")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 19
Examining the Role of GLU/GABA to GLN Metabolic Cycle in the Pathogenesis of Post-Stroke Depressive Disorder and Insomnia
Authors Zhang XH, Zhang X, Liu XW, Lai PH, Cao CC, Wang YL, Ren LJ
Received 9 October 2023
Accepted for publication 4 December 2023
Published 22 December 2023 Volume 2023:19 Pages 2833—2840
DOI https://doi.org/10.2147/NDT.S443844
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yuping Ning
Xiao-Hua Zhang,1,* Xin Zhang,1,* Xuan-Wei Liu,1 Peng-Hui Lai,1 Chang-Chun Cao,1 Yu-Long Wang,2 Li-Jie Ren2
1Department of Rehabilitation, Shenzhen Dapeng New District Nanao People’s Hospital, Shenzhen, 518121, People’s Republic of China; 2Department of Rehabilitation, The First Affiliated Hospital, Shenzhen University, Shenzhen Second People’s Hospital, Shenzhen, 518000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yu-Long Wang; Li-Jie Ren, Department of Rehabilitation, The First Affiliated Hospital, Shenzhen University, Shenzhen Second People’s Hospital, 3002 Sungang West Road, Futian District, Shenzhen, 518035, People’s Republic of China, Tel +86 13923448395 ; +86 13631605966, Email [email protected]; [email protected]
Objective: This study aims to elucidate the potential links between the GLU/GABA to GLN metabolic cycle disruptions and the onset of depressive and insomnia disorders following a stroke. We particularly focus on understanding if these disorders share a common underlying pathogenic mechanism.
Methods: We examined 63 patients with post-stroke insomnia, 62 patients with post-stroke depression, and 18 healthy individuals. The study involved assessing insomnia using the Acute Insomnia Scale (AIS) and depression using the Hamilton Depression Rating Scale. We measured serum concentrations of GLN, GLU, and GABA and analyzed their correlations with AIS and HAMD scores.
Results: Our results indicate no significant difference in the serum levels of GLN, GLU, and GABA between the post-stroke insomnia and depression groups. However, these levels were notably lower in both patient groups compared to the healthy control group. A negative correlation between AIS scores and GABA levels was observed in the post-stroke insomnia group, suggesting a potential link between GABAergic disturbances and insomnia. Conversely, no significant correlation was found between Hamilton Depression Rating Scale scores and the levels of GABA, GLU, or GLN in the post-stroke depression group.
Conclusion: The study highlights that abnormalities in the GLU/GABA to GLN metabolic cycle, particularly the levels of GLN, GABA, and GAD, might be intricately linked to the pathogenesis of post-stroke insomnia and depression. Our findings suggest that GABAergic imbalances could be indicative of post-stroke insomnia, serving as potential biological markers for differential diagnosis in clinical settings. Further research is warranted to explore these relationships in greater depth, potentially leading to new diagnostic and therapeutic approaches for post-stroke neuropsychiatric disorders.
