")
Back to Journals » Cancer Management and Research » Volume 15
Evaluation of Sinonasal Outcome Test (SNOT-22) Domains in the Assessment of the Quality of Life in Patients with Nasopharyngeal Carcinoma
Authors Wu CN , Wang YM, Chen WC, Fang FM, Li SH, Huang TL, Hwang CF, Lee Y, Lin CY , Luo SD
Received 3 May 2023
Accepted for publication 4 July 2023
Published 18 July 2023 Volume 2023:15 Pages 719—728
DOI https://doi.org/10.2147/CMAR.S416353
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ahmet Emre Eşkazan
Ching-Nung Wu,1,2 Yu-Ming Wang,3,4 Wei-Chih Chen,1 Fu-Min Fang,3,4 Shau-Hsuan Li,5 Tai-Lin Huang,5 Chung-Feng Hwang,1 Yu Lee,6 Chung-Ying Lin,2,7– 9 Sheng-Dean Luo1,10,11
1Department of Otolaryngology, Kaohsiung Chang Gung Memorial Hospital and Chang Gung University College of Medicine, Kaohsiung, Taiwan; 2Department of Public Health, College of Medicine, National Cheng Kung University, Tainan, Taiwan; 3Department of Radiation Oncology, Kaohsiung Chang Gung Memorial Hospital and Chang Gung University College of Medicine, Kaohsiung, Taiwan; 4Proton and Radiation Therapy Center, Kaohsiung Chang Gung Memorial Hospital and Chang Gung University College of Medicine, Kaohsiung, Taiwan; 5Department of Hematology-Oncology, Kaohsiung Chang Gung Memorial Hospital and Chang Gung University College of Medicine, Kaohsiung, Taiwan; 6Department of Psychiatry, Kaohsiung Chang Gung Memorial Hospital and Chang Gung University College of Medicine Kaohsiung, Kaohsiung, Taiwan; 7Institute of Allied Health Sciences, College of Medicine, National Cheng Kung University, Tainan, Taiwan; 8Department of Occupational Health, College of Medicine, National Cheng Kung University, Tainan, Taiwan; 9Biostatistics Consulting Center, National Cheng Kung University Hospital, College of Medicine, National Cheng Kung University, Tainan, Taiwan; 10Graduate Institute of Clinical Medical Sciences, College of Medicine, Chang Gung University, Taoyuan, 333, Taiwan; 11School of Traditional Chinese Medicine, Chang Gung University College of Medicine, Taoyuan, 33302, Taiwan
Correspondence: Chung-Ying Lin, National Cheng Kung University Tainan, 70101, Taiwan, Tel +886-7-731-7123 ext: 2533, Email [email protected] Sheng-Dean Luo, Kaohsiung Chang Gung Memorial Hospital, No. 123, Dapi Road, Niaosong District, Kaohsiung City, 83301, Taiwan, Email [email protected]
Background: Few instruments are available for assessing the otorhinologic-related quality of life (QOL) in nasopharyngeal carcinoma (NPC) patients. Therefore, we evaluated whether the 22-item Sinonasal Outcome Test (SNOT-22) could be applied to these patients.
Methods: Patients diagnosed with NPC, who had been treated with standard protocol and followed up in our institute between 2019 and 2022, were invited to join the cross-sectional study during their clinic visits. All participants completed the SNOT-22 and Eustachian Tube Dysfunction Questionnaire-7 once they were recruited. Confirmatory factor analysis (CFA) was performed to decide the most suitable model for the underlying SNOT-22 subdomains, along with various validity and reliability tests.
Results: We identified a total of 275 patients, with 84 (30.5%) women and 191 (69.5%) men. The mean age was 54.1 years (standard deviation: 11.2). Among these patients, 171 (62.1%) were in late stages, and 260 (94.5%) received chemoradiotherapy as treatment. The median interval between primary RT treatment and questionnaire completion was 50 months (interquartile range: 29– 93). CFA supported a five-factor model for the SNOT-22 for NPC patients, including nasal, ear/facial, sleep, function, and emotion domains. The internal consistency and test-retest reliability of the SNOT-22 domain score were good. In addition, known-group validity was good for the SNOT-22 total score and domain scores according to the disease recurrence status.
Conclusion: Psychometric analyses supported the reliability and validity of a five-domain SNOT-22 for assessing otorhinologic-related QOL in NPC patients.
