Back to Journals » Nature and Science of Sleep » Volume 14
Evidence of White Matter Integrity Changes in the Anterior Cingulum Among Shift Workers: A Cross-Sectional Study
Authors Lee J, Kim M, Kim N, Hwang Y ![]() , Lee KH, Lee J, Lee YJ, Kim SJ
, Lee KH, Lee J, Lee YJ, Kim SJ ![]()
Received 2 April 2022
Accepted for publication 3 August 2022
Published 16 August 2022 Volume 2022:14 Pages 1417—1425
DOI https://doi.org/10.2147/NSS.S369192
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sarah L Appleton
Jiye Lee,1,* Minjeong Kim,1,* Nambeom Kim,2 Yunjee Hwang,1 Kyung Hwa Lee,3,4 Jooyoung Lee,1 Yu Jin Lee,3 Seog Ju Kim1
1Department of Psychiatry, Sungkyunkwan University College of Medicine, Samsung Medical Center, Seoul, Republic of Korea; 2Department of Biomedical Engineering Research Center, Gachon University, Incheon, Republic of Korea; 3Department of Psychiatry and Center for Sleep and Chronobiology, Seoul National University, College of Medicine and Hospital, Seoul, Republic of Korea; 4Division of Child and Adolescent Psychiatry, Department of Psychiatry, Seoul National University Hospital, Seoul, Republic of Korea
*These authors contributed equally to this work
Correspondence: Yu Jin Lee, Department of Psychiatry and Center for Sleep and Chronobiology, Seoul National University, College of Medicine and Hospital, Seoul, Republic of Korea, Email [email protected] Seog Ju Kim, Department of Psychiatry, Sungkyunkwan University College of Medicine, Samsung Medical Center, Seoul, Republic of Korea, Email [email protected]
Introduction: We investigated the white matter integrity in shift and non-shift workers and its associations with sleep and activity.
Methods: Diffusion tensor imaging (DTI) was performed on 61 shift workers and 31 non-shift workers. Their sleep and activity profiles were assessed using the Pittsburgh Sleep Quality Index (PSQI), sleep diaries, and actigraphy. Fractional anisotropy (FA) (a measure of white matter integrity) was calculated using DTI tractography.
Results: Shift workers exhibited higher FA values in the bilateral anterior cingulum than did non-shift workers. An increased FA in the right anterior cingulum was correlated with poor sleep quality (ie, a high PSQI score) in shift workers. An increased FA in the right anterior cingulum was also correlated with higher actigraphic activity indices (the mesor and M10 indices) in shift workers.
Discussion: The white matter integrity of the anterior cingulum was altered in shift workers, perhaps in association with sleep and activity disturbances.
Keywords: shift work, DTI, cingulum, sleep, activity
Introduction
Today, 15–20% of the working population is on duty outside of traditional daytime hours.1 Shift workers regularly experience sleep disturbances attributable to desynchronization of the homeostatic sleep pressure and circadian rhythm; thus, they are predisposed to the development of shift work disorder.2 A recent meta-analysis found that 26.5% of all shift workers met the diagnostic criteria for this disorder, thus severe disturbances during sleep and/or excessive sleepiness during waking.3
Several previous studies have described structural and functional brain changes in shift workers.4,5 Simulated night shift work reportedly changed the pattern of brain protein synthesis in a rat study.6 To the best of our knowledge, no study has yet reported white matter changes in shift workers. As white matter plays an important role in maintenance of the circadian rhythm,7,8 we sought white matter alterations in shift workers and the effects thereof on sleep and activity.
Sleep quality has been associated with structural white matter changes.8–11 Previous studies reported that white matter alterations were related to the sleep quality of college students10 and older adults.11 A relationship between white matter integrity and sleep quality has also been observed in patients with insomnia.12,13 Shift workers are physically over-active during both occupational and non-occupational hours.14,15 Previous studies have reported correlations between white matter integrity and physical activity; more physically active people evidenced more integrated white matter.16,17 Therefore, we investigated whether sleep quality and the activity level were associated with white matter alterations in shift workers.
Functional changes in the anterior cingulate cortex (ACC) have been reported in those with disturbed circadian rhythms. Changes in the functional connectivity of the ACC to other brain areas has been reported in night shift nurses18 and delirium patients with circadian rhythm disturbances.19 As white matter tracts structurally connect distant brain areas, white matter tract changes might occur in the anterior cingulum of those with circadian rhythm disturbances. However, no previous study on the anterior cingulum white matter tract of shift workers has appeared, although those with sleep disturbances were reported to exhibit white matter tract changes of cingulum.13 A comparison of white matter integrity between shift workers and non-shift workers would aid our understanding of how environmental circadian disturbances affect white matter integrity.
We compared the white matter integrity between shift workers and non-shift workers via diffusion tensor imaging (DTI) tractography. We also investigated the associations between white matter alterations and the subjective and objective sleep and activity characteristics of shift workers. Based on previous studies, we hypothesized that the white matter integrity in a specific region such as anterior cingulum would differ between shift and non-shift workers. Additionally, we hypothesized that white matter alterations in shift workers would correlate with their sleep and activity levels.