Keywords: glutamate, GLU, γ-aminobutyric acid, GABA, post-stroke depression, post-stroke insomnia
Introduction
Post-stroke sleep disorders (PSSD) represent the most prevalent complications that ensue after a stroke occurrence.1 In clinical practice, these disorders predominantly manifest as heightened instances of nocturnal awakenings and persistent insomnia, with insomnia accounting for a substantial 56.7% of reported cases.2 Insomnia can severely affect the recovery and quality of life of patients with stroke, and also increase the risk of recurrent strokes.3 Post-stroke depression (PSD) refers to a syndrome characterized by a series of depressive and corresponding somatic symptoms manifesting after a stroke. Post-stroke insomnia can lead to the onset of PSD, and depression can further exacerbate symptoms of insomnia. According to studies, depression and insomnia are positively correlated.4 The pathogenesis of PSD and insomnia is complex. Current studies suggest that neurotransmitter dysregulation may be a pivotal etiological factor.5
The primary excitatory neurotransmitter in the central nervous system is glutamate (GLU), which is produced from glutamine (GLN). Glial cells are the only sites for its synthesis. GLU is abundantly expressed in areas of the brain that controls emotions such as the hippocampus, hypothalamus, and amygdala, and it has a crucial role in maintaining the excitability of the nervous system.6 In contrast, γ-aminobutyric acid (GABA) is the primary inhibitory neurotransmitter in the nervous system.7 GLU decarboxylates to generate GABA under the control of the rate-limiting enzyme glutamic acid dehydrogenase (GAD). The GLU/GABA to GLN metabolic cycle is formed when presynaptic neuron vesicles release GABA into the synaptic cleft, where it is partially taken up by glial cells and converted into GLU.8 Extensive research, such as that conducted by Jennifer Zhao, Matthew Burke, Elisabeth Binder, and Gustavo Turecki (2018), has highlighted the prefrontal alterations in GABAergic and glutamatergic gene expression related to depression and suicide, indicating the potential implications of these neurotransmitters in mood disorders commonly observed post-stroke.6 Similarly, Tania Wise, Allan H. Young, and Cynthia H. Y. Fu (2018) discussed the glutamatergic hypofunction in major depression, suggesting a potential link between glutamate neurotransmission and depressive symptoms.8 Moreover, studies by Subimal Chowdhury, Qianzi Yang, and William Wisden (2019) and Xiang Yu, Caroline Kirkwood, and William Wisden (2019) have elucidated the role of GABA and glutamate neurons in sleep regulation, providing insights into how these neurotransmitters could contribute to sleep disorders post-stroke.9 Furthermore, research by Yi-Qun Huang, Li-Feng Jiang, and Zheng-Quan Yu (2020) on the interaction between melatonin and GABAergic neurons sheds light on the complex neurochemical interactions that regulate sleep, which might be disturbed post-stroke.10
Based on this, we hypothesize that disturbances in the GLU/GABA to GLN metabolic cycle may be one of the common pathological mechanisms for post-stroke depression and post-stroke insomnia. The primary chemicals in the GLU/GABA to GLN metabolic cycle are GLN, GLU, and GABA, and the purpose of this study was to measure their peripheral blood concentrations using the enzyme linked immunosorbent assay (ELISA). In order to provide molecular indicators and new targets for the diagnosis of these two disorders, differential diagnosis, and treatment, we plan to investigate the variations in the pathogenic mechanisms of the GLU/GABA to GLN metabolic cycle that underlie each of their two etiologies.
Resources and Methods
Post-Stroke Insomnia Group
General Information
For this study, a total of 63 patients diagnosed with stroke who were admitted to Nana’o People’s Hospital in Dapeng New District, Shenzhen, between April 2022 and March 2023 were selected. This research was reviewed and approved by the Medical Ethics Committee of Nan’ao People’s Hospital in Dapeng New District, Shenzhen. All participants were informed and voluntarily participated in the study.
Inclusion Criteria
(1) Patients diagnosed with stroke based on the revised diagnostic criteria from the 4th National Cerebrovascular Disease Academic Conference, and confirmed by CT (computed tomography) or MRI (magnetic resonance imaging) as having either a hemorrhagic stroke or ischemic stroke.(2) Brain tissue damage on one side as verified through cranial CT or MRI.(3) Patients who are conscious and successfully underwent associated scale assessments two weeks after the onset of the disorder.(4) Diagnosis of stroke-related insomnia should simultaneously meet the diagnostic criteria for both stroke and insomnia.11 (5) Participants who were informed about the research, consented to participate, and signed the informed consent form.
Exclusion Criteria
(1) Patients who had psychiatric or neurological symptoms before the onset of stroke or those uncooperative to the treatment.(2) Individuals with complications like loss of hearing, aphasia, or severe cognitive impairment that hinders regular communication.(3) Those in whom insomnia is due to severe coronary heart disease, respiratory disorders, or painful diseases.(4) Patients who have recently taken antidepressants, anti-anxiety medications, or sedatives.
