")
Back to Journals » International Journal of Women's Health » Volume 12
Evaluation of Vulvovaginitis and Hygiene Habits of Women Attended in Primary Health Care Units of the Family
Authors Felix TC, Araújo LB , Röder DVDB , Pedroso RS
Received 31 August 2019
Accepted for publication 3 January 2020
Published 30 January 2020 Volume 2020:12 Pages 49—57
DOI https://doi.org/10.2147/IJWH.S229366
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Elie Al-Chaer
Thais Chimati Felix,1 Lúcio Borges de Araújo,2 Denise Von Dolinger de Brito Röder,1,3 Reginaldo dos Santos Pedroso1,4
1Postgraduate Program in Health Sciences, Medical School, Federal University of Uberlândia, Uberlândia, Minas Gerais, Brazil; 2Faculty of Mathematics, Federal University of Uberlândia, Uberlândia, Minas Gerais, Brazil; 3Institute of Biomedical Sciences, Federal University of Uberlândia, Uberlândia, Minas Gerais, Brazil; 4Technical Course in Clinical Analysis, Health Technical School, Federal University of Uberlândia, Uberlândia, Minas Gerais, Brazil
Correspondence: Thais Chimati Felix
Email [email protected]
Background: This study aims to investigate the occurrence of vulvovaginal infections, to describe and to relate the hygiene habits of women who were treated at the Units of Primary Attention to Family Health in a municipality in the interior of Brazil.
Methods: This was a cross-sectional study that was carried out in two Primary Health Care Units of the Family of Uberlândia, Minas Gerais, Brazil. The population sample consisted of 100 women who underwent gynecological consultation in the health units. Data were collected through interviews and by the analysis of medical records. Results were reported according to laboratory reports.
Results: The participants’ ages ranged from 18 to 45 years, with a median of 36 years. Thirty women (30%) presented alterations in the microbiota from a Pap smear, where bacterial vaginosis (diagnosed with Amsel criteria) was the predominant microorganism (83.3%). More than half of the women in the study who had vulvovaginitis wore cotton panties (70%, p = 0.651) and tight jeans/pants (83.3%, p = 0.010). The habit of depilating the genital area was reported by all the women, with the razor blade being the most commonly used tool (68%; p = 0.196).
Conclusion: Bacterial vaginosis was the most commonly reported infection in the cytological exams. Care with genitalia and genital hygiene habits may be associated with the occurrence of vulvovaginitis.
Keywords: genital infection, women’s health, bacterial vaginosis, vulvovaginal candidiasis, female genitalia, genital hygiene
Background
Vulvovaginitis (VV) is characterized as an inflammatory or infectious condition of the vulva and vaginal mucosa and accounts for about 70% of women’s complaints in gynecological consultations.1 Symptoms include pruritus, erythema, pain, vulvar abrasions, as well as changes in the color, odor or amount of vaginal discharge.2 Due to the discomfort in the well-being and negative interference in the quality of life for women, the occurrence of VV can be considered a public health problem.3
The etiological diagnosis of VV is made through anamnesis, which addresses the clinical history and information about sexual practices and behaviors, menstrual cycles, hygiene habits, medications in use, clinical gynecological examination, and sample collection for laboratory analysis.4 Approximately 90% of the women presenting clinical signs of VV are due to an infection by agents of the vaginal microbiota itself, which arises when there is an imbalance in the genital microenvironment. Bacterial vaginosis (BV), vulvovaginal candidiasis (VVC), and trichomoniasis are prevalent.5–7
BV is the most common genital tract infection among women of reproductive age, with a prevalence ranging from 10% to 50%.5 It is a polymicrobial syndrome, which results in a decrease in the concentration of Lactobacillus and in an increase of pathogenic bacteria. Lactobacillus received attention due to its protective and probiotic properties, besides being responsible for the production of lactic acid, and therefore, an acidic pH (<4.5).8,9 The infection is usually caused by more than one bacterial species, including Gardnerella vaginalis, and Mobiluncus, Bacteroides, Prevotella and Mycoplasma species.1
The investigation of intimate habits such as depilation, sexual practices, types of clothing, vaginal douching, sanitary napkins and adornments may guide health professionals as to the appropriate orientation to women to avoid physiological disorders or infections.10,11 Adherence to hygienic measures and life-style changes towards medical practice is in line with medicine and public health used in disease prevention.10–13
Since caring for genitalia and genital hygiene are routinized habits, and VV is frequent in gynecological consultations, this study was proposed to investigate the occurrence of vulvovaginal infections, to describe and relate the hygiene habits of women who were treated in two Units of Primary Attention to Family Health in a municipality of the interior of Brazil. These units carry out activities of prevention and health promotion in a population within the competence of primary care, becoming the main point of contact between people and health services.