Methods
Participants
An opportunity sample was used. From June 2017 to December 2019, participants were recruited via advertisements placed at Seoul National University Hospital and Samsung Medical Center. Shift workers were defined as individuals with rotating or non-standard shifts. In a broad sense, shift workers can be defined as those with rotating work shifts (ie, the work shifts change over time) or those with non-standard shifts (ie, all working shifts are out of standard daytime working hours). In the current study, shift workers with both rotating and non-standard shifts were recruited. The inclusion criteria were as follows: 1) three-shift rotations each of 8 hours, 2) at least one work shift commencing before 7 AM or after 6 PM, and 3) shift work for more than 6 months. The inclusion criteria for non-shift workers were as follows: 1) no rotating work shifts, 2) working between 7 AM and 6 PM, and 3) an absence of sleep disturbance.
The Structured Clinical Interview for the Diagnostic and Statistical Manual of Mental Disorders-IV was performed by trained psychologists as screening for psychiatric disorders. Nocturnal polysomnography was conducted to screen for common sleep disorders including obstructive sleep apnea. The exclusion criteria were as follows: a prior serious medical or neurological illness; an apnea-hypopnea index score ≥ 30 or a periodic limb movement index score ≥ 50; an Axis I psychiatric disorder other than circadian rhythm sleep disorder, shift work type (as defined by the Diagnostic and Statistical Manual of Mental Disorders-IV); a sleep disorder other than shift work sleep disorder (SWD) (based on the International Classification of Sleep Disorders-3 criteria); pregnancy; and any contraindication for magnetic resonance imaging (MRI). Of the initially recruited individuals, two shift workers and three non-shift workers were excluded because of poor image quality (motion artifacts or b value errors). Finally, 61 shift workers (15 men and 46 women aged 30.84 ± 6.37 years, age 24–57 years) and 31 non-shift workers (8 men and 23 women aged 32.74 ± 6.36 years, age 23–48 years) participated (Supplementary Figure 1). The shift workers of the current study worked for 8 hours per shift (day, evening, and night shifts). Their weekly shifts were not fixed, but they reported approximately 1 or 2 shifts per week. This study was approved by the Institutional Review Board of Seoul National University Hospital and conducted in accordance with the declaration of Helsinki. All participants provided written informed consent before study commencement.
Self-Reported Data
The Pittsburgh Sleep Quality Index (PSQI) was used to evaluate subjective sleep quality during the previous month in terms of seven sleep domains (subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbance, use of sleep medications, and daytime dysfunction).20 The Epworth Sleepiness Scale (ESS) was employed to measure daytime sleepiness; participants rate the risks of falling asleep in eight different situations.21 The Insomnia Severity Index (ISI) was used to assess the severities of the nighttime and daytime components of insomnia.22
A sleep diary was employed to record subjective sleep parameters: total sleep time (TST), sleep efficiency (SE), wake time after sleep onset (WASO), and sleep onset latency (SOL). All participants were instructed to record sleep-related information daily in a diary for 2 weeks.
Actigraphy-Based Measurements of Sleep and Circadian Variables
Actigraphy is a non-invasive technique that objectively measures sleep parameters and activity cycles over days to weeks. All participants wore an Actiwatch 2 (Phillips Respironics; Murrysville, PA, USA) on the non-dominant wrist for 8 consecutive days. All data were collected in 30-s epochs. Actiware ver. 6.0.9 was used to calculate actigraphic data and sleep variables. Sleep diary data, rest periods, and excluded intervals were manually processed by technicians who were blinded to the other variables. Actigraphy yielded objective TST, SE, WASO, and SOL data.
The raw actigraphic data were subjected to cosinor analysis to calculate the mesor (midline of the oscillating curve; higher values suggest higher activity levels), the amplitude (the peak-to-nadir difference of the fitted curve; higher amplitudes suggest more robust rhythms or higher activity levels), the F-statistic (reflecting the robustness of circadian activity; higher values suggest more robust rhythms), and the acrophase (the time of peak activity during the day; a later time suggests a more delayed phase). Nonparametric variables were also calculated, including the most active 10-hour period (M10; a higher M10 represents a more active wake period), interdaily stability (IS; a higher IS indicates better synchronization to light and other environmental cues), intradaily variability (IV; a higher IV indicates greater fragmentation of the 24-hour rest-activity rhythm), relative amplitude (a higher relative amplitude indicates a more robust rhythm), and the least active 5-hour period (L5; a higher L5 indicates less restful sleep).23,24 The cosinor and nonparametric analyses were discussed previously.25,26
Diffusion Tensor Imaging (DTI)
A 3-T whole-body Siemens scanner (TrioTim Syngo) with a 12-channel, birdcage head coil was used for anatomical imaging and DTI. Anatomical images were acquired using a T1-weighted, three-dimensional (3D), magnetization-prepared, rapid gradient echo (3D MPRAGE) sequence (repetition time/echo time/inversion time/flip angle = 1670 ms/1.89 ms/900 ms/9°; slice thickness = 1.0 mm; in-plane resolution = 1×1 mm; field-of-view = 250 mm; matrix size = 256×256). DTI was performed in the axial plane using the following parameters: b = 0 and 900 s/mm,2 number of diffusion gradient directions = 30, repetition time = 12,000 ms, echo time = 82 ms, slice thickness = 2 mm, flip angle = 90°, and matrix size = 128×128.
