Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 14
Exacerbations and health care resource use among patients with COPD in relation to blood eosinophil counts
Authors Müllerová H ![]() , Hahn B
, Hahn B ![]() , Simard EP, Mu G
, Simard EP, Mu G ![]() , Hatipoğlu U
, Hatipoğlu U
Received 13 November 2018
Accepted for publication 25 February 2019
Published 22 March 2019 Volume 2019:14 Pages 683—692
DOI https://doi.org/10.2147/COPD.S194367
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Richard Russell
Hana Müllerová,1 Beth Hahn,2 Edgar P Simard,3 George Mu,3 Umur Hatipoğlu4
1Real-World Evidence, GSK, Stockley Park, Uxbridge, Middlesex, UK; 2US Medical Affairs, GSK, Research Triangle Park, NC, USA; 3Real-World Data and Analytics, GSK, Upper Providence, PA, USA; 4Center for Comprehensive Care in Chronic Obstructive Pulmonary Disease, Respiratory Institute, Cleveland Clinic, Cleveland, OH, USA
Purpose: Current understanding of the relationship between COPD phenotype and health care resource utilization (HCRU) is limited. This real-world study evaluated disease burden and HCRU for COPD subgroups prone to exacerbation as defined by blood eosinophil (EOS) count and multiple inhaler triple therapy (MITT) use.
Methods: This was a large-scale, retrospective, longitudinal, observational cohort study using data from the US IBM Watson Explorys real-world database (GSK Study HO-17-18395). The population of interest comprised patients with COPD ≥40 years of age with ≥2 moderate or ≥1 severe exacerbations (prior year) while on inhaled maintenance therapy, with ≥1 blood EOS count. Data were analyzed during the year prior to index date (last COPD encounter between January 1, 2011 and December 31, 2016). Four subgroups were analyzed based on a combination of EOS counts (<150 and ≥150 cells/μL) and MITT use (receiving or not receiving). Among these groups, clinical characteristics, exacerbations, and HCRU were described. A sensitivity analysis that further stratified EOS into four categories (<150, ≥150–<300, ≥300–<500, and ≥500 cells/μL) was also performed.
Results: The COPD population of interest comprised 34,268 patients. Subgroups with EOS ≥150 cells/µL vs ,150 cells/µL had more comorbidities and experienced significantly higher mean numbers of moderate exacerbations (not receiving MITT, ≥150 cells/µL vs <150 cells/µL: 1.93 vs 1.82, P<0.0001; receiving MITT 2.26 vs 2.16, P=0.0062) and COPDrelated emergency visits (not receiving MITT, ≥150 cells/µL vs <150 cells/µL: 3.0 vs 2.5, P<0.001; receiving MITT 3.4 vs 3.1, P=0.0011). Increasing EOS category was associated with higher HCRU.
Conclusion: Blood EOS ≥150/µL cells were associated with increased HCRU and higher exacerbation rates compared with EOS <150 cells/μL, irrespective of MITT use. COPD phenotyping using blood EOS could help identify candidates for additional therapies that target
eosinophilic inflammatory pathways.
Keywords: COPD, eosinophil, exacerbation, health care resource, phenotype
Plain language summary
COPD is characterized by persistent respiratory symptoms and difficulty in breathing, with increases in numbers of white blood cells, such as macrophages, neutrophils, and lymphocytes, in the airways, lungs, and pulmonary blood vessels. Patients with COPD may experience events of acute symptom worsening, which reduce their quality-of-life. To minimize these events and control day-to-day symptoms, patients are commonly treated with combinations of airway relaxant and inhaled anti-inflammatory medicines. However, some patients continue to have poor symptom control, despite using all currently recommended therapies. These patients may require additional medications targeting specific characteristics of their COPD. One such characteristic, high levels of inflammatory eosinophil cells in the blood, has been identified as a potential treatment target for such patients.
Current understanding of the link between COPD characteristics and patient health care use is an area of intense research. This study assessed the burden of COPD on the health care system based on the level of blood eosinophils and the type of medications used. Patients with blood eosinophil levels ≥150 cells/μL had more comorbid diseases, more acute exacerbations of COPD, and more emergency department visits than those with blood eosinophil levels <150 cells/μL; results were the same regardless of whether or not patients were using maximal therapy with three inhaled medicines. Furthermore, increasing blood eosinophil levels were associated with greater health care use.
In conclusion, measuring eosinophils in the blood of patients with COPD could help to identify those who may benefit from additional therapies that target eosinophils.
Introduction
COPD was the fourth leading cause of death worldwide during 2015.1 Patients with COPD may experience acute exacerbations, the frequency of which is directly related to their quality-of-life.2 Patients with a high symptom level and an increased risk for exacerbation are categorized as Global Initiative for Chronic Obstructive Lung Disease (GOLD) Group D. Recommended maintenance therapy for GOLD Group D is either a combination of a long-acting β2-agonist (LABA) and a long-acting anti-muscarinic antagonist (LAMA) or an inhaled corticosteroid (ICS) and a LABA.3 For patients who remain symptomatic or who continue to experience exacerbations, escalation to ICS-based inhaled triple therapy (comprising an ICS, a LABA, and a LAMA) is recommended.3 Several studies have shown that ICS-based inhaled triple therapy provides statistically significant reductions in exacerbation rates compared with either LAMA/LABA or ICS/LABA.4–8 However, some patients continue to experience symptoms despite treatment escalation.9 For these patients a precision medicine approach, focusing on treatable traits, may offer targeted therapeutic options.10
Eosinophilic airway inflammation has been observed in approximately 40% of patients during both stable and exacerbating COPD,11–13 and sputum eosinophilia (defined as >3% of non-squamous cells) has been found in approximately 28% of exacerbation events.14 As such, eosinophilic inflammation has been proposed as a treatable trait for patients with COPD.10 Targeting sputum eosinophils (EOS) in COPD has shown promise by reducing hospital visits in a randomized, parallel-group study.15 Although there are some studies in which no or unreliable correlations were found between sputum and blood eosinophil levels,16,17 a number of studies have shown that sputum EOS counts can be predicted by blood EOS counts, which are more readily measured in clinical settings.13,14,18,19 In addition, a blood EOS count ≥2%, which is approximate to ≥150 cells/μL,13 has been associated with increased exacerbations in COPD,14 and counts consistently ≥150 cells/μL are seen in approximately 50% of patients with COPD in primary care settings.20
There is little real-world epidemiological evidence exploring the relationship between blood EOS counts and clinical characteristics, health care resource utilization (HCRU), and pharmacotherapy among patients with moderate-to-severe COPD with eosinophilic inflammation, particularly from the US.
