")
Back to Journals » ClinicoEconomics and Outcomes Research » Volume 13
Evaluation of the Cost-Effectiveness of Iron Formulations for the Treatment of Iron Deficiency Anaemia in Patients with Inflammatory Bowel Disease in the UK
Authors Aksan A, Beales ILP, Baxter G, Ramirez de Arellano A, Gavata S, Valentine WJ, Hunt B
Received 19 March 2021
Accepted for publication 6 May 2021
Published 17 June 2021 Volume 2021:13 Pages 541—552
DOI https://doi.org/10.2147/CEOR.S306823
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Dean Smith
Aysegül Aksan,1,2 Ian LP Beales,3 Garth Baxter,4 Antonio Ramirez de Arellano,5 Simona Gavata,6 William J Valentine,7 Barnaby Hunt7
1Interdisciplinary Crohn Colitis Centre, Rhein-main, Frankfurt/Main, Germany; 2Institute of Nutritional Science, Justus-Liebig University, Giessen, Germany; 3Department of Gastroenterology, Norfolk and Norwich University Hospital, Norwich, UK; 4Vifor Pharma Group, HEOR, London, UK; 5Vifor Pharma Group, HEOR, Glattbrugg, Switzerland; 6Vifor Pharma Group, Market Access, Glattbrugg, Switzerland; 7Ossian Health Economics and Communications, Basel, Switzerland
Correspondence: Antonio Ramirez de Arellano
Vifor Pharma Group, HEOR, Flughofstrasse 61, Glattbrugg, 8152, Switzerland
Tel +41 58 851 82 43
Email [email protected]
Introduction: In patients with inflammatory bowel disease (IBD), iron deficiency anaemia (IDA) can impair quality of life and increase healthcare costs. Treatment options for IDA-associated IBD include oral iron and intravenous iron formulations (such as ferric carboxymaltose [FCM], ferric derisomaltose [FD, previously known as iron isomaltoside 1000], and iron sucrose [IS]). The present analysis compared the cost-effectiveness of FCM versus FD, IS, and oral iron sulfate in terms of additional cost per additional responder in the UK setting.
Methods: Cost-effectiveness was calculated for FCM versus FD, IS, and oral iron individually in terms of the additional cost per additional responder, defined as haemoglobin normalisation or an increase of ≥ 2 g/dL in haemoglobin levels, in a model developed in Microsoft Excel. Relative efficacy inputs were taken from a previously published network meta-analysis, since there is currently no single head-to-head trial evidence comparing all therapy options. Costs were calculated in 2020 pounds sterling (GBP) capturing the costs of iron preparations, healthcare professional time, and consumables.
Results: The analysis suggested that FCM may be the most effective intervention, with 81% of patients achieving a response. Response rates with FD, IS, and oral iron were 74%, 75%, and 69%, respectively. Total costs with FCM, FD, IS, and oral iron were GBP 296, GBP 312, GBP 503, and GBP 56, respectively. FCM was found to be more effective and less costly than both FD and IS, and therefore was considered dominant. Compared with oral iron, FCM was associated with an incremental cost-effectiveness ratio of GBP 2045 per additional responder.
Conclusions: FCM is likely to be the least costly and most effective IV iron therapy in the UK setting. Compared with oral iron, healthcare payers must decide whether the superior treatment efficacy of FCM is worth the additional cost.
Keywords: cost, cost-effectiveness, inflammatory bowel disease, iron deficiency anaemia, United Kingdom
A Letter to the Editor has been published for this article.
Introduction
The UK has the second highest prevalence of inflammatory bowel disease (IBD) in the world at 449.6 cases per 100,000 population, second only to the USA (464.5 cases per 100,000 population).1 IBD is an umbrella term covering specific chronic inflammatory diseases of the digestive tract; Crohn’s disease, ulcerative colitis and a smaller group with more undifferentiated or overlapping features. The prevalence of IBD is growing rapidly, with an 84% increase between 1990 and 2017 in the UK.1 The most frequent complication of IBD is anaemia, which has been shown to have far-reaching negative impacts on cognitive function and quality of life.2,3 In most cases, IBD-associated anaemia arises due to a combination of iron deficiency anaemia (IDA) and anaemia of inflammation.4 Iron deficiency is present in 36–90% of the patients with IBD-associated anaemia.5 Iron deficiency and IDA arise mainly as a result of chronic blood loss from the intestinal mucosa, impaired gastrointestinal absorption (due to inflammation, the impact of drugs used to treat IBD, persisting infection, and short bowel syndrome), and reduced dietary intake due to reduced appetite.6,7 In patients with IBD, IDA can substantially impair diverse aspects of quality of life, including physical, emotional, and cognitive functions, reduce ability to work, increase hospitalisation rates and increase healthcare costs.8
According to guidelines published by the European Crohn’s and Colitis Organisation (ECCO) and a review of guidelines published by Kaitha et al, the goals of iron supplementation therapy in patients with IBD and IDA are to replenish iron stores (serum ferritin >100 g/L); to normalise the levels of haemoglobin (Hb), serum ferritin and transferrin saturation; to avoid the need for blood transfusion, and to improve quality of life.9,10 Treatment options for IBD-associated IDA include oral and intravenous (IV) iron products. Oral iron is indicated for patients with mild anaemia and clinically inactive disease, who have not previously shown intolerance to oral iron.9 While oral iron is inexpensive and practical for home use, it has been found to have limited efficacy, especially as intestinal iron absorption may be impaired due to the underlying IBD, and is known to cause side effects (including abdominal pain, nausea, bloating and diarrhoea) which limit patient adherence to therapy. Moreover, unabsorbed iron can cause mucosal damage and oxidative stress in the intestinal tract, and thus potentially exacerbate IBD.5 The use of oral iron has also been shown to have a negative effect on the microbiome of the gut, compared with treatment of IDA subsequent to IBD with IV iron therapy.11 IV iron formulations are indicated for patients with severe anaemia (Hb <10 g/dL), those showing an intolerance or lack of response to oral iron, those with active IBD, where there is a need for a quicker response to treatment, or where longer-term iron supplementation is required.9,10 Compared with oral iron, IV iron therapy has been shown to be have greater efficacy in terms of iron replenishment. Furthermore, it has no gastrointestinal side effects, and can therefore be administered in patients with an IBD flare. However, IV administration of iron in the UK is generally only possible in a hospital setting, and although adverse reactions to modern IV iron formulations are rarely severe, there is a requirement for ready access to resuscitation equipment.9 In the UK, currently available IV iron formulations include ferric carboxymaltose (FCM) (Ferinject®, Vifor Pharma Group), ferric derisomaltose (previously known as iron isomaltoside 1000) (FD), (Monofer®, Pharmacosmos A/S), and iron sucrose (IS) (Venofer®, Vifor Pharma Group).
