Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Evaluation of Young Adults’ Physical Activity Status and Perceived Barriers in the Riyadh Region of Saudi Arabia
Authors Bashatah A, Qadhi OA, Al Sadoun A, Syed W ![]() , Al-Rawi MBA
, Al-Rawi MBA
Received 22 November 2022
Accepted for publication 20 February 2023
Published 28 February 2023 Volume 2023:16 Pages 557—569
DOI https://doi.org/10.2147/JMDH.S397341
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Adel Bashatah,1 Omaimah A Qadhi,2 Ahmed Al Sadoun,2 Wajid Syed,3 Mahmood Basil A Al-Rawi4
1Department of Nursing and Administration College of Nursing, King Saud University, Riyadh, Saudi Arabia; 2Department of Medical-Surgical, College of Nursing, King Saud University, Riyadh, Saudi Arabia; 3Department of Clinical Pharmacy, College of Pharmacy, King Saud University, Riyadh, Saudi Arabia; 4Department of Optometry, College of Applied Medical Sciences, King Saud University, Riyadh, Saudi Arabia
Correspondence: Wajid Syed, Email [email protected]
Background: Physical activity (PA) is any prolonged movement produced by muscular tissues that cause the muscles to exert force. Despite its beneficial effect, it is frequently neglected by individuals. The present study aimed to determine the PA among young adults living in Saudi Arabia.
Methods: This cross-sectional study was conducted among Saudi adults living in the Riyadh region of Saudi Arabia from June to August 2022 through a self-administered online survey. Global Physical Activity Questionnaire was used to assess the PA among participants. The data were analyzed using statistical software SPSS v. 26.0 (SPSS Inc., Chicago, IL, USA).
Results: Among the surveyed adult males were the predominant 67.8% (n= 240). Most of them were young, aged between 24 to 34 years 62.4% (n=221), and 37.6% (n=133) of them were between 35 and 44 years old. The current findings reported that 63% (n=223) of the adults had PA on weekly basis. Walking 45.2% (n=160) followed by bodybuilding 12.7% (n=45) was the most common type of PA identified among adults. The barriers identified for not practicing PA were lack of time 46.9% (n=166). With regard to a sedentary lifestyle, it was reported that 9.55 (SD= 4.887) hours per day are spent sedentary or in a constant sitting. The adults gender (p=0.046) employment (p=0.0001) and educational status (p=0.0001) was significantly associated with the type of PA engaged. Although being a female were shown more sitting behavior than males (p< 0.047), similarly the nationality of the adults (6.67; SD=1.649) (p < 0.001), education (p=0.028) and monthly household income (p =0.024) were significantly associated with the overall mean sitting behavior.
Conclusion: The findings of this study confirmed that Saudi adults yet posing highly sedentary behavior and physical inactivity, despite knowing the harmful outcomes of inactivity. Thus educating individuals about the importance of PA is warranted.
Keywords: walking, running, playing, football, weightlifting, sitting, sedentary behavior
Introduction
Physical activity (PA) is any prolonged movement produced by our muscular tissues that cause the muscles to exert force. 1 PA involves everyday activities of various types and intensity tiers, as well as light, medium, and strong intensity.1,2 PA offers numerous benefits, including improved social skills, maintaining good health and healthy body weight, and improved sleep quality.2 PA can help reduce the risks of premature death, coronary heart disease, strokes, high blood pressure, a specific form of cancer, type 2 diabetes, osteoporosis, obesity, and weight problems, as well as improve mental health.3–6 According to the World Health Organization (WHO), to acquire health benefits, adults aged 18–64 years must accumulate at least 150 minutes of moderate to vigorous intensity PA per week and muscle-strengthening activity at least 2 days a week.1,7 According to literature PA can be divided into occupational, sporting, conditioning, domestic, and other activities.3–7
With regard to the country-wise PA status, the Netherlands has the most physically active people, spending over 12 hours a week exercising or participating in sports, followed by Germany and Romania.8 In 2021, 19.3% of adult Americans were physically active with an average of 5.61 hours per day spent.9 While studies indicated 29.7% of the prevalence of PA in Saudi adults.10 On the contrary, in the European region 23% of adults 18 and over were not physically active enough, with more women being physically inactive than men.11 In United States Centre for disease control and prevention (CDC) and state health departments conduct the Behavioral Risk Factor Surveillance System (BRFSS), an ongoing state-based survey involving telephone interviews, there was an overall predominance of 25.3% of physical inactivity.8 Similarly, 81% of adolescents 11–17 years of age were insufficiently active, with girls being more inactive than boys.11
A high prevalence of physical inactivity was found among adults in Saudi Arabia.12–14 For instance, a recent national wide survey reported 82.6% of adults were inactive physically,12 while another study by Al-Nozha et al found 96.1% of the prevalence of physical inactivity.13 Similarly Amin et al, reported 80% of Saudi adults are not achieving adequate levels of PA with beneficial health effects.14 Previous research has demonstrated that Saudi Arabian adults do not engage in enough PA to have a positive impact on their health.5,12–14 The regular practice of PA has a positive impact on seven of the ten most common chronic diseases.7,8 Despite the positive health benefits of the PA, 80% of American adults do not meet basic aerobic and muscle-strengthening activity guidelines, and only half meet the aerobic activity standard.16 Healthcare expenses related to the lack of PA amount to over $117 billion annually, and almost 10% of all deaths are premature.16
The reason for the lack of PA among adults was various according to studies and across countries.5,17 For example, American Heart Association reported a lack of time, a lack of motivation, a lack of resources, too much work, or frequent travel because of the job are the hurdles that prevent persons from engaging in PA.17 However, a comprehensive analysis found that people in Saudi Arabia find PA a challenging choice because of rising urbanization, congested traffic, inclement weather, cultural hurdles, a lack of social support, the absence of female school PA programs, and a lack of time and resources.5 Furthermore, increased age, and monthly income were other possible barriers to physical inactivity among adults and was correlated with PA.5 Furthermore women’s barriers to involvement are higher than men’s and rise with age.18 At the same time, environmental factors showed the strongest relationship with physical inactivity.18 Similarly another recent study among Spanish Adults during the COVID-19 Pandemic found a positive correlation between PA and an active coping style, with adults who were frequently active physically during the pandemic, predicting anxiety symptoms. Furthermore, research revealed that adults used exercise as a coping mechanism to manage emotional distress indicating the beneficial effects of exercise for the control of negative states like anxiety which signifies the importance of PA for the mental well-being of the population.19
In the Eastern Mediterranean Region (EMR), Saudi Arabia is one of the largest and wealthiest countries. In recent decades, it has experienced rapid socioeconomic development, along with shifts in population standards of living toward sedentary behavior and a high-calorie diet pattern.20 Modern technological progress has led to humans lowering the amount of PA that they need, unfortunately, this led to a scenario of major negative changes in lifestyle and contributed to an increase in lifestyle-related NCDs in the country.15,21–23 Saudi vision plan 2030 had come forth with a social-related approach. One of the aims of Saudi Vision 2030, is to promote the practice of sports activities in the community which emphasizes the importance of PA for at least 30 minutes per week. This initiative is an indicator of the Vision Program’s Quality of Life Program. This innovative concept of attention to better people’s quality of life is only now emerging in developed and less developed countries. To address this gap in the literature, the present study described PA status among young adults aged between 24 and 40 years residing in the capital city of KSA and examined the frequency of intensity of PA in their daily routine, and common barriers. Thus the findings of this study aimed at assessing the PA status among adults in the Riyadh region of Saudi Arabia.
