) is the most well-known biomarker related to HCC and elevated levels >200 ng/mL have been associated with poor survival.102 Patients with HCC tumors that are characterized by PD-L1 and PD-1 expression have more favorable survival and response if treated with nivolumab versus patients who have tumors that lack these biomarkers.49,103,104 In addition, high VEGF expression and tumor mutational burden (TMB) have been associated with worse overall survival, especially among patients treated with sorafenib and Lenvatinib; TMB has also been demonstrated to be predictive of HCC progression and recurrence.105–109 Increases in certain phylums within the gut microbiome (Actinobacteria, Gemmiger, Parabacteroides, and lipopolysaccharide producers) have also been proposed as early biomarkers of HCC.110
The future of HCC treatment will likely involve the use of novel systemic/targeted/immuno-therapy for advanced disease, yet systemic adjuvant therapy will likely be increasingly used in the neoadjuvant/adjuvant setting for patients with resectable disease. Currently, there are several ongoing clinical trials investigating multimodal systemic therapy in the adjuvant setting after curative resection. The CheckMate 9DX (NCT03383458) is a Phase 3 trial looking at RFS with adjuvant Nivolumab versus placebo in the adjuvant setting after resection, whereas the KEYNOTE-937 (NCT03867084) is a phase 3 trial examining adjuvant pembrolizumab versus placebo. IMbrave050 (NCT04102098) and EMERALD-2 (NCT03847428) are also assessing adjuvant atezo/bev versus active surveillance and Durvalumab, and bevacizumab versus placebo, respectively, following curative-intent HCC resection.
Neoadjuvant therapy is also an active area of investigation with several ongoing clinical trials. The CaboNivo trial (NCT03299946) is a phase Ib trial assessing neoadjuvant cabozantinib and nivolumab followed by surgery. The Phase 2 trial NCT03337841 is investigating pembrolizumab prior to surgical resection with primary end point one-year RFS. Another phase 2 trial is the PLENTY202001, which is examining RFS among patients treated with neoadjuvant pembrolizumab and Lenvatinib followed by liver transplantation versus no intervention and liver transplantation. This study is unique in that the effects of immune checkpoint inhibitors in the setting of transplant is particularly unclear regarding allograft function and rejection.
Overall, treatment options for all stages of HCC have expanded exponentially in the past few years. Given the complexity of HCC, therapeutic inactivity and resistance are inevitable. The optimal treatment for advanced stage HCC may require multimodal immunotherapy that is tailored to tumor biology based on predictive biomarkers, underlying etiology of HCC, and the tumor microenvironment. While the main therapeutic modality for early-stage disease remains resection or transplantation, multimodal systemic therapy has emerged as first-line treatment for advanced disease. In the future, even patients with disease amenable to surgery are likely to be increasingly treated with neoadjuvant and/or adjuvant therapy.
Conclusion
Multiple advances have been made over the last decade regarding treatment of HCC, especially advanced disease. Resection and transplantation remain as cornerstone curative-intent treatment options. For patients who are not candidates for curative-intent therapy, exciting progress has been made in molecular and cellular approaches to systemic therapy for HCC including immunotherapies and tyrosine kinase inhibitors. Although the prognosis for advanced HCC remains poor, the armamentarium of therapies has increased, and valuable years of life can be gained with these therapies. Further research and progress into new targets for advanced disease as well as the role of neoadjuvant and adjuvant immunotherapy will be needed as we move into a new era of molecular and cellular treatments.
Disclosure
The authors report no conflicts of interest in this work.
References
1. McGlynn KA, Petrick JL, El-Serag HB. Epidemiology of hepatocellular carcinoma. Hepatology. 2021;73:4–13. doi:10.1002/hep.31288
2. Jemal A, Ward EM, Johnson CJ, et al. Annual report to the nation on the status of cancer, 1975–2014, featuring survival. J Natl Cancer Inst. 2017;109(9):1. doi:10.1093/jnci/djx030
3. Akinyemiju T, Abera S, Ahmed M, et al. The burden of primary liver cancer and underlying etiologies from 1990 to 2015 at the global, regional, and national level: results from the global burden of disease study 2015. JAMA Oncol. 2017;3(12):1683–1691.
