")
Back to Journals » Journal of Pain Research » Volume 17
Expert Consensus on Ion Channel Drugs for Chronic Pain Treatment in China
Authors Ma K, Cheng Z, Jiang H, Lin Z, Liu C, Liu X , Lu L, Lu Y , Tao W, Wang S, Yang X, Yi Q, Zhang X, Zhang Y, Liu Y
Received 17 October 2023
Accepted for publication 22 January 2024
Published 8 March 2024 Volume 2024:17 Pages 953—963
DOI https://doi.org/10.2147/JPR.S445171
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Robert Twillman
Ke Ma,1,* Zhixiang Cheng,2,* Hao Jiang,3,* Zhangya Lin,4,* Chuansheng Liu,5,* Xianguo Liu,6,* Lijuan Lu,7,* Yan Lu,8,* Wei Tao,9,* Suoliang Wang,10,* Xiaoqiu Yang,11,* Qishan Yi,12,* Xiaomei Zhang,13,* Ying Zhang,14,* Yanqing Liu15,*
1Department of Algology, Xinhua Hospital Affiliated to Shanghai Jiao Tong University School of Medicine, Shanghai, People’s Republic of China; 2Department of Algology, The Second Affiliated Hospital of Nanjing Medical University, Nanjing, People’s Republic of China; 3Department of Algology, The First Affiliated Hospital of Fujian Medical University, Fuzhou, People’s Republic of China; 4Department of Neurosurgery, The First Affiliated Hospital of Fujian Medical University, Fuzhou, People’s Republic of China; 5Department of Algology, The Affiliated Hospital of Qingdao University, Qingdao, People’s Republic of China; 6Pain Research Center, Zhongshan School of Medicine, Sun Yat-Sen University, Guangzhou, People’s Republic of China; 7Department of Pain Medicine, Nanjing Drum Tower Hospital, The Affiliated Hospital of Nanjing University Medical School, Nanjing, People’s Republic of China; 8Department of Algology, Xijing Hospital, The Fourth Military Medical University, Xian, People’s Republic of China; 9Department of Neurosurgery, Shenzhen University General Hospital, Shenzhen, People’s Republic of China; 10Department of Algology, The First Affiliated Hospital, Xi’an Jiaotong University, Xi’an, People’s Republic of China; 11Department of Algology, The First Affiliated Hospital of Chongqing Medical University, Chongqing, People’s Republic of China; 12Department of Algology, The Yibin First People’s Hospital Affiliated Chongqing Medical University, Yibin, People’s Republic of China; 13Department of Algology, The First Affiliated Hospital of Kunming Medical University, Kunming, People’s Republic of China; 14Department of Algology. Hospital (T.C.M) Affiliated to Southwest Medical University, Luzhou, People’s Republic of China; 15Department of Algology, Beijing Tiantan Hospital, Capital Medical University, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ke Ma, Department of Algology, Xinhua Hospital Affiliated to Shanghai Jiao Tong University school of medicine, Shanghai, 200092, People’s Republic of China, Tel +86133618792160, Email [email protected] Yanqing Liu, Department of Algology, Beijing Tiantan Hospital, Capital Medical University, Beijing, 100070, People’s Republic of China, Tel +8618601203409, Email [email protected]
Abstract: Ion channel drugs have been increasing used for chronic pain management with progress in the development of selective calcium channel modulators. Although ion channel drugs have been proven safe and effective in clinical practice, uncertainty remains regarding its use to treat chronic pain. To standardize the clinical practice of ion channel drug for the treatment of chronic pain, the National Health Commission Capacity Building and Continuing Education Center for Pain Diagnosis and Treatment Special Ability Training Project established an expert group to form an expert consensus on the use of ion channel drugs for the treatment of chronic pain after repeated discussions on existing medical evidence combined with the well clinical experience of experts. The consensus provided information on the mechanism of action of ion channel drugs and their recommendations, caution use, contraindications, and precautions for their use in special populations to support doctors in their clinical decision-making.
Keywords: chronic pain, ion channel drugs, voltage-gated calcium channels, voltage-gated sodium channel
Introduction
Chronic pain is defined as pain that persists for ≥3 months. The International Society for Pain (IASP) classifies chronic pain into two categories: chronic primary and secondary pain syndromes.1 Currently, there is relatively few epidemiological data regarding the prevalence of chronic pain according to the IASP classification in the 11th edition of the International Classification of Diseases (ICD-11). In 2019, Wang et al2 conducted a preliminary survey of 1545 patients with chronic pain according to the IASP ICD-11 chronic pain classification in five tertiary general hospitals in three provinces and four regions in China and found that the proportion of chronic secondary pain syndrome was as high as 98.64% (1524 cases), while primary pain only accounted for 1.36% (21 cases). Among them, the population with chronic secondary pain syndrome included 32.87% (501) patients with chronic neuropathic pain, 29.20% (445) with chronic secondary headache or maxillofacial pain, 22.57% (344) with chronic secondary musculoskeletal pain, 11.55% (176) with chronic secondary visceral pain, 2.10% (32) with chronic cancer-related pain, and 1.71% (26) with chronic postoperative or posttraumatic pain.
Drugs are the primary treatment modality for chronic pain.3 At present, besides traditional non-steroidal analgesics and opioids, ion channel drugs have been increasing used for chronic pain management with progress in the development of selective calcium channel modulators, state-dependent sodium channel antagonists, and similar drugs.4–6 Recent studies have revealed that abnormal expression of voltage-dependent ion channels plays a key role in peripheral sensitivity, central sensitivity, and neuroplastic changes in chronic pain.7,8 Ion channel drugs could inhibit the peripheral sensitization and central sensitization to alleviate chronic pain. Although ion channel drugs have been proven safe and effective in clinical practice, uncertainty remains regarding its use to treat chronic pain. To date, there have been no reference standards to guide clinical practice and no relevant expert consensus on this product, in China. In this context, we invited experts in basic and clinical medicine of pain management to develop a Chinese expert consensus and provide a reference for the standard application of ion channel drugs in chronic pain.
A panel of 15 Chinese pain medicine experts was organized by the National Health Commission Capacity Building and Continuing Education Center for Pain Diagnosis and Treatment Special Ability Training Project and a consensus meeting was held online on 20/08/2022. PubMed/MEDLINE, Embase, Cochrane, CNKI, and Wanfang electronic databases were searched to identify related publications, including systematic reviews, meta-analyses, randomized and non-randomized controlled trials, observational cohort studies, and case studies published in English and Chinese. Based on this evidence and clinical experience, the experts reached a consensus on the recommendations. For the quality and strength of evidence, the grading of recommendations, assessment, development, and evaluation (GRADE) system was used. For recommendation grading, the quality of evidence, clinical benefits and harm, cost, patient preference, and value were considered.