The present study evaluated different COPD subgroups based on blood EOS counts and maintenance therapy in patients exhibiting a history of exacerbations. The disease burden of each COPD subgroup was described using data from the US IBM Watson Health Explorys database.
Methods
Study design
This was a retrospective, longitudinal, observational cohort database study using data from the IBM Watson Health Explorys (Explorys) database (GSK Study ID: HO-17-18395). The data are comprised of both electronic health record fields captured during routine clinical care (including but not limited to data on health care encounters, diagnoses, tests ordered, laboratory test results, and drugs prescribed) and limited information from medical and pharmacy claims. The Explorys database is an aggregation of data from 23 Integrated Delivery Networks (IDNs), community-based networks, and value-based care programs across the US, with data from approximately 360 acute care facilities and more than 55 million patients.
The study period covered January 1, 2011 to December 31, 2016. The index date for each patient was the last COPD encounter during this time period, defined as any COPD encounter including COPD maintenance medication prescription (Figure 1). The study period was defined as the 24 months prior to the index date and included two 12-month periods: the observation period (the 12 months immediately prior to the index date) and the pre-period (24–12 months prior to the index date) to establish COPD diagnosis.
 | Figure 1 Study design. |
This research was a retrospective analysis of de-identified data from the Explorys database, and as such this analysis did not require approval from an ethics committee or institutional review board. The de-identified data are only accessible to organizations with appropriate data governance processes in place.
Study populations and descriptors
To be included in the study, patients were required to have ≥1 International Classification of Diseases code for COPD (ICD-9-CM codes 491.xx, 492.xx, or 496.xx; ICD-10-CM: J40, J41.xx, J42, J43.xx, J44.xx) recorded within the period from January 1, 2011 to 24 months prior to the index date (Figure 1). This ensured that patients had a COPD diagnosis for ≥1 year prior to the observation period. Patients were also required to be ≥40 years of age at first COPD diagnosis; have continuous electronic medical records activity for ≥2 years, including the observation period and pre-period; have ≥1 outpatient blood EOS count recorded in the previous 12 months; and dispensed ≥1 inhaled maintenance therapy, which included either ICS, LABA, or LAMA, or a combination of these medications. To be included in the population of interest, patients were also required to have a history of exacerbations (≥2 moderate or ≥1 severe COPD exacerbations in the previous year). In addition to the overall patient population, the following subgroups were investigated: (1) receiving multiple inhaler triple therapy (MITT), with blood EOS <150 cells/μL; (2) receiving MITT, with blood EOS ≥150 cells/μL; (3) not receiving MITT, with blood EOS <150 cells/μL; and (4) not receiving MITT, with blood EOS ≥150 cells/μL. MITT was defined as either three individual inhalers of ICS, LABA, and LAMA, or any 2+1 combination of ICS, LABA, and LAMA that was dispensed within a 30-day period in the observation period, with each component expected to be taken for ≥30 days. Moderate exacerbations were defined as exacerbations needing an outpatient or emergency department (ED) visit with a diagnosis of COPD and requiring treatment with an oral corticosteroid (OCS) and/or antibiotic 7 days before or after the visit; severe exacerbations were defined as exacerbations needing hospitalization with a primary diagnosis of COPD. COPD exacerbation definitions used in this study differ from those in the GOLD 2018 guidelines in that moderate exacerbations required an outpatient or ED visit in this study but not in GOLD guidelines.3 The criteria used here are in line with other previous epidemiological studies.21,22
Disease characteristics
Data were collected on demographic and lifestyle factors, EOS, selected comorbidities, COPD exacerbations, COPD-related and all-cause HCRU (including inpatient admissions, ED visits, outpatient office visits, other outpatient visits, and pharmacy prescriptions), and COPD-related pharmacy prescriptions. Where multiple blood EOS counts were measured for an individual, the highest count was used to characterize the patient.
Study analyses
Differences between subgroups were evaluated with unequal variance t-tests and chi-square tests at a significance level of α=0.05. A sensitivity analysis was performed on patients receiving MITT stratified by four EOS categories: <150 cells/μL, ≥150-<300 cells/μL, ≥300-<500 cells/μL, and ≥500 cells/μL. All analyses were conducted using SAS, version 9.3 or later (SAS Institute, Cary, NC, USA).
Ethics approval
This research was a retrospective analysis of de-identified data from the Explorys database, and as such this analysis did not require approval from an ethics committee or institutional review board. The de-identified data are only accessible to organizations with appropriate data governance processes in place.
Results
Demographic and clinical characteristics
Among 97,529 patients who met all study criteria, 34,268 additionally met the exacerbation criteria and comprised the population of interest: 3,199 (9.3%) and 7,697 (22.5%) were receiving MITT and had EOS <150 or ≥150 cells/μL, respectively (Figure 2). Greater proportions of female patients and patients with lower BMIs were observed in the subgroups with EOS <150 cells/μL than in subgroups with EOS ≥150 cells/μL, regardless of MITT use (Table 1). The subgroups not receiving MITT had lower levels of private, Medicaid, self-pay, and other public coverage compared with subgroups receiving MITT.