4. Llovet JM, Kelley RK, Villanueva A, et al. Hepatocellular carcinoma. Nat Rev Dis Primers. 2021;7(1):6.
5. Marrero JA, Kulik LM, Sirlin CB, et al. Diagnosis, staging, and management of hepatocellular carcinoma: 2018 practice guidance by the American Association for the Study of Liver Diseases. Hepatology. 2018;68(2):723–750.
6. Farinati F, Marino D, De Giorgio M, et al. Diagnostic and prognostic role of alpha-fetoprotein in hepatocellular carcinoma: both or neither? Am J Gastroenterol. 2006;101(3):524–532.
7. Natsuizaka M, Omura T, Akaike T, et al. Clinical features of hepatocellular carcinoma with extrahepatic metastases. J Gastroenterol Hepatol. 2005;20(11):1781–1787.
8. Bruix J, Castells A, Bosch J, et al. Surgical resection of hepatocellular carcinoma in cirrhotic patients: prognostic value of preoperative portal pressure. Gastroenterology. 1996;111(4):1018–1022.
9. Johnson PJ, Berhane S, Kagebayashi C, et al. Assessment of liver function in patients with hepatocellular carcinoma: a new evidence-based approach - the ALBI grade. J Clin Oncol. 2015;33(6):550–558.
10. Martin AP, Bartels M, Hauss J, Fangmann J. Overview of the MELD score and the UNOS adult liver allocation system. Transplant Proc. 2007;39(10):3169–3174. doi:10.1016/j.transproceed.2007.04.025
11. Henderson JM, Sherman M, Tavill A, Abecassis M, Chejfec G, Gramlich T. AHPBA/AJCC consensus conference on staging of hepatocellular carcinoma: consensus statement. HPB. 2003;5(4):243–250. doi:10.1080/13651820310015833
12. Vauthey JN, Dixon E, Abdalla EK, et al. Pretreatment assessment of hepatocellular carcinoma: expert consensus statement. HPB. 2010;12(5):289–299. doi:10.1111/j.1477-2574.2010.00181.x
13. Shindoh J, Andreou A, Aloia TA, et al. Microvascular invasion does not predict long-term survival in hepatocellular carcinoma up to 2 cm: reappraisal of the staging system for solitary tumors. Ann Surg Oncol. 2013;20(4):1223–1229. doi:10.1245/s10434-012-2739-y
14. Cho YK, Chung JW, Kim JK, et al. Comparison of 7 staging systems for patients with hepatocellular carcinoma undergoing transarterial chemoembolization. Cancer. 2008;112(2):352–361. doi:10.1002/cncr.23185
15. Reig M, Forner A, Rimola J, et al. BCLC strategy for prognosis prediction and treatment recommendation: the 2022 update. J Hepatol. 2022;76(3):681–693. doi:10.1016/j.jhep.2021.11.018
16. Doyle A, Gorgen A, Muaddi H, et al. Outcomes of radiofrequency ablation as first-line therapy for hepatocellular carcinoma less than 3 cm in potentially transplantable patients. J Hepatol. 2019;70(5):866–873. doi:10.1016/j.jhep.2018.12.027
17. Mehta N, Bhangui P, Yao FY, et al. Liver transplantation for hepatocellular carcinoma. working group report from the ILTS transplant oncology consensus conference. Transplantation. 2020;104(6):1136–1142. doi:10.1097/TP.0000000000003174
18. Ferrer-Fàbrega J, Sampson-Dávila J, Forner A, et al. Limited tumour progression beyond Milan criteria while on the waiting list does not result in unacceptable impairment of survival. J Hepatol. 2021;75(5):1154–1163. doi:10.1016/j.jhep.2021.06.015
19. Zhong JH, Ke Y, Gong WF, et al. Hepatic resection associated with good survival for selected patients with intermediate and advanced-stage hepatocellular carcinoma. Ann Surg. 2014;260(2):329–340. doi:10.1097/SLA.0000000000000236
20. Yin L, Li H, Li AJ, et al. Partial hepatectomy vs. transcatheter arterial chemoembolization for resectable multiple hepatocellular carcinoma beyond Milan Criteria: a RCT. J Hepatol. 2014;61(1):82–88. doi:10.1016/j.jhep.2014.03.012
21. Kim GH, Kim JH, Ko HK, et al. Surgical resection plus intraoperative radiofrequency ablation versus chemoembolization for the treatment of intermediate-stage (BCLC B) hepatocellular carcinoma with preserved liver function: a propensity score-matched analysis. Cancers. 2022;14(10):1.