Since the recommended doses and dosing frequencies of the available IV iron formulations differ, as described in the respective Summaries of Product Characteristics (SmPCs), dosing patterns and schedules differ in clinical practice. With FCM, doses of up to 1000 mg iron can be delivered in a single infusion.12 When FD is used, the dose that can be administered per infusion is based on the patient’s body weight, with a limit of 20 mg of iron per kg body weight (eg a dose of 1000 mg can be delivered in a patient weighing 50 kg, but 1200 mg can be delivered in a patient weighing 60 kg).13 Dosing with IS is restricted to a maximum dose of 200 mg iron per infusion.14 While studies have assessed FCM versus IS, and each of FCM, FD, and IS, individually, versus oral iron, no single study has evaluated all treatment options in a single population.15–19 However, the five existing randomised controlled trials (RCTs) of FCM, FD, IS and oral iron for treatment of patients with IDA subsequent to IBD were compared by Aksan et al in a network meta-analysis (NMA), with outcomes adjusted to take into account differing trial populations and study designs.20 Using a dichotomous variable for treatment response (normalisation of Hb levels or an increase of ≥2 g/dL in Hb), in line with the treatment goals stated in current ECCO guidelines, FCM was shown to be associated with a significantly greater response rate than oral iron (Table 1). FD and IS were associated with a non-statistically significant increase in responder rates versus oral iron. When the IV iron formulation were compared, no statistically significant difference was observed. However, rank probability assessment found that there was an 83% probability that FCM was the most effective treatment, with a 14% probability that FD was the most effective treatment.
 |
Table 1 Treatment Efficacy: Odds Ratio for Response Rate |
As the National Health Service (NHS) comes under increasing pressure, it is important to choose therapies that are both effective and good value for money, with the aim of maximizing healthcare gains despite constrained financial resources. The National Institute for Health and Care Excellence (NICE) recommends the use of cost-utility analyses.21 Quality-adjusted life expectancy and direct costs associated with an intervention and a comparator are projected, and the incremental cost-effectiveness ratio (ICER) is calculated, expressed as the additional cost per additional quality-adjusted life year (QALY) gained. To date, however, data linking IDA therapies to quality-adjusted life expectancy are lacking. Where cost-utility analysis is not possible, NICE recommends that cost-effectiveness analyses are conducted using “natural units”.21 For example, the cost-effectiveness of screening programs are often evaluated based on “cost per case detected”, and fertility treatments often using “cost per live birth”.22,23 In IDA, the “natural unit” can be considered to be a patient who responds to treatment. While willingness to pay thresholds are not available in terms of additional cost per additional responder, this approach provides valuable information on the relative cost-effectiveness of treatments for IBD-associated IDA.
A previously published budget impact analysis of IV iron formulations for the treatment of IDA in patients with IBD in the UK assumed that all IV iron formulations the same clinical efficacy.24 However, as described above, the NMA suggests that this may not be the case.20 The aim of the present analysis was to calculate the cost-effectiveness of FCM versus FD, IS, and oral iron in terms of additional cost per additional responder for the treatment of IBD-associated IDA in the UK setting, based on the demonstrated variances in clinical efficacy of different iron formulations in an IBD population.20
Methods
Modelling Approach
The percentage of patients with IBD and IDA achieving a response, defined according to ECCO guidelines as Hb normalisation or an increase of ≥2 g/dL in Hb levels, and costs of treatment with FCM, FD, IS and oral iron over one cycle of treatment in the UK setting were assessed in a cost-effectiveness model developed in Microsoft Excel. Since a lower baseline Hb is associated with a faster and greater increase in Hb value, a continuous variable such as mean Hb increase may be influenced by baseline Hb levels. The choice of a dichotomous variable (ie, response versus no response) reduces this effect and is therefore a better parameter for a model to predict efficacy.
