Back to Journals » Neuropsychiatric Disease and Treatment » Volume 19
Evidence-Supported Interventions for Reducing Secondary Stroke Risk in Sub-Saharan Africa: A Systematic Review
Authors Kaddumukasa M, Edwards AM ![]() , Najjuma JN, Mbalinda SN
, Najjuma JN, Mbalinda SN ![]() , Nakibuuka J, Burant CJ
, Nakibuuka J, Burant CJ ![]() , Moore SM, Blixen C, Katabira ET, Sajatovic M, Kaddumukasa M
, Moore SM, Blixen C, Katabira ET, Sajatovic M, Kaddumukasa M ![]()
Received 24 August 2023
Accepted for publication 18 November 2023
Published 28 November 2023 Volume 2023:19 Pages 2597—2606
DOI https://doi.org/10.2147/NDT.S428627
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Martin Kaddumukasa,1 Alyssa M Edwards,2 Josephine Nambi Najjuma,3 Scovia Nalugo Mbalinda,4 Jane Nakibuuka,1 Christopher J Burant,5 Shirley M Moore,6 Carol Blixen,2 Elly T Katabira,1 Martha Sajatovic,2 Mark Kaddumukasa1
1Department of Internal Medicine, College of Health Sciences, Makerere University, Kampala, Uganda; 2Neurological and Behavioral Outcomes Center, University Hospitals Cleveland Medical Center and Case Western Reserve University School of Medicine, Cleveland, OH, USA; 3Department of Nursing, Mbarara University of Science and Technology, Mbarara, Uganda; 4Department of Nursing, College of Health Sciences, Makerere University, Kampala, Uganda; 5Louis Stokes VA Medical Center, Geriatric Research Education, and Clinical Center, Cleveland, OH, USA; 6Frances Payne Bolton School of Nursing, Case Western Reserve University, Cleveland, OH, USA
Correspondence: Martin Kaddumukasa, Email [email protected]
Abstract: The study set out to perform a systematic literature review of evidence-based interventions that target the reduction of secondary stroke risk in Africa. The review analyzed longitudinal intervention studies conducted in Sub-Saharan Africa, focusing on adult participants who had suffered a prior stroke. It encompassed publications and peer-reviewed papers sourced from reputable databases, including PubMed, Ovid, Cochrane, and Web of Science. Three randomized clinical trial (RCT) studies were included with sample sizes ranging from 16 to 400 participants, mean age ranged between 50 and 66 years, with 64.5% male participants. All studies applied multidisciplinary team interventions of enhanced patient follow-up involving care givers, nurse educators, physicians, and social workers. Interventions ranged from comprehensive patient education, tracking of medication adherence and enforcing healthy lifestyle behaviors (regular exercise, regular BP checks, and dietary changes). We found a decrease in Systolic Blood Pressure over time in 2 of 3 treatment groups, an improvement in medical adherence in all treatment groups, and a decrease in cholesterol levels in 1 treatment group. Evidence-based interventions involving multidisciplinary teams and comprehensive patient education were found to demonstrate promising results in reducing secondary stroke risk in Africa, leading to significant improvements in medical adherence and reductions in systolic blood pressure in the majority of treatment groups. However, more research is required to confirm the influence of these interventions on cholesterol levels and to establish their lasting advantages in preventing strokes among African communities.
Keywords: secondary stroke risk, risk interventions, Sub-Saharan Africa
Introduction
Stroke is a major cause of death globally1 with approximately 80% of all deaths occurring in developing countries.2 While high-income countries have experienced a significant decline in stroke burden of over 40% over the past four decades,3–5 lower and middle-income countries (LMICs) have witnessed a notable rise of more than 100% in stroke burden during the same period.6 Notably, Africa accounts for 8% of all first-ever strokes, and African individuals make up 5% of the 30 million stroke survivors worldwide.7 Stroke also affects younger people in developing nations about 10–15 years earlier compared to developed countries.1,8 Survivors of stroke face a heightened risk of recurrent stroke and other cardiovascular events.9 The 5-year major cardiovascular event rate is estimated at 24%,10 pointing to a growing urgency for stroke management and secondary prevention strategies. Over the past decade, preventive measures targeting cardiovascular risk factors, such as hypertension, high cholesterol, and smoking, have led to a reduction in stroke incidence and mortality.11,12 However, it is important to note that these positive trends are not consistently observed across all populations.13
Population-wide interventions targeting risk factors, including hypertension, alcohol abuse, smoking, high cholesterol, and physical inactivity, have been reported as crucial in reducing the incidence of strokes and associated fatalities.14 These interventions form an integral part of secondary stroke prevention measures. It is important to continue to advance research on how best to manage individuals who have had stroke, as these individuals are at risk for recurrent stroke. Addressing risk factors for recurrent stroke through targeted interventions has the potential to mitigate disparities associated with this condition. Due to the disproportionate burden of stroke in African populations, we conducted a systematic review of the literature review with the aim of identifying interventions that effectively reduce secondary stroke risk among Africans. The aims of this review were twofold: (1) to present an overview of the approaches studied for reducing secondary stroke risk in Africans, and (2) to identify the expected outcomes from effective interventions.
