Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 16
Examining the Links Between Physical Activity, Sitting Time, and Renal Function in T2DM Patients
Authors Wang X, Yan N ![]() , Pan R, Dang Y, Wang L
, Pan R, Dang Y, Wang L
Received 15 February 2023
Accepted for publication 9 August 2023
Published 16 August 2023 Volume 2023:16 Pages 2469—2476
DOI https://doi.org/10.2147/DMSO.S408677
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Gian Paolo Fadini
Xiaoyu Wang,1,* Ning Yan,2,* Ruiping Pan,3 Yuqi Dang,4 Liqun Wang5,6
1School of Traditional Chinese Medicine, Ningxia Medical University, Yinchuan, People’s Republic of China; 2Heart Centre & Department of Cardiovascular Diseases, General Hospital of Ningxia Medical University, Yinchuan, People’s Republic of China; 3Department of Chinese Medicine, The Second People’s Hospital of Shizuishan, Shizuishan, People’s Republic of China; 4Department of Endocrinology, Yinchuan Hospital of Traditional Chinese Medicine, Yinchuan, People’s Republic of China; 5Department of Epidemiology and Statistics, School of Public Health at Ningxia Medical University, Yinchuan, People’s Republic of China; 6Key Laboratory of Environmental Factors and Chronic Disease Control, Ningxia Medical University, Yinchuan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Liqun Wang, Department of Epidemiology and Statistics, School of Public Health at Ningxia Medical University, Yinchuan, People’s Republic of China, Tel +86 13649513216, Email [email protected]
Background: Sitting time and physical activity are related to renal function among type 2 diabetes mellitus (T2DM); however, the mechanism of how it contributes to renal function is not well understood. The current study attempts to explore the relationship between sitting time and renal function among T2DM patients, with a particular focus on the mediating role of physical activity.
Methods: This research uses the data of 1761 Chinese T2DM patients from Ningxia Province. Sitting time and physical activity were obtained during a face-to-face survey, and renal function was assessed by the estimated glomerular filtration rate (eGFR). The bootstrap method is used to test the mediating effect.
Results: The research found that sitting time was negatively associated with eGFR and physical activity after controlling for covariates. Physical activity was positively associated with eGFR. Physical activity has mediated the relationship between sitting time and eGFR among T2DM patients (explaining 16.1% of the total variance).
Conclusion: The present findings suggest that sitting time negatively affects eGFR among T2DM patients and provides new evidence that physical activity could attenuate the association between sitting time and eGFR. Hence, intervention strategies focusing on sitting time and physical activity should be paid more attention in the future.
Keywords: sitting time, physical activity, eGFR, mediating effect, T2DM patients
Introduction
With the development of the economy, the change of diet structure, and the acceleration of population aging, type 2 Diabetes mellitus (T2DM) is alarmingly increasing in both developed and underdeveloped countries,1,2 especially in China. According to the statistics, T2DM accounting for the highest prevalence globally and reaching 116.4 million in 2019,3 and results in different macrovascular and microvascular complications,4–6 and about forty percent of patients with T2DM develop diabetic kidney disease,7 further progresses to severe status, mortality, and substantial social and economic burden.8 There is a need to prevent the onset and progression of diabetic kidney disease and protect the renal function of T2DM patients via an array of strategies.
The determinants of diabetic kidney disease include demographic characteristics (age, gender, marital status, educational attainment, residence), health-related behaviors (smoking, drinking, body mass index, physical activity), and other chronic diseases; meanwhile, disease duration can influence diabetic kidney disease.9–11 The benefits of a healthy lifestyle can be seen in T2DM patients. Physical activity is associated with renal function in T2DM patients12 and is considered an effective target in preventing diabetic kidney disease.13 A recent meta-analysis indicated that physical activity effectively improves diabetic kidney disease and slows its progression.14
Another potential factor related to the renal function of T2DM patients is sitting time, which generally refers to any waking activity in a sitting, reclining, or lying posture, such as reading, writing or watching television, etc.15 A considerable body of evidence shows that sedentary behavior is associated with several health outcomes, like depression,16 cardiovascular health,17 and mortality.18 Sedentary behavior or sitting time is highly prevalent in kidney function19 and diabetic kidney disease.20 However, gaps still existed about the relationship between sitting time combined with physical activity with renal function in T2DM patients. In the current study, renal function was assessed by the estimated glomerular filtration rate (eGFR). Therefore, the present study’s hypotheses included:
Hypothesis 1: sitting time will be negatively and directly related to eGFR. Hypothesis 2: sitting time will be negatively and directly related to physical activity. Hypothesis 3: physical activity will be positively and directly related to eGFR. Hypothesis 4: sitting time will indirectly be related to eGFR via physical activity.
