Back to Journals » Infection and Drug Resistance » Volume 19
Evolution in Epidemiology and Antimicrobial Resistance Patterns of Bacteria Among Dermatology Patients: A Retrospective Study in a Tertiary Dermatology Hospital in China (2018–2023)
Received 9 November 2025
Accepted for publication 25 February 2026
Published 12 March 2026 Volume 2026:19 580159
DOI https://doi.org/10.2147/IDR.S580159
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Hazrat Bilal
Shi Chen,1 Xinzheng Li,2 Jiyun Tian1
1Department of Microbiology Laboratory, Hangzhou Third People’s Hospital, Hangzhou Third Hospital Affiliated to Zhejiang Chinese Medical University, Hangzhou, People’s Republic of China; 2Department of Clinical Laboratory, Hangzhou Third People’s Hospital, Hangzhou Third Hospital Affiliated to Zhejiang Chinese Medical University, Hangzhou, People’s Republic of China
Correspondence: Xinzheng Li, Department of Clinical Laboratory, Hangzhou Third People’s Hospital, Hangzhou Third Hospital Affiliated to Zhejiang Chinese Medical University, No. 38 Xihu Avenue, Hangzhou, 310009, People’s Republic of China, Email [email protected]
Purpose: This study analyzed the epidemiology and antimicrobial resistance of dermatology patients to supplement general surveillance with dermatology-related data, guide the prudent use of antimicrobials, provide a template for antimicrobial stewardship programme and interrupt the spread of drug-resistant bacteria.
Methods: A retrospective study analyzed bacterial isolates from dermatology patients between 2018 and 2023. Statistical analysis was carried out using WHONET 2023, IBM SPSS 26, Excel 2021, and R 4.3.3, using chi-square and Cochran-Armitage tests to identify differences and trends.
Results: The study found the bacterial isolation rate of 32.88% in dermatology patients. Positive cultures were more common in males, aged 60 or older, outpatients, and dermatologic surgery patients. Gram-positive bacteria (GPB) isolation rates increased from 2018 to 2020 and decreased thereafter. Secretion was most common in positive specimen types. Primary infections had higher isolation rates than secondary infections. Eczema, dermatitis, and herpes zoster were the most diagnosed skin conditions. Staphylococcus aureus was the most common pathogen, while coagulase-negative Staphylococcus (CoNS) exhibited higher antimicrobial resistance. Clindamycin resistance in β-hemolytic Streptococcus (BHS) and tetracycline resistance in Enterococcus spp. were the highest among GPB. Except for ampicillin, the resistance rates of Enterobacterales to common antimicrobials were below 30%. Acinetobacter baumannii and Pseudomonas aeruginosa exhibited low antimicrobial resistance to most common antimicrobials. Rates of methicillin-resistant S. aureus and CoNS (MRSA and MRCoNS), and carbapenem-resistant A. baumannii (CRAB) decreased while erythromycin-resistant BHS (ERBHS), linezolid-resistant Enterococcus (LRE), extended-spectrum β-lactamases-producing Enterobacterales (ESBL-E), and carbapenem-resistant P. aeruginosa (CRPA) rates increased, and carbapenem-resistant Enterobacterales (CRE) rates remained stably low.
Conclusion: The findings revealed that the bacterial distribution and antimicrobial resistance patterns among dermatology patients exhibit distinct characteristics. Ongoing surveillance is crucial for tracking these patterns and supporting informed decisions on anti-infective therapies.
Keywords: dermatology, skin and soft tissue infections, bacteria, antimicrobial resistance, multidrug resistant
Introduction
The skin barrier protects the human body from invasion by exogenous and pathogenic microorganisms.1 Due to the damage caused by dermatological conditions to the skin barrier, patients are susceptible to primary or secondary skin and soft tissue infections (SSTIs), which are localized and less systemic. Bacterial infections are common among dermatology patients and can be classified into primary and secondary categories.2 Primary SSTIs typically develop on seemingly healthy and intact skin, such as impetigo, folliculitis, furuncle, etc. Secondary SSTIs, on the other hand, are caused by preexisting skin diseases or damage, such as lesions, burns, eczema, or herpes zoster. Due to these conditions, the skin loses its resistance to pathogenic bacteria. Treatment by antimicrobials is one of the main approaches used by modern medicine to combat infectious diseases, include SSTIs.3,4 At the same time, antimicrobial resistance caused by overuse not only has a negative impact on the general hospital patients but also on dermatology hospital patients. Notably, antimicrobial-resistant bacteria have emerged and spread among dermatology patients, especially those included in World Health Organization (WHO) Bacterial Priority Pathogens List (BPPL) or classified as multidrug-resistant (MDR) bacteria.5,6 Because infections are often significantly harder and more expensive to treat, these drug-resistant bacteria have been a threat to public life and property.7,8 Effectively curbing the emergence and proliferation of drug-resistant bacteria is of paramount importance,9 particularly in dermatology, where the resistance of isolated bacteria tends to be initially low.
Currently, research on bacterial epidemiology and antimicrobial resistance in China predominantly focuses on comprehensive statistics from general hospital patients, such as China Antimicrobial Resistance Surveillance System (CARSS) and China Antimicrobial Surveillance Network (CHINET), or specialized studies related to SSTIs, like the SSTIs Surveillance Network of Staphylococcus aureus in Pediatrics in China.10 However, there is relatively limited research on long-term, comprehensive infections in patients from dermatology specialty hospitals. Infections in dermatology patients are not limited to SSTIs but may also involve concurrent infections in other sites, including bloodstream, lung, and urinary tract, etc. Moreover, the differences in patient complexity, pathogen species, and antimicrobial exposure between dermatology and general hospitals lead to variations in bacterial drug resistance dynamic patterns. Therefore, the aims of the 6-year retrospective study are to provide and analyze the results, changes and trends of the distribution and antimicrobial resistance of bacteria isolated from patients in a tertiary dermatology hospital in Hangzhou, China, from 2018 to 2023. As Zhejiang Dermatosis Clinical Diagnosis and Treatment Technology Guidance Center, Zhejiang Dermatology Research Center of Integrated Traditional Chinese and Western Medicine, the source of visiting patients is not limited to Hangzhou, thus possessing a certain regional representativeness. We expect this study to contribute more comprehensive information for the overall surveillance of China in terms of infections among dermatology patients, offering reference for comprehensive anti-infective therapy, appropriate use of antimicrobial agents, delaying the rise of bacterial resistance, and mitigating the emergence and spread of drug-resistant bacteria.11,12
Materials and Methods
Data Enrollment
We conducted a retrospective study involving patients’ information, bacteriological test results from a tertiary dermatology hospital in Hangzhou, Zhejiang Province, China, spanning from January 1, 2018 to December 31, 2023. Only the first isolate per patient per episode was included in the analysis to eliminate bias caused by duplicate isolates. Mycological and virological findings were excluded from this study. The resistance rates to antimicrobials were collected in the data. All the data were acquired from the hospital Laboratory Information System (LIS).
Strain Identification and Antimicrobial Susceptibility Testing
Samples were collected and examined according to the routine laboratory protocols, including secretion, throat swab, puncture fluid, abscess, urine, skin, swab, sputum, blood, and pus, among others. All the samples were inoculated on Sheep Blood Agar (Autobio, China), Chocolate Agar (Autobio, China) or China Blue Agar (Biocell, China) and incubated at 35°C, 5% CO2, for 24–48 h. The isolated bacteria strains were identified by Matrix-assisted Laser Desorption/Ionization Time-of-flight Mass Spectrometry system (MALDI-TOF MS, Bruker Daltonik MALDI Biotyper, BD Company, USA). The antimicrobial susceptibility testing (AST) of isolates was performed using an automatic instrument with AST cards (Vitek 2 Compact system, bioMérieux Company, France). These AST cards utilize unique fixed panels of antimicrobial agents specifically designed for Staphylococcus and Enterococcus (GP67, P639), Enterobacterales (GN16, N334), and non-fermenting Gram-negative bacteria (N335). In addition, disk-diffusion (Oxoid, UK) or E-test (Bio-kont, China) method on Mueller Hinton Agar (MHA, Autobio, China) for supplemental test, MHA with blood (Bio-kont, China) for Streptococcus, or Haemophilus test medium (HTM, Bio-kont, China) for Haemophilus influenzae. The AST procedures were conducted in accordance with both the contemporary manufacturer’s instructions and the Clinical and Laboratory Standards Institute (CLSI) guidelines effective during the respective year of testing. The defined results were interpreted as susceptible (S), intermediate (I), and resistant (R) according to the minimal inhibitory concentration (MIC) and zone diameter interpretive breakpoints recommended by CLSI. The internal quality control strains include Staphylococcus aureus ATCC 25923 and 29213, Escherichia coli ATCC 25922, Pseudomonas aeruginosa ATCC 27853. Internal quality controls (IQCs) of culture media, antimicrobial disks, and pathogen identification on the MALDI Biotyper were conducted once a week. Moreover, IQCs of AST for the Vitek 2 Compact system and E-test were conducted once a month or before using the new batch. Furthermore, the laboratory participated in the external quality assessment for bacterial identification and AST of the National Center for Clinical Laboratories, China.
Methicillin-resistant S. aureus (MRSA) and coagulase-negative Staphylococcus (MRCoNS), erythromycin-resistant β-hemolytic Streptococcus (ERBHS), high-level aminoglycoside-resistant Enterococcus (HLAR), linezolid-resistant Enterococcus (LRE), extended-spectrum β-lactamases-producing Enterobacterales (ESBL-E), carbapenem-resistant Enterobacterales (CRE), carbapenem-resistant Acinetobacter baumannii (CRAB), and carbapenem-resistant P. aeruginosa (CRPA) were defined based on their resistance to antimicrobial agents.5,6,13 ESBL test necessitates using both cefotaxime and ceftazidime, alone and in combination with clavulanate, and a ≥ 5-mm increase in a zone diameter or a ≥ 3 2-fold concentration decrease in an MIC for either antimicrobial agent tested in combination with clavulanate vs result of the agent when tested alone = ESBL. CRE are Enterobacterales resistant to imipenem or ertapenem. CRAB and CRPA refer to A. baumannii and P. aeruginosa that are resistant to imipenem or meropenem.
Statistical Analysis
Since this study was conducted using a population-based surveillance design, formal power calculations were not required. Statistical analysis was performed using WHONET 2023, IBM SPSS Statistics 26, Microsoft Excel 2021 and R software 4.3.3. WHONET 2023 facilitated the centralization and analysis of patients and isolates data, including strains identification and resistance data obtained from LIS, and generated annual databases. A comprehensive database was developed using Microsoft Excel 2021, encompassing patient details such as ID, gender, age, patient category, department, and diagnosis. Additionally, the database included specimen type, strains identification information and antimicrobial resistance data for the corresponding isolates obtained from WHONET 2023. Data from our study were analyzed with IBM SPSS Statistics 26, Microsoft Excel 2021 and R software 4.3.3. The chi-square (χ2) test was performed to compare the differences in proportion of positive cultures among the gender, age groups, patient categories, departments, and diagnosis types. Further, the Cochran - Armitage test for linear trends was performed to evaluate the significance of the annual trends in the proportion of different gram-stained bacteria and the changes of resistance to antimicrobials. Z>0 indicated an upward trend, and Z<0 indicated a downward trend. Significance was set at P<0.05.