Post-Stroke Depression Group
General Information
A total of 62 patients with stroke admitted to Nan’ao People’s Hospital in Dapeng New District, Shenzhen, from April 2022 to March 2023 were selected for this study. This research was reviewed and approved by the Medical Ethics Committee of Nan’ao People’s Hospital in Dapeng New District, Shenzhen. All participants were informed and voluntarily participated in the study.
Inclusion Criteria
(1) Patients who are at least 20 years old and not older than 75, with no gender restrictions. (2) Those in whom depression is caused by cerebrovascular disease, and who can actively cooperate without communication barriers. (3) Patients with a score of ≥ 8 on the Hamilton Depression Rating Scale, and no history of depression or other psychiatric disorders before the onset. (4) Patients who have not taken any antidepressants or any other medications that might affect mental health within a month before the onset. (5) The informed consent form has been signed by the patients or their guardians.
Exclusion Criteria
(1) Patients who had psychiatric or neurological symptoms before the onset of stroke or those uncooperative to treatment. (2) Individuals with complications like loss of hearing, aphasia, or severe cognitive impairment preventing regular communication. (3) Those with insomnia caused by severe coronary heart disease, respiratory disorders, or painful diseases. (4) Patients who have recently taken antidepressants, anti-anxiety medications, or sedatives.
Healthy Control Group
General Information
From April 2022 to March 2023, a total of 18 healthy volunteers were selected from the community, consisting of 13 males and 5 females.
Inclusion Criteria
(1) Aged between 18 and 65 years old. (2) A score less than 7 on the Hamilton Depression Rating Scale (HAMD-17). (3) Acute ischemic stroke (AIS) score less than 6. (4) Individuals with at least a junior high school education. (5) No neurological disorders or other physical diseases.
Exclusion Criteria
(1) Those that have irregular sleep patterns in the recent two weeks or those who work in shifts. (2) Those who have traveled across two or more time zones or went on long-distance journeys in the past two weeks.(3) Individuals who have blood relations with the case group.
Observation Indicators
General Condition Scale
A customized general condition scale was created to record the socio-demographic data of the participants and status of their disease progression. Gender, age, level of education, marital status, job, age of first onset, nature of onset, total duration of disease, timing of the current episode, atypical symptoms during past depressive episodes, number of depressive episodes, past treatment history, family history, etc., were some of the factors taken in to account. Only demographic details were captured for the healthy control group.
Athens Insomnia Scale (AIS)
The AIS is a commonly used self-assessment tool primarily for evaluating quality of sleep.12 It requires respondents to evaluate their sleep conditions over the past month and record incidents that occur at least three times a week. The scale consists of 8 items, each rated from “no symptom” (0) to “severe” (3), accumulating scores from each section. The total score of the scale ranges from 0 to 24. A higher score indicates poor quality of sleep. A score less than 4 suggest “no sleep disturbance”, a score between 4 and 6 indicates probable insomnia, and a score over 6 confirms insomnia.
Hamilton Depression Rating Scale (HAMD)
The Hamilton Depression Rating Scale score is used to assess depression.13 Scores below 8 are considered normal, scores between 8 and 17 indicate mild depression, scores between 17 and 24 indicate moderate depression, and scores greater than 24 are indicative of severe depression. A deputy chief physician who was blind to the diagnosis of the participants completed the scoring of the scale in order to preserve uniformity in the measurement outcomes.
Detection of Serum Biomarkers
Blood samples were taken from all the participants while they were fasting, between 8 am and 9 am, a day after they were enrolled in the study. This was carried out before the participants engaged in any physical therapy or prior to taking any medication. The left cubital vein was used as the standard collection site for the blood sample. Blood samples were collected in dry tubes, incubated at 4 °C for 30 minutes without being disturbed, and then centrifuged at 3000 rotations/minute at low temperature (4 °C) for 10 minutes. The supernatant was transferred to another cryotube and stored in a freezer at −80 °. Once a sufficient number of samples had been collected (not stored longer than 6 months), they were batch processed for ELISA testing to detect serum levels of GLN, GLU, and GABA. The levels of GLN, GLU and GABA were detected using an enzyme immunoassay instrument (manufacturer: Shenzhen Mindray Bio-Medical Electronics Co., Ltd.; model: MR-96A). All the reagent kits used were purchased from Shanghai Bohu Biotechnology Co., Ltd., and all procedures were strictly conducted in accordance with the instruction manual of the kit.