Materials and Methods
Subjects and Procedure
The analyses are based on hospital data, in which participants completed a questionnaire from August 2019 through November 2020. A probability proportionate to size (PPS) sampling method was developed to recruit the participants. A similar sampling procedure was described previously.21 A total of 1761 patients (Supplementary Table 1) were analyzed in this study. Patients who met the study eligibility criteria were invited to participate in the study once medical records were reviewed by two physicians. The inclusion criteria: 1) ≥18 years of age; 2) living at their residence for more than six months. Exclusion criteria: 1) with a severe mental disorder or a severe illness or language barrier that prevented communication; 2) pregnant or lactating, had diabetic ketoacidosis in the past month, 3) had a malignant tumor; 4) patients with end-stage renal disease; 5) mobility-related disorders (eg, arthrosis, history of fracture of lower limbs, or another disease that affects the balance) or 6) refused to sign the informed consent were excluded. The Institutional Review Board of the Yinchuan Hospital of Traditional Chinese Medicine approved the study. All the participants provided a written consent form at the beginning of the survey. Research procedures involving human participants conformed with the 1964 Helsinki Declaration and its later amendments.
Renal Function
Renal function was estimated by eGFR and it was calculated using the eGFR equations based on serum creatinine levels as follows:  .22 Serum creatinine was tested as follows: after overnight fasting for more than 12h, the patient’s venous blood was drawn in the morning of the next day. After collecting, the blood was stored in vacuum blood collection vessels without anticoagulants and kept still for 5 min to make it coagulate and centrifuged at 3500r/min 5~10 minutes at room temperature; then the supernatant was stored at 4°C. The serum creatinine was measured by commercially available kits (Shanghai Roche Diagnostic Products Co., Ltd, China) and automatic biochemical analyzer (SIEMENS ADVIA Chemistry XPT System – Siemens Healthineers, USA). All the tests were conducted by the hospital laboratory center.
.22 Serum creatinine was tested as follows: after overnight fasting for more than 12h, the patient’s venous blood was drawn in the morning of the next day. After collecting, the blood was stored in vacuum blood collection vessels without anticoagulants and kept still for 5 min to make it coagulate and centrifuged at 3500r/min 5~10 minutes at room temperature; then the supernatant was stored at 4°C. The serum creatinine was measured by commercially available kits (Shanghai Roche Diagnostic Products Co., Ltd, China) and automatic biochemical analyzer (SIEMENS ADVIA Chemistry XPT System – Siemens Healthineers, USA). All the tests were conducted by the hospital laboratory center.
Physical Activity and Sitting Time
Physical activity was described with the following question: “The frequency of your entertainment or physical activities (such as sports, exercise, square dancing, etc.)”. The participants respond with four answers (1. Never or few 2. 2–3 times/month 3. 1–2 times/week 4.>3 times/week).
Sitting time was assessed with the following question: “How much time do you usually spend sitting or reclining on a typical day?” The respondents were asked to include the amount of waking time spent “sitting or reclining at work, at home, or at school, including time spent sitting at a desk, sitting with friends, reading, playing cards, watching television, or using a computer, but except sleeping time”.
Covariates
The covariates include age, gender (male vs female), marital status (married vs unmarried), residence (urban vs rural), and educational attainment (illiterate vs non-illiterate). Body mass index (BMI = weight (kg)/height (m)2), smoking (defined as at least one cigarette per day and last for six months or more), alcohol use (defined as a drink at least one glass of alcohol, which is equal to 1/2 bottle of beer or 125-milliliter grape wine or fruit wine or 40-milliliter white wine, in the past 12 months). Other chronic diseases (yes vs no), T2DM complications (yes vs no), fasting blood glucose (mmol/L), and disease duration (years), Glycated hemoglobin (HbA1c, HbA1c level) was assayed using high performance liquid chromatography (BIO-RAD Diagnostic Group, CA, USA). Triglyceride (TG, mmol/L); Total cholesterol (TC, mmol/L); High-density lipoprotein (HDL, mmol/L); Low-density lipoprotein (LDL, mmol/L); urea (mmol/L).
Statistical Analyses
Analyses were performed using the Statistical Package for the Social Sciences (SPSS) version 24.0 (IBM Inc., Chicago, Illinois, USA). Continuous variables were expressed as mean ± SD; categorical variables were expressed as counts and proportions. Partial correlation was used to analyze the correlation matrix after controlling for covariates. Linear regression models were carried out to determine the relationship between sitting time, physical activity, and eGFR. In short, model 1 only included physical activity and sitting time; model 2 added the covariate variables (age, gender, marital status, educational attainment, residence, BMI, smoking, alcohol use, other chronic diseases, disease duration, fasting blood glucose, T2DM complications, HbA1c, TG, TC, HDL, LDL, urea). Model 3 added the interaction effect between physical activity and sitting time based on model 2. Bootstrap methods of PROCESS developed by Hayes were employed to test the mediation effect of physical activity on the relationship between sitting time, and eGFR.23 The bias-corrected percentile bootstrap confidence interval does not contain 0, indicating that the mediation effect is statistically significant.24
Results
The Characteristics of Participants
The participant characteristics are shown in Table 1. The mean age was 58.6 ± 12.2 years, and slightly half of the participants were males (54.8%). The mean sitting time was 4.8 ± 2.6 hours per day. Approximately one in three participants had no physical activity, and 39.8% had physical activity 3 times a week. Among all T2DM patients, the mean eGFR was 123.8 ± 39.7 mL/min/1.73m2.