Methods
Search and Selection of Studies
In this systematic literature review, we searched relevant peer-reviewed articles published before June 2021 in electronic databases, including PubMed, Cochrane, and Web of Science.
Search strategy. In June 2021, extensive searches were performed in each database using various combinations of search terms. The search terms served two purposes: they helped narrow search results to the target sample population in question, and they helped to identify interventional studies. Some terms we used to isolate our populations of interest included “sub Saharan Africa”. The final search terms we used to run our searches were as follows: ((“stroke”[MeSH Terms] OR “stroke”[All Fields]) AND (“survivors”[MeSH Terms] OR “survivors”[All Fields]) AND (“risk reduction behavior”[MeSH Terms] OR (“risk”[All Fields] AND “reduction”[All Fields] AND “behavior”[All Fields]) OR “risk reduction behavior”[All Fields] OR (“risk”[All Fields] AND “reduction”[All Fields]) OR “risk reduction”[All Fields] OR “adaptation, psychological”[MeSH Terms] OR (“adaptation”[All Fields] AND “psychological”[All Fields]) OR “psychological adaptation”[All Fields]) AND “interventions”[All Fields] AND (“random allocation”[MeSH Terms] OR (“random”[All Fields] AND “allocation”[All Fields]) OR “random allocation”[All Fields] OR “randomized”[All Fields]) AND study[All Fields]) AND “sub Saharan Africa”[All Fields].
These terms were also combined with search terms specifically related to interventions targeting secondary stroke risk reduction. After a comprehensive review, a total of four articles describing 3 studies were selected that met both the inclusion and exclusion criteria listed in Table 1.
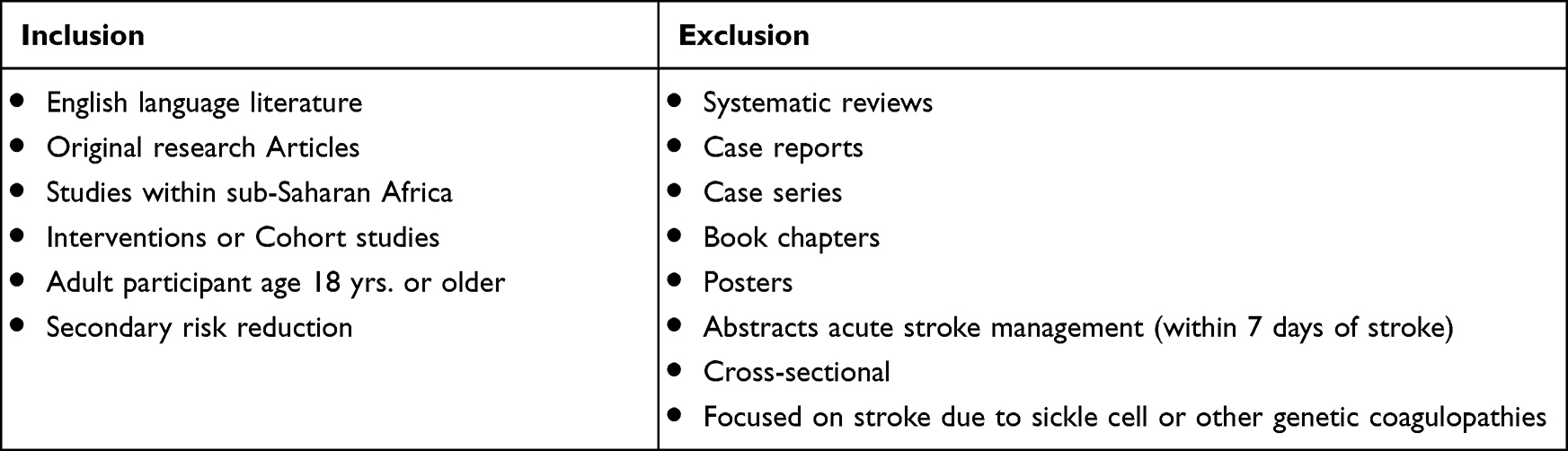 |
Table 1 Inclusion and Exclusion Criteria for the Selected Articles |
Article Selection and Quality Assessment
One reviewer (MK) conducted a prescreening of all abstracts for relevance, using title and abstract information as the basis for assessment. Studies with participants who had encountered a stroke, transient ischemic attack (TIA), or intracranial hemorrhage were included in the review. The studies were eligible for inclusion if they investigated the impact of interventions or exposures aimed at reducing stroke risk, encompassing randomized control trials, cohort studies, and quasi-experiments. Two authors (KMN and AE), then, independently screened these abstracts for potential inclusion, and any inconsistencies around inclusion criteria were resolved by a third author (KM). Next, selected full-text articles were retrieved and underwent a detailed review based on the inclusion and exclusion criteria. The focus of this literature review was on interventions aimed at reducing secondary stroke risk. Studies that solely described stroke management in the acute phase (within 7 days of onset of stroke) or cross-sectional studies (collecting data at a single point in time and do not involve any intervention or follow-up over time) were