Results
Clinical Features of Patients
From 2018 to 2023, a total of 17678 dermatology patients were enrolled. The overall bacterial isolation rate was 32.88%. The isolation rate in men (39.16%) was significantly higher than that in women (26.47%), with P<0.001, and the male-to-female ratio was 1.51:1 (3497/2316). The overall isolation rate in the age group of ≥60 years (38.82%) was significantly higher than that in the age group of ≤17 (35.33%, P<0.05) and 18–59 (28.55%, P<0.001) years. The isolation rates of outpatients (48.07%) and surgical departments (51.94%) were significantly higher than that of inpatients (31.71%) and medical departments (31.58%), respectively (P<0.001) (Table 1).
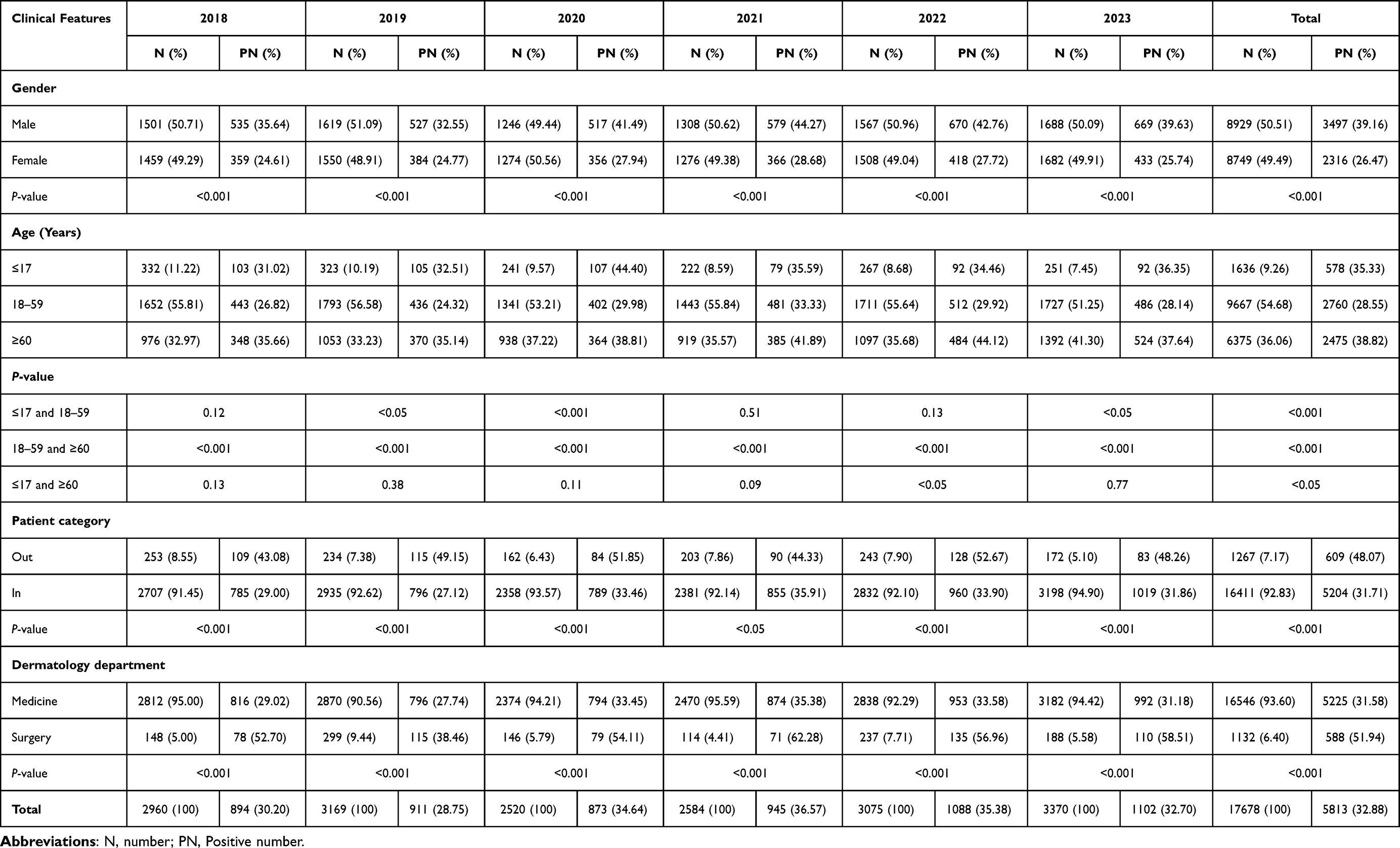 |
Table 1 Clinical Features of Dermatology Patients |
Distribution of Bacteria
Of 6212 bacterial isolates obtained, 11 dominant bacterial isolates were recorded (the number of isolates >100), including S. aureus (46.97%), Staphylococcus epidermidis (7.44%), Klebsiella pneumoniae (6.83%), Staphylococcus haemolyticus (6.62%), E. coli (3.53%), P. aeruginosa (3.22%), Staphylococcus capitis (2.24%), Streptococcus agalactiae (2.24%), Streptococcus dysgalactiae (2.21%), Streptococcus pyogenes (1.90%), and Enterococcus faecalis (1.87%) (Figure 1A).
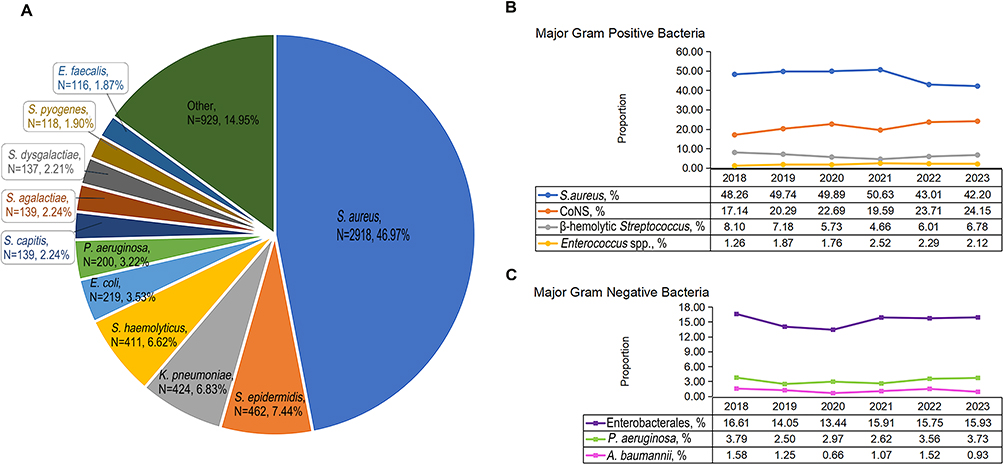 |
Figure 1 Datasets for bacteria in dermatology patients from 2018 to 2023. (A) Distribution of isolated bacterial strains, (B) Trends of major gram-positive bacteria, (C) Trends of major gram-negative bacteria. |
In positive cultures, Gram-positive bacteria (GPB) and Gram-negative bacteria (GNB) accounted for 78.93% and 21.07% of the bacterial isolates, respectively. Although no significant trend was observed in the 6-year isolation rate of GPB overall (P=0.38), annual data revealed completely divergent trends before and after 2020. From 2018 to 2020, the isolation rate of GPB showed an upward trend (76.55%-82.05%, Z=2.97, P<0.01). However, from 2020 to 2023, this isolation rate exhibited a downward trend (82.05%-78.93%, Z=−2.60, P<0.01) (Table 2).
 |
Table 2 Isolation of Gram-Positive Bacteria and Gram-Negative Bacteria |
Among the major GPB, the isolation rate of S. aureus exhibited a downward trend from 48.26% to 42.20% (Z=−4.07, P<0.001), while that of coagulase-negative Staphylococcus (CoNS) showed an upward trend from 17.14% to 24.15% (Z=4.02, P<0.001) (Figure 1B). Meanwhile, the isolation rate fluctuations of major GNB, including Enterobacterales, P. aeruginosa, and A. baumannii were all less than 1%, with all P-values >0.05 (Figure 1C).
Distribution of Bacterial Isolates from Different Clinical Specimens
The major 10 types of specimens accounted for 99.45% of all 6345 bacterial culture-positive clinical specimens. Secretion was consistently the top specimen type in six years. S. aureus had the highest isolation rates in secretion, throat swab, puncture fluid, skin abscess, skin, blood, and pus samples, ranging from 35.86% (blood) to 62.39% (skin), with a rate of 21.43% in sputum, second to K. pneumoniae (28.02%). E. coli (46.56%) and S. haemolyticus (26.18%) exhibited the highest isolation rates in urine and swab, respectively (Table 3).
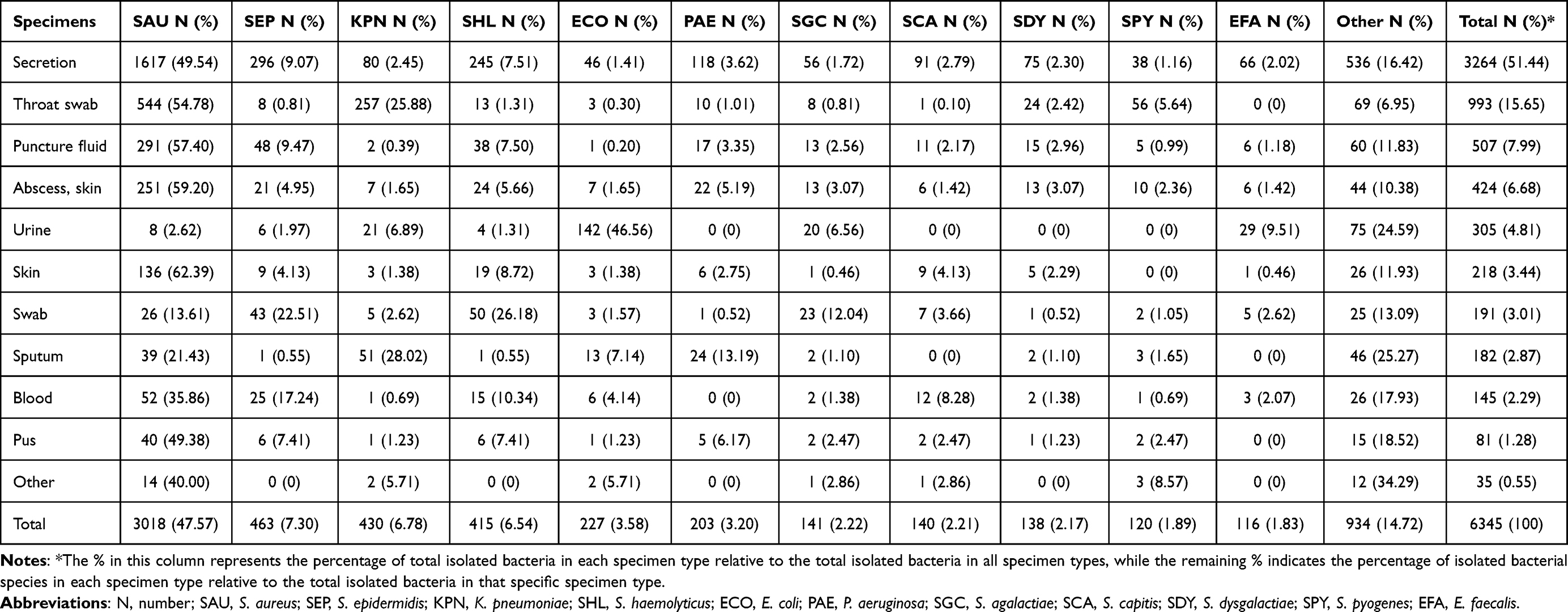 |
Table 3 Isolation of Major Bacteria from Different Specimens |
Distribution of Diseases and Associated Bacteria
In this study, a total of 18220 cases were diagnosed across all submitted specimens, encompassing primary SSTIs, secondary SSTIs, and infections at other sites. The isolation rate of primary SSTIs was 44.09%, which was significantly higher than that of secondary SSTIs at 31.91% (P<0.001) (Table 4).