The cost-effectiveness model took a probabilistic approach, with a cohort of patients with IBD and IDA generated by sampling patient characteristics (Hb and weight) from defined distributions. The use of sampling in this approach, rather than simply using mean values, allows the uncertainty around differences in the efficacy between the treatment arms to be captured based on the NMA published by Aksan et al (see the “Efficacy Calculation” section), as well as generating a representative cohort of patients, each with differing characteristics who therefore would require differing doses of iron, resulting in differing costs of treatment (see the “Cost Calculation” section). A total of 5000 modelled patients were evaluated, with all inputs resampled for each generated patient, as calculated results were stable at this number of iterations. No discounting was applied to the calculated outcomes, as all projections were within a 1-year time horizon (discounting aims to adjust future costs and outcomes of health‐care interventions to “present value”, and this was not required as projections over the long term were not made25). The analysis was conducted and reported in line with the Consolidated Health Economic Evaluation Reporting Standards (CHEERS) guidelines.26
Efficacy Calculation
The percentage of patients achieving a response (Hb normalisation or an increase of ≥2 g/dL in Hb levels) in the FCM arm was calculated by taking a weighted average of the two RCTs of FCM included in the previously published NMA.20 These RCTs were reported by Evstatiev et al in 2011 and Kulnigg et al in 2008.15,16 Across the two studies, a total of 81% of the patients receiving FCM were classified as responders. In each iteration of the modelling analysis, this percentage was sampled based on a standard deviation of 2.1%, derived assuming a binomial proportion confidence interval. The percentages of patients achieving a response with FD, IS and oral iron were calculated by applying an odds ratio for each comparator versus FCM, sampled based on the mean and 95% credible interval (CI) calculated by Aksan et al, using a normal distribution (Table 1). This captured the full range of the difference identified in the NMA. The mean and standard deviation (SD) of patients achieving a response across all model iterations were calculated for FCM, FD, IS and oral iron. Number needed to treat, expressed as the number of patients who would need to be treated with FCM instead of the comparator in order to achieve one additional responder, was calculated by taking the reciprocal of the differences between the number of responders with FCM and with the comparator. Number needed to treat values are conventionally rounded up to the next integer value.
Cost Calculation
All costs included in the analysis were captured in 2020 pounds sterling (GBP). To calculate the cost of treating IDA in patients with IBD using IV iron, the required iron dose was calculated based on the patient’s body weight and Hb level by employing the simplified dosing table as recommended in the ECCO anaemia guidelines (Table 2).9,12 Alternative methods of calculating the iron dose were explored in scenario analyses (see below).
 |
Table 2 Simplified Dosing Table |
 |
Table 3 Resource Use Associated with Infusion of IV Iron Formulations |
 |
Table 4 Pack Contents and Pack Costs of IV Iron Formulations |
In each model iteration, the patient body weight and Hb were sampled based on the RCTs of FCM.15,16 Mean body weight was 66.6 kg (standard error of 0.7 kg) and mean Hb was 9.6 g/dL (standard error of 0.1 g/dL). For example, the mean patient would require an iron dose of 1,500 mg. The required iron dose for each sampled patient was then used to calculate the required number of infusions with FCM, FD, and IS according to the different specified dosing schedules outlined in the SmPC of each formulation (see above).
The cost of each infusion was calculated using a micro-costing approach (adding together the unit costs of all medical resources used) taking into account the pharmacy cost of the respective iron product, the healthcare professional time required to deliver the infusion (based on the SmPC for each product, capturing preparation time, infusion time and post-infusion supervision), and consumables required to deliver the infusion (giving sets, cannula and dressings) (Table 3). Therefore, costs were assessed from an NHS Hospital Trust perspective. In the modelling analysis, it was assumed that clinicians chose the most appropriate vial or combination of vials to deliver the required iron dose at the lowest possible cost, taking into account wastage if the entire contents of a vial were not administered (Table 4).27 The total cost of a course of IV iron treatment was calculated as the sum of the costs of all required infusions. Costs associated with oral iron were calculated based on an appointment with a general practitioner, a laboratory blood test, and an 84-day course of 100 mg oral ferrous sulfate twice daily.27–29 This dosing schedule was chosen to match the oral iron dosing schedule in the RCT comparing FCM with oral iron captured in the NMA.16 Other studies used alternative oral iron treatment regimens. The study which compared IS with oral iron used a dosing schedule of 100 mg of ferrous sulfate twice daily (ie, 200 mg per day) for 20 weeks. However, the studies comparing ISM and IS with oral iron prescribed patients 100−200 mg of ferrous sulfate per day for 8 weeks. Therefore, the chosen treatment regimen reflected the average of the trials included in the NMA.
Cost-Effectiveness Calculation
Cost-effectiveness was calculated for FCM versus FD, IS, and oral iron individually in terms of the additional cost per additional responder, to give an ICER. For each comparator in turn, the mean cost of treatment with the intervention was subtracted from the mean cost of treatment with FCM, and the mean percentage of patients achieving a response with the comparator was subtracted from the mean percentage of patients achieving a response with FCM. The difference in cost was then divided by the difference in the percentage of responders. In an economic evaluation, an intervention that is both clinically superior and cost-saving is referred to as an economically “dominant” strategy versus the comparator. Therefore, in comparisons where FCM was associated with an increased response rate and cost savings, no calculation of an ICER was required, since the decision-making process for a healthcare payer would be clear.
Scenario Analyses
A series of scenario analyses were performed, capturing alternative methods of estimating the iron deficit. As an alternative to the simplified dosing table, the Ganzoni formula can be used to estimate the required iron dose. The formula takes into account patient body weight, Hb, target Hb and iron stores. For simplicity and in line with convention in clinical practice, iron stores were assumed to be 500 mg and target Hb was assumed to be 15 mg/dL in all patients. For example, the mean patient with body weight of 66.6 kg and Hb of 9.6 g/dL would require an iron dose of 1,363 mg:
Iron deficit = body weight * (target Hb - Hb) * 2.4 + iron stores
In scenario analysis 1, the Ganzoni formula was applied in all IV iron arms. In scenario analysis 2, the Ganzoni formula was applied only in the FD and IS arms, based on the fact that the SmPC for FD recommends use of the Ganzoni formula in patients with anaemia due to bleeding, as is the case in IBD, and the SmPC for IS recommends use of the Ganzoni formula for all patients.13,14
Sensitivity Analyses
In addition to the scenario analyses, a number of sensitivity analyses were prepared to assess the robustness of the modelled results and how variation in model inputs affected the calculated outcomes. To assess the impact of uncertainty in the outcomes of the NMA on which the study was based, analyses were performed with the upper and lower 95% CIs of the odds ratios for achieving a response with the comparator versus FCM.