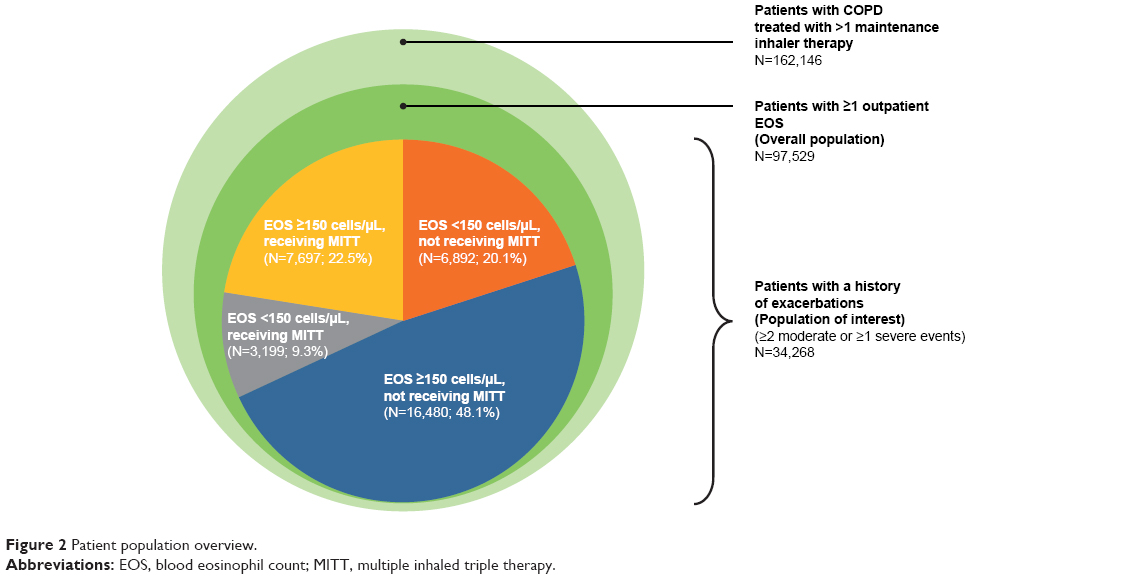 | Figure 2 Patient population overview. |
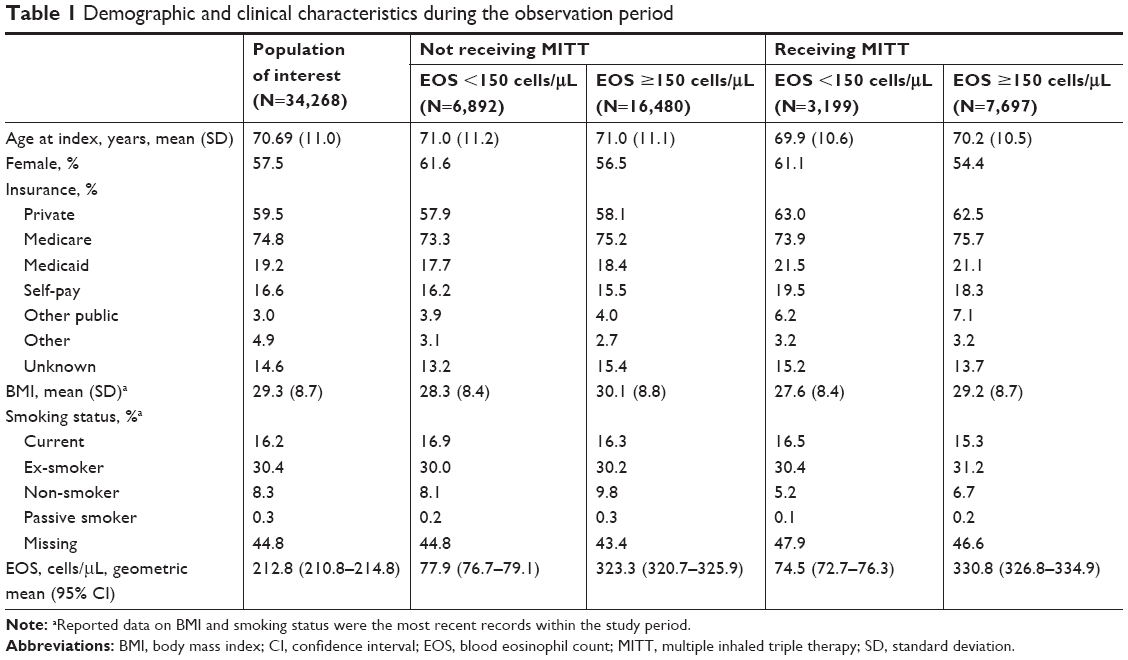 | Table 1 Demographic and clinical characteristics during the observation period |
The most common comorbidities were hypertension, diabetes, anxiety, and congestive heart failure (Table 2). The Quan-Charlson comorbidity index was higher in the subgroups with EOS ≥150 cells/μL compared with the subgroups with EOS <150 cells/μL. Subgroups not receiving MITT had higher proportions of allergic rhinitis and acute and chronic sinusitis compared with subgroups receiving MITT. Subgroups not receiving MITT also had a lower frequency of chronic heart failure, asthma, anxiety, depression, and respiratory tract neoplasm compared with subgroups receiving MITT.