excluded from the review. Other notable criteria for article exclusion included opinion pieces, editorials, book chapters, and other literature reviews that did not qualify as primary research articles directly examining interventions to mitigate the risk of secondary stroke. Figure 1 shows an overview of the identification and selection process. The Newcastle–Ottawa Scale (NOS) was used to assess the quality of each retrieved article13,15 (see NOS scores in Table 2). The NOS is widely utilized to assess the quality of various study components, including 1) sample representativeness, 2) choice of intervention and control groups, 3) level of exposure, etc. The adapted NOS used in this study had a possible scoring range of 0 to 12, where higher scores indicated higher quality of methodology.
 |
Table 2 Summary of Study Goal, Design, Sample Size, and Primary Outcomes |
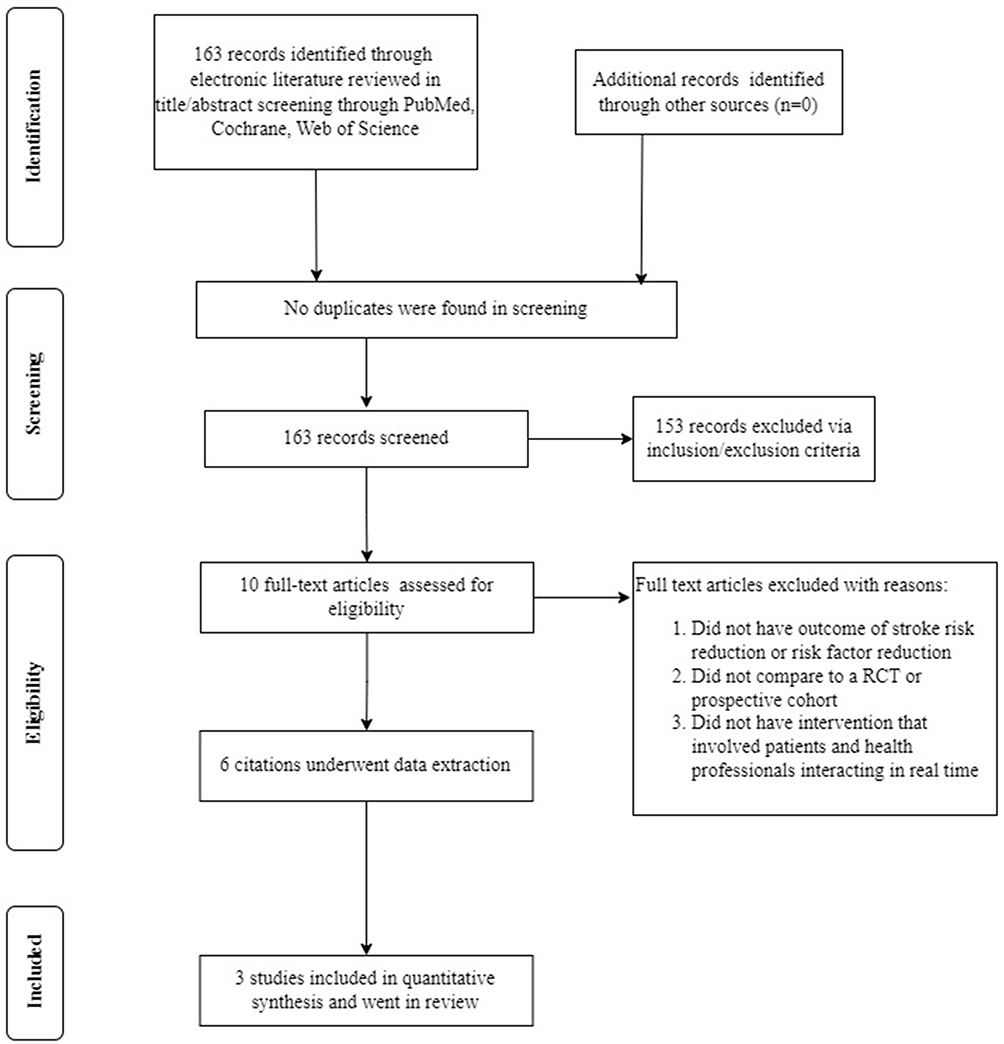 |
Figure 1 Overview of the identification and selection process. |
Data Extraction
Data extracted from the studies included the year of the study, intervention components, project objective, sample size, methods, results, conclusion, and strengths/limitations of the study. Quantitative data on blood pressure control interventions, medical adherence and behavioral risks were collected regarding stroke risk reduction in SSA.
Results
Study Quality
The NOS ratings for the three studies ranged from 7, the lowest, to 9, the highest. A major strength of all these studies was their prospective experimental design, focusing on intervention testing rather than being observational in nature. All studies included in the review were RCTs.16,18,19 One study had a sample size of only 16,19 one had a sample of 60,16,17 and one of 400 participants18 Study participants had suffered a stroke and were above 18 years of age. Two of the studies16,19 included hypertension >140/90 as part of their inclusion criteria. Regarding stroke eligibility, most studies included participants who had suffered a stroke within the past 1 month to a 5-year period.
Overview of Studies
Out of the 163 reports initially reviewed, only 3 studies met the inclusion criteria and were included in the final analyses. Of these, sample sizes ranged from 16 to 400 participants, mean age between 50 and 66 years, with 64.5% male participants. These publications represented three different countries, with one each from Ghana, Nigeria, and Uganda. Of these, two studies were single-centered18,19 and one was a multicenter study.18 Follow-up periods ranged from 6 to 12 months. The Risk reduction interventions addressed included blood pressure, diabetes, alcohol use, smoking, and cholesterol control.
Study Design and Interventions