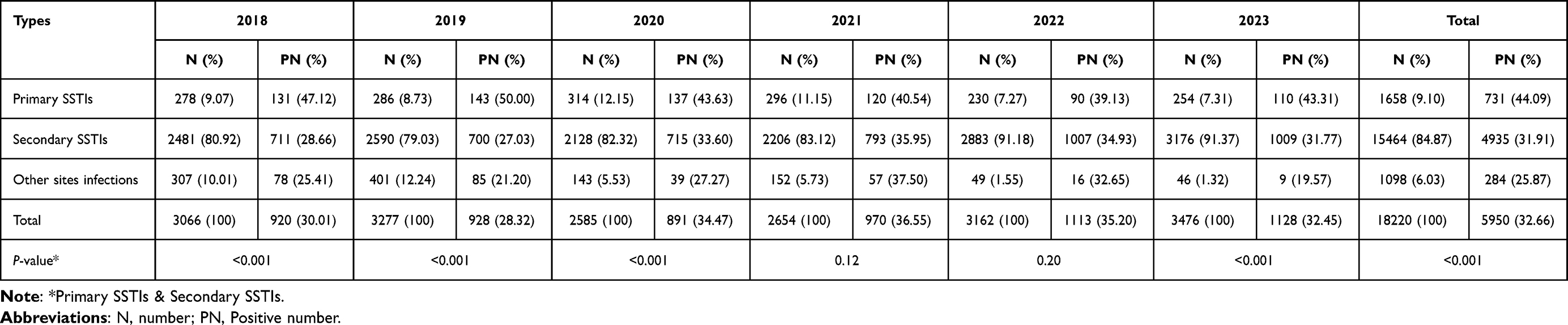 |
Table 4 Isolation Rates of the Different Diagnosis Types in Dermatology Patients |
The top fifteen diagnoses (the number of cases ≥100) accounted for 80.22% of all cases included. S. aureus was consistently the most prevalent pathogen isolated from each of these fifteen diagnoses, with the isolation rates ranging from 24.03% (ulcer) to 68.00% (erythroderma). The isolation rates of S. epidermidis and K. pneumoniae ranged from 0.95% (vasculitis) to 18.54% (herpes zoster) and 1.56% (SSTIs, other) to 22.86% (urticaria), respectively (Table 5).
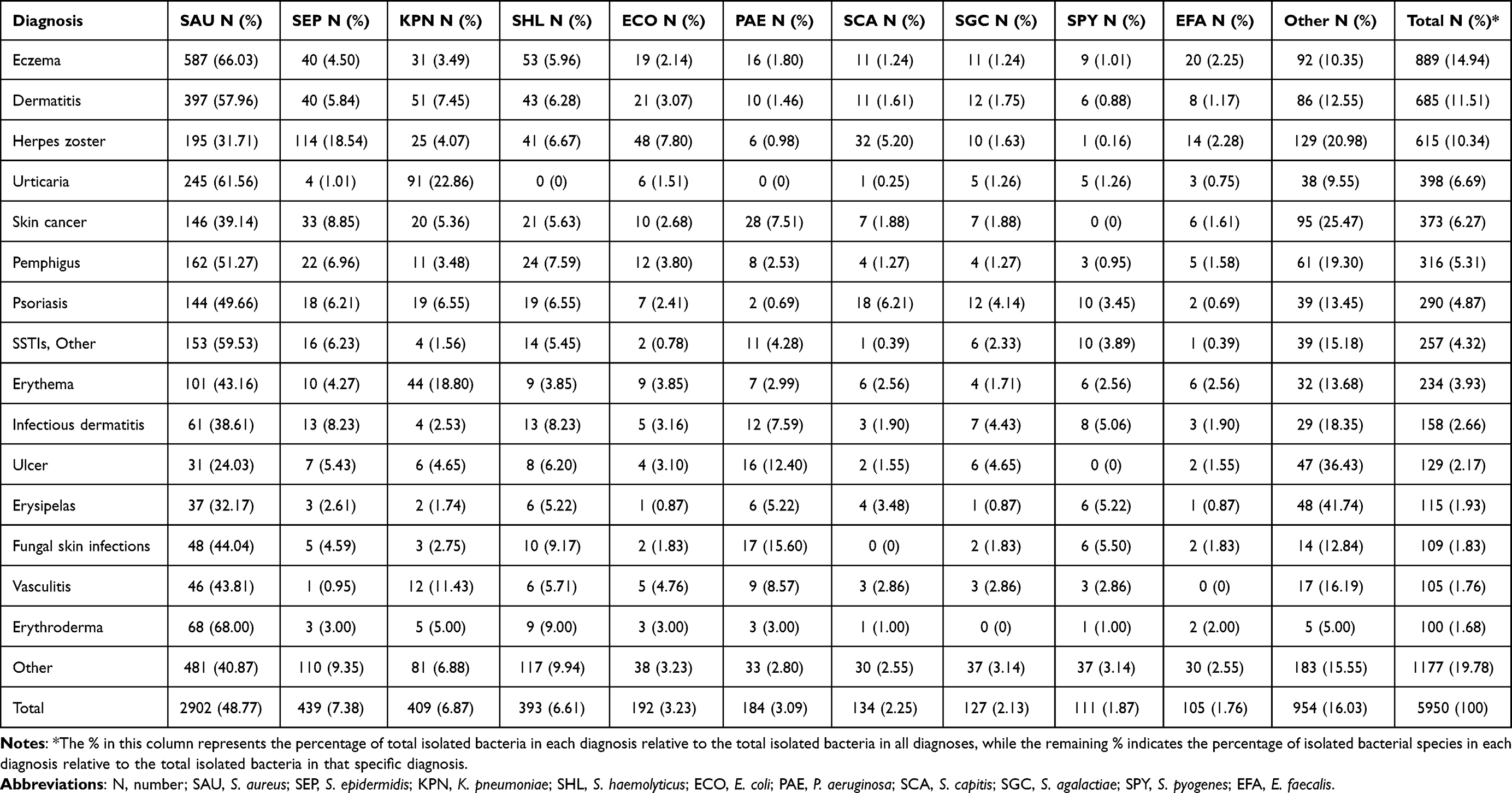 |
Table 5 Isolation of Major Bacteria from Different Diagnoses |
Antimicrobial Resistance Analysis
S. aureus isolated from dermatology patients exhibited the highest resistance rate to penicillin (87.73%). The resistance rates to erythromycin, clindamycin, trimethoprim/sulfamethoxazole and gentamicin exhibited downward trends from 54.90% to 43.78% (Z=−3.43, P<0.001), 52.07% to 40.96% (Z=−3.03, P<0.01), 18.30% to 7.43% (Z=−4.91, P<0.001), and 11.55% to 5.22% (Z=−3.17, P<0.01), respectively. CoNS exhibited higher resistance rates to most antimicrobials compared to S. aureus. Erythromycin resistance of CoNS was the highest among GPB. No resistant strains of S. aureus and CoNS to ceftaroline (S. aureus only), daptomycin, vancomycin, teicoplanin, nitrofurantoin (CoNS only), linezolid, and tigecycline were isolated (Tables 6 and 7).