Diffusion MRI Processing
Diffusion data files were analyzed using DSI Studio (http://dsi-studio.labsolver.org/). First, the DICOM files were converted to NIFTI files using MRIConverter (https://lcni.uoregon.edu/downloads/mriconvert); the NIFTI files were imported into DSI Studio. An automated mask was applied prior to rendering of the 3D DTI volumes. Diffusion data were reconstructed via q-space diffeomorphic reconstruction; this yielded individual fractional anisotropy (FA) maps aligned to the Montreal Neurological Institute space via non-linear registration. The FA file for each subject was based on the Human Connectome Project (HCP) 1065 template.26 Parcellation was performed using ICBM152 non-linear atlases.26 FA data were extracted to allow group connectometry analysis. Both connectometry and demographic datasets were prepared. Diffusion MRI connectometry27 was used to derive the correlational tractography (dti_fa) that correlated with shift work. A nonparametric, Spearman partial correlation was used for this purpose; the effects of age and sex were removed via multiple regression. In total, 92 participants were included in the analysis. In terms of the group connectometry, the T-score threshold was set to 2.5. The trajectories of the fiber pathways were determined using the deterministic fiber-tracking algorithm in DSI studio.28 This yielded correlational tractography data. No specific brain area was chosen as a seeding, end, or terminative region. Further, no specific brain area was chosen as a region of interest (ROI) or region of avoidance (ROA) in DSI studio. Thus, the whole brain was regarded as the seeding region and the ROI for correlational tractography. The tracks were filtered via topology-informed pruning (five iterations) to remove false connections.29 A length threshold of 20 voxels was used to select tracks. To estimate the false discovery rate (FDR), 8000 randomized permutations were applied to the group label to obtain the null distribution of the track length. For further analysis, mean FA values were extracted for regions that exhibited significant differences between the groups as revealed by group connectometry.
Statistical Analysis
To compare the demographic and clinical characteristics of the two groups, independent t-tests were used for continuous variables, while chi-squared tests were used for categorical variables. The Shapiro–Wilk test was performed to explore data normality. Variables that were not normally distributed were compared using the Mann–Whitney U-test. Partial correlation analyses and regression analyses were performed within each group to identify associations between the mean FAs of identified white matter and the clinical variables after adjusting for age and sex. An additional regression analysis was performed to explore how FA might be predicted by shift work status, sleep/circadian disturbances, and their interactions after controlling for age and sex. All statistical analyses were performed using R software (R Development Core Team, Vienna, Austria); p-values < 0.05 were considered to indicate statistical significance.
