Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Examining Ethnic Disparities in Digital Healthcare Services Utilization: Insights from Israel
Authors Obeid S, Mashiach-Eizenberg M, Gur A ![]() , Lavy I
, Lavy I
Received 22 August 2023
Accepted for publication 24 October 2023
Published 17 November 2023 Volume 2023:16 Pages 3533—3544
DOI https://doi.org/10.2147/JMDH.S429121
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Samira Obeid,1,2 Michal Mashiach-Eizenberg,3 Amit Gur,3 Ilana Lavy4
1Department of Nursing, The Max Stern Yezreel Valley College, Yezreel Valley, Israel; 2Public Health Research Department, North District, the Ministry of Health, Nof Hagalil, Israel; 3Department of Health Systems Management, The Max Stern Yezreel Valley College, Yezreel Valley, Israel; 4Department of Information Systems, The Max Stern Yezreel Valley College, Yezreel Valley, Israel
Correspondence: Samira Obeid, The Max Stern Yezreel Valley College, Emek Yezreel, 1930600, Israel, Tel +972-4- 6557894 ; +972-50-624-3784, Email [email protected]
Purpose: The purpose of this study was to examine ethnic disparities in the utilization of digital healthcare services (DHS) in Israel and explore the characteristics and factors influencing DHS use among the Arab minority and Jewish majority populations.
Methods: A cross-sectional correlational design was employed to collect data from 606 Israeli participants, 445 Jews, and 161 Arabs. Participants completed a digital questionnaire that assessed DHS utilization, digital health literacy, attitudes towards DHS, and demographic variables.
Results: The findings reveal significant disparities in DHS utilization and attitudes between these ethnic groups, with Jewish participants demonstrating higher rates of utilization and positive attitudes toward DHS. The study also explores the predictive role of digital health literacy and attitudes in DHS use while considering ethnicity as a potential moderator. Significant predicting factors related to DHS utilization among Jews include positive attitudes and high health literacy. Among the Arabs, only attitudes towards DHS significantly predict the extent of DHS use. Digital health literacy affects the extent of use through attitudes at the two groups of the moderator significantly, but it is stronger among the Arab group.
Conclusion: To improve healthcare outcomes and reduce disparities, efforts should focus on ensuring equitable access to DHS for the Arab minority population. Targeted interventions, including digital literacy education, removing technology access barriers, offering services in Arabic, and collaborating with community organizations, can help bridge the gap and promote equal utilization of DHS.
Keywords: health literacy, digital health literacy, Arabs, minority, Jews
Introduction
Digital healthcare services (DHS) have become an integral part of the health services provided by healthcare organizations in Israel and in the world, and it has been called as “virtual service revolution”.1 It is part of the technological revolution developed in many fields and offers solutions to the growing burdens in the health systems. In addition, the DHS aims to decrease the gap between the requirements of available and accessible services and the lack of resources.2 DHS can support health systems to deliver more health care, to promote health and prevent diseases.3,4 Such services were also effective in hospitals, and they can reduce demand for (in-house) consultations, medical procedures, and unnecessary hospitalizations and improve postoperative monitoring of patients.5,6 DHS can also be beneficial for individuals and patients with chronic diseases; it supports self-management and preventive behaviors related to chronic diseases.3,7
It seems that in recent years the tendency to rely on technology in the field of healthcare services is expanding.8,9 DHS includes a wide range of services like mobile applications of digital information technologies and more. In Israel, the four health maintenance organizations (HMOs) started developing such services many years ago, and it became essential after the outbreak of the corona virus. It includes websites, consultation with different specialized physicians, maternity care, service for receiving prescriptions and information about pharmacies, administrative services, and more.
The utilization of DHS was less among certain groups based on various factors. These factors include advanced age, male gender, lower levels of education and income, and a disadvantaged socioeconomic background.10–13 Obstacles to DHS utilization can also arise from the breakdown or interference of established resources or systems.14 Huxley et al15 in their review refer to barriers among marginalized groups (itinerant populations such as refugees, homeless people, unemployments) compared to the general population. The review revealed that marginalized groups reported access difficulties and stigmatizing reactions from health professionals and other patients. Previous qualitative, quantitative, and mixed articles analysis review16 showed that eHealth can widen the gap between those at risk of social health inequalities and the rest of the population. Ethnicity and low income were the most commonly used characteristics to identify people at risk of social health inequality.
Norman & Skinner17 found that high levels of health literacy in general, and digital health literacy in particular, is needed for the utilization of DHS. Health literacy is defined as “the degree to which individuals can obtain, process, understand, and communicate about health-related information needed to make informed health decisions” p.16.18 When digital health literacy, in addition, requires more skills to obtain online health information.17,19 Previous research indicated that higher levels of digital health literacy related to better health, healthy behaviors, and increased knowledge regarding the management of chronic diseases.20 Levels of digital health literacy were low among disadvantaged population groups with low socioeconomic status. A literature review and meta-analysis21 found that accessibility to infrastructure and low levels of education were the main factors for this. Digital health literacy is a crucial means that now goes beyond restricted access to information to the denial of actual healthcare services. It is imperative to recognize that in the third millennium, digital literacy has evolved beyond mere technological expertise and has become a tool that empowers individuals to access various services, including healthcare, on an equal footing.
Other studies also report that the most powerful predictors of not using information technology among older adults are cognitive decline associated with aging processes and attitudes such as anxiety about computer use and the perception that the technology was not useful for them.22–24 Numerous models have been created to explore and comprehend the factors that influence the acceptance of computer technology. The technology acceptance model (TAM) proposed by Davis25 was one of those theories. The theory proposes that user acceptance, which is affected by three elements, namely perceived usefulness, perceived ease of use, and attitudes towards usage of the system, can determine the effectiveness of a system. The theoretical frameworks utilized to examine user acceptance, adoption, and usage behavior.