Mechanism of Ion Channel Drugs
Multiple complex pathophysiological mechanisms are responsible for the development and progression of chronic pain. Chronic pain can cause changes in the synaptic plasticity in the cerebral cortex, leading to augmented pain transmission. Peripheral and central sensitizations are major causes of hypersensitivity in patients and may initially be triggered by peripheral nerve injury and inflammation.9 A reduction in the activation threshold of sensing channels induced by nerve injury, including changes in sodium and calcium ion channels, is an important mechanism that leads to peripheral sensitization.10 The dorsal root ganglion (DRG) expresses a variety of ion channel proteins, such as sodium and calcium. After neuronal injury, a series of functional and density changes in voltage-dependent sodium and calcium channels occur on the membrane of DRG neurons, resulting in a large number of abnormal action potentials in this area, which is one of the mechanisms that cause chronic pain.11
Altered N-type voltage-gated calcium channel (VGCC) function in sensory neurons has been implicated in one of these mechanisms. N-type VGCCs contribute significantly to the synaptic transmission of pain signals in DRG neurons and play major roles in pain information processing by controlling neurotransmitter release from nociceptive nerve fibers and modulating synaptic plasticity at the first synapse of the nociceptive pathways.12 VGCC opens when the body is subjected to noxious stimulation or nerve injury, and a large Ca2+ influx activates protein kinase C (PKC, an intracellular second messenger that plays an important role in the transmission of noxious stimuli), promoting the occurrence and development of pain. Calcium channel modulators inhibit the influx of calcium ions and reduce the release of neurotransmitters, thereby reducing the abnormal excitation of pain transduction pathways to achieve pain relief.13 Gabapentin and pregabalin are the most frequently prescribed calcium channel modulators for neuropathic pain. Gabapentin interacts with subunits α2δ of the VGCC, which are mainly located in the neocortex, hippocampus, amygdala, and spinal cord. Gabapentin was first used for the treatment of epilepsy and is now used for treating neuropathic pain. Pregabalin is a new-generation drug based on gabapentin that has been approved for the treatment of diabetic peripheral and postherpetic neuralgia.
The voltage-gated Na + channel (VGSC) is a microporous transmembrane protein that is widely distributed on the membranes of excitable cells, such as neurons, and is mainly responsible for the transmembrane transport of Na +. VGSCs play a key role in the initiation and propagation of electrical signaling in excitable cells.14,15 VGSCs consist of pore-forming and auxiliary subunits. Nociceptors express multiple subtypes of α-subunits. Tissue and nerve damage leads to changes in the expression and function of α-subunits that in turn can lead to changes in the excitability of sensory neurons. Changes in the excitability of sensory neurons are thought to underlie chronic pain conditions.16 To date, at least nine distinct sodium channel isoforms have been detected in the nervous system, and the sodium channel subtypes Nav1.3, Nav1.7, Nav1.8, and Nav1.9 are associated with various pain states.17 They are useful analgesic drug targets for various types of pain, including neuropathic pain. Sodium channel blockers include carbamazepine, lidocaine, and bulleyaconitine A (BLA). They block different types of voltage-dependent sodium channels and inhibit overexcited sensory neurons.
Ion Channel Drugs in the Treatment of Chronic Pain Diseases
Chronic Neuropathic Pain
Postherpetic Neuralgia
Postherpetic neuralgia (PHN) is the most common type of neuropathic pain, defined as pain lasting ≥1 month after Herpes Zoster (HZ) onset or healing, and is the most common complication of HZ. Meta-analysis data show that the annual incidence of PHN in the population ranges from 3.9 to 42.0/100,000, with PHN occurring in 9–34% of patients with HZ. At present, it is believed that peripheral sensitization and central sensitization are important mechanisms of PHN, and the up-regulation of voltage-gated calcium channel α2-δ subunit and sodium channel is the main reason for central sensitization.18,19 Therefore, ion-channel drugs can be used as treatment options for patients with PHN. Compared with oral administration, topical administration can directly act on the target with better tolerance and compliance and fewer adverse gastrointestinal tract reactions.20 The therapeutic status of ion channel drugs (gabapentin, pregabalin, and lidocaine plaster) in PHN has been clarified by the expert consensus.21–23
Recommendations: Calcium channel modulators (pregabalin and gabapentin) are first-line drugs for the treatment of PHN. In addition, 5% lidocaine patches can also be used as a first-line treatment, especially for patients who have difficulties in oral medications, such as those with dysphagia, since lidocaine has less systemic absorption, does not require dose adjustment, and is more convenient to use. Alternatively, carbamazepine is also effective in the treatment of PHN; however, the evidence for its use is limited, and its combination with other drugs is recommended. Although BLA has been recommended for the treatment of PHN, no large randomized controlled clinical studies have been conducted.
A systematic review24 evaluated the analgesic effects of pregabalin in patients with PHN. A total of 2192 patients from seven clinical studies were included (pregabalin group = 1381, control group, 811). Pregabalin was associated with a higher percentage of 30% and 50% of pain responders, respectively, than the controls (P<0.05). Meanwhile, the pregabalin group had lower sleep interference scores and better PGIC scores compared to the control group (P<0.05). Another systematic review25 evaluated the analgesic effects of gabapentin on patients with PHN. Seven trials involving 2039 participants were identified. A pooled analysis showed that gabapentin significantly reduced PHN-related pain compared with the placebo (P<0.001). Gabapentin is an effective and well-tolerated treatment for PHN. Lidocaine-medicated plaster in single or combined regimens can help relieve PHN pain and improve quality of life and sleep. A two-stage adaptive, randomized, open-label, multicenter, non-inferiority study26 compared the efficacy and safety of 5% lidocaine-medicated plaster with pregabalin in 96 patients with PHN and reported that 5% lidocaine-medicated plaster is comparable to pregabalin in terms of pain relief in PHN but is better tolerated and has fewer adverse effects than pregabalin (Table 1). In patients with refractory PHN, nerve block therapy combined with lidocaine external plasters can be considered to improve the therapeutic effect.27 Studies have shown that carbamazepine combined with other drugs has good efficacy in the treatment of PHN (Table 1). A randomized controlled clinical study28 evaluated the clinical efficacy and safety of pregabalin combined with carbamazepine in 114 patients with PHN. The results showed that the visual analogue scale (VAS) score significantly decreased in the three groups after treatment (P<0.05) (carbamazepine, pregabalin, and combination groups), and the VAS score in the combination group was significantly lower than that in the other groups (P<0.05) (Table 1). According to a Chinese expert consensus18 on PHN, BLA has also been used to treat PHN. However, there are only a few reports on the use of BLA in the treatment of PHN. Nevertheless, evidence from large-scale clinical trials is limited. In patients with HZ pain, combination treatment with BLA is recommended to prevent PHN.
