Back to Journals » International Journal of Nanomedicine » Volume 21
Exosome–Biomaterial Platforms for Diabetic Skin Infections: Microenvironment Remodeling, Responsive Delivery, and Clinical Translation
Authors Xiao J, He Z, Bu Y ![]() , Lu Y, Liang S
, Lu Y, Liang S ![]()
Received 6 March 2026
Accepted for publication 6 June 2026
Published 26 June 2026 Volume 2026:21 607504
DOI https://doi.org/10.2147/IJN.S607504
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 6
Editor who approved publication: Professor Lijie Grace Zhang
Jian Xiao,1,* Zekun He,2,* Yitian Bu,1,* Yan Lu,1 Shuibin Liang3
1The First People’s Hospital of Jiashan, Jiashan Hospital Affiliated to Jiaxing University, Jiaxing, 314100, People’s Republic of China; 2Department of Rehabilitation Treatment, Nanchang Mingzhou Rehabilitation Hospital, Nanchang, 330096, People’s Republic of China; 3Jiaxing Hospital of Traditional Chinese Medicine Affiliated to Zhejiang Chinese Medical University, Jiaxing, 314000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Shuibin Liang, Jiaxing Hospital of Traditional Chinese Medicine Affiliated to Zhejiang Chinese Medical University, Jiaxing, 314000, People’s Republic of China, Email [email protected]
Abstract: Diabetic skin infections, particularly diabetic foot ulcers (DFU), remain difficult to treat because infection, biofilm formation, persistent inflammation, oxidative stress, hypoxia, impaired angiogenesis, and extracellular matrix (ECM) disruption coexist within a hostile wound microenvironment. Conventional treatments, including antibiotics, surgical debridement, negative pressure wound therapy, and standard dressings, are indispensable but often fail to simultaneously suppress infection and restore regenerative healing. Exosomes have emerged as promising acellular mediators for diabetic wound repair because they can coordinate immune regulation, angiogenesis, matrix remodeling, and re-epithelialization. However, direct exosome administration is limited by rapid clearance, poor local retention, dilution by wound exudate, dose inconsistency, and manufacturing heterogeneity. Biomaterial platforms, including hydrogels, microneedle patches, membranes, cryogels, porous scaffolds, and responsive nanocomposite systems, provide a rational strategy to protect exosome bioactivity, prolong local retention, and enable sustained or stimulus-responsive release. More importantly, these materials can be engineered to actively regulate infection-associated pathological barriers, including biofilm persistence, excessive oxidative stress, hypoxia, and impaired tissue reconstruction. This review summarizes recent advances in exosome–biomaterial systems for diabetic skin infections, with emphasis on delivery design, microenvironment-responsive release, anti-infective and regenerative mechanisms, platform comparison, and clinical translation. We further discuss key translational challenges, including exosome source selection, dose standardization, potency assays, scalable manufacturing, storage stability, biosafety, regulatory classification, and clinical trial design. Current evidence suggests that exosome–biomaterial systems can improve wound closure, vascularization, collagen deposition, re-epithelialization, and infection control in preclinical models. Nevertheless, high-quality clinical evidence remains limited. Future studies should prioritize clinically relevant infected diabetic wound models, standardized quality-control frameworks, and simplified delivery systems compatible with routine wound care.
Keywords: diabetic skin infection, diabetic foot ulcers, exosomes, biomaterials, microenvironment reprogramming, regenerative medicine
Introduction
Diabetic skin infections, particularly diabetic foot ulcers (DFU), are among the most severe complications of diabetes and remain a major challenge in wound care. DFU markedly impair quality of life and are closely associated with hospitalization, lower-limb amputation, and increased mortality.1 Recent epidemiological data indicate that approximately 18.6 million people are affected by DFU worldwide each year, and these ulcers precede more than 80% of non-traumatic lower-limb amputations in patients with diabetes.2 The high recurrence rate, prolonged treatment course, and substantial healthcare costs further highlight the need for therapeutic strategies that can control infection while promoting durable tissue repair.3,4 The difficulty in treating diabetic skin infections results from the coexistence of bacterial colonization, biofilm formation, persistent inflammation, oxidative stress, vascular insufficiency, and impaired matrix remodeling.5 These abnormalities interact with each other and create a self-sustaining pathological microenvironment in which infection is difficult to eradicate and tissue regeneration remains incomplete. Current clinical management, including antibiotic therapy, surgical debridement, negative pressure wound therapy, offloading, vascular assessment, and wound dressings, remains essential. However, these approaches mainly reduce pathogen burden or support wound coverage and often do not actively reprogram the diabetic wound microenvironment.6,7 Therefore, single-modality treatments frequently fail to address the combined challenges of infection persistence, immune dysfunction, impaired angiogenesis, and delayed epithelial repair.
Exosomes have attracted increasing attention as acellular therapeutic mediators for diabetic wound repair. These nanoscale extracellular vesicles carry regulatory cargos, including microRNAs, proteins, lipids, and other bioactive molecules, and can modulate macrophage polarization, inflammatory signaling, angiogenesis, fibroblast activity, collagen remodeling, and re-epithelialization.8–10 These pleiotropic effects make exosomes attractive for multi-target regulation of diabetic wounds. Nevertheless, direct administration remains limited by rapid clearance, poor local retention, dilution by wound exudate, degradation in the hostile wound environment, uncertain dose-response relationships, and difficulties in standardized production and quality control.11 These limitations have prompted growing interest in biomaterial-assisted exosome delivery.
Biomaterials provide a practical interface between exosome bioactivity and the complex diabetic wound microenvironment. Hydrogels, microneedle patches, membranes, cryogels, porous scaffolds, and responsive nanocomposite systems can improve exosome stability, prolong local retention, enable sustained or stimulus-responsive release, and provide structural or biochemical support for tissue repair.12 Importantly, biomaterials can also be engineered with antibacterial, antioxidant, oxygen-generating, adhesive, injectable, or microenvironment-responsive properties, thereby expanding their role from passive carriers to active regulators of infected diabetic wounds. However, biomaterials alone often lack sufficient biological complexity to restore immune–vascular–matrix coordination across different stages of healing.
The combination of exosomes and biomaterials therefore represents a rational strategy for diabetic skin infections. In such systems, biomaterials improve the spatial and temporal presentation of exosomes, whereas exosomes provide immunomodulatory, pro-angiogenic, antioxidant, and regenerative signals that strengthen material-based wound repair. Several preclinical studies have shown that exosome-loaded hydrogels, scaffolds, microneedle patches, and nanocomposite systems can reduce inflammation, enhance vascularization, improve collagen deposition, accelerate re-epithelialization, and support infection control.13 However, current evidence remains largely preclinical, and clinical translation is limited by exosome source heterogeneity, dose standardization, scalable manufacturing, storage stability, biosafety, regulatory classification, and clinical trial design.
This review focuses on exosome–biomaterial combinatorial therapies for diabetic skin infections, with particular attention to infected diabetic wounds and DFU. We first summarize the pathological barriers that guide the design of exosome–biomaterial systems. We then discuss the limitations of exosomes and biomaterials as independent therapeutic strategies and review major delivery platforms, including hydrogels, microneedle patches, membranes, cryogels, porous scaffolds, engineered exosomes, and responsive nanocomposite systems. Finally, we compare platform-specific advantages and limitations, synthesize their anti-infective and reparative mechanisms, and discuss key translational challenges. By integrating delivery design, microenvironment remodeling, and clinical translation, this review aims to clarify how exosome–biomaterial systems may progress from promising preclinical platforms toward clinically applicable therapies for refractory diabetic skin infections.
Pathological Microenvironment and Therapeutic Targets of Diabetic Skin Infections
Diabetic skin infections and their progression to non-healing ulcers represent a major disruption of the normal tissue repair cascade. Unlike acute wounds in non-diabetic individuals, diabetic wounds are continuously exposed to systemic metabolic disturbances induced by hyperglycemia, resulting in a complex pathological microenvironment characterized by persistent inflammation, oxidative stress, impaired angiogenesis, extracellular matrix (ECM) degradation, and bacterial biofilm formation. These factors interact with each other and form a self-sustaining vicious cycle that impairs host defense, delays tissue regeneration, and promotes recurrent infection. A clear understanding of these pathological features is essential for identifying therapeutic targets and guiding the design of exosome–biomaterial platforms (Figure 1).
 |
Figure 1 Complex pathological microenvironment of diabetic skin infections and corresponding targeted reprogramming therapeutic strategies. The figure is organized into two interrelated modules: (A) the pathological microenvironment underlying chronic non-healing diabetic skin infections, and (B) therapeutic strategies for microenvironmental reprogramming. In module A, (I) immune-inflammatory dysregulation is driven by persistent M1 macrophage polarization, defective M1-to-M2 phenotypic transition, AGEs–RAGE–NF-κB-dependent cytokine amplification, NLRP3 inflammasome activation, and excessive NET/MMP-9 release. These events collectively accelerate the degradation of collagen fibers, growth factors, and extracellular matrix components, thereby perpetuating tissue destruction. (II) Oxidative stress and defective ECM remodeling are characterized by sustained ROS accumulation, impaired Keap1/Nrf2 antioxidant signaling, reduced HO-1 expression, lipid peroxidation, DNA damage, ferroptotic injury, and fibroblast senescence-associated secretory phenotype. Together, these abnormalities compromise collagen deposition, promote ECM depletion, and delay re-epithelialization. (III) Vascular dysfunction and ischemia–hypoxia arise from PTEN-mediated suppression of PI3K/AKT signaling, attenuated VEGF/eNOS activity, disruption of endothelial junction integrity, increased vascular leakage, impaired endothelial migration and lumen formation, and insufficient HIF-1α-mediated hypoxic adaptation. (IV) Biofilm barrier formation reflects the establishment of extracellular polymeric substance-rich bacterial biofilms composed of extracellular DNA, polysaccharides, and proteins, which promote bacterial persistence, quorum sensing, immune evasion, antibiotic tolerance, and recurrent infection. Collectively, these pathological processes reinforce one another, forming a self-sustaining vicious cycle of infection, inflammation, oxidative injury, vascular insufficiency, and impaired tissue repair. In module B, (I) immune reprogramming strategies aim to restrain NF-κB-driven inflammatory cascades through pharmacological inhibitors or siRNA-based approaches, thereby reducing TNF-α, IL-1β, and IL-6 production and promoting macrophage repolarization toward a reparative M2 phenotype with enhanced secretion of anti-inflammatory and pro-regenerative mediators, including IL-10 and TGF-β. (II) Antioxidant defense reconstruction focuses on restoring redox homeostasis by activating Nrf2 signaling or applying SOD/CAT-like nanozymes to scavenge excessive ROS, generate oxygen, reduce ferroptotic injury, and protect fibroblast and endothelial cell function. (III) Pro-angiogenic regulation targets the PTEN/PI3K/AKT/VEGF signaling axis via PTEN inhibition, gene-silencing strategies, or agents such as empagliflozin, thereby enhancing endothelial survival, migration, tubulogenesis, and functional neovascularization. (IV) Biofilm-targeted nanoplatforms integrate photothermal therapy, photodynamic therapy, microenvironment-responsive nanocarriers, antibiotic delivery, and quorum-sensing inhibitors to disrupt the EPS matrix, improve drug penetration into biofilms, suppress bacterial communication, and enhance bacterial eradication. Black arrows denote activation, progression, or downstream biological effects; T-shaped lines indicate inhibition or blockade; red downward arrows represent reduced expression, activity, or functional capacity; and circular arrows highlight the interconnected pathological loop that sustains non-healing diabetic infected wounds. |
Macrophage Polarization Blockage and Immune-Inflammatory Cascade Dysregulation
Immune dysfunction is one of the major pathological features of diabetic skin infections. During normal wound healing, macrophages gradually transition from the pro-inflammatory M1 phenotype to the repair-promoting M2 phenotype, thereby promoting inflammation resolution and tissue remodeling. However, under persistent hyperglycemic stimulation, this transition is markedly impaired. Advanced glycation end products (AGEs) can activate the receptor for AGEs (RAGE) and downstream nuclear factor-kappa B (NF-κB) signaling, causing macrophages to remain in a pro-inflammatory state and continuously release cytokines such as tumor necrosis factor-alpha (TNF-α), interleukin-1 beta (IL-1β), and IL-6.14 This sustained inflammatory signaling prevents the timely transition toward an M2 phenotype and prolongs the inflammatory phase of wound healing.
In addition, excessive activation of the NLRP3 inflammasome has been observed in diabetic wounds. Hyperglycemia and reactive oxygen species (ROS) can act as danger-associated molecular patterns (DAMPs), inducing NLRP3 inflammasome assembly, caspase-1 activation, and the maturation and release of IL-1β and IL-18. This inflammatory response can also promote neutrophil extracellular trap (NET) formation. Excessive NETs and proteases, especially matrix metalloproteinase-9 (MMP-9), accelerate the degradation of newly synthesized collagen and growth factors such as PDGF and VEGF, thereby impairing granulation tissue formation and tissue repair.15 Therefore, correcting macrophage polarization and suppressing excessive inflammatory signaling are important therapeutic targets for diabetic infected wounds.
Oxidative Stress Compensation Failure and Extracellular Matrix Remodeling Failure
Persistent oxidative stress is another central feature of the diabetic wound microenvironment. Chronic hyperglycemia promotes mitochondrial dysfunction and excessive ROS production. Under physiological conditions, cells rely on antioxidant defense pathways, particularly nuclear factor erythroid 2-related factor 2 (Nrf2), to eliminate excess ROS. However, in diabetic wounds, Nrf2 activation and nuclear translocation are impaired, resulting in reduced expression of antioxidant enzymes such as heme oxygenase-1 (HO-1).16 The imbalance between ROS production and antioxidant defense contributes to lipid peroxidation, protein oxidation, DNA damage, and cellular senescence.
Recent studies have also highlighted the role of ferroptosis, an iron-dependent form of lipid peroxidation-mediated cell death, in diabetic non-healing wounds.17–19 ROS accumulation and reduced glutathione peroxidase 4 (GPX4) activity can promote lipid peroxidation in fibroblasts and endothelial cells, leading to functional cell loss and impaired tissue regeneration.20 Senescent fibroblasts lose their ability to synthesize collagen and may acquire a senescence-associated secretory phenotype (SASP), further releasing inflammatory factors and proteases such as IL-6, IL-1β, and MMPs.21 These processes disrupt the balance between ECM synthesis and degradation, resulting in fragile granulation tissue, poor matrix organization, and delayed re-epithelialization.
Endothelial Dysfunction and Persistent Ischemia-Hypoxia
Impaired angiogenesis and microvascular dysfunction are major obstacles to diabetic wound healing. Hyperglycemia and oxidative stress damage endothelial progenitor cells and mature endothelial cells, reducing their migration, proliferation, and tube formation capacity.22 Although diabetic wounds are often hypoxic, the compensatory stabilization of hypoxia-inducible factor-1 alpha (HIF-1α) is impaired.23,24 As a result, hypoxic signaling fails to effectively induce vascular endothelial growth factor (VEGF) expression and angiogenic repair.
The PTEN/AKT/VEGF signaling axis is an important pathway involved in this process. In the diabetic microenvironment, abnormal PTEN upregulation inhibits PI3K/AKT signaling, resulting in reduced VEGF production and endothelial nitric oxide synthase (eNOS) dysfunction.25 Consequently, endothelial cell survival, migration, and neovascularization are impaired. In addition, hyperglycemia disrupts endothelial tight junction proteins such as ZO-1 and Claudin-5, leading to immature and leaky neovessels.26 These vascular abnormalities limit oxygen, nutrient, and immune cell supply to the infected wound and further aggravate tissue necrosis and delayed healing.
Physical Barrier Collapse and Bacterial Biofilm Formation
Immune dysfunction, tissue necrosis, and microcirculatory impairment collectively weaken the physical and biological barrier functions of diabetic skin. This creates a favorable environment for pathogen colonization, especially by Staphylococcus aureus and Pseudomonas aeruginosa. In the hyperglycemic and exudative wound environment, bacteria can rapidly proliferate and form biofilms composed of extracellular polysaccharides, proteins, and extracellular DNA.27,28
Biofilm formation is a key reason why diabetic skin infections are difficult to eradicate. The biofilm matrix limits antibiotic penetration and creates hypoxic and acidic microdomains that allow bacteria to enter a low-metabolic persistent state.29 Bacteria within biofilms can also communicate through quorum sensing, coordinate virulence factor expression, and evade host immune responses.30 This cycle of bacterial colonization, biofilm formation, immune evasion, and tissue damage contributes to recurrent infection, delayed healing, and progression to deep tissue infection or osteomyelitis.
Potential Therapeutic Strategies for Targeting the Pathological Microenvironment
Given the complexity of the diabetic skin infection microenvironment, single therapies focused solely on infection control or growth promotion are often ineffective. Current therapeutic strategies are gradually shifting from symptom control to microenvironment reprogramming. By intervening in key molecular switches, actively breaking the pathological vicious cycle formed by inflammation, oxidative stress, vascular damage, and biofilm formation, has become a frontier in the field. Based on a thorough understanding of the molecular mechanisms of the complex pathological microenvironment described above, recent research has focused on developing new therapeutic targets and intervention strategies capable of actively reprogramming the microenvironment.