Body weight is a key factor in determining the iron dose required, and also in determining the dose of FD that can be delivered in a single infusion. Therefore, a sensitivity analysis was performed with mean body weight increased by 10 kg to 76.6 kg. This moves the mean body weight into the higher weight category within the simplified dosing table. Two additional analyses were performed with the mean Hb level increased and decreased by 1 g/dL, respectively, in order to evaluate the impact of variation in IDA severity on cost-effectiveness outcomes.
Compliance with Ethics Guidelines
This article is based on previously conducted studies and does not contain any studies with human participants or animals performed by any of the authors.
Results
Base Case Analysis
Based on the previously published NMA, FCM was found to be the most effective intervention, with 81% (SD 2%) of patients with IBD-associated IDA achieving a response (Table 5). FD and IS were similarly effective, with response rates of 74% (SD 6%) and 75% (SD 4%), respectively. Oral iron was the least effective therapy, with 69% (SD 4%) of patients achieving a response. When expressed as number needed to treat, 16, 17 and 9 patients would need to switch treatment from FD, IS and oral iron, respectively, to achieve one additional responder (Figure 1).
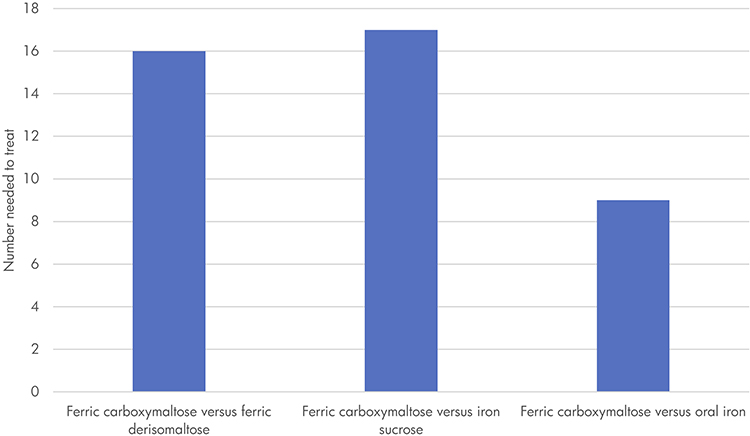 |
Figure 1 Number needed to treat to bring achieve one additional responder with ferric carboxymaltose versus other therapy options. Number needed to treat was expressed as the number of patients who would need to be treated to with ferric carboxymaltose instead of the comparator in order achieve one additional responder. Number needed to treat values are conventionally rounded up to the next integer value. Only the difference between the efficacy of FCM and oral iron was based on a statistically significant difference in the model input. |
In order to deliver the required mean dose of 1,441 mg (SD 431), a mean of 1.7 (SD 0.5) infusions were required with FCM, a mean of 1.6 (SD 0.5) infusions were required with FD, and a mean of 7.5 (SD 1.1) infusions were required with IS (Table 5). Total treatment costs for FCM amounted to GBP 296 (SD GBP 81), compared with total costs of GBP 312 (SD GBP 88) for FD, GBP 503 (SD GBP 147) for IS, and GBP 56 (SD GBP 0) for oral iron. Therefore, FCM was associated with cost savings of GBP 16 when compared with FD, and of GBP 206 when compared with IS (Table 5). However, FCM therapy was associated with increased costs of GBP 240 versus oral iron. Cost savings associated with FCM resulted from a lower unit cost per mg of infused iron versus FD, and from fewer infusions, and consequently reduced hospital-based healthcare professional time and use of consumables versus IS.
 |
Table 5 Results of the Base Case Modelling Analysis |
In terms of cost-effectiveness, FCM was found to be more effective and less costly than both FD and IS. Therefore, no ICERs were calculated and FCM was considered dominant versus both FD and IS. Compared with oral iron, FCM was associated with a greater response rate but also increased costs, yielding an ICER of GBP 2,045 per additional responder. FD was associated with an ICER of GBP 5146 per additional responder versus oral iron, with IS associated with ICERs of GBP 29,161 and GBP 7940 per additional responder versus FD and oral iron, respectively. A cost-effectiveness scatterplot is presented in Figure 2, showing the variation in results due to the sampling of model inputs.
 |
Figure 2 Scatterplot of the base case results. GBP, 2020 pounds sterling. Response was defined as a patient who achieved normalisation of haemoglobin levels or an increase in haemoglobin of ≥2 g/dL. |
Scenario Analysis
Application of the Ganzoni formula to estimate the required iron dose in place of the simplified dosing table resulted in lower doses of iron than in the base case analysis. Therefore, mean costs fell in all treatment arms. Effectiveness outcomes remained unchanged from the base case analysis, with FCM more effective than FD, IS and oral iron. In scenario 1, FCM remained more effective and less costly than FD and IS (Table 6). When the respective recommended dosing schemes for each product (simplified dosing table for FCM and Ganzoni formula for FD and IS) were applied in scenario 2, FCM remained more effective and less costly than both FD and IS.
 |
Table 6 Scenario Analysis Results |
Sensitivity Analyses
When alternative model inputs were applied in sensitivity analyses, results remained similar to the base case analysis (Table 7). Applying the upper 95% CI of the odds ratio for achieving a response with each of FD, IS and oral iron versus FCM resulted in increased response rates of 86%, 81% and 79%, respectively, while the percentage of responders with FCM therapy remained unchanged from the base case (81%). Use of the lower 95% CI had the converse effect, with the response rates falling with FD (59%), IS (67%) and oral iron (58%). In these two analyses, costs were unchanged from the base case values, with FCM the least costly IV iron formulation, but more costly than oral iron.
