Back to Journals » Infection and Drug Resistance » Volume 16
Evaluation of the Most Visible Symptoms Associated with COVID-19 Vaccines Among the Residents of Makkah, Saudi Arabia: An Observational, Cross-Sectional Study
Authors Qashqari FS, Alfelali M, Barasheed O, Almaimani R, Alghamdi A ![]() , Alharbi SS, Balahmar E, S Alhothali A, Alsharif RH, Jalal NA
, Alharbi SS, Balahmar E, S Alhothali A, Alsharif RH, Jalal NA ![]() , Makhdoom H
, Makhdoom H
Received 15 March 2023
Accepted for publication 8 July 2023
Published 8 August 2023 Volume 2023:16 Pages 5107—5119
DOI https://doi.org/10.2147/IDR.S409200
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Fadi S Qashqari,1 Mohammad Alfelali,2 Osamah Barasheed,3,4 Ruba Almaimani,5 Anas Alghamdi,6 Sarah S Alharbi,7 Eman Balahmar,8 Ammar S Alhothali,9 Rahaf Hashim Alsharif,10 Naif A Jalal,1 Hatim Makhdoom11
1Department of Microbiology, College of Medicine, Umm Al-Qura University, Makkah, Saudi Arabia; 2Department of Family and Community Medicine, Faculty of Medicine, King Abdulaziz University, Jeddah, Saudi Arabia; 3Research and Innovation Center, King Abdullah Medical City, Makkah, Saudi Arabia; 4Basira Center for Health Research Training and Consulting, Makkah, Saudi Arabia; 5Health Promotion and Education Department, Faculty of Public Health and Health Informatics, Umm Al-Qura University, Makkah, Saudi Arabia; 6Faculty of Dental Medicine, Umm Al-Qura University, Makkah, Saudi Arabia; 7Faculty of Pharmacy, Umm Al-Qura University, Makkah, Saudi Arabia; 8College of Medicine, King Saud bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia; 9Faculty of Medicine and Surgery, College of Medicine, Umm Al-Qura University, Makkah, Saudi Arabia; 10Department of Nursing, King Abdullah Medical City, Makkah, Saudi Arabia; 11Department of Laboratory Technology, College of Applied Medical Sciences, Taibah University, Medina, Saudi Arabia
Correspondence: Fadi S Qashqari, Tel +966 553552660, Email [email protected]
Background: This research evaluated the most visible symptoms associated with coronavirus (COVID-19) vaccines among residents in Makkah of Saudi Arabia.
Methods: A cross-sectional study was conducted in 2021 among a representative sample of residents receiving COVID-19 vaccination at King Abdullah Medical City, Al Ukayshiyyah, and Umm Al-Qura University vaccination centers. A total of 805 participants selected by a census sampling method were included. Data regarding characteristics, medical history, and post-vaccination symptoms were obtained with an interview-based questionnaire.
Results: The participants’ mean age was 25.20 ± 15.5 years. Of them, 61.7% and 38.3% received one and two doses of the COVID-19 vaccine, respectively. 2.2% have an allergic reaction to the COVID-19 vaccine. 25.3% were infected with COVID-19, 23% were infected before the first dose, and only 1.6% were infected after the first dose. Significant statistical associations were found between males and females in smoking status, age, body mass index, history of diabetes mellitus, and types of COVID-19 vaccines (P-value < 0.05). After adjustment for confounding variables, male participants had lower odds of having swelling, redness, or pain at the injection site, muscle or joint pain, headache, dizziness, and nausea compared to female participants [OR = 0.596, 95% CI = (0.388– 0.916)], [OR = 0.272, 95% CI = (0.149– 0.495)], [OR = 0.529, 95% CI = (0.338– 0.828)], [OR = 0.263, 95% CI = (0.125– 0.554)], and [OR = 0.145, 95% CI = (0.31– 0.679), P < 0.05 for all], respectively.
Conclusion: The female participants may have a higher risk of post-COVID-19 vaccination symptoms than males among Makkah residents of Saudi Arabia.
Keywords: COVID-19, evaluation, Saudi Arabia, symptoms, vaccines
Introduction
In December 2019, Wuhan City, China, experienced an outbreak of COVID-19 caused by SARS-CoV-2. The World Health Organization declared it a public health emergency. Over 16,000 deaths and 2.8 million new cases occurred in 28 days, with 764 million confirmed cases and 6.9 million fatalities.1,2
Ensure reliable diagnostic laboratory operations, avoid cross-contamination, and follow proper laboratory practices and guidelines. Maintain unidirectional workflow and follow the aseptic technique in each step to prevent cross-contamination and ensure proper handling of biological specimens.3
COVID-19 patients typically experience mild-to-moderate respiratory illness and recover without therapy. Serious diseases are more common in older individuals and those with underlying medical disorders.4
COVID-19 causes respiratory symptoms like fever, coughing, and shortness of breath, potentially leading to pneumonia, severe acute respiratory syndrome, and death.5 Preventing spread involves hand hygiene, covering the nose and mouth, and avoiding close contact with those with fever and cough.6 COVID-19 is a mysterious infection requiring extensive study and collaboration for containment, prevention, and treatment.7 A safe and effective vaccine is crucial for addressing the pandemic.8
Saudi Arabia has experienced 475,500 COVID-19 cases and 7000 fatalities.9 The country has implemented preventive measures, including banning international flights, closing mosques, schools, and universities, and implementing a reliable vaccine program to mitigate the impact of disease.10,11
The Saudi Arabian Food and Drug Authority approved four COVID-19 vaccines, including Pfizer-BioNTech, Oxford-AstraZeneca, Johnson & Johnson, and Moderna, nationwide. The program began in December 2021 and has immunized around 16 million people.12–14 Vaccine campaign targeted high-risk groups, including the elderly and healthcare professionals.15 Saudi Arabia initiates early immunization drive to combat COVID-19.10,16
Saudi Arabia Food and Drug Authority approved four COVID-19 vaccines, but differences in vaccination effectiveness may be due to faster development and mRNA vaccines, a new technology.17–19 Saudi Arabia’s Ministry of Health combines multiple COVID-19 vaccines amid scarcity.20 Accordingly, the study assesses post-vaccination side effects of mixed and matched COVID-19 vaccines in Makkah, Saudi Arabia, focusing on prominent adverse effects.