Methods
This was a cross-sectional study conducted in two Primary Care Units for Family Health (PCU) in Uberlândia, Minas Gerais state, Brazil, between July 2017 and June 2018. The city of Uberlândia, located in the Southeast region of Brazil, is the second-most populous municipality in the state of Minas Gerais and the 12th most populous in the country. Uberlândia has an estimated population of 683,247 people, according to the Brazilian Institute of Geography and Statistics (IBGE) in 2018,14 is located 422 km from Brasilia, the capital of the country, and 537 km from Belo Horizonte, the state capital. As for the distribution of the population based on sex, women represent the highest percentage at 51.17% and the age group 20 to 24 years old has the highest percentage (9.9%) of the total population, according to the IBGE census in 2010.
This study was conducted in accordance with the Declaration of Helsinki and the ethical approval was granted by the Research Ethics Committee of the Federal University of Uberlândia under number 2173985/2017. Participation in the research was voluntary and written informed consent was obtained from all participants.
The two Units of Primary Attention to Family Health were selected in a random manner. After being chosen to participate in the survey, they were the first two units to accept the invitation, following previous telephone contact.
At the first PCU (PCU1), about 180 women were cared for year. In the second PCU (PCU2), about 240 patients were treated for gynecological examinations in the same period, and the population was considered for the sample calculations. To calculate the sample size, it was considered that the proportion of the population with VVC was 35%, and the proportion suggested for this study was 20%, at a significance level of 5% and a test power of 90%, the results for the calculated minimum sample size were 46 patients from PCU1 and 48 patients from PCU2. Thus, a sample size of 50 participants was adopted for each PCU, totaling 100 women.
The population sample studied consisted of women aged between 18 and 45 years who spontaneously sought the health units for gynecological consultation. Women unable to give samples of vaginal secretions because of menstruation, menopause, pregnancy, malignant neoplasm or conditions of clinical immunosuppression (HIV, syphilis, and lupus, among others), and that have been confirmed to have Human Papillomavirus (HPV) were not selected to participate in the study.