The Ministry of Health in Israel in 20172 declared a policy to encourage the use of digital services in order to improve the quality of care. They initiated a “National program for digital health”. Even though surveys show significant disparities between groups in utilizing DHS. Low rates were found to be among Arab minorities in Israel.2 Previous research from other countries also found low adherence rates of utilizing DHS among minority populations.1,26
This research focused on the Arab minority living in Israel. They constitute about 21% of the population in Israel.27 Almost 50% live in Northern region, 10% in the central region, 20% in Haifa, and 20% in the southern part of the country. The Arab community is characterized by low socioeconomic status and higher health disparities.28,29
Little is known about utilizing DHS among the Arab community. Recent published data (in Hebrew) of Laron et al30 found that more than 90% of Arabs use the internet and have smartphones. 60% of them reported that they use telehealth services just to set a doctor appointment. Two-thirds did use the health plan’s application. The main barrier for using such services was a lack of awareness about using DHS, when previous acquaintances with the doctor and services in Arabic were facilitating factors. There was a significant correlation between education level and the utilization of telehealth for written communication with a known healthcare professional. They concluded that even though high percent of the Arabs have an access to the internet, the usage of the DHS is still limited. Thus, this research aims to deepen the knowledge about the other characteristics and barriers of DHS among the Arab community compared to the Jewish community in Israel and to examine the general model of literacy, including attitudes and usage, and to investigate the impact of ethnicity on individuals’ patterns of use.
Following, the research hypotheses are:
- There will be differences in the research variables (extent of use, attitudes towards DHS, and digital health literacy) between the ethnic groups and genders.
- There will be a positive relationship between digital health literacy and the extent of use of DHS between the two ethnic groups.
- There will be a positive relationship between attitudes towards DHS and the extent of use of DHS between the two ethnic groups.
- Attitudes towards DHS will mediate the relationship between digital health literacy and the extent of use of DHS.
Materials and Methods
Study Design
This study used a cross-sectional correlational design. An online survey was conducted during 13 September to 01 October 2022 using a closed digital questionnaire. The questionnaire was administered via a well-known survey institute to a panel of optional respondents sample of 609 Israeli citizens. The survey was conducted in Hebrew and Arabic. Participation in the survey was voluntary, and participants were not offered any compensation.
Participants and Data Collection
A representative sample of 609 subjects participated in the study: 165 from the central region, 123 from Tel Aviv, 88 from the northern region, 83 from Haifa, 80 from the southern region, 45 from Jerusalem, and 23 from the Judea and Samaria region. The inclusion criteria were Israeli adults Arabs and Jews. It should be noted that the Arab population in Israel is overrepresented in this study, and the sample represents the distribution of the insured in the various health maintenance organizations. Participants were first informed about the purpose of the study and maintained participant confidentiality. They were informed about the option to refuse to complete the questionnaire or stop filling it out at any time without any consequence to themselves. They then gave their informed consent.
Variables and Measurements
Demographic Characteristics
The following demographic data were collected: gender, year of birth, place of residence, marital status, number of children, religion, level of religiousness, occupation, education, financial status, health status, and membership in a health fund.
The Extent of Use of Digital Healthcare Services (DHS) Questionnaire
The extent of use of DHS questionaire based on a questionnaire developed by Even-Zohar et al31 and included eight digital healthcare services such as scheduling appointments and viewing test results. To validate the questionnaire and adapt it to the research purpose, it was forwarded to three experts who were asked about the degree of relevance of each of the items. In light of the experts’ comments, one item was omitted from the questionnaire, and 3 new items were added. The final questionnaire included 10 items. The participants were asked to mark the frequency of use for each service on a scale between 6 levels: 0 – not familiar, 1 – familiar but never used, 2 – seldom, 3 – sometimes, 4 – in most cases, and 5 – whenever necessary. For data processing, one average was calculated for the scale of extent of use of DHS and a high score indicates a greater extent of use of DHS. The questionaire internal reliability (Cronbach’s alpha) was α=0.87.
Attitudes Towards the Use of DHS Questionnaire
The questionnaire was designed for the present study. The questionnaire consists of 6 positive attitudes towards DHSs, for example: “The digital services allow me to perform actions quickly” and 4 negative attitudes, for example, “It is difficult for me to use the digital services”. The degree of agreement on each item is measured on a Likert scale between 1 – do not agree at all and 5 – agree to a very large extent. To validate the questionnaire, it was passed to three experts who were asked about the degree of relevance of each of the items. Considering the experts’ comments, the wording of three of the items was corrected and 2 new (inverted) items were added. The final questionnaire included 12 items. For data processing, one average was calculated for the scale of attitudes towards using DHS (after reversing the negative items), and a high score indicates more positive attitudes toward DHS. The internal reliability (Cronbach’s alpha) of the questioniare was α=0.86.
Digital Health Literacy Questionnaire
The questionnaire is based on Norman’s and Skinner’s17 research questionnaire. The questionnaire included eight items measuring knowledge and skill in locating, evaluating, and applying health information from digital sources. For example: “I know where to find effective health information on the Internet”. For each item, there are five answer options: 1 – do not agree at all and up to 5 – agree to a large extent. The Arabic version of the questionnaire was translated and validated by Wångdahl et al32 and high internal reliability was found (0.92). For data processing, one average was calculated for the scale of digital health literacy and a high score indicates a higher literacy towards DHS. In the present study, the internal reliability (Cronbach’s alpha) was α=0.91.
Data Analysis
Analyses were conducted using the IBM SPSS Statistics 25.0. The analysis was calculated on 606 responses. The missing values were less than 0.02% and were not replaced. Cronbach’s α coefficient was measured to verify the reliability of the measurement tools used in the study. Group comparisons were performed using the t-test for continuous variables and the χ2 test for categorical variables. To compare the means of the research variables between the ethnic groups and gender we used 2×2 ANOVA’s. Correlations between the study variables were analyzed using Pearson correlations. We used Fisher r-to-z transformation to compare the correlations between the two ethnic groups. We conducted a hierarchical regression analysis to test all relationship variables contribution to predicting the extent of the use of DHS. Finally, we conducted an analysis using the PROCESS macro for SPSS (model 7) to examine the moderated mediation model for predicting the extent of use of DHS.33 A 95% confidence interval (CI) was calculated for each regression coefficient included in the model. The moderated mediation approach utilizes a bootstrap test, for which we generated 5000 samples, to produce 95% confidence intervals, which indicate a significant indirect effect if they do not include 0.34
Results
Participant Demographic Characteristics
The study included 606 participants from two ethnic groups: 445 Jews and 161 Arabs. Table 1 shows significant differences in gender, religiousness, income level, number of children and health condition between the two ethnic groups. Among the Jews, 55.3% were women, 60.9% were married, whose ages ranged from 20 to 84 years (M = 43.9, SD = 16.4), and parents to an average of 1.9 children (SD=1.8). Most of the Jews reported that they were secular or traditional (83.1%). Moreover, more than half of them have an academic education (55.5%), and most are salaried employees (70.9%) and almost half with lower than average level of income (41.6%). Most of the Jews participants reported being in good or very good health (90.3%), while only 28.8% have a chronic disease. Among the Arabs, 38.5% were women, 72.0% were married, whose ages ranged from 21 to 69 years (M = 41.7, SD = 11.9), and parents to an average of 2.5 children (SD=2.1). Most of the Arabs reported that they are secular or traditional (62.1%). Additionally, half of them hold an academic education (50.3%), and most are salaried employees (71.9%) and with lower-than-average levels of income (82.6%). Finally, most of the Arabs reported being in good or very good health (74.5%), with only 28.0% have a chronic disease.