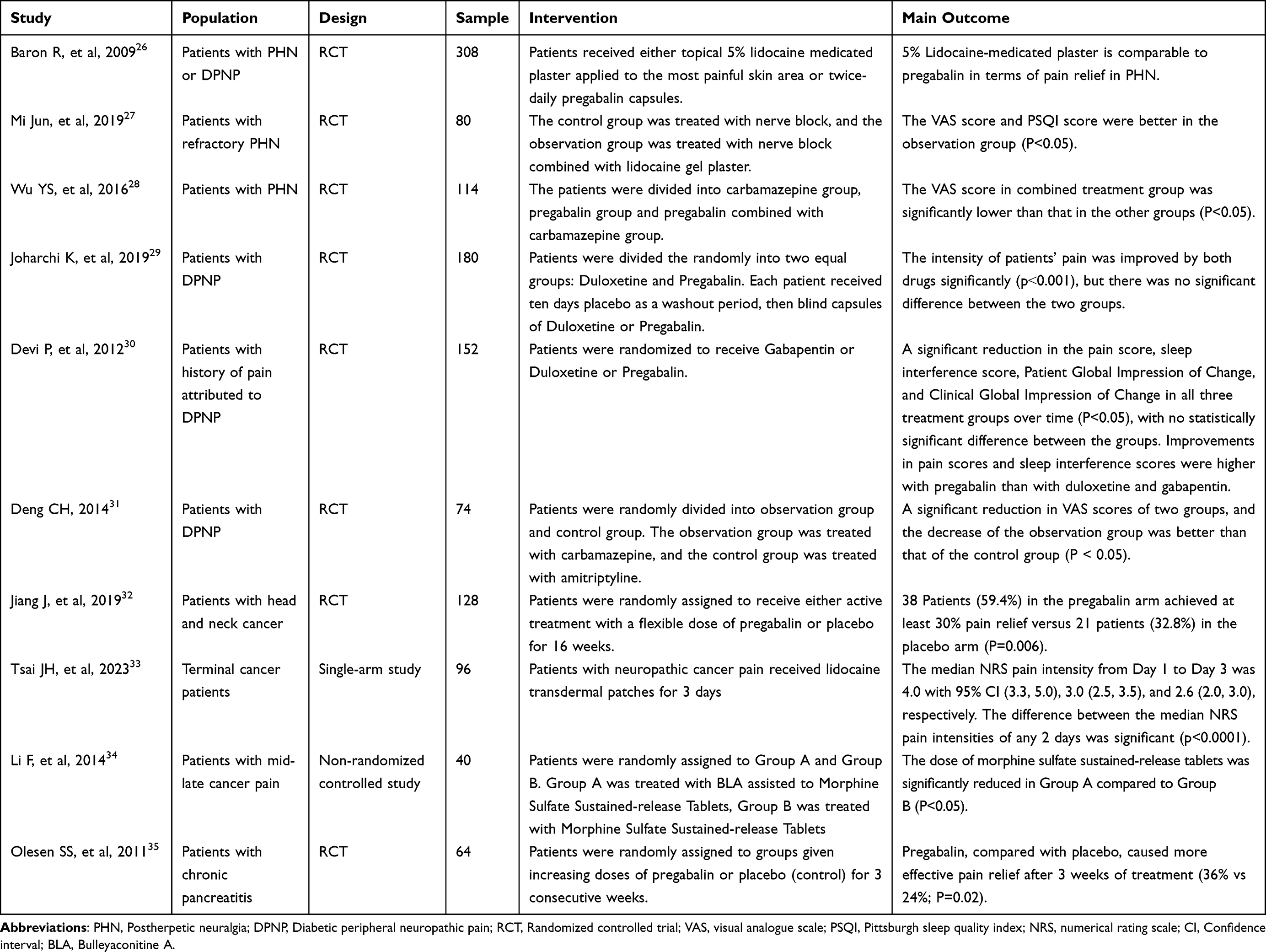 |
Table 1 The Relatively High-Quality Clinical Studies of Ion Channel Drugs in Chronic Pain |
Diabetic Peripheral Neuropathic Pain
Diabetic peripheral neuropathic pain (DPNP) is peripheral neuropathic pain caused by diabetes or prediabetes. The general manifestation is symmetrical peripheral neuropathic pain mainly involving the distal extremities, which may also manifest as non-neuralgic pain or neuralgia in the brachial or lumbosacral plexus.36 The prevalence of DPNP is 10–26%.37–39 More than 70% of patients with DPNP have moderate to severe persistent pain, insomnia, poor quality of life, and mood disturbances, resulting in a 5-fold increase in medical costs compared to patients with diabetes.40–42 Peripheral sensitization, central sensitization, and ion channel changes are the main pathogenesis of DPNP, and the high expression of α2-δ subunits on calcium ion channels is the main reason for central sensitization.43 The therapeutic status of ion channel drugs (gabapentin, pregabalin, lidocaine plaster) in DPNP has been clarified in the multiple expert consensus.21,36,44
Recommendations: Calcium channel modulators (gabapentin and pregabalin) are recommended for the treatment of DPNP. For patients who have difficulty taking oral medications, the use of a lidocaine patch is recommended for the treatment of DPNP. Carbamazepine is recommended for DPNP treatment. The sodium channel antagonist, BLA, can also be used to treat DPNP; however, no large randomized controlled clinical studies have been conducted.
