Back to Journals » Advances in Medical Education and Practice » Volume 16
Evaluation of the Application of a Dental Virtual Simulator to Pre-Clinical Pediatric Dental Training
Authors Guo Y, Wang W, Li J ![]() , Gan Y, Wu X, Huang J, Xu H
, Gan Y, Wu X, Huang J, Xu H
Received 17 May 2025
Accepted for publication 22 October 2025
Published 7 November 2025 Volume 2025:16 Pages 2029—2041
DOI https://doi.org/10.2147/AMEP.S518434
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Md Anwarul Azim Majumder
Yidan Guo,1,* Wenjun Wang,1,* Jing Li,1 Yena Gan,2,3 Xiaoran Wu,1 Jinwei Huang,4 He Xu1
1Department of Pediatric Dentistry, Peking University School and Hospital of Stomatology, Beijing, People’s Republic of China; 2Clinical Comprehensive Evaluation Group, International Research Center for Medicinal Administration, Peking University, Beijing, People’s Republic of China; 3Department of Pharmacy Administration and Clinical Pharmacy, School of Pharmaceutical Sciences, Peking University, Beijing, People’s Republic of China; 4Department of General Dentistry II, Peking University School and Hospital of Stomatology, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: He Xu, Department of Pediatric Dentistry, Peking University School and Hospital of Stomatology, Beijing, People’s Republic of China, Tel +86-010-82195929, Email [email protected]
Background: As a dental simulator, the Simodont Dental Trainer (SDT) is widely used in preclinical dental training in many dental schools. This study aimed to compare and evaluate the effectiveness of SDT training versus the traditional operation training based on head-simulator (HS) in enhancing undergraduate students’ dental operative skills. Furthermore, the study intends to investigate the optimal sequence for integrating SDT training with the traditional training curriculum in order to optimize the overall course design..
Methods: Eighty-two undergraduate dental students were recruited and randomized into two groups. Group A initially practiced on the SDT and group B practiced on the KaVo head-simulator (HS) first. Subsequently, both groups practiced again on the HS system. The two groups then exchanged training systems for practice, and underwent test on the HS system. A questionnaire was administered to all the students when the training sequences were completed.
Results: Both the short-term teaching effectiveness of virtual training and the impact of training sequence on students’ long-term performance varied depending on the specific dental operation. Students encountered varying levels of technical difficulty across the two training systems, even when practicing the same procedure. Virtual training is generally acknowledged by students, yet more than half of them perceived real-world head-simulator-based practice more beneficial for improving operational proficiency.
Conclusion: The SDT serves as a useful supplement to traditional preclinical dental training, providing students with a platform to refine their technical skills efficiently. However, obvious difference in the sensory experiences is notable between the virtual reality and real-world training systems. SDT may be particularly beneficial for procedures requiring distinct tactile feedback. The widespread acceptance of virtual training by undergraduate dental students highlights virtual reality’s promise in dental education, though systematic integration and training curriculum design still require continuous exploration and refinement.
Keywords: preclinical training, simodont dental trainer, KaVo head-simulator, dental education, virtual reality
Introduction
Application of virtual simulation technology in preclinical dental training has been widely recognized as a key advance in the development of dental education in recent years.1,2 Compared to traditional training attachments, dental simulators provide standardized training and assessment models, upon which students can operate on standardized three-dimensional virtual teeth with real-time feedback and evaluation of their operations.3 This makes it possible to digitize and quantify training, and assessment. Most importantly, it allows students to operate repeatedly within limited time frames, without significantly increasing the dental school’s expenditure.4,5 Virtual simulation exercises can also provide a safer practice environment, preventing beginners from accidental injuries such as drills that might harm themselves.6 In addition, virtual training is more cost-effective than using real materials, which can be expensive and have a limited lifespan. Virtual training allows students to practice at their own pace and on their own schedule. Students can then repeat procedures as many times as needed, which helps to consolidate their skills and understanding. Many virtual training systems provide immediate feedback, which is crucial for learning and improvement. This advantage is particularly prominent for the preclinical training in pediatric dentistry, as dental treatment for children requires high-precision operations in relatively limited time. Abundant virtual practice before actual patient interactions can help dental students accumulate operating experiences as well as self-confidence.2,5
The Simodont Dental Trainer MOOG, Nieuw-Vennep, Netherlands (SDT), developed by MOOG in Nieuw-Vennep, Netherlands, is a dental simulator that has been widely used in many dental schools. It includes operation practice modules of hand flexibility, cariology, and crown preparations.7 Previous studies on the application of this simulator mainly focused on the following four aspects: questionnaire investigation of students’ opinions about SDT practice; evaluation of students’ performance of one particular dental operation after single use of the SDT; evaluations of technical improvements of the SDT system, such as 3D versus 2D vision, and the importance and necessity to apply force feedback technology during practice.1,5,8,9 In general, research on the effectiveness of SDT application has been relatively limited.10 Meanwhile, further research is needed determine if the training effect of SDT vary among different dental operations and to assess how the timing of SDT training within the preclinical curriculum affects students’ improvement in operational ability.
At the School of Stomatology in Peking University, the undergraduate dental students enter the pre-clinical training phase during their fourth year of study. By this stage, students have completed the theoretical coursework in stomatology. The pre-clinical training for pediatric dentistry focuses on the fundamental clinical procedures that are commonly used in dental practice, such as Class II cavity preparation and pulp chamber access for pulpotomy. Only after successfully completing all pre-clinical training courses and passing the associated assessments are the students allowed to progress to the clinical internship phase, where they begin treating real patients.