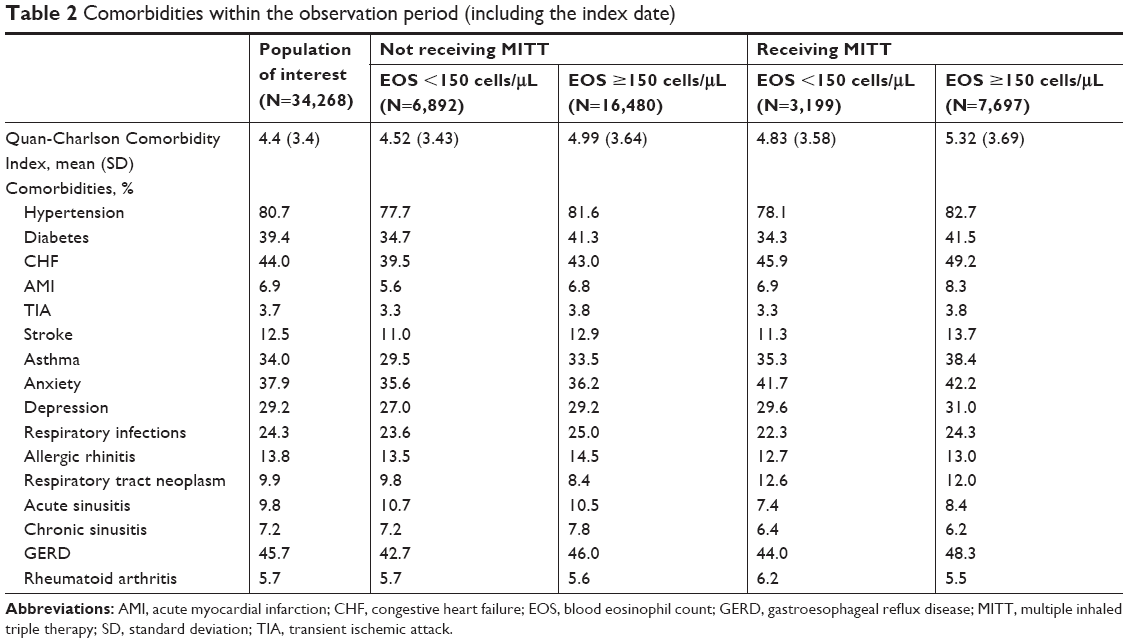 | Table 2 Comorbidities within the observation period (including the index date) |
Exacerbations and HCRU among subgroups
Patients receiving MITT with EOS ≥150 cells/μL had the highest mean numbers of moderate exacerbations compared with the other subgroups, a mean of 2.26 events vs a range of 1.82–2.16 events per patient per year (Figure 3). Moderate exacerbations were significantly more frequent in the subgroups with EOS ≥150 cells/μL vs those with EOS <150 cells/μL, regardless of MITT therapy (not receiving MITT: P<0.0001; receiving MITT: P=0.0062). No significant differences in severe exacerbations were observed for the subgroups with EOS <150 cells/μL vs ≥150 cells/μL (with or without MITT), with mean event rates per patient per year ranging between 0.65 and 0.85.
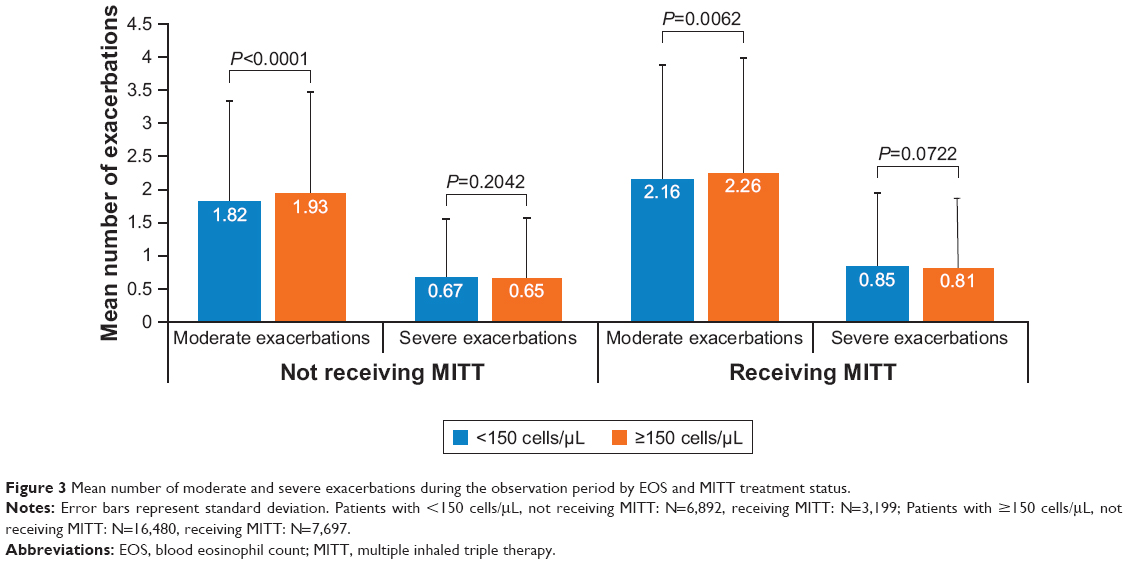 | Figure 3 Mean number of moderate and severe exacerbations during the observation period by EOS and MITT treatment status. |
In general, COPD-related HCRU was highest in the subgroup receiving MITT and with EOS ≥150 cells/μL compared with the other subgroups (Figure 4). In the subgroups not receiving MITT, ED visits, outpatient office visits, and pharmacy prescriptions were significantly higher for the subgroup with EOS ≥150 cells/μL vs <150 cells/μL (P≤0.01 for all). Similarly, in the subgroups receiving MITT, significantly higher numbers of ED visits and pharmacy prescriptions were observed for the subgroup with EOS ≥150 cells/μL vs <150 cells/μL (P=0.0011 and P=0.0141, respectively). All-cause HCRU followed a similar pattern to COPD-related HCRU (Figure S1).