Methods
Study Design and Period
This observational cross-sectional study was conducted between June 29, 2021, and August 11, 2021.
Study Setting
The study was conducted at King Abdullah Medical City Specialist Hospital, Al Ukayshiyyah, and Umm Al-Qura University vaccination centers in Al-Abdiyah, Makkah, Saudi Arabia.
Study Participants
The study included 805 participants aged 12–87 from Saudi Arabia who received COVID-19 vaccinations at King Abdullah Medical City Specialist Hospital, Al Ukayshiyyah, and Umm Al-Qura University. Pregnant, lactating women and serious illness participants were excluded.
Study Sampling
The study involved 805 participants from King Abdullah Medical City Specialist Hospital, Al Ukayshiyyah, and Umm Al-Qura University vaccination centers in Al-Abdiyah, Makkah, Saudi Arabia, with a response rate of 89.4%.
Data Collection
Interview Based Questionnaire
The study used an interview-based questionnaire to gather demographic data, medical history, and post-COVID-19 symptoms. The questionnaire’s face and content validity were independently validated by seven experts.21 The pilot study involved 30 participants, with a Cronbach’s alpha of 0.85. Participants received COVID-19 vaccines, were informed of study purposes, and were given communication methods like Call, WhatsApp, or Telegram. Study participants were contacted via a preferred method to discuss post-COVID-19 vaccine symptoms. Results were shared on the first, seventh, and twenty-eighth days of receiving the first- and second-dose vaccines (Figure 1).
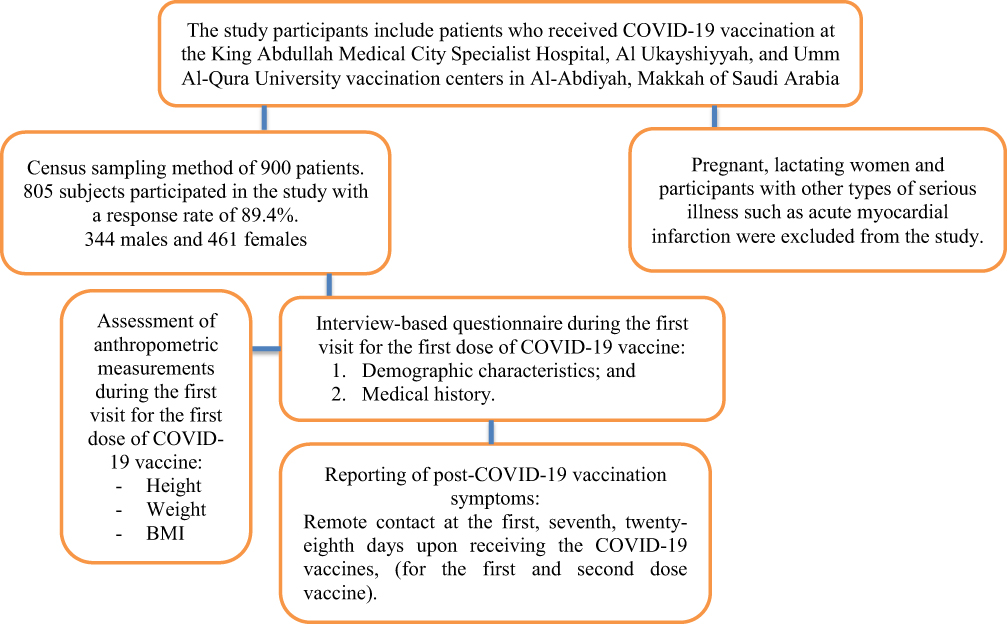 |
Figure 1 Schematic diagram of the recruitment plan of the study participants. |
The study used a census sampling method to reduce bias and ensure qualified data collectors conducted data collection. The independent variable was COVID-19 vaccination, while the dependent variables were visible symptoms associated with the vaccine and other factors.
Assessment of Anthropometric Measurements
A measuring rod attached to a balanced beam scale was used to measure each participant’s height (in centimeters) after receiving the first dose of the COVID-19 vaccination. Participants were asked to stand barefoot with their heads up. A standard scale (Seca) was used to measure weight (kg). Participants were requested to remove their bulky outerwear before stepping on the scale, and weight was recorded to the nearest 0.1 kg. By dividing a person’s weight in kilograms by their height in square meters, the body mass index (BMI) was determined.22
Data Analysis
SPSS for Windows (version 25), a statistical program for social science, was used for data analysis. Descriptive statistics were used to characterize both continuous and categorical data. The significance of the differences between category variables was determined using the chi-square test. The differences between the mean were tested by independent samples t-test. Furthermore, crude and adjusted odds ratio (OR) and 95% confidence interval (CI) for the most visible symptoms among the study participants after the COVID-19 vaccine by gender were calculated using binary logistic regression.
Ethics Considerations
The study protocol, which complies with the Declaration of Helsinki (HAPO-02-K-012-2021-08-713), was approved by the College of Medicine at Umm Al Qura University.
Additionally, permission was obtained from the vaccination facilities at King Abdullah Medical City Specialty Hospital, Al Ukayshiyyah, and Umm Al-Qura University. Participants under 18 further provided informed consent signed by a parent or legal guardian. In addition, written informed consent was obtained from each participant.