The preclinical training phase constitutes a pivotal stage in dental education. The primary objective of this training phase is to enable students to rapidly enhance their clinical operational skills within limited time, thereby laying a solid foundation for subsequent patient care involving real cases. Virtual reality (VR) -based teaching methodologies have demonstrated significant potential in meeting these educational demands. However, several critical challenges remain unresolved: Under equivalent training durations, does VR-based instruction yield superior outcomes compared to traditional teaching methods in terms of skill acquisition? Furthermore, how should virtual teaching be systematically integrated into the teaching curriculum? These questions still lack definitive answers or a systematically established framework.
This study introduces the SDT virtual training into the preclinical training phase in pediatric dentistry, aiming to compare and evaluate the effectiveness of SDT training versus the traditional operation training based on head-simulator (HS) in enhancing undergraduate students’ clinical operative skills. Furthermore, the study intends to investigate the optimal sequence for integrating SDT training with the traditional curriculum in order to optimize the overall course design.
Material and Methods
Ethics Approval
This study was approved by the Institutional Review Board of Peking University Hospital of Stomatology (PKUSSIRB-202275067). Written informed consents were obtained from all participants before the courses started.
Participants
The preclinical training was carried out when the undergraduate dental students had completed all the theoretical courses of pediatric dentistry and passed their unified theory test. At this stage, they had no experience with acrylic teeth or with patients previously. Eighty-five undergraduate dental students were recruited. None of them had any previous dental preclinical training or operational experience. Students would be excluded from the study if they failed to complete all the preclinical training courses as scheduled, due to sick leave or personal reasons.
Study Design
The 85 students were randomly assigned into two groups: Group A (n=42) and Group B (n=43) using a computer-generated randomization sequence. The whole training process was carried out in four class sessions. In the first session, all students received the “Precautions and Evaluation Criteria for Class II Cavity Preparation and Pulpotomy on Primary Molars” (see Tables 1 and 2) and the “Simodont System Operation Manual” for preview. A senior teacher illustrated and demonstrated the technical points of each operation. Following the instruction, Group A students used the SDT, while Group B used the KaVo head-simulator system (HS) to practice Class II cavity preparation on the lower right first primary molar for one hour and pulpotomy on the lower right second primary molar for another hour. Their scores were recorded as AS and B1, respectively.
 |
Table 1 Scoring Criteria of the Coronal Preparation in Pulpotomy on the Lower Right Second Primary Molar |
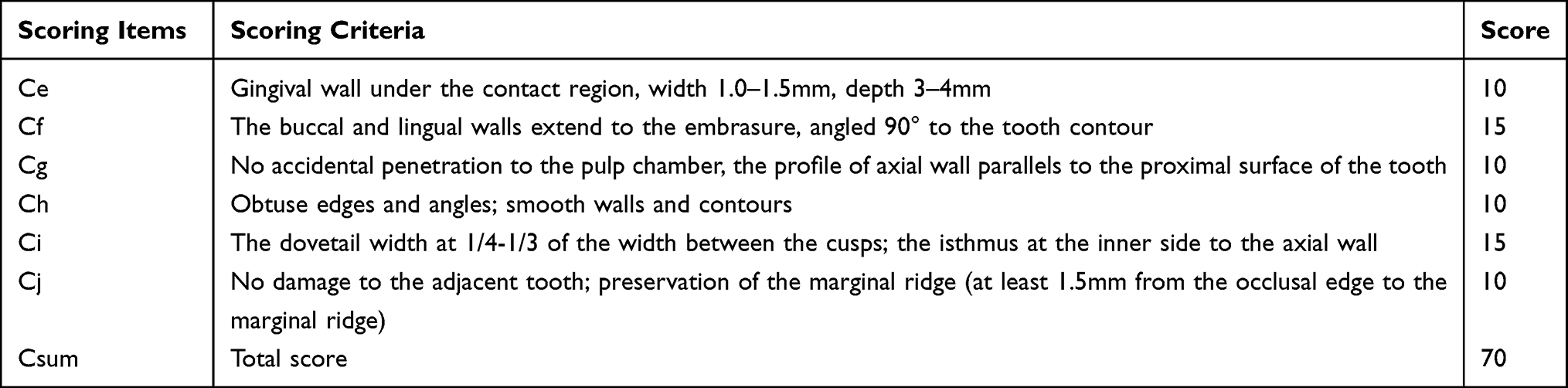 |
Table 2 Scoring Criteria of Dental Preparation of Class II Cavity on the Lower Right First Primary Molar |
In the second session, both two groups practiced on the HS system for the same time allocation, the relative scores were recorded as A2 and B2. In the third session, for exchange, Group A used the HS system while Group B used the SDT system, the relative scores were recorded as A3 and BS. In the fourth session, all the students were tested on the HS system, with scores recorded as A4 and B4 (Figure 1).
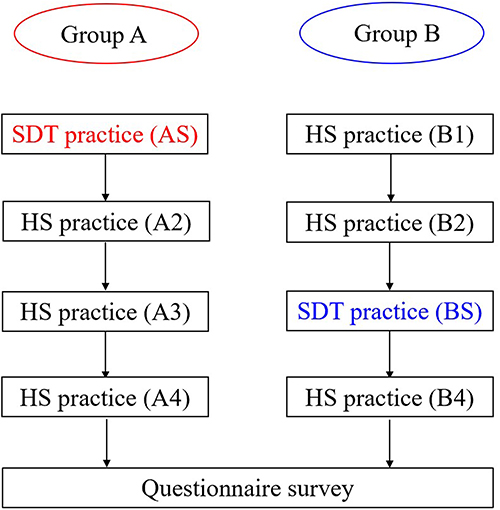 |
Figure 1 Flow chart diagram of the study. Color red marks the SDT session in group A. Color blue marks the SDT session in group B. |
By the end of the training curriculum, three students (one in Group A and two in Group B) were excluded in this study because of sick leave, leaving 41 students in Group A and 41 students in Group B completed the study. Assessment and scoring were performed in a single-blinded fashion by three senior pediatric dentists (Tables 2 and 3). A consistency test of scoring was conducted prior to the initiation of the study (Kendall’s W = 0.834, P < 0.05).