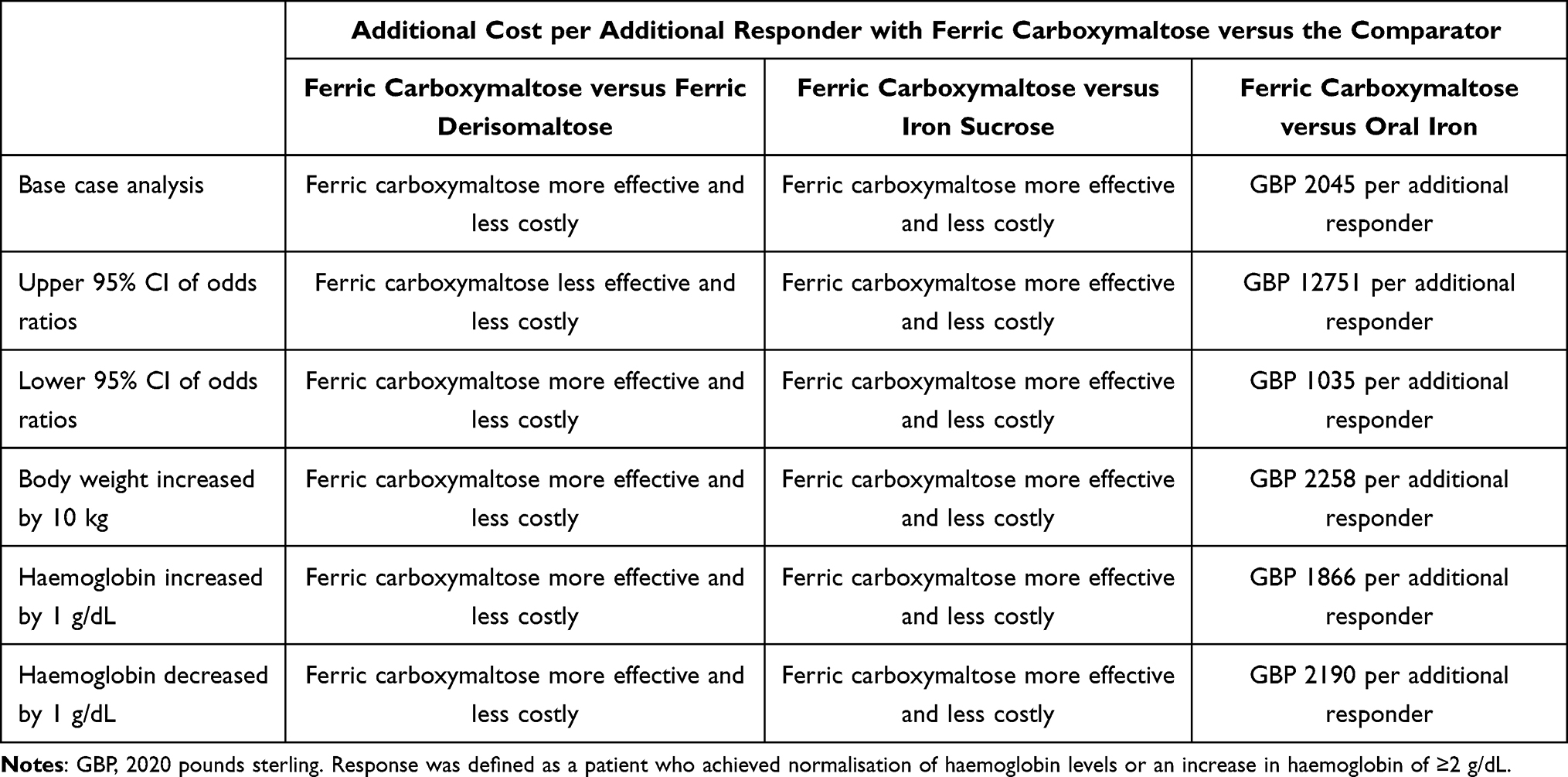 |
Table 7 Sensitivity Analysis Results |
Using a higher baseline body weight to calculate the iron requirement resulted in increased iron doses and therefore increased costs in all treatment arms. FCM remained more effective and less costly compared with FD and IS. Increasing the mean baseline Hb by 1 g/dL resulted in a lower dose of iron in all treatment arms. FCM remained more effective and less costly compared with both FD and IS, and was associated with an additional cost of GBP 1,866 per additional responder versus oral iron. Decreasing the mean baseline Hb by 1 g/dL did not notably change the result of the analysis from those generated in the base case.
Discussion
The present analysis suggests that the use of FCM to treat patients with IBD-related IDA is associated with an increased number of responders, defined as patients whose Hb levels are normalised or increased by ≥2 g/dL, compared with FD, IS and oral iron, based on a previously published NMA. Compared with FD, a course of treatment with FCM was associated with an increased number of infusions but reduced costs. In contrast, IS, with a maximum dose limited to 200 mg, requires multiple infusions, resulting in higher costs compared with the other IV iron formulations. Therefore, according to this analysis, FCM is likely to be the least costly and most effective IV iron therapy in the UK setting. While treatment costs with oral iron are comparatively low, there are other factors to be considered that make the decision-making process more nuanced. Healthcare payers must decide whether the superior treatment efficacy of FCM, and the consequent rapid improvement of anaemia, with its implications for hospitalisation rates, comorbidities and patient quality of life, is worth an additional cost of GBP 2045 per additional responder.8,9 However, it should also be borne in mind that oral iron intake can exacerbate IBD-associated inflammation and cause mucosal damage and gastrointestinal symptoms, with a considerable negative impact on both quality of life and treatment adherence. The choice of a cost-effective and rapid-acting therapy is especially relevant in patients with IBD-related IDA, since episodes of iron deficiency and anaemia frequently reoccur during renewed flares of inflammation and bleeding, and patients may, therefore, require long-term iron supplementation, with repeated courses of iron therapy.