Results
Eight hundred and five individuals with a mean age of 25.20 ± 15.5 years who lived in Makah and received the COVID-19 vaccine participated in this study. 33.9% of the study participants were from the King Abdullah Medical City Specialist Hospital vaccination center, 32.9% were from the Al Ukayshiyyah vaccination center, and 33.1% were from the Umm Al-Qura University vaccination center. Only 2.2% (n = 18) of them are allergic to the COVID-19 vaccine. 9.6% of the study participants were smokers. More than two-third of the study participants (75.0%) were Saudi. 14.8% of them were classified as underweight (BMI below 18.5 kg/m2), 13.9% were classified as Overweight (BMI 25.0–29.9 kg/m2), and 13.9% were classified as obese (BMI > 30.0kg/m2). Significant statistical associations were found between males and females in smoking status, age, and body mass index (P-value < 0.05) (Table 1).
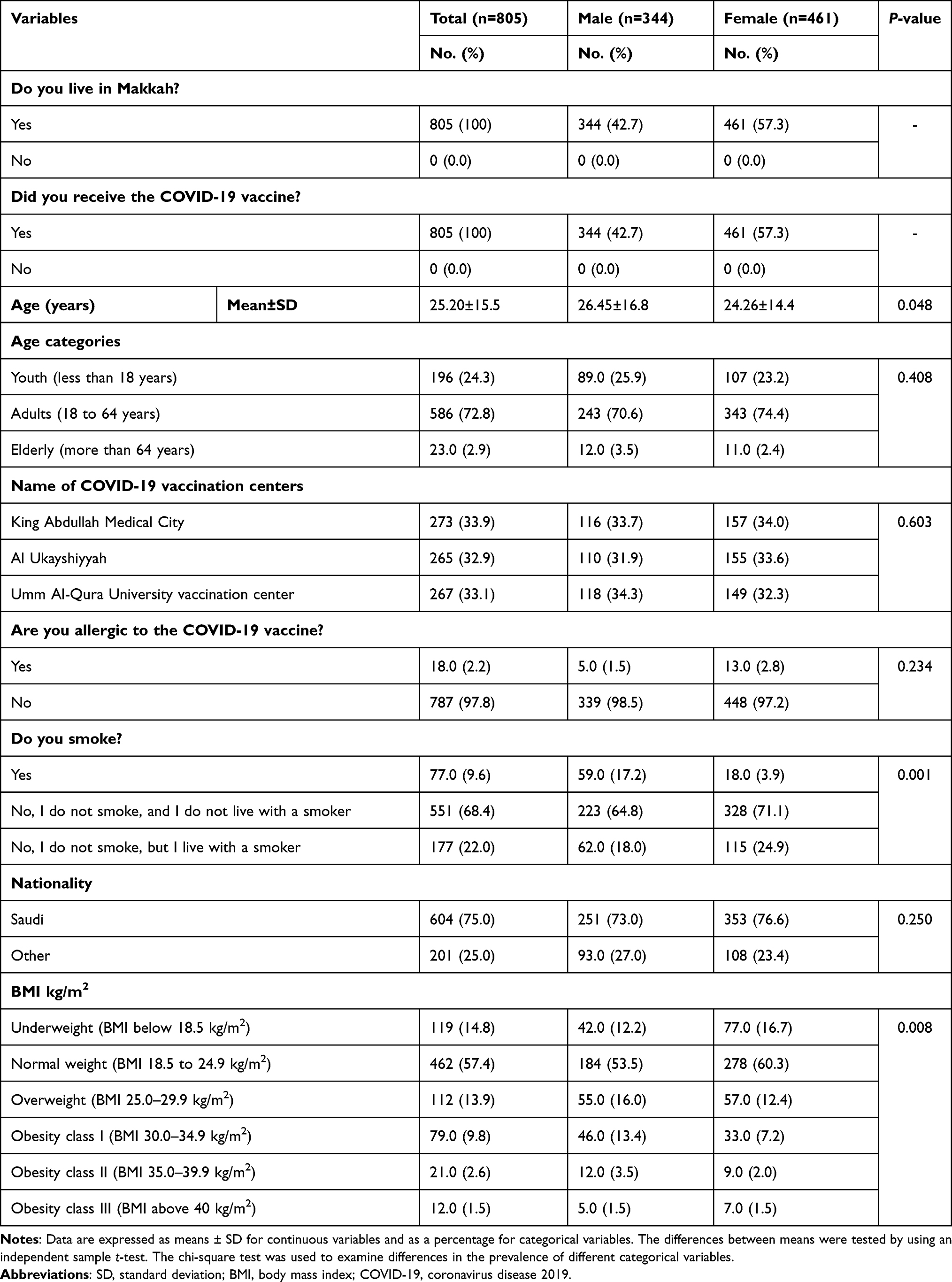 |
Table 1 Characteristics of the Study Population by Gender |
The medical history of the study participants showed that only 4.2% use anticoagulant drugs, 2.9% use corticosteroid therapy, and 1.0% use immunosuppressive drugs. No participants use cancer treatments or have a history of AIDs. 6.8% of the study participants suffered from hypertension, 5.8% from respiratory diseases, and 0.7% from cancer.
61.7% (n = 497) and 38.3 (n = 308) of the study participants received one and two doses of COVID-19 vaccine, respectively. 87.1% and 12.9% of the study participant received Pfizer-BioNTech, and Oxford/AstraZeneca COVID-19 vaccines for the first dose, respectively. 29.3%, 8.3%, and 0.6% of the study participants received Pfizer-BioNTech, Oxford/AstraZeneca, and Johnson and Johnson COVID-19 vaccine for the second dose, respectively. 25.3% of the study participants were infected with COVID-19; 23% were infected before the first dose, and only 1.6% were infected after the first dose.
Significant statistical associations were found between males and females in having diabetes mellitus, type of COVID-19 vaccine for the first dose, and type of COVID-19 vaccine for the second dose (P-value < 0.05) (Table 2).