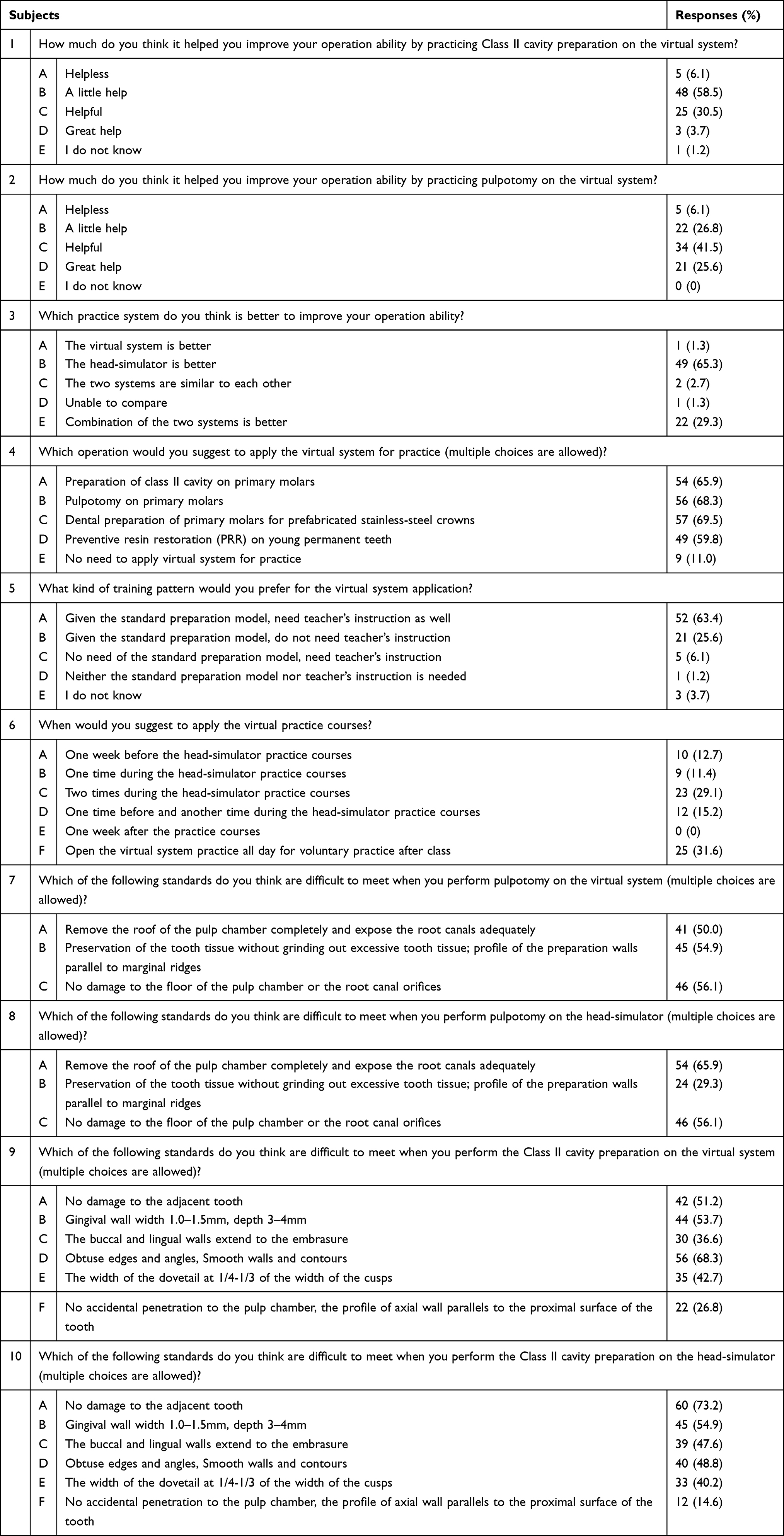 |
Table 3 Questionnaire Responses of Students’ Experience of Class II Cavity Preparation and Pulpotomy with Both Training Systems |
Questionnaire Survey
Upon completion of all four sessions, all the students were invited to complete a questionnaire pertaining regarding their practice experience and to provide suggestions of the virtual training (Supplementary Figure 1).
Statistical Analysis
All statistical analysis was performed using R software version 4.2.0 (R Foundation for Statistical Computing, Vienna, Austria). After a normality test using the Shapiro–Wilk method, Wilcoxon rank sum test was used to analyze the difference in the students’ operational scores (inspection level, α = 0.05 [bilateral]). Linear regression analysis was also applied to explore the specific direction of detected differences and to analyze the technical difficulties of each dental operation. A P-value less than 0.05 was considered statistically significant.Results
General Information and Quality Control
By the end of the cohort, 41 students in Group A and another 41 students in Group B were finally recruited. No differences were detected in gender or their scores of the theory test (P > 0.05) (Supplementary Table 1).
Evaluation of the Short-Term Training Effectiveness of Virtual Practice
Comparison A2 and B2 scores investigated students’ performance on the head-simulator model after practicing for the same duration in two different systems (Figures 2 and 3, Supplementary Tables 2 and 3, Table 4). In the pulpotomy operation, there were no significant differences in the total score or in the scores of most technical items. In the Class II cavity preparation, both total score and scores of certain technical items were lower in the SDT system compared to the HS system. This suggested that students’ performance experiences from single-session virtual practice may not accumulate as effectively as experiences from the same practice on a real-world head-simulator. Moreover, these results also indicated that the short-term teaching effectiveness of virtual training varies among different dental operation tasks.