A double-blind randomized clinical trial conducted by Joharchi K29 included 180 patients with DPNP to evaluate the efficacy and safety of duloxetine and pregabalin. The results showed that the intensity of pain was significantly improved by both drugs significantly (p˂0.001), with no significant difference between the two groups (Table 1). However, in the duloxetine and pregabalin groups, 74% and 37% of patients, respectively, reported adverse drug reactions (ADRs). The discontinuation rates owing to ADRs were 19% and 7%, respectively. Accordingly, despite having the same efficacy, pregabalin was better tolerated than duloxetine. Another prospective randomized open-label study conducted by Devi P30 included 152 patients with DPNP and compared the efficacy and safety of gabapentin, duloxetine, and pregabalin in patients with DPNP. The results showed a significant reduction in the VAS score, sleep interference score, Patient Global Impression of Change, and Clinical Global Impression of Change in all three treatment groups over time (P<0.05), with no statistically significant difference between the groups. Improvements in VAS scores and sleep interference scores were higher with pregabalin than with duloxetine and gabapentin (Table 1). A network meta-analysis comparing 5% lidocaine plaster with other related agents for DPNP pain relief showed that 5% lidocaine plaster provided comparable pain relief to amitriptyline, capsaicin, gabapentin, and pregabalin and that topical agents had fewer adverse effects than systemic agents.45 A randomized controlled clinical study conducted by Deng31 included 74 patients with DPNP and evaluated the clinical efficacy of carbamazepine in the treatment of DPNP. The results showed that the VAS scores significantly decreased after carbamazepine treatment (Table 1). Previous studies using BLA acupuncture point injection in the treatment of DPNP, showed that the physical pain of the total effective rate was 84%.46
Chronic Postsurgical or Posttraumatic Pain
The incidence of postoperative chronic pain ranges from 5–85% and varies greatly depending on the type of surgery. The incidence of phantom limb pain after amputation is 30–85%, after lumbar surgery is 10–40%, and after multiple traumas is 46–85%.47 Central or peripheral pain sensitization is the main pathogenesis of postoperative chronic pain, and the high expression of α2-δ subunits on calcium ion channels is the main reason for central sensitization.43 The therapeutic status of calcium ion channel drugs (gabapentin and pregabalin) in chronic postoperative or posttraumatic pain has been clarified in the multiple clinical practice guidelines and expert consensus.48–50
Recommendations: Gabapentin and pregabalin are recommended in combination with conventional analgesics for patients with chronic pain after surgery or trauma.
Eight studies were included in a meta-analysis, in which six gabapentin trials demonstrated a moderate-to-large reduction in the development of chronic postsurgical pain (pooled OR 0.52; 95% CI, 0.27 to 0.98; P = 0.04), and two pregabalin trials found a significantly large reduction in the development of chronic postsurgical pain (pooled OR 0.09; 95% CI, 0.02 to 0.79; P = 0.007).51 After including 55 studies, a meta-regression was performed to assess the impact of individual doses and frequency of pregabalin administration on analgesic efficacy. When all doses and administration regimens were combined, pregabalin was associated with a significant reduction in pain scores at rest and during movement and opioid consumption at 24h compared with placebo {mean difference [95% confidence interval (CI)]= −0.38 (−0.57, −0.20), −0.47 (−0.76, −0.18), and −8.27 mg morphine equivalents (−10.08, −6.47), respectively}.52
Chronic Musculoskeletal Pain (CMP)
CMP refers to pain that occurs in the muscles, bones, joints, tendons, or soft tissues for > 3 months. The incidence of CMP increases annually, leading to pain and disability in older adults.53 Lower back pain is the most common type of CMP, with an incidence of 30–40% in adults.54 Central and peripheral sensitization are the main pathogens of CMP along with the abnormal opening of gated sodium and calcium channels and decreased regulatory ability of the spinal cord and central nervous system. The therapeutic status of calcium ion channel drugs (gabapentin, pregabalin) and sodium ion channel drugs (lidocaine) in chronic postoperative or posttraumatic pain has been clarified in the multiple expert consensus.53,55
Recommendations: Pharmacological treatment with anti-inflammatory drugs (NSAIDs) should be considered as the first-line therapy for patients with CMP. Ion-channel drugs can be added to or replaced to NSAIDs in patients who do not respond well or have contraindications (gastrointestinal and cardiovascular diseases). Moreover, they may be preferred in patients with marked central or peripheral sensitization. Gabapentin and pregabalin are recommended for chronic neuropathic limb pain; whereas, gabapentin is recommended for chronic lower back pain. Lidocaine plaster is recommended for treating chronic low back pain and neuropathic limb pain. BLA is recommended for the treatment of pain in the joints and soft tissues of the extremities, neck, shoulder, waist, and leg caused by intervertebral disc disease and for pain in patients with rheumatic immune diseases.
A systematic review of 15 trials (1468 participants) on pharmacotherapy for chronic pain found that gabapentin was more efficacious than the placebo (42% vs 19%) in decreasing chronic pain by 50% in patients with neuropathic pain, phantom limb pain, spinal cord injury, and other neuropathies. Lidocaine plasters block gated sodium channel transmission in nociceptors at the peripheral level. Plasters may have modest efficacy in the management of chronic pain secondary to LBP and various neuropathies.56 An open, single-arm clinical study conducted by Liu57 et al included 200 patients with chronic pain and evaluated the treatment of joint pain; soft tissue pain; and chronic pain of the neck, shoulder, waist, and leg caused by intervertebral disc lesions using BLA. The results showed that the total effective rate for joint and soft tissue pain was 80%. The total efficacy rate was 81%, and the VAS score was significantly lower after 1–4 weeks of treatment. BLA have dual pharmacological effects on central and peripheral analgesia, as well as immunoregulatory effects. Several clinical studies have shown that BLA have good clinical efficacy in treating osteoarthritis (OA), rheumatoid arthritis (RA), and knee osteoarthritis and can significantly reduce the VAS score.58–61
Chronic Cancer-Related Pain
Cancer-related pain refers to pain caused by direct aggression or indirect action of the cancer itself and various anti-tumor treatments, as well as pain due to other complications and non-tumor factors such as psychosocial factors.62 The treatment of cancer pain is often based on the principle of indirect action.63 Ion channel drugs can increase the analgesic effect of opioids, reduce the dose of opioids, and can be used for cancer-related neuropathological pain treatment and complementary treatment.64,65
Recommendations: Gabapentin, pregabalin, lidocaine, and BLA can be used for the treatment and adjuvant therapy of cancer-related neuropathic pain and can increase the analgesic effect of opioids and reduce the dose of opioids.
This randomized double-blind study included 128 patients to test the efficacy and safety of pregabalin versus placebo for the treatment of radiotherapy-related neuropathic pain. 38 Patients (59.4%) in the pregabalin arm achieved at least 30% pain relief versus 21 patients (32.8%) in the placebo arm (P=0.006)32 (Table 1). A systematic review of 10 studies identified articles on the use of prophylactic gabapentin in patients undergoing head and neck cancer therapy. Prophylactic gabapentin appears to be a promising treatment option for preventing pain, reducing opioid use, and reducing weight loss in patients undergoing head and neck cancer therapy.66 In a prospective, open-label, single-arm study, 5% lidocaine transdermal patches reduced the numerical rating scale (NRS) pain intensity in patients with neuropathic cancer already receiving opioid treatment33 (Table 1). Li34 et al used BLA capsules combined with morphine sulfate sustained-release tablets to treat advanced cancer. The results showed that when satisfactory analgesia was achieved (VAS<3), the dose of morphine sulfate sustained-release tablets was significantly reduced in combination with BLA compared to morphine sulfate sustained-release tablets alone (P<0.05) (Table 1).