The data presented in this study were obtained through interviews with the participants, as well as by the analysis of their medical records. Individual interviews were carried out including sociodemographic data (age, race, employment outside home, practice of physical activity, among others – Table 1), genital hygiene habits and behaviors (Table 2). Medical records were analyzed for clinical data and laboratory test results (Papanicolaou´s test). Vulvovaginitis diagnosis was based on clinical data and cytopathological reports. Bacterial vaginosis was diagnosed using the Amsel criteria.15,16
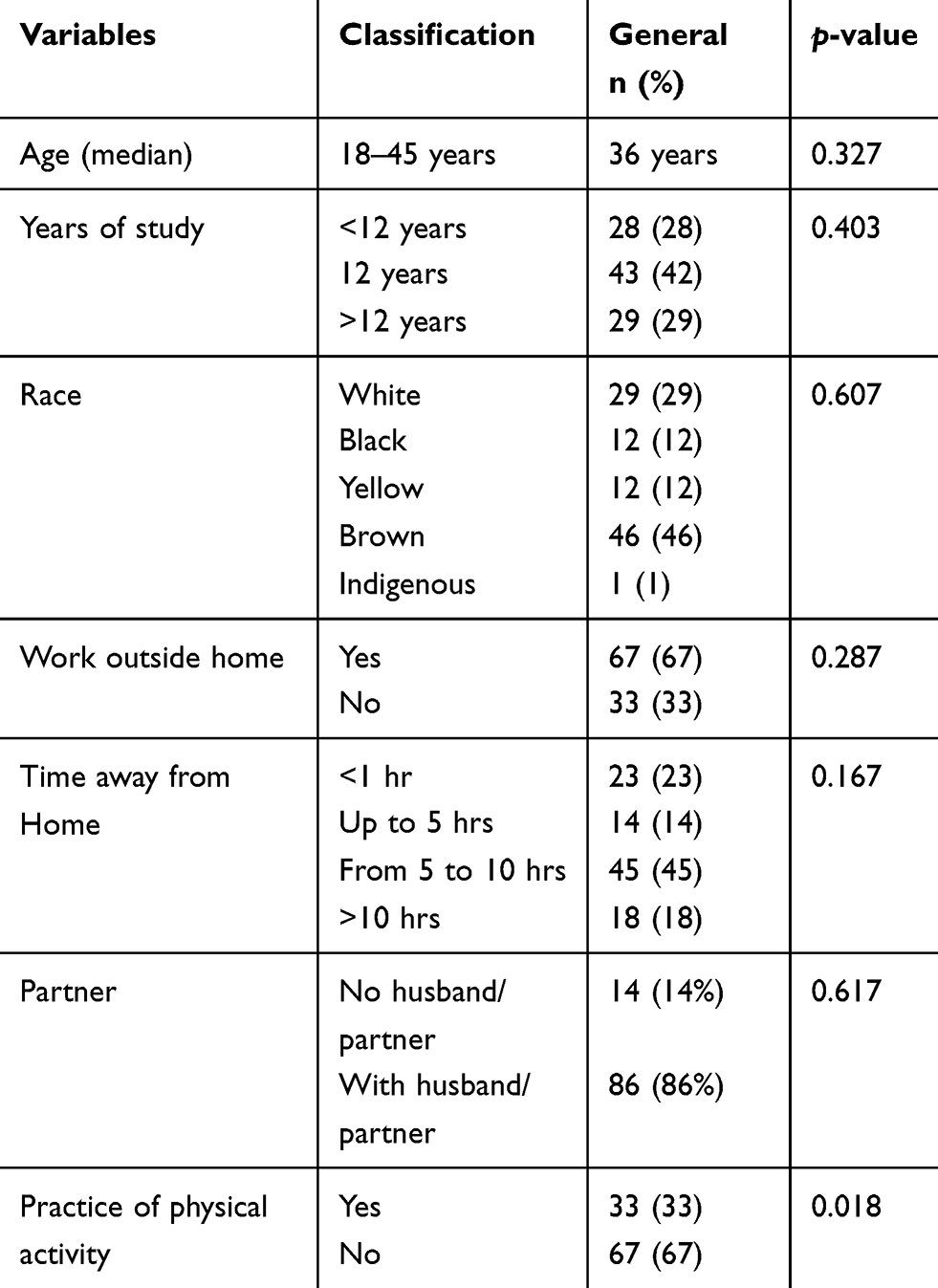 |
Table 1 Sociodemographic Data of Women Who Were Treated at the Two Primary Health Care Units of the Family for a Gynecological Examination |
 |
Table 2 Genital Hygiene and Genitalia Habits Among Women with or Without Vulvovaginitis Treated at Primary Health Care Units of the Family |
The analysis of the variables was described, within each group, using the mean and median, along with the maximum and minimum standard deviation. In addition, the Shapiro–Wilk normality test was applied. For all variables that did not present a normal distribution, the Mann–Whitney test was used to perform comparisons between the PCUs.17 Qualitative variables were described by frequency and percentage analysis. The associations of the qualitative variables with the groups (PCU) were evaluated using the likelihood ratio test.18 Risk factors for infection were assessed by univariate logistic regression, as well as by multiple logistic regression, followed by a stepwise selection of variables.19 All tests were applied using a significance level of 5% (p<0.05). The procedures were performed using the SPSS software v.20.
Results
The age of the women ranged from 18 to 45 years, where the average and median ages were 34.4 and 36 years, respectively. Seventy percent of women have completed 12 years of education. Of 100 women, 30 (30%) presented abnormalities in the microbiota, according to reports from the cytological exams, 18 from PCU1 and 12 from PCU2. The most frequently reported microorganism was coccobacilli [bacterial vaginosis] (n = 25, 83.3%), followed by Candida spp. (n = 3, 10%) and the simultaneous presence of both (n = 2, 6.7%), as shown in Table 3. However, no other microorganism, such as Trichomonas vaginalis and Actinomyces spp., were reported.