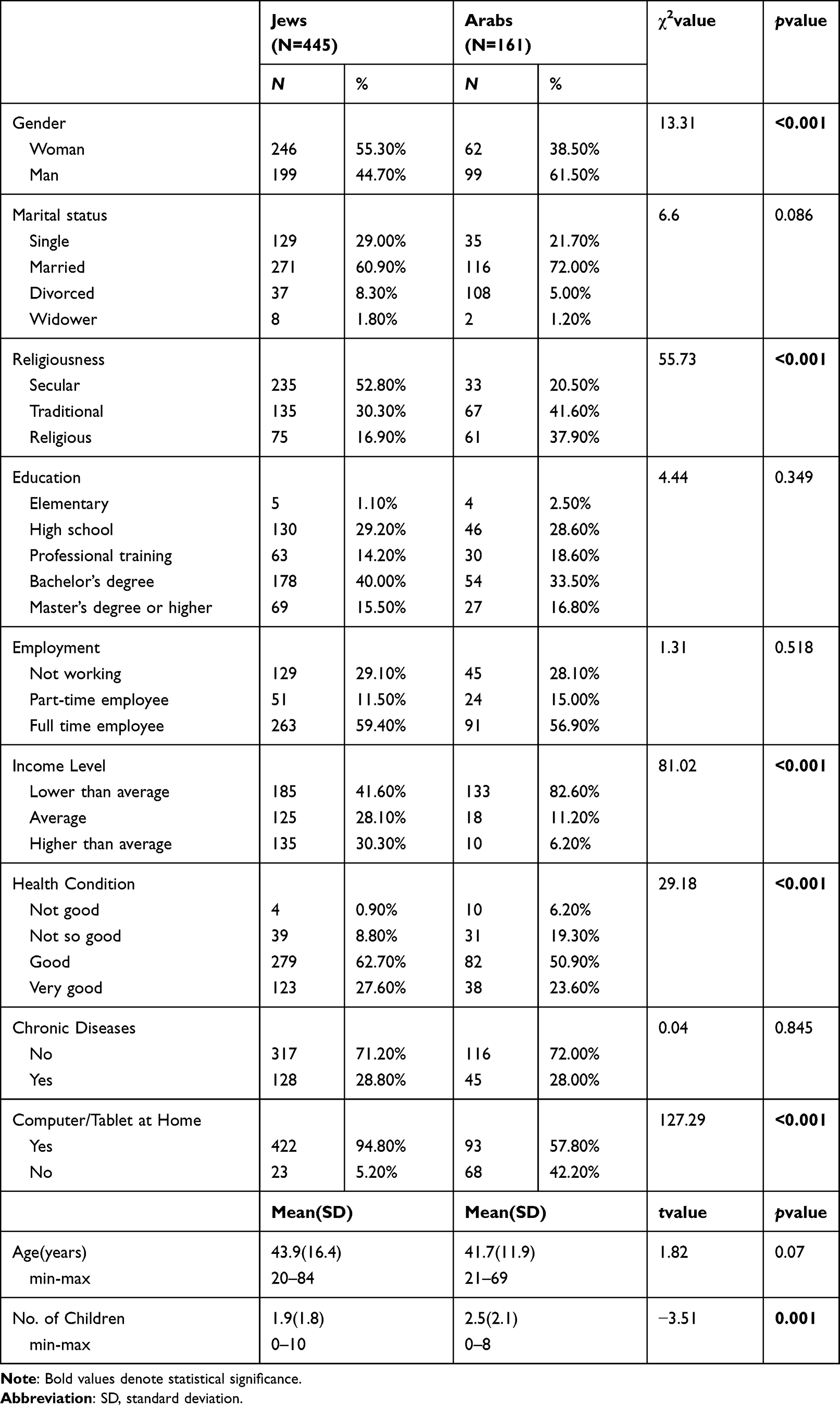 |
Table 1 Comparison of Demographic Characteristics Between the Ethnic Groups (N=606) |
Differences in the Research Variables Between the Ethnic Groups and Gender
A 2×2 ANOVA was performed in order to compare the means of the research variables between the Jews and Arabs and between woman and men. Table 2 presents the results of these analyses.
 |
Table 2 Mean Differences in the Research Variables Between the Ethnic Groups and Gender |
Significant main effect of ethnicity was found for the extent of use of DHS [F (1,602) = 31.20, p<0.001, ηp2=0.05)], and for attitudes towards DHS [F(1,602)=45.06, p<0.001, ηp2=0.07)]. On average, the Jewish participants use more DHS and have more positive attitudes towards them than Arab participants. There were no significant differences in digital health literacy between Jews and Arabs. In addition, there was no significant main effect for gender in all research variables. Finally, there was no significant interaction effect between gender by ethnicity in any of the measures.
Table 3 shows χ2 tests to examine the differences between Jews and Arabs in each item of the extent of DHS utilization. The table shows that except of using online pharmacy (item 10) the Jews use all operations more frequently than Arabs do.