22. Zhang T, Zeng Y, Huang J, Liao M, Wu H. Combined resection with radiofrequency ablation for bilobar hepatocellular carcinoma: a single-center experience. J Surg Res. 2014;191(2):370–378. doi:10.1016/j.jss.2014.03.048
23. Espinosa W, Liu YW, Wang CC, et al. Combined resection and radiofrequency ablation versus transarterial embolization for intermediate-stage hepatocellular carcinoma: a propensity score matching study. J Formos Med Assoc. 2018;117(3):197–203. doi:10.1016/j.jfma.2017.03.014
24. Yan J, Man Z, Lu Q, Ma K. Long-term survival in patients receiving combination therapy with resection and radiofrequency ablation for multi-focal hepatocellular carcinoma classified as Barcelona clinic liver cancer stage B: a retrospective controlled study. Cancer Manag Res. 2020;12:2613–2621. doi:10.2147/CMAR.S237635
25. Tsilimigras DI, Bagante F, Sahara K, et al. Prognosis after resection of Barcelona Clinic Liver Cancer (BCLC) stage 0, A, and B hepatocellular carcinoma: a comprehensive assessment of the current BCLC classification. Ann Surg Oncol. 2019;26(11):3693–3700. doi:10.1245/s10434-019-07580-9
26. Wada H, Eguchi H, Noda T, et al. Selection criteria for hepatic resection in intermediate-stage (BCLC stage B) multiple hepatocellular carcinoma. Surgery. 2016;160(5):1227–1235. doi:10.1016/j.surg.2016.05.023
27. Llovet JM, Fuster J, Bruix J. Intention-to-treat analysis of surgical treatment for early hepatocellular carcinoma: resection versus transplantation. Hepatology. 1999;30(6):1434–1440. doi:10.1002/hep.510300629
28. Bruix J, Sherman M. Management of hepatocellular carcinoma. Hepatology. 2005;42(5):1208–1236.
29. Famularo S, Ceresoli M, Giani A, et al. Is it just a matter of surgical extension to achieve the cure of hepatocarcinoma? A Meta-analysis of propensity-matched and randomized studies for anatomic versus parenchyma-sparing liver resection. J Gastrointest Surg. 2021;25(1):94–103.
30. Famularo S, Di Sandro S, Giani A, et al. Long-term oncologic results of anatomic vs. parenchyma-sparing resection for hepatocellular carcinoma. A propensity score-matching analysis. Eur J Surg Oncol. 2018;44(10):1580–1587.
31. Zhou JM, Zhou CY, Chen XP, Zhang ZW. Anatomic resection improved the long-term outcome of hepatocellular carcinoma patients with microvascular invasion: a prospective cohort study. World J Gastrointest Oncol. 2021;13(12):2190–2202.
32. Liu H, Hu FJ, Li H, Lan T, Wu H. Anatomical vs nonanatomical liver resection for solitary hepatocellular carcinoma: a systematic review and meta-analysis. World J Gastrointest Oncol. 2021;13(11):1833–1846.