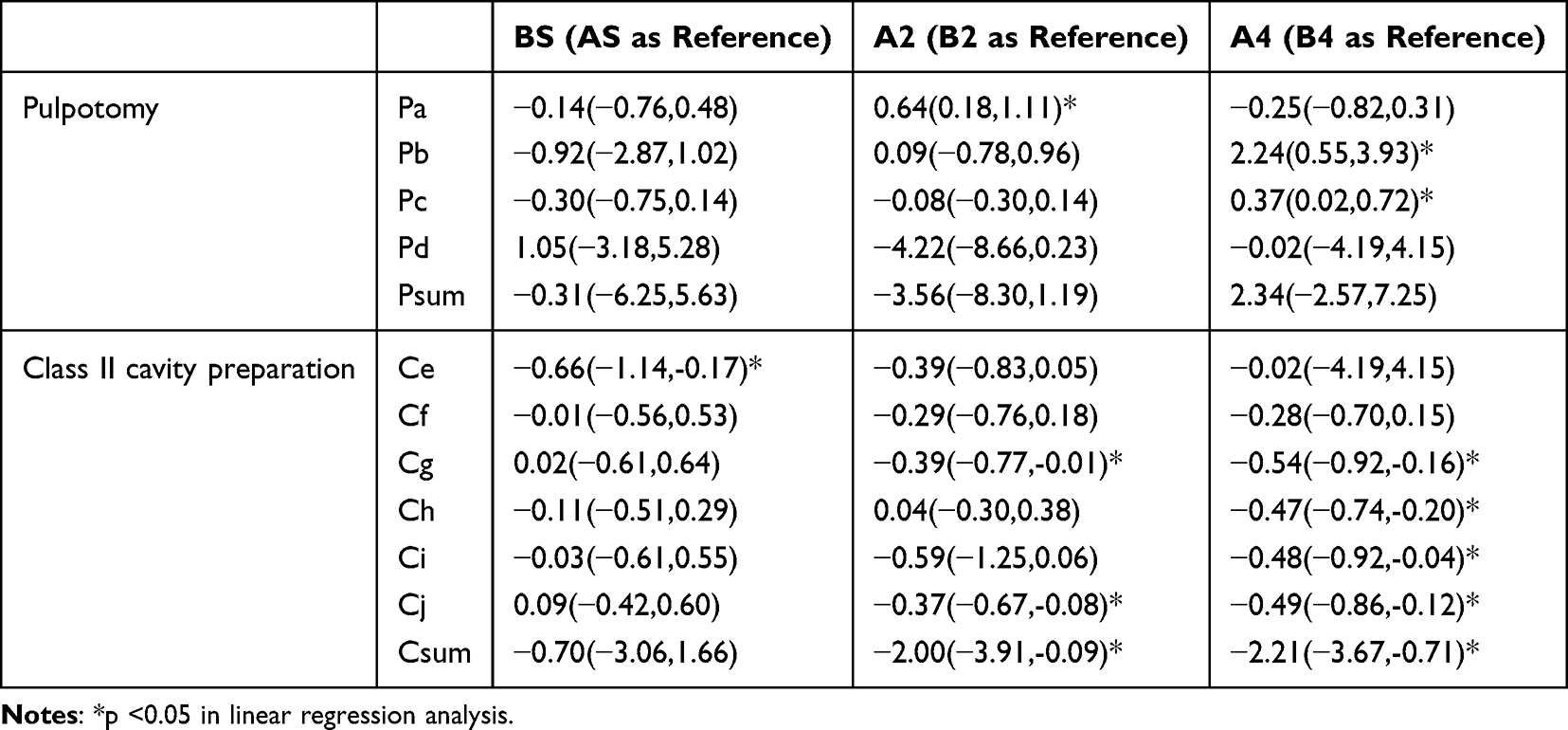 |
Table 4 Inter-Group Analysis of Dental Practice That Were Carried Out Based on the Same Training System |
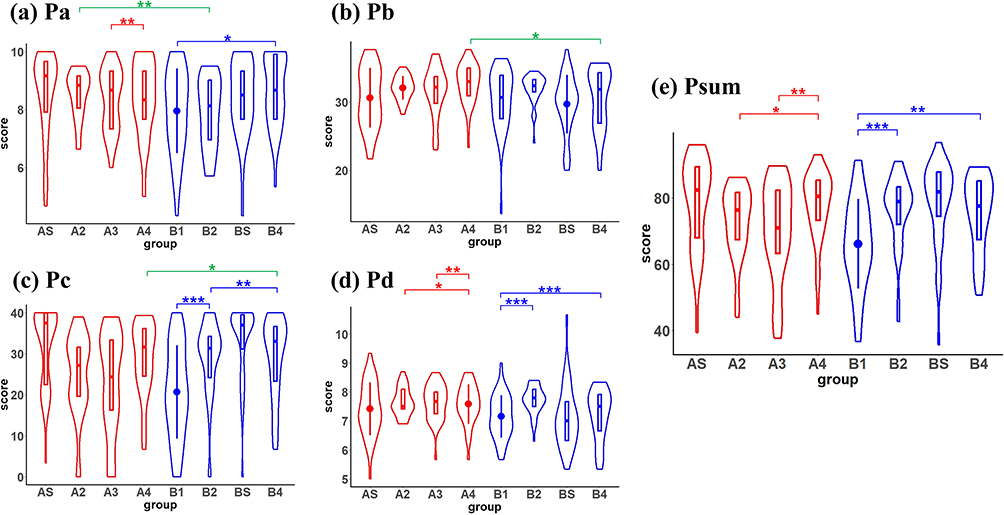 |
Figure 2 The intra-group and inter-group comparison the students’ operational scores of pulpotomy. Color red represents Group A. Color blue represents Group B. Color green represents the intra-group analysis. (a) Pa: Remove the roof of the pulp chamber completely and expose the root canals adequately; (b) Pb: Preservation of the tooth tissue without grinding out excessive tooth tissue; profile of the preparation walls parallel to marginal ridges; (c) Pc: Smooth contours and edges; (d) Pd: No damage to the floor of the pulp chamber or the root canal orifices; (e) Psum: Total score. Both intra-group and inter-group analysis (AS vs BS, A2 vs B2, A4 vs B4) of the difference in the students’ operational scores were carried out by the Wilcoxon rank sum test. *.01 < p <0.05; **.001 < p <0.01; ***p <0.001. |
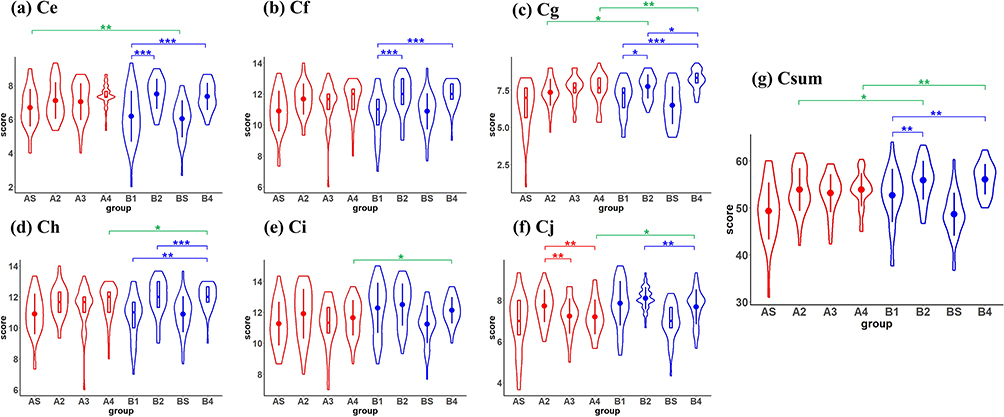 |
Figure 3 The intra-group and inter-group comparison of the students’ operational scores of the Class II cavity preparation. Color red represents Group A. Color blue represents Group B. Color green represents the intra-group analysis. (a) Ce: Gingival wall under the contact region, width 1.0–1.5mm, depth 3–4mm; (b) Cf: The buccal and lingual walls extend to the embrasure, angled 90° to the tooth contour; (c) Cg: No accidental penetration to the pulp chamber, the profile of axial wall parallels to the proximal surface of the tooth; (d) Ch: Obtuse edges and angles; smooth walls and contours; (e) Ci: The dovetail width at 1/4-1/3 of the width between the cusps; the isthmus at the inner side to the axial wall; (f) Cj: No damage to the adjacent tooth; preservation of the marginal ridge (at least 1.5mm from the occlusal edge to the marginal ridge); (g) Csum: Total score. Both intra-group and inter-group analysis (AS vs BS, A2 vs B2, A4 vs B4) of the difference in the students’ operational scores were carried out by the Wilcoxon rank sum test. *.01 < p <0.05; **.001 < p <0.01; ***p <0.001. |
Evaluation of Training Effectiveness of the Curriculum Design of Virtual Reality Training