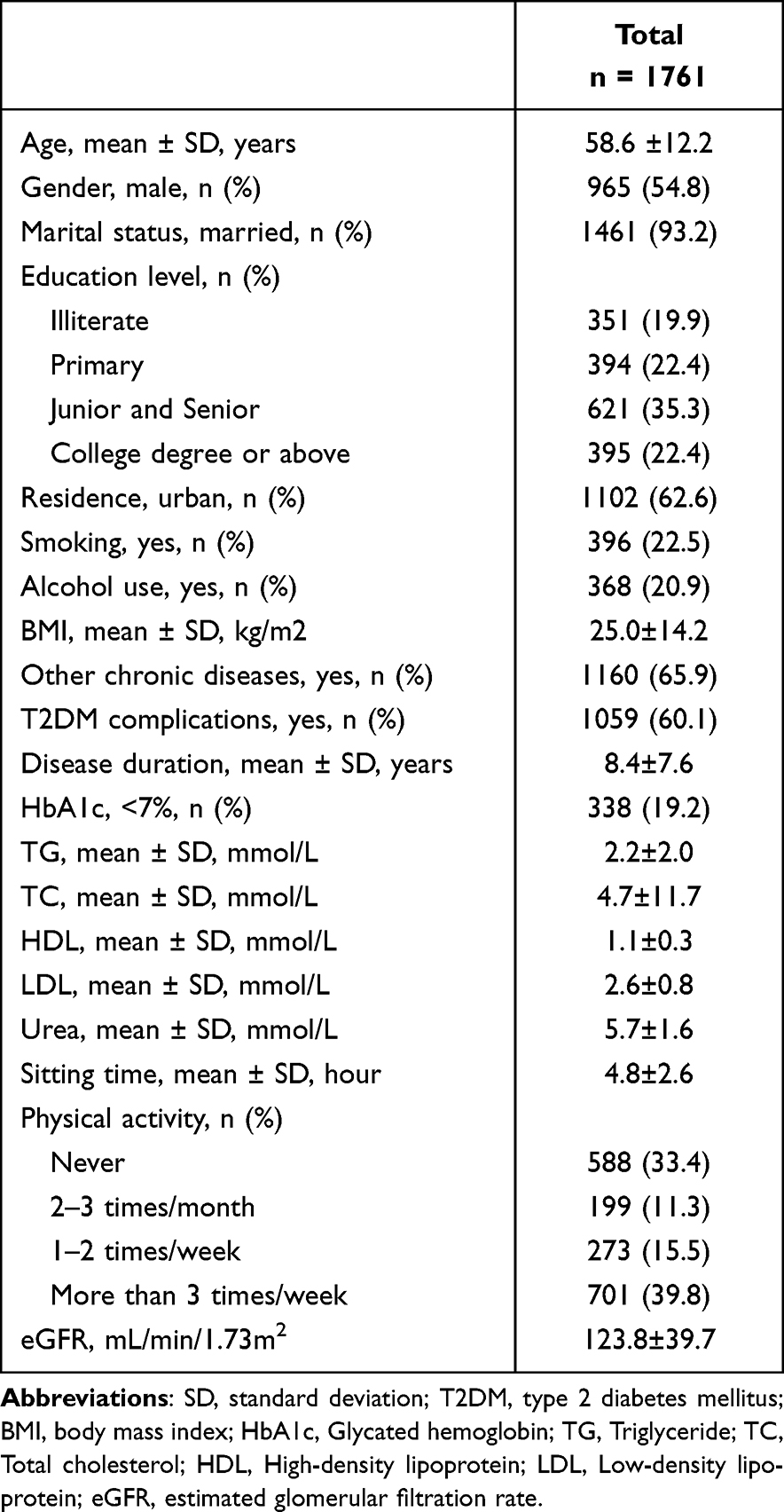 |
Table 1 Demographic Characteristics of Participants |
Partial Correlation Analysis
As shown in Table 2, after controlling for covariates (age, gender, marital status, educational attainment, residence, BMI, smoking, alcohol use, other chronic diseases, disease duration, fasting blood glucose, T2DM complications, TG, TC, HDL, LDL, urea), sitting time was negatively associated with eGFR (r = −0.05, P = 0.048) and sitting time (r = −0.12, P < 0.001). Physical activity was positively associated with eGFR (r = 0.06, P = 0.003).