33. Sun Z, Li Z, Shi XL, He XW, Chen J, Song JH. Anatomic versus non-anatomic resection of hepatocellular carcinoma with microvascular invasion: a systematic review and meta-analysis. Asian J Surg. 2021;44(9):1143–1150.
34. Jiao S, Li G, Zhang D, Xu Y, Liu J, Li G. Anatomic versus non-anatomic resection for hepatocellular carcinoma, do we have an answer? A meta-analysis. Int J Surg. 2020;80:243–255.
35. Moris D, Tsilimigras DI, Kostakis ID, et al. Anatomic versus non-anatomic resection for hepatocellular carcinoma: a systematic review and meta-analysis. Eur J Surg Oncol. 2018;44(7):927–938.
36. Mazzaferro V, Regalia E, Doci R, et al. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N Engl J Med. 1996;334(11):693–699.
37. Yao FY, Ferrell L, Bass NM, et al. Liver transplantation for hepatocellular carcinoma: expansion of the tumor size limits does not adversely impact survival. Hepatology. 2001;33(6):1394–1403.
38. Hong G, Suh KS, Suh SW, et al. Alpha-fetoprotein and (18) F-FDGpositron emission tomography predict tumor recurrence better than Milan criteria in living donor liver transplantation. J Hepatol. 2016;64(4):852–859.
39. Cucchetti A, Serenari M, Sposito C, et al. Including mRECIST in the Metroticket 2.0 criteria improves prediction of hepatocellular carcinoma-related death after liver transplant. J Hepatol. 2020;73(2):342–348.
40. Salem R, Gordon AC, Mouli S, et al. Y90 Radioembolization significantly prolongs time to progression compared with chemoembolization in patients with hepatocellular carcinoma. Gastroenterology. 2016;151(6):1155–1163.e1152.
41. Nagahama H, Okada S, Okusaka T, et al. Predictive factors for tumor response to systemic chemotherapy in patients with hepatocellular carcinoma. Jpn J Clin Oncol. 1997;27(5):321–324.
42. Llovet JM, Ricci S, Mazzaferro V, et al. Sorafenib in advanced hepatocellular carcinoma. N Engl J Med. 2008;359(4):378–390.
43. Wilhelm SM, Carter C, Tang L, et al. BAY 43-9006 exhibits broad spectrum oral antitumor activity and targets the RAF/MEK/ERK pathway and receptor tyrosine kinases involved in tumor progression and angiogenesis. Cancer Res. 2004;64(19):7099–7109.
44. Chang YS, Adnane J, Trail PA, et al. Sorafenib (BAY 43-9006) inhibits tumor growth and vascularization and induces tumor apoptosis and hypoxia in RCC xenograft models. Cancer Chemother Pharmacol. 2007;59(5):561–574.
45. Kudo M, Finn RS, Qin S, et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: a randomised phase 3 non-inferiority trial. Lancet. 2018;391(10126):1163–1173.
46. Cheng AL, Kang YK, Chen Z, et al. Efficacy and safety of sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcinoma: a phase III randomised, double-blind, placebo-controlled trial. Lancet Oncol. 2009;10(1):25–34.
47. Bruix J, Raoul JL, Sherman M, et al. Efficacy and safety of sorafenib in patients with advanced hepatocellular carcinoma: subanalyses of a phase III trial. J Hepatol. 2012;57(4):821–829.
48. Jackson R, Psarelli EE, Berhane S, Khan H, Johnson P. Impact of viral status on survival in patients receiving sorafenib for advanced hepatocellular cancer: a meta-analysis of randomized phase III trials. J Clin Oncol. 2017;35(6):622–628.
49. Yau T, Park JW, Finn RS, et al. Nivolumab versus sorafenib in advanced hepatocellular carcinoma (CheckMate 459): a randomised, multicentre, open-label, phase 3 trial. Lancet Oncol. 2022;23(1):77–90.