Results
Demographic, Clinical, Sleep, and Circadian Characteristics
The mean age did not significantly differ between shift workers (30.84 ± 6.37 years) and non-shift workers (32.74 ± 6.36 years; t = 1.36, p = 0.18); neither did the sex ratio (shift workers, 46 women, 75.41%; non-shift workers, 23 women, 74.19%; chi-squared = 28.03, p = 0.26) (Table 1). Among shift workers, the mean duration of such work was 65.05 ± 52.49 months (Table 1).
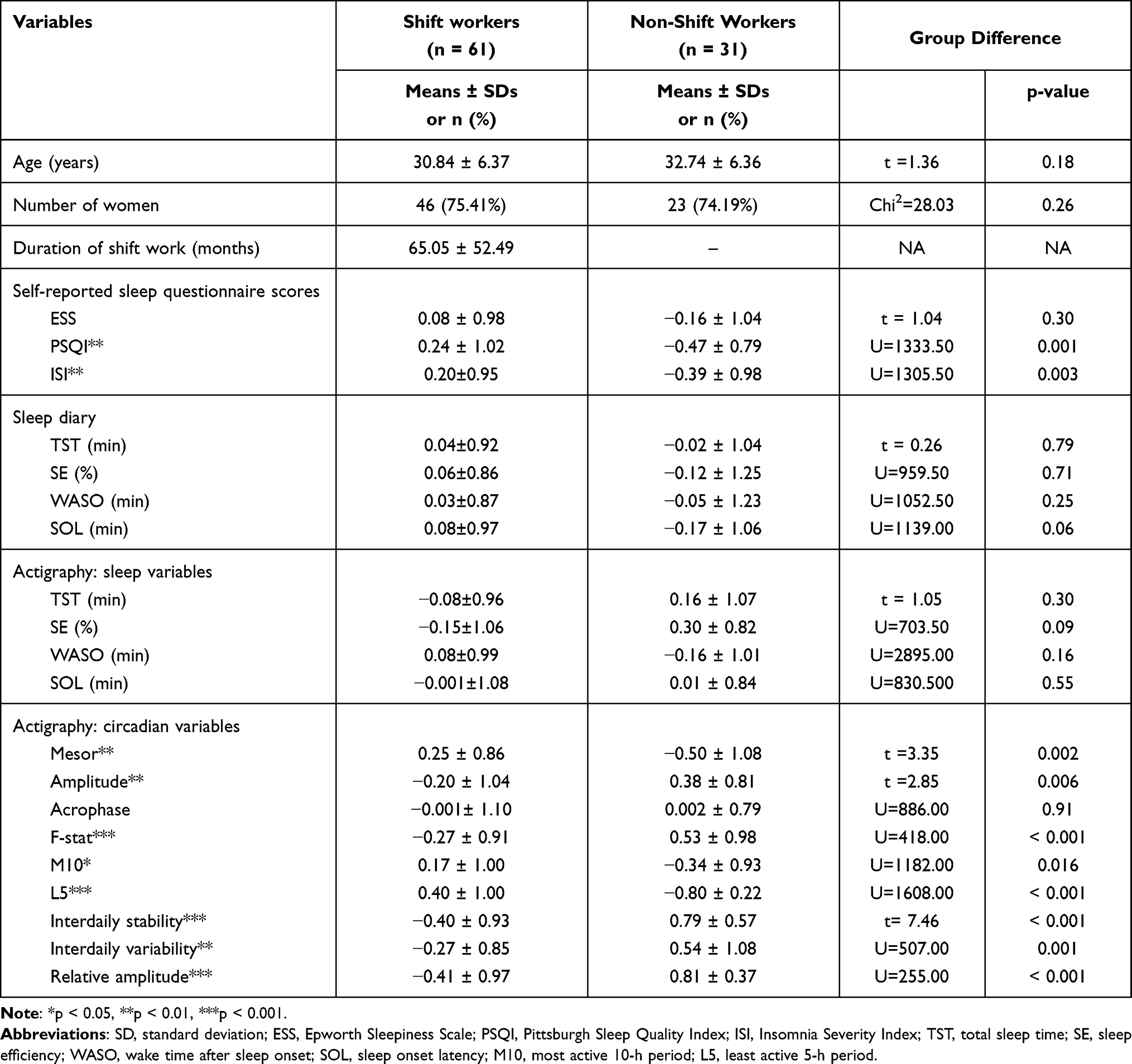 |
Table 1 Demographic, Clinical, Sleep, and Circadian Characteristics of All Participants |
The PSQI (w = 0.94 p < 0.01), ISI (w = 0.95, p = 0.002), actigraphic variables such as SOL (w = 0.87, p < 0.01), SE (w = 0.93, p < 0.01), WASO (w = 0.90, p < 0.01), acrophase (w = 0.85, p <0.01), F-statistic (w = 0.88, p < 0.01), M10 (w = 0.95, p = 0.001), L5 (w = 0.87, p < 0.01), relative amplitude (w = 0.90, p < 0.01), and IV (w = 0.97, p = 0.022) and sleep diary variables such as SE (w=0.97, p= 0.02), WASO (w=0.86, p<0.001), SOL (w=0.86, p<0.001) were not normally distributed.
Shift workers exhibited higher PSQI and ISI scores than did non-shift workers (U = 1,333.50, p = 0.001 and U = 1,305.50, p = 0.003, respectively). We found no significant difference in ESS scores between shift workers and non-shift workers. In terms of circadian variables, shift workers had a higher mesor (t = 3.35, p = 0.002), M10 (U = 1182.00, p = 0.016), and L5 (U = 1608.00, p < 0.01) than did non-shift workers; however, shift workers had a lower amplitude (t = 2.85, p = 0.006), F-statistic (U = 418.00, p < 0.001), IS (t = 7.46, p < 0.001), IV (U = 507.00, p = 0.001), and relative amplitude (U = 255.00, p < 0.01). Both subjective (sleep diary) and objective (actigraphic data) sleep variables did not differ between shift workers and non-shift workers.
Comparison of FA Between Shift Workers and Non-Shift Workers
Shift workers showed higher FA values in the right cingulum and left cingulum (right = 0.12 ± 1.00, left = 0.11 ± 0.93) than non-shift workers (right = –0.23 ± 0.97, left = –0.21±1.11). On whole brain analysis, shift workers exhibited higher FA values than did non-shift workers in the bilateral anterior cingulum after adjustment for age and sex (center x = 37, center y = 30, center z = 37, volume = 630 voxels, FDR = 0.004) (Figure 1).