Chronic Visceral Pain (CVP)
CVP is one of the most common forms of pain reported clinically in chronic pain with an incidence of up to 20%. Visceral pain refers to pain in the body’s internal organs and is often associated with various diseases such as acute and chronic pancreatitis and functional gastrointestinal diseases such as irritable bowel syndrome (IBS). Adjunctive drugs should be introduced during the early stages of pain management in the presence of central sensitization (hyperalgesia and allodynia). Currently, the main clinical applications are ion channel drugs.67,68
Recommendations: Gabapentin, pregabalin, and BLA are recommended as adjuvant analgesics in CVP treatment.
Both gabapentin and pregabalin have been demonstrated to reduce pain in patients with chronic pancreatitis and IBS.69–71 In a randomized controlled trial, adjuvant pregabalin resulted in more effective pain relief at 3 weeks and was associated with improved health status in patients with chronic pancreatitis compared to placebo35 (Table 1). BLA has been demonstrated to reduce pain in patients with CVP and IBS.72,73
Caution Use and Contraindications of Ion Channel Drugs
Use with Caution
Coronary artery disease or other cardiac impairments (except heart block), hypovolemia, or shock. Patients with liver and kidney dysfunction, chronic obstructive pulmonary disease, blood system adverse reaction history, diabetes, endocrine disorders, psychiatric history, newborns, premature infants, the elderly, and infirmities.
Contraindications
Patients who are allergic to ion channel drugs along with acute cardiogenic cerebral ischemic syndrome (A-S syndrome), pre-excitation syndrome, heart block (including sinoatrial, atrioventricular, and intraventricular conduction blocks), lactating women, patients with a history of myelopathic depression, patients with severe abnormal serum iron, patients with a history of hepatic porphyria, patients with severe hepatic insufficiency, and patients with acute pancreatitis should not be prescribed ion channel drugs.
Adverse Reactions and Treatment Principles of Ion Channel Drugs
Carbamazepine
Common side effects include blurred vision, dizziness, fatigue, nausea, and vomiting, which mostly occur 1–2 weeks after the treatment. Rashes, urticaria, liver dysfunction, and hypothyroidism are rare. Granulocytopenia, bone marrow suppression, arrhythmia, and liver and kidney failures are rare complications. Carbamazepine has a narrow therapeutic window and is associated with multiple adverse systemic reactions. Carbamazepine causes Stevens–Johnson syndrome (SJS), toxic epidermal necrolysis, and other serious diseases that are highly correlated with the variant alleles HLA-B *15:02 and LA-A*31:01 carried by patients.74 Special attention should also be paid to hyperalgesia caused by carbamazepine withdrawal.4
Oxcarbazepine
The most common adverse effects were rash, dizziness, headache, and drowsiness. The total incidence of adverse effects was 45.22%, most of which were mild and alleviated or disappeared after 3–4 weeks. Oxcarbazepine can also cause a severe rash, such as life-threatening SJS and toxic epidermal necrolysis, with a lower incidence than carbamazepine (1 to 6/10,000 for carbamazepine vs 0.5 to 6/1,000,000 for oxcarbazepine).75 During treatment, it is necessary to monitor for signs of depression, suicidal thoughts, or abnormal behavioral and mood changes.76
Lidocaine Plaster
The side effects of 5% lidocaine plaster include moderate skin reactions, such as erythema and rash. The use of lidocaine plasters should be avoided in patients taking oral class I antiarrhythmic drugs, such as mexiletine, and in patients with severe liver impairment. Intravenous lidocaine should be administered in an environment that includes monitoring and rescue conditions. Additionally, the concentration, total amount, and infusion speed of the drug should be strictly controlled. Patients who are allergic to amide local anesthetics or other ingredients in the product are contraindicated.
BlA
No drug tolerance, addiction, or adverse gastrointestinal effects were observed. Very few patients experienced transient mild palpitations, nausea, lip numbness, or palpitations. The response is transient and can be relieved after treatment.77 The interval between the two administrations of BLA should not be < 6h. BLA should also be used with caution in patients with heart diseases, such as arrhythmia.
Gabapentin
Common adverse effects include dizziness, drowsiness, ataxia, and peripheral edema. The symptoms of withdrawal include disturbances of consciousness, disorientation, non-specific gastrointestinal reactions, hyperhidrosis, and tremors. Gabapentin dosage should be adjusted according to the patient’s renal function. During the medication period, the withdrawal of gabapentin or the addition of a new treatment plan should be gradually carried out, and the time should be at least 1 week. The plasma concentration of gabapentin may increase in patients treated with morphine at the same time.78 Even if gabapentin was administered per the prescribed dosage, the reaction rate was reduced. Therefore, individuals engaged in driving and manipulating complex machinery should use them cautiously.
Pregabalin
The adverse effects include dizziness, somnolence, ataxia, headaches, language barriers, and tremors. Pregabalin can cause peripheral edema and a prolonged PR interval and should be used with caution in patients with congestive heart failure and heart function grade III or IV. Adverse endocrine effects include an increase in body weight, with an occurrence rate of 4% to 12%. Muscular skeletal adverse effects include elevated creatine kinase levels, myoclonus, and stripe muscle dissolution. Pregabalin treatment occasionally causes mild transient increases in liver enzymes, saliva deficiency, constipation, thrombocytopenia, blurred vision, diplopia, and amblyopia.79 The pregabalin dosage needs to be adjusted according to the patient’s renal function. During treatment, it is necessary to monitor for signs of depression, suicidal thoughts, or abnormal behavioral and mood changes.76
Gabapentin and pregabalin are addictive, and sudden withdrawal increases the frequency of seizures and produces withdrawal symptoms, such as nausea, headache, and diarrhea. Therefore, when discontinuing the drug, the dosage should be gradually reduced for at least 1 week.