Statistical Methods
Statistical analysis was conducted using SPSS 19.0 software. Counted data was analyzed using the chi-squared test. For data with a normal distribution, the t-test was used for comparisons between two groups, while one-way ANOVA (Analysis of Variance) was used for comparisons between multiple groups. The Student-Newman-Keuls method, generally known as the q-test, was developed to compare groups in pairs. Standard deviation (SD) and mean were used to describe statistical findings. Non-parametric tests (either the Mann–Whitney U analysis or the Kruskal–Wallis H analysis) were used with the median as the relevant statistical description for data without a normal distribution. Correlation analysis between two variables was conducted using either Pearson’s correlation analysis or Spearman correlation analysis. All tests were two-tailed. The level of significance (α) was set at 0.05.
Results
Comparative Study Participant Data
There were 63 participants in the post-stroke insomnia group and 62 participants in the post-stroke depression group. There were no significant statistical differences between the two groups in terms of age, gender, and nature of the stroke (P > 0.05). Results from the chi-squared test and independent samples t-test showed that there were no significant differences in gender ratio, age, and nature of the stroke between the participants, signifying that the background information of the participants was consistent between the groups. Details are shown in Table 1.
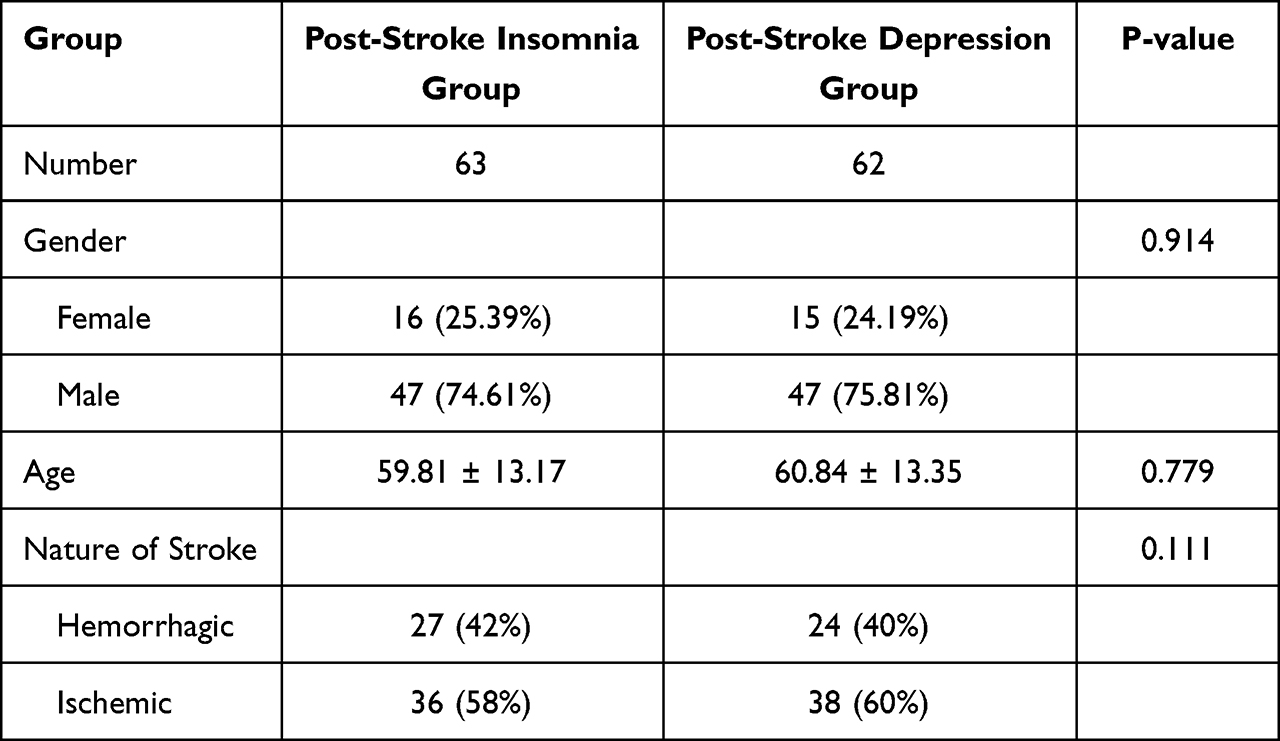 |
Table 1 Comparison of the General Information Between the Two Observation Groups |
Comparison of Serum GLN, GLU, and GABA Levels Between the Post-Stroke Depression Group, Insomnia Disorder Group, and Healthy Control Group
When comparing the plasma levels of GLN, GLU, and GABA between the groups, there were no statistically significant difference between the post-stroke depression group and the post-stroke insomnia group (P > 0.05). However, the levels of GLN, GLU, and GABA in both the post-stroke depression group and post-stroke insomnia group were significantly lower than those in the healthy control group, showing statistical significance (P < 0.05). Details are shown in Table 2.
 |
Table 2 Comparison of Serum GLN, GLU, and GABA Levels Between the Three Observation Groups |
Correlation Between Serum GLN, Glu, and GABA Levels, and AIS, PSD Scores