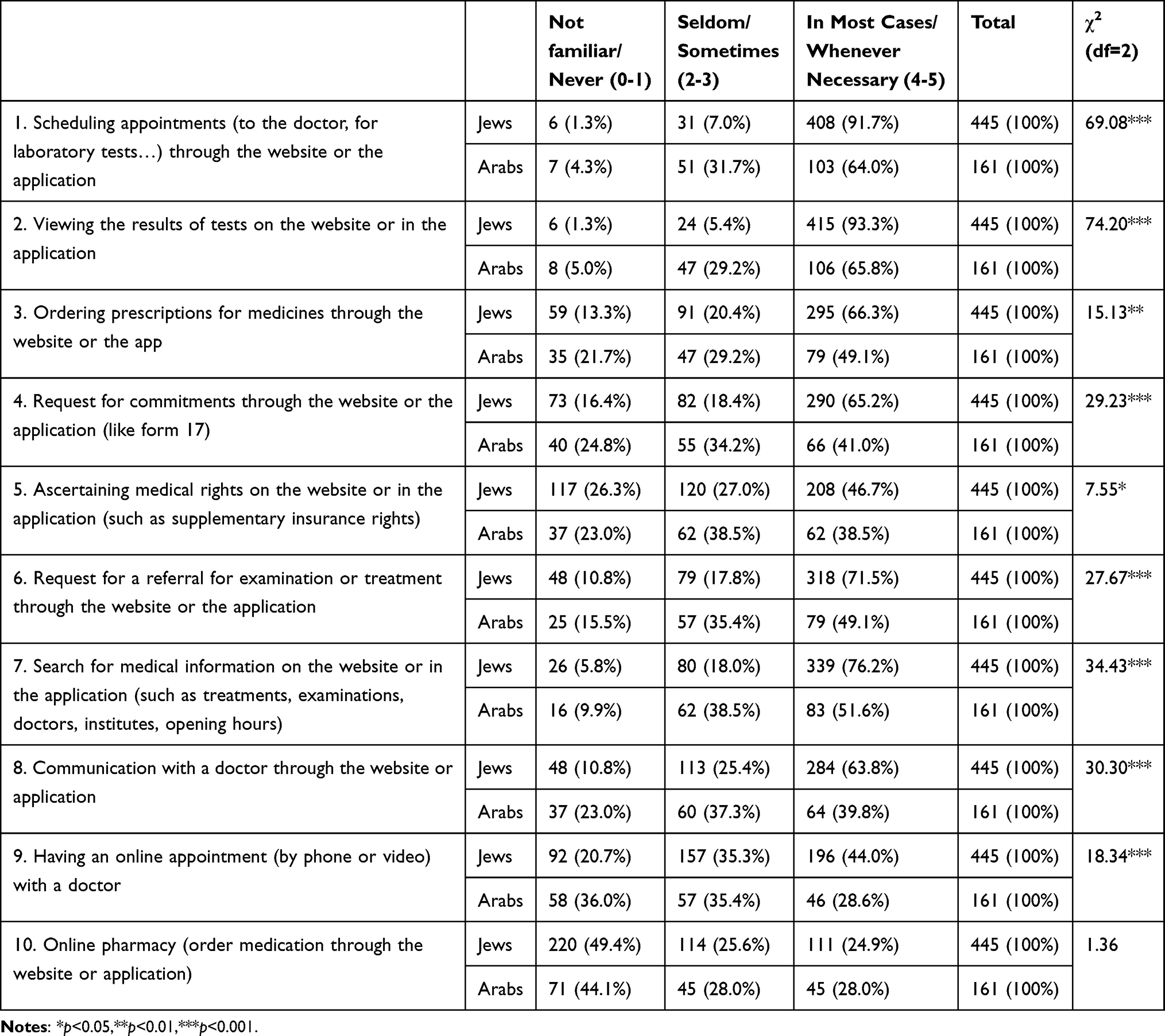 |
Table 3 Differences in the Extent of Use of DHS Between Ethnic Groups |
Relationship Among the Research Variables in the Two Ethnic Groups
Correlations between the research variables (extent of use, attitudes, and digital literacy) were explored and are reported in Table 4.
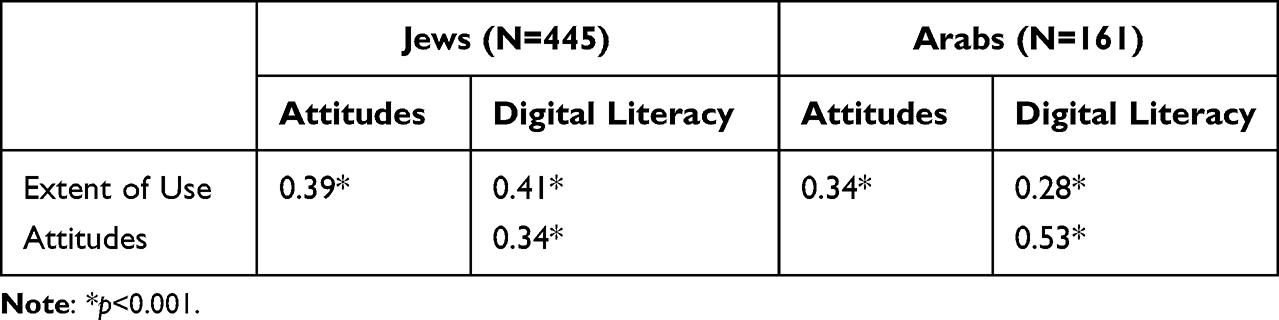 |
Table 4 Pearson Correlations Between the Research Variables Among the Two Ethnic Groups |
As can be seen, in both groups there was a significant positive correlation between the extent of use of DHS and attitudes towards DHS (r=0.39 for Jews and r=0.34 for Arabs). In Fisher Z test no significant difference was found between those correlations (z=0.62, p>0.05). In addition, a significant positive correlation was found between the extent of the use of DHS and digital health literacy in both groups. Although the correlation is stronger among the Jews (r=0.41) than among the Arabs (r=0.28), in Fisher Z test no significant difference was found between those correlations (z=1.60, p>0.05).
In contrast, the correlation between digital health literacy and attitudes towards DHS is significantly stronger among Arabs (r=0.53) than Jews (r=0.34). In Fisher Z test, significant differences were found between those correlations (z = −2.55, p < 0.01).
Hierarchical Linear Regression Analysis for Predicting Extent of Use of DHS
Hierarchical linear regression was used to predict the extent of the use of DHS in the two ethnic groups. Step one included demographic variables: gender (1-woman, 0-man), religiousness (1–religious/very religious, 0–secular/traditional), income (1–average or above, 0–below average), health condition (1–good, 0–not good), and number of children. Step two included the following variables: attitudes toward DHS and digital health literacy. The results of these analyses are presented in Table 5.