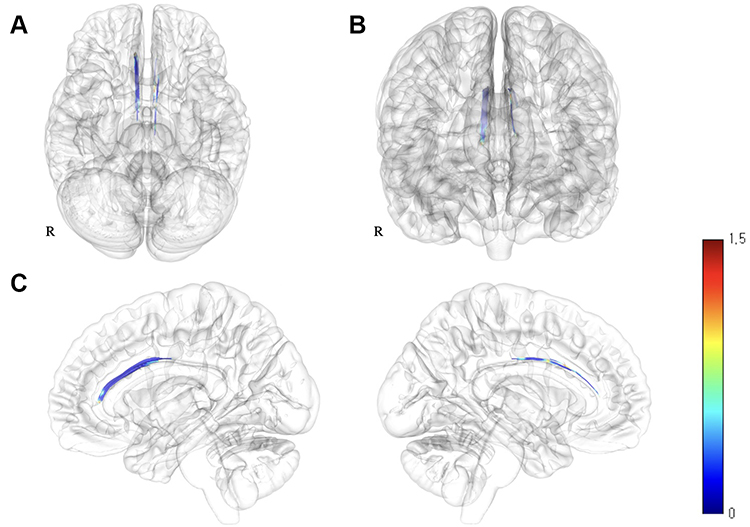 |
Figure 1 White matter images showing increased FAs in shift workers compared to non-shift workers. Brain regions showing increased FAs in shift workers (compared to non-shift workers) are shown in the (A) axial plane, (B) coronal plane, and (C) right and left sagittal planes. These areas correspond to the bilateral anterior cingula. Abbreviation: FA, fractional anisotropy. |
Associations Between FA and Sleep/Activity Variables
In shift workers, the mean FA of the right anterior cingulum was positively correlated with the PSQI score (r = 0.26, p = 0.04) (Figure 2). This correlation remained significant after adjustment for age and sex (r = 0.26, p = 0.04). After excluding one outlier with a high PSQI score and FA values of right cingulum, there was no significant correlation between the right cingulum PSQI score and shift worker status (r = 0.22, p = 0.10). The mean FA of the right anterior cingulum was not significantly correlated with the PSQI score of non-shift workers (Supplementary Tables 1 and 2). There was no significant correlation between left cingulum FA and the PSQI score (Supplementary Tables 1 and 2). No other subjective sleep variable (including the ISI) was significantly correlated with the mean FA of the right or left anterior cingulum (Supplementary Tables 1 and 2).
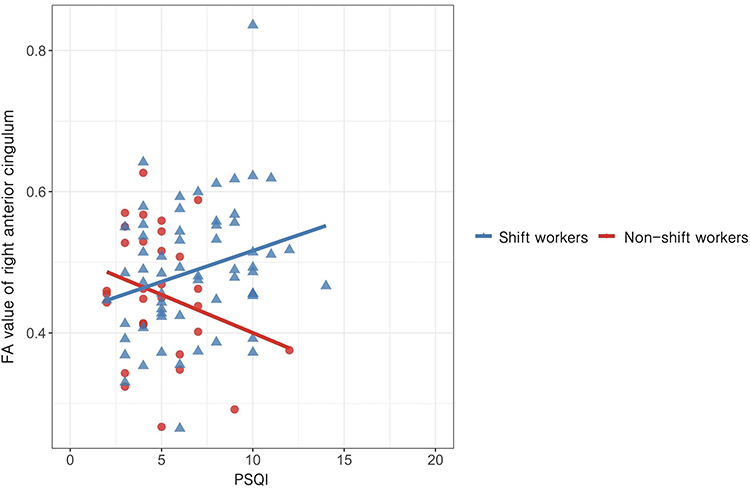 |
Figure 2 Correlations between the PSQI score and the mean FA of the right anterior cingulum in shift workers and non-shift workers. In shift workers, the mean FA of the right anterior cingulum was positively correlated with the PSQI score before (r = 0.26, p = 0.04) and after (r = 0.26, p = 0.04) adjustment for age and sex (blue). The mean FA of the right anterior cingulum was not significantly correlated with the PSQI score in non-shift workers (red). The FA value of the right cingulum was significantly predicted by the interaction between shift work status and PSQI score (β = 0.03, p= 0.03). Abbreviations: PSQI, Pittsburgh Sleep Quality Index; FA, fractional anisotropy. |
In shift workers, the mean FA of the right anterior cingulum was positively correlated with the mesor (r = 0.39, p = 0.002) and M10 (r = 0.33, p = 0.01). After adjustment for age and sex, the mean FA of the right anterior cingulum remained significantly correlated with the mesor (r = 0.39, p = 0.002) and M10 (r = 0.33, p = 0.01). Shift work duration did not significantly correlate with FA values of right cingulum (r = 0.20, p = 0.13) or left cingulum (r = –0.2, p = 0.87). In the regression model, higher FA values of right cingulum predicted a higher mesor (β = 0.40, p < 0.01), M10 (β = 0.34, p = 0.01), and PSQI score (β = 0.27, p = 0.045) in shift workers.
In non-shift workers, the mean FA of the left anterior cingulum was positively correlated with the mesor (r = 0.39, p = 0.03) and M10 (r = 0.44, p = 0.02). After adjustment for age and sex, the mean FA of the left anterior cingulum remained significantly correlated with the mesor (r = 0.49, p = 0.008) and M10 (r = 0.54, p = 0.003). No other actigraphic variable was significantly correlated with the mean FA of the right or left anterior cingulum. In the regression model, higher FA values of the right cingulum predicted amplitude in non-shift workers (β = 0.46, p = 0.02).