Targeted Reprogramming Strategies for the Immune Microenvironment
The core of reshaping the immune microenvironment lies in correcting the imbalance in macrophage polarization and preventing the subsequent cascade of tissue destruction. The primary strategy to interrupt the upstream inflammatory activation is to block the continuous activation of the NF-κB signaling pathway, which is a major source of pro-inflammatory factors. Using small molecule inhibitors or specific nucleic acid interference techniques (siRNA/shRNA) to target the phosphorylation of IκB kinase (IKK) can prevent the NF-κB p65 subunit from entering the nucleus, thus significantly reducing the expression of key pro-inflammatory cytokines such as TNF-α, IL-1β, and IL-6 at the transcriptional level. This intervention not only alleviates the direct damage of the cytokine storm to the local tissue but also blocks the self-sustaining loop of M1 macrophages.14
While inhibiting pro-inflammatory signals, actively inducing M2 macrophage polarization is a key step in initiating tissue repair.31 Traditional strategies involve the direct delivery of anti-inflammatory cytokines like IL-4 or IL-10 to induce phenotype conversion, but their use is limited by the short half-life of these factors.32 Emerging strategies utilize biomaterials with immune-regulatory functions (such as nanostructures with specific surface morphologies or chemical modifications) to mimic ECM signals, directly regulating macrophage cytoskeletal rearrangement and gene expression. This, in turn, promotes the secretion of growth factors such as TGF-β and VEGF, thereby fostering a regenerative microenvironment.33 Additionally, addressing the issue of matrix degradation downstream of inflammation is critical. Restoring the metabolic balance between MMPs and TIMPs is essential. The use of MMP inhibitors (such as doxycycline) or gene engineering approaches to upregulate the expression of TIMPs can effectively neutralize excess MMP-9 activity, protecting the newly synthesized collagen scaffold from degradation and providing the necessary physical support for stable granulation tissue growth.34,35
Active Defense Reconstruction of Oxidative Stress
Restoring cellular redox homeostasis is fundamental to recovering the functionality of diabetic wound cells. Activating the Nrf2 signaling pathway is considered a primary therapeutic target for antioxidant treatment.36 Given the pathological characteristics of Nrf2 nuclear translocation being inhibited in the diabetic environment, research has focused on developing novel small molecule agonists (such as tert-butylhydroquinone, sulforaphane) or using gene delivery systems to overexpress Nrf2. These strategies aim to reactivate the endogenous antioxidant defense system, systemically upregulating the expression of key enzymes such as HO-1 and NAD(P)H: quinone oxidoreductase 1 (NQO1).37 This process not only efficiently clears accumulated ROS but also protects mitochondrial integrity, preventing cells from undergoing lipid peroxidation-induced ferroptosis, thereby rescuing fibroblasts and endothelial cells from senescence.16
As a supplement to endogenous defense mechanisms, nanozyme technology has provided a new approach to antioxidant therapy. Metal-based nanomaterials with superoxide dismutase (SOD) or catalase (CAT)-like activities (eg, cerium oxide, Prussian blue, or manganese-based nanomaterials) can simulate natural enzyme catalytic processes, efficiently clearing superoxide anions and hydrogen peroxide at the wound site.38,39 More innovatively, these nanozymes can convert harmful H2O2 into oxygen, improving the local hypoxic environment while eliminating oxidative stress, significantly enhancing treatment efficacy.40,41
Regulation of the Angiogenesis Signaling Axis for Targeting Microvascular Regeneration
To address the persistent microcirculatory disturbances in diabetic wounds, the restoration of a functional vascular network primarily relies on the precise regulation of angiogenesis signaling pathways. The PTEN/AKT/VEGF signaling axis is a core hub in this process.42,43 Due to the abnormal overexpression of PTEN in diabetic wounds and its potent inhibitory effect on angiogenesis, specifically inhibiting PTEN activity or downregulating its expression has become an effective strategy for promoting vascularization. For example, using specific inhibitors or miRNA interference techniques to silence PTEN can relieve its inhibitory effect on the PI3K/AKT pathway, restoring AKT phosphorylation levels and reactivating downstream VEGF-mediated endothelial cell proliferation and tubulogenesis.44 Notably, the commonly used antidiabetic drug SGLT2 inhibitor empagliflozin has recently been found to have significant angiogenic effects, with its mechanism being through inhibition of PTEN expression and activation of the AKT/VEGF pathway, effectively reversing endothelial dysfunction and promoting wound vascular network reconstruction. This provides important molecular evidence for the repurposing of old drugs for the treatment of DFU.25
Nanomaterial Platforms Targeting Bacterial Biofilms
Given the challenge of antibiotic resistance and immune evasion caused by bacterial biofilms, therapeutic strategies must shift from simple bactericidal approaches to comprehensive interventions, including physical disruption, targeted delivery, and signaling blockade. Photothermal and photodynamic therapies (PTT/PDT) use near-infrared light-responsive nanomaterials to generate controlled high temperatures or cytotoxic singlet oxygen at the wound site. This physical disruption directly damages the extracellular polysaccharide matrix (EPS) of the biofilm, exposing the deeper bacteria and disrupting their cell membrane structure, while minimizing the risk of inducing bacterial resistance.45
To improve drug delivery efficiency, the design of microenvironment-responsive delivery systems takes advantage of the pathological features specific to the infection microenvironment (such as acidic pH and high concentrations of hyaluronidase or gelatinase). Recent smart antibacterial gels have further extended this concept by combining antibacterial activity, multidrug-resistant infection control, wound-state monitoring, and diabetic wound repair within a single integrated platform.46 Smart nanocarriers are designed to undergo charge inversion (from negative to positive, enhancing bacterial adsorption) or scaffold degradation upon reaching the infection site, thus achieving targeted, burst release of antibacterial drugs deep within the biofilm. Additionally, the application of quorum-sensing inhibitors (QSIs) aims to interfere with bacterial communication networks. By blocking bacterial quorum-sensing signals, the initial adhesion phase of biofilm formation can be suppressed, and the expression of virulence factors can be reduced, restoring bacterial susceptibility to host immune systems and conventional antibiotics, ultimately eradicating chronic infections.47 The use of these multifunctional platforms signifies the advancement of diabetic skin infection treatments toward microenvironment-targeted, integrated interventions.
Current Applications and Limitations of Existing Therapies
Diabetic skin infections, particularly DFU-related infections, are still primarily managed with antibiotic therapy, surgical debridement, negative pressure wound therapy (NPWT), and standard dressing. However, the complex pathological microenvironment created by hyperglycemic toxicity, persistent inflammation, microcirculatory disorders, and biofilm barriers in diabetic patients makes it difficult for traditional therapies to not only control infection but also reverse key obstacles such as immune imbalance, oxidative stress, and impaired tissue regeneration. With the global rise of AMR and the challenges posed by biofilm-induced drug resistance, it is crucial to systematically evaluate the boundaries and limitations of existing therapies in order to define the design direction for the next generation of multifunctional strategies. Meanwhile, exosomes and biomaterials, as emerging intervention methods, have shown potential in promoting microenvironment remodeling in preclinical studies, but their standalone application still faces limitations such as delivery issues, stability, and insufficient functional coverage. This section will review the limitations of traditional therapies and summarize the current status of exosomes and biomaterial applications in diabetic wounds, providing an evidence base and logical support for subsequent combined strategies.
Limitations of Current Traditional Therapies
Currently, traditional treatments for diabetic skin infections primarily include antibiotic therapy, surgical debridement, NPWT, and routine dressing management. While these approaches have fundamental value in controlling infection and maintaining basic wound management, their overall effectiveness remains suboptimal in the context of immune dysfunction, microcirculatory disturbances, and the prevalence of multidrug-resistant strains. Epidemiological data show that the incidence of DFU infection can reach 50%–70%, with an increasing proportion of multidrug-resistant bacteria (eg, methicillin-resistant Staphylococcus aureus, MRSA), which is closely associated with treatment failure and increased amputation risk.5,48,49
Antibiotic therapy is the core component of DFU infection management, but it faces the increasing challenge of drug resistance. Common pathogens in DFU include Gram-positive bacteria (eg, Staphylococcus aureus) and Gram-negative bacteria (eg, Pseudomonas aeruginosa). In some Asian countries, the detection rate of multidrug-resistant strains can reach 40%–80%.50 The empirical use of broad-spectrum antibiotics not only accelerates the evolution of resistance mechanisms (eg, biofilm-associated tolerance, horizontal gene transfer) but also increases systemic adverse reactions and medical costs.7 Systematic reviews indicate that empirical antibiotic treatment failure rates in DFU can reach 30%, with one key reason being biofilm barriers that hinder drug penetration and effective concentration, leading to prolonged infections and continuous tissue necrosis.49 Furthermore, diabetic patients often have underlying conditions such as renal dysfunction, further limiting the range of antibiotic choices and the optimization of dosages, thereby increasing treatment difficulty.
Surgical debridement can reduce pathogen load by removing necrotic tissue and part of the biofilm, but its effectiveness depends on the operator’s experience and carries risks of secondary injury. In the diabetic microenvironment, delayed healing after debridement is not uncommon, with healing rates only around 30%–50%.51 NPWT can provide some benefits by draining exudate, reducing edema, and improving local microcirculation, but its efficacy in severely infected DFU is still limited, and it comes with high equipment and nursing costs.52,53 Routine dressings (eg, gauze, foam dressings) can maintain a moist environment and absorb exudates, but they often lack biological activity and targeted regulatory capabilities, making it difficult to effectively intervene in core pathological processes such as persistent inflammation, angiogenesis impairment, and tissue regeneration deficits, resulting in chronic wounds being stuck in the inflammatory phase for extended periods.54
Overall, the key limitation of traditional therapies is their relatively narrow intervention scope: antibiotics and debridement focus on pathogen load control, NPWT and dressings focus on wound management, but none can simultaneously reprogram the pathological microenvironment of diabetic wounds, making it difficult to address multiple obstacles such as uncontrolled inflammation, sustained oxidative stress, and infection resistance/biofilm formation. This current situation highlights the urgent need for multifunctional treatment strategies that combine infection control with regenerative capabilities and enable precise spatiotemporal regulation.
Current Application of Exosomes in Diabetic Wounds
Exosomes are extracellular vesicles, approximately 30–150 nm in diameter, secreted by various cell types and carrying bioactive molecules such as miRNAs, proteins, lipids, and other regulatory cargos. Their biocompatibility, low immunogenicity, relative stability, and ability to participate in intercellular communication make them promising acellular therapeutic candidates for diabetic wound repair.8 A growing body of preclinical evidence suggests that exosomes can regulate several key processes involved in diabetic wound healing, including inflammation resolution, angiogenesis, fibroblast and keratinocyte activity, collagen deposition, ECM remodeling, and re-epithelialization.55–57 Compared with cell-based therapies, exosomes may reduce some safety concerns related to tumor formation, immune rejection, and poor cell survival after transplantation.58
Exosomes used for diabetic wound repair are mainly derived from mesenchymal stem cells (MSCs), including adipose-derived, bone marrow-derived, and umbilical cord-derived MSCs, as well as endothelial cells, immune cells, and emerging plant-derived exosome-like nanoparticles. Different sources may provide distinct therapeutic advantages. MSC-derived exosomes are widely studied because of their broad immunomodulatory, pro-angiogenic, and matrix-remodeling effects.59 Endothelial cell-derived exosomes may be more directly related to vascular repair, whereas M2 macrophage-derived or immunologically preconditioned exosomes may be more suitable for wounds dominated by persistent inflammation and impaired macrophage phenotype transition. Immune cell-derived vesicles, engineered antibacterial vesicles, and drug-loaded exosomes may provide additional value in wounds characterized by bacterial burden, biofilm-associated infection, or molecular debridement needs. Recent reviews have emphasized that exosomes from different cellular origins may carry distinct cargos and functions, supporting a source-specific rather than source-neutral view of exosome therapy.60 Therefore, exosome source selection should be based on cargo composition, potency assays, manufacturing reproducibility, safety profile, and stage-specific wound requirements.
Despite source heterogeneity, many exosomes contain regulatory cargos associated with angiogenesis, immune regulation, and tissue regeneration, such as miR-21, miR-126, miR-132, and multiple functional proteins.61 These cargos can regulate key pathways, including PI3K/AKT, NF-κB, HIF-1α/VEGF, TGF-β/Smad, and Nrf2-related signaling.8,58,62 In diabetic wound models, exosomes have been shown to reduce excessive inflammatory cytokine production, promote macrophage polarization toward a reparative phenotype, enhance endothelial cell tube formation, stimulate fibroblast migration, improve collagen deposition, and accelerate re-epithelialization.63–67 These effects suggest that exosomes can regulate the diabetic wound microenvironment through multiple coordinated mechanisms.
However, direct exosome administration still faces important translational barriers. Exosomes may be rapidly cleared from the wound bed, diluted by wound exudate, degraded by proteases, or inactivated in a hostile oxidative and inflammatory microenvironment. Their short local residence time often requires repeated administration or high doses, which increases treatment cost and batch-related variability. In addition, limited production yield, batch-to-batch heterogeneity, and the lack of standardized purification and quality-control methods remain major obstacles to large-scale clinical translation.68,69 Exosome dosage is also insufficiently standardized in diabetic wound studies. Current preclinical reports use heterogeneous metrics, including particle number, total protein content, and cell-equivalent dose, making direct comparison across studies difficult. Inadequate dosing may fail to maintain sufficient local concentrations for durable immune regulation, angiogenesis, antioxidant protection, and ECM remodeling, whereas excessive dosing may increase manufacturing cost and safety concerns without proportional therapeutic benefit. In diabetic infected wounds, effective dose is further influenced by exudation, protease activity, bacterial burden, local retention time, and release kinetics. Biomaterial-based delivery platforms may partially address these limitations by improving exosome retention, protecting vesicle bioactivity, and enabling sustained or responsive release.
Overall, exosomes have accumulated a substantial preclinical evidence base as acellular regenerative tools for diabetic wound repair. Their therapeutic potential is expected to be further improved through rational source selection, engineering modification, dosage standardization, and integration with biomaterial-based delivery systems.
Optimization Strategies for Enhancing Exosome Therapeutic Potency
Several optimization strategies have been explored to enhance the therapeutic potency of exosomes before transplantation. Donor-cell preconditioning is one commonly used approach, as hypoxic stimulation, inflammatory priming, pharmacological pretreatment, three-dimensional culture, or biomaterial-assisted culture can alter the molecular cargo of parental cells and enrich exosomes with pro-angiogenic, anti-inflammatory, or antioxidant signals. Exosome optimization for diabetic skin wounds has also been discussed in terms of source selection, engineering, dosage adjustment, and improved delivery strategies. Genetic engineering of donor cells provides another strategy by promoting the selective enrichment of therapeutic miRNAs, lncRNAs, or proteins in secreted exosomes, thereby strengthening specific regulatory pathways involved in macrophage polarization, endothelial cell function, fibroblast migration, or oxidative stress resistance. Recent reviews of bioengineered MSC-derived exosomes have summarized three major strategies, including parental-cell engineering, direct exosome engineering, and the combination of engineered exosomes with biomaterials for diabetic wound healing. In addition, exosomes can be directly loaded with therapeutic cargo, including miRNAs, siRNAs, antibiotics, antioxidants, or small molecules, to combine endogenous vesicle-mediated signaling with programmable drug delivery. Surface modification and ligand conjugation may further improve targeting ability, tissue retention, and interaction with wound-resident cells. When combined with biomaterial platforms, these optimized exosomes can achieve improved stability, sustained release, and stronger local bioactivity in diabetic infected wounds. However, such optimization also increases the need for rigorous quality control, cargo characterization, potency assays, safety evaluation, and scalable manufacturing protocols.
Role of Biomaterials in Wound Healing
Biomaterials have become an important strategy to complement traditional wound treatments by providing mechanical support, optimizing the local microenvironment, and enabling controlled release of active components.12 In diabetic skin infections, particularly DFU, biomaterials can intervene at both structural and functional levels to address pathological obstacles such as chronic inflammation, oxidative stress, impaired angiogenesis, biofilm formation, and delayed tissue regeneration.70 The therapeutic performance of biomaterials is largely determined by their physicochemical design and biological interactivity. Beyond wound coverage, biomaterial platforms can be engineered to regulate stiffness, porosity, surface chemistry, degradation kinetics, hydrophilicity, adhesion, and fluid-handling capacity.71 These properties influence cell–material interactions, exudate absorption, oxygen and nutrient diffusion, bacterial adhesion, and therapeutic cargo retention. Different biomaterial architectures provide complementary functions: hydrogels support moist wound management and sustained release; nanofibers and porous scaffolds facilitate cell infiltration and ECM reconstruction; films and dressings provide barrier protection and exudate control; and microneedle patches enhance localized delivery across wound barriers.72
At the mechanistic level, biomaterials can promote wound repair through several pathways. By mimicking the ECM microenvironment through surface morphology, chemical groups, and pore structure, biomaterials can support the adhesion, migration, and proliferation of fibroblasts, endothelial cells, and keratinocytes, while regulating pathways such as PI3K/AKT and TGF-β/Smad to improve collagen deposition and ECM remodeling.73 Biomaterials can also reduce external contamination, limit bacterial adhesion, maintain a moist wound environment, and serve as delivery platforms for active components such as nitric oxide donors, growth factors, antimicrobial agents, antioxidants, or exosomes.74
In recent years, stimulus-responsive biomaterials have attracted increasing attention. These materials can respond to characteristic signals in diabetic or infected wounds, including acidic pH, high ROS, high glucose, specific enzymes, temperature, or light, thereby enabling on-demand release.75 For example, pH-responsive hydrogels can enhance antibiotic release or bacterial adsorption in acidic environments; ROS-responsive materials can reduce oxidative stress while releasing antioxidant or pro-angiogenic molecules; and glucose-responsive materials can adjust release behavior according to hyperglycemic wound conditions. Injectable and self-healing hydrogel dressings with wound-monitoring capacity have also been developed to integrate dynamic wound coverage, local microenvironment regulation, and wound-state assessment.76,77 However, stimulus-responsive biomaterials may not always behave predictably in complex diabetic infected wounds. Pathological signals such as pH, ROS, glucose, and enzyme activity are spatially and temporally heterogeneous rather than uniformly distributed across the wound bed. This heterogeneity may lead to premature release, insufficient release, off-target activation, delayed release, or loss of responsiveness caused by excessive exudate, necrotic tissue, bacterial biofilm, and protease-mediated degradation. Therefore, the performance of responsive biomaterials should not be evaluated only under simplified in vitro conditions. More robust designs require appropriate response thresholds, improved stability, and validation in infected, ischemic, high-exudate, and biofilm-containing wound models.
In diabetic skin infection applications, single biomaterials have shown the ability to reduce infection risk and improve the local microenvironment to some extent. For example, chitosan-based dressings exhibit inherent antimicrobial and hemostatic properties and can inhibit multidrug-resistant strains such as MRSA and Pseudomonas aeruginosa in preclinical models. Collagen/hyaluronic acid composite materials can maintain a moist environment and provide ECM-like support to enhance fibroblast activity and collagen organization.70,78 Nevertheless, single biomaterials often cannot fully address the multiple pathological loops of diabetic wounds, including persistent inflammation, oxidative stress, angiogenesis impairment, and biofilm-associated infection. Therefore, current research is shifting toward multifunctional composite systems that integrate biomaterials with active components such as antimicrobial nanoparticles, growth factors, antioxidants, nitric oxide donors, or exosomes.
Overall, biomaterials have evolved from passive dressings into active platforms capable of regulating the wound microenvironment. Future development should focus on optimizing degradation kinetics, improving responsiveness, enhancing biosafety, and integrating multifunctional therapeutic modules while maintaining manufacturability and clinical usability.
Joint Application and Advantages of Exosomes and Biomaterials
In diabetic skin infections, the combined use of exosomes and biomaterials has developed from a simple delivery-enhancement strategy into a multifunctional approach that integrates infection control and tissue regeneration. Early studies mainly focused on improving the poor retention and stability of exosomes in chronic wounds. Because diabetic wounds are often characterized by abundant exudate, high protease activity, and excessive ROS accumulation, directly applied exosomes are easily diluted, degraded, or cleared from the wound site. Local retention and sustained release therefore became key design goals. Incorporating MSC-derived exosomes into ECM-based materials or natural polymer hydrogels can physically retain exosomes, protect their bioactivity, and extend their therapeutic window. For example, integrating adipose-derived stem cell (ADSC) exosomes into ECM hydrogels improved the inflammatory state of diabetic wounds and promoted collagen deposition and skin regeneration.79
With increasing understanding of infected diabetic wounds, it has become clear that prolonging exosome retention alone is insufficient to address bacterial load, immune imbalance, hypoxia, oxidative stress, and impaired regeneration. Recent studies have therefore begun to integrate antimicrobial, antioxidant, immune-regulatory, oxygen-generating, and responsive-release modules into exosome–biomaterial systems. In these designs, biomaterials not only serve as carriers but also actively participate in microenvironment regulation. For example, in an MRSA-infected diabetic wound model, a multifunctional hydrogel with bacterial membrane interference and ROS-responsive release properties enhanced exosome release during the infection phase, reduced bacterial burden, and improved wound healing outcomes.80
The advantages of exosome–biomaterial systems arise from their complementary functions. Biomaterials improve the spatial and temporal presentation of exosomes by enhancing retention, controlling release, and providing structural support. Exosomes, in turn, provide biological signals for immune regulation, angiogenesis, fibroblast activation, ECM remodeling, and epithelial regeneration. This division of labor is particularly important in infected diabetic wounds, where infection control and tissue regeneration must be coordinated rather than treated as separate processes. Overall, the field is shifting from simple exosome delivery toward multifunctional platforms that actively remodel the infected diabetic wound microenvironment. Exosomes are no longer only independent pro-repair signals, and biomaterials are no longer only passive carriers. Instead, their combination provides a coordinated therapeutic strategy that integrates antibacterial activity, immune regulation, oxidative stress control, angiogenesis, and tissue reconstruction.