The Precautions of Ion Channel Drugs in Special Populations
Precautions for Children
Most ion-channel drugs can be used in children; however, pregabalin is not suitable for patients <17 years of age. BLA has not yet been tested as a medication in children, so it should be used with caution in children. Although hypothyroidism is a rare adverse reaction to oxcarbazepine, children <2 years of age should undergo a Meth test before initiation of oxcarbazepine treatment.80
Precautions for Pregnancy and Lactation
This drug is not suitable for pregnant women because it can be secreted through breast milk, and therefore, it is contraindicated in lactating women. Additionally, simultaneous use of oxcarbazepine and oral hormonal contraceptives is associated with contraceptive failure.81
Precautions for Elderly People
Elderly individuals can selectively use ion-channel drugs according to their liver and kidney function. However, elderly patients are more sensitive to carbamazepine because it frequently causes cognitive impairment, anxiety, confusion, atrioventricular block, and aplastic anemia. Accordingly, these drugs need to be carefully selected.80,81 BLA has not been tested as a medication for the elderly; therefore, it should be used with caution.
Conclusion
Based on the existing medical evidence and experts’ clinical experience, this consensus put forward suggestions regarding the use of ion channel drugs for the treatment of chronic pain, such as pregabalin, gabapentin, lidocaine patch, carbamazepine and BLA. At present, there is relatively abundant evidence for gabapentin, pregabalin, and lidocaine patch in the treatment of chronic pain. However, the evidence for carbamazepine and BLA is relatively limited. It is hoped that this consensus will support doctors in their clinical decision-making.
Acknowledgments
The authors thank the support of KPC Pharmaceuticals, Inc.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by National Natural Science Foundation of China (peripheral mechanism of Mrgprd regulating opioid tolerance by a specific lncRNA in the dorsal root ganglion) (NSFC-82371224).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Treede RD, Rief W, Barke A, et al. Chronic pain as a symptom or a disease: the IASP classification of chronic pain for the International Classification of Diseases (ICD-11). Pain. 2019;160(1):19–27. doi:10.1097/j.pain.0000000000001384
2. Wang JL, Zhang WJ, Luo WJ, et al. Investigation on the status quo of patients in pain department in some areas based on ICD-11 chronic pain classification. Chin J Pain Med. 2019;25(4):267–275.
3. Yamamoto PA, Conchon Costa AC, Lauretti GR, et al. Pharmacogenomics in chronic pain therapy: from disease to treatment and challenges for clinical practice. Pharmacogenomics. 2019;20(13):971–982. doi:10.2217/pgs-2019-0066
4. Rogers M, Tang L, Madge DJ, et al. The role of sodium channels in neuropathic pain. Semin Cell Dev Biol. 2006;17(5):571–581. doi:10.1016/j.semcdb.2006.10.009
5. Markman JD, Dworkin RH. Ion channel targets and treatment efficacy in neuropathic pain. J Pain. 2006;7(Suppl 1):S38–47. doi:10.1016/j.jpain.2005.09.008
6. Skerratt SE, West CW. Ion channel therapeutics for pain. Channels. 2015;9(6):344–351. doi:10.1080/19336950.2015.1075105
7. De Logu F, Geppetti P. Ion channel pharmacology for pain modulation. Handb Exp Pharmacol. 2019;260:161–186.
8. Bell DC, Dallas ML. Using automated patch clamp electrophysiology platforms in pain-related ion channel research: insights from industry and academia. Br J Pharmacol. 2018;175(12):2312–2321. doi:10.1111/bph.13916
9. Phillips K, Clauw DJ. Central pain mechanisms in chronic pain states--maybe it is all in their head. Best Pract Res Clin Rheumatol. 2011;25(2):141–154. doi:10.1016/j.berh.2011.02.005
10. Tang XP, Jing YL. Observation on the prevention of chronic pain symptoms with sodium ion channel blockers. Chin J Clin Rehabil. 2005;36:190–192.
11. Chen HL, Zhou LL, Hu L, et al. Research progress of neurophysiological mechanism of chronic pain. Chongqing Med. 2021;50(10):1777–1781.
12. Adams DJ, Berecki G. Mechanisms of conotoxin inhibition of N-type (Ca(v)2.2) calcium channels. Biochim Biophys Acta. 2013;1828(7):1619–1628. doi:10.1016/j.bbamem.2013.01.019
13. Chincholkar M. Analgesic mechanisms of gabapentinoids and effects in experimental pain models: a narrative review. Br J Anaesth. 2018;120(6):1315–1334. doi:10.1016/j.bja.2018.02.066
14. Xu L, Ding X, Wang T, et al. Voltage-gated sodium channels: structures, functions, and molecular modeling. Drug Discovery Today. 2019;24(7):1389–1397. doi:10.1016/j.drudis.2019.05.014
15. Hodgkin AL, Huxley AF. Currents carried by sodium and potassium ions through the membrane of the giant axon of Loligo. J Physiol. 1952;116(4):449–472. doi:10.1113/jphysiol.1952.sp004717
16. Nassar MA, Levato A, Stirling LC, et al. Neuropathic pain develops normally in mice lacking both Na(v)1.7 and Na(v)1.8. Mol Pain. 2005;1:24. doi:10.1186/1744-8069-1-24
17. Dib-Hajj SD, Waxman SG. Diversity of composition and function of sodium channels in peripheral sensory neurons. Pain. 2015;156(12):2406–2407. doi:10.1097/j.pain.0000000000000353
18. Yu SY, Wan Y, Wan Q, et al. Chinese expert consensus on the diagnosis and treatment of postherpetic neuralgia. Chin J Pain Med. 2016;22(03):161–167.
19. van Hecke O, Austin SK, Khan RA, et al. Neuropathic pain in the general population: a systematic review of epidemiological studies. Pain. 2014;155(4):654–662. doi:10.1016/j.pain.2013.11.013
20. Stanos SP. Topical agents for the management of muscul oskeletal pain. J Pain Symptom Manage. 2007;33(3):342–355. doi:10.1016/j.jpainsymman.2006.11.005
21. Zhu Q, Fan B, Zhang D, et al. Chinese expert consensus on diagnosis and treatment of peripheral neuropathic pain. Chin J Pain Med. 2020;26(5):321–328.
22. Finnerup NB, Attal N, Haroutounian S, et al. Pharmacotherapy for neuropathic pain in adults: a systematic review and meta-analysis. Lancet Neurol. 2015;14(2):162–173. doi:10.1016/S1474-4422(14)70251-0
23. Kawai K, Gebremeskel BG, Acosta CJ. Systematic review of incidence and complications of herpes zoster: towards a global perspective. BMJ Open. 2014;4(6):e004833. doi:10.1136/bmjopen-2014-004833
24. Wang SL, Wang H, Nie HY, et al. The efficacy of pregabalin for acute pain control in herpetic neuralgia patients: a meta-analysis. Medicine. 2017;96(51):e9167. doi:10.1097/MD.0000000000009167
25. Meng FY, Zhang LC, Liu Y, et al. Efficacy and safety of gabapentin for treatment of postherpetic neuralgia: a meta-analysis of randomized controlled trials. Minerva Anestesiol. 2014;80(5):556–567.