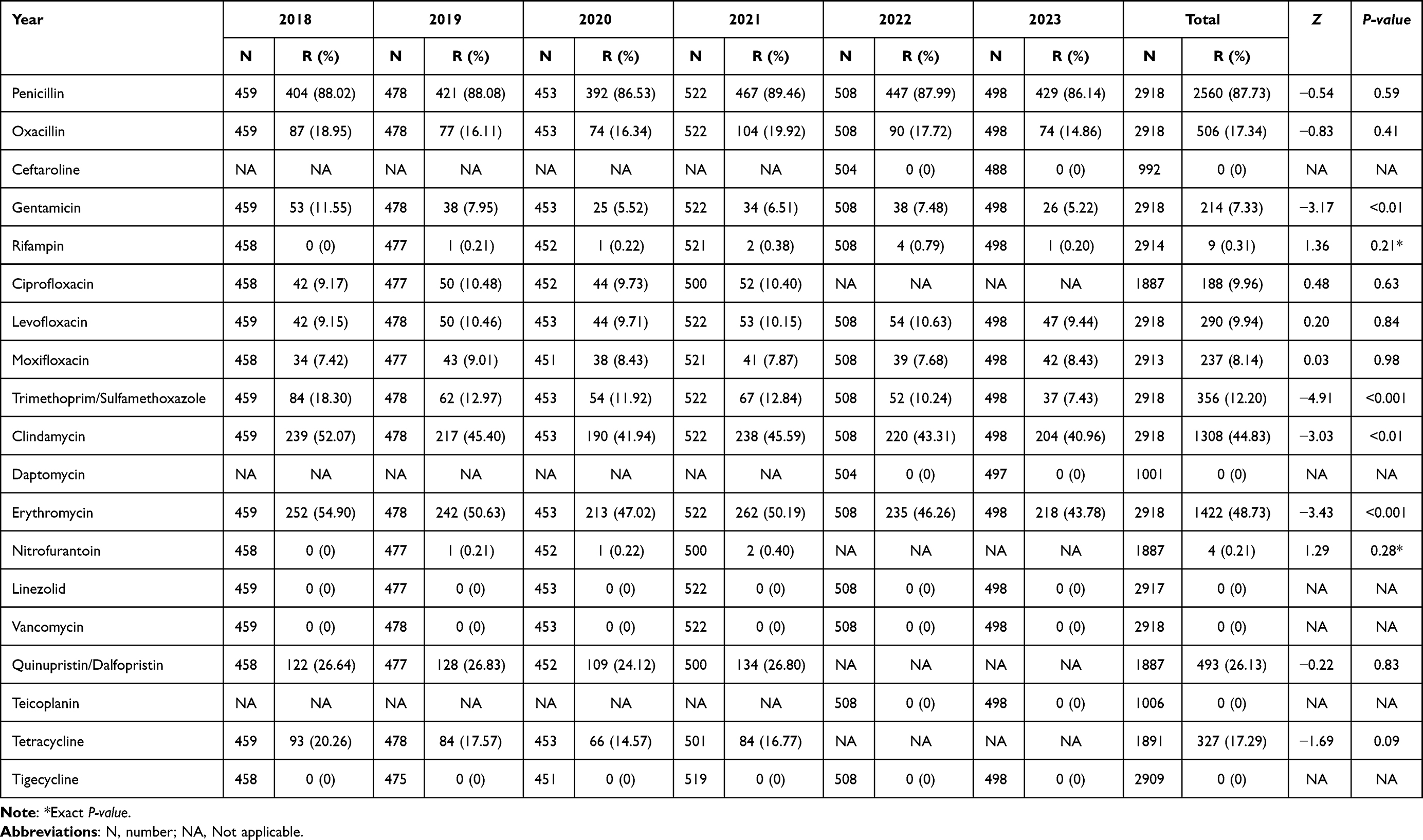 |
Table 6 Antimicrobial Resistance of Staphylococcus aureus |
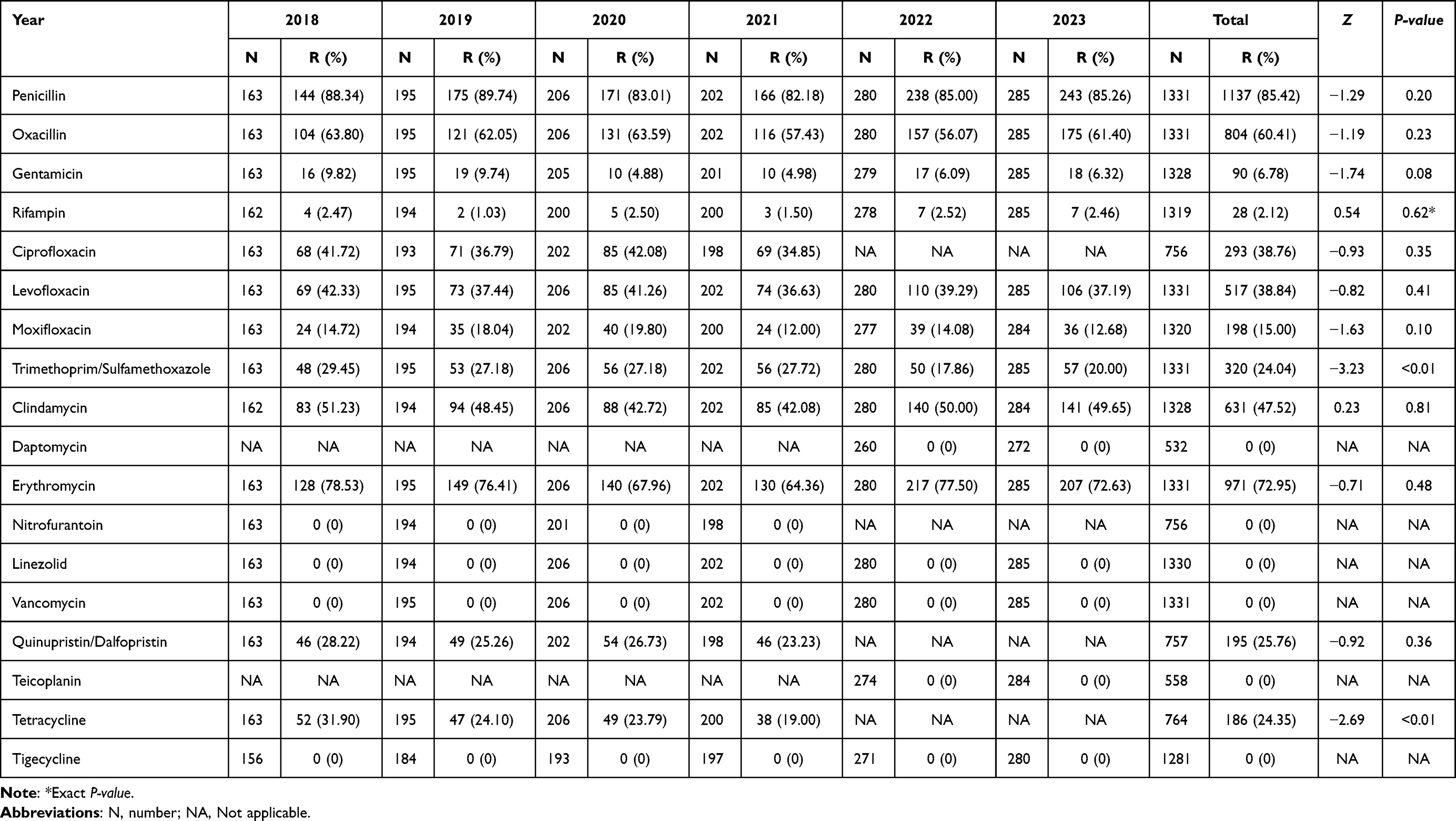 |
Table 7 Antimicrobial Resistance of Coagulase-Negative Staphylococcus |
BHS isolated from dermatology patients exhibited high resistance rates to erythromycin (71.98%), clindamycin (69.54%), and tetracycline (69.37%), respectively, with clindamycin resistance being the highest among GPB. No resistant strains of BHS to penicillin, cefotaxime, ceftriaxone, and vancomycin were isolated. (Table 8).
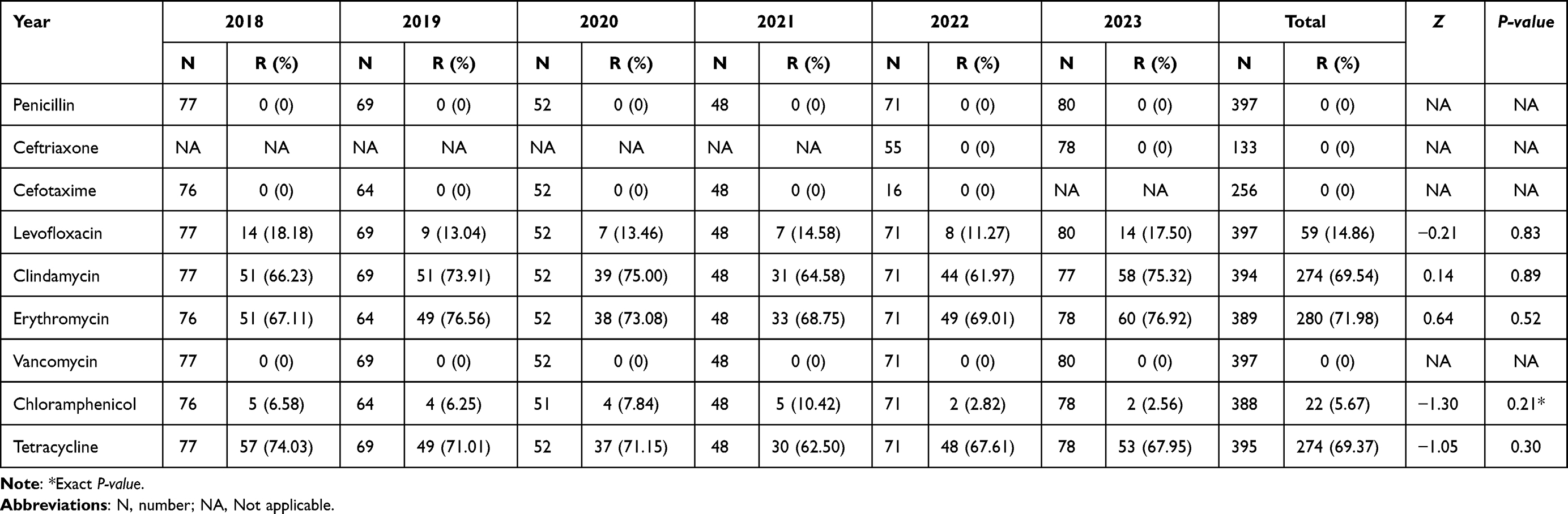 |
Table 8 Antimicrobial Resistance of β-Hemolytic Streptococcus |
Enterococcus spp. isolated from dermatology patients, including E. faecalis (116 strains), E. faecium (7 strains), and E. avium (1 strains), exhibited high resistance rates to tetracycline (80.28%) and erythromycin (65.32%), respectively, with tetracycline resistance being the highest among GPB. Notably, linezolid resistance rate of Enterococcus spp. reached 12.40%. In comparison, Enterococcus spp. showed lower resistance to penicillin (8.06%), ampicillin (7.26%), and nitrofurantoin (4.29%). No resistant strains isolated for daptomycin, vancomycin, teicoplanin, and tigecycline. (Table 9).
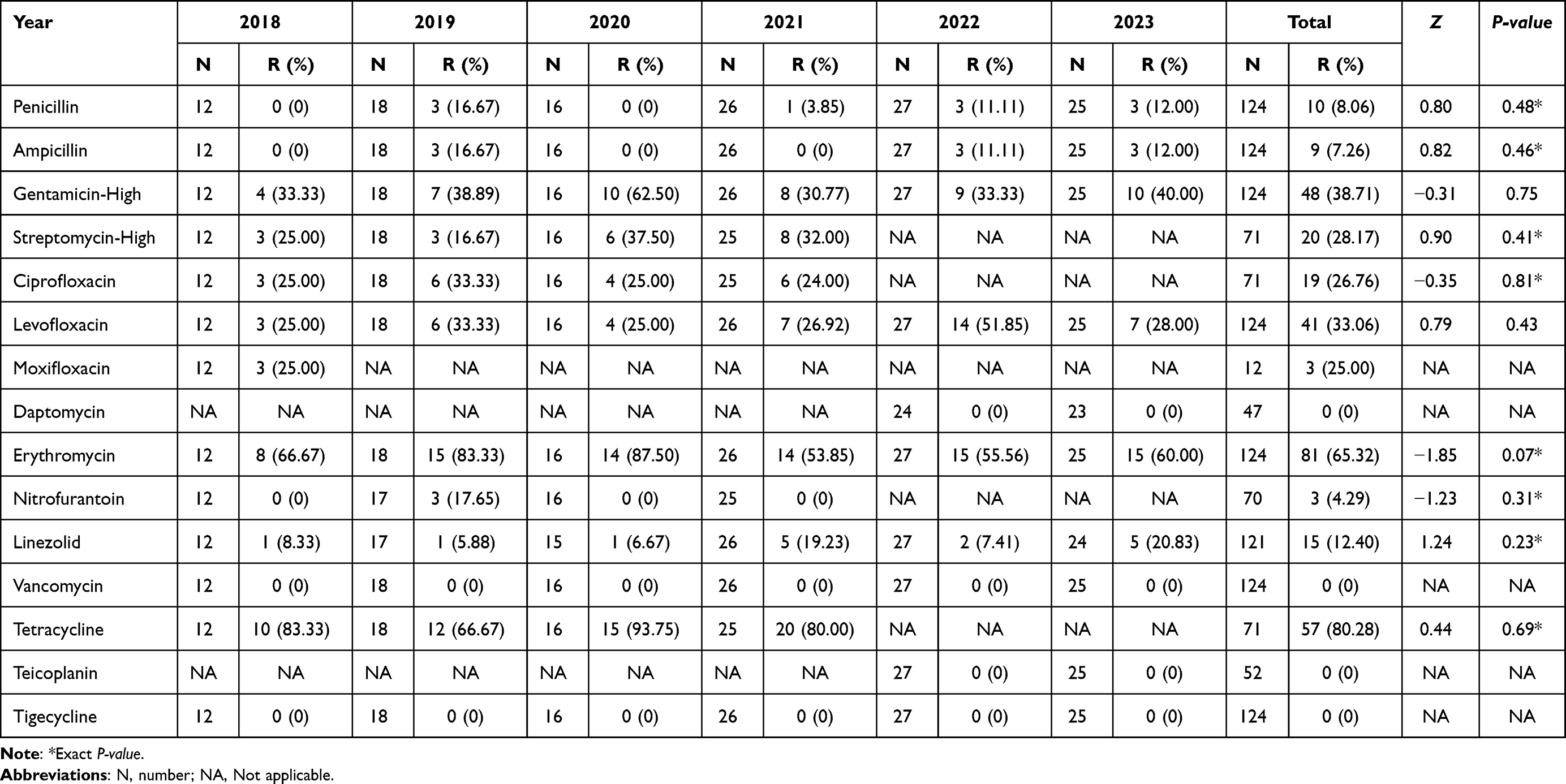 |
Table 9 Antimicrobial Resistance of Enterococcus spp. |
Enterobacterales isolated from dermatology patients exhibited the highest resistance rates to ampicillin (73.26%). The resistance rate to ceftriaxone (18.12%) was higher than that to ceftazidime (6.42%, P<0.001). Notably, resistance rates to cefepime demonstrated an upward trend (Z=3.34, P<0.001). Enterobacterales showed low resistance to β-lactam combination agents and carbapenems, including amoxicillin/clavulanic acid (8.96%), cefoperazone/sulbactam (1.35%), piperacillin/tazobactam (3.17%), ertapenem (1.16%) and imipenem (1.65%). The resistance rate to cefoxitin (7.33%) exhibited a downward trend from 14.84% to 3.36% (Z=−3.00, P<0.01). For aminoglycosides, gentamicin (15.26%) and tobramycin (15.22%) had higher resistance rates than amikacin (2.21%, both P<0.001). Among quinolones, the overall resistance rate to ciprofloxacin (27.57%) was higher than that to levofloxacin (20.04%, P<0.001). No strains resistant to tigecycline were isolated (Table 10).