As with all economic analyses, the strengths and weaknesses of the analysis must be evaluated to provide context. The clinical effectiveness inputs for the analysis were based on an NMA, since there is currently no single head-to-head trial evidence comparing all therapy options for treatment of patients with IDA and IBD in a single population.20 This use of indirect evidence could be considered a weakness, with the authors noting that health researchers should use rank probabilities cautiously when making important decisions. The efficacy of FCM and FD have been compared in an observational study of patients with IBD-associated IDA in Norway, with efficacy endpoints included as secondary endpoints, which identified no differences between the two IV iron formulations.30 While two identically designed, open-label RCTs with a pre-specified pooled analysis have directly compared FCM and FD (the first RCTs to directly compare the two interventions), in the majority of enrolled patients (68.5%), the cause of IDA was not IBD, but a gynaecological condition.31 Therefore, the results of this study have limited relevance to the population of patients with IBD-associated IDA. Further RCTs are required, which should specifically enrol patients with IBD-associated IDA.
The NMA used to inform the efficacy inputs of the present analysis has a number of limitations, which have been discussed previously, in both the original publication and in subsequent correspondence with the journal, including study design heterogeneity within the included trials, variation in patient characteristics, differences in iron dosing, and only five trials being included.20,32–35 Since all economic evaluations are dependent on the input data, factors affecting the reliability of the results of the NMA also affect the present analysis. The systematic review conducted by Aksan et al additionally extracted data on adverse events occurring in patients with IBD and IDA receiving iron supplementation therapy.20 Adverse event rates were low for all IV iron products, the most common being infusion site reactions, transient increases in liver enzymes, headache, hyperferritinaemia, and hypophosphataemia. A more recent NMA found that the overall incidence of adverse events was similar with all IV iron treatments, but the adverse events experienced most frequently differed.36 The most common adverse events with FCM and IS were headache and transient hyperferritinaemia, while the most comment adverse events with FD were flushing, hypersensitivity and hepatic enzyme increases. Future cost-effectiveness studies should look to capture the impact of adverse events on both cost and clinical outcomes. Healthcare decision makers must make evidence-based recommendations with imperfect information, and, in the absence of direct evidence, the NMA published by Aksan et al, despite its limitations, represents the best available evidence source on differences in clinical outcomes in patients with IBD-associated IDA receiving IV iron therapy.
The present analysis evaluated outcomes over one cycle of treatment and did not capture retreatment of patients with IDA. Retreatment may be required due to non-response to initial therapy, or due to recurrence of IDA, especially in the context of IBD-related inflammation and bleeding.37 Inclusion of retreatment due to non-response would have resulted in increased costs in all treatment arms. However, the impact would be greatest for the less effective therapies and smallest for the most effective treatment arms. Furthermore, inclusion of retreatment due to recurrence of IDA would be unlikely to have a substantial impact on the additional cost per additional responder, as additional treatment courses would result in similar costs and numbers of responders as a single cycle.
A previously published budget impact analysis for the UK setting found that FCM was more costly per patient over a 5-year time horizon than FD, with a retreatment period of 10 months.24 The present analysis, assessing clinical outcomes over a single cycle of treatment, found that FCM was associated with reduced costs compared with FD. The key differences between the two analyses that drive this variation in outcomes are likely to be the mean body weight and mean Hb used in the two analyses. The present analysis used a mean of body weight of 66.6 kg based on data from two RCTs, compared with 75.4 kg in the previously published analysis, and a mean Hb of 9.6 g/dL compared with 9.99 g/dL. Due to the differences in dosing recommendations, with FCM dosing limited to a maximum of 1,000 mg per infusion irrespective of body weight, while FD dosing is dependent on body weight (up to 20 mg/kg can be infused per infusion), a higher mean body weight and higher Hb in the analysed baseline cohort will favour FD over FCM. The present analysis presents similar data to the previously published budget impact analysis, but expands on it by also presenting clinical outcomes in terms of response rates. In the present analysis, by defining treatment response in line with ECCO guidelines as a dichotomous variable describing not only patients achieving a Hb increase of 2 g/dL but also those whose Hb levels returned to normal, it was possible to reduce the influence of Hb variances at baseline.
The results of cost-utility analyses that assess the additional cost per additional QALY gained can be compared with willingness to pay thresholds to evaluate whether a therapy represents good value for money, as the NHS aims to maximise health benefit within a constrained budget. This comparability across therapeutic areas is a key advantage of using the QALY as an outcome measure. However, no such thresholds exist for analyses assessing the additional cost per additional responder, and the present analysis is the first to use this approach to assess the cost-effectiveness of interventions for IDA in the UK. However, an additional cost per additional responder approach has been used in a number of other therapeutic areas in which quality-adjusted life expectancy cannot be used as an outcome measure, including IBD generally, rather than IDA and IBD. In a cost-effectiveness analysis of selenium-75-homocholic acid taurine (SeHCAT) for investigation of bile acid malabsorption in chronic diarrhoea, a responder was defined as a patient for whom diarrhoea resolved.38 Similar analyses have also been conducted to evaluate treatments for glioblastoma, rheumatoid and psoriatic arthritis, chronic obstructive pulmonary disease, chronic immune thrombocytopenia, psoriasis.39–43 These analyses provide a precedent for the present modelling approach, and provide some context to the results.