The interventions in the three studies differed significantly in terms of format, delivery, and duration, with the majority focusing on behavioral and educational approaches aimed at reducing secondary stroke risk. In the study conducted by Kaddumukasa et al,19 authors assessed, over a period of 6-months, the impacts of a culturally tailored behavioral intervention – the Targeted Management Intervention (TEAM). This intervention involved using peer dyads, consisting of patients who had experienced a stroke or transient ischemic attack (TIA) and their care partners, exemplifying behaviors aimed at reducing future stroke risk in 16 individuals identified as being at high risk for stroke. In the study by Mayowa et al,18 the impact of increased follow-up visits and pre-appointment phone texts was investigated;20 in addition to support for patient self-management through patient report cards, post-clinic follow-up phone texts, and educational videos. The study involved 400 stroke survivors. Similarly, Sarfo et al17 evaluated the efficacy of a nurse-guided intervention facilitated by mHealth technology, initiated within one month of symptom onset in stroke patients. The study aimed to improve blood pressure (BP) control at 3 and 9 months after the intervention. All participants in the studies had a diagnosis of TIA and/or ischemic stroke and were recruited from secondary care settings, predominantly from stroke units. Each of the studies (n = 3) included patient self-management components as part of their interventions. While one study used peer dyads consisting of stroke or TIA survivors and their care partners,19 the other two studies17,19 relied on enhanced patient follow-up with healthcare professionals including research assistants,21 nurse educators,22 and social workers.20 Mayowa et al18 introduced a patient self-management intervention where participants were given report cards to assess their grasp of the challenges and enablers of stroke prevention. Additionally, they received an informative educational video in which stroke scenarios and educational messages were dramatized. The interventions included meetings with peers and caregivers to facilitate self-management support, stroke risk education, and training in healthy coping strategies. The duration of the interventions varied, ranging from a 4-session education program18 to 24-week programs.19
Control groups in all the selected studies were used to compare the effectiveness of the interventions. The control groups received “standard” stroke care, mainly consisting of monthly follow-up visits with primary care givers. Additionally, the control groups commonly received short text messages focusing on healthy lifestyle behaviors and reminders for drug refills.17
Outcomes
The primary measure employed to assess the impact of interventions in the studies under consideration was the alteration in systolic blood pressure (SBP). Furthermore, in one of the studies,19 laboratory measurements were documented including data on cholesterol levels and Glycosylated hemoglobin (HbA1c). Table 2 presents an analysis of several supplementary variables, including awareness of stroke risk factors, medical adherence, side effects, hypertension and stroke knowledge, smoking, alcohol use, and physical activity.