Exosome-Biomaterial Combined Strategies Based on Local Microenvironment Remodeling
Among existing strategies, hydrogels remain the most common delivery form for exosome-based treatments. Their clinical advantages lie not only in maintaining a moist, closed environment to reduce the risk of contamination and secondary infections but also in significantly improving exosome retention and stability at the wound site due to their network structure. Hydrogels can also adapt to irregular wounds and dynamic stress environments through features such as injectability, in situ gelation, and self-healing. Studies focusing on ECM/matrix-based strategies emphasize the importance of reconstructing a tissue-like microenvironment. In these approaches, exosomes do not act alone but function within the adhesive sites, mechanical support, and degradable matrix provided by the material. This enhances cell recruitment, inflammation alleviation, and tissue remodeling. For example, integrating adipose-derived MSC exosomes into ECM hydrogels improves the inflammatory state of diabetic wounds and promotes collagen deposition and re-epithelialization, thereby accelerating skin regeneration (Figure 2A).79 Similarly, combining endothelial cell-derived exosomes with ADM-derived composite hydrogels strengthens diabetic wound angiogenesis and tissue remodeling through matrix support and angiogenesis signaling (Figure 2B).81 Recent material designs have also focused on optimizing pore structures, cell infiltration, and exudate management. For example, a microporous soybean protein hydrogel with EGCG regulates pore structure while managing local inflammation and infection risks, providing a favorable “repair-like microenvironment” for exosome entry and epithelial regeneration, thus enhancing re-epithelialization and healing quality in chronic, high-risk wounds (Figure 2C).82 These results indicate that hydrogels are evolving from focusing on retention time to rebuilding a renewable microenvironment, making exosome activity easier to translate into observable histological improvements.
 |
Figure 2 Exosome–biomaterial combinatorial strategies centered on local microenvironment reprogramming: functional expansion of hydrogels from delivery depots to microenvironment-modulating platforms. (A) Adipose-derived MSC exosomes integrated with ECM-/matrix-mimetic hydrogels. In situ gelation improves conformal coverage and enables sustained release, attenuating inflammation while promoting collagen deposition and re-epithelialization in diabetic wounds, thereby improving skin regeneration outcomes.79 (B) Endothelial cell–derived exosomes combined with an ADM-derived composite hydrogel. The coupled effects of matrix support and pro-angiogenic signaling enhance neovascularization and accelerate tissue remodeling.81 (C) A microporous soy-protein injectable hydrogel with pore architecture tuned by EGCG to optimize exudate management while mitigating local inflammatory/infectious risk. This structural microenvironment facilitates exosome-supported cell infiltration and epithelial repair, improving re-epithelialization and healing quality in high-risk chronic wounds.82 (D) An adaptive-release hydrogel for MRSA-infected diabetic wounds that couples bacterial membrane disruption with ROS-responsive release, enabling infection-burden–aligned enhancement of exosome delivery and more appropriately scaled intervention intensity across infection control and regenerative progression.80 (E) A living microalgae–hydrogel system enabling light-triggered, phase-tailored intervention: photothermal activity reduces bacterial burden, sustained oxygen generation alleviates hypoxia, and induced/concomitant release of antioxidant vesicles suppresses ROS accumulation, collectively facilitating the transition of infected diabetic wounds toward a regenerative phase.83 (F) A self-healing injectable dynamic oxidized xanthan gum network co-delivering exosomes and matrine. By maintaining dressing integrity and providing coordinated antibacterial, immunomodulatory, and pro-angiogenic actions, this platform further optimizes the local microenvironment and repair outcomes in high-risk wounds.84 |
In infection-related scenarios, hydrogel systems are following a platform-based trend, where exosome delivery is closely integrated with material properties, such as antibacterial, antioxidant, and microenvironment-responsive release. This allows for dynamic adjustment of treatment intensity based on the lesion status. For example, an adaptive release system for MRSA-infected diabetic wounds integrates bacterial membrane interference and ROS-responsive release mechanisms into the hydrogel network, realizing a strategy where the release is stronger during higher infection loads, providing comprehensive intervention tailored to the disease course (Figure 2D).80 Similarly, a live microalgae-hydrogel system uses light-responsive mechanisms to achieve photothermal sterilization, continuous oxygen supply, and antioxidant vesicle release, addressing infection, hypoxia, and ROS accumulation while facilitating the transition of infected diabetic wounds from the inflammation phase to the regeneration phase (Figure 2E).83 Furthermore, a self-healing injectable oxidized yellow original gel system combined with exosomes and matrilin maintains long-term dressing integrity and improves the wound microenvironment through synergistic effects on antibacterial, immune regulation, and angiogenesis (Figure 2F).84 pH/ROS dual-responsive hyaluronic acid hydrogels loaded with ginseng-derived exosomes (for a diabetic oral ulcer model) offer a representative paradigm using an acidic, high ROS microenvironment as a release switch, with anti-inflammatory, antioxidant, and tissue regeneration mechanisms highly analogous to skin infections and high-risk wounds, demonstrating strong migratory validation potential.85 Similarly, pH-responsive hydrogels delivering curcumin-pretreated MSC exosomes further exemplify the enhanced exosome potency and material delivery enhancement strategy.86 Additionally, sprayable/rapidly formable exosome hydrogels for clinical irregular wounds use photopolymerization to achieve rapid coverage with adjustable release cycles, offering stable synergy in infection risk control, antioxidant effects, and angiogenesis.87 Overall, hydrogels in these combined strategies have evolved from focusing on exosome retention and stability to providing tissue-like support and synergistically regulating infection-related microenvironments, enabling exosome activity to transition more efficiently from molecular signaling to inflammation alleviation, angiogenesis, and tissue remodeling endpoints (Table 1).88
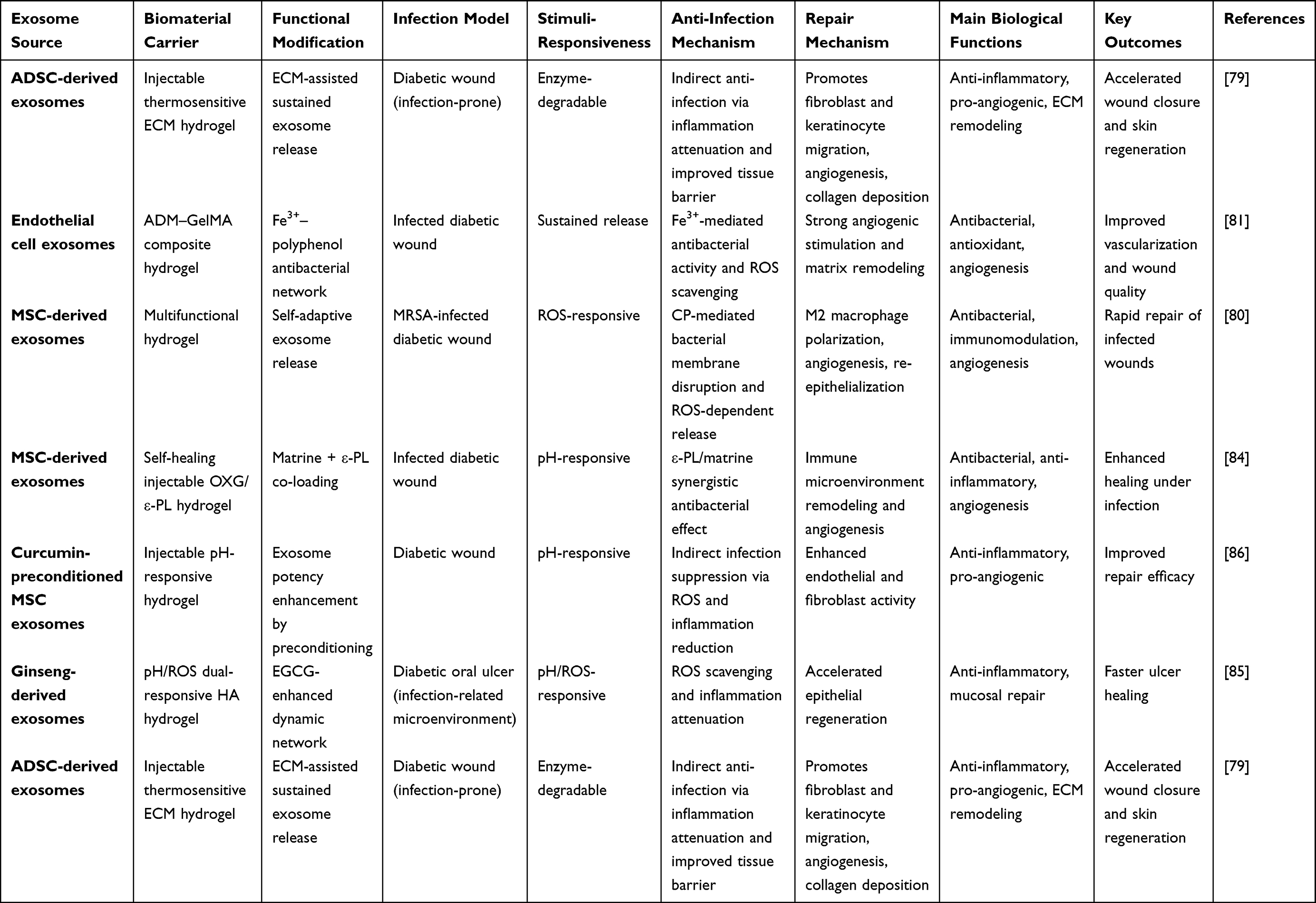 |
Table 1 Exosome-Biomaterial Combined Strategies Based on Local Microenvironment Remodeling |
Exosome Delivery Systems Optimized for Clinical Operations and Delivery Efficiency
In contrast to hydrogel-based platforms, which primarily emphasize prolonged retention and modulation of the wound microenvironment, device-enabled dressings and structured delivery systems are designed to more directly address key bottlenecks in clinical wound care. These include insufficient delivery depth, incomplete coverage of irregular wound geometries, increased risk of secondary contamination associated with frequent dressing changes, and constraints imposed by patient adherence. Accordingly, the translational value of this technology class is often reflected in integrated gains across therapeutic efficacy, operational feasibility, and safety (Table 2).
 |
Table 2 Exosome Delivery Systems Optimized for Clinical Operations and Delivery Efficiency |
Microneedle patches represent a prototypical shift from superficial coverage toward intratissue delivery. A composite microneedle system based on methacrylated silk fibroin and methacrylated hyaluronic acid, loaded with exosomes, enables more efficient localized deposition through a microneedle array and enhances angiogenesis and re-epithelialization, thereby accelerating diabetic wound repair (Figure 3A).89 Notably, as infection immunobiology has become increasingly central to diabetic wound research, device-based platforms have begun to move beyond delivery enhancement alone. Emerging designs integrate bacteria-responsive signaling with immunomodulatory correction, approaching a framework more aligned with infection-oriented immunotherapy.
 |
Figure 3 Device-enabled and structured exosome delivery systems: optimization for clinical handling and localized delivery efficiency. (A) An exosome-loaded SilMA/HAMA composite microneedle patch enables intratissue delivery via a microneedle array, increasing effective deposition and local bioavailability of exosomes within wound tissue. This enhances angiogenesis and re-epithelialization, thereby accelerating diabetic wound repair.89 (B) A “fate reversal” patch platform couples exosome-mediated restoration of macrophage function/phenotypic correction with bacteria-signal–triggered responsive release, enabling parallel control of infectious burden and correction of immune dysfunction. This design supports the transition of infected diabetic wounds from an inflammatory state toward regenerative healing.90 (C) A multifactor-integrated microneedle patch exemplifies a design paradigm that combines device-based delivery, microenvironment responsiveness, and phase-tailored combination therapy within a single platform. By orchestrating infection control, inflammation modulation, and regenerative promotion in a time-resolved manner, it provides a reference blueprint for system-level integration along device-enabled routes.92 (D) A chitosan-based nanomembrane dressing incorporating nanovesicles derived from aloe vera, neem, and ginger provides rapid coverage and barrier protection to maintain a moist wound environment and reduce contamination. Vesicle-associated bioactivity further supports repair-related processes.91 |
A representative example is the “fate reversal” strategy, which combines exosome-mediated restoration of macrophage function with bacteria-responsive release mechanisms within a patch/device platform. This concept underscores that effective therapy should not only reduce bacterial burden but also rectify hyperglycemia-associated immune dysfunction and persistent inflammation, thereby establishing a more robust biological basis for simultaneous infection control and regenerative progression (Figure 3B).90 In addition, although the “Multifaceted Microneedle Patch” does not primarily use exosomes as its payload, it exemplifies a design paradigm in which device-enabled delivery is coupled with microenvironmental responsiveness and phase-tailored multimodal interventions. This paradigm is instructive for understanding the field’s shift from single-factor pro-repair approaches toward more system-level strategies that balance infection management with regeneration (Figure 3C).92
By comparison, membrane materials and nanomembrane dressings prioritize rapid coverage and barrier protection, offering clear advantages in scalability and compatibility with routine nursing workflows. A chitosan-based nanomembrane integrating nanovesicles derived from aloe vera, neem, and ginger aims to reduce contamination and bacterial colonization through barrier function and moisture management, while leveraging vesicle-associated bioactivity to support tissue repair (Figure 3D).91 It should be noted, however, that evidence supporting plant-derived vesicles/extracellular vesicles for wound healing remains constrained by translational challenges, including limited standardization of sources and manufacturing processes, incomplete attribution of active components and mechanisms, lack of unified dose-metrics and quality-control criteria, and difficulties in ensuring batch-to-batch consistency. Therefore, evaluation of such systems should explicitly weigh their manufacturability and workflow compatibility against persistent barriers in source standardization and quality assurance.93
Long-Acting Dressing Architectures Centered on Hypoxia and Oxidative Stress Regulation
Infected diabetic wounds are frequently characterized by increased exudation, local hypoxia, and sustained oxidative stress. These factors mutually reinforce bacterial colonization, biofilm formation, and inflammatory amplification, thereby trapping the wound in a maladaptive steady state characterized by high inflammation and limited regeneration. In this context, three-dimensional porous dressings with prolonged structural stability—such as cryogels and porous scaffolds—offer distinctive advantages over extended time scales. Porous architectures facilitate exudate handling, gas exchange, and cellular infiltration, while also providing an appropriate reservoir for oxygen-generating, antioxidant, and antibacterial modules. These functional components can act in sustained synergy with the immunoregulatory and pro-regenerative signaling of exosomes, reducing the ongoing microenvironmental damage that otherwise perpetuates impaired healing.
The OxOBand cryogel exemplifies this approach by integrating exosome delivery with oxygen release as well as antioxidant and antibacterial functionality, directly targeting the interconnected barriers of hypoxia, reactive oxygen species burden, and infection. This multimodal design demonstrates enhanced overall reparative performance in both diabetic and infected wound settings (Figure 4A).94 Similarly, a HA@MnO2/FGF-2/exosome composite hydrogel mitigates persistent oxidative stress in hyperglycemic conditions via MnO2-mediated reactive oxygen species scavenging and oxygen generation. In parallel, staged release of exosomes and FGF-2 supports a stepwise regulatory trajectory encompassing cytoprotection, angiogenesis enhancement, and matrix remodeling, ultimately improving neovascularization and the quality of collagen deposition in oxidative diabetic wounds (Figure 4B).95
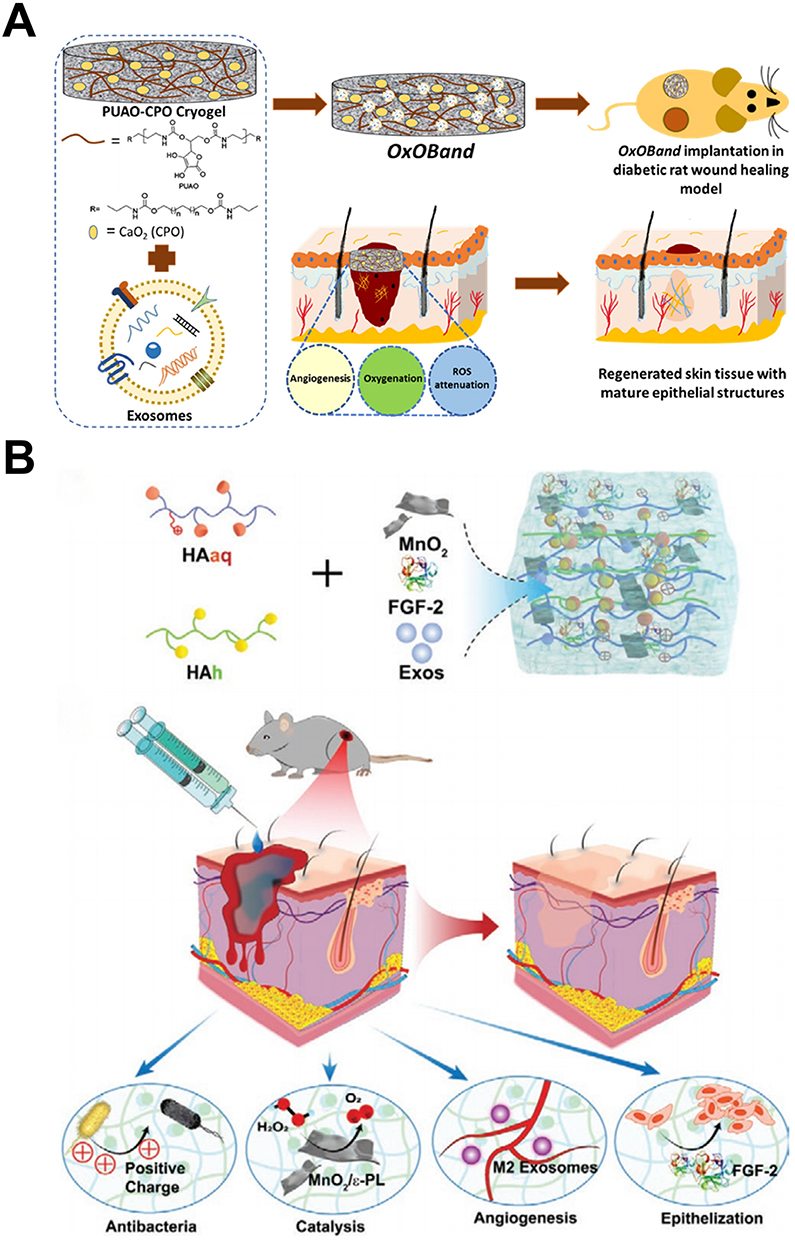 |
Figure 4 Long-acting dressings targeting hypoxia and oxidative stress: three-dimensional porous architectures enable exudate management and sustained functional coupling. (A) OxOBand cryogel, as a three-dimensional porous, long-acting dressing, integrates exosome delivery with sustained oxygen release and antioxidant/antibacterial modules. This platform alleviates the coupled microenvironmental constraints of hypoxia, ROS accumulation, and bacterial burden in infected diabetic wounds, thereby supporting infection control and tissue repair over an extended therapeutic time window.94 (B) A HA@MnO2/FGF-2/exosome composite system improves hyperglycemia-associated oxidative stress and hypoxia through MnO2-mediated ROS scavenging and in situ oxygen generation. Coupled with phase-programmed release of exosomes and FGF-2, it enables a stepwise regulatory trajectory spanning antioxidant protection, angiogenesis enhancement, and matrix reconstruction, ultimately improving neovascularization and the quality of collagen deposition in oxidative diabetic wounds.95 |
Within porous sponge/scaffold systems, a gallium/chitosan/silk fibroin/umbilical cord MSC exosome composite couples the sustained antibacterial effect of Ga3⁺ with the pro-angiogenic and pro-matrix remodeling activity of exosomes. By leveraging porous structure to improve ventilation and exudate control, this design achieves a more stable balance between infection-risk containment and repair quality.96 Overall, long-acting three-dimensional porous dressings use structural support, exudate and gas-exchange management, and sustained-release capacity as foundational features, enabling prolonged coupling of oxygenation, antioxidation, and antibacterial modules with exosome-driven immunomodulatory and regenerative signaling. This design logic aligns closely with the chronic, intertwined nature of hypoxia, oxidative stress, and infection in diabetic wounds. At the same time, device form factors and compatibility with care pathways—coverage, fixation, replacement frequency, and adherence—are increasingly recognized as essential criteria for translational assessment of these systems (Table 3).97
 |
Table 3 Long-Acting Dressing Architectures Centered on Hypoxia and Oxidative Stress Regulation |
Engineered Exosomes and Nano-Integrated Multifunctional Platforms
As therapeutic objectives advance from promoting closure to achieving stronger efficacy, higher precision, and phase-matched coordination between infection control and regeneration, engineered exosomes and nanocomposite systems are emerging as a key toolbox for multi-target intervention. One representative route involves integrating inorganic or two-dimensional materials with exosomes, thereby combining material-derived antibacterial, antioxidant, or triggerable physical effects with exosome-mediated immunomodulation and pro-angiogenic activity. Such combinations offer a materials-enabled strategy to address the mechanistic coupling of infection susceptibility and impaired regeneration.