Methods
Study Design, Setting, and Population
A cross-sectional study was carried out by young adults in Riyadh region, Saudi Arabia to assess and capture the PA status. It was a prospective self-reporting survey using an online questionnaire-based study conducted between June to August 2022. Our targeted population includes adults aged ≥18 years, both genders, able to understand Arabic, and willing to complete the survey. Others who do not match the inclusion criteria, and living in other regions of Saudi Arabia, mentally ill adults, or adults with psychological illness were excluded from the study. Respondent’s anonymity and confidentiality were ensured throughout the study. Furthermore, this study followed the guidelines of the Declaration of Helsinki, as well as appropriate safeguards regarding the rights and welfare of the human participants.24
Sample Size Estimation
According to previous reports, the prevalence of PA among Saudi adults was 29.7%.10 The sample size for the given study was calculated by using the following equation:

where n is the minimum sample size, z is the constant (1.96), p is the prevalence of PA (0.297%), q is (1 − p), Z is the standard normal deviation of 1.96 corresponding to the 95% confidence interval, and d is the desired degree of accuracy.
n = (1.96)2 ×0.297 (1−0.297)/ (0.05)2
n= 320
but we decided to survey 400 individuals in an attempt to ensure higher reliability. A total of 354 filled responses were obtained giving a response rate of 88.5%.
To capture the status of PA the questionnaire was adopted based on previous studies published in a similar context.12,25 The questionnaire was initially designed in the English language and later translated into the local Arabic language using forward and backward translation procedures. A prevalidated Global Physical Activity (GPA) Questionnaire developed by the world health organization consisted of a total of 16 items.25 The 16-item tool was further divided into four domains. Domain one focused on Activity at work with a total of six items, which includes work involving vigorous activity that significantly raises breathing or heart rate, such as carrying or lifting heavy loads, or work involving moderate activity that raises breathing or heart rate only slightly, such as brisk walking for at least 10 minutes continuously, spending time performing such activities. In addition to this, this domain also collected information weekly on how many days and how long you spend engaging in moderately intense activity.
However, domain two focused on traveling to and from locations (3 items), such as using a bicycle or walking, and how much time and the number of days was spent on these activities each week. Recreational activities consisted of 6-items which includes vigorous-intensity and moderate-intensity sports, fitness or recreational (leisure) activities playing games or running for at least 10 minutes, the number of days (In a week), and time (in a day) of doing such activity and the last domain focused on sedentary behavior with one item (How much time do you usually spend sitting or reclining on a typical day). All these questionnaires were assessed on the binary scale and continuous scale. Similarly, to previous studies,26–33 before beginning the study, the designed questionnaire was validated in two steps. First, the initial draft is evaluated by a research expert in the related field, to check the accuracy of the content and flow of the questionnaire. Secondly, a pilot study was conducted among a randomly selected sample of (n=30) individuals to give their opinions and also to know the feasibility of the study and also for pre-testing the questionnaire. Written informed consent was obtained from the undergraduate students. If any amendments from the pilot study are then unified into the final questionnaire. The reliability test was done by calculating Cronbach’s alpha using SPSS v.26, which was found to be 0.85. The data from the pilot study was not included in the final analysis.
The final questionnaire was then distributed using online survey tools. Google Form was created, and participants were invited through the social media applications such as WhatsApp, Twitter, and Facebook. Other methods to improve the response rate were considered such as Emails. An invitation link containing a survey questionnaire was sent to the participants. For the data collection, we used the snowball technique where any person recruited to do the survey provides multiple referrals.
Statistical Analysis
To summarize data on socio-demographic characteristics, descriptive statistical methods were used. For categorical variables, data were summarized as frequencies (n) and percentages (%). The continuous data were presented in the form of mean and standard deviations. Statistical Package for Social Sciences version 26.0 (SPSS Inc., Chicago, IL, USA) was used to analyze the data. To find out the significant association between the variables, the chi-square or Fisher exact test was used and a p-value of 0.05 was considered statistically significant.