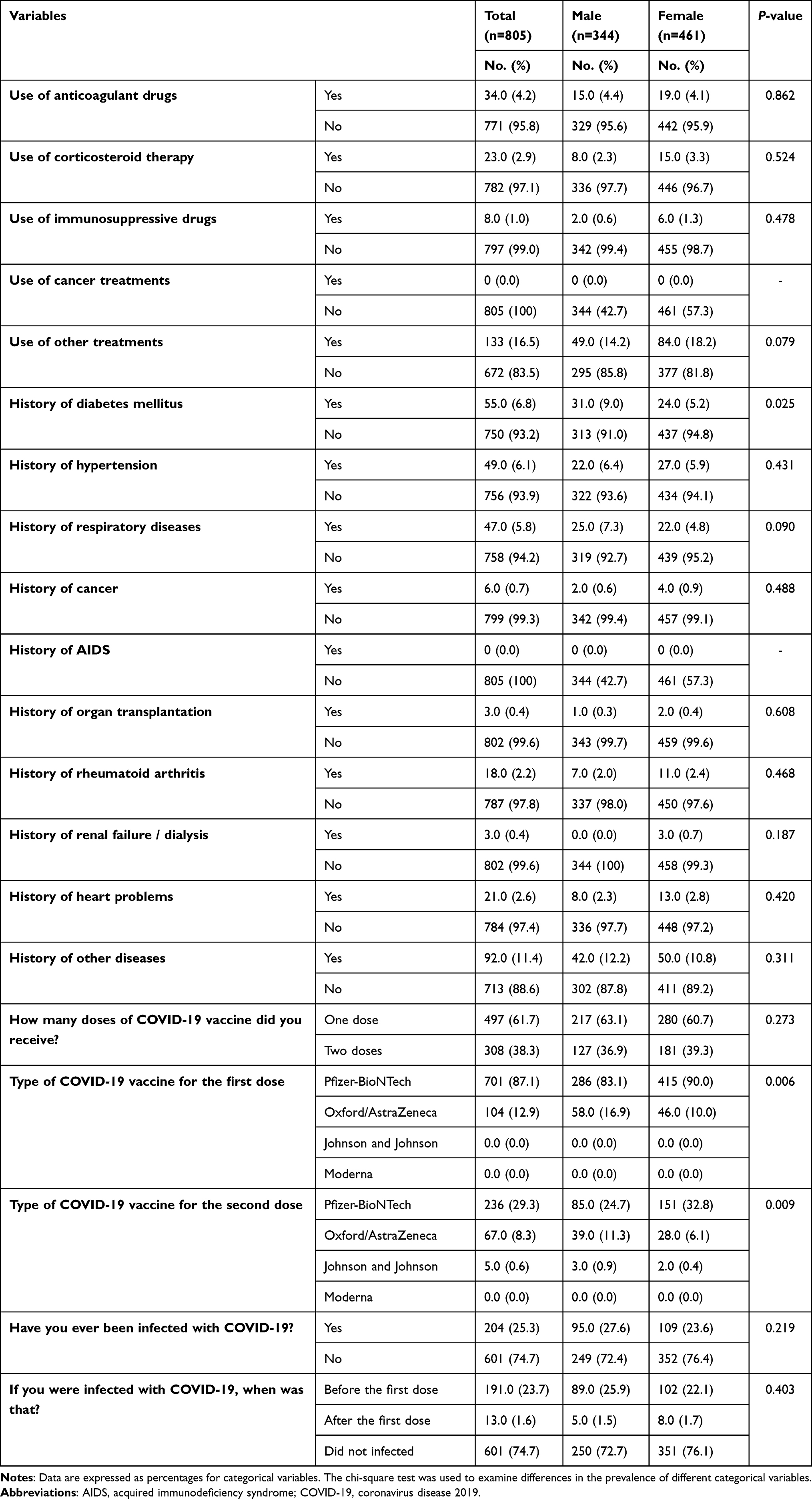 |
Table 2 Medical History Variables for the Study Population by Gender |
Table 3 shows the most visible symptoms among the study population after the COVID-19 vaccine by gender. The results revealed that 24.1% of the study participants experienced swelling, redness, or pain at the injection site after the COVID-19 vaccine, followed by headache (14.5%) and exhaustion (14.2%). In addition, 10.6% experienced an increase in body temperature above 36.5 °C, 9.8% experienced muscle or joint pain, 6.2% of the study participants had dizziness, and 7.7% had insomnia. Only 0.9% of the study participants experienced gastritis, 2.0% experienced nausea, 0.4% experienced loss of consciousness, 1.6% experienced shortness of breath or difficulty breathing, 1.0% experienced ringing in the ear, 1.7 experienced harshnesses, 0.5% experienced blood clots, and 2.4% experienced other symptoms.