For example, MXene–M2 exosome nanocomposites emphasize immune microenvironment restoration under hyperglycemia-induced immunosuppression while promoting angiogenesis, providing a plausible material implementation of coordinated immune correction and regenerative enhancement in infection-prone diabetic wounds (Figure 5A).98 Similarly, covalent organic framework (COF)-based engineered exosome-integrated nanoformulations reflect an increasingly platform-oriented direction, using tunable nanoscaffolds to synergize exosome immunomodulation with antibacterial and antioxidant capacity for comprehensive treatment of diabetic ulceration and infection risk (Figure 5B).99 In a related design, gold nanorods combined with M2 macrophage-derived exosomes yield a near-infrared-responsive composite in which photothermal antibacterial activity is coupled with exosome-driven immunoregulation and angiogenesis, illustrating a trigger-enabled route to synchronize infection suppression with regenerative progression (Figure 5C).100 Phase-tailored delivery concepts also recur in this space; for instance, “all-in-one” systems that temporally program exosome and FGF release while incorporating antioxidant modules highlight the value of treatment choreography aligned with wound-healing dynamics.95
 |
Figure 5 Engineered exosomes and nano-integrated platforms: multifunctional coupling for coordinated infection–regeneration intervention. (A) A MXene–M2 macrophage–derived exosome nanocomposite integrates the physicochemical attributes of a two-dimensional material with exosome-mediated immunoregulatory and pro-angiogenic signaling. By correcting hyperglycemia-associated immune dysregulation and promoting angiogenesis, this platform improves the local immune microenvironment for intervention in infection-prone diabetic wounds.98 (B) A COF–engineered exosome–integrated nanoplatform leverages a tunable framework to stabilize delivery and amplify exosome bioactivity, while adding material-enabled antibacterial and antioxidant functions for an integrated, multifunctional treatment of diabetic ulceration and infection-risk wounds.99 (C) A near-infrared (NIR)–responsive composite assembled from gold nanorods and M2-derived exosomes enables photothermally triggered rapid antibacterial activity and biofilm perturbation, synergizing with exosome-driven immunomodulation and angiogenesis to concurrently reinforce infection control and regenerative progression.100 (D) Composite nanoparticles function as integrated carriers that combine antibacterial, anti-inflammatory, and pro-angiogenic activities. Multicomponent synergy supports multitarget intervention while improving local effective exposure and temporal alignment of therapeutic actions.101 (E) An ECM-mixed hydrogel incorporating activated neutrophil exosome mimetics addresses limitations in natural exosome yield and batch consistency by using a manufacturable, high-output mimetic source, while introducing innate immune–linked antibacterial effects; the ECM component further contributes tissue compatibility and regenerative support.102 (F) Engineered nanovesicles enriched in bactericidal proteins emphasize direct neutralization or clearance of bacteria and infection-associated harmful factors/pro-inflammatory mediators, thereby dampening infection-driven inflammatory amplification and facilitating progression toward a regenerative phase.103 (G) Responsive materials and microcarriers are employed to enhance lesion-matched release and stabilize local bioactivity of exosome delivery. For example, glycyrrhizic acid hydrogel microparticles encapsulating MSC exosomes enable more controllable release under hyperglycemic conditions, prolonging effective exposure and maintaining a sustained therapeutic window.102 |
Another major direction uses composite nanoparticles as integrated carriers for antibacterial, anti-inflammatory, and pro-angiogenic functions, leveraging multicomponent synergy to achieve multi-objective intervention in infected diabetic wounds (Figure 5D).101 Meanwhile, from a source and manufacturability perspective, the introduction of exosome mimetics and immune cell-derived vesicles reflects practical needs for higher yield, functional stability, and robust antimicrobial performance in infection settings. For example, activated neutrophil exosome mimetics combined with an ECM hydrogel aim to mitigate limitations in exosome yield and batch variability while incorporating innate immune-associated antibacterial effects to support infected wounds (Figure 5E).102 Engineered nanovesicles enriched in bactericidal proteins further advance the concept of “molecular debridement”, emphasizing direct antimicrobial activity and removal of infection-associated detrimental factors (Figure 5F).103
In the context of drug-loaded exosomes, antibiotic-loaded formulations (eg, gentamicin-loaded exosomes) represent a plausible strategy to improve infection control by enhancing local drug enrichment while reducing systemic exposure, effectively extending exosomes from passive signaling carriers to active drug-delivery units.104 Beyond small-molecule loading, nucleic acid delivery via exosomes is also entering the diabetic wound arena. For instance, milk-derived exosomes delivering siRNA targeting KEAP1 modulate oxidative stress through the Keap1/Nrf2 pathway and promote angiogenesis and repair, highlighting an alternative advantage of scalable sourcing combined with programmable function.105 Other approaches, such as glycyrrhizic acid hydrogel microparticles encapsulating MSC exosomes and glucose-responsive hydrogels carrying exosomes, address the constraints imposed by hyperglycemic microenvironments on release kinetics and therapeutic efficiency at the carrier-material level (Figure 5G).106,107
Collectively, these studies illustrate a broader transition in which exosomes are evolving from relatively passive bioactive signal carriers into designable, programmable therapeutic units. Through engineered loading (small molecules or nucleic acids), manufacturability supplementation via exosome mimetics or immune cell-derived vesicles, and functional coupling with inorganic/two-dimensional or triggerable responsive materials, exosome-based therapies gain expanded capacity for phase-matched, multi-target synergy. This shift provides greater therapeutic programmability for concurrent infection control and tissue regeneration (Table 4).
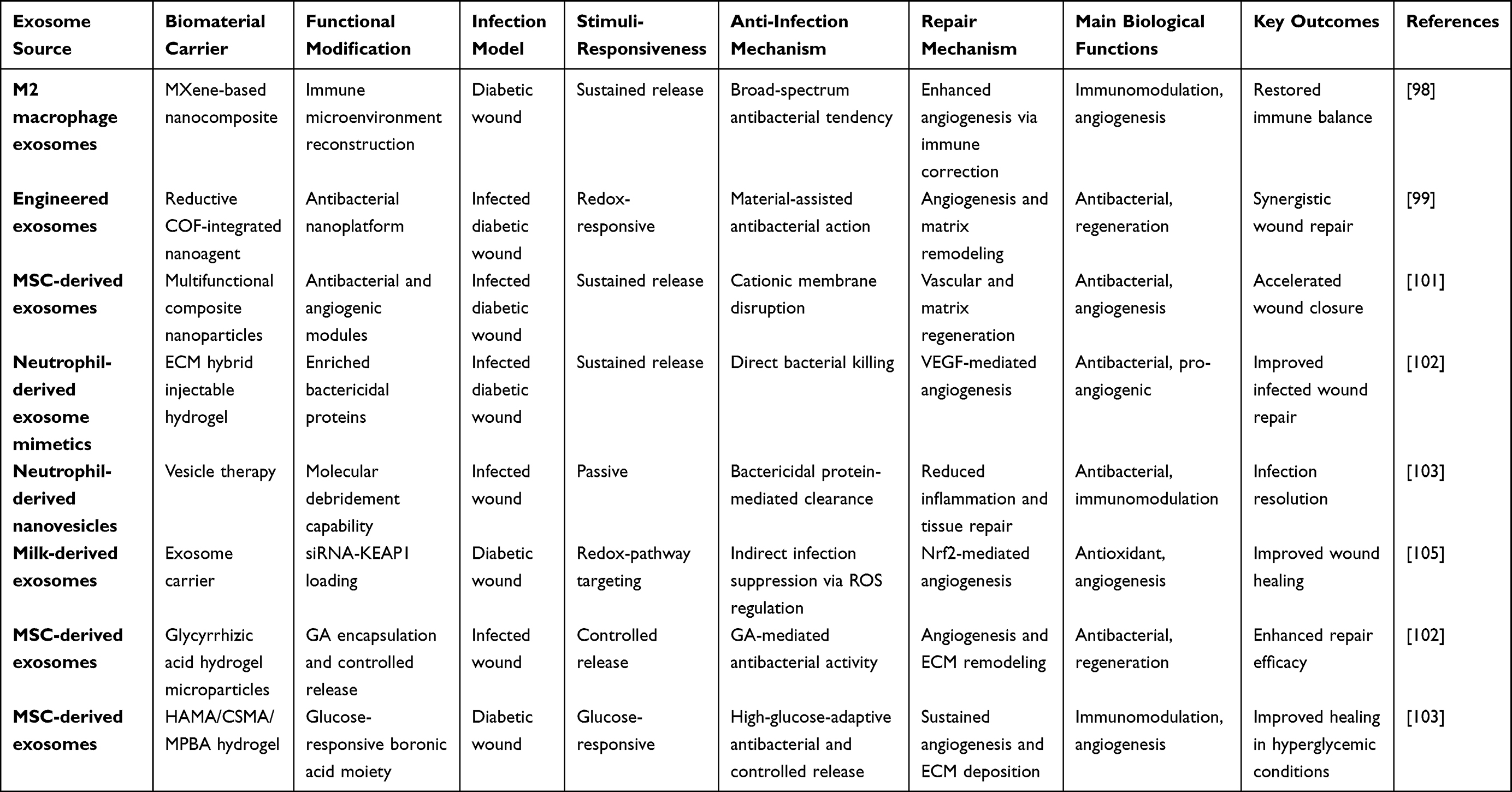 |
Table 4 Engineered Exosomes and Nano-Integrated Multifunctional Platforms |
Comparison of Biomaterial Platforms for Exosome Delivery
The preceding sections highlight that biomaterials should not be viewed merely as passive carriers for exosomes, but as therapeutic interfaces that determine where, when, and how exosomal signals are presented within diabetic infected wounds. The key distinction among different biomaterial platforms lies not only in their composition, but also in the delivery problems they are designed to solve. Hydrated networks such as hydrogels primarily address the rapid loss, dilution, and proteolytic degradation of exosomes by improving local retention and enabling sustained release. Hydrogel-based exosome systems have therefore been widely explored for diabetic wound repair because they can combine vesicle protection with moist wound management and conformal wound coverage.108 However, this advantage is often counterbalanced by limited mechanical robustness, unstable adhesion in highly exudative wounds, and batch variability when naturally derived polymers are used. Thus, hydrogels are best understood as retention- and release-oriented platforms rather than universally applicable solutions.
By contrast, microneedle patches, films, membranes, cryogels, porous scaffolds, and nano-integrated systems each occupy different positions along the axes of delivery depth, structural support, operational simplicity, and biological functionality. Microneedles can overcome the superficial distribution of topically applied exosomes by enabling localized intradermal or intratissue deposition, but their utility may decrease in large, deep, fragile, or heavily infected wounds where patch fixation and reliable insertion are difficult. Membrane and film-like dressings are more compatible with routine clinical wound care because they provide barrier protection, reduce external contamination, and simplify dressing handling, yet they generally offer weaker control over deep delivery and active microenvironmental remodeling. Porous scaffolds and cryogels provide a more durable three-dimensional niche for exudate management, gas exchange, cellular infiltration, and prolonged release, making them conceptually attractive for hypoxic or highly exudative chronic wounds. Their greater structural complexity, however, may complicate storage, sterilization, bedside application, replacement, and scale-up.
A more critical issue is whether increasingly complex biomaterial systems necessarily translate into better therapeutic platforms. Nanocomposite and stimulus-responsive materials can integrate antibacterial, antioxidant, photothermal, pH-responsive, ROS-responsive, or glucose-responsive functions with exosome-mediated immunomodulation and regeneration. Such designs are particularly relevant to infected diabetic wounds, where bacterial burden, oxidative stress, hypoxia, and impaired tissue repair coexist. Engineered MSC-derived exosome strategies have increasingly been combined with biomaterials to overcome poor targeting, rapid clearance, low local concentration, and limited exosome yield.109 Nevertheless, functional integration also raises the translational threshold. Each additional module may introduce new uncertainties related to long-term biosafety, degradation-product toxicity, immune response, manufacturing reproducibility, regulatory classification, and cost-effectiveness. Therefore, a highly multifunctional system is not necessarily superior to a simpler platform if its added functions do not match the dominant pathological barrier of the target wound.
From a translational perspective, the selection of biomaterials for exosome delivery should shift from a material-centered strategy to a wound-phenotype-oriented strategy. Irregular and moderately exudative wounds may benefit most from adhesive or injectable hydrogels that prioritize retention and sustained release. Superficial or localized wounds may be more suitable for microneedle-based delivery when controlled tissue penetration is required. Wounds requiring frequent nursing care may favor membrane or film dressings because of their handling simplicity and barrier function. Hypoxic, highly exudative, or structurally unstable wounds may require porous scaffolds or cryogels that provide fluid handling, oxygen exchange, and mechanical support. In contrast, wounds dominated by bacterial biofilm, excessive ROS, or dynamic pH/glucose changes may justify the use of responsive or nanocomposite platforms. This scenario-based framework helps avoid the assumption that the most complex material is the most effective one and instead emphasizes rational matching between wound pathology, exosome function, material properties, and clinical workflow. In brief, for irregular and moderately exudative wounds, injectable or self-healing hydrogels are preferred due to conformal coverage and sustained retention; for superficial wounds requiring localized intradermal delivery, microneedle patches offer better penetration; for wounds needing frequent nursing care, membrane or film dressings provide simplicity and barrier protection; for hypoxic or highly exudative wounds, porous scaffolds or cryogels enable exudate management and gas exchange; and for wounds dominated by biofilm or excessive ROS, responsive or nanocomposite systems, despite higher translational complexity, provide on-demand multi-target synergy.
Synergistic Anti-Infective and Reparative Mechanisms of Exosome–Biomaterial Combinatorial Therapies
Infected diabetic wounds—particularly diabetic foot infection—exhibit a convergence of pathological features, including high bacterial burden with biofilm homeostasis, increased exudation, persistent hypoxia, elevated oxidative stress, and dysregulated immune responses. These characteristics impose an intrinsically “dual-objective” therapeutic architecture: rapid suppression of the pathogen niche and interruption of infection-amplifying loops at the early stage, followed by restoration of immune–regenerative coupling to drive vascularization and structural tissue reconstruction in subsequent phases. Consequently, synergy in exosome–biomaterial combination strategies should not be viewed as a simple additive overlay of exosomal and material functions. Rather, it reflects division of labor and coordinated coupling within the same spatial domain: biomaterials provide immediately deployable and tunable antibacterial/anti-biofilm pressure and microenvironmental correction, whereas exosomes—operating under a reduced infectious burden—reshape immune trajectories and sustain pro-angiogenic, pro-matrix remodeling, and pro-epithelialization signaling. Together, these mechanisms reduce relapse risk while improving reconstruction quality and the predictability of healing outcomes (Figure 6).
 |
Figure 6 Evolution of combined exosome and biomaterial application in the treatment of diabetic infected wounds and its synergistic intervention mechanisms. The top section of the figure first highlights the severe challenges faced in treatment, namely the complex, hostile microenvironment formed by bacterial biofilm colonization (eg, MRSA), excessive accumulation of reactive oxygen species (ROS), pro-inflammatory cytokine storms, tissue hypoxia, and immune imbalance dominated by M1 macrophages. The central area compares two different strategic pathways: the traditional static delivery model, which treats biomaterials merely as passive exosome carriers that rely on diffusion to achieve local retention, resulting in relatively singular efficacy, versus the current approach, which has evolved into a dynamic, multifunctional responsive platform. This platform not only enables on-demand exosome release through ROS or pH-responsive mechanisms specific to the infection microenvironment, but also integrates the antimicrobial properties of the material itself (eg, using MXene or EGCG to interfere with bacterial membranes) along with engineered exosomes that carry targeted nucleic acids or signaling molecules. The lower part of the figure clearly elucidates the infection treatment-tissue regeneration synergistic advantage produced by this multifunctional platform: by first achieving pathogen clearance to reduce the infection load, followed by ROS clearance and oxygen supply to reconstruct the microenvironment, the engineered exosomes correct immune dysfunction, promote macrophage polarization to the repair-promoting M2 phenotype, and, ultimately, drive robust angiogenesis and high-quality matrix remodeling based on immune rebalancing, thereby accelerating the high-quality regenerative healing of diabetic chronic wounds. |
Synergistic Anti-Infective Mechanisms in Exosome–Biomaterial Systems
The refractoriness of infected diabetic wounds reflects not only pathogen burden, but also diabetes-driven defects in local immune clearance and delayed execution of reparative programs. Together, these host–pathogen constraints stabilize an infection-permissive niche marked by enhanced bacterial adhesion, biofilm persistence, and self-sustaining inflammation. In this context, exosome–biomaterial combinations are increasingly designed as a staged, mechanistically coupled intervention: biomaterials provide early, controllable antibacterial and anti-biofilm pressure to open a lower-burden therapeutic window; immune cell–derived or engineered vesicles can add innate-like clearance functions to accelerate removal of pathogens and damage-associated inflammatory cues; and microenvironment-responsive release architectures align dosing intensity with the evolving infection trajectory, enabling phase-tailored delivery while exosome-mediated immune reprogramming restores host-level anti-infective competence and shifts the system from external killing toward infection-niche correction.