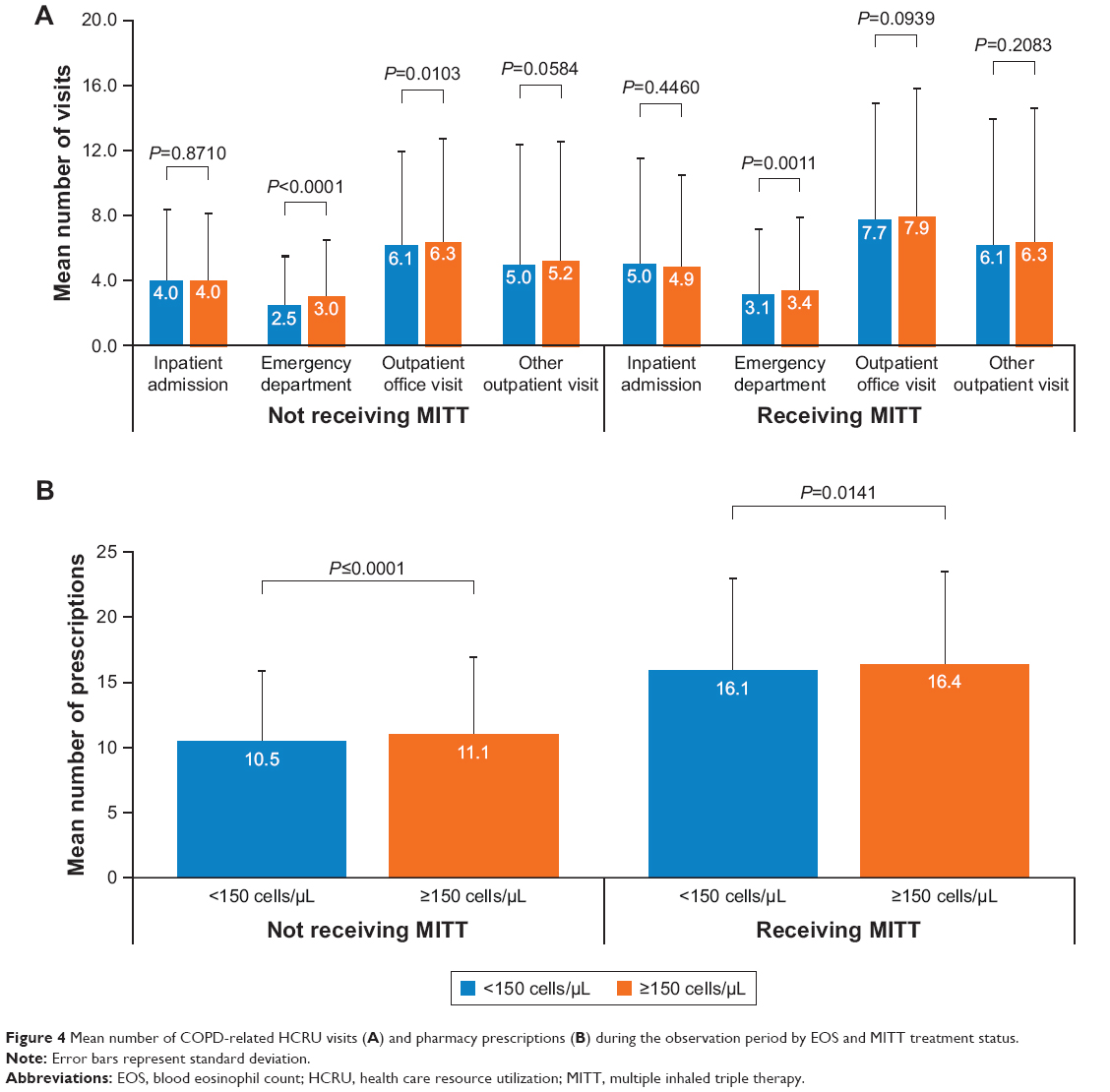 | Figure 4 Mean number of COPD-related HCRU visits (A) and pharmacy prescriptions (B) during the observation period by EOS and MITT treatment status. |
COPD-related pharmacy encounters
For subgroups not receiving MITT, there were lower proportions of COPD-related pharmacy encounters for all drug classes compared with the subgroups receiving MITT (Table S1).
Sensitivity analysis by different EOS categories
Patients receiving MITT were further stratified according to different blood EOS count categories in a sensitivity analysis. An examination of demographic and clinical characteristics of these subgroups showed that, although patients in the <150, ≥150–<300, ≥300–<500, and ≥500 cells/μL subgroups were predominantly female, there was a declining representation of female gender with increasing EOS count (61.1%, 56.9%, 53.9%, and 50.2%, respectively) (Table S2).
The Quan-Charlson Index increased with EOS count, with a mean of 4.83 in the <150 cells/μL subgroup, rising to a mean of 5.67 in the ≥500 cells/μL subgroup (Table S3). The prevalence of acute myocardial infarction, transient ischemic attack, hypertension, diabetes, chronic heart failure, asthma, depression, and stroke increased with increasing EOS count (Table S4).
All pair-wise comparisons between the EOS categories for moderate exacerbations were statistically significant (all P<0.05), but for severe exacerbations only the comparisons between the <150 cells/μL and ≥150-<300 cells/μL categories and between the <150 cells/μL and ≥500 cells/μL categories were statistically significant (P=0.0029 and P=0.0202, respectively) (Figure S2; Table S5).
Regarding COPD-related HCRU, mean numbers of outpatient office visits and other outpatient visits were highest in the EOS ≥500 cells/μL category compared with the other categories (Figures S3A and S4A; Table S5). The same pattern was also observed for all-cause HCRU (Figures S3B and S4B; Table S5).
Discussion
The current understanding of the relationship between COPD phenotypes and clinical characteristics and HCRU is limited by a lack of real-world epidemiological data, with available studies including relatively small population sizes. This study provides detailed data on a large, real-world patient population, including approximately 35,000 patients, stratified by blood EOS thresholds and MITT use. These two criteria were chosen to inform identification of subgroups as they were judged to be indicators of exacerbation frequency or response to treatment. Indeed, the EOS threshold chosen to inform subgroups in the current study was based on the association between EOS ≥150 cells/μL and increased COPD exacerbations; similar measures were also used to identify COPD populations at greater risk of exacerbation in the METREX and METREO studies.9 The subgroup defined by a combination of exacerbation history, EOS ≥150 cells/μL and MITT use (~8% of study population) had the highest disease burden among the subgroups examined. Furthermore, there were indications that increased EOS levels were associated with higher disease burden, as measured by the prevalence of comorbidities, numbers of moderate exacerbations, and HCRU.