Results
A total of 354 young adults completed the questionnaires giving a response rate of 88.5% (Figure 1). Among those males were the predominant participants (n= 240; 67.8%). Most of them were young, aged between 24 and 34 years (n=221;62.4), followed by 37.6% (n=133) of the adults between the age ranges of 35–44. years and were Saudi nationals (91.0%). More than half of the adults (57%) reported a monthly income of >7000 Saudi Riyals. More than half 63% of the adults had a university level of education while most of the adults were employed (41.2%) respectively. The demographic characteristics of the adults in the study sample are shown in Table 1
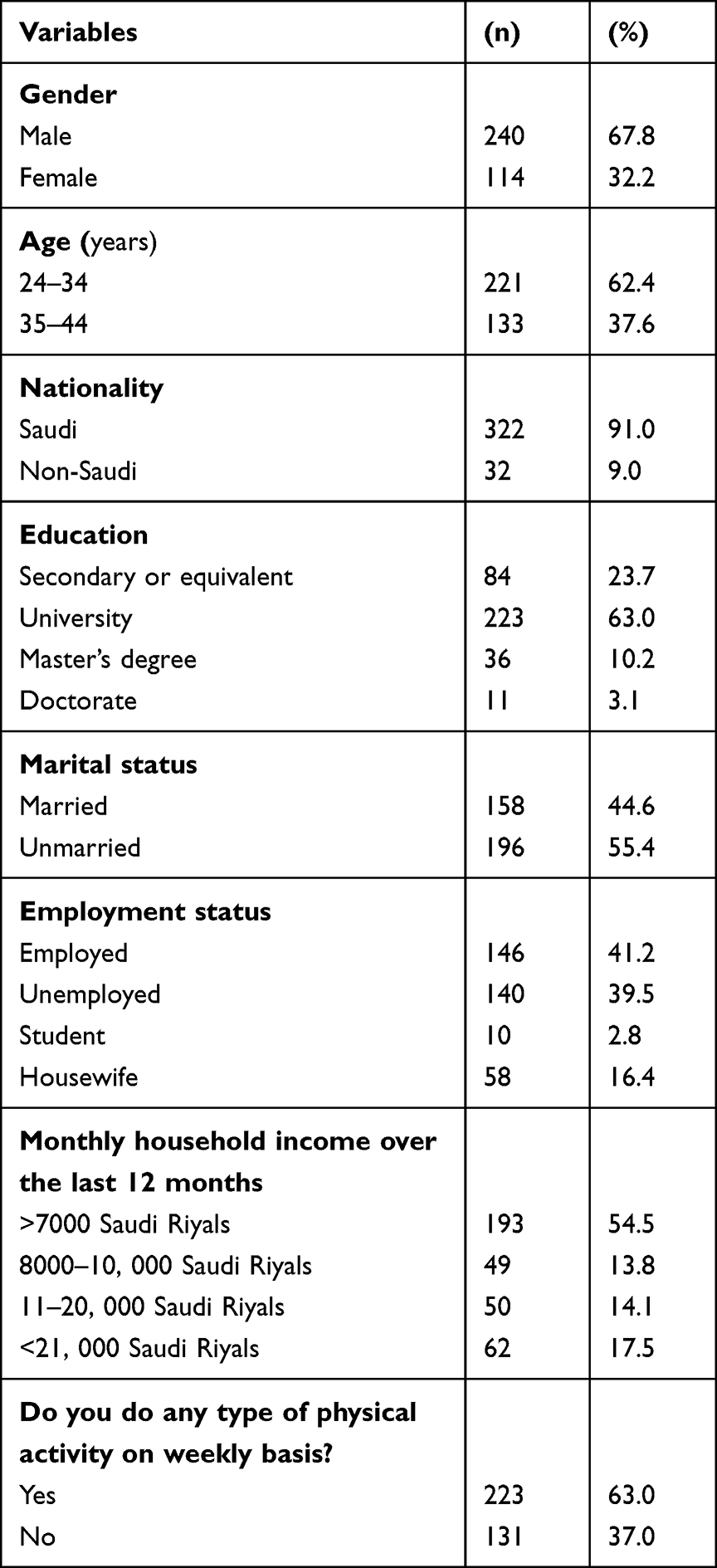 |
Table 1 Baseline Characteristics of the Participants (n = 354) |
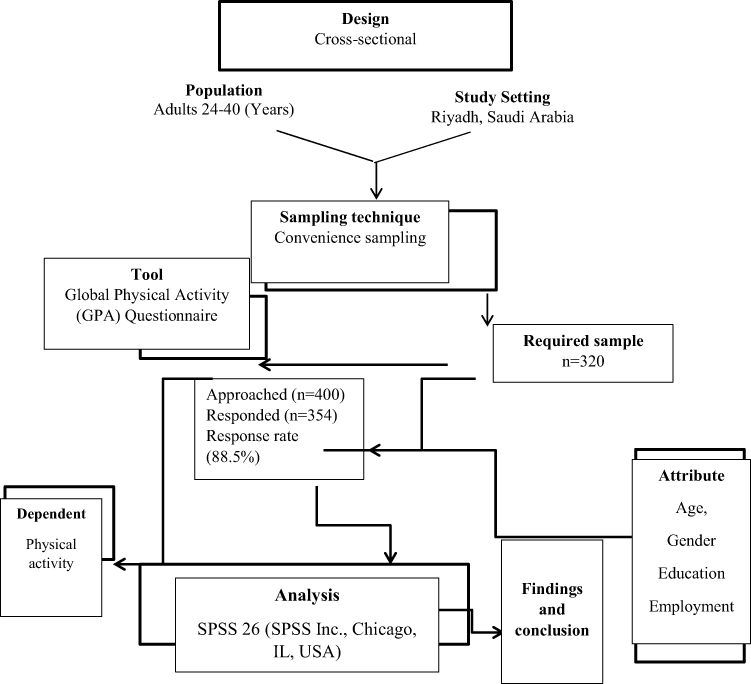 |
Figure 1 Flow chart of the study. |
The current findings reported that two third of the adults 63% (n=223) had PA on weekly basis, while 37.0% of them were do not do any PA. With regard to the most common type of PA was walking (n=160) at 45.2% followed by bodybuilding (n=45) at 12.7% and playing football or volleyball at 6.2%, running at 3.1% (n=11), swimming at 2.0% (n=7), cycling 3.7% (n=13) respectively (Figure 2).
 |
Figure 2 Most common types of physical activity. |
Among the adults, the most commonly identified barrier for not practicing PA was lack of time 46.9% (n=166), followed unwillingly to practice due to unknown reasons 17.8 (n=63), other reasons 30.8% (n=109) lack of facilities 2.3% (n=8) and injury 2.3% (n=8) (Figure 3).
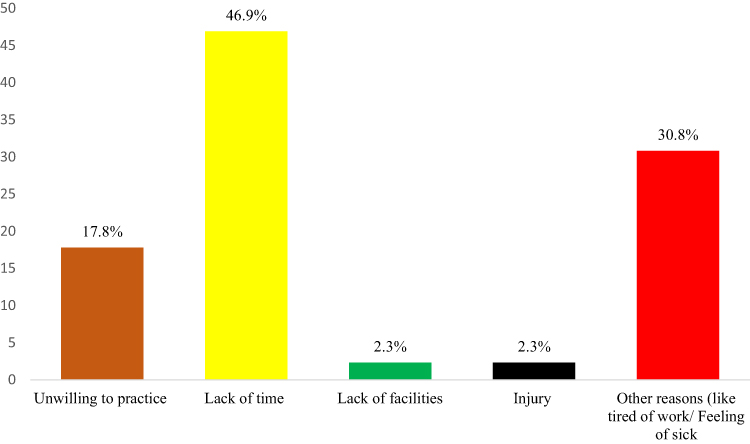 |
Figure 3 Barriers of physical activity among participants. |
Table 2 illustrates the time and characteristics of different types of PA in a typical week. In at least 10 minutes of work, only 23.2% (n=82) involved vigorous-intensity activity that caused high levels of breathing or heart rate (carrying or lifting heavy loads, digging, or construction work). In a typical week, 6.26 (1.569) were the average number of days’ adults spent active in vigorous intensity activities, while 5.11 hours (SD=0.907) (median= 5) were the average number of hours they spent active (Table 2).