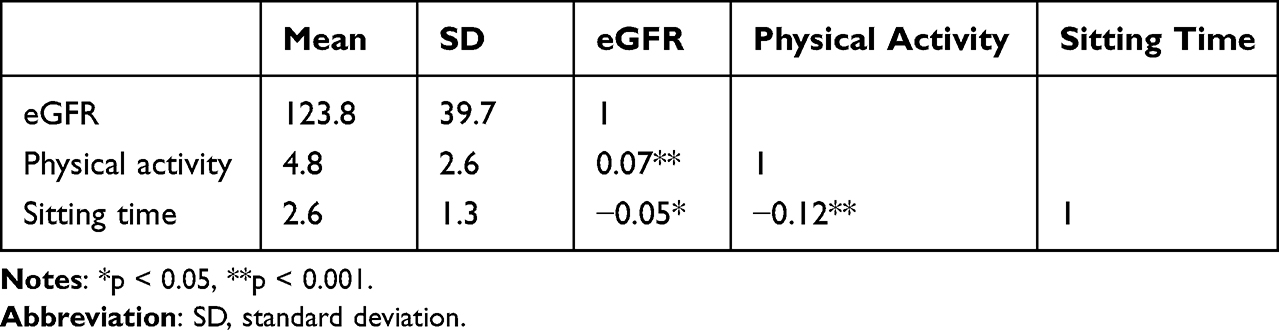 |
Table 2 Correlation Matrix (n = 1761) |
Linear Regression Analysis
The results of the three separate linear regression models are summarized in Table 3. The single-factor model (Model 1) showed that physical activity was significantly and positively associated with eGFR; those with more physical activity may predict better renal function. On the contrary, sitting time was inversely associated with eGFR. After controlling for covariates, those relationships still persisted (Model 2). In model 3, when adding the interaction between physical activity and sitting time, the association between sitting time and eGFR disappeared, indicating that physical activity is a possible mediator.
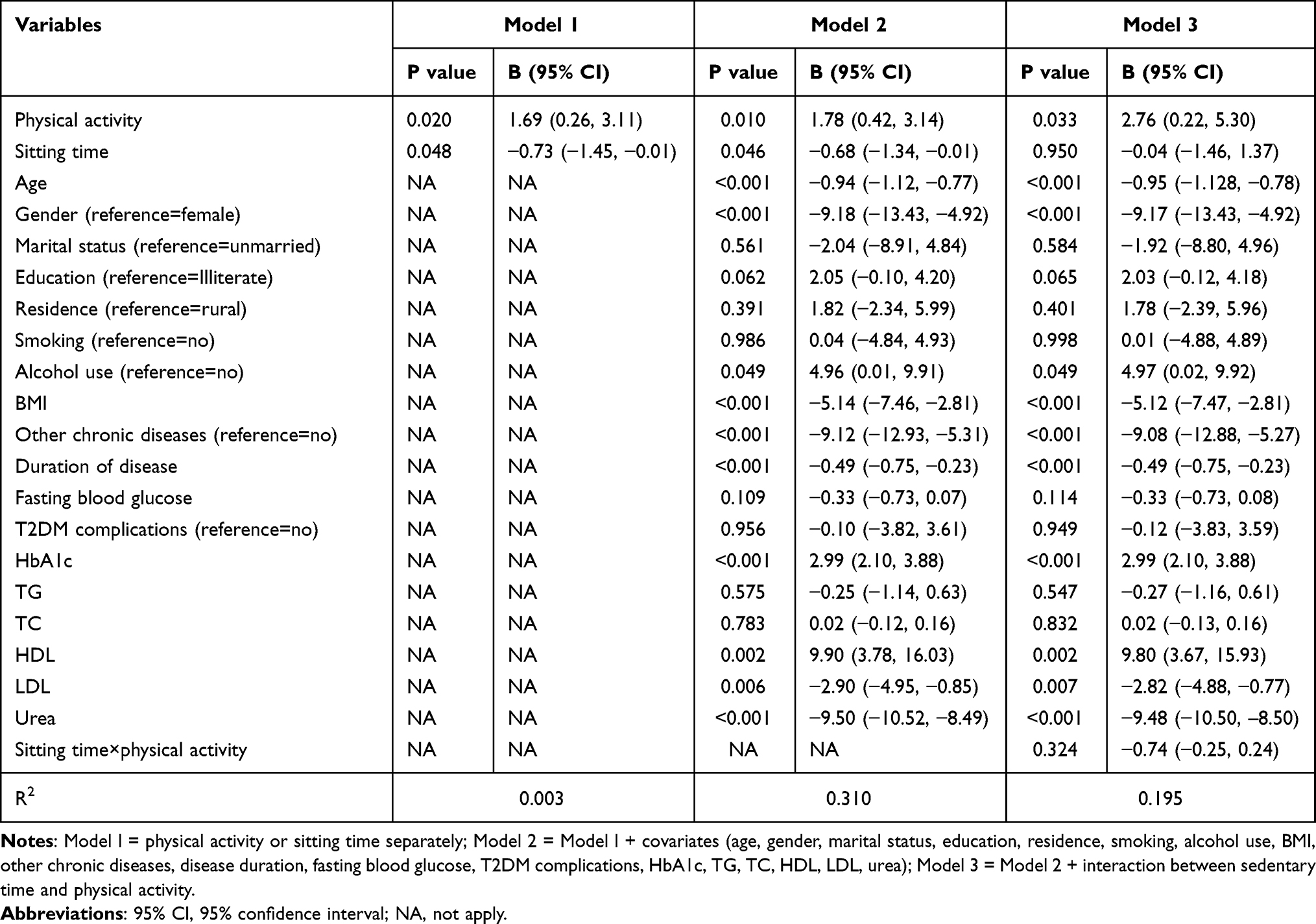 |
Table 3 Linear Regression Model for Interaction Between Physical Activity and Sitting Time on eGFR (n = 1761) |
Mediation Effect of Physical Activity on the Relationship of Sitting Time and eGFR Among T2DM Patients
As shown in Table 4, these results suggested that the relationship between sitting time and eGFR was partially mediated by physical activity, and bootstrap tests indicated that the total effect (95% CI: −1.212, −0.006) and mediation effect (95% CI: −0.215, −0.024) were significant. The mediation effect explained 16.1% (−0.098/-0.609) of the total variance. Considering the possible relationship between age and physical activity, the exploring analysis was conducted stratified by age (use cutoff points of 45 and 60 years old). The mediation effect of physical activity on the relationship between sitting time and eGFR was significant in those who were ≥60 years old (Table 5).
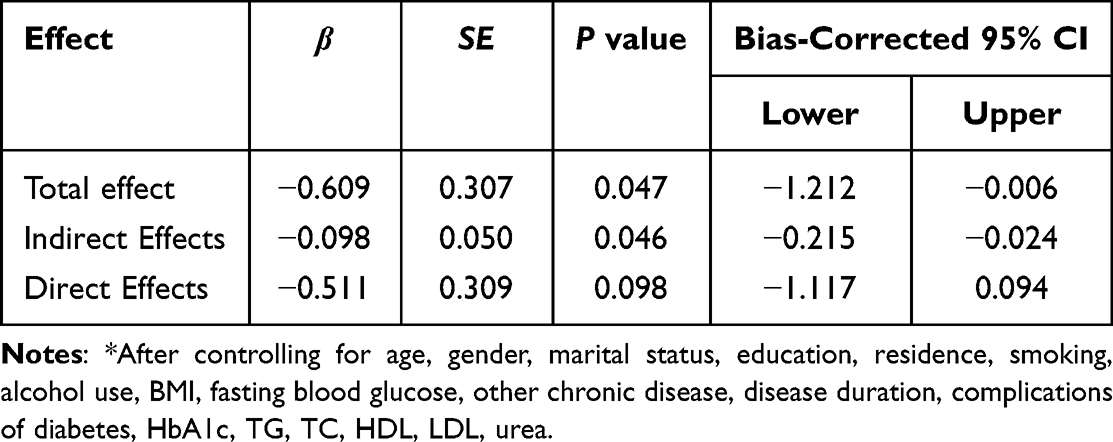 |
Table 4 The Mediating Effect of Physical Activity on the Relationship Between Sitting Time and eGFR* |
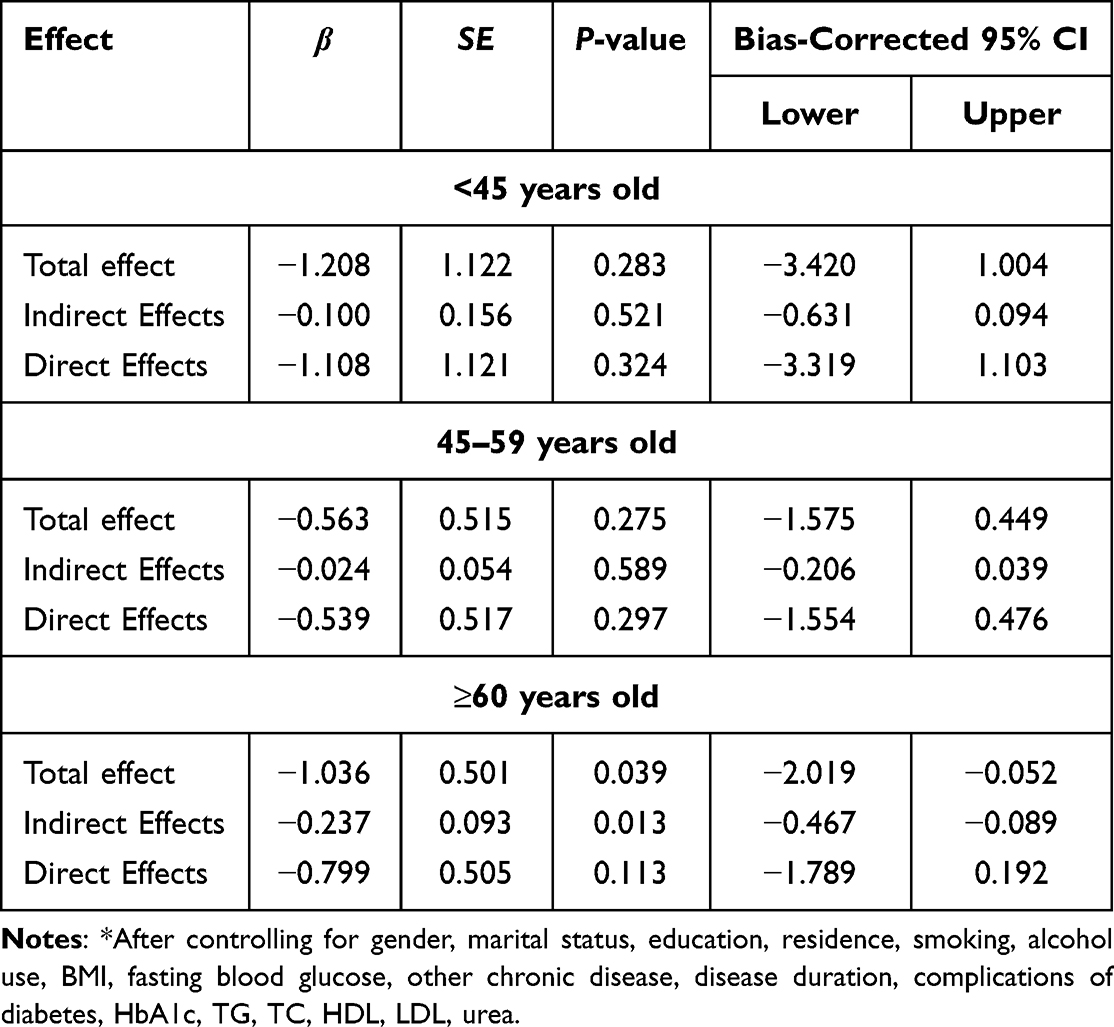 |
Table 5 The Mediation Model of Physical Activity Stratified by Age* |