50. Lee MS, Ryoo BY, Hsu CH, et al. Atezolizumab with or without bevacizumab in unresectable hepatocellular carcinoma (GO30140): an open-label, multicentre, phase 1b study. Lancet Oncol. 2020;21(6):808–820.
51. Finn RS, Qin S, Ikeda M, et al. Atezolizumab plus bevacizumab in unresectable hepatocellular carcinoma. N Engl J Med. 2020;382(20):1894–1905.
52. Cheng AL, Qin S, Ikeda M, et al. Updated efficacy and safety data from IMbrave150: atezolizumab plus bevacizumab vs. sorafenib for unresectable hepatocellular carcinoma. J Hepatol. 2022;76(4):862–873.
53. Bruix J, Chan SL, Galle PR, Rimassa L, Sangro B. Systemic treatment of hepatocellular carcinoma: an EASL position paper. J Hepatol. 2021;75(4):960–974.
54. Kumar V, Shinagare AB, Rennke HG, et al. The safety and efficacy of checkpoint inhibitors in transplant recipients: a case series and systematic review of literature. Oncologist. 2020;25(6):505–514.
55. Galle PR, Finn RS, Qin S, et al. Patient-reported outcomes with atezolizumab plus bevacizumab versus sorafenib in patients with unresectable hepatocellular carcinoma (IMbrave150): an open-label, randomised, phase 3 trial. Lancet Oncol. 2021;22(7):991–1001.
56. Casak SJ, Donoghue M, Fashoyin-Aje L, et al. FDA Approval summary: atezolizumab plus bevacizumab for the treatment of patients with advanced unresectable or metastatic hepatocellular carcinoma. Clin Cancer Res. 2021;27(7):1836–1841.
57. Sonbol MB, Riaz IB, Naqvi SAA, et al. Systemic therapy and sequencing options in advanced hepatocellular carcinoma: a systematic review and network meta-analysis. JAMA Oncol. 2020;6(12):e204930.
58. Gordan JD, Kennedy EB, Abou-Alfa GK, et al. Systemic therapy for advanced hepatocellular carcinoma: ASCO guideline. J Clin Oncol. 2020;38(36):4317–4345.
59. Sperandio RC, Pestana RC, Miyamura BV and Kaseb AO. (2022). Hepatocellular Carcinoma Immunotherapy. Annu Rev Med, 73(1), 267–278. 10.1146/annurev-med-042220-021121
60. Ren Z, Xu J, Bai Y, et al. Sintilimab plus a bevacizumab biosimilar (IBI305) versus sorafenib in unresectable hepatocellular carcinoma (ORIENT-32): a randomised, open-label, phase 2–3 study. Lancet Oncol. 2021;22(7):977–990.
61. Abou-Alfa GKCS, Kudo M, Lau G, et al. Phase 3 randomized, open-label, multicenter study of tremelimumab (T) and durvalumab (D) as first-line therapy in patients (pts) with unresectable hepatocellular carcinoma (uHCC): HIMALAYA (abstract 379). J Clin Oncol. 2022;40:379.
62. Kelley RK, Sangro B, Harris W, et al. Safety, efficacy, and pharmacodynamics of tremelimumab plus durvalumab for patients with unresectable hepatocellular carcinoma: randomized expansion of a phase I/II study. J Clin Oncol. 2021;39(27):2991–3001.
63. Zhu AX, Finn RS, Mulcahy M, et al. A phase II and biomarker study of ramucirumab, a human monoclonal antibody targeting the VEGF receptor-2, as first-line monotherapy in patients with advanced hepatocellular cancer. Clin Cancer Res. 2013;19(23):6614–6623.