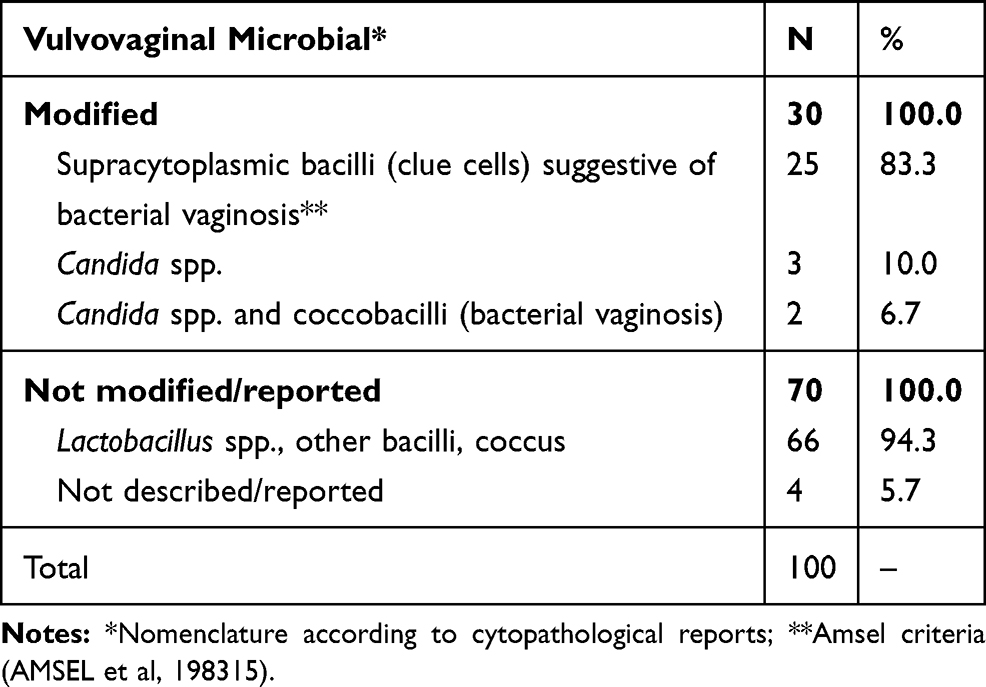 |
Table 3 Occurrence of Microorganisms Present in the Vaginal Microbiota of Women Who Treated at the Two Primary Health Care Units |
The main signs and symptoms reported by these patients (n = 30) were vaginal discharge (46.6%), odor (26.6%), and dyspareunia (13.3%). Seventy-one percent used some contraceptive methods, with hormones accounting for 55% of the women who used them. For these studied variables, no statistically significant differences were found comparing the sectors and the occurrence of infection. Other descriptive data and sociodemographic aspects of the participants are shown in Table 1.
In relation to genital hygiene and genitalia (Table 2), the frequency with which women without VV cleaned their genitalia (only with water and/or soap and water) was three or more times per day (45.7%), while those with VV cleaned their genitalia twice per day (50%).
Patients who had cytological results with altered microbiota (p<0.05) had altered odor (odds ratio, OR = 4.69, p = 0.0155), the habit of practicing genital hygiene with toilet paper, wiping from back to front (OR = 4.9, p = 0.0212), an infection or cutaneous/dermatitis reactions due to depilation in the genital area (OR = 3.3, p = 0.0438), and wore tight jeans (OR = 4.0526, p = 0.0107).
Discussion
This study examined the occurrence of vulvovaginal infections in women treated at primary health care units in a municipality in the interior of Brazil, as well as related and described hygiene habits and care of the genitalia of these women. The study allowed for the identification of the practices most commonly used by them, in addition to care.
The most frequent microorganism was coccobacilli causing bacterial vaginosis (n = 25, 83.3%), which is in line with results from reported by other researchers.20,21 However, Andrade et al22 and Silva et al23 reported VVC as the most common infection, with a prevalence of 71.4% and 19%, respectively, followed by coccobacilli (bacterial vaginosis) (25% and 16.4%, respectively). BV causes vaginal discharge in women of reproductive age24–26 in which half of the women were 36 years or younger. The variable occurrence of VV, in different studies, showed that the prevalence varied according to geographical region, socioeconomic level, and educational level. Moreover, BV mainly affects women of reproductive age because this group has an active sex life, they use contraceptives, in addition to possibly having more than one sexual partner and using an intrauterine device (IUD) as a contraceptive method. Those conditions are considered risk factors for the occurrence of BV.27 In this context, it is interesting to propose measures for health education in this group of women, addressing forms of acquisition, management, and prevention of this type of health problem, as well as the recognition of their presence.
Regarding the occupation of the participants, most Brazilian women today have intense professional and social activities, leaving them in unpleasant situations regarding their genital hygiene.28 In this context, it was evidenced in our study that women with VV washed their genitalia fewer times (twice a day) than women without VV (three or more times a day), which may be related to the appearance of signs and symptoms, and contribute to the onset of genital infections. Moreover, the work environment outside their home does not provide favorable and appropriate conditions for these women to be able to perform genital hygiene in the proper manner and frequency. As for the frequency of daily of hygiene, in warm weather, one should cleanse the intimate area one to three times a day, and in the cold climate at least once a day. These recommendations should also consider the woman’s biotype, skin type, physical activity, and clothing type.29
In this study, there was a statistically significant difference (p = 0.018) in the practice of physical activity among the health units, but it was not possible to confirm the relation between physical activity and VV.
Most of the participants reported that the form of hygiene after urination and evacuation was the use of toilet paper. A study conducted by Czerwinski,30 with American women, showed that soap with water was used most frequently for genital hygiene after urination or evacuation (50% to 60%). A Brazilian study by Giraldo et al10 found that VV women used more antibacterial soap to perform daily genital hygiene (p<0.0001), but women without VV reported using intimate liquid soap with more frequently than those with VV (p<0.05).