It is known that patients with COPD, particularly those with frequent exacerbations, may display signs of systemic inflammation, such as elevated blood EOS counts, circulating inflammatory cytokines, and acute-phase proteins.23 Systemic inflammation may, in turn, contribute to higher levels of comorbid disease and poor clinical outcomes.23 In our observational study, patients with blood EOS counts ≥150 cells/μL and MITT use had high all-cause disease burden as measured by Quan-Charlson Comorbidity Index, and more all-cause HCRU visits and pharmacy prescriptions than the other subgroups assessed. In particular, they had higher proportions of cardiovascular comorbidities; increased risk of cardiovascular diseases is associated with systemic inflammation,23 and some cardiovascular conditions are linked to increased blood EOS counts.24 We speculate that patients with blood EOS counts ≥150 cells/μL and using MITT also have persistent systemic inflammation and other potential clinical complications related to EOS.24
Previous studies have suggested that patients with COPD and blood EOS counts ≥150 cells/μL are likely to have elevated sputum EOS counts and potentially eosinophilic infiltration within the airways.14,18 Sputum EOS have been reported to be a trigger for COPD exacerbations, and a cluster analysis of COPD exacerbations showed that sputum EOS-associated exacerbations were the most predominant after bacteria-associated exacerbations.14 The role of EOS in promoting exacerbations is yet unclear;18 however, the mediators that they can release are associated with increased exacerbations, lung function decline, and signs of airway remodeling.18,25 During degranulation, they release basic proteins (ie, major basic protein, eosinophil cationic protein, eosinophil peroxidase, eosinophil-derived neurotoxin), which are cytotoxic and are capable of disrupting the protective pulmonary epithelial barrier.25 They also secrete pro-inflammatory mediators (eg, interleukins, tumor necrosis factor, and chemokines) that can propagate inflammatory responses.25 Treatments directed towards lowering EOS counts (sputum or blood) have lowered exacerbations in patients with COPD,9,15,25 further suggesting a link between eosinophilic airway inflammation and high burden of disease.
The sensitivity analysis performed in this study further supports the use of blood EOS counts in clinical management of patients with COPD. Moderate exacerbations, comorbidities, and most forms of COPD-related and all-cause HCRU increased with increasing EOS counts. Moreover, HCRU remained higher among patients who were receiving maximal inhaled therapy. These results suggest that, in clinical practice, this association could help identify patients with COPD who are candidates for further anti-inflammatory treatment, including biological agents that target eosinophilic inflammation. By doing so, clinicians may have the possibility to reduce both COPD-related and all-cause disease burden.
Recent evidence suggests that there is a continuous association between increasing EOS and greater risk of exacerbations, but the definition of clinically relevant eosinophilic inflammation in COPD remains unclear.26–28 Previous observational studies have investigated EOS thresholds to identify patients with COPD and a high disease burden, with varying results.26–28 In a recent retrospective study by Zeiger et al27 that accessed administrative pharmacy and HCRU data from 2009 to 2012, it was shown that patients with COPD and EOS ≥300 cells/μL experienced more COPD exacerbations during a 1-year follow-up than patients with <300 cells/μL. Similarly, the study by Vedel-Krogh et al26 found a 3.21-fold increased risk of severe exacerbations within the clinical COPD population with EOS ≥340 cells/μL. In contrast, the multicenter study by Hastie et al28 was unable to find any association between increased COPD exacerbations requiring corticosteroids and disease burden with EOS ≥200 cells/μL, but did find increased airway wall thickness, higher St George’s Respiratory Questionnaire symptom scores, and increased wheezing in these patients compared with those with EOS <200 cells/μL. These observations are similar to those for severe asthma. The threshold of 150 cells/μL has been suggested as a marker of therapeutic response;29 however, the relationship of blood EOS with disease severity varies across publications with various threshold levels used.30,31 These differing results highlight that the EOS thresholds chosen, in addition to inter-study variability in EOS measurement methodology or populations studied, could impact study outcomes. In the current study, patients with EOS ≥150 cells/μL experienced significantly more moderate exacerbations compared with those with <150 cells/μL, regardless of MITT use. Studies have shown that patients who experience moderate exacerbations have significantly higher COPD-related health care costs than those who do not experience exacerbations.32,33
Limitations
This study had several limitations. First, the data used were collected from a US database and, therefore, it may limit extrapolation of these results to other countries across the world. Furthermore, there may be coding inaccuracies within the dataset, which could introduce errors and skew the results. Second, approximately 30% of included patients also had asthma, which may have contributed to the HCRU recorded in the database. Third, the frequency of blood EOS testing is not currently standardized in the US. A fourth limitation is expected poor treatment adherence by patients, which could potentially affect the division of patients amongst the MITT subgroups. A further factor that may have affected allocation of patients to the relevant subgroups is the lowering impact of ICS on blood EOS,16 which may have led to patients with high EOS being included in the <150 cells/μL MITT subgroup rather than the ≥150 cells/μL MITT subgroup. Additionally, differences in adherence to medications could account for some of the differences between the groups in HCRU, as those patients with poor adherence would be less likely to seek out health care resources. Fifth, there is a possible detection bias for moderate exacerbations. Since patients with high EOS counts generally have more comorbidities, they may have been followed more closely with a lower threshold for treatment leading to high HCRU. However, this bias would be unlikely to affect COPD-related hospitalizations and ED visits. Sixth, this study contained only descriptive analyses. Seventh, indications requiring a complete blood count were not controlled for; therefore, an EOS count may have been performed preferentially in patients with indications requiring blood draws, such as those with increased comorbidities and hospitalization. Finally, several studies have discussed persistent, intermittent, and persistently low EOS counts, defining eosinophilic inflammation over time.19,34,35 As identification of eosinophilic inflammation was frequently dependent on a single assessment, patients with intermittent eosinophilic inflammation who did not have eosinophilic inflammation at the time of the assessment may have been incorrectly categorized. The impact of this limitation may have been reduced by only including patients with ≥2 EOS counts available. However, this would have substantially reduced the size of the study population and may also have created a bias towards the inclusion of patients with more severe disease, given that EOS counts are not performed as part of routine clinical practice. Furthermore, evidence indicates that, in those patients with stable COPD with eosinophilic inflammation, EOS levels were unlikely to fluctuate.36 As EOS testing becomes more embedded in clinical practice analyses, the impact of EOS variation over time will be easier to evaluate.