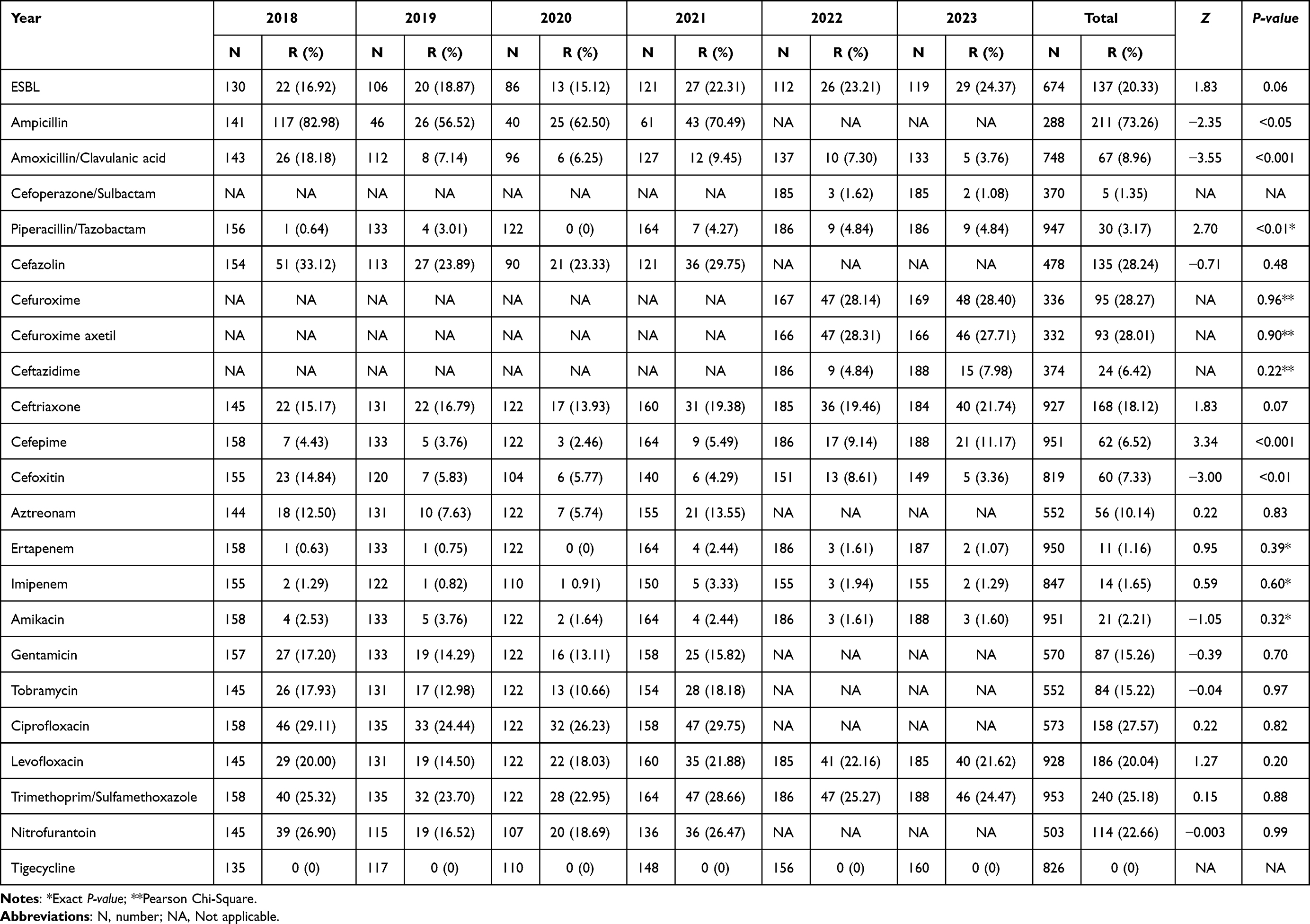 |
Table 10 Antimicrobial Resistance of Enterobacterales |
The overall resistance rates of A. baumannii isolated from dermatology patients to antimicrobials were all below 13%. The overall resistance rates to imipenem and meropenem were 6.85% and 3.57% respectively. No resistant strains to cefoperazone/sulbactam, amikacin, colistin, and tetracyclines were isolated (Table 11).
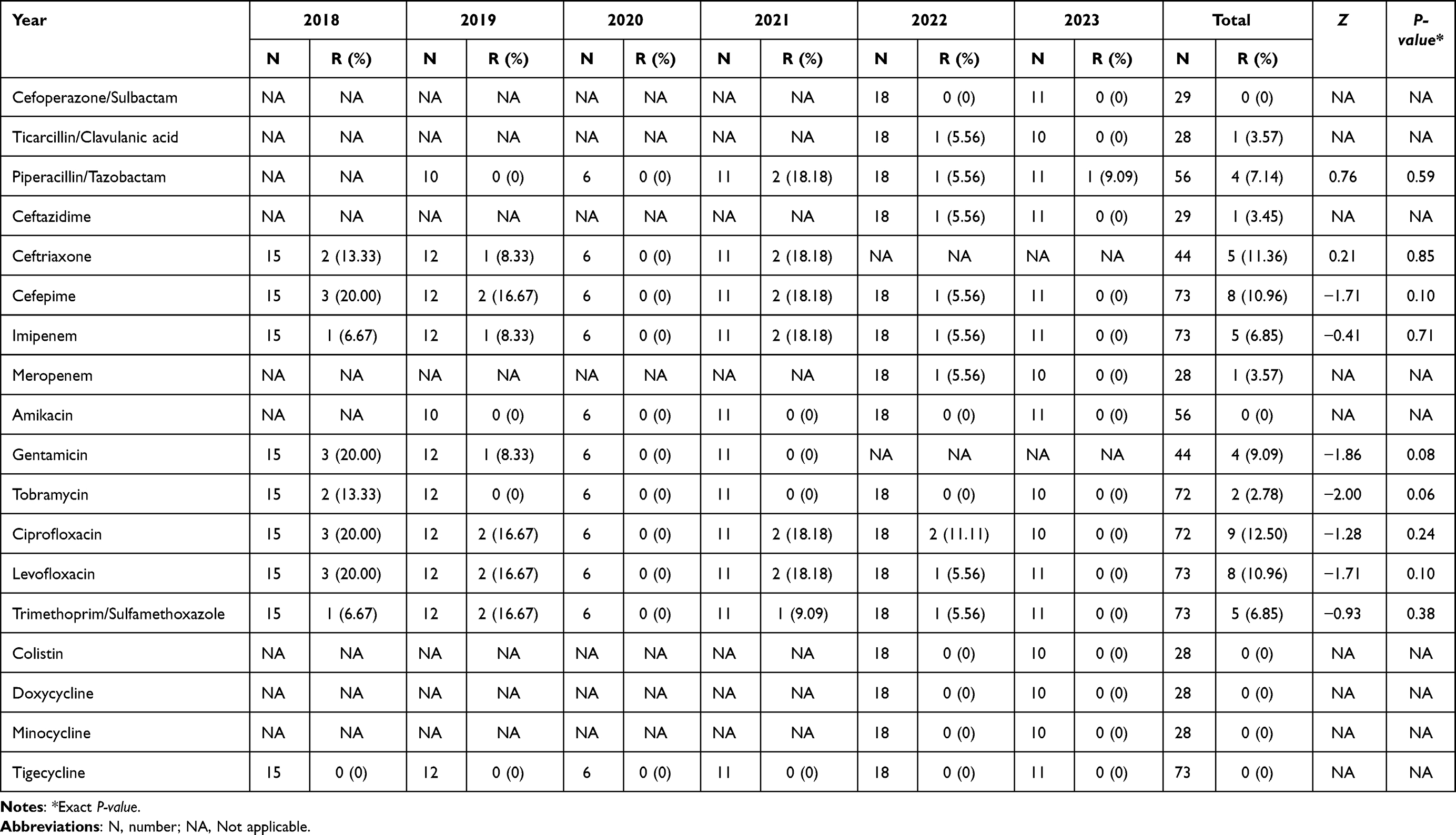 |
Table 11 Antimicrobial Resistance of Acinetobacter baumannii |
P. aeruginosa isolated from dermatology patients exhibited low antimicrobial resistance, with overall resistance rates to tested antimicrobials being ≤10%, except for ticarcillin/clavulanic acid (19.75%). No resistant strains were isolated for colistin, gentamicin and tobramycin (Table 12).