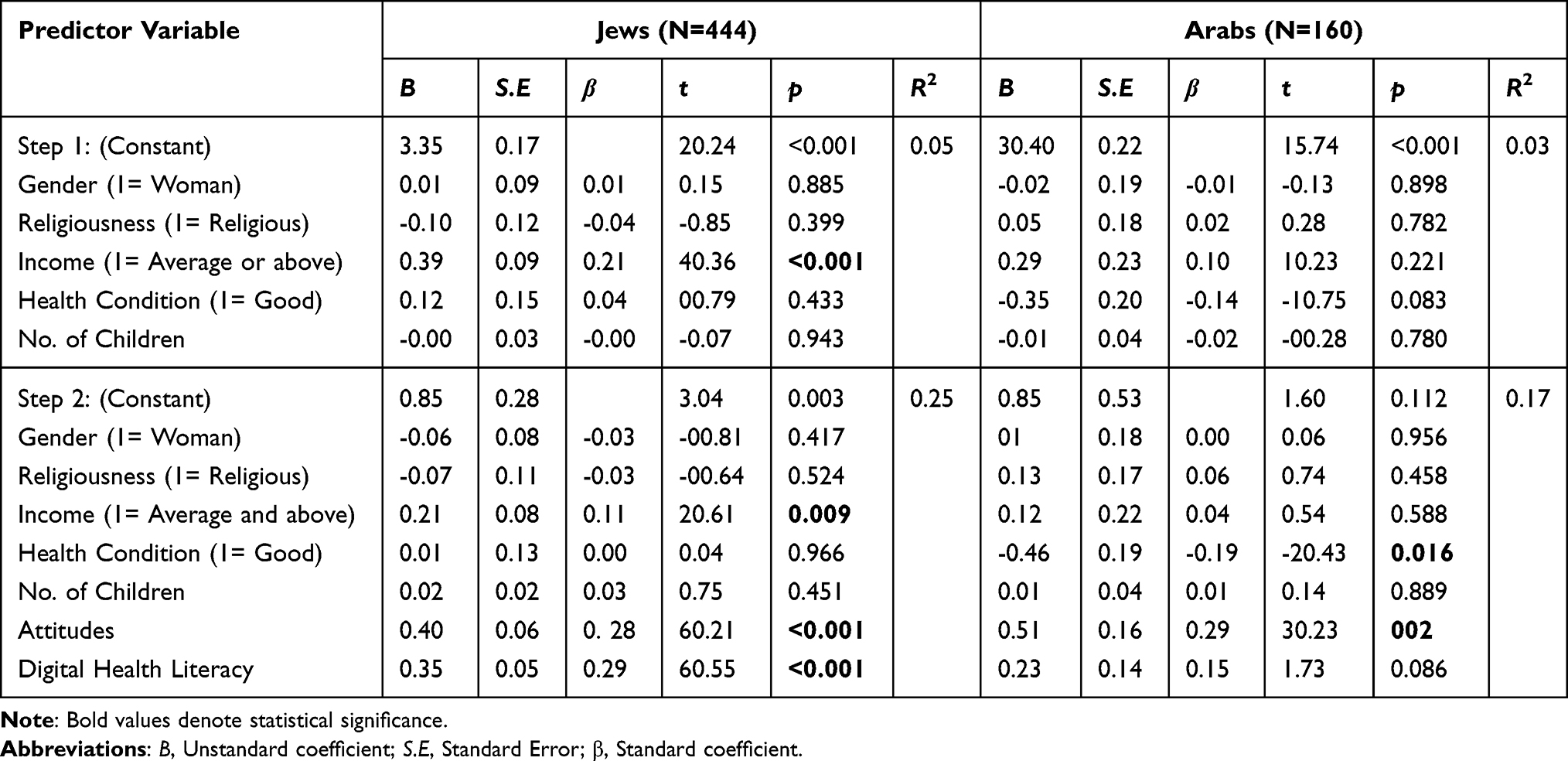 |
Table 5 Hierarchical Linear Regression Analysis for Predicting the Extent of Use of DHS Among the Ethnic Groups |
In step one, income was found to be a significant predictor of the extent of use of DHS among the Jews, whereby Jewish subjects with an average income and above use digital health services to a greater extent. Among the Arabs, the demographic variables do not significantly predict the use of DHS. Combined, the demographic variables explained 5% of the variance of the extent of use among the Jews and 3% among the Arabs. In step two, attitudes towards DHS and digital health literacy were significant predictors of the extent of use among the Jews. It was found that the more positive the attitudes and the higher the literacy, the greater the extent of use of DHS. These research variables added an additional 20% to the explained variance. Among the Arabs, only attitudes towards DHS were found to be significant predictor of the extent of use of DHS. Step 2 added an additional 14% to the explained variance. In total, our model explained 25% of the variance of the extent of use among the Jews and 17% among the Arabs. Moreover, the model is statistically significant in both groups [F(7,436)=20.93, p<0.001 for Jewish and F(7,152)=4.50, p<0.001 for Arabs].
Moderated Mediation Model for Predicting the Extent of Use of DHS
To test the moderated mediation model for predicting the extent of use of DHS, linear regression was used using Model 7 in the macro-PROCESS.33 The independent variable was digital health literacy, and the mediating variable was attitudes toward DHS. The Ethnicity was chosen as moderating the relationship between digital health literacy and the attitudes towards DHS since a significant difference was found in the correlation between these two variables between Jews and Arabs. The results of this analysis are presented in Figure 1.
 |
Figure 1 A Moderated Mediation Model for Predicting the Extent of Use of DHS. The model based on Hayes’ (2017) PROCESS model 7, unstandardized regression coefficients are provided along the paths. *p<0.05, **p<0.001. Abbreviation: Int, Interaction. |
The bootstrap analysis (5000 samples)34 was used in PROCESS 3.0 Model 7.33 The results of the analysis are presented in Table 6.