Every study incorporated in the review documented alterations in systolic blood pressure (SBP). Out of these, two studies observed a decline in SBP over the study time in the intervention group. Mayowa et al found that SBP in the intervention group decreased by 11.7 mm Hg (95% CI 5.61–16.75) and that in the standard care group, it decreased by 11.2 mm Hg (95% CI 7.01–16.41) between baseline and 12-month follow-up. Nevertheless, this reduction did not demonstrate statistical significance between the groups (p = 0.7451) and lacked clinical significance. The remaining two studies found statistically significant improvements in SBP between the two test groups. Kaddumukasa et al observed a significant decrease in SBP in the intervention group (p = 0.021). SBP decreased from 162.9 at baseline to 149.1 mm Hg at 24 weeks.
In addition, Kaddumukasa et al19 measured cholesterol levels including HDL, LDL, and total cholesterol. The changes in HDL and LDL cholesterol were not clinically significant. No distinctions were observed between the baseline measurements and those at week 12 (p = 0.062), as well as between measurements at week 12 and week 24 (p > 0.999). However, there was a significant change in the proportion of individuals who had values above the optimal target for serum total cholesterol. A scrutiny of diabetes management within the same intervention group indicated a substantial decrease in HbA1C levels by week 24, dropping from 10.7% (±1.7%) to 5.8% (±2.9%); p = 0.031. On the other hand, alcohol use disorders as assessed using the AUDIT tool,23 tobacco-use as measured by the Global Adult Tobacco Survey (GATS) questionnaire,24 and global physical activity25 as assessed using the Global Physical Activity Questionnaire GPAQ found no significant differences in these behaviors from baseline to 24 weeks.
In two publications, Sarfo et al documented their findings regarding the practicability and effectiveness of a nurse-guided intervention utilizing m-Health technology to manage blood pressure levels. The studies showed that scores for self-autonomous regulation exhibited significant improvement from a mean of 64.7 to 80.2 (p = 0.0001) in the intervention group and from 68.4 to 82.3 (p < 0.0001) in the control group over the 9-month study period. Likewise, there was a notable enhancement in perceived confidence among participants in both the intervention (82.2% to 92.7% (p = 0.001)) and control (86.3% to 95.7% (p = 0.007)) groups regarding adhering to physician-prescribed medication regimens.
Discussion
The focus of this review was to investigate the existing evidence on interventions aimed at reducing secondary stroke risk in the SSA population, which faces a disproportionately high burden from stroke. Despite the heavy and growing burden of stroke in SSA, the review found a limited number of studies (n = 3) with a combined sample size of less than 500 participants. The mean age was relatively low, ranging from 51–68-years. In SSA, instances of stroke commonly manifest in individuals below the age of 60, in contrast to Western countries where strokes typically impact older individuals aged 70 to 75.5 Behavior lifestyle differences and younger patients with poor BP control likely contribute to this higher stroke risk.