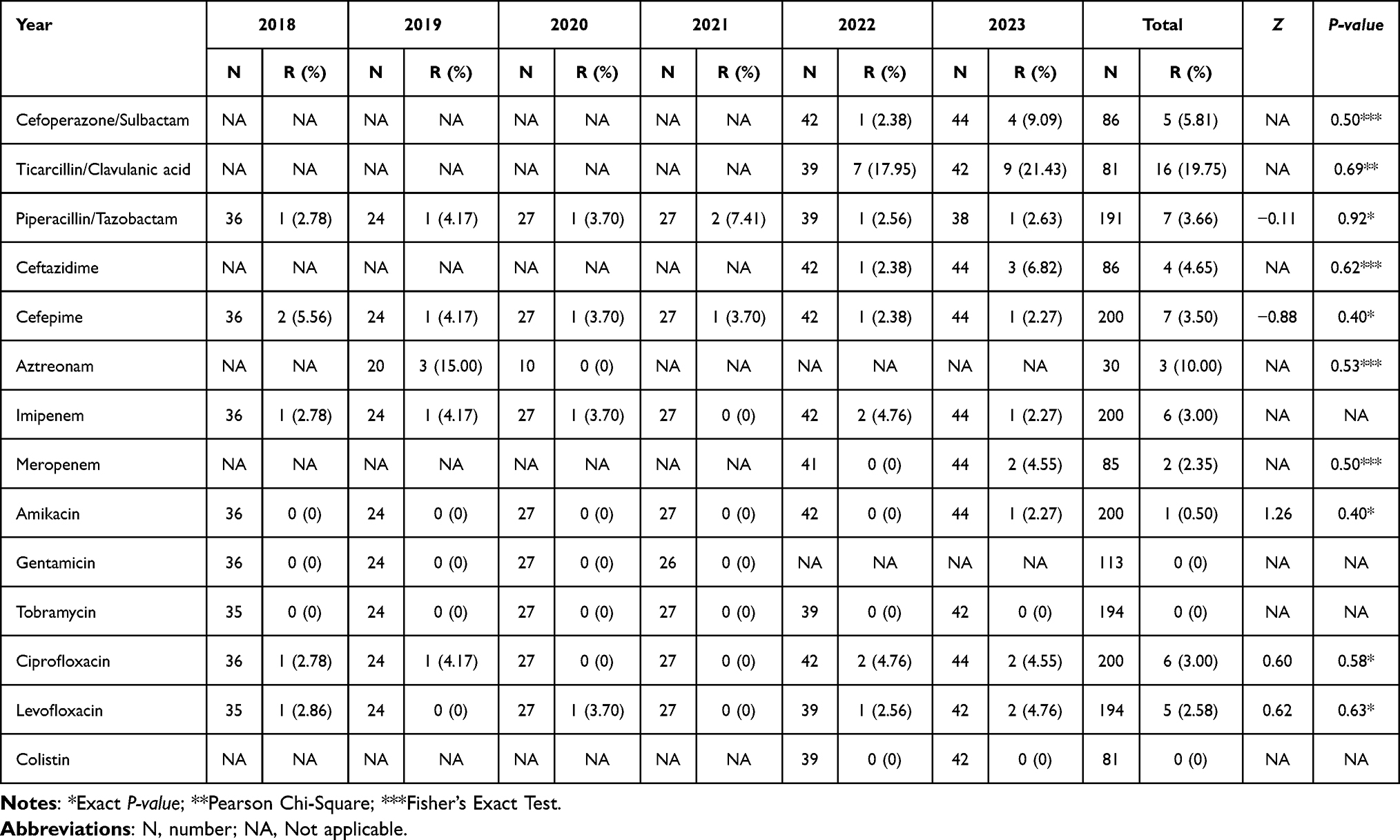 |
Table 12 Antimicrobial Resistance of Pseudomonas aeruginosa |
Distribution of Major Drug-Resistant Bacteria
MRSA, MRCoNS and CRAB decreased over the study period. MRSA decreased from 18.95% to 14.86%, with a peak of 19.92% in 2021 (Figure 2A). MRCoNS decreased from 63.80% to 61.40%, with a trough of 56.07% in 2022 (Figure 2B). CRAB fluctuated greatly, from 6.67% to 0%, reaching a peak of 18.18% in 2021, and the lowest rates of 0% in both 2020 and 2023 (Figure 2C).
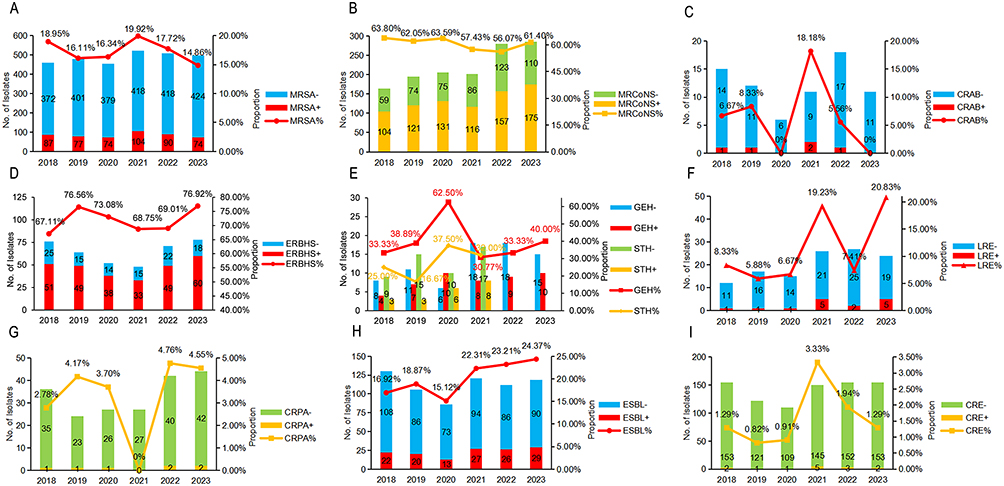 |
Figure 2 Incidences of major drug-resistant bacteria in dermatology patients from 2018 to 2023. (A) Methicillin-resistant S. aureus, 4.09% decrease, (B) Methicillin-resistant coagulase-negative Staphylococcus, 2.40% decrease, (C) Carbapenem-resistant A. baumannii, 6.67% decrease, (D) Erythromycin-resistant β-hemolytic Streptococcus, 9.81% increase, (E) High-level aminoglycoside-resistant Enterococcus, GEH-resistance 6.67% increase and STH-resistance 7.00% increase, (F) Linezolid-resistant Enterococcus, 12.50% increase, (G) Carbapenem-resistant P. aeruginosa, 1.77% increase, (H) Extended-spectrum β-lactamases-producing Enterobacterales, 7.45% increase, (I) Carbapenem-resistant Enterobacterales, 0% change. |
In contrast, ERBHS, HLAR, LRE, ESBL-E, and CRPA, increased with some fluctuations. ERBHS increased from 67.11% to 76.92% (Figure 2D). HLAR, including high-level gentamicin (GEH)-resistant and high-level streptomycin (STH)-resistant strains, increased 6.67% and 7.00%, respectively (Figure 2E). Notably, LRE rose from 8.33% to 20.83%, resulting in an overall increase of 12.50% (Figure 2F). CRPA increased from 2.78% to 4.55%, with the lowest rate of 0% occurred in 2021, but quickly rebounded to the highest rate of 4.76% in 2022 (Figure 2G). ESBL-E, except for the lowest at 15.12% in 2020, increased from 16.92% to 24.37% (Figure 2H). Except for a peak of 3.33% in 2021, the incidence of CRE remained at below 2% (Figure 2I).
Discussion
Empirical antimicrobial therapy serves as the cornerstone of dermatological management for suspected infections.14 The core challenge lies in the pathogen’s unknown status at treatment initiation, necessitating physicians to select antimicrobial regimens based on “best speculation”. Without accurate and timely epidemiological data, such speculation may readily result in inadequate initial treatment coverage or induce drug resistance. The systematic isolation and antimicrobial resistance surveillance data of pathogenic bacteria in this study provide critical localized and real-time evidence-based support for addressing this challenge.
This study describes the distribution and antimicrobial resistance of bacteria isolated from patients in a dermatology hospital, Hangzhou, China. We found that slightly more than one-third of the study population experienced bacterial isolation, suggesting the infection risk faced by dermatology patients. Similar to previous research findings,8,15,16 males (39.16%), patients aged 60 and above (38.82%), outpatients (48.07%), and dermatosurgical patients (51.94%) had relatively higher isolation rates. Interestingly, the isolation rate of minors (≤17 years) decreased from 2020 to 2022, whereas an opposite pattern was observed in the elderly (≥60 years). This may be associated with the asymmetrical shifts in SSTIs exposure risks, which were influenced by behavioral changes among minors and the elderly due to public health policies during the three-year COVID-19 pandemic.17 This could account for the observation that, despite no significant difference in the annual comparison of isolation rates between minors and the elderly in most years, a notable disparity emerges when analyzing the comprehensive data spanning six years. This issue warrants further investigation in future longitudinal studies to ascertain whether the difference will persist.
Our findings indicate that the isolation rate of primary SSTIs (44.09%) was higher than that of secondary SSTIs (31.91%) and other site infections (25.87%). However, the pathogens were predominantly isolated from patients with secondary SSTIs (84.87%), such as eczema (14.94%), dermatitis (11.51%), and herpes zoster (10.34%). Compared with other studies,8,18 these findings remind us that the prevalence of skin diseases has certain regional characteristics, and in addition to treating primary skin diseases, measures to prevent secondary SSTIs and infections at other sites are also necessary.19 Secretions accounted for 51.44% of bacterial isolates in clinical specimens, whereas previous studies have reported that abscesses were more prevalent.16,20,21 This may be related to the characteristics of the infections and the sampling methods. GPB (78.93%) remained the most prevalent isolate, similarly to previous research.12 Within this group, S. aureus (46.97%) was the predominant pathogen, leading in various dermatological conditions and most specimen types, which is consistent with its known threat,22,23 indicating risks of its activation of colonizing strains due to the low immune status of certain skin diseases or transmission through the bloodstream. CoNS (16.30%) exhibited high isolation rates in swabs and herpes zoster cases, which may be attributed to their prevalence on human skin, frequently becoming pathogens when skin integrity is compromised, typically affecting the elderly or immunocompromised individuals.2,21 Compared to GPB, GNB are more common in hospital-related SSTIs.7,24,25 Similar to previous literature,26,27 the isolation rates of K. pneumoniae (6.83%), E. coli (3.53%), and P. aeruginosa (3.22%) ranked the top three among GNB. In sputum and urine samples, K. pneumoniae (28.02%) and E. coli (46.56%) were the predominant species respectively, showing no difference from the general population.28,29 K. pneumoniae was also the second most common pathogen in urticaria (22.86%), erythema (18.80%), and vasculitis (11.43%). Due to the high risk of antimicrobial resistance and high virulence associated with K. pneumoniae, this situation warrants serious attention.30 In cases of fungal skin infections, P. aeruginosa (15.60%) ranked second, which may be related to the immunocompromised state of these patients, as well as the intrinsic resistance and biofilm properties of the strains.31 Overall, the prevalence of the top ten bacterial species showed changes compared to historical data from different regions, with CoNS and K. pneumoniae increasing while Enterococcus spp. and P. aeruginosa decreased,27,32 indicating a shift in the infection patterns among dermatology patients. Notably, species with lower prevalence accounted for 14.95% of total infections, indicating the diversity of pathogens in dermatology patients, and advances in detection technology may reveal more previously rare cases.