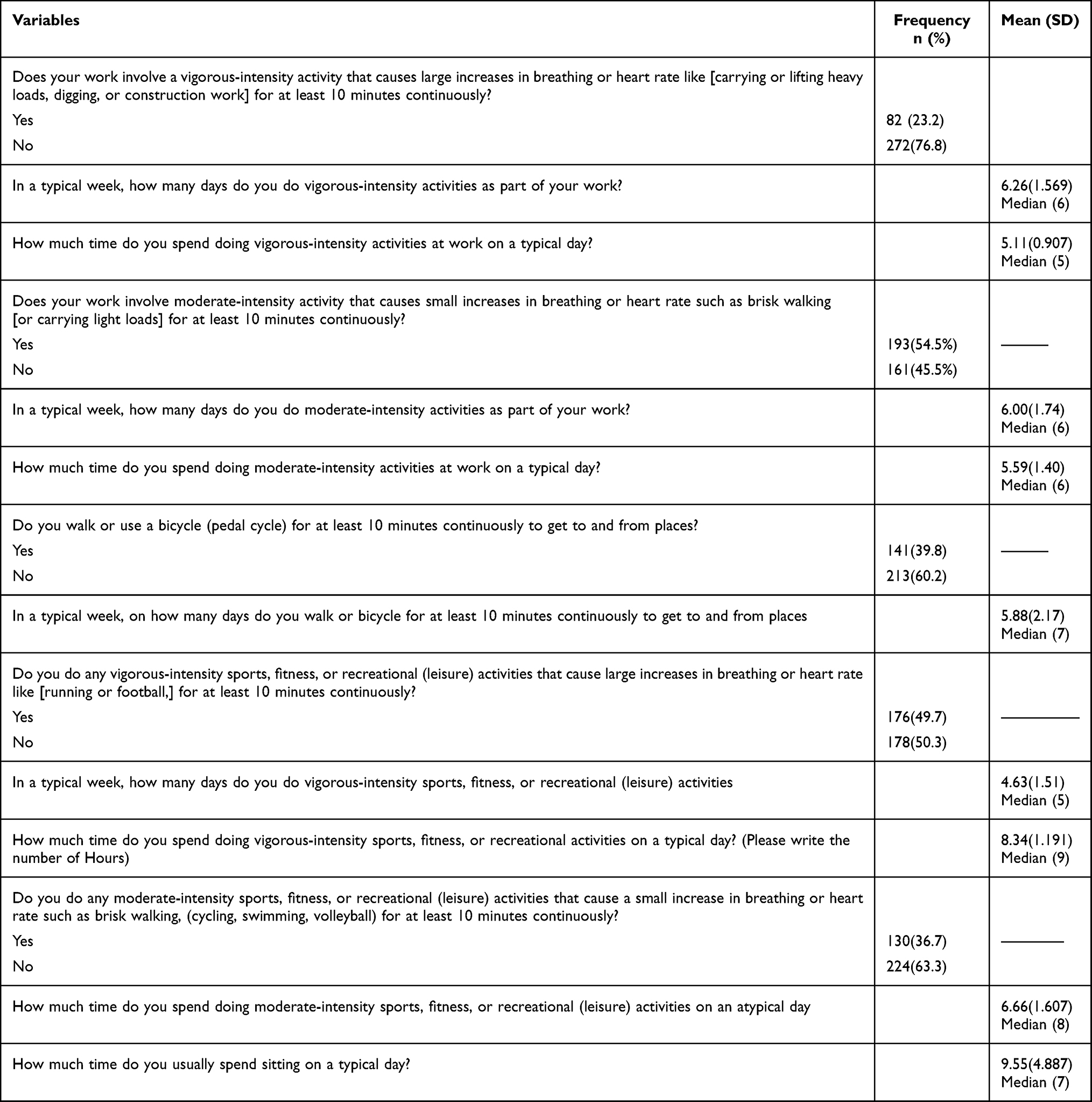 |
Table 2 Time and Characteristics of Different Types of PA in a Typical Week |
According to this study, on a typical workday, adults spend 5.11 hours (SD 0.907) doing vigorous-intensity activities. In contrast, 54.5% (n=193) of the adult’s work involves moderate-intensity activity that causes small increases in breathing or heart rate, such as brisk walking (or carrying light objectives). In terms of moderate-intensity activity, every week, adult’s spent an average of 6.00 days (SD=1.74), and 5.59 hours (SD1.40) were spent practicing moderate-intensity activity in a day. There were 39.8% (n=141) of adults who cycled their bicycles for at least 10 minutes to and from places. In terms of the number of days spent walking or cycling for 10 minutes continuously to get to and from places in a week, 5.88 were the average number of days (Table 2).
Moreover, 49.7% (n=176) of the adults performed vigorous-intensity sports, fitness, or recreational activities that cause large increases in breathing or heart rate like running or football for at least 10 minutes continuously. A mean of 4.63 hours (1.51) per day was devoted to vigorous-intensity sports and fitness activities by the adults in this study. Over one-third of 130 (36.7) of the adult’s work involves moderate-intensity sports, fitness, or recreational (leisure) activities that cause a small increase in breathing or heart rate such as brisk walking, (cycling, swimming, volleyball) for at least 10 minutes continuously. With regards to a sedentary lifestyle, it was reported that 9.55 (SD 4.887) hours per day are spent sedentary or in a constant sitting. The detailed responses of the patients were given in Table 2.
Our analysis revealed that 35.3% (n=125) of the adults engaged in vigorous-intensity activity twice a week, while 44 (12.4%) did so three times a week. About 27.4% (n=97) of the adults participated in moderate-intensity activities twice a week, and 116 (32.8%) participated in vigorous-intensity activities once a week. Detailed descriptions of the responses are shown in Table 3.