In terms of interaction, the FA value of the right cingulum was significantly predicted by the interaction between shift work status and the PSQI score (β = 0.03, p = 0.03), and by the interaction between shift work status and the ISI score (β = 0.37, p = 0.04), indicating that the associations between the FA value of the right cingulum and the PSQI or ISI score was more prominent in shift workers than non-shift workers. The FA value of the left cingulum was significantly predicted by the mesor (β = 0.48, p < 0.01) and M10 (β = 0.61, p < 0.01). In addition, amplitude (β = –0.45, p = 0.04), M10 (β = –0.45, p = 0.02), and L5 (β = –1.52, p = 0.04) exhibited significant interactions with shift work in terms of predicting the FA value of the left cingulum. The associations between the left cingulum FA value, and the amplitude, M10, and L5 were more prominent in non-shift workers than shift workers. The results of our regression analysis remained significant after excluding one outlier with a high FA value of right cingulum.
Discussion
We found differences in the white matter integrities of shift workers and non-shift workers. Specifically, shift workers exhibited higher FAs of the bilateral anterior cingulum than did non-shift workers. Additionally, a higher FA in the right anterior cingulum was associated with poorer subjective sleep quality and higher objective activity in shift workers.
In terms of sleep variables, shift workers exhibited higher PSQI and ISI scores than did non-shift workers. Thus, shift workers experience sleep disturbances and severe insomnia. In terms of circadian variables, although shift workers exhibited higher levels of activity (a higher mesor and M10), they experienced less restful sleep (a higher L5). Additionally, they exhibited less robust circadian rhythms (a lower relative amplitude) and more circadian misalignment (a lower IS) compared to non-shift workers. Shift workers often complain of insomnia and disrupted circadian rhythms;1,30 our study participants were thus typical.
Consistent with our hypothesis, white matter integrity differed between shift workers and non-shift workers. We found a significantly increased FA in the bilateral anterior cingulum of shift workers compared to non-shift workers. Previous studies suggested that structural alterations in the cingulum were associated with sleep disturbances and insomnia.14,31 We speculate that structural changes in the cingulum caused by shift work induce sleep disturbances. Additionally, the anterior cingulum has been suggested to participate in cognitive and memory functions32 as well as emotional processing (as a component of the Papez circuit).33 Shift workers are thus vulnerable to cognitive impairment and poor mental health.34,35 The altered white matter integrity of the anterior cingulum suggests that this cingulum may regulate sleep and the effects of sleep on cognition, memory, and emotion in shift workers.
In the present study, interactions were apparent between shift work and sleep/activity, and the white matter integrity of the anterior cingulum. The associations between sleep disturbances and cingulum integrity were “more” prominent in shift workers, whereas the associations between activity and cingulum integrity were “less” prominent in shift workers. Moreover, a higher FA of the right anterior cingulum was associated with poorer sleep quality in shift workers, whereas poor sleep quality correlated with decreased white matter integrity of the right anterior cingulum in non-shift workers. Thus, the association between the cingulum and sleep may differ in shift and non-shift workers, perhaps because shift workers experience poorer sleep quality and more severe insomnia than do non-shift workers. Higher white matter integrity in the cingulum has been associated with poor sleep quality in insomniacs.14 Another possible explanation for the increased FA in shift workers (and the association thereof with sleep quality) is a circadian adaptation to shift work, which would be absent in non-shift workers. Functional changes in the cingulum were associated with recovery from jetlag, which can be interpreted as re-alignment after circadian disruption.9 However, it remains unclear why the increased FA correlated with poor sleep quality in shift workers but not in non-shift workers. A future study featuring long-term longitudinal imaging is required.
We found that shift workers exhibited higher levels of activity and increased white matter integrity of the bilateral cingulum. Moreover, shift workers with higher activity levels exhibited increased FA of the right anterior cingulum. Previous studies reported associations between cingulum features and physical activity. Increased white matter integrity of the anterior cingulum was associated with higher activity levels.36–38 The higher levels of activity in shift workers may explain the increased white matter integrity of the anterior cingulum.
Our work has certain implications. The white matter tract changes of anterior cingulum in shift workers correlated with the sleep-activity cycle. This suggests that the change may serve as a biomarker of sleep disorders. Also, the work suggests that the ACC and connected areas could be the targets of neuro-modulation therapy for the sleep disorders of shift workers.
Our study had several limitations. First, as we employed a cross-sectional design, causal relationships cannot be determined. A longitudinal analysis is required to identify causal relationships; this also avoids recall bias. Second, we used sleep diaries and actigraphy to measure sleep variables. The PSQI may not be ideal to assess shift workers with disturbed sleep-wake rhythms; the PSQI is designed to assess (principally) subjective sleep quality. In the current study, the objective sleep-wake rhythm was measured by actigraphy. However, compared to polysomnography, actigraphy is less specific.39 Polysomnographic sleep parameters may be more reliable. Third, selection bias may have been in play when exploring the effects of shift work. As work shifts are chosen by workers, the baseline characteristics of shift workers may differ from those of non-shift workers. Those who regard themselves as tolerant of circadian disturbances may be less reluctant to choose night shifts. Lastly, we were unable to control for all potential confounders that may cause sleep disturbances (caffeine, alcohol, chronic pain, asthma, and heart disease). Although the FDR was used to correct the multiple comparisons of the imaging analysis, multiple comparison issues may still be in play. As shift workers may consume more caffeine or have more diseases than others, these confounders could affect the results.