Inadequate genital hygiene can be understood as a lack of or excess in hygiene causing alterations in the genital homeostasis, and the lack of information on these hygiene practices negatively interferes with female genital health, favoring the emergence of VV. Soaps, although they are commonly used, for reasons of lower cost, tradition or ease of use, have components that can dissolve fat, in addition to a neutral/alkaline pH that, with routine use in the genital area, can have undesired consequences, such as dryness and decreased skin acidity (different from the physiological skin-acid pH).28 Some vaginal products, such as antibacterial soaps, may be harmful to Lactobacillus bacteria and are able to alter the vaginal environment; therefore, they should be used with caution.31
Hygiene after evacuation, in the posteroanterior direction, presented a statistically significant difference for the occurrence of infection (OR = 4.9, p = 0.0212). Although the majority of participants in the present study had at least 12 years of schooling, it was observed that nine patients (9%) performed hygiene after evacuation in the posteroanterior direction, and of these, eight (88.8%) presented up to 12 years of study. A study conducted in Egypt by Hamed32 showed that women who had a vaginal infection did not cleanse the genital area correctly (64–75%). Another study conducted in Turkey by Cangöl33 reported the frequency of genital infections at 38.1% in those participants who cleansed the genital area incorrectly. This inadequate form of hygiene facilitates the contamination and transference of microorganisms from the anus to the vagina, and consequently, can lead to vaginal infections.34–36 One point that was not pointed out in this study is the use of the vaginal douching (VD). According to some studies, VD seems to have no influence on the incidence of some infections, such as trichomoniasis,37 however, may increase the risk of pelvic inflammatory disease.38
The habit of depilating the genital area was reported by all women in the study. The most common method of depilation was a razor blade, reported by 68% of the women, where 80% that had VV and 62.8% that did not have VV used razor blade for hair removal (Table 2 ). For the infection/reactions and dermatitis due to depilation, there was a statistically significant difference for the occurrence of infection (OR= 3.3, p = 0.0438). Although depilation products are used to facilitate genital and aesthetic hygiene, the aggression caused by the blades or other products used to remove hair from the genitalia may cause skin dryness, traumatize, and irritate the area.29 A Brazilian study by Bardin et al39 showed that 94.1% of participants used to have hair removed from their genital area, and most used a razor blade to do so. De Maria et al40 stated in her their study that 60% of the participants presented at least one health complication due to the removal of pubic hair, the most common being epidermal abrasion and ingrown hairs. There is no consensus in the literature regarding the removal of hair from the genital area, although there is a recommendation for its removal due to the accumulation of residues and disruption of the genitalia, which facilitate the occurrence of infections. On the other hand, the periodic mechanical removal of the hairs, using a razor blade or other depilatory products, may promote irritation and inflammation of the region and should be as short as possible. Therefore, some recommendations suggest that the hair in the genital area should be cut approximately 0.5 cm, instead of being completely removed, to help maintain the health of the genital area, and genital depilation should respect the individual sensitivity of each woman.29,41
The use of jeans by our participants was statistically significant for the occurrence of infection (OR= 4.0526, p = 0.0107). More than half of the women with VV reported using cotton panties (70%) and wearing tight jeans/pants (83.3%). Clothing can cause alterations in the vaginal microbiota, due to temperature variation, local humidity, and compromised ventilation of the external genitalia, altering the genital ecosystem and causing irritation, an allergic reaction or discharge.12,13,29,42 Cotton panties allow more aeration and absorb more moisture, allowing perspiration, and cotton underwear was the most commonly used item by women in the present study. However, the fact that they also wore tight jeans or tight pants often caused a restriction of ventilation and compression of the vulva, promoting occlusion and friction, which may be harmful, thus negating the beneficial effect of cotton panties. Elegbe and Botu43 reported that women wearing wide trousers had fewer episodes of VVC, suggesting that tight clothing may predispose women to this VV.
Despite all the relevant issues raised in this study, the scientific literature is still sparse and controversial on this subject. However, in the context presented, the importance of genital hygiene habits and care related to women’s health and well-being is clear, and thus, preventive actions and health education are strongly indicated. Although the orientation in the clinical part by the health professionals is conducted in an empirical way, and little reason, due to the few works on the subject, the personalized evaluation of each woman is important, considering their peculiarities about their health problems.