Conclusions
The present analysis is the first to assess the cost-effectiveness of available treatment options (IV and oral iron) for patients with IBD and IDA in the UK setting. This analysis found that FCM is likely to be the least costly and more effective IV iron therapy in the UK setting. Oral iron therapy is inexpensive, and it was confirmed to be less costly than all IV treatments analysed. However, oral iron compounds are often of limited efficacy, and are associated with frequent gastrointestinal side effects, and poor adherence in patients with IBD.20 Healthcare payers must decide whether the increased efficacy of FCM compared with oral iron, and the consequent rapid improvement of anaemia, with all its implications for comorbidities, hospitalisation rates and not least, patient quality of life and time lost from work, is worth the additional cost of GBP 2045 per additional responder.
Data Sharing Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Compliance with Ethics Guidelines
This article is based on previously conducted studies and does not contain any studies with human participants or animals performed by any of the authors.
Acknowledgments
The abstract of this paper was presented at Virtual ISPOR Europe 2020 as a poster presentation with interim findings. The poster’s abstract was published in Value in Health, volume 23, supplement 2, page S742: https://doi.org/10.1016/j.jval.2020.08.2012.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study was supported by funding from Vifor Pharma Group.
Disclosure
Aysegül Aksan has received consulting or speaker fees from the following Immundiagnostik and Vifor Pharma, and research funding from Immundiagnostik. Ian LP Beales has received fees for consulting and advisory boards from Vifor Pharma Group, Pharmacosmos UK Limited and Norgine Limited. Garth Baxter, Antonio Ramirez de Arellano and Simona Gavata are employees of Vifor Pharma Group. William J Valentine and Barnaby Hunt are employees of Ossian Health Economics and Communications, which received consulting fees from Vifor Pharma Group to support the preparation of the analysis. The authors report no other conflicts of interest in this work.
References
1. GBD 2017 Inflammatory Bowel Disease Collaborators. The global, regional, and national burden of inflammatory bowel disease in 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol Hepatol. 2020;5(1):17–30.
2. Gasche C. Complications of inflammatory bowel disease. Hepatogastroenterology. 2000;47(31):49–56.
3. Wells CW, Lewis S, Barton JR, Corbett S. Effects of changes in hemoglobin level on quality of life and cognitive function in inflammatory bowel disease patients. Inflamm Bowel Dis. 2006;12(2):123–130.
4. Stein J, Dignass AU. Management of iron deficiency anemia in inflammatory bowel disease - a practical approach. Ann Gastroenterol. 2013;26(2):104–113.
5. Kulnigg S, Gasche C. Systematic review: managing anaemia in Crohn’s disease. Aliment Pharmacol Ther. 2006;24(11–12):
6. Nielsen OH, Ainsworth M, Coskun M, Weiss G. Management of iron-deficiency anemia in inflammatory bowel disease: a systematic review. Medicine. 2015;94:e963.
7. Guagnozzi D, Lucendo AJ. Anemia in inflammatory bowel disease: a neglected issue with relevant effects. World J Gastroenterol. 2014;20:3542–3551.
8. Gomollón F, Gisbert JP. Anemia and inflammatory bowel diseases. World J Gastroenterol. 2009;15(37):4659–4665.
9. Dignass AU, Gasche C, Bettenworth D, et al. European Crohn’s and Colitis Organisation [ECCO]. European Consensus on the Diagnosis and Management of Iron Deficiency and Anaemia in Inflammatory Bowel Diseases. J Crohns Colitis. 2015;9(3):211–222.
10. Kaitha S, Bashir M, Ali T. Iron deficiency anemia in inflammatory bowel disease. World J Gastrointest Pathophysiol. 2015;6(3):62–72.
11. Lee T, Clavel T, Smirnov K, et al. Oral versus intravenous iron replacement therapy distinctly alters the gut microbiota and metabolome in patients with IBD. Gut. 2017;66(5):863–871.
12. Electronic Medicines Compendium. Ferinject (ferric carboxymaltose). Available from: https://www.medicines.org.uk/emc/product/5910/smpc.
13. Electronic Medicines Compendium. Monofer 100mg/mL solution for injection/infusion. Available from https://www.medicines.org.uk/emc/product/5676.
14. Electronic Medicines Compendium. Venofer (iron sucrose) 20 mg iron/mL, solution for injection or concentrate for solution for infusion. https://www.medicines.org.uk/emc/product/5911.
15. Evstatiev R, Marteau P, Iqbal T, et al.; FERGI Study Group. FERGIcor, a randomized controlled trial on ferric carboxymaltose for iron deficiency anemia in inflammatory bowel disease. Gastroenterology. 2011;141(3):
16. Kulnigg S, Stoinov S, Simanenkov V, et al. A novel intravenous iron formulation for treatment of anemia in inflammatory bowel disease: the ferric carboxymaltose (FERINJECT) randomized controlled trial. Am J Gastroenterol. 2008;103(5):1182–1192.
17. Lindgren S, Wikman O, Befrits R, et al. Intravenous iron sucrose is superior to oral iron sulphate for correcting anaemia and restoring iron stores in IBD patients: a randomized, controlled, evaluator-blind, multicentre study. Scand J Gastroenterol. 2009;44(7):838–845.
18. Reinisch W, Staun M, Tandon RK, et al. A randomized, open-label, non-inferiority study of intravenous iron isomaltoside 1,000 (Monofer) compared with oral iron for treatment of anemia in IBD (PROCEED). Am J Gastroenterol. 2013;108(12):1877–1888.
19. Schröder O, Mickisch O, Seidler U, et al. Intravenous iron sucrose versus oral iron supplementation for the treatment of iron deficiency anemia in patients with inflammatory bowel disease–a randomized, controlled, open-label, multicenter study. Am J Gastroenterol. 2005;100(11):2503–2509.