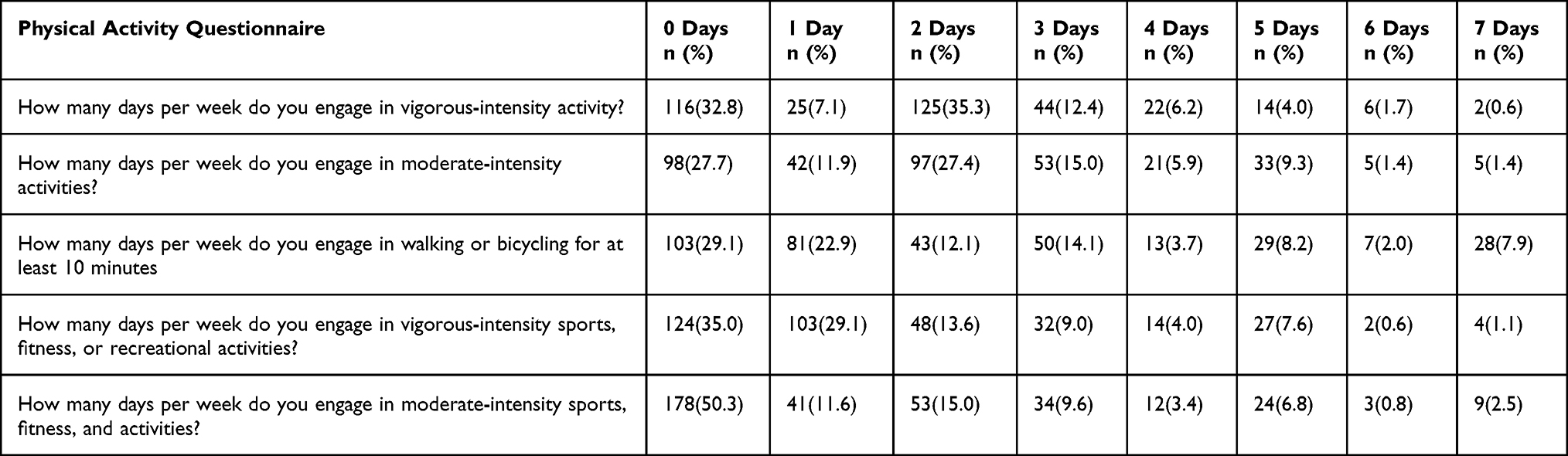 |
Table 3 Frequency of Participants in Engaging Physical Activity on Weekly Basis |
The most common physical activity and the demographic characteristics of the study participants were significantly associated. For example, gender was substantially associated with the type of physical activity engaged (p=0.046). The type of physical activity among adults was also associated with the participants’ employment (p=0.0001) and educational status (p=0.0001). The current findings reported that there was no association between the participants’ age, marital status, and the type of physical activity they engaged in during the study (see Table 4).
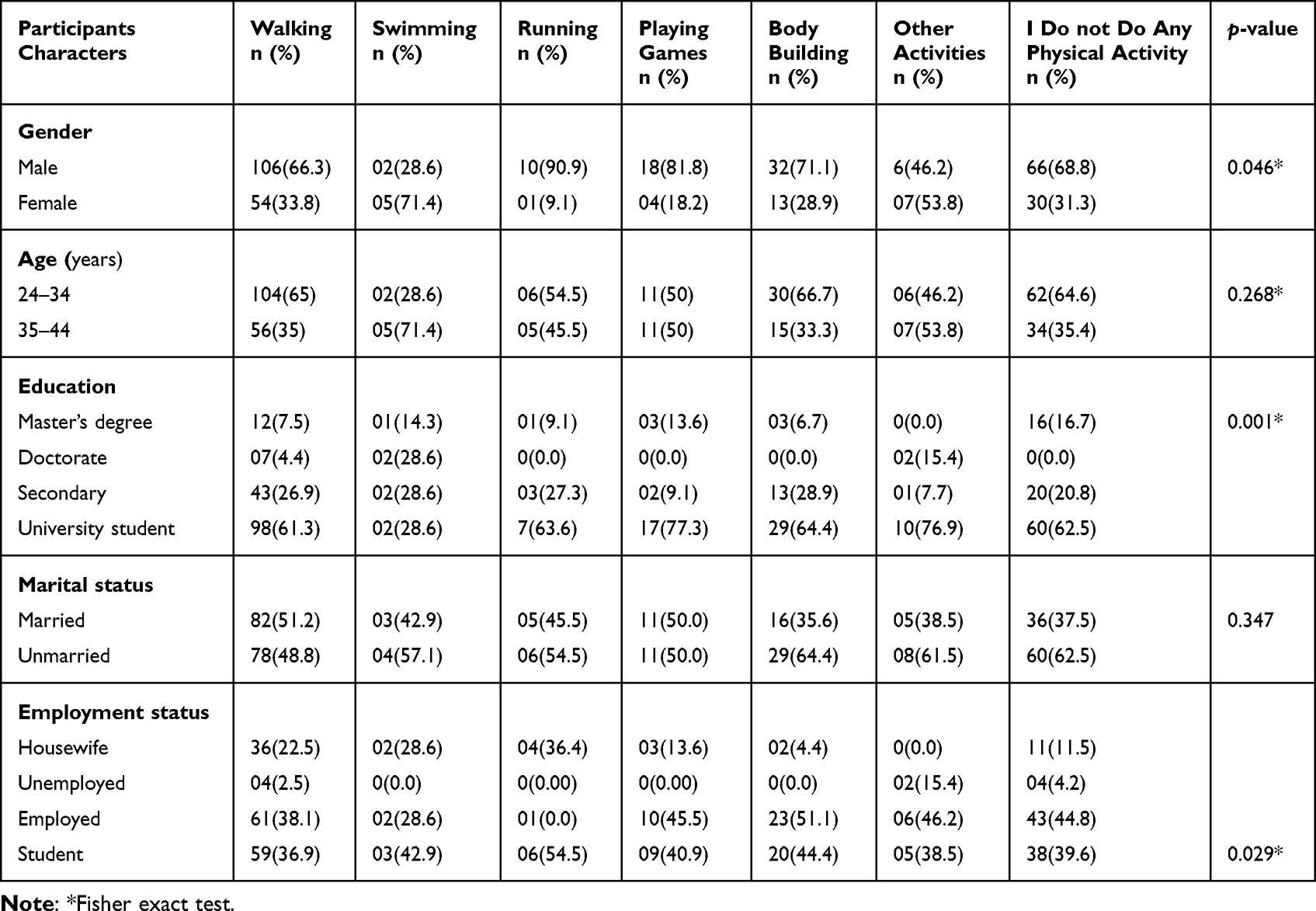 |
Table 4 Cross-Tabulation Between the Participant’s Demographic Characters and Type of Physical Activity Engaged |
Regarding the association between age, gender, nationality, and Physical activity status, we found that there was no significant effect on the Physical activity status of adults (p=0.05) concerning their demographics (Table 5). Although the overall mean sitting behavior among the adults was significantly associated with gender, where being a female were shown more sitting behavior than males (p<0.047). Similarly, the nationality of the adults, (where being a Saudi was shown more sitting behavior than non-Saudi) (6.67; SD=1.649) (p <0.001), education (p=0.028) and monthly household income (p =0.024) of the adults were significantly associated with mean sitting behavior of the adults. Detailed information Influence of adults ‘characteristics on their sitting behavior was given in Table 6.