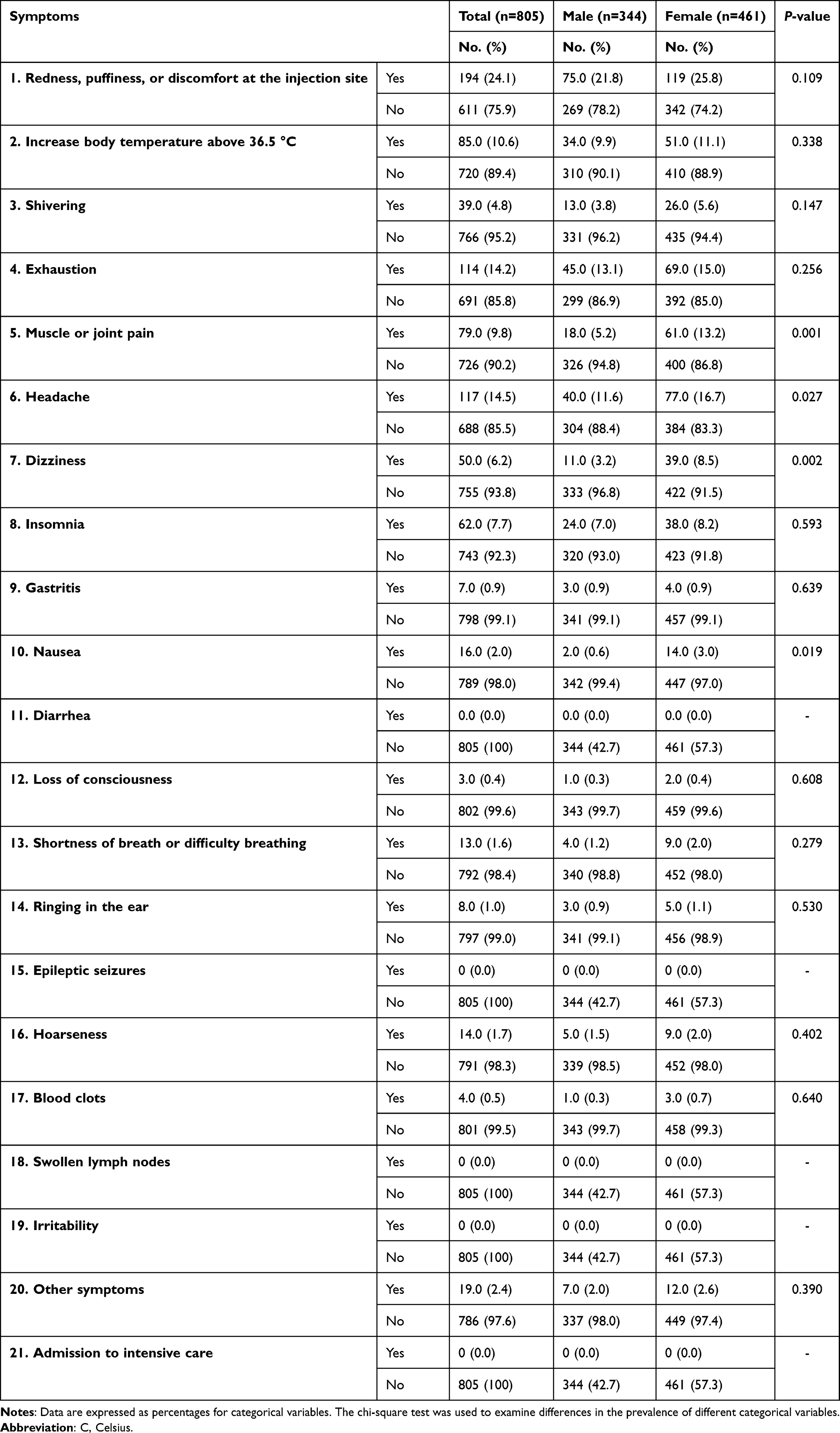 |
Table 3 The Most Visible Symptoms Among the Study Population After the COVID-19 Vaccine by Gender |
Symptoms such as diarrhea, epileptic seizures, swollen lymph nodes, irritability, and admission to intensive care were not reported. Significant statistical associations were found between males and females in the symptoms of muscle or joint pain, headache, dizziness, and nausea (P-value < 0.05) (Table 3).
Finally, the binary logistic regression was employed to calculate the crude and adjusted OR and 95% CI for the most visible symptoms among the study population after the COVID-19 vaccine by gender (Table 4). The findings showed that, after adjusting for confounding factors, the male participants had lower odds of having swelling, redness, or pain at the injection site, muscle or joint pain, headache, dizziness, and nausea compared to female participants [OR = 0.596, 95% CI = (0.388–0.916)], [OR = 0.272, 95% CI = (0.149–0.495)], [OR = 0.529, 95% CI = (0.338–0.828)], [OR = 0.263, 95% CI = (0.125–0.554)], and [OR = 0.145, 95% CI = (0.31–0.679), P < 0.05 for all], respectively.
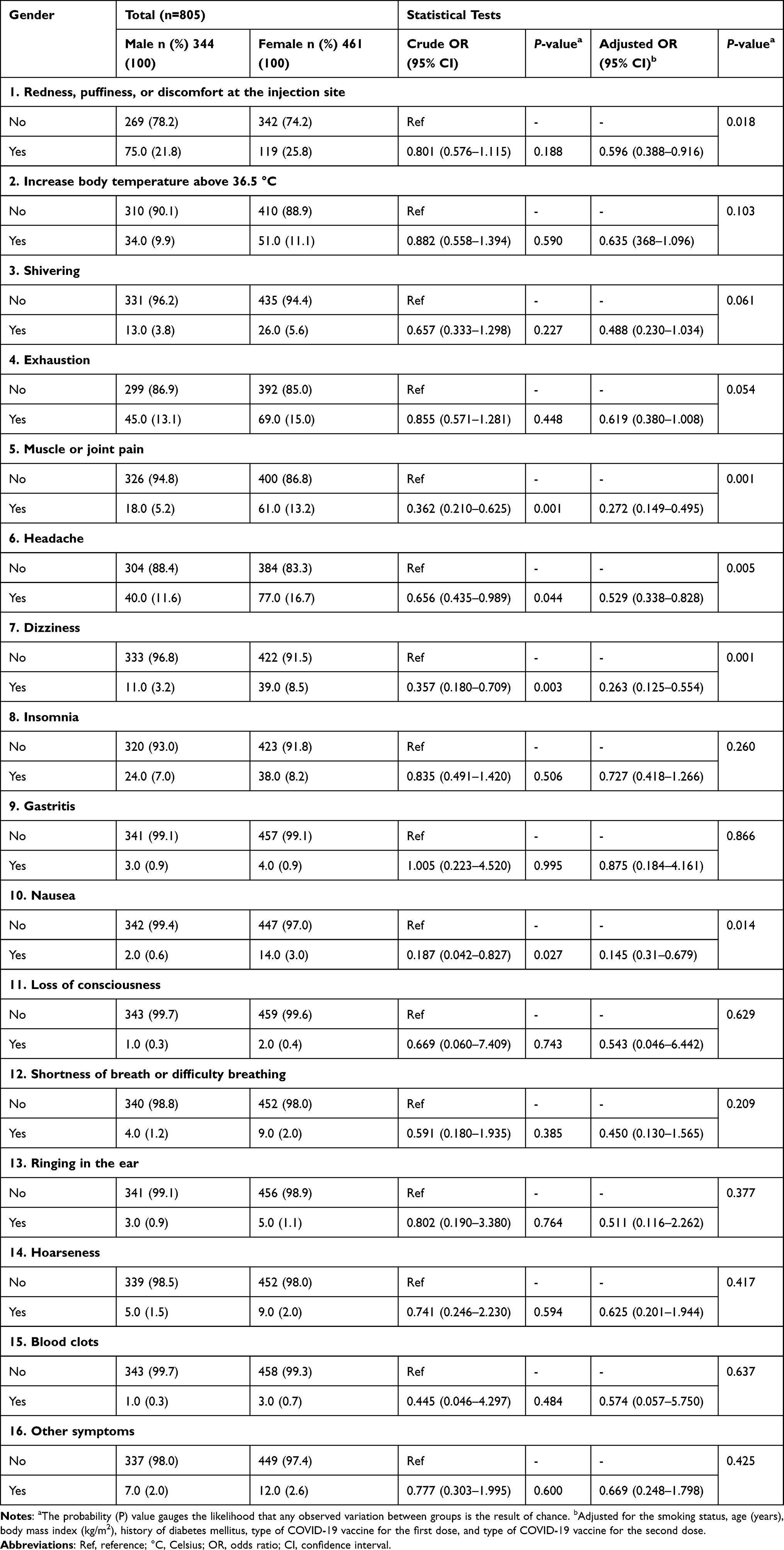 |
Table 4 Crude and Adjusted Odds Ratio and 95% Confidence Interval for the Most Visible Symptoms Among the Study Population After COVID-19 Vaccine by Gender |
Discussion
The COVID-19 pandemic began in 2020; nations prioritize preventative measures for safe and effective vaccinations 10. Vaccine candidates were created concurrently; only a few were granted Emergency Use Authorization (EUA).23
Saudi Arabia initiates early COVID-19 vaccination campaign as part of efforts.23,24 Saudi Arabia’s population’s willingness to receive the COVID-19 vaccine varies due to rapid development and mRNA vaccines, which may factor in the difference.17,18,25,26
Recent publications highlight potential severe post-vaccination side effects due to key variables.24,26
This study assessed short-term adverse effects and symptoms of COVID-19 vaccines in Saudi Arabia, focusing on individuals receiving Pfizer-BioNTech, Oxford/AstraZeneca, and Johnson and Johnson vaccinations. Results showed 60% to 80% of side effects influenced by age, vaccine type, and dose.27,28
The study found frequent side effects and symptoms after COVID-19 vaccines, including fatigue (14.2%), headache (14.5%), and swelling (24.1%). These symptoms occurred on the first, seventh, or twenty-eighth days, mainly for those receiving double dosage.27–30
Menni et al report soreness and local pain as common adverse effects after injections.31 70–80% of Saudi Arabian trial participants experienced injection site pain.32 The study finds younger participants experiencing fatigue and headaches, contrasting previous research, mainly due to their younger ages.31,32 Research shows younger people experience more side effects.27,33
Alhazmi et al study show that 60% of respondents experienced adverse effects from COVID-19 vaccines, including weariness and soreness.29