In conclusion, we found that shift workers exhibited increased FAs in the bilateral anterior cingulum. The increased FA in the right anterior cingulum was associated with poorer sleep quality and higher activity levels. These results suggest that the right anterior cingulum may be correlated with sleep/activity in shift workers.
Acknowledgments
This research was supported by the Brain Research Program through the National Research Foundation of Korea, funded by the Ministry of Science, ICT and Future Planning (No. 2016R1A2B4011561; No. 2020M3E5D9080561), and the grant of the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (No. HR21C0885).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Potter GDM, Wood TR. The future of shift work: circadian biology meets personalised medicine and behavioural science. Front Nutr. 2020;7:116. doi:10.3389/fnut.2020.00116
2. James SM, Honn KA, Gaddameedhi S, Van Dongen HPA. Shift work: disrupted circadian rhythms and sleep-implications for health and well-being. Curr Sleep Med Rep. 2017;3(2):104–112. doi:10.1007/s40675-017-0071-6
3. Pallesen S, Bjorvatn B, Waage S, Harris A, Sagoe D. Prevalence of shift work disorder: a systematic review and meta-analysis. Front Psychol. 2021;12:638252. doi:10.3389/fpsyg.2021.638252
4. Torquati L, Mielke GI, Brown WJ, Burton NW, Kolbe-Alexander TL. Shift work and poor mental health: a meta-analysis of longitudinal studies. Am J Public Health. 2019;109(11):e13–e20. doi:10.2105/AJPH.2019.305278
5. Kim JB, Kim JH. Regional gray matter changes in shift workers: a voxel-based morphometry study. Sleep Med. 2017;30:185–188. doi:10.1016/j.sleep.2016.10.013
6. Marti AR, Patil S, Mrdalj J, et al. No escaping the rat race: simulated night shift work alters the time-of-day variation in BMAL1 translational activity in the prefrontal cortex. Front Neural Circuits. 2017;11:70. doi:10.3389/fncir.2017.00070
7. Marti AR, Pedersen TT, Wisor JP, et al. Cognitive function and brain plasticity in a rat model of shift work: role of daily rhythms, sleep and glucocorticoids. Sci Rep. 2020;10(1):13141. doi:10.1038/s41598-020-69969-x
8. Park YK, Kim JH, Choi SJ, Kim ST, Joo EY. Altered regional cerebral blood flow associated with mood and sleep in shift workers: cerebral perfusion magnetic resonance imaging study. J Clin Neurol. 2019;15(4):438–447. doi:10.3988/jcn.2019.15.4.438
9. Zhang F, Yang Z, Qin K, et al. Effect of jet lag on brain white matter functional connectivity. Psychoradiology. 2021;1(2):55–65. doi:10.1093/psyrad/kkaa003
10. Khalsa S, Hale JR, Goldstone A, et al. Habitual sleep durations and subjective sleep quality predict white matter differences in the human brain. Neurobiol Sleep Circadian Rhythms. 2017;3:17–25. doi:10.1016/j.nbscr.2017.03.001
11. Bai Y, Zhang L, Liu C, Cui X, Li D, Yin H. Association of white matter volume with sleep quality: a voxel-based morphometry study. Brain Imaging Behav. 2021. doi:10.1007/s11682-021-00569-7
12. Sexton CE, Zsoldos E, Filippini N, et al. Associations between self-reported sleep quality and white matter in community-dwelling older adults: a prospective cohort study. Hum Brain Mapp. 2017;38(11):5465–5473. doi:10.1002/hbm.23739
13. Chen L, Shao Z, Xu Y, et al. Disrupted frontostriatal connectivity in primary insomnia: a DTI study. Brain Imaging Behav. 2021;15(5):2524–2531. doi:10.1007/s11682-021-00454-3
14. Rostampour M, Gharaylou Z, Rostampour N, et al. Asymmetric alterations of white matter integrity in patients with insomnia disorder. Brain Imaging Behav. 2021;16(1):389–396. doi:10.1007/s11682-021-00512-w
15. Roskoden FC, Krüger J, Vogt LJ, et al. Physical activity, energy expenditure, nutritional habits, quality of sleep and stress levels in shift-working health care personnel. PLoS One. 2017;12(1):e0169983. doi:10.1371/journal.pone.0169983
16. Loef B, Hulsegge G, GCW Wendel-Vos, et al. Non-occupational physical activity levels of shift workers compared with non-shift workers. Occup Environ Med. 2017;74(5):328–335. doi:10.1136/oemed-2016-103878
17. Rodriguez-Ayllon M, Derks IPM, van den Dries MA, et al. Associations of physical activity and screen time with white matter microstructure in children from the general population. Neuroimage. 2020;205:116258. doi:10.1016/j.neuroimage.2019.116258
18. Wu X, Bai F, Wang Y, et al. Circadian rhythm disorders and corresponding functional brain abnormalities in young female nurses: a preliminary study. Front Neurol. 2021;12:664610. doi:10.3389/fneur.2021.664610