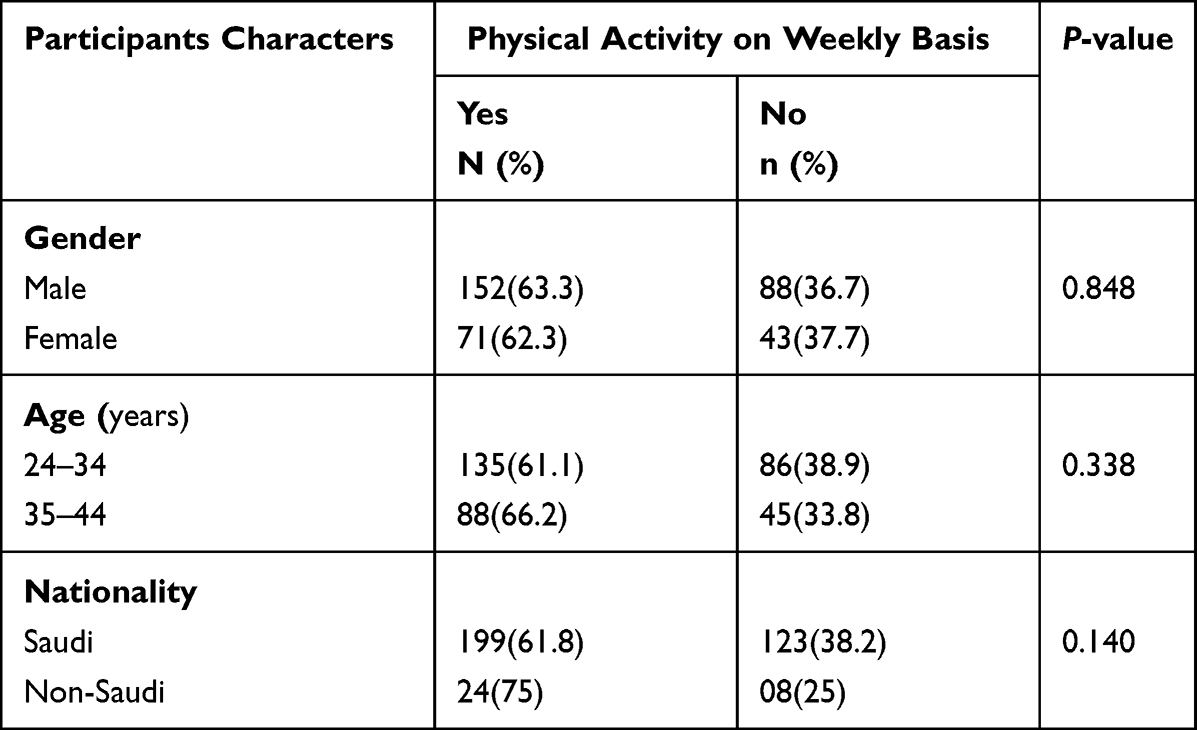 |
Table 5 Influence of Age, Gender and Nationality on Their Physical Activity Status |
 |
Table 6 Influence of Respondents’ Characteristics on Their Sitting Behavior |
Discussion
This study assesses PA among adults in Saudi Arabia using a cross-sectional survey. It was evidenced that PA has significant and positive various health outcomes. Although our study demonstrated that 63.6% of adult Saudis were physically active. These findings were better than earlier findings of Badar et al, 28.3% of the adults in Saudi Arabia and Mengesha in 54.9% of Ethiopia adults, and Al-Zalabani in the Saudi adults reported 33.4% were physically active.12,34,35 Thus the current findings evidenced that a considerable amount of adults in Riyadh were yet inactive. These findings were comparable to earlier national and international findings.12,34,35 The reason for the physical inactivity could be due to strict laws in the respective countries, such as Saudi Arabia, where women are not allowed to leave the country, or due to the country’s harsh climatic nature, such as high or low temperatures, and the occurrence of storms.
However, the current findings were still lower than those reported by Lau et al in 2021, who indicated that 83.3% of adults were physically active.36 On the other hand, a recent review of the assessment of PA prevalence in Arab countries revealed PA prevalence between 34.2 to 96.9% respectively.37 Similarly, another study in Armenia found that just 78.4% of participants were physically active.38 The variance in incidence and prevalence rates was due to differences in the instruments used to assess PA as well as the case definition for ‘physically active.37 Furthermore, adults who were physically active their entire lives were shown to be significantly less susceptible to the disease than those who lived a more sedentary lifestyle. Furthermore, physical inactivity is on the rise these days for a variety of causes, including the adoption of Western culture or unhealthy eating habits.
In this study, the most commonly practiced PA among adults was walking, followed by bodybuilding and playing football or volleyball. Similar results were reported in a recent study by Badar et al, who found 56% of individuals reported walking was the commonly practiced PA, followed by playing football and bodybuilding.12 This is because the preference for PA is mainly depending on comfort and availability as well as access ability, for instance, walking is a free easy exercise with little effort and benefits your physical as well as mental health. Most people consider walking as a simple and incredibly beneficial form of PA that is very accessible.
Although in this study work-related vigorous-intensity activity that causes large increases in breathing or heart rate was reported among 23.2% of the adults. Similarly, 54.5% of them agreed that their work involves moderate-intensity activity that causes small increases in breathing or heart rate such as brisk walking. These findings are following the preceding findings from Saudi Arabia and other developing countries.34,35 For instance, a population-based study found that 15.5% of the participants performed a vigorous-intensity activity that causes large increases in breathing.34 On the other hand, 56% of them performed, a moderate-intensity activity that causes small increases in breathing.34 Similarly the data from Saudi Arabia shows that 20.2% of the population was physically active at work side.35
Interestingly a majority of physically active adults also reported being sedentary with an average of 9.55 hours in a typical day, while Meyer et al in 2020, among American adults, reported similar findings where the author concluded that constant sitting of > 8 h/day, despite being physically active.39 Similarly, another study in Saudi Arabia reported a high prevalence of sedentary behavior.35 Sedentary behaviors are most widespread among adults as a result of inactivity during leisure time as well as sedentary conduct at work, home, or work from home and adopting technologies in transportation to reach on the time to their workplaces.
The results of the current study also showed that women are more likely than men to engage in sedentary activity. While these findings were opposed to previous findings in Saudi Arabia where the author found that PA was reported higher among females (21.9%) than males (18. 3%).35 In this study we did not find any significant association between age, gender, nationality, and Physical activity status, of adults. Although the overall mean sitting behavior among the adults was significantly associated with the nationality of the adults, education, and monthly household income. While another study found that college students, those who practice manual tasks, those who are single, and respondents from one-member families were significantly associated with doing physical activity.40 Being a foreigner tends to make a person more loyal at work than being a native since all ex-pats leave their country in search of employment opportunities, so they may work better. Women are constantly preoccupied with taking care of household duties and managing family-related activities in addition to their professional responsibilities, and some of the women in this study did not work for pay. The high rates of sedentary behavior among females and participants’ nationality may be attributed to these causes.