The study finds that female participants in Makkah, Saudi Arabia, have a higher risk of visible COVID-19 symptoms than males, consistent with previous research.29,31 Adam et al found males more likely to experience adverse effects after COVID-19 vaccination.30 The study suggests lower male percentages may cause increased side effects in females, including injection site reactions, fatigue, headache, muscle pain, chills, and nausea.
The study found that 87.1% and 12.9% of participants received Pfizer-BioNTech and Oxford/AstraZeneca COVID-19 vaccines, respectively. The second dose had a higher risk of systemic side effects.34 Future studies are needed to confirm Saudi Arabian findings.
Mild-to-moderate COVID-19 vaccination side effects were reported.27–29,31,32 The study found non-life-threatening COVID-19 vaccine side effects, with 25.3% infected, 23% infected before, and 1.6% after. Age, sex, serostatus, and comorbidities may influence vaccine half-life.35–37
Concerns about mRNA vaccines spreading COVID-19 are unfounded as they were not created using live COVID-19. Insufficient time for T- and B-lymphocyte production after immunization allows for “breakthrough cases” and potential infection.38,39
Research on COVID-19 vaccine adverse effects may increase public trust in vaccine safety, potentially hastening immunization. Addressing vaccine hesitancy through friendly organizations and government-induced policy measures could shift public disbelief to confidence.40 The study reveals women’s gender decreases vaccine hesitancy, while older age, education, and adherence to prevention increase it.41 The study found no serious health issues and raised awareness of COVID-19 vaccine benefits and safety. It dispelled misconceptions about post-vaccination effects and recommended future studies on booster shots. Long-term health care and strategic financial planning are top priorities in many nations.42
This study evaluates visible symptoms of COVID-19 vaccines in Makkah, Saudi Arabia, following participants for the first, seventh, and 28th days. Although it is the first in Saudi Arabia to discuss side effects and symptoms, its cross-sectional design limits generalizability. Additionally, many participants did not receive the second dose, and the predominant circulating variant of COVID-19 did not report during the study period, potentially affecting vaccine efficacy and severity.
Conclusion
The study assessed COVID-19 vaccine-related symptoms in Makkah, Saudi Arabia, revealing common side effects like pain, edema, redness, fatigue, and headache. Female participants were more likely to experience these symptoms. A larger population study is needed to evaluate vaccine effectiveness and long-term side effects.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Harapan H, Itoh N, Yufika A, et al. Coronavirus disease 2019 (COVID-19): a literature review. J Infect Public Health. 2020;13(5):667–673. doi:10.1016/j.jiph.2020.03.019
2. World Health Organization. Weekly epidemiological update on COVID-19. World Health Organization; 2023. Available from: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19---27-april-2023.