26. Baron R, Mayoral V, Leijon G, et al. 5% lidocaine medicated plaster versus pregabalin in post-herpetic neuralgia and diabetic polyneuropathy: an open-label, non-inferiority two-stage RCT study. Curr Med Res Opin. 2009;25(7):1663–1676. doi:10.1185/03007990903047880
27. Jun M, Lijun H. Effect of nerve block combined with lidocaine gel patch on postherpetic neuralgia. Chin J Med Clin. 2019;21(01):66–68.
28. Wu YS, Fu JM, Dong JJ, et al. Clinical efficacy and safety of pregabalin combined with carbamazepine in the treatment of postherpetic neuralgia. Medical Theory and Practice. 2016;29(24):3326–3328.
29. Joharchi K, Memari M, Azargashb E, et al. Efficacy and safety of duloxetine and Pregabalin in Iranian patients with diabetic peripheral neuropathic pain: a double-blind, randomized clinical trial. J Diabetes Metab Disord. 2019;18(2):575–582. doi:10.1007/s40200-019-00427-w
30. Devi P, Madhu K, Ganapathy B, et al. Evaluation of efficacy and safety of gabapentin, duloxetine, and pregabalin in patients with painful diabetic peripheral neuropathy. Indian J Pharmacol. 2012;44(1):51–56. doi:10.4103/0253-7613.91867
31. Deng CH. Clinical effect of carbamazepine on diabetic painful neuropathy. Mod Diagno Ther. 2014;25(14):3234–3236.
32. Jiang J, Li Y, Shen Q, et al. Effect of pregabalin on radiotherapy-related neuropathic pain in patients with head and neck cancer: a randomized controlled trial. J Clin Oncol. 2019;37(2):135–143. doi:10.1200/JCO.18.00896
33. Tsai JH, Liu IT, Su PF, et al. Lidocaine transdermal patches reduced pain intensity in neuropathic cancer patients already receiving opioid treatment. BMC Palliat Care. 2023;22(1):4. doi:10.1186/s12904-023-01126-3
34. Li F, Ni JX, Wu BS, et al. Clinical study of bulleyaconitine A assisted to morphine sulfate sustained-release tablets in the treatment of mid-late cancer pain. J Changchun Univ Chin Med. 2014;30(3):460–462. doi:10.1007/s11802-014-2123-6
35. Olesen SS, Bouwense SA, Wilder-Smith OH, et al. Pregabalin reduces pain in patients with chronic pancreatitis in a randomized, controlled trial. Gastroenterology. 2011;141(2):536–543. doi:10.1053/j.gastro.2011.04.003
36. Expert consensus on diagnosis and treatment of diabetic peripheral neuropathic pain. Chin J Pain Med. 2018;24(08):561–567.
37. Ziegler D. Painful Diabetic Neuropathy. Diabetes Care. 2009;32(Suppl 2):s414–9. doi:10.2337/dc09-S350
38. Schmader KE. Epidemiology and impact on quality of life of postherpetic neuralgia and painful diabetic neuropathy. Clin J Pain. 2002;18(6):350–354. doi:10.1097/00002508-200211000-00002
39. Ziegler D, Rathmann W, Dickhaus T, et al. Neuropathic pain normal glucose tolerance: the MONICA/ KORA Augsburg Surveys S2. Pain Med. 2009;10(2):393–400. doi:10.1111/j.1526-4637.2008.00555.x
40. Sloan G, Selvarajah D, Tesfaye S. Pathogenesis, diagnosis and clinical management of diabetic sensorimotor peripheral neuropathy. Nat Rev Endocrinol. 2021;17(7):400–420. doi:10.1038/s41574-021-00496-z
41. Tesfaye S, Chaturvedi N, Eaton SE, et al. Vascular risk factors and diabetic neuropathy. N Engl J Med. 2005;352(4):341–350. doi:10.1056/NEJMoa032782
42. Sadosky A, Mardekian J, Parsons B, et al. Healthcare utilization and costs in diabetes relative to the clinical spectrum of painful diabetic peripheral neuropathy. J Diabetes Complications. 2015;29(2):212–217. doi:10.1016/j.jdiacomp.2014.10.013
43. Peltier A, Goutman SA, Callaghan BC. Painful diabetic neuropathy. BMJ. 2014;348:g1799. doi:10.1136/bmj.g1799
44. Diabetes Society of Chinese Medical Association. Expert consensus on diagnosis and treatment of diabetic neuropathy (2021). Chin J Diabetes. 2021;13(6):540–557.
45. Wolffff RF, Bala MM, Westwood M, et al. 5% lidocaine medicated plaster in painful diabetic peripheral neuropathy (DPN): a systematic review. Swiss Med Wkly. 2010;140(21–22):297–306. doi:10.4414/smw.2010.12995
46. Li FX. Acupoint injection of bulleyaconitine A in the treatment of diabetic peripheral neuropathy. Chin Med Sci Technol Press. 1999;3:101–102.
47. Feng Y, Xu JJ, Lin XQ, et al. Chronic postoperative or post-traumatic pain. Chin J Pain Med. 2021;27(04):241–245.
48. Coccolini F, Corradi F, Sartelli M, et al. Postoperative pain management in non-traumatic emergency general surgery: WSES-GAIS-SIAARTI-AAST guidelines. World J Emerg Surg. 2022;17(1):50. doi:10.1186/s13017-022-00455-7
49. Aubrun F, Nouette-Gaulain K, Fletcher D, et al. Revision of expert panel’s guidelines on postoperative pain management. Anaesth Crit Care Pain Med. 2019;38(4):405–411. doi:10.1016/j.accpm.2019.02.011
50. Xu JG. Expert consensus on postoperative pain management in adults. J Clin Anesthesiol. 2017;33(09):911–917.
51. Clarke H, Bonin RP, Orser BA, et al. The prevention of chronic postsurgical pain using gabapentin and pregabalin: a combined systematic review and meta-analysis. Anesth Analg. 2012;115(2):428–442. doi:10.1213/ANE.0b013e318249d36e
52. Mishriky BM, Waldron NH, Habib AS. Impact of pregabalin on acute and persistent postoperative pain: a systematic review and meta-analysis. Br J Anaesth. 2015;114(1):10–31. doi:10.1093/bja/aeu293
53. Chinese Association of Pain Physicians, Medical Cluster for Pain Disorders, Beijing Center for Quality Control and Improvement of Pain Management. Expert Consensus on pharmacotherapy for chronic musculoskeletal pain (2018). Chin J Pain Med. 2018;24(12):881–887.