Furthermore, according to WHO, the majority of the world’s population (80%) is physically inactive, and one in every four persons globally does not meet the global recommendation levels of PA.1 Individuals should engage in at least 150 minutes of moderate-intensity PA or 75 minutes of vigorous-intensity PA per week. Although physical inactivity is a substantial public health issue connected with the development of numerous metabolic disorders. Furthermore, they discovered that insufficiently active persons had a 20% to 30% higher risk of death than sufficiently active people.1 Therefore, it was crucial to comprehend and motivate people to engage in physical activity because it has numerous positive effects on a human’s body. Even though it is the responsibility of today’s adults to educate and counsel the next generation about various health-related advice, doing so helps someone live a healthy life, and determining a person’s PA status would help them better achieve a healthy presence. Additionally, it is essential to provide teaching initiatives about PA through a variety of awareness-raising campaigns and poster displays. It can benefit adults’ knowledge and practice of PA to have such activities and standards present in Arabic culture.
This study has some limitations. First, the results were based on a self-completed questionnaire, which may have increased the possibility of biases such as social desirability bias or recall bias. Second, the results were derived from a single region in Saudi Arabia, third, the participation rate is considered low among the whole sample and extremely low from the total population of Riyadh region, which limited the generalizability of the results making them not-representative of others, and not generalizable globally. Fourthly, the study did not involve adults aged above 45 years and old as it was conducted in the young generation. Lastly, the data were collected using google forms, for this purpose one should have internet access, given this, lacking internet might be one of the reasons for the lower sample size or not reaching the survey in all young adults. Furthermore, it is purely descriptive and focuses on capturing the status of physical activity from various perspectives. Despite these limitations, such a report is critical in revealing such issues first, if excess inactivity exists, then further investigating their clinical impact and demonstrating strategies to fix them later. Our findings suggest more emphasis on increasing the awareness of youth towards the impotence of PA to make them more competent in raising awareness and posing a healthy lifestyle.
Conclusion
In conclusion, the majority of Saudi adults engaged in physical activity. Walking, bodybuilding, and playing football were the most often mentioned physical activities. Furthermore, despite being aware of the negative effects of inactivity, the individuals in this study continue to exhibit excessively sedentary behavior and physical inactivity. It is commonly recognized that both excessive sitting and inactivity harm one’s physical and mental health. Our research could aid in the investigation of the most practical methods for increasing adults’ awareness and knowledge about Physical activity. Educating and creating awareness about the importance of physical activity as well as the establishment of additional facilities like open parks, grounds and foot walk in their facilities where peoples live are all important things to take. Incorporating Physical activity into everyday practice will undoubtedly enhance health outcomes, reduce the incidence of various cardiovascular and other diseases, and have a favorable impact on an individual’s health in the future.
Institutional Review Board Statement
This study was approved by the ethics committee at the college of medicine King Saud University, Riyadh Saudi Arabia with the following Approval of the Research Project (E-22-7368). Although before the beginning of the study or questionnaires, there was a statement about the informed consent and confidentiality of the data, who agreed and proceed to the study were considered as informed consent (Verbal) and included in the study.
Acknowledgments
The authors of this study extend their appreciation to the Research Supporting Project, King Saud University, Riyadh, Saudi Arabia, for supporting this study (RSP-2023/378) and for funding this work.
Funding
The author(s) disclosed receipt of the following financial support for the research, and/or publication of this article. This study was supported by the Research Supporting Project, King Saud University, Riyadh, Saudi Arabia, (RSP-2023/378) which provided funding for this work.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. World health organization. Physical activity. Available from: https://www.who.int/news-room/fact-sheets/detail/physical-activity#:~:text=In%20high%2Dincome%20countries%2C%2026,or%20rising%20gross%20national%20product.
2. Joy V, Vincent J. The prevalence of physical activity among MBBS students in a medical college in Kerala. Public Health Rev Int J Public Health Res. 2020;7(4):28–34. doi:10.17511/ijphr.2020.i04.01
3. Rejali M, Mostajeran M, Ashrafi M. Assessment of physical activity in medical and public health students. J Educ Health Promot. 2013;2:2. doi:10.4103/2277-9531.106638
4. Janampa-Apaza A, Pérez-Mori T, Benites L, et al. Physical activity and sedentary behavior in medical students at a Peruvian public university. Medwave. 2021;21:5. doi:10.5867/medwave.2021.05.8210
5. Al-Hazzaa HM. Physical inactivity in Saudi Arabia revisited: a systematic review of inactivity prevalence and perceived barriers to active living. Int J Health Sci. 2018;12(6):50–64.
6. Banday AH, Want FA, Alris FF, Alrayes MF, Alenzi MJ. A cross-sectional study on the prevalence of physical activity among primary health care physicians in aljouf region of Saudi Arabia. Mater Sociomed. 2015;27(4):263–266. doi:10.5455/msm.2015.27.263-266
7. Centers for Disease control and prevention (CDC). Physical activity. Available from: https://www.cdc.gov/physicalactivity/basics/adults/index.
8. CDC. Centers for disease control and prevention. Behavioral risk factor surveillance system. Available from: https://www.cdc.gov/brfss/index.html.
9. Statista. Average amount of time spent on leisure and sports by U.S. civilian population from 2009 to 2021. Available from: https://www.statista.com/statistics/189498/daily-average-time-spent-on-sports-and-leisure-in-the-us/.
10. GASTAT. General Authority for Statistics (GASTAT). Available from: https://www.stats.gov.sa/en/news/431#:~:text=According%20to%20the%20publication%20results,20%25%20during%20the%20year%202019.
11. Centers for disease control and prevention. Physical activity. adult physical inactivity prevalence maps by race/ethnicity. Available from: https://www.cdc.gov/physicalactivity/data/inactivity-prevalence-maps/index.html.
12. Alqahtani BA, Alenazi AM, Alhowimel AS, Elnaggar RK. The descriptive pattern of physical activity in Saudi Arabia: analysis of national survey data. Int Health. 2021;13(3):232–239. doi:10.1093/inthealth/ihaa027
13. Al-Nozha MM, Al-Hazzaa HM, Arafah MR, et al. Prevalence of physical activity and inactivity among Saudis aged 30–70 years. A population-based cross-sectional study. Saudi Med J. 2007;28(4):559–568.