Within the context of our correlation analysis, where we assessed the relationship between AIS scores in the post-stroke insomnia group and the biochemical levels of GABA, Glu, and GLN, the outcomes of Pearson’s correlation analysis revealed noteworthy patterns. Specifically, we observed a negative correlation between the AIS scores of individuals in the post-stroke insomnia group and GABA levels (r = −8.96, P = 0.0466), signifying an inverse relationship. However, it is noteworthy that no significant correlations were observed with respect to GLU levels (r = −0.03, P = 0.0594) and GLN levels (r = −0.00, P = 0.0778). In both of these latter cases, the calculated P-values exceeded the significance threshold of 0.05, indicating the absence of a statistically significant relationship. The Hamilton Depression Rating Scale score for the post-stroke depression group had a correlation with the GABA level (r= −0.01, P = 0.01766), but there was no correlation with the GLU level (r = −0.04, P = 0.3091) or GLN level (r = −0.00, P = 0.0121), both of which had P values > 0.05, indicating no significant correlation. Details are shown in Table 3 and Figure 1.
 |
Table 3 Correlation of Serum GLN, GLU, and GABA Levels with AIS and PSD |
 |
Figure 1 Correlation between serum levels of Gln, Glu, GABA and AIS, PSD. |
Discussion
According to research, insomnia is a primary symptom in patients with depression.7 Additionally, patients with stroke, who experience symptoms of insomnia also exhibit psychological issues such as anxiety and depression, with a significantly higher risk of depression. This raises the question of whether there is a shared mechanism underlying the development and onset of both these conditions. Currently, scale evaluations are used as diagnostic tools in clinical diagnosis, which is primarily dependent on the symptom level. Biological markers that aid in diagnosis and differential diagnosis are noticeably lacking.14 The GLU/GABA to GLN metabolic cycle system is a crucial component of human neural function regulation, and serves as the primary component foundation for maintaining the balance of neural excitation and inhibition in humans.8 Anomalies in the GLU/GABA to GLN metabolic cycle have been linked to the pathology and pharmacological therapy of primary depression and insomnia in earlier studies.15 Nevertheless, it is unclear whether these anomalies are linked to depression and insomnia following a stroke.