Women make up the majority of the Brazilian population and the main users of the Unified Health System (in Portuguese, Sistema Único de Saúde, SUS). Thus, women make up a fundamental social fraction for health policies, not only because of their numerical importance, but especially because of gender issues as one of the determinants of health to be considered in the formulation of public policies. It is important to consider the fact that certain problems affect men and women differently. In the case of health problems associated with the exercise of sexuality, women are particularly affected. Women’s health issues have long been kept out of the scope of government public policies. However, this situation has changed and new dimensions related to the female experience deserve attention by the public power to promote the improvement of health in Brazilian women, by guaranteeing legally constituted rights and increasing access to means and services of promotion, prevention, care, and recovery of health.44
Health education has the purpose of identifying and using ways to preserve and improve the quality of life of the individual, helping people to acquire autonomy, and helping to prevent diseases, since the understanding of the determinants of health or disease provides subsidies for the adoption of new habits and health behaviors.45 A good educational action has the objective of providing knowledge and provoking a change of attitude. Moreover, it is considered an important tool for health promotion, which requires a combination of educational support aimed at achieving actions and conditions of life conducive to health.46 Thus, the search for health promotion and prevention strategies in health services through the dissemination of information, through campaigns, educational folders, lectures, waiting rooms, and other pedagogical actions of orientation are extremely important to the population.
The limitations of this study include the use of a questionnaire that was not validated. Although the work was performed in two distinct units, no statistically significant differences were observed between them. The occurrence data of VV were collected from reports of colpocytological results. Thus, it was not possible to verify more detail about the infectious microbiota, especially the presence of VVC. The comparison between the diagnosis or clinical hypothesis was also not performed, which limited the interpretation of the data.
Conclusion
Female well-being involves diverse variables and social customs and cultural issues often negatively interfere, especially when it comes to genital health. The habits of caring for the genitalia and the knowledge of self-care and diseases that affect the female genitalia can contribute to the decrease, management, and prevention of infections.
In the present study, we examined the main hygiene and genitalia care habits of women, with and without VV who treated in two health units. The main habits were cleaning the genitalia with toilet paper in the backwards direction, genital waxing, which caused infections or dermatitis, and wearing tight jeans. Inadequate care related to the female genital area was also observed in addition to the association of these factors with the occurrence of genital infections. In this context, the present study may contribute to the understanding of health professionals about the importance of the topic and its approach to patients, since health professionals should encourage women to take care of themselves through educational actions aimed at building knowledge and consequently contributing to mitigate the problem.
While genital hygiene habits are the target of some studies, the scope of and/or the number of researches need to be expanded, and the studies should always be updated, since there are few investigations that show the promotion of good hygiene practices for the population. The lack of studies on good genital hygiene practices may be related to the focus that is given to chronic-degenerative diseases, which are long-lasting, and require a large investment from health services. It is extremely important to control the signs and symptoms, triggered by incorrect habits, preventing the onset of vulvovaginal infections.
Abbreviations
BV, Bacterial vaginosis; VVC, Vulvovaginal candidiasis; HPV, Human Papillomavirus; IBGE, Brazilian Institute of Geography and Statistics; IUD, Intrauterine device; OD, Odds ratio; PCU, Primary Care Units for Family Health; SUS, Unified Health System; VV, Vulvovaginitis.
Data Sharing Statement
Available upon request from the corresponding author.
Acknowledgments
The authors thank the participants who made this study possible. The City Hall of Uberlândia for the authorization of the research in the Units of Primary Attention to Family Health. To the nurses Fernanda Vieira da Mota and Leandra Fonseca Duarte for allowing the study of their units, for the valuable contribution in the patients’ approach, support with the data collection, reading and access to gynecological results.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
This study was supported by Foundation for Research in the State of Minas Gerais, Brazil (FAPEMIG); Coordination of Improvement of Higher Education Personnel – Brazil (CAPES) – Financing Code 001; Foundation for University Support (FAU 002/2018), Pro-Rectory for Research and Graduate Studies (ProPP, Federal University of Uberlândia).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Schalkwyk JV, Yudin MH. Vulvovaginitis: screening for and management of trichomoniasis, vulvovaginal candidiasis, and bacterial vaginosis. J Obstet Gynaecol Can. 2015;37:266–274.
2. Attieh E, Maalouf S, Roumieh D, Abdayem P, Abitayeh G, Kesrouani A. Feminine hygiene practices among female patients and nurses in Lebanon. Reprod Health. 2016;13:1–6. doi:10.1186/s12978-016-0182-4
3. Tabile PM, Lucena H, Chaves J, Fischborn J, Juca RB. Clinical characteristics and prevalence of vulvovaginitis in a clinic in the interior of the Rio Rio Grande o Sul. J Health Biol S. 2016;4:160–165. doi:10.12662/2317-3076jhbs.v4i3.657.p160-165.2016
4. Nyirjesy P. Management of persistent vaginitis. Obstet Gynecol. 2014;124:1135–1146. doi:10.1097/AOG.0000000000000551
5. Milhomens PM, Machado MCAM, Moraes FC, Borges KRA, Diniz MRF. Prevalence of etiological agents of vulvovaginitis through results of cytopathology. Rev Investig Bioméd. 2014;6:92–102.