All studies were designated as experimental studies, comparing enhanced treatment to usual standard care. All studies used behavioral interventions targeting modifiable risk factors for CVD/stroke. These interventions were delivered in hospitals or in the community and included patient education and teaching. The interventions were multidimensional and were delivered by registered nurses in collaboration with other healthcare professionals such as social workers, physician assistants, and research assistants (Table 3). Some interventions used integrated healthcare professionals and patients through increased follow-up visits, reappointment phone texts, meetings, education sessions, or educational videos. The involvement of a transdisciplinary team of health personnel and administrators in these studies indicates that individuals with diverse expertise in cardiovascular health, and associated lifestyle management can play essential roles in such intervention programs. This implies that interventions aimed at mitigating stroke risks within susceptible subgroups could potentially be applied universally across various healthcare providers.
 |
Table 3 Stroke Interventions and Group Involved in Stroke Prevention |
Interventions with self-management and pharmacological programs demonstrated better and significant outcomes in terms of blood pressure control than the standard of care. They comprised sessions involving peers or caregivers to provide self-management assistance, educational modules focusing on prevalent stroke risk factors, and instruction in enhancing problem-solving abilities and adopting healthy coping strategies. These interventions facilitated individuals and care partners in recognizing stroke risk factors and encouraged healthy behavior change through personalized motivational text messages, improved follow-up visits, and enhanced medical adherence.16–19 Kaddumukasa et al included eight in-person follow-ups with the nurse educator, while Sarfo et al had 15 in-person follow-ups with a peer dyad and nurse educator. All the interventions focused on improving knowledge and re-enforcing appropriate behaviors that are pertinent to stroke risk reduction among a high-risk group.
These studies demonstrate that self-management practices can be adopted and integrated into health care settings in SSA. Currently, there is limited evidence available on effectively supporting the implementation and integration of stroke self-management interventions within clinical practice. Harmonizing the quality of educational materials or guides for self-management is needed to ensure similar messaging and integration into routine clinics by various health care cadres. In the literature, self-management interventions have been found to significantly improve symptom management26 and have the most substantial impact on enhancing medication adherence.27
All studies (n = 3) had BP as a primary outcome, with follow-up ranging from 3 to 12 months. In all studies, the researchers found that the interventions improved both systolic and diastolic blood pressures. Three studies reported a mean decrease in systolic BP of 11 mmHg and one study showed a decrease of 16.7 mmHg from baseline to the end of the study period.17–19 This study revealed a statistically notable decrease in blood pressure scores, which was credited to the impact of the intervention. This discovery carries population-level relevance given that a 2mmHg reduction in SBP was approximated to a 10% decrease in stroke-related mortality as well as 7% decrease in the risk of ischemic heart disease and other vascular causes.13,28,29. Notably, in one study, the intervention did not show any significant association with SBP reduction compared to the control group. However, both the intervention and control groups exhibited a similar significant decrease in mean blood pressure from baseline to 1 year.18
Study Strengths and Limitations
This systematic review encountered certain limitations primarily due to the scarcity of regionally relevant studies in the research area. Only three studies met the inclusion criteria, which restricted our ability to conduct a quantitative analysis (meta-analysis) due to insufficient data for comparing differences across groups and risk factors. Additionally, the included studies exhibited a lack of heterogeneity. Another limitation stemmed from the varying durations of follow-up, which ranged from 24 weeks to 1 year. This diversity in follow-up duration posed a challenge in assessing the impact of rehabilitation interventions over time. It is worth noting that this study was not registered in the Prospero registry, although we followed all the necessary methodologies. Therefore, when interpreting the results, caution is warranted. The shorter study durations may not have provided ample time for rehabilitation interventions to effectively influence modifiable vascular risk factors. Furthermore, the concept of intervention intensity remained poorly defined across the studies, contributing to heterogeneity within the complex interventions under investigation.
This review contributes to an increasing body of evidence highlighting the importance of informed, prepared, and motivated patients as crucial stakeholders in blood pressure control. It underscores the need for further studies focusing on SSA patients to better understand and address this important aspect of healthcare. Results also suggest that patient education interventions are likely to improve modifiable risk factor control and that integrating self-management approaches is feasible and achieves the desired blood pressure control. Additional study through large-scale, well-designed randomized controlled trials (RCTs) using appropriate objective outcome measures is imperative to establish the most effective strategies for secondary stroke prevention. There is a demand for research reports that provide more detailed information on the frequency and intensity of interventions, the optimal timing for initiating secondary prevention strategies, exploration of their implementation into usual care, and evaluation of cost-effectiveness.