The Impact of Curriculum Design of Virtual Training on the Students’ Virtual Performance
Comparison of AS and BS scores investigated whether the students’ virtual performance was related to the curriculum design of the virtual training. No significant differences were detected in either the overall scores or the majority of technical items, with the exception of one specific technical item (Ce) (Figures 2 and 3, Supplementary Tables 2 and 3, Table 4). This suggested that these beginner students got similar scores in their first virtual practice, irrespective of any prior real-world HS experience.
The Impact of Curriculum Design of Virtual Training on the Students’ Long-Term Performance
Comparison of A4 and B4 scores investigated the influence of different training sequences on the students’ final performance. Notably, divergent trends were observed between the two dental operations. In Class II cavity preparation task, Group A demonstrated lower scores in both the total score and approximately two-thirds of all technical items. In contrast, in the pulpotomy operation, Group A achieved higher scores in nearly half of the technical items, with no difference in the total score (Figures 2 and 3, Supplementary Tables 2 and 3, Table 4).
These findings indicate that the impact of training sequence on students’ long-term performance varies depending on the specific dental operation. Consequently, the optimal timing of virtual training within the overall preclinical curriculum should be determined based on the specific training content.
Evaluation of Consistency of the Operational Technical Difficulties Across the Two Training Systems
Linear regression analysis was applied to evaluate the relative difficulty of the technical items between the two training systems. On the SDT system, the more challenging items were identified as Pc (in pulpotomy) and Cg (in cavity preparation), while Cj was rated as relatively easy. In contrast, on the HS system, more difficult items included Pd and Ce, whereas Pa, Pb, Ch, and Cj were considered relatively easier (Table 5). This suggested that students encountered varying levels of technical difficulty across the two training systems, even when practicing the same procedure.