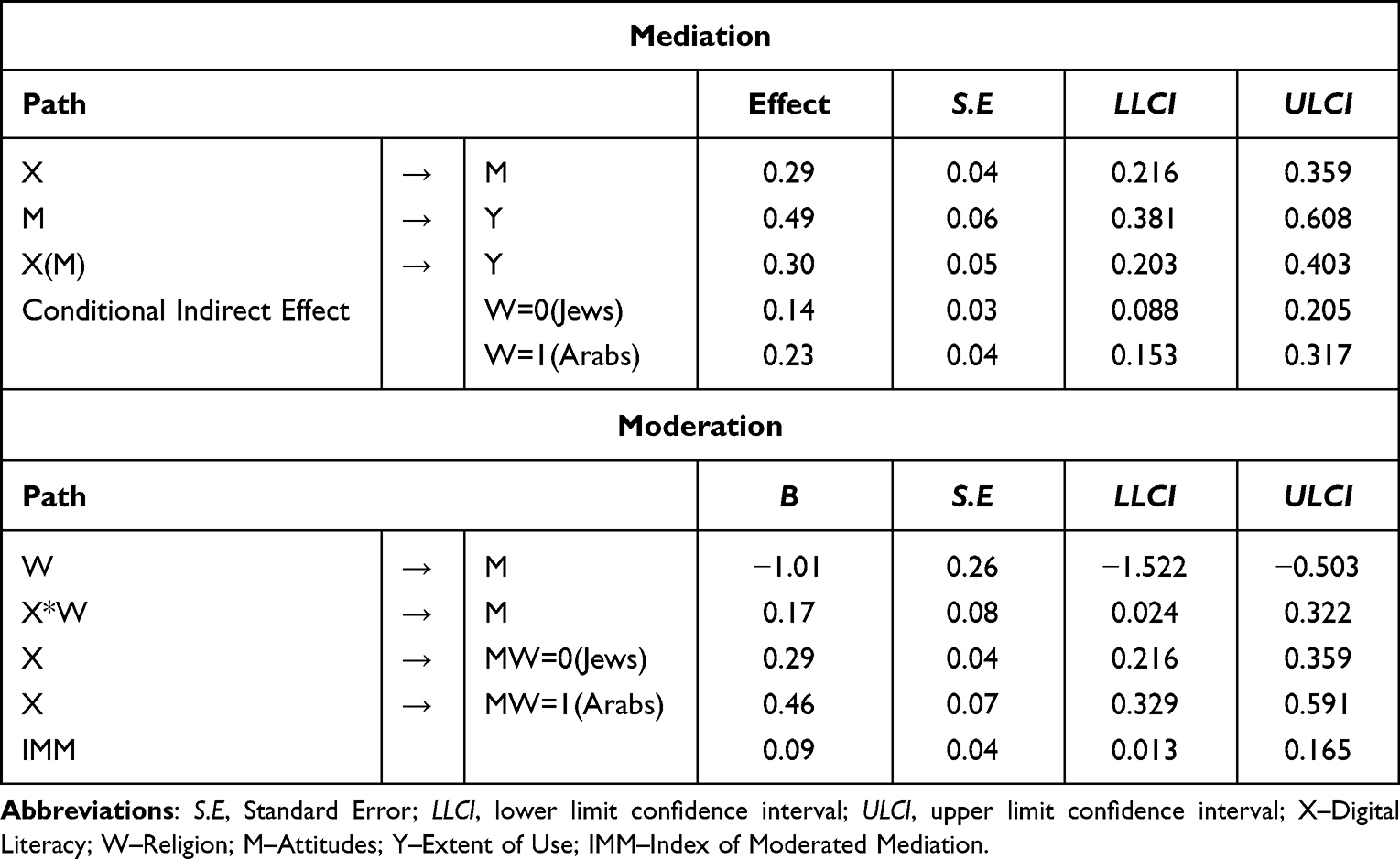 |
Table 6 Results of the PROCESS Model 7 Analysis (N=606) |
As can be seen in Table 6, the interaction between digital health literacy (X) and religion (W) is significant. The effect of digital literacy (X) on attitudes (M) was more substantial for Arabs (b=0.46) than for Jews (b=0.29). In addition, the index of moderated mediation (IMM) indicated that religion (W) moderated the indirect effect of digital health literacy (X) on extent of use (Y) through attitudes (M). The indirect effect of digital health literacy on the extent of use through attitudes was significant at the two groups of the moderator but is stronger among the Arab group. This finding suggests that the effect of digital health literacy via attitudes on the extent of use was moderated by ethnicity.
Discussion
DHS has the potential to improve healthcare access and outcomes for all populations, including minorities. However, minority communities may face barriers in utilizing digital health tools due to a lack of technological access, lower income, language barriers, and limited digital health literacy. The current research investigated the characteristics of DHS utilization and the barriers related to it and compared among the communities living in Israel Jews as a majority and Arabs as a minority. The results show that on average, the Jewish participants use more digital services and have more positive attitudes toward them than the Arabs have. Examining the differences in the extent of use of DHS between Jews and Arabs in each of the utilizing issues revealed that Jews use all operations more frequently than Arabs except for online pharmacy (both have low usage rates). Significant predicting factors related to DHS utilization among Jews include positive attitudes and high digital health literacy. Among the Arabs, only attitudes towards DHS were found to be a significant predictor of the extent of DHS use. Moreover, digital health literacy significantly affects the extent of use through attitudes in both groups but it is stronger among the Arab group. This finding suggests that the effect of digital health literacy via attitudes on the extent of use was moderated by ethnicity.
The Arab minority do not have limited access to technology, as the latest unpublished data from 2021 shows that more than 90% of Arabs use the internet and have smartphones.30 Another research held in 2019 also reported small differences between the Jewish and Arab communities in the daily rate of internet use (82% compared to 77%, respectively) and a considerable gap in the rate of computer use among the same groups (77% Jews compared to 46% among Arabs).35 Despite these facts, the results of the current study still indicate disparities in utilizing DHS between Arabs and Jews. One of the factors related to these disparities is cultural barriers. There may be a distrust that leads to discomfort in using this technology and utilizing DHS among the Arab community, which may prevent them from using it. Lack of trust can emerge due to concerns about privacy, data security, and the accuracy of health information obtained through digital platforms. Previous research indicates trust as a necessary aspect of successfully using electronic health records and other electronically stored health information.36 It is particularly important for low-income communities.37 Mistrust of the Arab community on the health system raised on the recent years during and after the COVID 19 pandemic. Research conducted in 2021 and 202238,39 found moderate to low levels of trust in the health system among the Arab community. A related concern to safety use is the fact that private information is being recorded and stored.40
Moreover, language can be another cultural barrier to using DHS as it affects a person’s ability to understand and navigate the technology. If DHS is not offered in a person’s native language or if the language used is not accessible or understandable, it can limit their ability to use these services and benefit from them effectively. This can also lead to mistrust, confusion, and, ultimately, decreased usage of DHS among certain cultural groups. Language barriers can also affect the accuracy of information exchanged and the quality of care received, leading to further disparities in healthcare access and outcomes.41–43 The participants reported on language translation and cultural adaptation as a crucial factors enabling them to use the DHS. Therefore, digital health providers need to consider the linguistic diversity of their target population and offer services in multiple languages to ensure equitable access and utilization of these resources.