64. Zhu AX, Park JO, Ryoo BY, et al. Ramucirumab versus placebo as second-line treatment in patients with advanced hepatocellular carcinoma following first-line therapy with sorafenib (REACH): a randomised, double-blind, multicentre, phase 3 trial. Lancet Oncol. 2015;16(7):859–870.
65. Zhu AX, Kang YK, Yen CJ, et al. Ramucirumab after sorafenib in patients with advanced hepatocellular carcinoma and increased α-fetoprotein concentrations (REACH-2): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2019;20(2):282–296.
66. Finn RS, Ryoo BY, Merle P, et al. Pembrolizumab as second-line therapy in patients with advanced hepatocellular carcinoma in KEYNOTE-240: a randomized, double-blind, phase III trial. J Clin Oncol. 2020;38(3):193–202.
67. Yau T, Kang YK, Kim TY, et al. Efficacy and safety of nivolumab plus ipilimumab in patients with advanced hepatocellular carcinoma previously treated with sorafenib: the CheckMate 040 randomized clinical trial. JAMA Oncol. 2020;6(11):e204564.
68. Vogel A, Martinelli E. Updated treatment recommendations for hepatocellular carcinoma (HCC) from the ESMO clinical practice guidelines. Ann Oncol. 2021;32(6):801–805.
69. Motzer RJ, Penkov K, Haanen J, et al. Avelumab plus axitinib versus sunitinib for advanced renal-cell carcinoma. N Engl J Med. 2019;380(12):1103–1115.
70. D’Angelo SP, Russell J, Lebbé C, et al. Efficacy and safety of first-line avelumab treatment in patients with stage iv metastatic Merkel cell carcinoma: a preplanned interim analysis of a clinical trial. JAMA Oncol. 2018;4(9):e180077.
71. Patel MR, Ellerton J, Infante JR, et al. Avelumab in metastatic urothelial carcinoma after platinum failure (JAVELIN Solid Tumor): pooled results from two expansion cohorts of an open-label, phase 1 trial. Lancet Oncol. 2018;19(1):51–64.
72. Lee DW, Cho EJ, Lee JH, et al. Phase II study of avelumab in patients with advanced hepatocellular carcinoma previously treated with sorafenib. Clin Cancer Res. 2021;27(3):713–718.
73. Kudo M, Motomura K, Wada Y, et al. Avelumab in combination with axitinib as first-line treatment in patients with advanced hepatocellular carcinoma: results from the phase 1b VEGF liver 100 trial. Liver Cancer. 2021;10(3):249–259.
74. Kelley RK, Verslype C, Cohn AL, et al. Cabozantinib in hepatocellular carcinoma: results of a phase 2 placebo-controlled randomized discontinuation study. Ann Oncol. 2017;28(3):528–534.
75. Abou-Alfa GK, Meyer T, Cheng AL, et al. Cabozantinib in patients with advanced and progressing hepatocellular carcinoma. N Engl J Med. 2018;379(1):54–63.
76. Choueiri TK, Powles T, Burotto M, et al. Nivolumab plus cabozantinib versus sunitinib for advanced renal-cell carcinoma. N Engl J Med. 2021;384(9):829–841.
77. Pal SK, McGregor B, Suárez C, et al. Cabozantinib in combination with atezolizumab for advanced renal cell carcinoma: results from the COSMIC-021 study. J Clin Oncol. 2021;39(33):3725–3736.
78. Agarwal N, McGregor B, Maughan BL, et al. Cabozantinib in combination with atezolizumab in patients with metastatic castration-resistant prostate cancer: results from an expansion cohort of a multicentre, open-label, phase 1b trial (COSMIC-021). Lancet Oncol. 2022;23(7):899–909.
79. Ikeda K, Kudo M, Kawazoe S, et al. Phase 2 study of lenvatinib in patients with advanced hepatocellular carcinoma. J Gastroenterol. 2017;52(4):512–519.
80. Finn RS, Ikeda M, Zhu AX, et al. Phase Ib study of lenvatinib plus pembrolizumab in patients with unresectable hepatocellular carcinoma. J Clin Oncol. 2020;38(26):2960–2970.