Despite the above limitations, to our knowledge, this provides the first systematic literature review on evidence-based stroke risk reduction interventions and their effects on patient outcomes in the African region.
To conclude, this review underscores the pivotal role of incorporating training on patient self-management into patient care strategies, as it proves instrumental in mitigating secondary stroke risk within the African population. These interventions show significant potential in improving stroke outcomes, particularly for individuals dealing with uncontrolled hypertension. The counseling and follow-up approaches employed in the studied interventions seem to have broad applicability for multidisciplinary healthcare teams. Moreover, increasing the frequency of stroke-specific follow-up may lead to even more favorable results. Further, randomized controlled trials that include lifestyle interventions, sociocultural aspects, and community-based interventions are still urgently needed.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research project was funded by the National Institute of Neurological Disorders and Stroke and Stroke of the National Institutes of Health under award number R01NS118544. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Disclosure
Shirley Moore and Martha Sajatovic report grants from NIH, during the conduct of the study; Martha Sajatovic reports grants from Otsuka, Alkermes, International Society for Bipolar Disorders (ISBD), National Institutes of Health (NIH), Centers for Disease Control and Prevention (CDC), Patient-Centered Outcomes Research Institute (PCORI), and personal fees from Alkermes, Otsuka, Janssen, Lundbeck, Teva, Neurelis, Springer Press, Johns Hopkins University Press, Oxford Press, UpToDate, outside the submitted work; The authors report no other conflicts of interest in this work.
References
1. Lemogoum D, Degaute JP, Bovet P. Stroke prevention, treatment, and rehabilitation in sub-saharan Africa. Am J Prev Med. 2005;29(5 Suppl 1):95–101. doi:10.1016/j.amepre.2005.07.025
2. Feigin VL, Stark BA, Johnson CO, et al. Global, regional, and national burden of stroke and its risk factors, 1990–2019: a systematic analysis for the global burden of disease study 2019. Lancet Neurol. 2021;20(10):795–820. doi:10.1016/S1474-4422(21)00252-0
3. Feigin VL, Norrving B, Mensah GA. Global burden of stroke. Circ Res. 2017;120(3):439–448.
4. Namale G, Kamacooko O, Kinengyere A, et al. Risk factors for hemorrhagic and ischemic stroke in sub-saharan Africa. J Trop Med. 2018;2018:4650851. doi:10.1155/2018/4650851
5. Donkor ES. Stroke in the 21(st) century: a snapshot of the burden, epidemiology, and quality of life. Stroke Res Treat. 2018;2018:3238165.
6. Chin JH. Stroke in sub-saharan Africa: an urgent call for prevention. Neurology. 2012;78(13):1007–1008. doi:10.1212/WNL.0b013e318248df95
7. Truelsen T. Stroke incidence studies in Africa. Lancet Neurol. 2010;9(8):755–757. doi:10.1016/S1474-4422(10)70161-7
8. Boot E, Ekker MS, Putaala J, Kittner S, De Leeuw F-E, Tuladhar AM. Ischaemic stroke in young adults: a global perspective. J Neurol Neurosurg Psych. 2020;91(4):411–417. doi:10.1136/jnnp-2019-322424
9. Poledník I, Sulzenko J, Widimsky P. Risk of a coronary event in patients after ischemic stroke or transient ischemic attack. Anatol J Cardiol. 2021;25(3):152–155.
10. Hackam DG, Spence JD. Combining multiple approaches for the secondary prevention of vascular events after stroke: a quantitative modeling study. Stroke. 2007;38(6):1881–1885. doi:10.1161/STROKEAHA.106.475525
11. Mensah GA, Wei GS, Sorlie PD, et al. Decline in cardiovascular mortality: possible causes and implications. Circ Res. 2017;120(2):366–380. doi:10.1161/CIRCRESAHA.116.309115
12. Lackland DT, Roccella EJ, Deutsch AF, et al. Factors influencing the decline in stroke mortality: a statement from the American Heart Association/American Stroke Association. Stroke. 2014;45(1):315–353. doi:10.1161/01.str.0000437068.30550.cf
13. Cao C, Jain N, Lu E, Sajatovic M, Still CH. Secondary stroke risk reduction in black adults: a systematic review. J Racial Ethn Health Disp. 2022;31–13.