The study found that digital literacy and attitudes toward using DHS are factors that explain the differences in the use of DHS among different groups. According to the Technology Acceptance Model (TAM),25 a person will use digital services if they have both the perceived ability and the skills to do so and perceive the usefulness of it. The study found that Jews had more positive attitudes towards using DHS and higher digital literacy levels, which led to higher usage of digital health services. However, among Arabs, the low levels of general literacy, which affects digital literacy and brings them to have negative attitudes towards using digital services, resulted in lower usage of DHS. It was also found that people with low digital literacy would only use technology for simple tasks, such as playing games or browsing websites.44
To conclude, the study showed that compared to Arabs, Jews have more positive attitudes toward the use of DHS and a higher digital health literacy, which perhaps leads to higher utilization rates. The use of DHS has already been proven to contribute to improving and maintaining health in most studies, and it can also contribute to closing the gaps in health between population groups of different socioeconomic status, such as the Jewish and Arab populations. Addressing these barriers and ensuring equal access to DHS is essential to reducing healthcare disparities among the Arab communities in Israel. It can be done through targeted digital literacy education, removing barriers to technology access, offering services in Arabic, designing and implementing reward strategies to motivate them to use DHS, and collaborating with community organizations to reach underserved populations.
Limitations
Although the sample in the study was a representative, the questionnaire was distributed online, through the Internet. This method can be convenient, on the one hand, as the researchers can reach a large number of participants. Yet, on the other hand, it can be a limitation. Since online surveys may only reach a limited sample, as not all people have access to or are comfortable using the internet or electronic devices. This can lead to the underrepresentation of certain groups and might limit the generalizability of the findings. Participants in online surveys self-select to participate, which can introduce bias into the sample. People who choose to participate may differ from those who do not in important ways, which can affect the accuracy of the results. While the research, conducted in the form of a cross-sectional survey and testing a moderated mediation model, indicates a possible causal link between variables, it's essential to emphasize that the analysis serves as a supplementary tool and cannot definitively establish causal relationships. Thus, the model in this research provides evidence for a possible explanation of the relationship between variables, but it does not prove that the relationship is causal.
Ethics Considerations
This study complies with the Declaration of Helsinki. Ethical approval was obtained from the Yezreel Valley College Ethics Committee before data collection (Approval No. YVC EMEK 2022-61).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sieck CJ, Sheon A, Ancker JS, Castek J, Callahan B, Siefer A. Digital inclusion as a social determinant of health. NPJ Digit Med. 2021;17(1):52. doi:10.1038/s41746-021-00413-8
2. Israel Ministry of Health. Digital Health: strategy. Hebrew. Available from: https://health.gov.il/PublicationsFiles/DigitalHealthStrategyApril2017.pdf.
3. Argent R, Daly A, Caulfield B. Patient involvement with home-based exercise programs: can connected health interventions influence adherence? JMIR mHealth uHealth. 2018;6(3):e8518. doi:10.2196/mhealth.8518
4. Dillingham R, Ingersoll K, Flickinger TE, et al. Positive Links: a mobile health intervention for retention in HIV care and clinical outcomes with 12-month follow-up. AIDS Patient Care STDS. 2018;32(6):241–250.
5. Pollock DA. Digital platforms as a method of invention for infection surveillance. Surg Infect. 2019;20(7):581–583. doi:10.1089/sur.2019.147
6. Singh K, Drouin K, Newmark LP, et al. Developing a framework for evaluating the patient engagement, quality, and safety of mobile health applications. Issue Brief. 2016;18(1):11.
7. Wang Y, Min J, Khuri J, et al. Effectiveness of mobile health interventions on diabetes and obesity treatment and management: systematic review of systematic reviews. JMIR mHealth uHealth. 2020;8(4):e15400. doi:10.2196/15400
8. Bolton RN, McColl-Kennedy JR, Cheung L, et al. Customer experience challenges: bringing together digital, physical and social realms. J Serv Manag. 2018;29(5):776–808. doi:10.1108/JOSM-04-2018-0113
9. McColl-Kennedy JR, Hogan SJ, Witell L, Snyder H. Co- creative customer practices: effects of health care customer value co- creation practices on well-being. J Bus Res. 2017;70:55–66. doi:10.1016/j.jbusres.2016.07.006
10. Kim H, Mahmood A, Goldsmith JV, Chang H, Kedia S, Chang CF. Access to broadband internet and its utilization for health information seeking and health communication among informal caregivers in the United States. J Med Syst. 2021;45(2):1–9. doi:10.1007/s10916-021-01708-9
11. Nwokeji U, Spaulding EM, Shan R, et al. Health information technology use among persons with self-reported atherosclerotic cardiovascular disease: analysis of the 2011–2018 National Health Interview Survey. J Med Internet Res. 2021;23(8):e23765. doi:10.2196/23765
12. Onyeaka H, Firth J, Kessler RC, Lovell K, Torous J. Use of smartphones, mobile apps and wearables for health promotion by people with anxiety or depression: an analysis of a nationally representative survey data. Psychiatry Res. 2021;304:114120. doi:10.1016/j.psychres.2021.114120
13. Onyeaka HK, Acquah I, Firth J, et al. Trends and factors associated with use of digital health technology among adults with serious psychological distress in the United States: a secondary data analysis of the National Health Interview Survey. Popul Med. 2022;10(4):1–7. doi:10.18332/popmed/145913