Conclusion
In this large, retrospective real-world study, an association was found between elevated EOS in patients with COPD and increased HCRU, irrespective of intensive inhaled therapy (MITT). Both patients and the health care system are likely to benefit from new treatment options targeted at reducing exacerbations in patients with COPD who have elevated EOS levels and continue to experience exacerbations despite maximal inhaled therapy. Further clinical investigation is required to confirm or refute this hypothesis.
Abbreviations list
ED, emergency department; EOS, blood eosinophil count; GOLD, Global Initiative for Chronic Obstructive Lung Disease; HCRU, health care resource utilization; ICS, inhaled corticosteroid; IDNs, Integrated Delivery Networks; LABA, long-acting β2-agonist; LAMA, long-acting anti-muscarinic antagonist; MITT, multiple inhaled triple therapy; OCS, oral corticosteroid.
Data sharing statement
GlaxoSmithKline (GSK) makes available anonymized individual participant data and associated documents from interventional clinical studies which evaluate medicines, upon approval of proposals submitted to www.clinicalstudydatarequest.com. To access data for other types of GSK sponsored research, for study documents without patient-level data and for clinical studies not listed, please submit an enquiry via the website. The data that support the findings of this study are available from IBM Watson Health, but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available.
Acknowledgments
This work was funded by GSK (HO-17-18395). The authors would like to thank Yunhao Liu, from GSK, for quality control of the data analysis. Editorial support (in the form of writing assistance, assembling tables and figures, collating author comments, grammatical editing, and referencing) was provided by Liz Morgan, PhD, and Roisin McCorkell, MSc, from Fishawack Indicia Ltd, UK, and was funded by GSK. Abstract accepted and presented at the 2018 American Thoracic Society International Conference: 12925 – Identifying populations with severe COPD and eosinophil counts ≥150 cells/μL; B36 Biomarkers in COPD; Thematic Poster Session; Monday May 21, 2018, 9:15 am to 4:15 pm.
Author contributions
HM, EPS, and BH developed the concept of the study, HM, EPS, and GM were involved in data acquisition, and all authors contributed to data analysis and interpretation. All authors drafted the work or revised it critically for important intellectual content, approved the final version for publication, made the decision to submit the manuscript for publication, and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Disclosure
HM, BH, EPS, and GM are all GSK employees and own stock in GSK. All authors report no other conflicts of interest in this work.
References
World Health Organization. The top 10 causes of death. 2017; http://www.who.int/mediacentre/factsheets/fs310/en/. Accessed April 2018. | ||
Seemungal TA, Donaldson GC, Paul EA, Bestall JC, Jeffries DJ, Wedzicha JA. Effect of exacerbation on quality of life in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1998;157(5 Pt 1):1418–1422. doi:10.1164/ajrccm.157.5.9709032 | ||
Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease 2018 report. Global initiative for chronic obstructive lung disease; 2018. | ||
Frith PA, Thompson PJ, Ratnavadivel R, et al. Glycopyrronium once-daily significantly improves lung function and health status when combined with salmeterol/fluticasone in patients with COPD: the GLISTEN study, a randomised controlled trial. Thorax. 2015;70(6):519–527. doi:10.1136/thoraxjnl-2014-206670 | ||
Lipson DA, Barnacle H, Birk R, et al. FULFIL trial: once-daily triple therapy for patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2017;196(4):438–446. doi:10.1164/rccm.201703-0449OC | ||
Siler TM, Kerwin E, Tombs L, Fahy WA, Naya I. Triple therapy of umeclidinium + inhaled corticosteroids/long-acting beta2 agonists for patients with COPD: pooled results of randomized placebo-controlled trials. Pulm Ther. 2016;2:43–58. doi:10.1007/s41030-016-0012-4 | ||
Singh D, Papi A, Corradi M, et al. Single inhaler triple therapy versus inhaled corticosteroid plus long-acting beta2-agonist therapy for chronic obstructive pulmonary disease (TRILOGY): a double-blind, parallel group, randomised controlled trial. Lancet. 2016;388(10048):963–973. doi:10.1016/S0140-6736(16)31354-X | ||
Lipson DA, Barnhart F, Brealey N, et al. Once-daily single-inhaler triple versus dual therapy in patients with COPD. N Engl J Med. 2018;378(18):1671–1680. doi:10.1056/NEJMc1711583 | ||
Pavord ID, Chanez P, Criner GJ, et al. Mepolizumab for eosinophilic chronic obstructive pulmonary disease. N Engl J Med. 2017;377(17):1613–1629. doi:10.1056/NEJMoa1708208 | ||
Agusti A, Bel E, Thomas M, et al. Treatable traits: toward precision medicine of chronic airway diseases. Eur Respir J. 2016;47(2):410–419. doi:10.1183/13993003.01359-2015 | ||
Leigh R, Pizzichini MM, Morris MM, Maltais F, Hargreave FE, Pizzichini E. Stable COPD: predicting benefit from high-dose inhaled corticosteroid treatment. Eur Respir J. 2006;27(5):964–971. doi:10.1183/09031936.06.00072105 | ||
Brightling CE, Monteiro W, Ward R, et al. Sputum eosinophilia and short-term response to prednisolone in chronic obstructive pulmonary disease: a randomised controlled trial. Lancet. 2000;356(9240):1480–1485. doi:10.1016/S0140-6736(00)02872-5 | ||
Singh D, Kolsum U, Brightling CE, et al. Eosinophilic inflammation in COPD: prevalence and clinical characteristics. Eur Respir J. 2014;44(6):1697–1700. doi:10.1183/09031936.00003814 | ||