3. Albano PM, Notarte KI, Macaranas I, Maralit B. Cross-contamination in molecular diagnostic laboratories in low-and middle-income countries. PJP. 2020;5(2):7–11. doi:10.21141/PJP.2020.09
4. World Health Organization. Getting your workplace ready for COVID-19: how COVID-19 spreads. World Health Organization; 2020.
5. Pal M, Berhanu G, Desalegn C, Kandi V. Severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2): an update. Cureus. 2020;12(3). doi:10.7759/cureus.7423
6. Parravano M, Borrelli E, Costanzo E, Sacconi R, Varano M, Querques G. Protect healthcare workers and patients from COVID-19: the experience of two tertiary ophthalmology care referral centers in Italy. Ophthalmol Ther. 2020;9(2):231–234. doi:10.1007/s40123-020-00251-z
7. Umakanthan S, Sahu P, Ranade AV, et al. Origin, transmission, diagnosis and management of coronavirus disease 2019 (COVID-19). Postgrad Med J. 2020;96(1142):753–758. doi:10.1136/postgradmedj-2020-138234
8. Ruiz‐Hitzky E, Darder M, Wicklein B, et al. Nanotechnology responses to COVID‐19. Adv Healthcare Mater. 2020;9(19):2000979. doi:10.1002/adhm.202000979
9. Choudhury N, Mathur A, Smit Sibinga CT. COVID‐19 Pandemic–blood supply challenges and approaches in AATM member countries. ISBT Sci Ser. 2020;15(4):353–361. doi:10.1111/voxs.12578
10. Algaissi AA, Alharbi NK, Hassanain M, Hashem AM. Preparedness and response to COVID-19 in Saudi Arabia: building on MERS experience. J Infect Public Health. 2020;13(6):834–838. doi:10.1016/j.jiph.2020.04.016
11. Raja AT, Alshamsan A, Al-Jedai A. Current COVID-19 vaccine candidates: implications in the Saudi population. Saudi Pharm J. 2020;28(12):1743–1748. doi:10.1016/j.jsps.2020.10.019
12. Ahmed S, Khan S, Imran I, et al. Vaccine development against COVID-19: study from pre-clinical phases to clinical trials and global use. Vaccines. 2021;9(8):836. doi:10.3390/vaccines9080836
13. Qattan AM, Alshareef N, Alsharqi O, Al Rahahleh N, Chirwa GC, Al-Hanawi MK. Acceptability of a COVID-19 vaccine among healthcare workers in the Kingdom of Saudi Arabia. Front Med. 2021;8:644300. doi:10.3389/fmed.2021.644300
14. Barry M, BaHammam AS. COVID-19 vaccine in the Kingdom of Saudi Arabia: an actual operation warp speed. J Nat Sci Med. 2021;4(2):92.
15. Fayed AA, Al Shahrani AS, Almanea LT, et al. Willingness to receive the COVID-19 and seasonal influenza vaccines among the Saudi population and vaccine uptake during the initial stage of the national vaccination campaign: a cross-sectional survey. Vaccines. 2021;9(7):765. doi:10.3390/vaccines9070765
16. Arashkia A, Jalilvand S, Mohajel N, et al. Severe acute respiratory syndrome‐coronavirus‐2 spike (S) protein based vaccine candidates: state of the art and future prospects. Rev Med Virol. 2021;31(3):e2183. doi:10.1002/rmv.2183
17. Larson HJ, Cooper LZ, Eskola J, Katz SL, Ratzan S. Addressing the vaccine confidence gap. Lancet. 2011;378(9790):526–535. doi:10.1016/S0140-6736(11)60678-8
18. Bono SA, Faria de Moura Villela E, Siau CS, et al. Factors affecting COVID-19 vaccine acceptance: an international survey among low-and middle-income countries. Vaccines. 2021;9(5):515. doi:10.3390/vaccines9050515
19. Al-Qahtani WS, Alsafhi FA. A commentary on realities of developing COVID-19 vaccines discussed through the global health safety perspective. Vaccines. 2021;9(3):274. doi:10.3390/vaccines9030274
20. World Health Organization. Evaluation of COVID-19 vaccine effectiveness: interim guidance. World Health Organization; 2021.
21. Lynn MR. Determination and quantification of content validity. Nurs Res. 1986;35(6):382–386. doi:10.1097/00006199-198611000-00017
22. El Bilbeisi AH, Hosseini S, Djafarian K. Association of dietary patterns with diabetes complications among type 2 diabetes patients in Gaza Strip, Palestine: a cross-sectional study. J Health. 2017;36(1):1–11.
23. Dal-Ré R, Caplan AL, Gluud C, Porcher R. Ethical and scientific considerations regarding the early approval and deployment of a COVID-19 vaccine. Am Coll Phys. 2021;174:258–260.
24. PHA. Interim guidelines for the use of SARS-CoV-2 vaccine. Public Health Authority; 2021. Available from: https://covid19.cdc.gov.sa/professionals-health-workers/interim-guidelines-for-the-use-of-sars-cov-2-vaccine/.
25. Dubé E, Laberge C, Guay M, Bramadat P, Roy R, Bettinger JA. Vaccine hesitancy: an overview. Hum Vaccin Immunother. 2013;9(8):1763–1773. doi:10.4161/hv.24657
26. Alfageeh EI, Alshareef N, Angawi K, Alhazmi F, Chirwa GC. Acceptability of a COVID-19 vaccine among the Saudi population. Vaccines. 2021;9(3):226. doi:10.3390/vaccines9030226
27. Polack FP, Thomas SJ, Kitchin N, et al. Safety and efficacy of the BNT162b2 mRNA Covid-19 vaccine. N Engl J Med. 2020;383:2603–2615. doi:10.1056/NEJMoa2034577
28. Voysey M, Clemens SAC, Madhi SA, et al. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: an interim analysis of four randomized controlled trials in Brazil, South Africa, and the UK. Lancet. 2021;397(10269):99–111.