Discussion
In this cross-sectional study of T2DM patients, we examined the relationship between sitting time, physical activity, and renal function. As we hypothesized, the study found: (1) sitting time was negatively related to eGFR and negatively associated with physical activity; physical activity was positively related to eGFR; and (2) in the relationship between sitting time and eGFR, physical activity mediated the association, the mediation effect accounting for 16.1% of the total effect.
In line with the previous findings, sitting time was negatively associated with eGFR, namely, is positively associated with impaired renal function in T2DM patients. A study showed similar findings that increased sedentary time were associated with lower eGFR after controlling for confounding factors.25 Whilst a recent narrative review also reported that a sedentary lifestyle is associated with impaired kidney function.26 The possible mechanism underpinning the long-sitting adverse effects are abnormal blood pressure,27 inflammation,28 and metabolic syndrome,29 and they can contribute to reduced renal function.
Our study showed that physical activity was positively associated with eGFR. This finding was consistent with a previous study that found increased physical activity was associated with increase in eGFR.30 Furthermore, several meta-analyses have also shown that exercise training slightly improves the eGFR in patients with kidney disease.31,32 A previous study reported that the possible mechanism might be that exercise or physical activity could improve mitochondrial β-oxidation, which can slow down the progression of kidney disease.33 We also found that physical activity was inversely associated with sitting time, consistent with several previous researches.34–36 Moreover, our mediation analysis results suggest that physical activity mediated the relationship between sitting time and eGFR. Namely, sitting time at least a part affected eGFR through physical activity among T2DM patients. Therefore, increased levels of physical activity may reduce sedentary time to achieve the reduction of renal outcomes.
The strength of our study is that most studies focused on the general population, and only a few studies were conducted among individuals with diabetes; meanwhile, we examined the possible mechanism that physical activity plays a mediating role in the relationship between sitting time and renal function. However, several limitations still need to be discussed. First, this was a cross-sectional study with limitations to conducting causal links of sitting time, physical activity, and eGFR. Second, other potential mediators of the relationship between sitting time and renal function, such as obesity, and inflammation, were not assessed. Besides, the information regarding physical activity and sitting time was self-reported by participants, which may have memory bias and present lower reliability although it be commonly used in epidemiological study due to the feasibility consideration. Meanwhile, we carefully defined our survey questions, and the interviews were conducted by well-trained interviewers. Third, the patients were from a single province, when promoting and applying the results to other regions of China or other countries should be cautious.
Conclusions
The present findings suggest that sitting time has a negative effect on eGFR among T2DM patients. Furthermore, the study provides new evidence that physical activity could attenuate the association between sitting time and eGFR among T2DM patients. Clinicians can suggest patients, especially old patients, to increase levels of physical activity to reduce prolonged time in a seated position and to aim the reduction of renal outcomes. Hence, intervention strategies focusing on sitting time and physical activity should be paid more attention in the future.