81. Bruix J, Qin S, Merle P, et al. Regorafenib for patients with hepatocellular carcinoma who progressed on sorafenib treatment (RESORCE): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2017;389(10064):56–66.
82. Lin JX, Xu YC, Lin W, et al. Effectiveness and safety of apatinib plus chemotherapy as neoadjuvant treatment for locally advanced gastric cancer: a nonrandomized controlled trial. JAMA Netw Open. 2021;4(7):e2116240.
83. Qin S, Li Q, Gu S, et al. Apatinib as second-line or later therapy in patients with advanced hepatocellular carcinoma (AHELP): a multicentre, double-blind, randomised, placebo-controlled, phase 3 trial. Lancet Gastroenterol Hepatol. 2021;6(7):559–568.
84. Xu J, Shen J, Gu S, et al. Camrelizumab in combination with apatinib in patients with advanced hepatocellular carcinoma (RESCUE): a nonrandomized, open-label, phase II trial. Clin Cancer Res. 2021;27(4):1003–1011.
85. Qin S, Bi F, Gu S, et al. Donafenib versus sorafenib in first-line treatment of unresectable or metastatic hepatocellular carcinoma: a randomized, open-label, parallel-controlled phase II–III trial. J Clin Oncol. 2021;39(27):3002–3011.
86. Huang AC, Orlowski RJ, Xu X, et al. A single dose of neoadjuvant PD-1 blockade predicts clinical outcomes in resectable melanoma. Nat Med. 2019;25(3):454–461.
87. Jia XH, Xu H, Geng LY, et al. Efficacy and safety of neoadjuvant immunotherapy in resectable nonsmall cell lung cancer: a meta-analysis. Lung Cancer. 2020;147:143–153.
88. Necchi A, Anichini A, Raggi D, et al. Pembrolizumab as neoadjuvant therapy before radical cystectomy in patients with muscle-invasive urothelial bladder carcinoma (PURE-01): an open-label, single-arm, phase II study. J Clin Oncol. 2018;36(34):3353–3360.
89. van Dijk N, Gil-Jimenez A, Silina K, et al. Preoperative ipilimumab plus nivolumab in locoregionally advanced urothelial cancer: the NABUCCO trial. Nat Med. 2020;26(12):1839–1844.
90. Pinato DJ, Cortellini A, Sukumaran A, et al. PRIME-HCC: phase Ib study of neoadjuvant ipilimumab and nivolumab prior to liver resection for hepatocellular carcinoma. BMC Cancer. 2021;21(1):301.
91. Woei AJF, Weijl NI, Burgmans MC, et al. Neoadjuvant treatment with angiogenesis-inhibitor dovitinib prior to local therapy in hepatocellular carcinoma: a phase II study. Oncologist. 2021;26(10):854–864.
92. Löffler MW, Gori S, Izzo F, et al. Phase I/II multicenter trial of a novel therapeutic cancer vaccine, HepaVac-101, for hepatocellular carcinoma. Clin Cancer Res. 2022;28(12):2555–2566.
93. Kelley RK, Ryoo BY, Merle P, et al. Second-line cabozantinib after sorafenib treatment for advanced hepatocellular carcinoma: a subgroup analysis of the phase 3 CELESTIAL trial. ESMO Open. 2020;5(4):1.
94. Masatoshi Kudo AM, Santoro A, Melero I, et al. Checkmate-040: nivolumab (NIVO) in patients (pts) with advanced hepatocellular carcinoma (aHCC) and Child-Pugh B (CPB) status. J Clin Oncol. 2019;37(4_suppl):327.
95. Ha J, Yan M, Aguilar M, et al. Race/ethnicity-specific disparities in cancer incidence, burden of disease, and overall survival among patients with hepatocellular carcinoma in the United States. Cancer. 2016;122(16):2512–2523.