20. Aksan A, Işık H, Radeke HH, Dignass A, Stein J. Systematic review with network meta-analysis: comparative efficacy and tolerability of different intravenous iron formulations for the treatment of iron deficiency anaemia in patients with inflammatory bowel disease. Aliment Pharmacol Ther. 2017;45(10):1303–1318.
21. National Institute for Health and Care Excellence. Developing NICE guidelines: the manual: 7 Incorporating economic evaluation Available from: https://www.nice.org.uk/process/pmg20/chapter/incorporating-economic-evaluation.
22. Khunti K, Gillies CL, Taub NA, et al. A comparison of cost per case detected of screening strategies for Type 2 diabetes and impaired glucose regulation: modelling study. Diabetes Res Clin Pract. 2012;97(3):505–513.
23. Katz P, Showstack J, Smith JF, et al. Costs of infertility treatment: results from an 18-month prospective cohort study. Fertil Steril. 2011;95(3):915–921.
24. Pollock RF, Muduma G. Intravenous iron treatments for iron deficiency anemia in inflammatory bowel disease: a budget impact analysis of iron isomaltoside 1000 (Monofer) in the UK. Expert Opin Drug Deliv. 2017;14(12):1439–1446.
25. Severens JL, Milne RJ. Discounting health outcomes in economic evaluation: the ongoing debate. Value Health. 2004;7(4):397–401.
26. Husereau D, Drummond M, Petrou S, et al.; CHEERS Task Force. Consolidated Health Economic Evaluation Reporting Standards (CHEERS) statement. Value Health. 2013;16(2):e1–5.
27. National Institute for Health and Care Excellence. British National Formulary. Available from: www.nice.org.uk/bnf. Accessed
28. Curtis L, Burns A. Unit Costs of Health and Social Care 2019, Personal Social Services Research Unit. Canterbury: University of Kent; 2018. doi:10.22024/UniKent/01.02.79286
29. National Institute for Health and Care Excellence. Implementing the NICE guideline on anaemia management in people with chronic kidney disease (NG8). Available from: https://www.nice.org.uk/guidance/ng8/resources/costing-statement-pdf-72504685.
30. Detlie TE, Lindstrøm JC, Jahnsen ME, et al. Incidence of hypophosphatemia in patients with inflammatory bowel disease treated with ferric carboxymaltose or iron isomaltoside. Aliment Pharmacol Ther. 2019;50(4):397–406.
31. Wolf M, Rubin J, Achebe M, et al. Effects of iron isomaltoside vs ferric carboxymaltose on hypophosphatemia in iron-deficiency anemia: two randomized clinical trials. JAMA. 2020;323(5):432–443.
32. Kennedy NA, Goodhand JR, Rampton DS. Editorial: which iron preparation for patients with IBD? Aliment Pharmacol Ther. 2017;46(2):194–195.
33. Aksan A, Işık H, Radeke HH, Dignass A, Stein J. Editorial: which iron preparation for patients with IBD? Authors’ reply. Aliment Pharmacol Ther. 2017;46(2):195–196.
34. Reinisch W, Lindgren S. Letter: the importance of dosing and baseline haemoglobin when establishing the relative efficacy of intravenous iron therapies. Aliment Pharmacol Ther. 2017;46(7):704–705.
35. Aksan A, Işık H, Radeke HH, Dignass A, Stein J. Letter: the importance of dosing and baseline haemoglobin when establishing the relative efficacy of intravenous iron therapies-authors’ reply. Aliment Pharmacol Ther. 2017;46(7):705–706.
36. Aksan A, Işık H, Aksan S, Tuğal D, Dignass A, Stein JM. P585 Evaluation and comparison of the safety profiles of different intravenous iron preparations and oral iron for treatment of iron deficiency anaemia: preliminary results from the IBD subgroup analysis. J Crohn’s Colitis. 2020;14(Supplement_1):S490–S490.
37. Kulnigg S, Teischinger L, Dejaco C, Waldhör T, Gasche C. Rapid recurrence of IBD-associated anemia and iron deficiency after intravenous iron sucrose and erythropoietin treatment. Am J Gastroenterol. 2009;104(6):1460–1467.
38. Riemsma R, Al M, Ramos I, et al. SeHCAT [tauroselcholic (selenium-75) acid] for the investigation of bile acid malabsorption and measurement of bile acid pool loss: a systematic review and cost-effectiveness analysis. Health Technol Assess. 2013;17(61).
39. Baguet T, Verhoeven J, De Vos F, Goethals I. Cost-effectiveness of [18F] fluoroethyl-L-tyrosine for temozolomide therapy assessment in patients with glioblastoma. Front Oncol. 2019;9:814.
40. Wehler E, Boytsov N, Nicolay C, Herrera-Restrepo O, Kowal S. A budget impact and cost per additional responder analysis for baricitinib for the treatment of moderate-to-severe rheumatoid arthritis in patients with an inadequate response to tumor necrosis factor inhibitors in the USA. Pharmacoeconomics. 2020;38(1):39–56.
41. Strand V, Elaine Husni M, Betts KA, et al. Network meta-analysis and cost per responder of targeted Immunomodulators in the treatment of active psoriatic arthritis. BMC Rheumatol. 2018;2:3.
42. Rajagopalan K, Bloudek L, Marvel J, Dembek C, Kavati A. Cost-effectiveness of twice-daily indacaterol/glycopyrrolate inhalation powder for the treatment of moderate to severe COPD in the US. Int J Chron Obstruct Pulmon Dis. 2018;13:3867–3877.
43. Armstrong AW, Betts KA, Sundaram M, Thomason D, Signorovitch JE. Comparative efficacy and incremental cost per responder of methotrexate versus apremilast for methotrexate-naïve patients with psoriasis. J Am Acad Dermatol. 2016;75(4):740–746.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.