54. Briggs AM, Woolf AD, Karsten D, et al. Reducing the global burden of musculoskeletal conditions. Bulletin of the World Health Organization. 2018;96(5):366–368. doi:10.2471/BLT.17.204891
55. Chinese Aging Well Association. Expert consensus on diagnosis and treatment of musculoskeletal chronic pain. Orthopedics. 2021;12(05):389–395.
56. Kroenke K, Krebs EE, Bair MJ. Pharmacotherapy of chronic pain: a synthesis of recommendations from systematic reviews. Gen Hosp Psychiatry. 2009;31(3):206–219. doi:10.1016/j.genhosppsych.2008.12.006
57. Liu YQ, Ding XN, Wang YD. Clinical study on the treatment of common chronic pain with bulleyaconitine A tablets. Chin J Pain Med. 2011;17(5):314–315.
58. Zhang YC, Yang QR, He Y, et al. Clinical observation on the treatment of osteoarthritis and rheumatoid joint with bulleyaconitine A. Pharmacol Clin Chin Med. 2000;16(2):43–45.
59. Xu N, Liu R, Zang JJ, et al. Efficacy and safety evaluation of bulleyaconitine A tablets in the treatment of osteoarthritis. ChinMed. 2014;9(8):1170–1173.
60. Wang YS, By LIU, Ah Z, et al. Clinical observation of 35 cases of rheumatoid arthritis treated with bulleyaconitine A capsules. Hunan J of Trad Chin Med. 2009;25(1):6–8.
61. Du N, Zhu D. Effect of bulleyaconitine A tablets combined with Tripterygium wilfordis tablets on knee osteoarthritis. J Henan Univ. 2015;34(1):50–52.
62. National Administration of Traditional Chinese Medicine, National Health Commission of the People’s Republic of China. Cancer pain diagnosis and treatment code (2018). Clin Educ Gener Pract. 2019;17(01):4–8.
63. Fallon M, Giusti R, Aielli F, Management of cancer pain in adult patients: ESMO clinical practice guidelines. Ann Oncol. 2018;29(Suppl):4.
64. Qin WJ, Ren XY, Li R, et al. Expert consensus on cancer pain management. Chin J Pain Med. 2019;25(11):801–807.
65. Fallon M, Giusti R, Aielli F, et al.; ESMO Guidelines Committee. Management of cancer pain in adult patients: ESMO Clinical Practice Guidelines. Ann Oncol. 2018;29(Suppl 4):iv166–iv191. doi:10.1093/annonc/mdy152
66. Smith LE, Murphy BA, Smith DK. Prophylactic gabapentin during head and neck cancer therapy: a systematic review and meta-analysis. Support Care Cancer. 2023;31(4):221. doi:10.1007/s00520-023-07683-w
67. Zhang H, Sun Y, Xu GY. New progress in pathologic mechanism and clinical treatment of chronic visceral pain. Chin J Pain Med. 2017;23(01):2–20.
68. Olesen AE, Farmer AD, Olesen SS, et al. Management of chronic visceral pain. Pain Manag. 2016;6(5):469–486. doi:10.2217/pmt-2015-0011
69. Lee KJ, Kim JH, Cho SW. Gabapentin reduces rectal mechanosensitivity and increases rectal compliance in patients with diarrhoea-predominant irritable bowel syndrome. Aliment Pharmacol Ther. 2005;22(10):981–988. doi:10.1111/j.1365-2036.2005.02685.x
70. Houghton LA, Fell C, Whorwell PJ, et al. Effect of a second-generation alpha2delta ligand (pregabalin) on visceral sensation in hypersensitive patients with irritable bowel syndrome. Gut. 2007;56(9):1218–1225. doi:10.1136/gut.2006.110858
71. Olesen SS, Graversen C, Bouwense SA, et al. Quantitative sensory testing predicts pregabalin efficacy in painful chronic pancreatitis. PLoS One. 2013;8(3):e57963. doi:10.1371/journal.pone.0057963
72. Huang S. Study on the anti-visceral pain and anti-anxiety effect of monoponitine. Shang Jiao Tong Univ. 2019;2:4.
73. Huang SN, Wei J, Huang LT, et al. Bulleyaconitine A inhibits visceral nociception and spinal synaptic plasticity through stimulation of microglial release of dynorphin A. Neural Plast. 2020;2020:1484087. doi:10.1155/2020/1484087
74. Phillips EJ, Sukasem C, Whirl-Carrillo M, et al. Clinical pharmacogenetics implementation consortium guideline for HLA genotype and use of carbamazepine and oxcarbazepine: 2017 update. Clin Pharmacol Ther. 2018;103(4):574–581. doi:10.1002/cpt.1004
75. Zhou M, Chen N, He L, et al. Oxcarbazepine for neuropathic pain. Cochrane Database Syst Rev. 2017;12(12):CD007963. doi:10.1002/14651858.CD007963.pub3
76. Moulin D, Boulanger A, Clark AJ, et al. Pharmacological management of chronic neuropathic pain: revised consensus statement from the Canadian Pain Society. Pain Res Manag. 2014;19(6):328–335. doi:10.1155/2014/754693
77. Xiao H, Ma K, Huang D, et al. Expert consensus of the Chinese Association for the Study of Pain on ion channel drugs for neuropathic pain. World J Clin Cases. 2021;9(9):2100–2109. doi:10.12998/wjcc.v9.i9.2100
78. McGeeney BE. Pharmacological management of neuropathic pain in older adults: an update on peripherally and centrally acting agents. J Pain Symptom Manage. 2009;38(2 Suppl):S15–27. doi:10.1016/j.jpainsymman.2009.05.003
79. Derry S, Bell RF, Straube S, et al. Pregabalin for neuropathic pain in adults. Cochrane Database Syst Rev. 2019;1(1):CD007076. doi:10.1002/14651858.CD007076.pub3
80. Lee JE, Min KR, Kim SH, et al. Analysis of adverse drug reactions with carbamazepine and oxcarbazepine at a tertiary care hospital. Yonsei Med J. 2020;61(10):875–879. doi:10.3349/ymj.2020.61.10.875
81. Johnson KD, Miller LN, Pouliot JD, et al. Retrospective analysis of oxcarbazepine in pregnant women with substance use disorders: focus on safety. J Pharm Pract. 2021;34(1):28–34.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.