Bafadhel M, McKenna S, Terry S, et al. Acute exacerbations of chronic obstructive pulmonary disease: identification of biologic clusters and their biomarkers. Am J Respir Crit Care Med. 2011;184(6):662–671. doi:10.1164/rccm.201104-0597OC | ||
Siva R, Green RH, Brightling CE, et al. Eosinophilic airway inflammation and exacerbations of COPD: a randomised controlled trial. Eur Respir J. 2007;29(5):906–913. doi:10.1183/09031936.00146306 | ||
Kreindler JL, Watkins ML, Lettis S, Tal-Singer R, Locantore N. Effect of inhaled corticosteroids on blood eosinophil count in steroid-naive patients with COPD. BMJ Open Respir Res. 2016;3(1):e000151. doi:10.1136/bmjresp-2016-000151 | ||
Pascoe S, Locantore N, Dransfield MT, Barnes NC, Pavord ID. Blood eosinophil counts, exacerbations, and response to the addition of inhaled fluticasone furoate to vilanterol in patients with chronic obstructive pulmonary disease: a secondary analysis of data from two parallel randomised controlled trials. Lancet Respir Med. 2015;3(6):435–442. doi:10.1016/S2213-2600(15)00106-X | ||
Kolsum U, Damera G, Pham T-H, et al. Pulmonary inflammation in patients with chronic obstructive pulmonary disease with higher blood eosinophil counts. J Allergy Clin Immunol. 2017;140(4):1181–1184.e1187. doi:10.1016/j.jaci.2017.04.027 | ||
Kim VL, Coombs NA, Staples KJ, et al. Impact and associations of eosinophilic inflammation in COPD: analysis of the AERIS cohort. Eur Respir J. 2017;50(4):1700853. doi:10.1183/13993003.00711-2017 | ||
Landis S, Suruki R, Maskell J, Bonar K, Hilton E, Compton C. Demographic and clinical characteristics of COPD patients at different blood eosinophil levels in the UK clinical practice research datalink. Copd. 2018;15(2):177–184. doi:10.1080/15412555.2018.1441275 | ||
Wells JM, Washko GR, Han MK, et al. Pulmonary arterial enlargement and acute exacerbations of COPD. N Engl J Med. 2012;367(10):913–921. doi:10.1056/NEJMoa1203830 | ||
Kim JK, Lee SH, Lee BH, et al. Factors associated with exacerbation in mild- to-moderate COPD patients. Int J Chron Obstruct Pulmon Dis. 2016;11:1327–1333. doi:10.2147/COPD.S105583 | ||
Barnes PJ. Inflammatory mechanisms in patients with chronic obstructive pulmonary disease. J Allergy Clin Immunol. 2016;138(1):16–27. doi:10.1016/j.jaci.2016.05.011 | ||
Seguela PE, Iriart X, Acar P, Montaudon M, Roudaut R, Thambo JB. Eosinophilic cardiac disease: molecular, clinical and imaging aspects. Arch Cardiovasc Dis. 2015;108(4):258–268. doi:10.1016/j.acvd.2015.01.006 | ||
George L, Brightling CE. Eosinophilic airway inflammation: role in asthma and chronic obstructive pulmonary disease. Ther Adv Chronic Dis. 2016;7(1):34–51. doi:10.1177/2040622315609251 | ||
Vedel-Krogh S, Nielsen SF, Lange P, Vestbo J, Nordestgaard BG. Blood eosinophils and exacerbations in chronic obstructive pulmonary disease. The Copenhagen general population study. Am J Respir Crit Care Med. 2016;193(9):965–974. doi:10.1164/rccm.201509-1869OC | ||
Zeiger RS, Tran TN, Butler RK, et al. Relationship of blood eosinophil count to exacerbations in chronic obstructive pulmonary disease. J Allergy Clin Immunol Pract. 2018;6(3) e945:944–954. doi:10.1016/j.jaip.2017.10.004 | ||
Hastie AT, Martinez FJ, Curtis JL, et al. Association of sputum and blood eosinophil concentrations with clinical measures of COPD severity: an analysis of the SPIROMICS cohort. Lancet Respir Med. 2017;5(12):956–967. doi:10.1016/S2213-2600(17)30234-5 | ||
Pavord ID, Korn S, Howarth P, et al. Mepolizumab for severe eosinophilic asthma (DREAM): a multicentre, double-blind, placebo-controlled trial. Lancet. 2012;380(9842):651–659. doi:10.1016/S0140-6736(12)60988-X | ||
Bjermer L, Lemiere C, Maspero J, Weiss S, Zangrilli J, Germinaro M. Reslizumab for inadequately controlled asthma with elevated blood eosinophil levels: a randomized phase 3 study. Chest. 2016;150(4):789–798. doi:10.1016/j.chest.2016.03.032 | ||
Coumou H, Westerhof GA, de Nijs SB, Amelink M, Bel EH. Diagnosing persistent blood eosinophilia in asthma with single blood eosinophil or exhaled nitric oxide level. Respir Med. 2018;141:81–86. doi:10.1016/j.rmed.2018.06.025 | ||
Pasquale MK, Sun SX, Song F, Hartnett HJ, Stemkowski SA. Impact of exacerbations on health care cost and resource utilization in chronic obstructive pulmonary disease patients with chronic bronchitis from a predominantly medicare population. Int J Chron Obstruct Pulmon Dis. 2012;7:757–764. doi:10.2147/COPD.S36997 | ||
Punekar YS, Shukla A, Mullerova H. COPD management costs according to the frequency of COPD exacerbations in UK primary care. Int J Chron Obstruct Pulmon Dis. 2014;9:65–73. doi:10.2147/COPD.S60179 | ||
Casanova C, Celli BR, de-Torres JP, et al. Prevalence of persistent blood eosinophilia: relation to outcomes in patients with COPD. Eur Respir J. 2017;50:5. doi:10.1183/13993003.00711-2017 | ||
Oshagbemi OA, Burden AM, Braeken DCW, et al. Stability of blood eosinophils in patients with chronic obstructive pulmonary disease and in control subjects, and the impact of sex, age, smoking, and baseline counts. Am J Respir Crit Care Med. 2017;195(10):1402–1404. doi:10.1164/rccm.201701-0150WS | ||
Landis SH, Suruki R, Hilton E, Compton C, Galwey NW. Stability of blood eosinophil count in patients with COPD in the UK clinical practice research datalink. Copd. 2017;14(4):382–388. doi:10.1080/15412555.2017.1313827 |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.