Keywords: SNOT-22, nasopharyngeal carcinoma, quality of life, psychometrics, chronic rhinosinusitis
Introduction
Despite being uncommon cancer overall, nasopharyngeal carcinoma (NPC) has a regional incidence of about 3–20 cases per 100,000 individuals in several endemic areas, especially Southern China (eg, Hong Kong) and Southeast Asia.1,2 Radiotherapy (RT) is the primary treatment for NPC, either alone or in combination with chemotherapy.3 Due to the proximity of the nasopharynx to the skull base, however, RT for NPC has various locoregional adverse effects, such as chronic rhinosinusitis (CRS), hearing loss, eustachian tube dysfunction (ETD), and xerostomia. Specifically, the incidence of postirradiation otitis media and CRS can be even up to 29.4% and 16.7%, respectively.4 These local adverse effects, and the general toxicity of the treatment, seriously impact the health-related quality of life (QOL) of NPC patients.5 However, a comprehensive QOL scale specific to otorhinologic-related domains for NPC patients is limited.
Although the QOL of NPC patients has been widely studied, most instruments used for assessing QOL are not specific to NPC. The tools most commonly used for QOL assessment in NPC patients include the European Organization for the Research and Treatment of Cancer Quality of Life Questionnaire (QLQ-C30) and EORTC Quality of Life Head and Neck Module (QLQ-H&N35).6 Global health status, physical functioning, and xerostomia-related QOL have also been well studied.7,8 However, the QLQ-H&N35 and QLQ-C30 were initially validated for head and neck cancer patients, and most of the symptomatic items pertain to oral and pharyngeal function.9 There are no items regarding the local otorhinologic side effects of RT in NPC patients, including sinonasal and otologic symptoms. Two NPC-specific QOL instruments, the Functional Assessment of Cancer Therapy–Nasopharyngeal (FACT-NP)10 and quality of life scale for nasopharyngeal carcinoma patients (QOL-NPC),11 have been developed in recent years. Although the FACT-NP and QOL-NPC have good psychometric properties, they do not do much in assessing otorhinologic regions either. Only 4 of 16 and 3 of 26 items in FACT-NP and QOL-NPC are specific to sinonasal and otologic domains. An appropriate QOL instrument that assesses otorhinologic QOL is still lacking for clinicians and NPC patients.
The 22-item Sinonasal Outcome Test (SNOT-22) is one of the most robust CRS-specific inventories translated to many languages worldwide.12 It has been recommended for routine use in clinical evaluations and trials.13 The SNOT-22 captures symptom severity (rhinologic, otologic, and facial), some of the social and emotional impact of disease, and some of the consequences thereof for productivity and sleep, which are also highly considered in the QOL of NPC patients. Although the SNOT-22 has been used to measure QOL in NPC patients,14,15 it has not been evaluated for that population. Indeed, the factor structure of SNOT-22 has varied widely in prior studies conducted with varied types of clinical populations and therefore merits further examination if SNOT-22 is to be used to evaluate NPC patients.
Therefore, the objective of the present cross-sectional study was to evaluate the factorial validity of SNOT-22 using data collected from NPC patients. In addition, we also assessed convergent and divergent validity and known-group validity according to the examined factor structure. We determined whether the SNOT-22 is suitable for evaluating otorhinologic-related QOL in NPC patients.
Materials and Methods
Patient Selection and Data Collection
This study was approved by the Institutional Review Board of Kaohsiung Chang Gung Memorial Hospital (KCGMH) (Ref. No: 202200901B0 and 202100470B0 and 202200543B0), which complies with the Declaration of Helsinki. Written informed consent was obtained from the study participants before the study commencement. Patients diagnosed with NPC, who had been treated with standard protocol and followed up in KCGMH between March 2019 and October 2022, were invited to join the cross-sectional study during their clinic visits. The inclusion was not limited to disease status (eg, recurrent or metastatic disease). All participants were explained by principal Investigators first and completed the SNOT-22 and Eustachian Tube Dysfunction Questionnaire-7 (ETDQ-7) once they were recruited. SNOT-22 and ETDQ-7 are self-reported questionnaires; however, an experienced research assistant was available during the survey if assistance was required. In addition, a subset of participants who were scheduled to visit any clinics in KCGMH within one month was invited to complete the SNOT-22 again during the revisit. Patients who could not communicate verbally or in writing were excluded, as were those with impaired functioning who could not complete questionnaires. Additionally, patients who had undergone radiotherapy within a 6-month period were excluded from the study in order to avoid the inference of acute toxicity from primary treatment. The demographic and clinical data of the patients were collected through a chart review. Age, sex, tumor-node-metastasis (TNM) stage, the primary treatment regimen, the time between RT and questionnaire completion, and the recurrence status of all patients were recorded.