14. Mair FS, May C, O’Donnell C, Finch T, Sullivan F, Murray E. Factors that promote or inhibit the implementation of e-health systems: an explanatory systematic review. Bull World Health Organ. 2012;90(5):357–364. doi:10.2471/BLT.11.099424
15. Huxley CJ, Atherton H, Watkins JA, Griffiths F. Digital communication between clinician and patient and the impact on marginalised groups: a realist review in general practice. Br J Gen Pract. 2015;65(641):e813–21. doi:10.3399/bjgp15X687853.65/641/e813
16. Latulippe K, Hamel C, Giroux D. Social health Inequalities and eHealth: a literature review with qualitative synthesis of theoretical and empirical studies. J Med Internet Res. 2017;19(4):e136. doi:10.2196/jmir.6731
17. Norman CD, Skinner HA. eHEALS: the eHealth literacy scale. J Med Internet Res. 2006;8(4):e507. doi:10.2196/jmir.8.4.e27
18. Berkman ND, Davis TC, McCormack L. Health literacy: what is it? J Health Commun. 2010;31(S2):9–19. doi:10.1080/10810730.2010.499985
19. Ortiz DN. Digital health literacy. In
20. Van Der Vaart R, Drossaert C. Development of the digital health literacy instrument: measuring a broad spectrum of health 1.0 and health 2.0 skills. J Med Internet Res. 2017;19(1):e27. doi:10.2196/jmir.6709
21. Marta E, Semedo G, Roque F, Ferreira PL, Herdeiro MT. Sociodemographic determinants of digital health literacy: a systematic review and meta-analysis. Int J Med Inform. 2023;177:105124. doi:10.1016/j.ijmedinf.2023.105124
22. Charness N, Boot WR. Aging and information technology use. Curr Dir Psychol Sci. 2009;18(5):253–258. doi:10.1111/j.1467-8721.2009.01647.x
23. Czaja SJ, Lee CC. The impact of aging on access to technology. Univ Access Inf Soc. 2006;5(4):341–349. doi:10.1007/s10209-006-0060-x
24. Werner JM, Carlson M, Jordan-Marsh M, Clark F. Predictors of computer use in community-dwelling, ethnically diverse older adults. Hum Factors. 2011;53(5):431–447. doi:10.1177/0018720811420840
25. Davis FD. Perceived usefulness, perceived ease of use, and user acceptance of information technology. MIS Q. 1989;1(3):319–340. doi:10.2307/249008
26. Klonoff DC, Shang T, Zhang JY, Cengiz E, Mehta C, Kerr D. Digital connectivity: the sixth vital sign. J Diabetes Sci Technol. 2022;16(5):1303–1308. doi:10.1177/19322968211015241
27. Central Bureau of Statistics. Population - statistical abstract of Israel – no 71. Available from: https://www.cbs.gov.il/en/publications/Pages/2020/Population-Statistical-Abstract-of-Israel-2020-No-71.aspx.
28. Ghanem AA, Khatib I. The nationalisation of the Israeli ethnocratic regime and the Palestinian minority’s shrinking citizenship. Citizensh Stud. 2017;17(8):889–902. doi:10.1080/13621025.2017.1380651
29. Muhsen K, Green MS, Soskolne V, Neumark Y. Inequalities in non-communicable diseases between the major population groups in Israel: achievements and challenges. Lancet. 2017;389(10088):2531–2541.
30. Laron M, Penn N. Use and barriers to the use of telehealth services among the Arab population in Israel: Michal Laron. Eur J Public Health. 2022;32(Supplement_3):ckac131–181. doi:10.1093/eurpub/ckac131.181
31. Even-Zohar A, Ironi A, Ben-Yzhak R. Online digital health for the elder citizens in Maccabi Health Services. Gerontol Geriatr. 2017; 2:77–110. In Hebrew.
32. Wångdahl J, Dahlberg K, Jaensson M, Nilsson U. Arabic version of the electronic health literacy scale in Arabic-speaking individuals in Sweden: prospective psychometric evaluation study. J Med Internet Res. 2021;23(3):e24466. doi:10.2196/24466
33. Hayes AF. Mediation, moderation, and conditional process analysis. Introduction to mediation, moderation, and conditional process analysis: a regression-based approach; 2014:335–337.
34. Preacher KJ, Rucker DD, Hayes AF. Addressing moderated mediation hypotheses: theory, methods, and prescriptions. Multivariate Behav Res. 2007;42(1):185–227. doi:10.1080/00273170701341316
35. Dorot R Media influence matrix: Israel. CEU center for media, data and society; 2020. Available from: https://cmds.ceu.edu/sites/cmcs;ceu.hu/files/attachment/basicpage/1860/mimisraelfunding.pdf.
36. Hawley K. Trust and distrust between patient and doctor. J Eval Clin Pract. 2015;21(5):798–801. doi:10.1111/jep.12374
37. Kruse CS, Stein A, Thomas H, Kaur H. The use of electronic health records to support population health: a systematic review of the literature. J Med Syst. 2018;42(11):1–6. doi:10.1007/s10916-018-1075-6
38. Ali-Saleh O, Obeid S. Compliance with COVID-19 preventive guidelines among minority communities: the case of Israeli Arabs. J Racial Ethnic Health Disparities. 2022. doi:10.1007/s40615-022-01344-0
39. Satran C, Ali Selah O, Mashiach-Aizenberg M, Bord S. Stress and perceived discrimination among Israeli Arabs: the mediation role of threat and trust. Eur J Public Health. 2021;31(Supplement_3):ckab164–012. doi:10.1093/eurpub/ckab164.012
40. Ross J, Sebastian I, Beath C, Mocker M, Moloney K, Fonstad N. Designing and executing digital strategies: completed research paper. In
41. Flores G. The impact of medical interpreter services on the quality of health care: a systematic review. Med Care Res Rev. 2005;62(3):255–299. doi:10.1177/1077558705275416
42. Grow RW, Sztajnkrycer MD, Moore BR. Language barriers as a reported cause of prehospital care delay in Minnesota. Prehosp Emerg Care. 2008;12(1):76–79. doi:10.1080/10903120701709878
43. Karliner LS, Jacobs EA, Chen AH, Mutha S. Do professional interpreters improve clinical care for patients with limited English proficiency? A systematic review of the literature. Health Serv Res. 2007;42(2):727–754. doi:10.1111/j.1475-6773.2006.00629.x
44. Koufaris M. Applying the technology acceptance model and flow theory to online consumer behavior. Inf Syst Res. 2002;13(2):205–223. doi:10.1287/isre.13.2.205.83
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.