We found that the resistance to penicillin of Staphylococcus strains remained persistently high, similar to previous research.33,34 However, the resistance rates to gentamicin, erythromycin, clindamycin, and trimethoprim/sulfamethoxazole — commonly recommended for treating staphylococcal SSTIs or incisional surgical site infections (ISSIs) — were on downward trends,35,36 consistent with the observed reduction in methicillin-resistant strains over the study period. Except for penicillin, quinupristin/dalfopristin and gentamicin, CoNS had higher resistance rates to most antimicrobials than S. aureus, especially with erythromycin resistance being the highest among GPB. These are mainly due to the higher isolation rate of MRCoNS (60.41%) compared to MRSA (17.34%). Although as reported in the literature,37 the majority of reported cases were attributed to methicillin-sensitive strains, the high and stable isolation rate of MRCoNS still warrants attention and monitoring of its progression.
Penicillin, third-generation cephalosporins, vancomycin, chloramphenicol, and levofloxacin, as recommended by the Infectious Diseases Society of America (IDSA) for treating SSTIs caused by BHS,35,38 continue to exhibit low resistance rates. For penicillin-allergic patients, IDSA suggests macrolides and clindamycin as alternatives. However, our study found high resistance to these two antimicrobials among BHS strains, ranking first (71.98%) and second (69.54%) among GPB, respectively. Regarding Enterococcus spp., the high resistance rates to tetracycline (80.28%) and erythromycin (65.32%) were observed. Note that the increasing isolation rate of LRE is alarming, even reaching 20.83% in 2023. Existing literatures have elucidated the resistance mechanisms and the risk of cross-transmission in hospital of LRE.39,40 From 2018 to 2020, the isolation rates of GEH-resistant Enterococcus were persistently higher than those of STH-resistant strains, but a shift occurred in 2021.
The increasing resistance to third and fourth generation cephalosporins of Enterobacterales were concerning, which might be related to the increase of ESBL-E. Nevertheless, the isolation rate of ESBL-E in this study remains lower than that reported in the general patients, or the dermatology patients in the other region.41–43 In third-generation cephalosporins, the resistance rate to ceftriaxone (18.12%) was higher than that to ceftazidime (6.42%). Notably, the resistance rates to amoxicillin/clavulanic acid (18.18%) and cefoxitin (14.84%) in 2018 were higher than in subsequent years, which may be attributed to the influence of special resistant phenotypes that were prevalent that year. It is reassuring that Enterobacterales maintained extremely low resistance rates to carbapenems, such as ertapenem (1.16%) and imipenem (1.65%), and the prevalence of CRE in dermatology patients was not increasing as sharply as reported in the general population.44,45 Considering the extensive use in anti-infection therapy, the resistance rate to quinolones among dermatology patients in this study was acceptable and lower than the overall resistance rates obtained from the surveillance networks in China.41 No Enterobacterales strains resistant to tigecycline were found in this study, indicating that despite the controversy, tigecycline remains one of the options for treating MDR-related infections.37,46 Notably, false non-susceptible results may occur with the disk-diffusion and automated instrument methods for tigecycline testing, and it is recommended to retest using E-test strips.
Although the antimicrobial resistance rates of hospital-associated strains remain concerning in most parts of the world,37 the overall antimicrobial resistance rates of A. baumannii and P. aeruginosa associated with SSTIs were relatively low for most antimicrobials in this study. In particular, the isolation rates of CRAB and CRPA were lower than reported data from the United States and Greece.26,47
Encouragingly, during the study period, dermatology patients exhibited lower rates and fewer changes in resistance to most tested antimicrobials compared to general patients, including significantly lower incidences of major drug-resistant bacteria (except for LRE).41,48 Furthermore, the variation in drug-resistant bacteria differed from current national surveillance data (CARSS & CHINET). For instance, the isolation rate of MRSA, unlike the continuous decline observed in national data, once rebounded to a six-year peak in 2021. CRPA isolation rates in our study, while exhibiting significantly lower than the national average, demonstrated a contrasting increase. Notably, the LRE isolation rates not only consistently exceeded national levels but also continued to rise, reaching approximately 20% in two years. These unique findings are all directions that need to be focused on in future surveillance.
This study period covers the COVID-19 pandemic era, during which the pandemic and related public health policies induced changes in social and medical-seeking behaviors, such as lockdown measures, increased social distancing, and directives to avoid unneeded care. Additionally, infection control practices reached unprecedented levels, including hand hygiene, environmental disinfection, and the use of personal protective equipment such as masks and gloves. Simultaneously, uncertainties surrounding COVID-19 and bacterial co-infections may have led to the overuse of broad-spectrum antimicrobials, thereby creating selective pressure.49 While these measures effectively interrupted viral transmission, they likely also significantly impacted the cross-transmission of common contact-transmitted pathogens (eg, S. aureus), resulting in a reduction in certain bacterial infections,17 while paradoxically increasing others. This phenomenon also drove changes in certain drug-resistant bacterial strains. In this study, in addition to the changes in isolation rates among different populations, our findings also showed that there were fluctuations in the number of patients, and in the isolation rates of major GPB and drug-resistant bacteria during the pandemic, and that the fluctuations varied by pathogens. These fluctuations partially compromised the significance of linear change trend of the statistical results. For instance, over the study period, the isolation rates of CoNS showed an upward trend, whereas S. aureus isolation rates—after showing gradual increases in earlier years—declined during the mid-to-late COVID-19 period, resulting in an overall downward trend. Under the influence of these two pathogens, the isolation rates of GPB showed a trend of first increasing and then decreasing, but the overall linear trend lacked statistical significance. Similar patterns were observed in analyses of major drug-resistant bacterial isolation rates and associated antimicrobial resistance rates. These findings indicate that the pandemic had broad and varied impacts on dermatology patients.17
Our study has several limitations. Firstly, the isolation rates of some bacteria from dermatology patients were particularly low, and different methods or panels of AST were used, which will influence the resistance rates statistics. Secondly, the study on major drug-resistant bacteria was based on confirmed resistant isolates, thus intermediate or non-sensitive data were not included, which may potentially affect further analysis of MDR bacteria beyond MRSA. Thirdly, a common limitation of all retrospective bacteria distribution and antimicrobial resistance studies, including ours, is that whether patients provide specimens for testing depends on the assessment of clinicians. In particular, it is common for dermatologists to use local empirical medication for mild patients without culturing, such as acne. Therefore, our findings represent more those patients with severe conditions who required clinical cultures. Fourthly, our study lacked detailed clinical data on antimicrobial exposure prior to culture, which means we could not adjust for or exclude the confounding effect of selective pressure on resistance patterns. Future research should prioritize systematic collection of detailed antimicrobial use histories to better elucidate the causal pathways leading to resistance. Finally, although our hospital serves as a regional dermatology treatment center with patient sources extending beyond Hangzhou to cover the whole province and neighboring regions, the single-center design inherently limits the generalizability of our results. Owing to heterogeneity in patient demographics, antimicrobial stewardship policies, infection prevention and control protocols, and community transmission dynamics, the observed outcomes may vary across different geographical regions. Consequently, these results should be considered as a complement to local epidemiological characteristics, rather than defining universal patterns. In the future, we plan to establish a comprehensive dermatology patient infections diagnosis and treatment platform. Building on this initial study, the data from different centers will be gradually included to provide a basis for establishing more widely applicable dermatological anti-infective diagnosis and treatment guidelines.
Conclusion
In conclusion, this study provides the characteristics and variations of bacterial epidemiology and antimicrobial resistance in dermatology patients, suggesting that anti-infective therapy should be based on the unique prevalence and resistance patterns of bacteria in local dermatology specialty hospitals. This also highlights the importance of continuous longitudinal surveillance studies for detecting and monitoring regional bacterial distribution and patterns of antimicrobial resistance. Therefore, we advocate for the establishment and refinement of a standardized pathogen surveillance system in specialized dermatology hospitals, with timely data feedback to frontline clinicians. This will foster a virtuous cycle of “surveillance-guided practice-renewed surveillance”, ultimately achieving precise and rational antimicrobial use. Finally, as a hospital consistently ranked among the top in China for annual dermatology outpatient visits for over a decade, we expect that the results presented here will provide valuable information to support clinical anti-infective treatment, antimicrobial stewardship, infection control and public health policy.
Ethics Approval
The study protocol received approval from the Ethics Committee of Hangzhou Third People’s Hospital (#2024KA147). The data used in this retrospective study was obtained from laboratory records. Given that medical records and patient information were anonymized, the Ethics Committee of Hangzhou Third People’s Hospital waived the requirement for informed consent. The Declaration of Helsinki’s guiding principles were followed in this study.
Acknowledgments
The authors thank Hangzhou Third People’s Hospital for providing permission to conduct the study. We also express our gratitude to the staff of the clinical microbiology laboratory at Hangzhou Third People’s Hospital for their diligent efforts in daily work that made this research possible.
Funding
The authors declare that no financial support was received for the research, authorship, and/or publication of this article.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Uberoi A, McCready-Vangi A, Grice EA. The wound microbiota: microbial mechanisms of impaired wound healing and infection. Nat Rev Microbiol. 2024;22(8):507–21. doi:10.1038/s41579-024-01035-z
2. Maher E, Anokhin A. Bacterial skin and soft tissue infections in older adults. Clin Geriat Med. 2024;40(1):117–130. doi:10.1016/j.cger.2023.09.006
3. Aslam B, Wang W, Arshad MI, et al. Antibiotic resistance: a rundown of a global crisis. Infect Drug Resist. 2018;11:1645–1658. doi:10.2147/idr.S173867
4. Storandt MH, Walden CD, Sahmoun AE, Beal JR. Trends and risk factors in the antibiotic management of skin and soft tissue infections in the United States. J Dermatological Treat. 2021;33(3):1576–1580. doi:10.1080/09546634.2020.1859442
5. WHO. WHO bacterial priority pathogens list, 2024: bacterial pathogens of public health importance, to guide research, development and strategies to prevent and control antimicrobial resistance. World Health Organization. 2024.
6. Magiorakos AP, Srinivasan A, Carey RB, et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect. 2012;18(3):268–281. doi:10.1111/j.1469-0691.2011.03570.x
7. Macesic N, Uhlemann AC, Peleg AY. Multidrug-resistant gram-negative bacterial infections. Lancet. 2025;405(10474):257–272. doi:10.1016/s0140-6736(24)02081-6
8. Grossi AP, Ruggieri A, Vecchio AD, et al. Skin infections in Europe: a retrospective study of incidence, patient characteristics and practice patterns. Int J Antimicrob Agents. 2022;60(3). doi:10.1016/j.ijantimicag.2022.106637
9. Liu G, Qin M, Wu X. Analysis of the distribution and antibiotic resistance of pathogens causing infections in hospitals from 2017 to 2019. Evid Based Complement Alternat Med. 2022;2022:1–17. doi:10.1155/2022/3512582
10. Su W, Liu Y, Wang Q, et al. Antibiotic susceptibility and clonal distribution of Staphylococcus aureus from pediatric skin and soft tissue infections: 10-year trends in multicenter investigation in China. Front Cell Infect Microbiol. 2023;13:1179509. doi:10.3389/fcimb.2023.1179509
11. Miller JM, Binnicker MJ, Campbell S, et al. Guide to utilization of the microbiology laboratory for diagnosis of infectious diseases: 2024 update by the Infectious Diseases Society of America (IDSA) and the American Society for Microbiology (ASM). Clinl Infect Dis. 2024. doi:10.1093/cid/ciae104
12. Wilcox MH, Dryden M. Update on the epidemiology of healthcare-acquired bacterial infections: focus on complicated skin and skin structure infections. J Antimicrob Chemother. 2021;76(Supplement_4):iv2–iv8. doi:10.1093/jac/dkab350
13. CLSI. Performance standards for antimicrobial susceptibility testing, M100-33th ed. Clinical and Laboratory Standards Institute. 2023.