14. Amin TT, Al Khoudair AS, Al Harbi MA, Al Ali AR. Leisure time physical activity in Saudi Arabia: prevalence, pattern and determining factors. Asian Pac J Cancer Prev. 2012;13(1):351–360. doi:10.7314/APJCP.2012.13.1.351
15. Lee IM, Shiroma EJ, Lobelo F, Puska P, Blair SN, Katzmarzyk PT; Lancet Physical Activity Series Working Group. Effect of physical inactivity on major non-communicable diseases worldwide: an analysis of burden of disease and life expectancy. Lancet. 2012;380(9838):219–229. doi:10.1016/S0140-6736(12)61031-9
16. Piercy KL, Troiano RP, Ballard RM, et al. The physical activity guidelines for Americans. JAMA. 2018;320(19):2020–2028. doi:10.1001/jama.2018.14854
17. American Heart Association. Breaking down barriers to fitness. Available from: https://www.heart.org/en/healthy-living/fitness/getting-active/breaking-down-barriers-to-fitness.
18. Gülü M, Ayyıldız E. Effect of the COVID-19 pandemic on barriers to middle-aged adults’ participation in physical activity in Turkey: a cross-sectional study. J Mens Health. 2022;2022:1.
19. Lara R, Fernández-Daza M, Zabarain-Cogollo S, et al.Active coping and anxiety symptoms during the COVID-19 pandemic in Spanish adults. Int J Environ Res Public Health. 2021;18(16):8240. PMID: 34443989; PMCID: PMC8392463. doi:10.3390/ijerph18168240
20. World health organization regional office for Europe. Factsheet. Physical activity. Available from: https://www.euro.who.int/__data/assets/pdf_file/0005/288041/WHO-Fact-Sheet-PA-2015.pdf.
21. Almahmeed W, Arnaout MS, Chettaoui R, et al. Coronary artery disease in Africa and the Middle East. Ther Clin Risk Manag. 2012;8:65. doi:10.2147/TCRM.S26414
22. Rahim HF, Sibai A, Khader Y, et al. Non-communicable diseases in the Arab world. Lancet. 2014;383(9914):356–367. doi:10.1016/S0140-6736(13)62383-1
23. Majeed A, El-Sayed AA, Khoja T, Alshamsan R, Millett C, Rawaf S. Diabetes in the Middle-East and North Africa: an update. Diabetes Res Clin Pract. 2014;103(2):218–222. doi:10.1016/j.diabres.2013.11.008
24. Williams JR. The Declaration of Helsinki and public health. Bull World Health Organ. 2008;86:650–652. doi:10.2471/BLT.08.050955
25. Armstrong T, Bull F. Development of the world health organization global physical activity questionnaire (GPAQ). J Publ Health. 2006;14(2):66–70. doi:10.1007/s10389-006-0024-x
26. Samreen S, Siddiqui NA, Wajid S, Mothana RA, Almarfadi OM. Prevalence and use of dietary supplements among pharmacy students in Saudi Arabia. Risk Manag Healthc Policy. 2020;13:1523–1531. doi:10.2147/RMHP.S256656
27. Bashatah A, Wajid S. Knowledge and disposal practice of leftover and expired medicine: a cross-sectional study from nursing and pharmacy students’ perspectives. Int J Environ Res Public Health. 2020;17(6):2068. doi:10.3390/ijerph17062068
28. Wajid S, Samreen S, Alsaleh SS, et al. Assessing Clinical Knowledge and Practice towards COVID-19–A Cross Sectional Community Study. J Young Pharm. 2021;13(2):178. doi:10.5530/jyp.2021.13.36
29. Wajid S, Samreen S, Sales I, Bawazeer G, Mahmoud MA, Aljohani MA. What has changed in the behaviors of the public after the COVID-19 pandemic? A cross-sectional study from the Saudi community perspective. Front Public Health. 2022;10:723229. doi:10.3389/fpubh.2022.723229
30. Syed W, Alsadoun A, Bashatah AS, Al-Rawi MB, Siddiqui N. Assessment of the knowledge beliefs and associated factors among Saudi adults towards blood donation in Saudi Arabia. Hematology. 2022;27(1):412–419. doi:10.1080/16078454.2022.2026026
31. Syed W, Iqbal A, Siddiqui NA, Mothana RA, Noman O. Attitudes and associated demographic factors contributing towards the abuse of illicit drugs: a cross-sectional study from health care students in Saudi Arabia. Medicina. 2022;58(2):322. doi:10.3390/medicina58020322
32. Syed W, Samarkandi OA, Alsadoun A, Harbi MKA, Al-Rawi MBA. Evaluation of clinical knowledge and perceptions about the development of thyroid cancer-An observational study of healthcare undergraduates in Saudi Arabia. Front Public Health. 2022;10:912424. doi:10.3389/fpubh.2022.912424
33. Syed W, Samarkandi OA, Sadoun AA, Bashatah AS, Al-Rawi MB, Alharbi MK. Prevalence, beliefs, and the practice of the use of herbal and dietary supplements among adults in Saudi Arabia: an observational study. Inquiry. 2022;59:469580221102202. doi:10.1177/00469580221102202
34. Mengesha MM, Roba HS, Ayele BH, Beyene AS. Level of physical activity among urban adults and the socio-demographic correlates: a population-based cross-sectional study using the global physical activity questionnaire. BMC Public Health. 2019;19(1):1. doi:10.1186/s12889-019-7465-y
35. Al-Zalabani AH, Al-Hamdan NA, Saeed AA. The prevalence of physical activity and its socioeconomic correlates in Kingdom of Saudi Arabia: a cross-sectional population-based national survey. J Taibah Univ Sci. 2015;10(2):208–215. doi:10.1016/j.jtumed.2014.11.001
36. Lau JH, Nair A, Abdin E, et al. Prevalence and patterns of physical activity, sedentary behaviour, and their association with health-related quality of life within a multi-ethnic Asian population. BMC Public Health. 2021;21(1):1939. doi:10.1186/s12889-021-11902-6
37. Murtagh E, Shalash A, Martin R, Rmeileh NA. Measurement and prevalence of adult physical activity levels in Arab countries. Public Health. 2021;198:129–140. doi:10.1016/j.puhe.2021.07.010
38. Tcymbal A, Andreasyan D, Whiting S, Mikkelsen B, Rakovac I, Breda J. Prevalence of physical inactivity and sedentary behavior among adults in Armenia. Front Public Health. 2020;8:157. doi:10.3389/fpubh.2020.00157
39. Meyer J, Herring M, McDowell C, et al. Joint prevalence of physical activity and sitting time during COVID-19 among US adults in April 2020. Prev Med Rep. 2020;20:101256. doi:10.1016/j.pmedr.2020.101256
40. Puciato D. Sociodemographic associations of physical activity in people of working age. Int J Environ Res Public Health. 2019;16(12):2134. doi:10.3390/ijerph16122134
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.