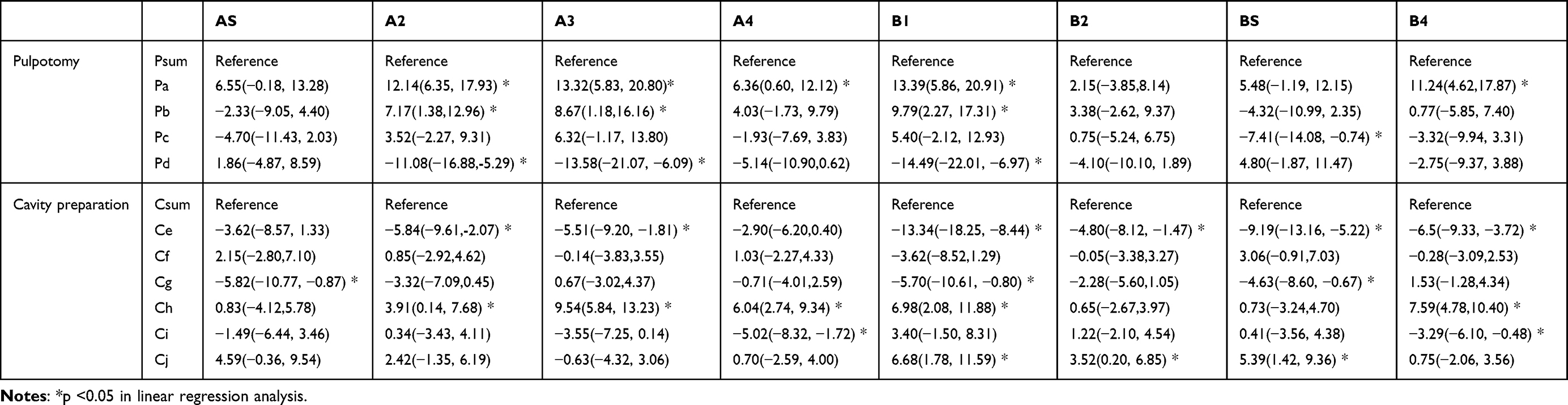 |
Table 5 Analysis of Difficult Technical Items in Each Operation |
In addition, in both Group A and B, Item Ce was consistently identified as difficult to score, while Item Pa and Ch were consistently recognized as easy to score on the HS system (Table 5). In the meantime, scores of Items Pd and Cg showed continuous improvement over the three HS practice sessions. This indicated that repeated practice on a consistent training system facilitates skill mastery and leads to progressive performance enhancement among students.
Students’ Feedback on Each Training System
This survey questionnaire was designed to assess the students’ perceptions of their training experience (Table 3). The vast majority of students acknowledged the positive effect of virtual training on the improvement of their operational skills, and over half expressed a desire for more virtual practice in various dental procedures (Questions 1and 4 in Table 3). These findings suggest widespread acceptance of virtual training among students and recognition of virtual reality as a promising direction for dental education. However, more than 60% of the students considered the head-simulator training more effective for skill enhancement than virtual training (Question 3 in Table 3), indicating that a notable disparity in the sensory experience between virtual practice and real-world practice at the present stage. Regarding specific procedural training, students showed a stronger preference for virtual pulpotomy exercises, a finding supported by their responses in this study (Question 2 in Table 3).
Moreover, the majority of students desired timely feedback and guidance during virtual practice. Over 60% believed that guidance from both a teacher and the virtual system with standardized preparations was essential, while about 25% considered that guidance from the virtual system alone was sufficient (Question 5 in Table 3). Approximately one-third of the students expressed a desire for access to the virtual system beside scheduled class hours for extended practice (Question 6 in Table 3).
Discussion
Dental education has undergone rapid advancements in recent years, as traditional instruction is now being supplemented and merged with advanced technological approaches.11,12 The virtual training systems for preclinical training in dental procedures utilize varying density parameters to simulate the tactile sensations of enamel and dentin abrading during tooth preparation, thus facilitating the operator’s perception of distances among various anatomical structures through haptic feedback.7,13 Through repeated practice, students can quickly improve their operational proficiency within a restricted time frame, compensating for the insufficiency of limited practice encountered in conventional head-simulator training. However, existing research data on dental simulators for skills training are predominantly descriptive, with insufficient high-level evidence-based support.14 This study focused on two key clinical procedures in pediatric dentistry, evaluated the teaching efficacy of the SDT virtual training system, explored the sequencing of virtual courses within the overall training curriculum, and quantitatively collected dental students’ feedback on the virtual teaching via structured questionnaires.
The Facilitating Effect of Virtual Reality Training in Preclinical Pediatric Dental Training
Our research demonstrates that the short-term educational efficacy of virtual training varies across different dental procedures. For certain specific types of operations, a single limited-time experience with a virtual reality system may not be as beneficial as the cumulative experience gained from the same practice model in the real world (head-simulator model). On the other hand, limited head-simulator training offers little assistance with the initial virtual performance. This implies that there are differences in how skills are acquired and retained between virtual and real-world practice.15 This difference may be attributed to the sensory disparity between virtual reality technology and the real-world experience. The lack of realism in the overall head, joint, and mouth opening in virtual practice is one reason why it could not replace the practice with head-simulator models.16
Conversely, this also reminds us that the operational experience accumulated in virtual teaching may need to bridge these experiential differences first, in order to effectively translate into real-world competency. This may be one of the reasons why the majority of students considered that the head-simulator training system to be more effective in improving operational skills than virtual training. These results are consistent with some previous studies suggesting that virtual systems can be applied as complement, but cannot fully replace traditional head-simulator training.16,17 This aligns with the prevailing consensus in current literature on virtual teaching research.18 Further research is needed to determine the exact impact of the sensory differences between virtual reality and real-world practice on training effectiveness.
The Learning and Mastery of Different Operational Difficulties by Students Under Two Training Systems
The results demonstrated significant differences in difficulty ratings between the two training systems for technical items. The undergraduates recruited in this study were all beginners with limited experience. We observed that The difficult items (Pd, Ce) on the head-simulator system primarily stemmed from three factors: (1) insufficient knowledge of primary tooth anatomy; (2) insufficient mastery of the accurate localization of standard cavity preparation margin positions; and (3) unfamiliarity with turbine handpiece operation during initial practice. These challenges showed potential for improvement through sustained practice and experience accumulation. However, such challenges were not evident in the virtual training system’s performance. It is very likely that repeated practice on the virtual system strengthens students’ grasp of the anatomical structure and management of the turbine handpiece in the short term, and thus rapidly improves their operational abilities in these particular technical items, reducing their perceived difficulty.