14. Muhaj FF, George SJ, Tyring SK. Bacterial antimicrobial resistance and dermatological ramifications*. Br J Dermatol. 2022;187(1):12–20. doi:10.1111/bjd.21033
15. Klein SL, Flanagan KL. Sex differences in immune responses. Nat Rev Immunol. 2016;16(10):626–638. doi:10.1038/nri.2016.90
16. Rochet NM, González-Barreto RM, Martín RF. Characterization of pathogens isolated from cutaneous abscesses in patients evaluated by the dermatology service at an emergency department. P R Health Sci J. 2020;39(3):260–263.
17. Merino P, Kupferwasser D, Flores EA, Phan Tran D, Ortega A, Miller LG. Skin and soft tissue infection incidence before and during the COVID-19 pandemic. Epidemiol Infect. 2023;151. doi:10.1017/s0950268823001802
18. Esposito S, Noviello S, Leone S. Epidemiology and microbiology of skin and soft tissue infections. Curr Opin Infect Dis. 2016;29(2):109–115. doi:10.1097/qco.0000000000000239
19. Salle R, Del Giudice P, Skayem C, Hua C, Chosidow O. Secondary bacterial infections in patients with atopic dermatitis or other common dermatoses. Am J Clin Dermatol. 2024;25(4):623–637. doi:10.1007/s40257-024-00856-1
20. Secombe P, Planche Y, Athan E, Ollapallil J. Critical care burden of skin and soft tissue infection in Central Australia: more than skin deep. Aust J Rural Health. 2019;27(6):550–556. doi:10.1111/ajr.12539
21. Natsis NE, Cohen PR. Coagulase-Negative staphylococcus skin and soft tissue infections. Am J Clin Dermatol. 2018;19(5):671–677. doi:10.1007/s40257-018-0362-9
22. Santin JT, Mariath LM, Rossato AM, Schuler‐Faccini L, Kiszewski AE. Prevalence and antimicrobial resistance profile of Staphylococcus aureus in inherited epidermolysis bullosa: a cross‐sectional multicenter study in Brazil. Int J Dermatol. 2021;60(9):1126–1130. doi:10.1111/ijd.15634
23. Li F, Wu Y, Bian W, et al. Features and associated factors of bacterial skin infections in hospitalized patients with pemphigus: a single-center retrospective study. Ann Clinic Microbiol Antimicrob. 2020;19(1). doi:10.1186/s12941-020-00388-6
24. Nelwan EJ, Tunjungputri RN, Tunjung N, Widodo D. Hospital-acquired skin and skin-structure infection in COVID-19 infected patient with prolonged hospitalization. Acta Med Indones. 2021;53(1):105–107.
25. Dryden MS. Complicated skin and soft tissue infection. J Antimicrob Chemother. 2010;65(Supplement 3):iii35–iii44. doi:10.1093/jac/dkq302
26. Ioannou P, Tsagkaraki E, Athanasaki A, Tsioutis C, Gikas A. Gram-negative bacteria as emerging pathogens affecting mortality in skin and soft tissue infections. Hippokratia. 2018;22(1):23–28.
27. Sandru F, Poenaru E, Stoleru S, et al. Microbial colonization and antibiotic resistance profiles in chronic wounds: a comparative study of hidradenitis suppurativa and venous ulcers. Antibiotics. 2025;14(1). doi:10.3390/antibiotics14010053
28. Hu F, Guo Y, Yang Y, et al. Resistance reported from China antimicrobial surveillance network (CHINET) in 2018. Eur J Clin Microbiol Infect Dis. 2019;38(12):2275–2281. doi:10.1007/s10096-019-03673-1
29. Stelzhammer P, Weber W, Binder H, Sagel U, Aspöck C, Trautinger F. The bacterial pathogen and resistance spectrum in a dermatological inpatient ward: a six-year, retrospective, epidemiological study. GMS Hyg Infect Control. 2022;17. doi:10.3205/dgkh000419
30. Paczosa MK, Mecsas J. Klebsiella pneumoniae: going on the offense with a strong defense. Microbiol Mol Biol Rev. 2016;80(3):629–661. doi:10.1128/mmbr.00078-15
31. Jabbour J-F, Kanj SS. Gram-Negative skin and soft tissue infections. Infect Dis Clin North America. 2021;35(1):157–167. doi:10.1016/j.idc.2020.10.008
32. Moet GJ, Jones RN, Biedenbach DJ, Stilwell MG, Fritsche TR. Contemporary causes of skin and soft tissue infections in North America, Latin America, and Europe: report from the SENTRY antimicrobial surveillance program (1998–2004). Diagnost Microbiol Infect Dis. 2007;57(1):7–13. doi:10.1016/j.diagmicrobio.2006.05.009
33. Yueh C-M, Chi H, Chiu N-C, et al. Etiology, clinical features, management, and outcomes of skin and soft tissue infections in hospitalized children: a 10-year review. J Microbiol Immunol Infect. 2022;55(4):728–739. doi:10.1016/j.jmii.2022.01.007
34. Aman BS, Taj MK, Taj I, Azam S, Khan S, Rashid R. The bacterial profile and antibiotic susceptibility in skin and soft tissue infections at tertiary care hospital of Quetta, Pakistan. J Pak Med Assoc. 2024;74(7):1249–1254. doi:10.47391/jpma.10261
35. Stevens DL, Bisno AL, Chambers HF, et al. Practice guidelines for the diagnosis and management of skin and soft tissue infections: 2014 update by the Infectious Diseases Society of America. Clinl Infect Dis. 2014;59(2):e10–e52. doi:10.1093/cid/ciu296
36. Belloni Fortina A, Neri L. Antibiotic therapy in the management of atopic dermatitis. G Ital Dermatol Venereol. 2015;150(3):321–325.
37. Barbier F, Timsit J-F. Risk stratification for multidrug-resistant bacteria in patients with skin and soft tissue infection. Curr Opin Infect Dis. 2020;33(2):137–145. doi:10.1097/qco.0000000000000642
38. Shulman ST, Bisno AL, Clegg HW, et al. Executive summary: clinical practice guideline for the diagnosis and management of group a streptococcal pharyngitis: 2012 update by the Infectious Diseases Society of America. Clinl Infect Dis. 2012;55(10):1279–1282. doi:10.1093/cid/cis847
39. Misiakou M-A, hertz FB, Schønning K, Häussler S, Nielsen KL. Emergence of linezolid-resistant Enterococcus faecium in a tertiary hospital in Copenhagen. Microbial Genomics. 2023;9(7). doi:10.1099/mgen.0.001055
40. Nasir SAR, Zeeshan M, Ghanchi N, et al. Linezolid-resistant Enterococcus faecium clinical isolates from Pakistan: a genomic analysis. BMC Microbiol. 2024;24(1). doi:10.1186/s12866-024-03491-2
41. Qin X, Ding L, Hao M, Li P, Hu F, Wang M. Antimicrobial resistance of clinical bacterial isolates in China: current status and trends. JAC-Antimicrob Resist. 2024;6(2). doi:10.1093/jacamr/dlae052
42. Li X, Chen Y, Gao W, Ouyang W, Wei J, Wen Z. Epidemiology and outcomes of complicated skin and soft tissue infections among inpatients in Southern China from 2008 to 2013. PLoS One. 2016;11(2). doi:10.1371/journal.pone.0149960
43. Justine B, Mushi M, Silago V, et al. Antimicrobial resistance surveillance of skin and soft tissue infections: hospital-wide bacterial species and antibiograms to inform management at a Zonal Tertiary Hospital in Mwanza, Tanzania. Infect Drug Resist. 2025;18:791–802. doi:10.2147/idr.S483953
44. Hu Y, Liu C, Shen Z, et al. Prevalence, risk factors and molecular epidemiology of carbapenem-resistant Klebsiella pneumoniae in patients from Zhejiang, China, 2008–2018. Emerging Microbes Infect. 2020;9(1):1771–1779. doi:10.1080/22221751.2020.1799721
45. Hou B, Niu X, Yu Q, Wang W. epidemiological trends and drug resistance patterns of carbapenem-resistant gram-negative bacteria: a retrospective study in a tertiary hospital in China (2019-2024). Infect Drug Resist. 2025;18:2867–2880. doi:10.2147/idr.S518461
46. Kuti JL, Dowzicky M, Nicolau DP. Pharmacodynamic performance of tigecycline versus common intravenous antibiotics for the empiric treatment of complicated skin and skin structure infections. Surg Infect. 2008;9(1):57–66. doi:10.1089/sur.2007.001
47. Sader HS, Castanheira M, Duncan LR, Flamm RK. Antimicrobial susceptibility of enterobacteriaceae and Pseudomonas aeruginosa isolates from United States medical centers stratified by infection type: results from the International Network for Optimal Resistance Monitoring (INFORM) surveillance program, 2015–2016. Diagnost Microbiol Infect Dis. 2018;92(1):69–74. doi:10.1016/j.diagmicrobio.2018.04.012
48. Luo Q, Lu P, Chen Y, et al. ESKAPE in China: epidemiology and characteristics of antibiotic resistance. Emerg Microbes Infect. 2024;13(1). doi:10.1080/22221751.2024.2317915
49. Ansari S, Hays JP, Kemp A, et al. The potential impact of the COVID-19 pandemic on global antimicrobial and biocide resistance: an AMR insights global perspective. JAC-Antimicrob Resist. 2021;3(2). doi:10.1093/jacamr/dlab038
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Bacterial Epidemiology and Antimicrobial Resistance Profiles of Respiratory Specimens of Children with Pneumonia in Hainan, China
Mai W, Liu Y, Meng Q, Xu J, Wu J
Infection and Drug Resistance 2023, 16:249-261
Published Date: 12 January 2023
Antimicrobial Resistance Surveillance of Skin and Soft Tissue Infections: Hospital-Wide Bacterial Species and Antibiograms to Inform Management at a Zonal Tertiary Hospital in Mwanza, Tanzania
Justine BN, Mushi MF, Silago V, Igembe Z, Muyombe J, Kishengena PP, Michael Jnr NS, Maganga MG, Massenga A, Tegete F, Massaga FA, Seni J
Infection and Drug Resistance 2025, 18:791-802
Published Date: 10 February 2025