Direct Bactericidal and Anti-Biofilm Effects: Biomaterial-Enabled Rapid Control as the Foundation for Synergy
In most combinatorial designs, direct antimicrobial intervention is placed at the front end of the therapeutic sequence to rapidly reduce bacterial load, destabilize biofilms, and attenuate inflammatory drivers, thereby enabling a more controllable window for exosome-mediated immune remodeling and regenerative progression. Photothermal modules represent a prototypical “instant-on” bactericidal modality. When M2-derived exosomes are integrated into a photothermal hydrogel, near-infrared irradiation induces localized hyperthermia that rapidly damages bacteria and perturbs biofilm architecture. In the subsequent phase, M2-exosome-driven anti-inflammatory and pro-angiogenic effects further reduce tissue injury and mitigate inflammation amplification, establishing a continuous chain spanning bacterial control, tissue protection, and regenerative initiation.100 In contrast, metal-ion strategies emphasize sustained antimicrobial pressure. For example, gallium ion–composited sponge scaffolds interfere with bacterial metal metabolism to impose long-term antibacterial constraints, while exosomes promote neovascularization and matrix remodeling, thereby coupling infection control with reparative advancement in a directionally aligned manner.96
Beyond photothermal and metal-ion approaches, antimicrobial polymers and bioactive small molecules are often incorporated to provide relatively mild yet persistent suppression, reducing the probability of recolonization and stabilizing the wound ecosystem. A self-healing injectable hydrogel incorporating ε-poly-L-lysine and matrine can inhibit bacterial re-adhesion via membrane-disruptive and microenvironment-modulating actions, synergizing with exosome immunoregulation to facilitate the transition from inflammation to proliferation.84 Glycyrrhizic acid hydrogel microparticles can function as an exosome depot while conferring anti-inflammatory/antimicrobial properties, reducing infectious pressure without compromising exosome-driven angiogenesis and tissue remodeling capacity.106 Antibiotic-loaded exosomes further reflect a strategy of enhanced local enrichment with reduced systemic exposure; for instance, gentamicin-loaded exosomes increase drug accumulation at the infection focus while lowering systemic burden, thereby creating a “cleaner” microenvironment for subsequent regeneration and offering a conceptual basis for dose-sparing without loss of efficacy under antimicrobial-resistance concerns.104 Meanwhile, membrane-based dressings provide an additional synergy paradigm through combined barrier and antimicrobial functions: chitosan-based nanomembranes incorporating plant-derived nanovesicles leverage barrier effects to reduce contamination and adhesion opportunities while using naturally derived bioactivity to attenuate inflammation and support repair.91
Importantly, biofilm formation markedly increases the likelihood of antimicrobial failure in infected diabetic wounds. Accordingly, an increasing number of systems introduce functional moieties that interact with bacterial surface charge or membrane structure to reduce adhesion and destabilize biofilm integrity. In an adaptive hydrogel designed for MRSA-infected diabetic wounds, charged groups confer intrinsic antibacterial effects through membrane interaction while infection-associated cues (eg, ROS) trigger exosome release. This design couples antimicrobial pressure with release kinetics, enabling tighter matching between infection severity and therapeutic intensity within a single platform.80
Immune Cell–Derived Vesicles: Innate Antibacterial Programs and “Molecular Debridement”
Beyond MSC-derived exosomes, immune cell–derived vesicles are increasingly explored in infected wound settings, with their central contribution being the introduction of clearance mechanisms more closely aligned with innate immunity. This enables more direct pathogen killing and removal of virulence-associated mediators during the early phase of infection control. Neutrophil-derived exosome mimetics or engineered nanovesicles are often naturally enriched in bactericidal proteins, generating localized bactericidal pressure accompanied by reduced inflammatory mediator levels—supporting the concept of “molecular debridement”.102,103 Compared with the typical MSC-exosome functional spectrum, which tends to emphasize immunoregulation and regeneration, immune cell–derived vesicles prioritize clearance, detoxification, and removal of key blocks to resolution. Mechanistically, they may accelerate the transition out of the locked state characterized by persistent inflammation and recurrent infection.
In practice, activated neutrophil-derived exosome mimetics/vesicles supported by material carriers (eg, ECM-mixed hydrogels) can extend residence time and increase local effective concentration, enabling bacterial control while preserving the requirements for angiogenesis and tissue reconstruction.102 Further engineered neutrophil nanovesicles broaden “molecular debridement” beyond bacterial removal to encompass clearance of necrosis-associated debris, virulence factors, and pro-inflammatory mediators that sustain chronic infection.103 When combined with ECM hydrogels or growth-factor systems, such vesicles often enhance antimicrobial outcomes while promoting vascularization and tissue rebuilding, suggesting distinctive mechanistic advantages in bridging infection control to repair. More broadly, these findings reinforce a key principle: therapeutic success in infected diabetic wounds depends less on maximal bactericidal intensity per se than on simultaneous relief of the infection niche’s dual suppression of immune competence and regenerative programming.
Responsive Release: Infection Microenvironment–Triggered on-Demand Dosing
Infected diabetic wounds provide multiple endogenous trigger signals that can be leveraged for responsive delivery, including elevated ROS, acidic pH, increased bacterial-associated molecules/enzymes, and hyperglycemia. The mechanistic value of responsive release lies in reconciling two competing needs: high-intensity antimicrobial and immunomodulatory intervention during the infection peak to suppress the pathogen niche, and a subsequent reduction in stimulation with a shift toward gentler, remodeling-oriented delivery once infection subsides, thereby avoiding excessive stress that may impede regeneration.
An adaptive exosome-releasing hydrogel for MRSA-infected diabetic wounds exemplifies this strategy. The material phase provides intrinsic antibacterial and biofilm-weakening effects via charged moieties, while infection-associated cues such as ROS induce network changes that accelerate exosome release on demand, aligning release kinetics with infection severity.80 Similarly, self-healing injectable hydrogels employ pH responsiveness to adapt to acidic inflammatory/infectious microenvironments and achieve co-delivery of antimicrobial polymers/small molecules with exosomes.84 Glucose-responsive hydrogels use hyperglycemia as a trigger variable, aiming to maintain more appropriate local concentration and release rhythms under high-glucose conditions associated with infection susceptibility.107
In addition to endogenous triggers, exogenous triggers can be used to couple clinical operations with release control. For example, sprayable–photocurable systems can rapidly conform to irregular wounds, with curing conditions tuning network architecture and degradation to achieve more predictable sustained release while reducing dressing-change frequency and thus secondary contamination risk.87 In device-enabled delivery systems, microneedle patches improve local deposition efficiency via spatially structured delivery, reducing washout by exudates; when combined with bacteria-responsive modules, they further enable a closed-loop mode in which release intensifies upon infection emergence.89,90,92 Overall, responsive release is not merely a controlled-release tactic; it operationalizes infection-course dynamics into programmable modulation of therapeutic intensity, improving the reliability of combined infection suppression and regenerative progression.
Immunomodulation: Exosome-Dominated Indirect Anti-Infective Mechanisms
In infected diabetic wounds, persistence is often not determined solely by bacterial load but is tightly linked to immune dysregulation. Convergent evidence indicates that exosomes can downregulate pro-inflammatory mediators, shift macrophages from a sustained M1-like inflammatory state toward an M2-like reparative phenotype, and improve endothelial function and angiogenesis. Through these effects, exosomes restore local anti-infective resilience and reduce the probability of infection chronicity. Even when studies do not employ strict bacterial inoculation models, improvements in the infection-prone microenvironment of diabetic wounds can serve as mechanistic evidence supporting indirect anti-infective benefit.
For example, studies on hUCMSC-derived exosomes for diabetic wound repair often highlight attenuation of oxidative stress, promotion of angiogenesis, and improvement of inflammatory status, collectively reducing the risk of secondary infection associated with prolonged wound openness.110 An ADSC-exosome plus ECM hydrogel system similarly reflects a logic in which inflammation reduction, angiogenesis enhancement, and barrier reconstruction shorten the infection-susceptible window.79 Endothelial cell exosomes combined with an ADM composite hydrogel further emphasize perfusion restoration and structural remodeling, thereby strengthening infection resistance via microenvironmental improvement.81
In work emphasizing correction of immune imbalance, MXene–M2 exosome nanocomposites are used to reconstruct hyperglycemia-induced immunosuppression while promoting angiogenic repair, based on the notion that the diabetic state features coexisting immunosuppression and chronic inflammation that compromises bacterial clearance; immune microenvironment remodeling can therefore mechanistically suppress infection persistence.98 The “fate reversal” strategy further elevates immune restoration as a central anti-infective pillar, combining exosome-driven macrophage functional recovery with bacteria-responsive release modules, shifting the anti-infective paradigm from exogenous sterilization toward a dual-engine approach of host immune restoration plus targeted antibacterial intervention.90 Collectively, these data suggest that the critical anti-infective contribution of exosomes is not direct bactericidal activity, but the reprogramming of immune trajectories and reconstruction of tissue barriers that systemically reduce relapse vulnerability.
Microenvironmental Reprogramming: From Bacterial Killing to Correction of the Infection Niche
Beyond direct antimicrobial effects, a parallel core pathway in combinatorial systems involves correction of the infection microenvironment. In diabetic wounds, persistently high ROS, hypoxia, and chronic inflammation not only directly damage tissue and delay repair but also markedly impair phagocyte bactericidal capacity and angiogenic efficiency, thereby sustaining an ecosystem favorable to bacterial colonization and biofilm stability. Hypoxia and ROS overload can be viewed as key amplifiers of infection persistence: hypoxia reduces immune-cell killing efficiency and suppresses angiogenesis, while ROS overload induces cell death, barrier disruption, and sustained inflammation, ultimately promoting bacterial adhesion and biofilm maintenance.
Accordingly, multiple studies couple oxygenation/antioxidant modules with exosome delivery—not merely to accelerate healing, but to weaken the conditions that sustain the infection niche via microenvironmental resetting. The OxOBand cryogel integrates sustained oxygen release with antioxidant/antibacterial background functions and exosome-driven regenerative signaling, providing an integrated intervention against reinforcing pathological loops linking hypoxia, oxidative stress, and infection; robust composite benefits have been observed in diabetic and infected wound models.94,111 A programmable microalgae gel further combines photothermal bacterial control, photosynthetic oxygenation, and antioxidant vesicle release, suggesting that the coupling among oxygen supply, immune functional recovery, and infection control can be engineered and amplified.83
At the pathway level, milk-derived exosomes delivering siRNA targeting KEAP1 reduce oxidative stress by modulating Nrf2-associated antioxidant responses, thereby improving the infection-prone microenvironment and promoting repair.105 Phase-tailored release strategies for oxidative diabetic wounds (eg, timed release of exosomes and FGF) similarly highlight that regenerative signaling output is more effective under an attenuated oxidative-stress context, reducing the long-term constraints imposed by persistent inflammation and infection risk.95 Relatedly, engineered exosomes combined with reductive COF nanoagents and multifunctional composite nanoparticle systems integrate antioxidant, immunomodulatory, and antibacterial modules at different levels, increasing the certainty of transition from inflammation to regeneration in infected wounds.99,101 A study using a polyphenol-modulated microporous soy protein injectable hydrogel loaded with placental stem cell exosomes underscores that structural and chemical microenvironment engineering can jointly establish a low-inflammation, pro-regenerative niche, supporting chronic wound repair while alleviating infection-associated blockage.82 A pH/ROS dual-responsive hydrogel–exosome combination (in a diabetic oral ulcer model) further indicates that concurrent regulation of ROS overload and acidification can weaken inflammation–infection amplification loops and promote regeneration,85 while a pH-responsive system delivering preconditioned MSC exosomes suggests that enhancing exosome potency together with microenvironment-triggered release may yield more stable efficacy under high oxidative/inflammatory burden.86 Overall, the mechanistic framework of this direction is shifting from competition over bactericidal strength toward ecological niche reprogramming—resetting the hypoxia–ROS–inflammation network to reduce the conditions that maintain infection and thereby lowering relapse risk at a system level.
Synergistic Reparative Mechanisms of Exosome–Biomaterial Combination Therapies
The poor healing capacity of infected diabetic wounds stems from concurrent impairment across multiple core reparative nodes: inflammation fails to resolve in a timely manner and does not effectively transition from the clearance phase to the reparative phase; angiogenesis and functional reperfusion are insufficient; hypoxia and oxidative stress persist; ECM is continuously degraded and cannot be efficiently reconstructed. As a consequence, re-epithelialization is delayed, barrier restoration is protracted, and the wound remains exposed to recurrent infection risk.
Exosome–biomaterial combinations enhance the continuity and reproducibility of repair through two mechanistically complementary routes. First, biomaterials markedly improve local retention, stability, and controllable release of exosomes, allowing exosome-mediated immunoregulatory and regenerative cues to overcome the dilution and inactivation barriers typical of chronic, highly exudative wounds. Second, biomaterials provide structural support and can integrate antibacterial, antioxidant, oxygen-generating, or stimulus-responsive modules to correct hostile microenvironmental constraints, thereby shifting repair from transient stimulation toward sustained driving forces.
Reprogramming the Immune Microenvironment
In infected diabetic wounds, persistently elevated inflammation not only suppresses the functions of fibroblasts, keratinocytes, and endothelial cells but also promotes protease activation and ECM destruction, collectively preventing the initiation of effective healing at a systems level. Whether repair can enter a productive proliferative phase largely depends on a successful switch from inflammatory clearance to reparative resolution.
Embedding exosomes within hydrogel or matrix networks can substantially increase local persistence and reduce washout by exudates or rapid loss in protease-rich environments. This improved local bioavailability enables more stable immunomodulation, typically manifested as downregulation of pro-inflammatory mediators, polarization of macrophage programs toward reparative phenotypes, and earlier onset of inflammatory “ebb”. Loading exosomes into ECM- or matrix-associated hydrogels enhances local retention and amplifies anti-inflammatory and immunoregulatory effects, thereby creating a permissive context for downstream angiogenesis and re-epithelialization.79 Consistently, hUCMSC-derived exosomes promote repair by alleviating oxidative stress and improving inflammatory status, supporting the principle that maintaining an effective local concentration is a practical prerequisite for immune reprogramming.110 In an MRSA infection model, an adaptive-release hydrogel functions not only as an exosome carrier but also as a microenvironmental corrector through intrinsic antibacterial/antioxidant properties; moreover, infection-associated cues modulate the intensity of exosome release, allowing immunoregulation to dynamically align with inflammatory burden and accelerating entry into the proliferative repair phase.80
When exosome sources expand beyond MSCs to vesicles with more defined immunoregulatory states, the immune–repair axis can be further strengthened. MXene–M2 exosome composite systems emphasize correction of hyperglycemia-associated immune insufficiency together with reinforcement of reparative signaling, producing a local milieu more supportive of angiogenesis and tissue reconstruction.98 This pattern suggests that diabetic wound repair requires not only inflammation dampening, but structural correction of the coupled pathology of immune inefficacy and inflammatory persistence. The “fate reversal” strategy further couples immune functional restoration with infection-triggered therapy, reframing repair from a passive outcome after infection control into an active, linked process in which immune competence recovery and reparative program activation proceed in concert.90
Angiogenesis and Reperfusion Restoration
Diabetic wounds often display the paradoxical coexistence of inadequate neovascularization and insufficient reperfusion. This dual deficit limits oxygen and nutrient supply while weakening immune-cell recruitment and effector function, thereby increasing the likelihood of infection persistence. Accordingly, the key pro-angiogenic objective of combinatorial systems is not merely the induction of angiogenic markers, but the formation, maturation, and stabilization of a functional microvascular network capable of effective perfusion.
The advantage of exosome–material combinations lies in synchronous provision of signaling cues and structural support. Exosome-borne pro-angiogenic factors and regulatory miRNAs enhance endothelial migration and tubulogenesis, while ECM/ADM-based materials provide a permissive scaffold and microenvironmental modulation that facilitates conversion of angiogenic signaling into stable, perfusable vasculature.79,81 This principle is particularly evident in systems combining endothelial cell–derived exosomes with ADM composite hydrogels, where vascular-lineage exosomes serve as potent angiogenic signal sources and matrix composites act as supportive scaffolds and local milieu regulators, resulting in improved angiogenic outcomes and higher-quality tissue remodeling.81
In systems that emphasize therapeutic choreography, multifunctional hydrogels that temporally program the release of exosomes and FGF indicate that early stabilization of oxidative burden and the wound microenvironment can enable later-stage pro-angiogenic and matrix-rebuilding signals to translate more effectively into vascular maturation and improved repair quality.95 In hypoxia-dominant infected diabetic wounds, oxygen-releasing cryogels elevate local oxygen tension and improve cellular metabolic state, providing a more favorable baseline for exosome-driven angiogenesis and yielding more stable vascular outcomes.94,111 In addition, gallium-ion composite sponge scaffolds impose sustained antibacterial constraints while improving exudate handling and ventilation via porous architecture, which can indirectly support reperfusion and vascular recovery by alleviating hostile environmental constraints.96
Regulation of Hypoxia and Oxidative Stress
Hypoxia and oxidative stress are not merely secondary features of infected diabetic wounds; they actively perpetuate immune dysfunction, compromise cellular viability, and reinforce ECM breakdown, thereby lowering the efficiency and durability of regeneration. Persistent hypoxia limits endothelial activity and vessel maturation, while excessive ROS amplifies tissue damage, sustains inflammatory signaling, and destabilizes barrier reconstruction. Therefore, many exosome–biomaterial platforms incorporate oxygenation and/or antioxidant modules to reset these constraints, enabling exosome-mediated immunoregulation and regeneration to operate within a more permissive microenvironment.
Oxygen-releasing cryogel systems, exemplified by OxOBand, combine sustained oxygen delivery with antioxidant/antibacterial functions and exosome-driven reparative signaling, providing integrated mitigation of the hypoxia–ROS burden while supporting repair progression under infectious or infection-prone conditions.94,111 More broadly, systems that couple staged regenerative signaling with early oxidative-pressure control further highlight that improving microenvironmental “baseline conditions” is often necessary for downstream angiogenesis and structural remodeling to become durable rather than transient.95 At the molecular level, milk-derived exosomes delivering siRNA against KEAP1 activate Nrf2-associated antioxidant responses, reducing oxidative stress and improving the microenvironmental permissiveness for regeneration in diabetic wounds.105 Collectively, these approaches position hypoxia/ROS correction as a mechanistic bridge that links infection-related microenvironmental hostility to impaired regeneration, and as a practical lever for increasing the stability of exosome-enabled repair.
Matrix Remodeling and Collagen Reorganization
High-quality healing is defined not only by wound closure but by whether matrix remodeling proceeds toward ordered, functional restoration. In infected diabetic wounds, insufficient matrix synthesis often coexists with excessive degradation, resulting in fragile granulation tissue, disorganized collagen architecture, and compromised biomechanical performance.
ECM/ADM-derived matrix materials synergize with exosomes by providing structural support together with signal amplification, enabling fibroblast migration, collagen deposition, and remodeling to proceed in a manner closer to physiological repair and potentially reducing the tendency toward aberrant scarring.79,81 In dynamic network systems, self-healing injectable hydrogels maintain material integrity and provide stress buffering, reducing mechanical disruption and dressing-change–associated damage to nascent tissue. Meanwhile, exosomes and co-delivered agents (eg, matrine, ε-poly-L-lysine) reduce inflammatory and infectious pressure, indirectly mitigating protease-driven matrix destruction and supporting more sustained collagen deposition and reorganization.84 A microporous soy-protein injectable hydrogel improves cellular infiltration and nutrient exchange through its porous architecture; together with polyphenol-mediated modulation that lowers local inflammation and degradation pressure, it establishes a more favorable niche for placental stem cell exosomes to promote granulation formation and matrix rebuilding.82 Additionally, depot-like systems such as glycyrrhizic acid hydrogel microparticles and glucose-responsive hydrogels prolong the exosome action window, shifting matrix remodeling from episodic stimulation to sustained driving—an approach well aligned with the long-term correction needed for hyperglycemia-associated imbalance between matrix synthesis and degradation.106,107
Re-Epithelialization and Barrier Restoration
The rate of re-epithelialization determines the duration of wound exposure; prolonged exposure increases susceptibility to secondary infection and relapse. In this phase, combination systems offer advantages through both biological and operational mechanisms: exosomes promote keratinocyte migration/proliferation and improve the inflammatory milieu, whereas biomaterials manage the wound surface environment, mechanical disturbance, and dressing-change frequency.