6. Kalra B, Kalra S. Vulvovaginitis and diabetes. J Pak Med Assoc. 2017;67:143–145.
7. Nunes RD, França CO, Traebert JF. Prevalence of vulvovaginitis in pregnancy and their relationship to perinatal complications. Arq Catarin Med. 2018;47:121–132.
8. Nami Y, Haghshenas B, Khosroushahi AY. Molecular identification and probiotic potential characterization of lactic acid bacteria isolated from human vaginal microbiota. Adv Pharm Bull. 2018;8:683–695. doi:10.15171/apb.2018.077
9. Ismail AM, Abbas AM, Shams AH, Kamel MA, Makarem MH. The effect of use of vaginal Lactobacillus rhamnosus for prevention of recurrence of vulvovaginal candidiasis: a randomized controlled trial. Thai J Obstet Gynaecol. 2017;25:62–68.
10. Giraldo PC, Polo RC, Amaral RL, Reis VV, Beghini J, Bardin MG. Habits and traditions of female college students related to intimate clothing, genital adornments, genital hair removal and sexual practices. Rev Bras Ginecol Obstet. 2013;35:401–406. doi:10.1590/S0100-72032013000900004
11. Shaaban OM, Abbas AM, Moharram AM, Farhan MM, Hassanen IH. Does vaginal douching affect the type of candidal vulvovaginal infection? Med Mycol. 2015;53:817–827. doi:10.1093/mmy/myv042
12. Roma I, Silva JA, Magolbo NG, Aquino RF, Marin MJS, Moravcik MYAD. Analysis of population perception about hygiene through an educational game. Rev Pesq Saúde. 2011;12:41–46.
13. Santos JKL, Santos SC, Sales PA, Araújo OMR, Batiston AP. Riverside women’s perception about sexual and reproductive health care. CIAIC. 2016;2:710.
14. IBGE. Brazilian Institute of Geography and Statistics. Available from: https://cidades.ibge.gov.br/brasil/mg/uberlandia/panorama.
15. Amsel R, Totten PA, Spiegel CA, Chen KC, Eschenbach D, Holmes KK. Nonspecific vaginitis. Diagnostic criteria and microbial and epidemiologic associations. Am J Med. 1983;74:14–22. doi:10.1016/0002-9343(83)91112-9
16. Paladine HL, Desai UA. Vaginitis: diagnosis and treatment. Am Family Phys. 2018;97:321–329.
17. Zar JH. Biostatistical Analysis. Prentice Hall; 1999:663.
18. Agresti A. An Introduction to Categorical Data Analysis.
19. Hosmer DW, Lemeshow S. Applied Logistic Regression.
20. Vasconcelos CTM, Neto JAV, Castelo ARP, Medeiros FC, Pinheiro AKB. Analysis of coverage and of the pap test exams not retired of a basic health unit. Rev Esc Enferm USP. 2010;44:323–328.
21. Soares MBO, Silva SR. Analysis of a municipal program of uterine cervical neoplasm prevention. Rev Bras Enferm. 2010;63:177–182. doi:10.1590/S0034-71672010000200002
22. Andrade SSC, Silva FMC, Oliveira SHS, Leite KNS, Costa TF, Zaccara AAL. Microbiological agents of vulvovaginites identified by pap smear. Rev Enferm UFPE on Line. 2014;8:338–345.
23. Silva CS, Pavani R, Ângelo A, Adad SJ, Souza MAH, Murta EFC. Frequency and age distribution of vaginal infection by Gardnerella vaginalis, Candida sp and Trichomonas vaginalis in pap smear. Rev Med Minas Gerais. 2003;13:92–96.
24. Febrasgo. Federação Brasileira das Associações de Ginecologia e Obstetrícia. Manual de Orientação do Trato Genital Inferior. São Paulo. 2010.