Additionally, students’ feedback indicated greater approval of the virtual system’s teaching effectiveness for access cavity preparation in pulpotomy operation, compared to cavity preparation. This aligns with previous research findings.19 In access cavity preparation, the sudden “drop” sensation when the turbine enters the pulp chamber corresponds to significant differences of force feedback in the virtual simulators. The virtual training may be particularly beneficial for procedures requiring distinct tactile feedback. A recent study on access cavity preparation further supported this notion.20
On the other hand, the difficult points in virtual practice centered on procedures that require precise control of bur movement trajectories and drilling depths (items Pc, Cg). This aligns with the students’ feedback that the force feedback sensation in the virtual system differs from the sensation of controlling the turbine handpiece in the real world, making it more challenging for beginners to control the fine movements of the handpiece in the virtual system. Correspondingly, the Item Cj, which does not involve fine control of the turbine handpiece, demonstrated consistently high scoring rates across both training platforms, confirming its relative technical simplicity.
Factors to Consider in Implementing Virtual Training in Dental Schools
One questionnaire survey used to show that the majority of students tend to prefer initiating their practice in prosthodontics with SDT before advancing to HS training.12 Nevertheless, findings from a research specifically targeting veneer preparation procedures suggested that the order in which virtual simulators are utilized did not have a statistically significant impact on students’ ultimate clinical performance.21 Our research findings indicate that students’ long-term performance is influenced by the type of dental operation and the scheduling of virtual training. Consequently, the integration of virtual training modules into dental curricula—and the optimal timing of their implementation—should be determined based on procedural specificity. From the students’ perspective, there is a desire for open access to virtual practice systems and a need for timely correction and guidance, whether from teachers or through comparison with standardized cavity preparation templates. The findings are consistent with previous research results.12 Against the background of rapidly advancing dental technologies and clinical practices, self-directed training in dental education is becoming increasingly important.22 Research indicates that concurrent feedback improves psychomotor skills by clearly outlining the steps needed to achieve the desired outcome, promptly directing students toward the correct approach.12,23 The integration of immediate feedback with repetitive practice can serve as an effective and efficient strategy for helping dental students enhance their clinical skills within a limited timeframe.22,24 This student feedback may hold significant guiding value for the future development of virtual training systems in dental education.
Given the practical conditions of dental educational institutions, if the virtual system is made available on a long-term basis with guidance based on standard cavity preparations, students will have the opportunity to repeatedly practice dental procedures before clinical contact with patients, thus accumulating operational experience and enhancing confidence.
Nevertheless, due to the inherent differences between the sensory experiences in virtual reality and real-world experiences, students still need to overcome the differences in operational experience brought about by the two scenarios before virtual training systems can facilitate in the real-world performance. Further research is required to explore these aspects.
This study has several limitations. This study focuses on the preclinical training curriculum for undergraduate dental students. During this phase, students have not yet engaged in clinical practice with real patients and are at a critical initial stage of practicing dental procedures. Theoretically, extending the practice duration during this stage would be more conducive to improving their operational proficiency. However, practical constraints including curriculum scheduling, limited access to the SDT equipment, and student enrollment numbers necessitated the specific training parameters: each dental procedure was limited to 1 hour of SDT practice and one resin tooth for HS training. These restrictions may have compromised the comprehensive evaluation of students’ technical skill acquisition. Furthermore, the generalizability of our findings is limited by the single-institution, single-cohort design, as the study was conducted exclusively with undergraduate dental students from one university. This is a widespread limitation observed in numerous studies on virtual teaching.25 Future research employing multi-center designs with expanded sample sizes would be essential to validate and generalize these preliminary conclusions.
In summary, virtual training can serve as a valuable adjunct to preclinical dental training. The SDT provides students with a platform to refine their technical skills prior to perform real clinical procedures on patient. Moreover, the benefits of virtual training may extend beyond its technological capabilities, as it has the potential to reduce anxiety levels among dental students. The immediate feedback provided by haptic devices facilitates self-assessment, enabling students to identify areas that requires improvement.5 In the future, with further iterations and advancements in haptic feedback technology within virtual training systems, it is anticipated that users’ sensory experiences will more closely approximate the tactile sensations of real-world clinical procedures, thereby enhancing the realism of virtual training. Furthermore, through extensive and systematic research efforts, it is possible to gradually identify the types of clinical procedures within various dental subspecialties that are particularly well-suited for virtual simulation-based training. This, in turn, enables the development of more targeted and efficient preclinical training programs.
Conclusion
Overall, despite numerous explorations, the application of virtual reality training in preclinical pediatric dental training is still in its early stage. Students’ long-term performance is influenced by both the type of dental operation and the scheduling of virtual training. Obvious difference in the sensory experiences in noted between the virtual reality and real-world training systems. Questionnaire survey of the undergraduate dental students suggests widespread acceptance of virtual training and recognition of virtual reality as a promising direction for dental education. Virtual reality training can serve as a supplement, but cannot fully replace the traditional training with head-simulator models and resin teeth. The systematic application and curriculum design of virtual reality training still require continuous exploration and refinement.
Abbreviations
VR, virtual reality; SDT, Simodont Dental Trainer; HS, KaVo head-simulator.
Data Sharing Statement
The data relevant to this study are available from the corresponding author upon reasonable request.
Consent for Publication
All authors have approved the final manuscript and provide their consent for publication.