Instruments
The SNOT-22 is a 22-item treatment outcome measure designed for people with chronic sinonasal conditions.16–20 The SNOT-22 has been evaluated and is based on a Likert scale where 0 = “No problem”, 1 = “Very mild problem”, 2 = “Mild or slight problem”, 3 = “Moderate problem”, 4 = “Severe problem”, and 5 = “Problem as bad as it can be.” Higher scores on SNOT-22 survey items indicate worse patient function or more severe symptoms (total score range: 0–110).13 Several factor structures of the SNOT-22 have been derived via factor analysis in previous literature (Table S1). Specifically, DeConde et al16 reported a five-factor model for the SNOT-22 for CRS patients who elected surgical intervention for continuing medically refractory symptoms at baseline and 6-month follow-up, based on exploratory factor analysis (EFA). The five factors were rhinological (items 1–5 and item 8), extranasal rhinological (items 6–8), ear/facial (items 9–12), sleep-related (items 13–17); and psychological (items 16–22). Sedaghat et al17 reported a four-factor model based on their principal component analysis from 177 consecutive CRS patients. The four factors were nasal (items 1–8), otologic (items 9–12), sleep (items 4 and 13–20), and emotional (items 21 and 22). Crump et al18 derived a five-factor model based on classic test theory and a two-parameter graded response model from CRS patients awaiting endoscopic sinus surgery. The five domains were rhinological (items 1–3 and 6–7), extranasal rhinological (items 4–5 and 8), ear/facial (items 9–12), sleep-related (items 13–20) and psychological (items 21–22). Feng et al19 derived a four-factor model based on EFA and confirmatory factor analysis (CFA) from CRS patients without the effect of sinus surgery. The four factors were nasal (items 1–8), otologic/facial pain (items 9–12), sleep-related (items 13–20), and emotional (items 21–22). Finally, Khan et al20 reported a five-factor model based on EFA and CFA from CRS patients with nasal polyps at baseline, mid-treatment time point, and end-of-treatment in clinical trials of dupilumab. The five factors were nasal (items 1–8), ear/facial (items 9–12), sleep-related (items 13–16), functional (items 17–19), and emotional (items 20–22).
The ETDQ-7 is an instrument used in adults with eustachian tube dysfunction (ETD). ETD is a known condition associated with both otologic and rhinological symptoms following RT to the nasopharyngeal region.21 The ETDQ-7 was previously examined with acceptable reliability (Cronbach α = 0.71). A good discriminant validity existed between a group of 50 consecutive adult patients diagnosed with ETD and a control group of 25 (p < 0.001).22 Each question in the ETDQ-7 is scored on a seven-point Likert scale, where 1 indicates no problem and 7 indicates the worst possible symptoms. The ETDQ-7 sum scores reflects ETD severity (total score range: 7–49). The participants were encouraged to complete all items in both the SNOT-22 and ETDQ-7.
Data Analysis
Factor Structure and Sensitivity Analysis
The factor structure of the SNOT-22 was examined using CFA and diagonally weighted least square (DWLS) estimation. We used six models, five of which were evaluated for CRS in previous studies (Models 1–5; Table S1); the sixth was a general model (Model 0; Table S1). Model 0 was a one-factor model with all items loaded on the general QOL factor; Models 1 (DeConde et al) and 3 (Crump et al) were five-factor models that included rhinological symptoms, extranasal rhinological symptoms, ear/facial symptoms, psychological dysfunction, and sleep dysfunction; Models 2 (Sedaghat et al) and 4 (Feng et al) were four-factor models that included nasal, otologic/facial pain, emotional, and sleep symptoms; and Model 5 (Khan et al) was also a five-factor model that had a functional instead of extranasal rhinological domain. The acceptable fit of CFA models is indicated by a non-significant χ2 test (χ2/df < 2), Tucker-Lewis index (TLI) and comparative fit index (CFI) > 0.9, and root mean square error of approximation (RMSEA) and standardized root mean square residual (SRMR) < 0.08.23 The χ2 difference test was used to compare the models, and the expected cross-validation index (ECVI), which a smaller value represents a better model fit, was calculated for comparing models with the same degrees of freedom.24
Due to the substantial variability in the time span of primary treatment completion among the patients included in the study, two sensitivity analyses were conducted on the most suitable model to address the potential impact on result reliability. We conducted one sensitivity analysis using questionnaires from patients who had undergone radiotherapy within a 2-year period to represent the performance of the model in the short-term post-treatment period. Additionally, we utilized questionnaires from patients who had undergone radiotherapy within a 5-year period for another sensitivity analysis to represent the model’s performance in the mid-term post-treatment period.