Sprayable exosome hydrogels can rapidly conform to irregular wounds and form a protective layer; photocrosslinking allows tuning of release profiles and dressing stability, reducing dressing-change frequency and mechanical disruption and thereby supporting continuous epithelial migration.87 Microneedle delivery systems enhance intratissue deposition by bypassing surface barriers, enabling more effective action at the epidermal–dermal interface to accelerate re-epithelialization while synchronizing with angiogenic progression.89 In infection-oriented device platforms, microneedle patches integrating multimodal anti-infective functions can rapidly advance barrier reconstruction once infectious pressure decreases, tightening the temporal coupling between infection control and barrier recovery.92 Chitosan nanomembranes incorporating plant-derived nanovesicles provide barrier protection while reducing bacterial adhesion and inflammatory escalation via natural bioactive components, supporting epithelial and granulation reconstruction.91 A dual-responsive exosome hydrogel (pH/ROS) in a diabetic oral ulcer model further suggests that reducing ROS burden and inflammatory load can substantially improve epithelial regeneration efficiency, offering mechanistic insights transferable to infection-associated cutaneous wounds.85 Likewise, pH-responsive delivery of preconditioned MSC exosomes indicates that combining enhanced exosome potency with on-demand release can help preserve the continuity of epithelialization and tissue remodeling under hostile microenvironmental conditions.86
Taken together, synergistic repair in exosome–biomaterial combinations can be distilled into a reusable mechanistic chain. By enhancing local retention and controllable release of exosomes, providing structural support, and correcting hostile factors such as hypoxia and oxidative stress, biomaterials enable sustained expression of exosome-mediated immunoregulation, angiogenesis promotion, matrix rebuilding, and re-epithelialization. As a result, these platforms can achieve faster closure and higher-quality tissue reconstruction even under conditions where infectious pressure persists or fluctuates.
Clinical Evidence, Ongoing Trials, and Translational Perspectives
Current Clinical Evidence and Evidence Gaps
Although exosome–biomaterial combinatorial systems have demonstrated encouraging therapeutic effects in diabetic infected wound models, most current evidence remains derived from in vitro experiments and small-animal studies. These studies are predominantly proof-of-concept investigations in rodent models, whereas large-animal model validation (eg, diabetic pigs) remains very limited. These preclinical investigations have provided important mechanistic support showing that exosome-loaded hydrogels, microneedle patches, cryogels, nanomembranes, and scaffold systems can regulate macrophage polarization, suppress excessive inflammation and oxidative stress, enhance angiogenesis, remodel the ECM, and accelerate re-epithelialization. However, direct clinical evidence specifically evaluating exosome–biomaterial combination platforms in infected DFU remains limited. Accordingly, current evidence supports the biological plausibility and translational promise of exosome–biomaterial platforms, while also underscoring the need for rigorous clinical validation before their efficacy can be generalized to infected DFU.
A critical prerequisite for interpreting this evidence is the precise use of extracellular vesicle nomenclature. In the literature, the terms “exosomes”, “small extracellular vesicles”, “microvesicles”, “engineered nanovesicles”, and “exosome mimetics” are sometimes used interchangeably, although they represent biologically and technically distinct entities. Exosomes are generally referred to as small extracellular vesicles, typically within the range of approximately 30–150 nm, that originate from the endosomal pathway and are released after the fusion of multivesicular bodies with the plasma membrane. They are enriched in regulatory RNAs, proteins, lipids, and signaling molecules, and are commonly associated with intercellular communication, immunomodulation, angiogenesis, and tissue repair. By contrast, microvesicles, also termed ectosomes in some contexts, are usually larger vesicles generated by outward budding and shedding of the plasma membrane. Their cargo composition may more directly reflect the plasma membrane and cytoplasmic status of parental cells, and they often show broader size and functional heterogeneity.112
Engineered nanovesicles and exosome mimetics should also be distinguished from naturally secreted exosomes. Engineered nanovesicles are vesicle-based systems modified through genetic, chemical, physical, or membrane-engineering approaches to improve targeting, cargo loading, stability, or therapeutic programmability. Exosome mimetics are artificially generated vesicle-like particles, commonly produced by extrusion, sonication, microfluidics, or cell membrane-derived methods, and are often developed to overcome the low yield and batch variability of natural exosomes. Although these systems may reproduce certain structural or functional features of exosomes, they should not be considered biologically identical to naturally secreted exosomes. Similarly, plant-derived vesicle-like nanoparticles and platelet-derived vesicle products may possess bioactive components and practical advantages for topical wound applications, but their active cargo attribution, dose equivalence, and quality-control criteria remain less standardized. Therefore, throughout exosome-based wound research, vesicle terminology should be defined according to biogenesis, preparation method, physical characterization, molecular markers, and functional properties, rather than being used as interchangeable labels.113
Despite the above terminology-related limitations, early clinical exploration of extracellular vesicle- or exosome-based therapies for DFU has begun to emerge. A randomized, double-blind, placebo-controlled clinical study registered as NCT06812637 evaluated Wharton’s jelly mesenchymal stem cell-derived exosome gel combined with standard care in patients with DFU. A related published clinical report described 110 patients with persistent DFU and showed that topical WJ-MSC-derived exosome treatment was associated with improved wound closure and shorter time to complete epithelialization compared with control groups.114 In addition, NCT06825884 investigates extracellular microvesicles as direct perilesional injections for chronic DFU that failed to heal after standard care. Another relevant translational direction is represented by NCT06319287, a phase 2a multicenter randomized controlled study evaluating topically applied purified exosome product combined with TISSEEL fibrin sealant in subjects with non-healing DFU.
These clinical studies are encouraging because they indicate that extracellular vesicle-based wound therapies are entering human evaluation. Nevertheless, they also highlight several important evidence gaps. First, most available clinical studies involve exosome gels, extracellular microvesicle injections, or platelet-derived exosome products, rather than the more complex multifunctional exosome–biomaterial systems discussed in this review, such as ROS-responsive hydrogels, photothermal nanocomposites, oxygen-releasing cryogels, antimicrobial microneedle patches, or engineered exosome–nanomaterial platforms. Second, clinical trials have generally focused on chronic non-healing DFUs, whereas infected DFUs, biofilm-associated wounds, multidrug-resistant bacterial infections, and osteomyelitis-prone ulcers remain insufficiently investigated. Third, standardized clinical endpoints are still needed. Future studies should not only assess wound closure rate and epithelialization time, but also include infection recurrence, bacterial burden, biofilm clearance, amputation rate, pain, patient-reported quality of life, cost-effectiveness, and long-term recurrence.
In addition to technology-related evidence gaps, patient heterogeneity is a central determinant of therapeutic response and should be incorporated into future trial design. Patients with DFU differ substantially in age, frailty, diabetes duration, glycemic control, nutritional status, renal function, cardiovascular disease burden, peripheral neuropathy, peripheral artery disease, immune status, infection severity, ulcer duration, ulcer depth, wound area, microbiological profile, and offloading adherence. These factors may influence multiple biological processes relevant to exosome–biomaterial therapy, including local perfusion, vesicle retention, inflammatory response, macrophage polarization, angiogenic capacity, bacterial clearance, matrix remodeling, and epithelial migration. For example, ischemic ulcers with severe peripheral artery disease may respond less effectively to pro-angiogenic or regenerative vesicle signals unless perfusion is restored, whereas patients with renal dysfunction, poor glycemic control, malnutrition, or systemic inflammation may have persistent oxidative and inflammatory stress that weakens reparative responses.115,116
Therefore, future clinical studies should move beyond simple enrollment based on the presence of DFU alone and adopt more refined stratification or enrichment strategies. Trial designs should consider stratifying patients according to infection severity, ischemia status, neuropathy, renal function, HbA1c, wound size, ulcer depth, ulcer duration, microbiological findings, vascular perfusion, and prior amputation history. Classification systems such as IWGDF/IDSA infection severity grading, Wagner or University of Texas wound classification, and perfusion-related parameters including ankle-brachial index, toe pressure, skin perfusion pressure, or transcutaneous oxygen pressure may help define more homogeneous study populations. Preplanned subgroup analyses and patient-centered endpoints will be important for identifying which patient populations are most likely to benefit from specific exosome–biomaterial platforms. Thus, although early clinical signals support the feasibility of extracellular vesicle-based therapy for diabetic wounds, the clinical translation of exosome–biomaterial combination platforms remains at an early stage and requires more rigorous, patient-stratified validation.
Translational Perspectives
Scalable Manufacturing, Quality Control, and Product Stability
The first major translational barrier is scalable and reproducible manufacturing. Conventional exosome isolation methods, including ultracentrifugation, density-gradient centrifugation, precipitation, and membrane filtration, are useful in laboratory research but may be difficult to standardize for clinical-grade production because of limited yield, variable purity, long processing time, and operator-dependent variability. For future clinical translation, upstream production should move toward standardized donor selection, well-characterized cell banks, serum-free or xeno-free culture conditions, and scalable expansion systems such as hollow-fiber bioreactors, three-dimensional culture, or suspension-compatible platforms. Downstream purification may require more clinically compatible approaches, including tangential flow filtration, size-exclusion chromatography, ion-exchange chromatography, or integrated purification workflows that can preserve vesicle integrity while reducing protein aggregates, nucleic acid contaminants, serum-derived particles, and endotoxin burden.117,118
Standardization is equally important because exosome potency is not determined solely by particle number. Source cell type, donor variability, cell passage, culture medium, oxygen tension, inflammatory preconditioning, isolation strategy, and storage condition can all influence vesicle cargo composition and biological activity. Achieving true scalability and batch-to-batch consistency requires not only standardized production protocols but also consensus on dose metrics (eg, particle number vs. protein content vs. functional units) and release specifications, which are currently lacking. Therefore, future studies should report not only particle concentration, size distribution, morphology, and canonical vesicle markers, but also purity, protein-to-particle ratio, residual host-cell DNA or RNA, endotoxin level, sterility, mycoplasma status, and batch-to-batch consistency. Functional potency assays are particularly important for exosome-based wound products. Depending on the intended therapeutic mechanism, these assays may include macrophage polarization, suppression of pro-inflammatory cytokines, endothelial tube formation, fibroblast migration, keratinocyte proliferation, ROS-scavenging capacity, collagen deposition, or antibacterial and anti-biofilm activity. For engineered exosomes, additional characterization should include loading efficiency, cargo stability, surface modification consistency, and off-target biological activity.119
For exosome–biomaterial combination products, quality control is even more complex. Biomaterial incorporation can alter exosome stability, release kinetics, cellular uptake, and biological potency. Therefore, evaluation should include encapsulation efficiency, spatial distribution of exosomes within the material, release profile under diabetic wound-relevant conditions, mechanical strength, swelling behavior, degradation kinetics, injectability or adhesiveness, sterilization compatibility, and preservation of exosome bioactivity after material loading. For stimuli-responsive systems, additional validation is needed to prove that release behavior is truly triggered by wound-relevant signals such as acidic pH, elevated ROS, high glucose, bacterial enzymes, or inflammatory mediators. These parameters are essential for transforming exosome-loaded biomaterials from experimental platforms into reproducible therapeutic products.
Storage stability and distribution also represent critical but often under-discussed issues. Extracellular vesicles may aggregate, lose membrane integrity, undergo cargo degradation, or show reduced biological potency during freezing, lyophilization, long-term storage, transportation, or repeated freeze–thaw cycles. Although cryoprotectants, lyoprotectants, and optimized buffer systems may improve stability, their effects on vesicle bioactivity, immunogenicity, and material compatibility must be carefully evaluated. When exosomes are incorporated into hydrogels, microneedles, cryogels, nanomembranes, or scaffold dressings, storage may also affect material structure, release behavior, sterility, and mechanical performance. Therefore, clinically relevant products should define shelf life, storage temperature, acceptable freeze–thaw cycles, reconstitution procedures, and ready-to-use or bedside-preparation feasibility. For chronic diabetic wounds, where repeated administration and frequent dressing changes may be required, storage stability and practical usability will strongly influence clinical adoption.120
Biosafety, Ethical Considerations, and Regulatory Pathways
Biosafety evaluation should be strengthened before exosome–biomaterial strategies can be broadly applied in patients with diabetic skin infections. Although exosomes are generally considered less tumorigenic and less immunogenic than live cell therapies, their long-term safety is not fully established. Donor-derived exosomes require strict donor screening, informed consent, pathogen testing, traceability, and documentation of cell source, passage number, and production history. Allogeneic MSC-derived exosomes may carry immunomodulatory cargo that is beneficial for resolving chronic inflammation, but excessive or poorly controlled immunosuppression could theoretically impair local bacterial clearance in infected wounds. Therefore, infection-oriented applications should carefully balance inflammation resolution with preservation of host antimicrobial defense.
Engineered and multifunctional systems require additional safety considerations. Exosomes loaded with antibiotics, nucleic acids, small molecules, or gene-regulatory cargo may introduce risks related to off-target effects, uncontrolled biodistribution, unexpected immune modulation, or long-term persistence. When combined with biomaterials, the degradation products of hydrogels, microneedles, cryogels, metal ions, two-dimensional nanomaterials, photothermal agents, and nanozymes should be systematically evaluated. In infected diabetic wounds, local tissue ischemia, impaired lymphatic drainage, renal dysfunction, and repeated application may further affect biodistribution, clearance, and cumulative exposure. The long-term in vivo fate of nanomaterials—including their degradation kinetics, tissue distribution, potential accumulation in organs such as the liver and spleen, and excretion pathways—remains largely unknown for most exosome–nanomaterial composites and requires dedicated long-term biodistribution studies before clinical translation. Thus, future preclinical studies should include not only short-term wound closure outcomes, but also local irritation, systemic toxicity, biodistribution, immunogenicity, genotoxicity where relevant, reproductive toxicity if applicable, and long-term recurrence or scarring.
Ethical considerations are also important. Umbilical cord-, placenta-, adipose tissue-, and bone marrow-derived exosomes involve different donor procurement procedures and ethical requirements. Umbilical cord and placental tissues are often considered ethically acceptable when obtained after informed consent, but standardized donor screening, privacy protection, and source traceability remain essential. For autologous vesicle products, individualized production may reduce immunological risk but may increase cost, time, and manufacturing complexity. For allogeneic products, scalable production is more feasible, but batch consistency and donor-to-donor variability must be tightly controlled. Plant-derived vesicles and exosome mimetics may reduce some donor-related ethical concerns, but they introduce separate questions regarding active component attribution, dose equivalence, and cross-kingdom biological mechanisms.
Regulatory classification remains one of the most important barriers to clinical adoption. Exosome–biomaterial products may be classified as biological products, drug-delivery systems, medical devices, advanced therapy medicinal products, or combination products depending on their source, composition, manufacturing process, and principal mode of action. Products involving engineered exosomes, nucleic acid loading, antibiotic loading, photothermal nanomaterials, or responsive biomaterial carriers are likely to face more complex regulatory requirements than unmodified exosome preparations. Regulatory submissions will need to address chemistry, manufacturing, and controls; identity; purity; potency; sterility; stability; release specifications; preclinical safety; and clinically meaningful efficacy endpoints. At present, the lack of universally harmonized technical standards for extracellular vesicle-based therapeutics continues to complicate cross-study comparison, product classification, and approval pathways.121 For combined biologic-material systems (eg, exosome-loaded hydrogels or responsive nanocomposites), regulatory challenges are even greater because they do not fit neatly into existing categories of biologics, devices, or drugs; this hybrid nature demands new guidance on quality control, sterilization, stability testing, and preclinical safety evaluation, which regulatory agencies are only beginning to address.
From a translational readiness perspective, among the various exosome–biomaterial platforms discussed in this review, simple exosome-loaded hydrogels and topical exosome gels (eg, those in NCT06812637) are realistically closer to clinical application, as they build upon existing wound dressing workflows and require less regulatory complexity. In contrast, multifunctional systems incorporating photothermal nanoparticles, multi-responsive release mechanisms, or engineered exosome–nanomaterial composites, while mechanistically attractive, remain at earlier proof-of-concept stages and face substantial hurdles in scalability, sterility, and safety validation before clinical testing. Overall, exosome–biomaterial combination therapy represents a promising but still early-stage strategy for diabetic skin infections. Its clinical value will depend on whether strong preclinical mechanisms can be translated into standardized, safe, scalable, and clinically effective products. Future studies should prioritize large-animal infected wound models, head-to-head comparisons with standard wound care, GMP-compatible manufacturing, long-term biosafety testing, and multicenter randomized controlled trials. In parallel, clinical trial design should distinguish non-infected diabetic wounds from infected or biofilm-associated ulcers, stratify patients according to vascular status, infection severity, metabolic control, renal function, and wound phenotype, and include both regenerative and anti-infective endpoints. With these advances, exosome–biomaterial systems may evolve from proof-of-concept regenerative platforms into clinically applicable multifunctional interventions for refractory diabetic wounds.
Future Perspectives: Toward Mechanism-Guided and Clinically Translatable Exosome–Biomaterial Platforms
Building on current preclinical progress and emerging clinical exploration, the next stage of exosome–biomaterial therapy for diabetic skin infections should shift from empirical combination toward mechanism-guided, stage-adaptive, patient-stratified, and clinically oriented design. Rather than merely enhancing wound closure, future platforms should aim to achieve durable infection control, immune microenvironment reprogramming, functional vascular reconstruction, organized matrix remodeling, and stable barrier restoration. This shift is particularly important because diabetic infected wounds are not static lesions, but dynamic pathological ecosystems characterized by fluctuating bacterial burden, biofilm maturity, inflammatory intensity, ROS accumulation, hypoxia, glucose concentration, protease activity, impaired perfusion, and host-level comorbidity burden.
A key priority is to clarify how exosome cargo composition, biomaterial properties, wound microenvironmental cues, and patient-specific factors interact to determine therapeutic outcomes. Exosomes derived from mesenchymal stem cells, endothelial cells, macrophages, neutrophils, plant sources, or engineered vesicle systems may differ substantially in their miRNA, protein, lipid, and metabolite profiles, thereby producing distinct immunomodulatory, pro-angiogenic, antioxidant, or antibacterial effects. Meanwhile, biomaterial stiffness, porosity, degradation kinetics, surface charge, adhesiveness, and stimulus-responsiveness can markedly influence exosome retention, release behavior, cellular uptake, and biological potency. These effects may be further modified by age, vascular insufficiency, renal dysfunction, systemic inflammation, glycemic control, nutritional status, and infection severity. Therefore, future studies should move beyond descriptive efficacy evaluation and establish causal relationships among vesicle source, material design, patient phenotype, microenvironmental remodeling, and therapeutic endpoints.