14. Kolapo KO, Vento S. Stroke: a realistic approach to a growing problem in sub-saharan Africa is urgently needed. Trop Med Int Health. 2011;16(6):707–710. doi:10.1111/j.1365-3156.2011.02759.x
15. CK-L L, Mertz D, Loeb M. Newcastle-Ottawa scale: comparing reviewers’ to authors’ assessments. BMC Med Res Method. 2014;14(1):45. doi:10.1186/1471-2288-14-45
16. Sarfo F, Treiber F, Gebregziabher M, et al. PINGS (Phone-Based Intervention Under Nurse Guidance After Stroke): interim results of a pilot randomized controlled trial. Stroke. 2018;49(1):236–239. doi:10.1161/STROKEAHA.117.019591
17. Sarfo FS, Treiber F, Gebregziabher M, et al. Phone-based intervention for blood pressure control among Ghanaian stroke survivors: a pilot randomized controlled trial. Int J Stroke. 2019;14(6):630–638. doi:10.1177/1747493018816423
18. Owolabi MO, Gebregziabher M, Akinyemi RO, et al. Randomized trial of an intervention to improve blood pressure control in stroke survivors. Circ Cardiovasc Qual Outcomes. 2019;12(12):e005904. doi:10.1161/CIRCOUTCOMES.119.005904
19. Kaddumukasa M, Nakibuuka J, Mugenyi L, et al. Feasibility study of a targeted self-management intervention for reducing stroke risk factors in a high-risk population in Uganda. J Neurol Sci. 2018;386:23–28. doi:10.1016/j.jns.2017.12.032
20. Afolayan TO, Ehikhamenor FA, Mejabi VO, Oyekunle RA, Bello OW, Balogun NA. Mobile phone usage in rural communities in Kwara state. Nigeria. 2015;2015:1.
21. Arulogun OS, Hurst S, Owolabi MO, et al. Experience of using an interdisciplinary task force to develop a culturally sensitive multipronged tool to improve stroke outcomes in Nigeria. eNeurologicalSci. 2016;4:10–14. doi:10.1016/j.ensci.2016.04.003
22. Rimmer JH, Braunschweig C, Silverman K, Riley B, Creviston T, Nicola T. Effects of a short-term health promotion intervention for a predominantly African-American group of stroke survivors. Am J Prev Med. 2000;18(4):332–338. doi:10.1016/S0749-3797(00)00129-X
23. Pradhan B, Chappuis F, Baral D, et al. The alcohol use disorders identification test (AUDIT): validation of a Nepali version for the detection of alcohol use disorders and hazardous drinking in medical settings. Subst Abuse Treat Prev Policy. 2012;7(1):42. doi:10.1186/1747-597X-7-42
24. Palipudi KM, Morton J, Hsia J, et al. Methodology of the global adult tobacco survey — 2008–2010. Global Health Promo. 2013;23(2_suppl):3–23.
25. Cleland CL, Hunter RF, Kee F, Cupples ME, Sallis JF, Tully MA. Validity of the Global Physical Activity Questionnaire (GPAQ) in assessing levels and change in moderate-vigorous physical activity and sedentary behaviour. BMC Public Health. 2014;14(1):1255.
26. Barlow J, Wright C, Sheasby J, Turner A, Hainsworth J. Self-management approaches for people with chronic conditions: a review. Patient Educ Couns. 2002;48(2):177–187.
27. Sakakibara BM, Kim AJ, Eng JJ. A systematic review and meta-analysis on self-management for improving risk factor control in stroke patients. Int J Behav Med. 2017;24(1):42–53. doi:10.1007/s12529-016-9582-7
28. Lennon O, Galvin R, Smith K, Doody C, Blake C. Lifestyle interventions for secondary disease prevention in stroke and transient ischaemic attack: a systematic review. Eur J Prev Cardiol. 2014;21(8):1026–1039. doi:10.1177/2047487313481756
29. Verdecchia P, Gentile G, Angeli F, Mazzotta G, Mancia G, Reboldi G. Influence of blood pressure reduction on composite cardiovascular endpoints in clinical trials. J Hypertens. 2010;28(7):1356–1365. doi:10.1097/HJH.0b013e328338e2bb
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.