Data Sharing Statement
The data used to support the findings of this study are included within Supplementary Table 1.
Funding
This work was supported by National Natural Science Foundation of China (grant number 82204955), the Ningxia Natural Science Foundation (2022AAC05058).
Disclosure
All authors declare that there is no conflict of interest.
References
1. Rey-Reñones C, Martinez-Torres S, Martín-Luján FM, et al. Type 2 diabetes mellitus and COVID-19: a narrative review. Biomedicines. 2022;11(1):10. doi:10.3390/biomedicines11010010
2. Sanaeinasab H, Saffari M, Yazdanparast D, et al. Effects of a health education program to promote healthy lifestyle and glycemic control in patients with type 2 diabetes: a randomized controlled trial. Prim Care Diabetes. 2021;15(2):275–282. doi:10.1016/j.pcd.2020.09.007
3. Li J, Qiu X, Yang X, et al. Relationship between illness perception and depressive symptoms among type 2 diabetes mellitus patients in china: a mediating role of coping style. J Diabetes Res. 2020;2020:3142495. doi:10.1155/2020/3142495
4. Abu Al-Halaweh A, Davidovitch N, Almdal TP, et al. Prevalence of type 2 diabetes mellitus complications among Palestinians with T2DM. Diabetes Metab Syndr. 2017;11(Suppl 2):S783–S787. doi:10.1016/j.dsx.2017.05.017
5. Viigimaa M, Sachinidis A, Toumpourleka M, Koutsampasopoulos K, Alliksoo S, Titma T. Macrovascular complications of type 2 diabetes mellitus. Curr Vasc Pharmacol. 2020;18(2):110–116. doi:10.2174/1570161117666190405165151
6. El Alami H, Haddou I, Benaadi G, et al. Prevalence and risk factors of chronic complications among patients with type 2 diabetes mellitus in Morocco: a cross-sectional study. Pan Afr Med J. 2022;41:182. doi:10.11604/pamj.2022.41.182.25532
7. Alicic RZ, Rooney MT, Tuttle KR. Diabetic kidney disease: challenges, progress, and possibilities. Clin J Am Soc Nephrol. 2017;12(12):2032–2045. doi:10.2215/CJN.11491116
8. Pan X, Lin X, Huang X, et al. The burden of diabetes-related chronic kidney disease in China from 1990 to 2019. Front Endocrinol. 2022;13:892860. doi:10.3389/fendo.2022.892860
9. Thomas MC, Cooper ME, Zimmet P. Changing epidemiology of type 2 diabetes mellitus and associated chronic kidney disease. Nat Rev Nephrol. 2016;12(2):73–81. doi:10.1038/nrneph.2015.173
10. Giandalia A, Giuffrida AE, Gembillo G, et al. Gender differences in diabetic kidney disease: focus on hormonal, genetic and clinical factors. Int J Mol Sci. 2021;23(1):22. doi:10.3390/ijms23010022
11. Russo GT, De Cosmo S, Viazzi F, et al. Diabetic kidney disease in the elderly: prevalence and clinical correlates. BMC Geriatr. 2018;18(1):38. doi:10.1186/s12877-018-0732-4
12. Bukht MS, Ahmed KR, Hossain S, Masud P, Sultana S, Khanam R. Association between physical activity and diabetic complications among Bangladeshi type 2 diabetic patients. Diabetes Metab Syndr. 2019;13(1):806–809. doi:10.1016/j.dsx.2018.11.069
13. Barcellos FC, Del Vecchio FB, Reges A, et al. Exercise in patients with hypertension and chronic kidney disease: a randomized controlled trial. J Hum Hypertens. 2018;32(6):397–407. doi:10.1038/s41371-018-0055-0
14. Cai Z, Yang Y, Zhang J. Effects of physical activity on the progression of diabetic nephropathy: a meta-analysis. Biosci Rep. 2021;41:BSR20203624.