25. Chen Y, Bruning E, Rubino J, Eder SE. Role of female intimate hygiene in vulvovaginal health: global hygiene practices and product usage. Womens Health (Lond). 2017;13:58–67. doi:10.1177/1745505717731011
26. Jain JP, Bristow CC, Pines HA, et al. Factors in the HIV risk environment associated with bacterial vaginosis among HIV-negative female sex workers who inject drugs in the Mexico-United States border region. BMC Public Health. 2018;18:1032. doi:10.1186/s12889-018-5965-9
27. Leite SRRF, Amorim MMR, Calábria WB, et al. Clinical and microbiological profile of women with bacterial vaginosis. Rev Bras Ginecol Obstet. 2010;32:82–87. doi:10.1590/S0100-72032010000200006
28. Bezerra PX, SouzaJBP, Carmo ES, Luis JAS. Analysis of labelling and quality parameters of intimatesoaps. Revista Brasileira De Ciências Da Saúde. 2016;20:51–60. doi:10.4034/RBCS.2016.20.01.08
29. Febrasgo. Brazilian Federation of Gynecology and Obstetrics Associations. Guia prático de condutas sobre higiene Genital Feminina/Practical Guide to Female Genital Hygiene Conducts. São Paulo. 2009. Available from: https://missali.site.med.br/fmfiles/index.asp/::XPR3638::/Guia_de_Higiene_Feminina.pdf. Accessed October 22, 2018.
30. Czerwinski BS. Variation in feminine hygiene practices as a function of age. J Obstet Gynecol Neonatal Nurs. 2000;29:625–633. doi:10.1111/j.1552-6909.2000.tb02076.x
31. Fashemi B, Delaney ML, Onderdonk AB, Fichorova RN. Effects of feminine hygiene products on the vaginal mucosal biome. Microb Ecol Health Dis. 2013;24:1–6.
32. Hamed AG. The impact of genital hygiene practices on the occurrence of vaginal infection and the development of a nursing fact sheet as prevention massage for vulnerable women. IOSR J Nurs Health Sci. 2015;4:55–64.
33. Cangöl E. The evaluation of genital infections and genital hygiene practices of women who applied to gynecology polyclinic. FN Hem Derg. 2010;21:85–89.
34. Güler G, Bekar M, Güler N, Kocataş S. Menstruation period hygiene in primary school girls. Sted. 2005;14:135–139.
35. McClelland RS, Lavreys L, Hassan WM, Mandaliya K, Ndinya-Achola JO, Baeten JM. Vaginal washing and increased risk of HIV-1 acquisition among African women: a 10-year prospective study. AIDS. 2006;20:269–273. doi:10.1097/01.aids.0000196165.48518.7b
36. Martin Hilber A, Hull TH, Preston-Whyte E, et al. A cross cultural study of vaginal practices and sexuality: implications for sexual health. Soc Sci Med. 2010;70:392–400. doi:10.1016/j.socscimed.2009.10.023
37. Galal LA, Shaaban OM, Abbas AM, Mitwaly ABA, William AN, Al-Hussaini TK. Diagnosis of Trichomonas vaginalis infection and its relation to internal vaginal hygiene. Int STD Res Rev. 2016;4:1–9. doi:10.9734/ISRR
38. Abbas AM, Shaaban OM, Badran SM, Shaltout AS, Nasr A, Abdullah SA. Risk factors and health hazards of vaginal infections in upper Egypt: a cross sectional study. Thai J Obstet Gynaecol. 2016;24:50–56.
39. Bardin MG, Giraldo PC, Pinto CLB, Piassaroli VP, Amaral RLG, Polpeta N. Association of sanitary pads and clothing with vulvovaginitis. J Bras Doenças Sex Transm. 2013;25:123–127. doi:10.5533/DST-2177-8264-201325302
40. De Maria AL, Flores M, Hirth JM, Berenson AB. Complications related to pubic hair removal. Am J Obstet Gynecol. 2014;210:528.
41. Giraldo P, Beghini J. Higiene Genital Feminina. São Paulo: Farol; 2015:196.
42. Michelin SR, Marchi JG, Hyeda IS, Heidemann ITSB, Nitschke RG. Women’s perception about health promotion during the nursing consultation. Cienc Cuid Saude. 2015;14:
43. Elegbe IA, Botu M. A preliminary study in dressing patterns and incidence of candidiasis. Am J Public Health. 1982;72:176–177. doi:10.2105/AJPH.72.2.176
44. Brasil. Conselho Nacional dos Direitos da Mulher. II Plano Nacional de Políticas para as Mulheres. Available from: https://www.mdh.gov.br/navegue-por-temas/politicas-para-mulheres/arquivo/arquivos-diversos/publicacoes/publ_ii_pnpm.
45. Salci MA, Maceno P, Rozza SG, Silva DMGV, Boehs AE, Heidemann ITSB. Health education and its theoretical perspectives: a few reflections. Texto Contexto Enferm. 2013;22:224–230. doi:10.1590/S0104-07072013000100027
46. Janini JP, Bessler D, Vargas AB. Health education and health promotion: impact on quality of life of elderly. Saúde Debate. 2015;39:480–490. doi:10.1590/0103-110420151050002015
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.