Thus, the goal of this study was to comprehensively examine whether abnormalities in the GLU/GABA to GLN metabolic cycle are linked to the pathological mechanism of depression and insomnia disorders following a stroke, and if they share a common pathological mechanism. In this study, we conducted a comparative analysis of the key substances in the GLU/GABA to GLN metabolic cycle, specifically GLN, GLU, and GABA, between patients with post-stroke depression, insomnia disorders, and a healthy control group. The results revealed that the serum levels of GLN, GABA, and GLN in the post-stroke depression and insomnia disorder groups were lower than in the healthy control group, with the differences being statistically significant. The GABA and GLN levels in the insomnia disorder group were lower than in the depression disorder group, while GLU levels were higher, although these differences were not statistically significant. According to these results, abnormalities in the GLU/GABA to GLN metabolic cycle may be one of the pathogenic pathways that contribute to the development of post-stroke depression and insomnia. Additionally, insomnia disorders may have more severe excitatory/inhibitory neural function imbalances.
Correlation analysis revealed a negative correlation between the levels of GABA and the total AIS score. This suggests that patients with post-stroke insomnia exhibit disturbances in GABAergic neuronal function, as well as an imbalance between excitatory and inhibitory neuronal functions. The quality of sleep declines as GABA levels drop. This indicates that abnormalities in the GLU/GABA to GLN metabolic cycle are related to the pathological mechanism of sleep disorders. In patients with post-stroke depression, serum levels of GLN, GABA, and GLU were found to be lower than in the healthy control group, with the differences being statistically significant. However, the correlation analysis found no apparent correlation between the levels of GLN, GABA, or Glu and the HAMD score. The imbalance in the GABAergic inhibitory neuron function in the GLU/GABA to GLN metabolic cycle seems to be more severe in patients with post-stroke insomnia. This implies that GABA levels might serve as biological markers for differential diagnosis between the two conditions. The intricate pathological mechanism underpinning post-stroke depression, which involves intricate interactions among neurotransmitters, may serve as a plausible explanation for the results obtained. It is conceivable that the observed disparities could also be influenced by factors such as the size and specificity of our sample population. Therefore, in order to corroborate and substantiate these findings, further research involving a more expansive and diverse sample size is imperative.
This study has certain limitations. The neurotransmitter system within the human body is an incredibly complex network. There is no existing evidence to confirm whether the expression levels of GLN, Glu, and GABA in peripheral blood can genuinely reflect changes in the central nervous system.
A more comprehensive understanding could be attained if we were able to simultaneously investigate alterations and correlations at both peripheral and central levels. Such an approach would furnish more robust evidence regarding the potential correlation between anomalies in the Glu/GABA to GLN metabolic cycle and the underlying pathological mechanisms of post-stroke depression (PSD) and post-stroke insomnia. Consequently, further research endeavors are essential to substantiate and validate these preliminary observations.
Conclusion
In summary, our study investigated the potential role of the GLU/GABA to GLN metabolic cycle in the pathogenesis of post-stroke depressive disorder and insomnia. While our findings indicate certain trends, such as abnormalities in GLN, GABA, and GAD levels in patients with post-stroke disorders compared to healthy controls, we acknowledge that these results are preliminary and do not conclusively prove the hypothesized pathogenic mechanisms. The observed variations in GABAergic inhibitory neuron function, particularly in the post-stroke insomnia group, suggest a potential avenue for future exploration. However, it is important to note that these findings should be interpreted with caution. Our study serves as an initial step in understanding the complex interplay of metabolic changes post-stroke and their potential impact on neuropsychiatric outcomes. We recommend further research with larger sample sizes and more comprehensive methodologies to validate these findings and fully elucidate the role of the GLU/GABA to GLN metabolic cycle in post-stroke depression and insomnia. Thus, while our study contributes to the existing body of knowledge, it primarily highlights the need for continued research in this area.
Data Sharing Statement
All data generated or analysed during this study are included in this article. Further enquiries can be directed to the corresponding author.
Ethics Approval and Consent to Participate
The study was conducted in accordance with the Declaration of Helsinki. The study was approved by Ethics Committee of the Shenzhen Dapeng New District Nanao People’s Hospital (No: 20220519001). Written informed consent was obtained from all participants.
Acknowledgments
We are particularly grateful to all the people who have given us help on our article.