96. Xu L, Kim Y, Spolverato G, Gani F, Pawlik TM. Racial disparities in treatment and survival of patients with hepatocellular carcinoma in the United States. Hepatobiliary Surg Nutr. 2016;5(1):43–52.
97. Mathur AK, Osborne NH, Lynch RJ, Ghaferi AA, Dimick JB, Sonnenday CJ. Racial/ethnic disparities in access to care and survival for patients with early-stage hepatocellular carcinoma. Arch Surg. 2010;145(12):1158–1163.
98. Gilligan AM, Alberts DS, Roe DJ, Skrepnek GH. Death or debt? National estimates of financial toxicity in persons with newly-diagnosed cancer. Am J Med. 2018;131(10):1187–1199.e1185.
99. Kim DW, Talati C, Kim R. Hepatocellular carcinoma (HCC): beyond sorafenib-chemotherapy. J Gastrointest Oncol. 2017;8(2):256–265.
100. Tang W, Chen Z, Zhang W, et al. The mechanisms of sorafenib resistance in hepatocellular carcinoma: theoretical basis and therapeutic aspects. Signal Transduct Target Ther. 2020;5(1):87.
101. Cabral LKD, Tiribelli C, Sukowati CHC. Sorafenib resistance in hepatocellular carcinoma: the relevance of genetic heterogeneity. Cancers. 2020;12(6):1576. doi:10.3390/cancers12061576
102. Chan SL, Mo F, Johnson PJ, et al. Performance of serum α-fetoprotein levels in the diagnosis of hepatocellular carcinoma in patients with a hepatic mass. HPB. 2014;16(4):366–372. doi:10.1111/hpb.12146
103. Sangro B, Melero I, Wadhawan S, et al. Association of inflammatory biomarkers with clinical outcomes in nivolumab-treated patients with advanced hepatocellular carcinoma. J Hepatol. 2020;73(6):1460–1469. doi:10.1016/j.jhep.2020.07.026
104. Zhu AX, Finn RS, Edeline J, et al. Pembrolizumab in patients with advanced hepatocellular carcinoma previously treated with sorafenib (KEYNOTE-224): a non-randomised, open-label phase 2 trial. Lancet Oncol. 2018;19(7):940–952. doi:10.1016/S1470-2045(18)30351-6
105. Brunetti O, Gnoni A, Licchetta A, et al. Predictive and prognostic factors in HCC patients treated with sorafenib. Medicina. 2019;55(10):707. doi:10.3390/medicina55100707
106. Cai H, Zhang Y, Zhang H, Cui C, Li C, Lu S. Prognostic role of tumor mutation burden in hepatocellular carcinoma after radical hepatectomy. J Surg Oncol. 2020;121(6):1007–1014. doi:10.1002/jso.25859
107. Finn RS, Kudo M, Cheng AL, et al. Pharmacodynamic biomarkers predictive of survival benefit with lenvatinib in unresectable hepatocellular carcinoma: from the phase III REFLECT study. Clin Cancer Res. 2021;27(17):4848–4858. doi:10.1158/1078-0432.CCR-20-4219
108. Shrestha R, Prithviraj P, Anaka M, et al. Monitoring immune checkpoint regulators as predictive biomarkers in hepatocellular carcinoma. Front Oncol. 2018;8:269. doi:10.3389/fonc.2018.00269
109. Wong M, Kim JT, Cox B, et al. Evaluation of tumor mutational burden in small early hepatocellular carcinoma and progressed hepatocellular carcinoma. Hepat Oncol. 2021;8(4):Hep39. doi:10.2217/hep-2020-0034
110. Ren Z, Li A, Jiang J, et al. Gut microbiome analysis as a tool towards targeted non-invasive biomarkers for early hepatocellular carcinoma. Gut. 2019;68(6):1014–1023. doi:10.1136/gutjnl-2017-315084
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.