29. Alhazmi A, Alamer E, Daws D, et al. Evaluation of side effects associated with COVID-19 vaccines in Saudi Arabia. Vaccines. 2021;9(6):674. doi:10.3390/vaccines9060674
30. Adam M, Gameraddin M, Alelyani M, et al. Evaluation of post-vaccination symptoms of two common COVID-19 vaccines used in Abha, Aseer Region, Kingdom of Saudi Arabia. Patient Prefer Adherence. 2021;15:1963. doi:10.2147/PPA.S330689
31. Menni C, Klaser K, May A, et al. Vaccine side-effects and SARS-CoV-2 infection after vaccination in users of the COVID symptom study app in the UK: a prospective observational study. Lancet Infect Dis. 2021;21(7):939–949. doi:10.1016/S1473-3099(21)00224-3
32. El-Shitany NA, Harakeh S, Badr-Eldin SM, et al. Minor to moderate side effects of Pfizer-BioNTech COVID-19 vaccine among Saudi residents: a retrospective cross-sectional study. Int J Gen Med. 2021;14:1389. doi:10.2147/IJGM.S310497
33. Ramasamy MN, Minassian AM, Ewer KJ, et al. Safety, and immunogenicity of ChAdOx1 nCoV-19 vaccine administered in a prime-boost regimen in young and old adults (COV002): a single-blind, randomized, controlled, Phase 2/3 trial. Lancet. 2020;396(10267):1979–1993. doi:10.1016/S0140-6736(20)32466-1
34. Funk CD, Laferrière C, Ardakani A. Target product profile analysis of COVID-19 vaccines in Phase III clinical trials and beyond an early 2021 perspective. Viruses. 2021;13(3):418. doi:10.3390/v13030418
35. Notarte KI, Catahay JA, Peligro PJ, et al. Humoral response in hemodialysis patients post-SARS-CoV-2 mRNA vaccination: a systematic review of literature. Vaccines. 2023;11(4):724. doi:10.3390/vaccines11040724
36. Notarte KI, Guerrero‐Arguero I, Velasco JV, et al. Characterization of the significant decline in humoral immune response six months post‐SARS‐CoV‐2 mRNA vaccination: a systematic review. J Med Virol. 2022;94(7):2939–2961. doi:10.1002/jmv.27688
37. Notarte KI, Ver AT, Velasco JV, et al. Effects of age, sex, serostatus, and underlying comorbidities on humoral response post-SARS-CoV-2 Pfizer-BioNTech mRNA vaccination: a systematic review. Crit Rev Clin Lab Sci. 2022;59(6):373–390. doi:10.1080/10408363.2022.2038539
38. Umakanthan S, Patil S, Subramaniam N, Sharma R. COVID-19 vaccine hesitancy and resistance in India explored through a population-based longitudinal survey. Vaccines. 2021;9(10):1064. doi:10.3390/vaccines9101064
39. Umakanthan S, Lawrence S. Predictors of COVID-19 vaccine hesitancy in Germany: a cross-sectional, population-based study. Postgrad Med J. 2022;98(1164):756–764. doi:10.1136/postgradmedj-2021-141365
40. Umakanthan S, Bukelo MM, Gajula SS. The Commonwealth Caribbean COVID-19: regions resilient pathway during pandemic. Front Public Health. 2022;10:844333. doi:10.3389/fpubh.2022.844333
41. Melanson SE, Zhao Z, Kumanovics A, et al. Tolerance for three commonly administered COVID-19 vaccines by healthcare professionals. Front Public Health. 2022;10:975781. doi:10.3389/fpubh.2022.975781
42. Notarte KI, Catahay JA, Velasco JV, et al. Impact of COVID-19 vaccination on the risk of developing long-COVID and on existing long-COVID symptoms: a systematic review. EClinicalMedicine. 2022;53:101624. doi:10.1016/j.eclinm.2022.101624
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Clinical Characteristics, Outcomes and Prognostic Factors for Critical Illness in Hospitalized COVID-19 Patients in Saudi Arabia: A Retrospective Cohort Study
El-Kady AM, Aldakheel FM, Allemailem KS, Almatroudi A, Dbas Alharbi R, Al Hamed H, Alsulami M, Alshehri WA, El-Ashram S, Kreys E, Mohamed K, Al-Megrin WAI, Elshabrawy HA
International Journal of General Medicine 2022, 15:6945-6963
Published Date: 31 August 2022
COVID-19 Vaccination Breakthrough Infections in a Real-World Setting: Using Community Reporters to Evaluate Vaccine Effectiveness
Reynolds MW, Xie Y, Knuth KB, Mack CD, Brinkley E, Toovey S, Dreyer NA
Infection and Drug Resistance 2022, 15:5167-5182
Published Date: 3 September 2022
Distinct Features of Vascular Diseases in COVID-19
Ceasovschih A, Sorodoc V, Shor A, Haliga RE, Roth L, Lionte C, Onofrei Aursulesei V, Sirbu O, Culis N, Shapieva A, Tahir Khokhar MA, Statescu C, Sascau RA, Coman AE, Stoica A, Grigorescu ED, Banach M, Thomopoulos C, Sorodoc L
Journal of Inflammation Research 2023, 16:2783-2800
Published Date: 6 July 2023
Dietary Supplement Consumption and Mental Health in Indonesian Adults During Second Wave of COVID-19 Pandemic
Yusof J, d'Arqom A, Andriani AP, Nasution MZ, Fatimah N, Mustika A, Handayani S, Syed Abdul Kadir SZ
Patient Preference and Adherence 2023, 17:1799-1811
Published Date: 24 July 2023
Knowledge, Attitude and Practice Toward Artificial Intelligence Among Healthcare Workers in Private Polyclinics in Jeddah, Saudi Arabia
Serbaya SH, Khan AA, Surbaya SH, Alzahrani SM
Advances in Medical Education and Practice 2024, 15:269-280
Published Date: 5 April 2024