Acknowledgments
We thank all of the participants for their willingness to participate in the study and the time that they devoted to the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Teaching Reformation Fund of Peking University School and Hospital of Stomatology (2020-PT-05).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Murbay S, Neelakantan P, Chang JWW, et al. ‘Evaluation of the introduction of a dental virtual simulator on the performance of undergraduate dental students in the pre-clinical operative dentistry course’. Eur J Dent Educ. 2020;24(1):5–16. doi:10.1111/eje.12453
2. Li Y, Ye H, Ye F, et al. The Current Situation and Future Prospects of Simulators in Dental Education. J Med Internet Res. 2021;23(4):e23635. doi:10.2196/23635
3. Urbankova A, Engebretson SP. The use of haptics to predict preclinic operative dentistry performance and perceptual ability. J Dent Educ. 2011;75(12):1548–1557. doi:10.1002/j.0022-0337.2011.75.12.tb05214.x
4. De Boer IR, Bakker DR, Wesselink PR, et al. The Simodont in dental education. Ned Tijdschr Tandheelkd. 2012;119(6):294–300. doi:10.5177/ntvt.2012.06.12105
5. Zafar S, Lai Y, Sexton C, et al. Virtual Reality as a novel educational tool in pre-clinical paediatric dentistry training: students’ perceptions. Int J Paediatr Dent. 2020;30(6):791–797. doi:10.1111/ipd.12648
6. Khalaf K, El-Kishawi M, Mustafa S, et al. Effectiveness of technology-enhanced teaching and assessment methods of undergraduate preclinical dental skills: a systematic review of randomized controlled clinical trials. BMC Med Educ. 2020;20(1):286. doi:10.1186/s12909-020-02211-4
7. Mirghani I, Mushtaq F, Allsop MJ, et al. Capturing differences in dental training using a virtual reality simulator. Eur J Dent Educ. 2018;22(1):67–71. doi:10.1111/eje.12245
8. De Boer IR, Wesselink PR, Vervoorn JM. Student performance and appreciation using 3D vs. 2D vision in a virtual learning environment. Eur J Dent Educ. 2016;20(3):142–147. doi:10.1111/eje.12152
9. De Boer IR, Lagerweij MD, De Vries MW, et al. The Effect of Force Feedback in a Virtual Learning Environment on the Performance and Satisfaction of Dental Students. Simul Healthc. 2017;12(2):83–90. doi:10.1097/SIH.0000000000000208
10. Nassar HM, Tekian A. Computer simulation and virtual reality in undergraduate operative and restorative dental education: a critical review. J Dent Educ. 2020;84(7):812–829. doi:10.1002/jdd.12138
11. Towers A, Field J, Stokes C, et al. A scoping review of the use and application of virtual reality in pre-clinical dental education. Br Dent J. 2019;226(5):358–366. doi:10.1038/s41415-019-0041-0
12. Daud A, Matoug-Elwerfelli M, Khalid A, et al. The impact of virtual reality haptic simulators in pre-clinical restorative dentistry: a qualitative enquiry into dental students’ perceptions. BMC Oral Health. 2024;24(1):988. doi:10.1186/s12903-024-04704-w
13. San Diego JP, Newton TJ, Sagoo AK, et al. Learning Clinical Skills Using Haptic vs. Phantom Head Dental Chair Simulators in Removal of Artificial Caries: cluster-Randomized Trials with Two Cohorts’ Cavity Preparation. Dent J. 2022;10(11). doi:10.3390/dj10110198.
14. Maliha SG, Diaz-Siso JR, Plana NM, et al. Haptic, Physical, and Web-Based Simulators: are They Underused in Maxillofacial Surgery Training? J Oral Maxillofac Surg. 2018;76(11):2424.e1–e11. doi:10.1016/j.joms.2018.06.177
15. Leblanc VR, Urbankova A, Hadavi F, et al. A preliminary study in using virtual reality to train dental students. J Dent Educ. 2004;68(3):378–383. doi:10.1002/j.0022-0337.2004.68.3.tb03754.x
16. Daud A, Matoug-Elwerfelli M, Daas H, et al. Enhancing learning experiences in pre-clinical restorative dentistry: the impact of virtual reality haptic simulators. BMC Med Educ. 2023;23(1):948. doi:10.1186/s12909-023-04904-y
17. Kwon HB, Park YS, Han JS. Augmented reality in dentistry: a current perspective. Acta Odontol Scand. 2018;76(7):497–503. doi:10.1080/00016357.2018.1441437
18. Buchanan JA. Use of simulation technology in dental education. J Dent Educ. 2001;65(11):1225–1231. doi:10.1002/j.0022-0337.2001.65.11.tb03481.x
19. Javed MQ, Arjumand B, Klarkodi SH, et al. Influence of virtual reality simulation (excluding augmented reality) on endodontic learning experiences of undergraduate dental students: a systematic review. BMC Med Educ. 2025;25(1):1013. doi:10.1186/s12909-025-07553-5
20. Wei Y, Peng Z. Application of Simodont virtual simulation system for preclinical teaching of access and coronal cavity preparation. PLoS One. 2024;19(12):e0315732. doi:10.1371/journal.pone.0315732
21. Li Y, Ye H, Wu W, et al. Effectiveness and Methodologies of Virtual Reality Dental Simulators for Veneer Tooth Preparation Training: randomized Controlled Trial. J Med Internet Res. 2025;27:e63961. doi:10.2196/63961
22. Patil S, Bhandi S, H AK, et al. Effectiveness of haptic feedback devices in preclinical training of dental students-a systematic review. BMC Oral Health. 2023;23(1):739. doi:10.1186/s12903-023-03410-3
23. Al-Saud LM, Mushtaq F, Allsop MJ, et al. Feedback and motor skill acquisition using a haptic dental simulator. Eur J Dent Educ. 2017;21(4):240–247. doi:10.1111/eje.12214
24. Al-Saud LM, Mushtaq F, Mann RP, et al. Early assessment with a virtual reality haptic simulator predicts performance in clinical practice. BMJ Simul Technol Enhanc Learn. 2020;6(5):274–278. doi:10.1136/bmjstel-2018-000420
25. Ma L, Lai H, Zhao W. Evaluating the Effectiveness of a Virtual Simulation Platform for Apexification Learning. Dent J. 2024;12(2). doi:10.3390/dj12020027
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.