Funding
This study was funded by the Science, Technology and Innovation Commission of Shenzhen Municipality (JCYJ20220530165211025).
Disclosure
The authors declare that they have no competing interests.
References
1. Baylans S, Griffiths S, Grant N, et al. Incidence and prevalence of post stroke insomnia: A systematic review and meta-analysis. Sleep Med Rev. 2020;5(49):101222. doi:10.1016/j.smrv.2019.101222
2. Hepburn M, Bollu PC, French B, et al. Sleep medicine: stroke and sleep. Mo Med. 2018;115(6):527–532.
3. Fulk GD, Boyne P, Hauger M, et al. The impact of sleep disorders on functional recovery and participation following stroke: a systematic review and meta-analysis. Neurorehabil Neural Repair. 2020;34(11):1050–1061. doi:10.1177/1545968320962501
4. Fan XW, Yang Y, Wang S, et al. Impact of persistent poor sleep quality on post-stroke anxiety and depression: a national prospective clinical registry study[J/OL]. Nat Sci Sleep. 2022;14:1125–1135. doi:10.2147/NSS.S357536
5. Duss SB, Brill AK, Bargiotas P, et al. Sleep-wake disorders in stroke-increased stroke risk and deteriorated recovery. An evaluation on the necessity for prevention and treatment. Curr Neurol Neurosci Rep. 2018;18(10):72. doi:10.1007/s11910-018-0879-6
6. Zhao J, Verwer RWH, Gao SF, et al. Prefrontal alterations in GABAergic and glutamatergic gene expression in relation to depression and suicide. J Psychiatr Res. 2018;102:261–274. doi:10.1016/j.jpsychires.2018.04.020
7. Hein M, Senterre C, Lanquart JP, et al. Hyperarousal during sleep in untreated primary insomnia sufferers: a polysomnographic study. Psych Res. 2017;253:71–78. doi:10.1016/j.psychres.2017.03.045
8. Wise T, Taylor MJ, Herane-Vives A, et al. Glutamatergic hypofunction in medication-free major depression: secondary effects of affective diagnosis and relationship to peripheral glutaminase. J Affect Disord. 2018;234:214–219. doi:10.1016/j.jad.2018.02.059
9. Chowdhury S, Matsubara T, Miyazaki T, et al. GABA neurons in the ventral tegmental area regulate non-rapid eye movement sleep in mice. Elife. 2019;8:e44928. doi:10.7554/eLife.44928
10. Huang Y, Li Y, Leng Z. Melatonin inhibits GABAergic neurons in the hypothalamus consistent with a reduction in wakefulness. Neuroreport. 2020;31(2):92–98. doi:10.1097/WNR.0000000000001374
11. Carroll Judith E, Ross Kharah M, Horvath S, et al. Postpartum sleep loss and accelerated epigenetic aging. Sleep Health. 2021;7(3):362–367. doi:10.1016/j.sleh.2021.02.002
12. Okajima I, Miyamoto T, Ubara A, et al. Evaluation of severity levels of the Athens insomnia scale based on the criterion of insomnia severity index. Int J Environ Res Public Health. 2020;17(23):8789. doi:10.3390/ijerph17238789
13. Fu P, Gibson CJ, Mendes WB, et al. Anxiety, depressive symptoms, and cardiac autonomic function in perimenopausal and postmenopausal women with hot flashes: a brief report. Menopause. 2018;25(12):1470–1475. doi:10.1097/GME.0000000000001153
14. Ogawa S, Koga N, Hattori K, et al. Plasma amino acid profile in major depressive disorder: analyses in two independent case-control sample sets. J Psychiatr Res. 2018;96:23–32. doi:10.1016/j.jpsychires.2017.09.014
15. Bradley KA, Alonso CM, Mehra LM, et al. Elevated striatal γ-aminobutyric Acid in youth with major depressive disorder. Progress Neuropsychopharmacol Biol Psychiatry. 2018;86:203–210. doi:10.1016/j.pnpbp.2018.06.004
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.