19. Kyeong S, Choi SH, Eun Shin J, et al. Functional connectivity of the circadian clock and neural substrates of sleep-wake disturbance in delirium. Psychiatry Res Neuroimaging. 2017;264:10–12. doi:10.1016/j.pscychresns.2017.03.017
20. Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. doi:10.1016/0165-1781(89)90047-4
21. Johns MW. A new method for measuring daytime sleepiness: the Epworth sleepiness scale. Sleep. 1991;14(6):540–545. doi:10.1093/sleep/14.6.540
22. Morin CM, Belleville G, Bélanger L, Ivers H. The Insomnia Severity Index: psychometric indicators to detect insomnia cases and evaluate treatment response. Sleep. 2011;34(5):601–608. doi:10.1093/sleep/34.5.601
23. Ancoli-Israel S, Cole R, Alessi C, Chambers M, Moorcroft W, Pollak CP. The role of actigraphy in the study of sleep and circadian rhythms. Sleep. 2003;26(3):342–392. doi:10.1093/sleep/26.3.342
24. Cespedes Feliciano EM, Quante M, Weng J, et al. Actigraphy-derived daily rest-activity patterns and body mass index in community-dwelling adults. Sleep. 2017;40(12):12. doi:10.1093/sleep/zsx168
25. Hwang JY, Byun MS, Choe YM, et al. Moderating effect of APOE ε4 on the relationship between sleep-wake cycle and brain β-amyloid. Neurology. 2018;90(13):e1167–e1173. doi:10.1212/WNL.0000000000005193
26. Yeh FC, Panesar S, Fernandes D, et al. Population-averaged atlas of the macroscale human structural connectome and its network topology. NeuroImage. 2018;178:57–68. doi:10.1016/j.neuroimage.2018.05.027
27. Yeh FC, Badre D, Verstynen T. Connectometry: a statistical approach harnessing the analytical potential of the local connectome. Neuroimage. 2016;125:162–171. doi:10.1016/j.neuroimage.2015.10.053
28. Yeh FC, Verstynen TD, Wang Y, Fernández-Miranda JC, Tseng WYI. Deterministic diffusion fiber tracking improved by quantitative anisotropy. PLoS One. 2013;8(11):e80713. doi:10.1371/journal.pone.0080713
29. Yeh FC, Panesar S, Barrios J, et al. Automatic removal of false connections in diffusion MRI tractography using Topology-Informed Pruning (TIP). Neurotherapeutics. 2019;16(1):52–58. doi:10.1007/s13311-018-0663-y
30. Drake CL, Roehrs T, Richardson G, Walsh JK, Roth T. Shift work sleep disorder: prevalence and consequences beyond that of symptomatic day workers. Sleep. 2004;27(8):1453–1462. doi:10.1093/sleep/27.8.1453
31. Kocevska D, Tiemeier H, Lysen TS, et al. The prospective association of objectively measured sleep and cerebral white matter microstructure in middle-aged and older persons. Sleep. 2019;42(10):zsz140. doi:10.1093/sleep/zsz140
32. Bubb EJ, Metzler-Baddeley C, Aggleton JP. The cingulum bundle: anatomy, function, and dysfunction. Neurosci Biobehav Rev. 2018;92:104–127. doi:10.1016/j.neubiorev.2018.05.008
33. Maldonado IL, Parente de Matos V, Castro Cuesta TA, Herbet G, Destrieux C. The human cingulum: from the limbic tract to the connectionist paradigm. Neuropsychologia. 2020;144:107487. doi:10.1016/j.neuropsychologia.2020.107487
34. Guarnieri B, Sorbi S. Sleep and cognitive decline: a strong bidirectional relationship. It is time for specific recommendations on routine assessment and the management of sleep disorders in patients with mild cognitive impairment and dementia. Eur Neurol. 2015;74(1–2):43–48. doi:10.1159/000434629
35. Göder R, Nissen C, Rasch B. Schlaf, Lernen und Gedächtnis: Relevanz für Psychiatrie und Psychotherapie. [Sleep, learning and memory: relevance for psychiatry and psychotherapy]. Nervenarzt. 2014;85(1):50–56. [German]. doi:10.1007/s00115-013-3894-5
36. Bracht T, Jones DK, Bells S, Walther S, Drakesmith M, Linden D. Myelination of the right parahippocampal cingulum is associated with physical activity in young healthy adults. Brain Struct Funct. 2016;221(9):4537–4548. doi:10.1007/s00429-016-1183-3
37. Marks BL, Katz LM, Styner M, Smith JK. Aerobic fitness and obesity: relationship to cerebral white matter integrity in the brain of active and sedentary older adults. Br J Sports Med. 2011;45(15):1208–1215. doi:10.1136/bjsm.2009.068114
38. Bashir S, Al-Sultan F, Jamea AA, et al. Physical exercise keeps the brain connected by increasing white matter integrity in healthy controls. Medicine. 2021;100(35):e27015. doi:10.1097/MD.0000000000027015
39. Marino M, Li Y, Rueschman MN, et al. Measuring sleep: accuracy, sensitivity, and specificity of wrist actigraphy compared to polysomnography. Sleep. 2013;36(11):1747–1755. doi:10.5665/sleep.3142
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.