The design logic of future exosome–biomaterial platforms should also evolve from simple sustained release toward phase-adaptive regulation. In infected diabetic wounds, early-stage treatment should prioritize bacterial clearance, biofilm disruption, ROS attenuation, and restoration of local immune competence. As infection burden decreases, therapeutic emphasis should gradually shift toward macrophage phenotype transition, angiogenesis, ECM reconstruction, and re-epithelialization. Multi-responsive hydrogels, microneedle patches, oxygen-generating cryogels, electroactive scaffolds, and nanocomposite dressings may provide useful platforms for achieving this temporal coordination. Ideally, next-generation systems should not only respond to single stimuli such as pH or ROS, but integrate multiple wound-specific signals to enable more precise and disease-stage-matched therapeutic release.
Another important direction is the establishment of experimental models that more faithfully reproduce the clinical complexity of diabetic skin infections. Many current studies rely on simplified diabetic wound models that do not fully capture the features of human diabetic foot infection, including polymicrobial colonization, mature biofilm formation, ischemia, neuropathy, repeated mechanical stress, peripheral vascular disease, lymphatic dysfunction, systemic metabolic instability, and multimorbidity. These gaps may partly explain why promising preclinical findings often face difficulties in clinical translation. Future studies should incorporate clinically relevant infected diabetic wound models, biofilm-associated infection, impaired perfusion, and long-term recurrence assessment. Large-animal models and standardized comparison with current standard-of-care therapies will be particularly valuable for evaluating therapeutic durability, safety, handling feasibility, and real-world applicability.
Advanced analytical technologies will further strengthen mechanism-guided and patient-stratified platform development. Single-cell sequencing, spatial transcriptomics, proteomics, metabolomics, high-resolution imaging, and lineage-tracing approaches can help reveal how exosome–biomaterial systems reshape immune cell states, endothelial cell behavior, fibroblast activation, keratinocyte migration, ECM organization, and host–pathogen interactions within infected diabetic wounds. In parallel, integration of clinical metadata, vascular assessment, infection grading, microbiological profiling, and biomarker analysis may help identify predictive signatures of treatment response and guide the rational selection of exosome sources, biomaterial carriers, and combination modules for different patient subgroups.
Overall, future development of exosome–biomaterial therapies should be guided by mechanistic precision, intelligent material engineering, disease-relevant modeling, patient stratification, and clinically meaningful validation. The ultimate goal should not be limited to faster wound closure, but should extend to durable infection suppression, functional tissue reconstruction, reduced recurrence, lower amputation risk, and improved patient-centered outcomes. By integrating biological mechanism mapping with advanced biomaterial design and rigorous translational evaluation, exosome–biomaterial platforms may progress from proof-of-concept regenerative systems toward more reliable therapeutic strategies for refractory diabetic skin infections.
Conclusion
Exosome–biomaterial combinatorial therapies provide a biologically rational strategy for diabetic skin infections because they address several core barriers of chronic infected wounds at the same time. These barriers include bacterial biofilm formation, persistent inflammation, oxidative stress, hypoxia, impaired angiogenesis, ECM degradation, and delayed epithelial restoration. In these systems, exosomes mainly provide immunomodulatory, pro-angiogenic, antioxidant, matrix-remodeling, and epithelial-regenerative signals. Biomaterials improve local retention, protect vesicle bioactivity, enable sustained or stimulus-responsive release, provide structural support, and may add antibacterial, oxygen-generating, antioxidant, or microenvironment-modulating functions. This complementary division of roles explains why exosome–biomaterial systems have shown encouraging effects on wound closure, vascularization, collagen deposition, re-epithelialization, and infection control in preclinical models.
The most important significance of this field is not simply that combined systems may accelerate wound closure, but that they offer a framework for coordinated microenvironment remodeling. Infected diabetic wounds are dynamic pathological ecosystems rather than isolated tissue defects. Effective treatment must therefore suppress pathogen persistence while also restoring host repair capacity. Among current platforms, injectable, sprayable, adhesive, and self-healing hydrogels appear particularly attractive for translation because they can conform to irregular wounds, improve exosome retention, and fit relatively well into clinical wound-care workflows. Membrane-like dressings and microneedle patches may also be clinically useful in selected wound types because of their handling convenience, barrier function, and localized delivery capacity. Moderately responsive systems that react to wound-relevant signals such as acidic pH, elevated reactive oxygen species, high glucose, or bacterial enzymes may further improve treatment precision. However, increasingly complex multifunctional platforms are not automatically superior. Their translational value will depend on whether each added module provides a clear biological benefit without creating excessive barriers in safety evaluation, sterilization, storage, manufacturing, regulatory approval, and cost control.
The current evidence should be interpreted with appropriate caution. Although exosome–biomaterial therapies have shown substantial promise in cell and animal studies, high-quality clinical evidence remains limited. Most available studies are still proof-of-concept investigations, and many use simplified wound models that do not fully reproduce the clinical complexity of diabetic foot infections, including polymicrobial colonization, mature biofilms, ischemia, neuropathy, repeated mechanical stress, vascular disease, systemic metabolic instability, and patient comorbidities. Therefore, future research should move beyond demonstrating accelerated closure in simplified models and should prioritize clinically relevant infected diabetic wound models, large-animal validation, recurrence assessment, and head-to-head comparison with standard wound care.
Several actionable priorities are essential for clinical translation. First, exosome production must be standardized with respect to source selection, donor variability, cell culture conditions, isolation methods, purity, storage, and batch consistency. Second, dose metrics should be harmonized because particle number, protein content, and cell-equivalent dose are not interchangeable. Third, potency assays should be linked to intended mechanisms of action, such as macrophage polarization, inflammatory suppression, endothelial tube formation, fibroblast migration, keratinocyte proliferation, collagen deposition, oxidative stress reduction, and antibacterial or anti-biofilm activity. Fourth, exosome–biomaterial combination products require additional quality-control parameters, including encapsulation efficiency, release kinetics, preservation of vesicle bioactivity, material degradation, mechanical properties, sterility, and responsiveness under diabetic wound-relevant conditions. Finally, regulatory classification and clinical trial design should be considered early in product development, especially for engineered exosomes, nucleic acid-loaded vesicles, antibiotic-loaded vesicles, photothermal nanomaterials, and multi-responsive biomaterial systems.
Overall, exosome–biomaterial combination therapy represents a promising but still early-stage direction for diabetic skin infections. Its future impact will depend on the ability to translate strong preclinical mechanisms into standardized, safe, scalable, and clinically effective products. The next stage of development should favor mechanism-guided, stage-adaptive, and clinically practical platforms rather than maximal material complexity. With rigorous manufacturing standards, clinically relevant validation models, long-term biosafety assessment, and well-designed controlled clinical trials, exosome–biomaterial systems may progress from experimental regenerative platforms toward clinically applicable multifunctional interventions for refractory diabetic wounds.
Acknowledgments
The authors confirm that no generative artificial intelligence (AI) tools were used in the preparation of this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. McDermott K, Fang M, Boulton AJM, Selvin E, Hicks CW. Etiology, epidemiology, and disparities in the burden of diabetic foot ulcers. Diabetes Care. 2023;46(1):209–38. doi:10.2337/dci22-0043
2. Zhang P, Lu J, Jing Y, Tang S, Zhu D, Bi Y. Global epidemiology of diabetic foot ulceration: a systematic review and meta-analysis †. Ann Med. 2017;49(2):106–116. doi:10.1080/07853890.2016.1231932
3. Armstrong DG, Tan TW, Boulton AJM, Bus SA. Diabetic foot ulcers: a review. JAMA. 2023;330(1):62–75. doi:10.1001/jama.2023.10578
4. Rice JB, Desai U, Cummings AKG, Birnbaum HG, Skornicki M, Parsons NB. Burden of diabetic foot ulcers for medicare and private insurers. Diabetes Care. 2014;37(3):651–658. doi:10.2337/dc13-2176
5. Ramirez-Acuña JM, Cardenas-Cadena SA, Marquez-Salas PA, et al. Diabetic foot ulcers: current advances in antimicrobial therapies and emerging treatments. Antibiotics. 2019;8(4):193. doi:10.3390/antibiotics8040193
6. Senneville É, Albalawi Z, van Asten SA, et al. IWGDF/IDSA guidelines on the diagnosis and treatment of diabetes-related foot infections (IWGDF/IDSA 2023). Clin Infect Dis. 2023:ciad527. doi:10.1093/cid/ciad527
7. Moya-Salazar J, Chamana JM, Porras-Rivera D, Goicochea-Palomino EA, Salazar CR, Contreras-Pulache H. Increase in antibiotic resistance in diabetic foot infections among peruvian patients: a single-center cross-sectional study. Front Endocrinol. 2023;14:1267699. doi:10.3389/fendo.2023.1267699
8. Yi J, Tang Q, Sun S, Xie H, Wang L, Yin X. Exosomes in diabetic wound healing: mechanisms, applications, and perspectives. Diabetes Metab Syndr Obes. 2025;18:2955–2976. doi:10.2147/DMSO.S532885
9. Li Y, Zhu Z, Li S, et al. Exosomes: compositions, biogenesis, and mechanisms in diabetic wound healing. J Nanobiotechnol. 2024;22(1):398. doi:10.1186/s12951-024-02684-1
10. Sun Y, Zhang S, Shen Y, et al. Therapeutic application of mesenchymal stem cell-derived exosomes in skin wound healing. Front Bioeng Biotechnol. 2024;12:1428793. doi:10.3389/fbioe.2024.1428793
11. Guo L, Xiao D, Xing H, Yang G, Yang X. Engineered exosomes as a prospective therapy for diabetic foot ulcers. Burns Trauma. 2024;12:tkae023. doi:10.1093/burnst/tkae023
12. Han C, Singla RK, Wang C. Application of biomaterials in diabetic wound healing: the recent advances and pathological aspects. Pharmaceutics. 2025;17(10):1295. doi:10.3390/pharmaceutics17101295
13. Yang Y, Cui J, Kong Y, Hou Y, Zhang H, Ma C. The role of hydrogel biomaterials in the intervention of wound healing and skin regeneration via exosomes: a systematic review and meta-analysis of preclinical animal studies. Adv Wound Care. 2025;14(12):669–684. doi:10.1089/wound.2024.0058
14. Zhu M, Sun X, Qi X, Xia L, Wu Y. Exosomes from high glucose-treated macrophages activate macrophages andinduce inflammatory responses via NF-κB signaling pathway in vitro and in vivo. Int Immunopharmacol. 2020;84:106551. doi:10.1016/j.intimp.2020.106551
15. Li N, Hu L, Li J, et al. The immunomodulatory effect of exosomes in diabetes: a novel and attractive therapeutic tool in diabetes therapy. Front Immunol. 2024;15:1357378. doi:10.3389/fimmu.2024.1357378
16. Li X, Xie X, Lian W, et al. Exosomes from adipose-derived stem cells overexpressing Nrf2 accelerate cutaneous wound healing by promoting vascularization in a diabetic foot ulcer rat model. Exp Mol Med. 2018;50(4):1–14. doi:10.1038/s12276-018-0058-5
17. Li S, Li Y, Wu Z, Wu Z, Fang H. Diabetic ferroptosis plays an important role in triggering on inflammation in diabetic wound. Am J Physiol Endocrinol Metab. 2021;321(4):E509–E520. doi:10.1152/ajpendo.00042.2021
18. Jiang Q, Tang L, Xiao S. Relationship between ferroptosis and healing of diabetic foot ulcer: a prospective clinical study. Front Endocrinol. 2024;15:1412373. doi:10.3389/fendo.2024.1412373
19. Shen K, Zheng R, Yu B, et al. Suppression the glucose-induced ferroptosis in endothelial cells by 4OI-loading exosomes hydrogel for the treatment of diabetic foot ulcer. Chem Eng J. 2024;497:154696. doi:10.1016/j.cej.2024.154696
20. Han Z, Wu W, Bai Z, Xiu Y, Zhou D. Beta-boswellic acid facilitates diabetic wound healing by targeting STAT3 and inhibiting ferroptosis in fibroblasts. Front Pharmacol. 2025;16:1578625. doi:10.3389/fphar.2025.1578625
21. Rezel-Potts E, Free C, Syred J, Baraitser P. Expanding choice through online contraception: a theory of change to inform service development and evaluation. BMJ Sex Reprod Health. 2020;46(2):108–115. doi:10.1136/bmjsrh-2018-200297
22. Kang H, Ma X, Liu J, Fan Y, Deng X. High glucose-induced endothelial progenitor cell dysfunction. Diab Vasc Dis Res. 2017;14(5):381–394. doi:10.1177/1479164117719058
23. Catrina SB, Okamoto K, Pereira T, Brismar K, Poellinger L. Hyperglycemia regulates hypoxia-inducible factor-1alpha protein stability and function. Diabetes. 2004;53(12):3226–3232. doi:10.2337/diabetes.53.12.3226
24. Catrina SB, Zheng X. Hypoxia and hypoxia-inducible factors in diabetes and its complications. Diabetologia. 2021;64(4):709–716. doi:10.1007/s00125-021-05380-z
25. Wang H, Bai Z, Qiu Y, et al. Empagliflozin-pretreated MSC-derived exosomes enhance angiogenesis and wound healing via PTEN/AKT/VEGF pathway. Int J Nanomed. 2025;20:5119–5136. doi:10.2147/IJN.S512074
26. Tien T, Barrette KF, Chronopoulos A, Roy S. Effects of high glucose-induced Cx43 downregulation on occludin and ZO-1 expression and tight junction barrier function in retinal endothelial cells. Invest Ophthalmol Visual Sci. 2013;54(10):6518–6525. doi:10.1167/iovs.13-11763
27. Luo Z, Yue S, Chen T, She P, Wu Y, Wu Y. Reduced growth of Staphylococcus aureus under high glucose conditions is associated with decreased pentaglycine expression. Front Microbiol. 2020;11:537290. doi:10.3389/fmicb.2020.537290
28. Vasiljevs S, Gupta A, Baines D. Effect of glucose on growth and co-culture of Staphylococcus aureus and Pseudomonas aeruginosa in artificial sputum medium. Heliyon. 2023;9(11):e21469. doi:10.1016/j.heliyon.2023.e21469
29. Niu H, Gu J, Zhang Y. Bacterial persisters: molecular mechanisms and therapeutic development. Signal Transduct Targeted Ther. 2024;9(1):174. doi:10.1038/s41392-024-01866-5
30. Raghav A, Tripathi P, Mishra BK, et al. Mesenchymal stromal cell-derived tailored exosomes treat bacteria-associated diabetes foot ulcers: a customized approach from bench to bed. Front Microbiol. 2021;12:712588. doi:10.3389/fmicb.2021.712588
31. Wynn TA, Vannella KM. Macrophages in tissue repair, regeneration, and fibrosis. Immunity. 2016;44(3):451–462. doi:10.1016/j.immuni.2016.02.015
32. Gordon S, Martinez FO. Alternative activation of macrophages: mechanism and functions. Immunity. 2010;32(5):593–604. doi:10.1016/j.immuni.2010.05.007
33. McWhorter FY, Wang T, Nguyen P, Chung T, Liu WF. Modulation of macrophage phenotype by cell shape. Proc Natl Acad Sci U S A. 2013;110(43):17253–17258. doi:10.1073/pnas.1308887110
34. Cao W, Peng S, Yao Y, et al. A nanofibrous membrane loaded with doxycycline and printed with conductive hydrogel strips promotes diabetic wound healing in vivo. Acta Biomater. 2022;152:61–73. doi:10.1016/j.actbio.2022.08.048
35. Stechmiller J, Cowan L, Schultz G. The role of doxycycline as a matrix metalloproteinase inhibitor for the treatment of chronic wounds. Biol Res Nurs. 2010;11(4):336–344. doi:10.1177/1099800409346333
36. Ma Q. Role of nrf2 in oxidative stress and toxicity. Annu Rev Pharmacol Toxicol. 2013;53:401–426. doi:10.1146/annurev-pharmtox-011112-140320
37. Tonelli C, Chio IIC, Tuveson DA. Transcriptional regulation by Nrf2. Antioxid Redox Signaling. 2018;29(17):1727–1745. doi:10.1089/ars.2017.7342
38. Yu X, Fu X, Yang J, et al. Glucose/ROS cascade-responsive ceria nanozymes for diabetic wound healing. Mater Today Bio. 2022;15:100308. doi:10.1016/j.mtbio.2022.100308
39. Li M, Jafari H, Okoro OV, Nie L, Shavandi A. Nanozymes as catalysts for accelerated healing of diabetic wounds. Cell Biomater. 2025;1(5):100049. doi:10.1016/j.celbio.2025.100049
40. Li Q, Dong M, Han Q, et al. Enhancing diabetic wound healing with a pH-responsive nanozyme hydrogel featuring multi-enzyme-like activities and oxygen self-supply. J Control Release. 2024;365:905–918. doi:10.1016/j.jconrel.2023.12.015
41. Rajab AM, Taqa GA, Al-Wattar WT. The effect of topically applied hyaluronic acid on skin wound healing in rabbits. J Appl Vet Sci. 2022;7(1):38–45. doi:10.21608/javs.2021.102235.1111
42. Carmeliet P, Jain RK. Molecular mechanisms and clinical applications of angiogenesis. Nature. 2011;473(7347):298–307. doi:10.1038/nature10144
43. Song MS, Salmena L, Pandolfi PP. The functions and regulation of the PTEN tumour suppressor. Nat Rev Mol Cell Biol. 2012;13(5):283–296. doi:10.1038/nrm3330
44. Wei Q, Su J, Meng S, et al. MiR-17-5p-engineered sEVs encapsulated in GelMA hydrogel facilitated diabetic wound healing by targeting PTEN and p21. Adv Sci. 2024;11(13):e2307761. doi:10.1002/advs.202307761
45. Bai Q, Han K, Dong K, et al. Potential applications of nanomaterials and technology for diabetic wound healing. Int J Nanomed. 2020;15:9717–9743. doi:10.2147/IJN.S276001