15. Tremblay MS, Aubert S, Barnes JD, et al. Sedentary Behavior Research Network (SBRN) - Terminology Consensus Project process and outcome. Int J Behav Nutr Phys Act. 2017;14(1):75. doi:10.1186/s12966-017-0525-8
16. Teychenne M, Ball K, Salmon J. Sedentary behavior and depression among adults: a review. Int J Behav Med. 2010;17(4):246–254. doi:10.1007/s12529-010-9075-z
17. Lavie CJ, Ozemek C, Carbone S, Katzmarzyk PT, Blair SN. Sedentary behavior, exercise, and cardiovascular health. Circ Res. 2019;124(5):799–815. doi:10.1161/CIRCRESAHA.118.312669
18. Stamatakis E, Gale J, Bauman A, Ekelund U, Hamer M, Ding D. Sitting time, physical activity, and risk of mortality in adults. J Am Coll Cardiol. 2019;73(16):2062–2072. doi:10.1016/j.jacc.2019.02.031
19. Hannan M, Ricardo AC, Cai J, et al. Sedentary behavior and change in kidney function: the Hispanic Community Health Study/Study of Latinos (HCHS/SOL). Kidney360. 2021;2(2):245–253. doi:10.34067/KID.0006202020
20. Anderton N, Giri A, Wei G, et al. Sedentary behavior in individuals with diabetic chronic kidney disease and maintenance hemodialysis. J Ren Nutr. 2015;25(4):364–370. doi:10.1053/j.jrn.2015.01.018
21. Wang L, Li J, Dang Y, Ma H, Niu Y. Relationship between social capital and depressive symptoms among type 2 diabetes mellitus patients in northwest china: a mediating role of sleep quality. Front Psychiatry. 2021;12:725197. doi:10.3389/fpsyt.2021.725197
22. Ma YC, Zuo L, Chen JH, et al. Modified glomerular filtration rate estimating equation for Chinese patients with chronic kidney disease. J Am Soc Nephrol. 2006;17(10):2937–2944. doi:10.1681/ASN.2006040368
23. Hayes AF. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach. Guilford Publications; 2013.
24. MacKinnon DP, Fritz MS, Williams J, Lockwood CM. Distribution of the product confidence limits for the indirect effect: program PRODCLIN. Behav Res Methods. 2007;39(3):384–389. doi:10.3758/BF03193007
25. Glavinovic T, Ferguson T, Komenda P, et al. CKD and sedentary time: results from the Canadian Health Measures Survey. Am J Kidney Dis. 2018;72(4):529–537. doi:10.1053/j.ajkd.2018.03.031
26. Volaklis K, Mamadjanov T, Meisinger C. Sedentary behavior and kidney function in adults: a narrative review. Wien Klin Wochenschr. 2021;133(3–4):144–152. doi:10.1007/s00508-020-01673-2
27. Yu Y, Chang C, Wu Y, Guo C, Xie L. Dose-effect relationship between brisk walking and blood pressure in Chinese occupational population with sedentary lifestyles: exercise and blood pressure. J Clin Hypertens. 2021;23(9):1734–1743. doi:10.1111/jch.14340
28. Falconer CL, Cooper AR, Walhin JP, et al. Sedentary time and markers of inflammation in people with newly diagnosed type 2 diabetes. Nutr Metab Cardiovasc Dis. 2014;24(9):956–962. doi:10.1016/j.numecd.2014.03.009
29. Shuval K, Sahar L, Gabriel KP, et al. Sedentary behavior, physical inactivity, and metabolic syndrome: pilot findings from the rapid assessment disuse index study. J Phys Act Health. 2020;17(10):1042–1046. doi:10.1123/jpah.2019-0645
30. Kosaki K, Tanahashi K, Matsui M, et al. Sedentary behaviour, physical activity, and renal function in older adults: isotemporal substitution modelling. BMC Nephrol. 2020;21(1):211. doi:10.1186/s12882-020-01869-8
31. Vanden Wyngaert K, Van Craenenbroeck AH, Van Biesen W, et al. The effects of aerobic exercise on eGFR, blood pressure and VO2peak in patients with chronic kidney disease stages 3–4: a systematic review and meta-analysis. PLoS One. 2018;13(9):e0203662. doi:10.1371/journal.pone.0203662
32. Villanego F, Naranjo J, Vigara LA, et al. Impact of physical exercise in patients with chronic kidney disease: sistematic review and meta-analysis. Nefrologia. 2020;40(3):237–252. doi:10.1016/j.nefro.2020.01.002
33. Afshinnia F, Rajendiran TM, Soni T, et al. Impaired β-oxidation and altered complex lipid fatty acid partitioning with advancing CKD. J Am Soc Nephrol. 2018;29(1):295–306. doi:10.1681/ASN.2017030350
34. Sebastião E, Bobitt J, Papini CB, Nakamura PM, Kokubun E, Gobbi S. Sedentary behavior is associated with low leisure-time physical activity and high body fatness in older Brazilian adults. Am J Lifestyle Med. 2021;15(3):286–292. doi:10.1177/1559827617753355
35. Vancampfort D, Firth J, Smith L, et al. Association between physical activity and leisure-time sedentary behavior among 140,808 adolescents aged 12 to 15 from 47 low- and middle-income countries. Public Health. 2021;199:1–9. doi:10.1016/j.puhe.2021.08.001
36. Mansoubi M, Pearson N, Biddle SJ, Clemes S. The relationship between sedentary behaviour and physical activity in adults: a systematic review. Prev Med. 2014;69:28–35.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Influence of Central Obesity on Associations Between Physical Activity, Sitting Time, and Metabolic Syndrome Among Middle-Aged and Older Adults in Urban China: A Cross-Sectional Study
He Y, Wang J, Wang J, Qiu R, Wang S, Jin T, Li H, Zheng F
Diabetes, Metabolic Syndrome and Obesity 2024, 17:2555-2569
Published Date: 21 June 2024