46. Wang Z, Qi B, Wang R, et al. Smart eutectogel with antibacterial activity for efficiently treating multidrug resistant infection, real-time monitoring and diabetic wound repair. Chem Eng J. 2025;520:166108. doi:10.1016/j.cej.2025.166108
47. Chen Z, Chan K, Li X, et al. Polymeric nanomedicines in diabetic wound healing: applications and future perspectives. Int J Nanomed. 2025;20:6423–6446. doi:10.2147/IJN.S514000
48. Baig MS, Banu A, Zehravi M, et al. An overview of diabetic foot ulcers and associated problems with special emphasis on treatments with antimicrobials. Life. 2022;12(7):1054. doi:10.3390/life12071054
49. Li W, Sadeh O, Chakraborty J, Yang E, Basu P, Kumar P. Multifaceted antibiotic resistance in diabetic foot infections: a systematic review. Microorganisms. 2025;13(10):2311. doi:10.3390/microorganisms13102311
50. Sultana R, Ahmed I, Saima S, Salam MT, Sultana S. Diabetic foot ulcer-a systematic review on relevant microbial etiology and antibiotic resistance in Asian countries. Diabetes Metab Syndr. 2023;17(6):102783. doi:10.1016/j.dsx.2023.102783
51. Gallagher KA, Mills JL, Armstrong DG, et al. Current status and principles for the treatment and prevention of diabetic foot ulcers in the cardiovascular patient population: a scientific statement from the American heart association. Circulation. 2024;149(4):e232–e253. doi:10.1161/CIR.0000000000001192
52. Gu H, Zhao X, Sun Y, Ding Y, Ouyang R. Negative-pressure wound therapy compared with advanced moist wound therapy: a comparative study on healing efficacy in diabetic foot ulcers. Surgery. 2025;180:109098. doi:10.1016/j.surg.2024.109098
53. Guo Q. Comparison and evaluation of negative pressure wound therapy versus standard wound care in the treatment of diabetic foot ulcers. BMC Surg. 2025;25(1):208. doi:10.1186/s12893-025-02885-x
54. Jones RE, Foster DS, Longaker MT. Management of chronic wounds-2018. JAMA. 2018;320(14):1481–1482. doi:10.1001/jama.2018.12426
55. Qiao Z, Wang X, Zhao H, et al. The effectiveness of cell-derived exosome therapy for diabetic wound: a systematic review and meta-analysis. Ageing Res Rev. 2023;85:101858. doi:10.1016/j.arr.2023.101858
56. Chen L, Liu J, He Y, Zeng C, Liao W, Luo C. A systematic review and meta-analysis to investigate the effectiveness of exosome for diabetic wounds. J Tissue Viability. 2025;34(3):100917. doi:10.1016/j.jtv.2025.100917
57. Yue G, Li Y, Liu Z, Yu S, Cao Y, Wang X. Efficacy of MSC-derived small extracellular vesicles in treating type II diabetic cutaneous wounds: a systematic review and meta-analysis of animal models. Front Endocrinol. 2024;15:1375632. doi:10.3389/fendo.2024.1375632
58. Jin W, Li Y, Yu M, Ren D, Han C, Guo S. Advances of exosomes in diabetic wound healing. Burns Trauma. 2025;13:tkae078. doi:10.1093/burnst/tkae078
59. Qin X, He J, Wang X, Wang J, Yang R, Chen X. The functions and clinical application potential of exosomes derived from mesenchymal stem cells on wound repair: a review of recent research advances. Front Immunol. 2023;14:1256687. doi:10.3389/fimmu.2023.1256687
60. Chen Y, Qi W, Wang Z, Niu F. Exosome source matters: a comprehensive review from the perspective of diverse cellular origins. Pharmaceutics. 2025;17(2):147. doi:10.3390/pharmaceutics17020147
61. Wang F, Yao J, Zuo H, Jiao Y, Wu J, Meng Z. Diverse-origin exosomes therapeutic strategies for diabetic wound healing. Int J Nanomed. 2025;20:7375–7402. doi:10.2147/IJN.S519379
62. Han C, Zhong T, Zhao Z, et al. Exosomes derived from platelet-rich plasma facilitates macrophage mitophagy in diabetic wound healing by targeting KNG1 via PI3K-AKT pathway. J Interferon Cytokine Res. 2025. doi:10.1177/10799907251391527
63. Thurlow LR, Hanke ML, Fritz T, et al. Staphylococcus aureus biofilms prevent macrophage phagocytosis and attenuate inflammation in vivo. J Immunol. 2011;186(11):6585–6596. doi:10.4049/jimmunol.1002794
64. Li W, Zhang H, Bai P, et al. ADMSC-derived exosomes promote diabetic wound healing by inhibiting neutrophil extracellular traps formation through delivering miR-92a-1-5p. Arch Biochem Biophys. 2026;778:110755. doi:10.1016/j.abb.2026.110755
65. Wolf SJ, Audu CO, Moon JY, et al. Diabetic wound keratinocytes induce macrophage JMJD3-mediated Nlrp3 expression via IL-1R signaling. Diabetes. 2024;73(9):1462–1472. doi:10.2337/db23-0968
66. Yuan T, Meijia L, Xinyao C, Xinyue C, Lijun H. Exosome derived from human adipose-derived stem cell improve wound healing quality: a systematic review and meta-analysis of preclinical animal studies. Int Wound J. 2023;20(6):2424–2439. doi:10.1111/iwj.14081
67. Bailey AJM, Li H, Kirkham AM, et al. MSC-derived extracellular vesicles to heal diabetic wounds: a systematic review and meta-analysis of preclinical animal studies. Stem Cell Rev Rep. 2022;18(3):968–979. doi:10.1007/s12015-021-10164-4
68. Ding L, Zhang T, Pan Y, et al. Extracellular vesicles in chronic wound therapy: engineering strategies and advanced delivery systems for enhanced regeneration. Mater Today Bio. 2025;35:102298. doi:10.1016/j.mtbio.2025.102298
69. Chen H, Li Q. Recent advances in scalable exosome production: challenges and innovations. Chin J Plast Reconstr Surg. 2025;7(3):149–163. doi:10.1016/j.cjprs.2025.05.001
70. Pei J, Palanisamy CP, Alugoju P, et al. A comprehensive review on bio-based materials for chronic diabetic wounds. Molecules. 2023;28(2):604. doi:10.3390/molecules28020604
71. Ansari M, Darvishi A. A review of the current state of natural biomaterials in wound healing applications. Front Bioeng Biotechnol. 2024;12:1309541. doi:10.3389/fbioe.2024.1309541
72. Sathyaraj WV, Prabakaran L, Bhoopathy J, Dharmalingam S, Karthikeyan R, Atchudan R. Therapeutic efficacy of polymeric biomaterials in treating diabetic wounds-an upcoming wound healing technology. Polymers. 2023;15(5):1205. doi:10.3390/polym15051205
73. Pal D, Das P, Mukherjee P, et al. Biomaterials-based strategies to enhance angiogenesis in diabetic wound healing. ACS Biomater Sci Eng. 2024;10(5):2725–2741. doi:10.1021/acsbiomaterials.4c00216
74. Ahmed R, Augustine R, Chaudhry M, et al. Nitric oxide-releasing biomaterials for promoting wound healing in impaired diabetic wounds: state of the art and recent trends. Biomed Pharmacother. 2022;149:112707. doi:10.1016/j.biopha.2022.112707
75. Jin X, Lan W, Yong W, Yuan Z, Li X, Cui X. Application and development of stimulus-responsive hydrogel biomaterials for diabetic wound healing: a literature review. Front Med. 2025;12:1740559. doi:10.3389/fmed.2025.1740559
76. Xie H, Wang Z, Wang R, Chen Q, Yu A, Lu A. Self-healing, injectable hydrogel dressing for monitoring and therapy of diabetic wound. Adv Funct Mater. 2024;34(36):2401209. doi:10.1002/adfm.202401209
77. Zhang S, Ge G, Qin Y, et al. Recent advances in responsive hydrogels for diabetic wound healing. Mater Today Bio. 2023;18:100508. doi:10.1016/j.mtbio.2022.100508
78. Su J, Liu C, Sun A, et al. Hemostatic and antimicrobial properties of chitosan-based wound healing dressings: a review. Int J Biol Macromol. 2025;306(Pt 2):141570. doi:10.1016/j.ijbiomac.2025.141570
79. Song Y, You Y, Xu X, et al. Adipose-derived mesenchymal stem cell-derived exosomes biopotentiated extracellular matrix hydrogels accelerate diabetic wound healing and skin regeneration. Adv Sci. 2023;10(30):e2304023. doi:10.1002/advs.202304023
80. Wang X, Dong J, Kang J, et al. Self-adaptive release of stem cell-derived exosomes from a multifunctional hydrogel for accelerating MRSA-infected diabetic wound repair. J Am Chem Soc. 2025;147(19):16362–16378. doi:10.1021/jacs.5c02184
81. Xiang K, Chen J, Guo J, et al. Multifunctional ADM hydrogel containing endothelial cell-exosomes for diabetic wound healing. Mater Today Bio. 2023;23:100863. doi:10.1016/j.mtbio.2023.100863
82. Liu H, Jiang W, Han L, Lu X. A natural polyphenol-regulated microporous soybean protein injectable hydrogel loaded with placental stem cell-derived exosomes for promoting chronic wound healing. Macromol Biosci. 2025;25(10):e00546. doi:10.1002/mabi.202400546
83. Kang Y, Xu L, Dong J, et al. Programmed microalgae-gel promotes chronic wound healing in diabetes. Nat Commun. 2024;15(1):1042. doi:10.1038/s41467-024-45101-9
84. Du J, Hu W, Liu J, Gao K. Self-healing injectable oxidized xanthan gum hydrogel loaded with exosomes and matrine modifies the microenvironment to promote diabetic wound healing. Int J Biol Macromol. 2025;322(Pt 2):146709. doi:10.1016/j.ijbiomac.2025.146709
85. Li D, Yu Y, Fan R, et al. An EGCG-enhanced pH/ROS dual-responsive hyaluronic acid hydrogel loaded with ginseng-derived exosomes for diabetic oral ulcers treatment. Int J Biol Macromol. 2026;339(Pt 2):149497. doi:10.1016/j.ijbiomac.2025.149497
86. Li S, Li Y, Chen Y, Guo J, Zou Q, Ding Q. pH-responsive hydrogel system loaded with curcumin-preconditioned mesenchymal stem cell exosomes for enhanced diabetic wound healing in orthopedic applications. Front Bioeng Biotechnol. 2025;13:1688905. doi:10.3389/fbioe.2025.1688905
87. Liu B, Chen L, Huang C, et al. A sprayable exosome-loaded hydrogel with controlled release and multifunctional synergistic effects for diabetic wound healing. Mater Today Bio. 2025;34:102159. doi:10.1016/j.mtbio.2025.102159
88. Gao Y, Chen X, He C, Zhang Z, Yu J. Stimulus-responsive hydrogels for diabetic wound management via microenvironment modulation. Biomater Sci. 2025;13(12):3192–3212. doi:10.1039/d4bm01657b
89. Xu X, Shen Y, Wu J, et al. Methacrylated sericin/methacrylated hyaluronic acid composite microneedles with exosomes for diabetic wound healing. Int J Biol Macromol. 2025;318(Pt 1):144957. doi:10.1016/j.ijbiomac.2025.144957
90. Zou J, Cui W, Deng N, et al. Fate reversal: exosome-driven macrophage rejuvenation and bacterial-responsive drug release for infection immunotherapy in diabetes. J Control Release. 2025;382:113730. doi:10.1016/j.jconrel.2025.113730
91. Miya MB, Ashutosh N, Maulishree N, et al. Accelerated diabetic wound healing using a chitosan-based nanomembrane incorporating nanovesicles from Aloe barbadensis, Azadirachta indica, and Zingiber officinale. Int J Biol Macromol. 2025;310(Pt 2):143169. doi:10.1016/j.ijbiomac.2025.143169
92. Xin H, Xu Y, Pan L, et al. Multifaceted microneedle patch: a one-stop solution to combat multitype wound infections. Biomater Res. 2025;29:290. doi:10.34133/bmr.0290
93. Miya MB, Chaturvedi P, Pathak V, Gupta PC, Kalani A. Healing wounds in diabetes: exploring cutting-edge natural extracellular vesicle therapeutics. Obes Med. 2025;54:100597. doi:10.1016/j.obmed.2025.100597
94. Shiekh PA, Singh A, Kumar A. Exosome laden oxygen releasing antioxidant and antibacterial cryogel wound dressing OxOBand alleviate diabetic and infectious wound healing. Biomaterials. 2020;249:120020. doi:10.1016/j.biomaterials.2020.120020
95. Xiong Y, Chen L, Liu P, et al. All-in-one: multifunctional hydrogel accelerates oxidative diabetic wound healing through timed-release of exosome and fibroblast growth factor. Small. 2022;18(1):e2104229. doi:10.1002/smll.202104229
96. Shi X, Li Y, Kang S, et al. Dual-functional gallium/chitosan/silk/umbilical cord mesenchymal stem cell exosome sponge scaffold for diabetic wound by angiogenesis and antibacteria. Int J Biol Macromol. 2024;274(Pt 2):133420. doi:10.1016/j.ijbiomac.2024.133420
97. He X, Wei Y, Xu K. Hydrogel-based treatment of diabetic wounds: from smart responsive to smart monitoring. Gels. 2025;11(8):647. doi:10.3390/gels11080647
98. Jiang X, Ma J, Xue K, et al. Highly bioactive MXene-M2-exosome nanocomposites promote angiogenic diabetic wound repair through reconstructing high glucose-derived immune inhibition. ACS Nano. 2024;18(5):4269–4286. doi:10.1021/acsnano.3c09721
99. Sun B, Wu F, Wang X, et al. An optimally designed engineering exosome-reductive COF integrated nanoagent for synergistically enhanced diabetic fester wound healing. Small. 2022;18(26):e2200895. doi:10.1002/smll.202200895
100. Li W, Wu S, Ren L, et al. Development of an antiswelling hydrogel system incorporating M2-exosomes and photothermal effect for diabetic wound healing. ACS Nano. 2023;17(21):22106–22120. doi:10.1021/acsnano.3c09220
101. Li X, Qu S, Ouyang Q, et al. A multifunctional composite nanoparticle with antibacterial activities, anti-inflammatory, and angiogenesis for diabetic wound healing. Int J Biol Macromol. 2024;260(Pt 2):129531. doi:10.1016/j.ijbiomac.2024.129531
102. Yu Y, Jin H, Li L, et al. An injectable, activated neutrophil-derived exosome mimetics/extracellular matrix hybrid hydrogel with antibacterial activity and wound healing promotion effect for diabetic wound therapy. J Nanobiotechnol. 2023;21(1):308. doi:10.1186/s12951-023-02073-0
103. Jin H, Wen X, Sun R, et al. Engineered nanovesicles from activated neutrophils with enriched bactericidal proteins have molecular debridement ability and promote infectious wound healing. Burns Trauma. 2024;12:tkae018. doi:10.1093/burnst/tkae018
104. García Coronado PL, Garza Martínez BA, Moreno Amador KA, et al. Gentamicin-loaded exosomes from IMMUNEPOTENT CRP enhance healing of infected diabetic wound in mice. Front Pharmacol. 2025;16:1682468. doi:10.3389/fphar.2025.1682468
105. Xiang X, Chen J, Jiang T, et al. Milk-derived exosomes carrying siRNA-KEAP1 promote diabetic wound healing by improving oxidative stress. Drug Deliv Transl Res. 2023;13(9):2286–2296. doi:10.1007/s13346-023-01306-x
106. Zhang L, Luo Z, Chen H, Wu X, Zhao Y. Glycyrrhizic acid hydrogel microparticles encapsulated with mesenchymal stem cell exosomes for wound healing. Research. 2024;7:496. doi:10.34133/research.0496
107. Yuan W, Huang C, Deng W, et al. Hyaluronic acid methacryloyl/chitosan methacryloyl/3-methacrylamidophenylboronic acid multifunctional hydrogel loading exosome for diabetic wound healing. Int J Biol Macromol. 2024;280(Pt 3):135562. doi:10.1016/j.ijbiomac.2024.135562
108. Zhang X, Liang Y, Luo D, et al. Advantages and disadvantages of various hydrogel scaffold types: a research to improve the clinical conversion rate of loaded MSCs-exos hydrogel scaffolds. Biomed Pharmacother. 2024;179:117386. doi:10.1016/j.biopha.2024.117386
109. Liu L, Liu D. Bioengineered mesenchymal stem cell-derived exosomes: emerging strategies for diabetic wound healing. Burns Trauma. 2024;12:tkae030. doi:10.1093/burnst/tkae030
110. Yan C, Xv Y, Lin Z, et al. Human umbilical cord mesenchymal stem cell-derived exosomes accelerate diabetic wound healing via ameliorating oxidative stress and promoting angiogenesis. Front Bioeng Biotechnol. 2022;10:829868. doi:10.3389/fbioe.2022.829868
111. Shiekh PA, Singh A, Kumar A. Data supporting exosome laden oxygen releasing antioxidant and antibacterial cryogel wound dressing OxOBand alleviate diabetic and infectious wound healing. Data Brief. 2020;31:105671. doi:10.1016/j.dib.2020.105671
112. Welsh JA, Goberdhan DCI, O’Driscoll L, et al. Minimal information for studies of extracellular vesicles (MISEV2023): from basic to advanced approaches. J Extracell Vesicles. 2024;13(2):e12404. doi:10.1002/jev2.12404
113. Van niel G, D’Angelo G, Raposo G. Shedding light on the cell biology of extracellular vesicles. Nat Rev Mol Cell Biol. 2018;19(4):213–228. doi:10.1038/nrm.2017.125
114. Kishta MS, Hafez AM, Hydara T, et al. The transforming role of wharton’s jelly mesenchymal stem cell-derived exosomes for diabetic foot ulcer healing: a randomized controlled clinical trial. Stem Cell Res Ther. 2025;16(1):559. doi:10.1186/s13287-025-04690-y
115. Xu J, Gao J, Li H, Zhu Z, Liu J, Gao C. The risk factors in diabetic foot ulcers and predictive value of prognosis of wound tissue vascular endothelium growth factor. Sci Rep. 2024;14(1):14120. doi:10.1038/s41598-024-64009-4
116. Chin BZ, Lee P, Sia CH, Hong CC. Diabetic foot ulcer is associated with cardiovascular-related mortality and morbidity – a systematic review and meta-analysis of 8062 patients. Endocrine. 2024;84(3):852–863. doi:10.1007/s12020-024-03696-5
117. Ahn SH, Ryu SW, Choi H, You S, Park J, Choi C. Manufacturing therapeutic exosomes: from bench to industry. Mol Cells. 2022;45(5):284. doi:10.14348/molcells.2022.2033
118. Yu W, Deng N, Feng Y, et al. Understanding multi-scale ion-transport in solid-state lithium batteries. eScience. 2025;5(1):100278. doi:10.1016/j.esci.2024.100278
119. Xu G, Jin J, Fu Z, et al. Extracellular vesicle-based drug overview: research landscape, quality control and nonclinical evaluation strategies. Signal Transduct Targeted Ther. 2025;10(1):255. doi:10.1038/s41392-025-02312-w
120. Ahmadian S, Jafari N, Tamadon A, Ghaffarzadeh A, Rahbarghazi R, Mahdipour M. Different storage and freezing protocols for extracellular vesicles: a systematic review. Stem Cell Res Ther. 2024;15(1):453. doi:10.1186/s13287-024-04005-7
121. Wang CK, Tsai TH, Lee CH. Regulation of exosomes as biologic medicines: regulatory challenges faced in exosome development and manufacturing processes. Clin Transl Sci. 2024;17(8):e13904. doi:10.1111/cts.13904
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Unveiling the Pathological Landscape of Intrauterine Adhesion: Mechanistic Insights and Exosome-Biomaterial Therapeutic Innovations
Qin Z, Yu Q, Long Y
International Journal of Nanomedicine 2025, 20:9667-9694
Published Date: 5 August 2025
Exosomes in Diabetic Wound Healing: Mechanisms, Applications, and Perspectives

Yi J, Tang Q, Sun S, Xie H, Wang L, Yin X
Diabetes, Metabolic Syndrome and Obesity 2025, 18:2955-2976
Published Date: 21 August 2025
Muco-Adhesive Hydrogels-Based Exosome Delivery for Periodontal Tissue Regeneration and Inflammation Reduction: A Review
Chen H, Zhang L, Duan Y, Lan X, Xu H, Wu L
International Journal of Nanomedicine 2025, 20:14413-14437
Published Date: 4 December 2025
Exosome-Mediated Rewiring of Oxidative Stress–Inflammation–ECM Remodeling Axis Mitigates UVB-Triggered Skin Photoaging
Yu F, Zhou J, Chen M, Liu Y, Qiu J, Chen J, Teng Y, Gou K, Tang Y, Xu Y, Wu Z, Zhang Z, Chen L
International Journal of Nanomedicine 2026, 21:600909
Published Date: 8 April 2026