Internal Consistency and Test-Retest Reliability
We used McDonald’s ω coefficient to assess internal consistency; a McDonald’s ω > 0.7 indicates acceptable reliability.25 Test-rest reliability was also evaluated for participants who repeated the questionnaires within one month by using intraclass correlation coefficient (ICC). The two-way mixed-effects mode was used in the ICC, and the estimate of ICC < 0.5, 0.5–0.75, 0.75–0.9, and > 0.90 are indicative of poor, moderate, good, and excellent reliability, respectively.26
Convergent, Divergent, and Known-Group Validity
We used Pearson’s correlation coefficient (r) to assess the correlations between SNOT-22 domains, which r = 0.3, 0.4–0.6, and 0.70 correspond to weak, moderate, and strong correlation, respectively.27 The convergent and divergent validity of the SNOT-22 domains was assessed by correlation analysis between SNOT-22 domain scores and ETDQ-7 scores. The ETDQ-7 measures eustachian tube symptoms, and the correlations with measures of related constructs (eg, ear/facial and nasal domains) were expected to be at least moderate (r ≥ 0.4) (convergent validity); the correlations with the other SNOT-22 domains were expected to be significantly smaller (divergent validity). The differences between correlation coefficients were examined using Fisher’s r-to-z transformation.28,29
Lastly, to assess the discriminatory ability of the SNOT-22, known-group validity was tested using the clinical characteristics, clinical American Joint Committee on Cancer (AJCC) staging system (ie, the TNM staging system), the utilization of chemotherapy in the primary treatment regimen, and according to NPC disease recurrence status, using the Mann–Whitney U-test. We hypothesized that NPC patients in a late clinical-stage (III–IV) or with the recurrent disease would have lower otorhinologic-related QOL compared to early-stage (I–II) patients and those without recurrence. However, it is possible that the period after completing RT, the utilization of chemotherapy, and other clinical characteristics would confound known-group validity. Therefore, multiple linear regression was used to adjust the effects of potential confounding on known-group validity analysis. All statistical analyses were performed using the lavaan and Psych packages of R software (version 4.0.5; R Foundation, Vienna, Austria) and SAS software (version 9.4; SAS Institute Inc., Cary, NC, USA). P-values < 0.05 were considered statistically significant.
Results
A total of 329 patients were asked to participate in the study. After excluding patients who declined to participate (n=28), patients who had undergone radiotherapy within a 6-month period (n=16), participants with incomplete demographics (n = 5), or questionnaire data (n = 5), 275 participants were analyzed. The clinical and demographic characteristics of these patients are shown in Table 1; 69.5% (191) were males, and the mean age at diagnosis was 54.1 years (range: 27–78 years). The median interval between primary RT treatment and questionnaire completion was 50 months (range: 7–312 months). The mean SNOT-22 score was 24.1 ± 19.9 (range: 0–84). The comparison between patients who agreed and who declined to participate is shown in Table S2; Patients who refused to participate were older and simultaneously had a significantly more extended survival period after completing RT.
 |
Table 1 Participant Characteristics (n = 275) |
The results of the CFA of the various models are shown in Table 2. The one-factor model (Model 0) had a significant χ2 with χ2/df > 2, so it was deemed an unsuitable model. There were no solutions found in Models 1 and 2 by the lavaan. Models 3–5 had acceptable fit indices, with Models 5 having a better fit than Models 3 to 4. The χ2 difference tests further showed that Model 5 significantly outperformed Models 4 (Model 5 vs 4: Δχ2 [Δdf = 4] = 59.84; P < 0.001). The χ2 difference test was not used for comparing Models 5 and 3 because they had the same degrees of freedom. Therefore, the ECVI was used; Model 5 had a lower ECVI than Model 3. We decided to subject Model 5, which had no cross-loading and all loadings > 0.5, to further psychometric testing (Figure 1). Both sensitivity analyses were conducted using data within a 2-year and 5-year timeframe, respectively. Model 5 exhibited acceptable fit indices in both sensitivity analysis models, except for a higher value of SRMR observed in the 2-year model (Table S3).
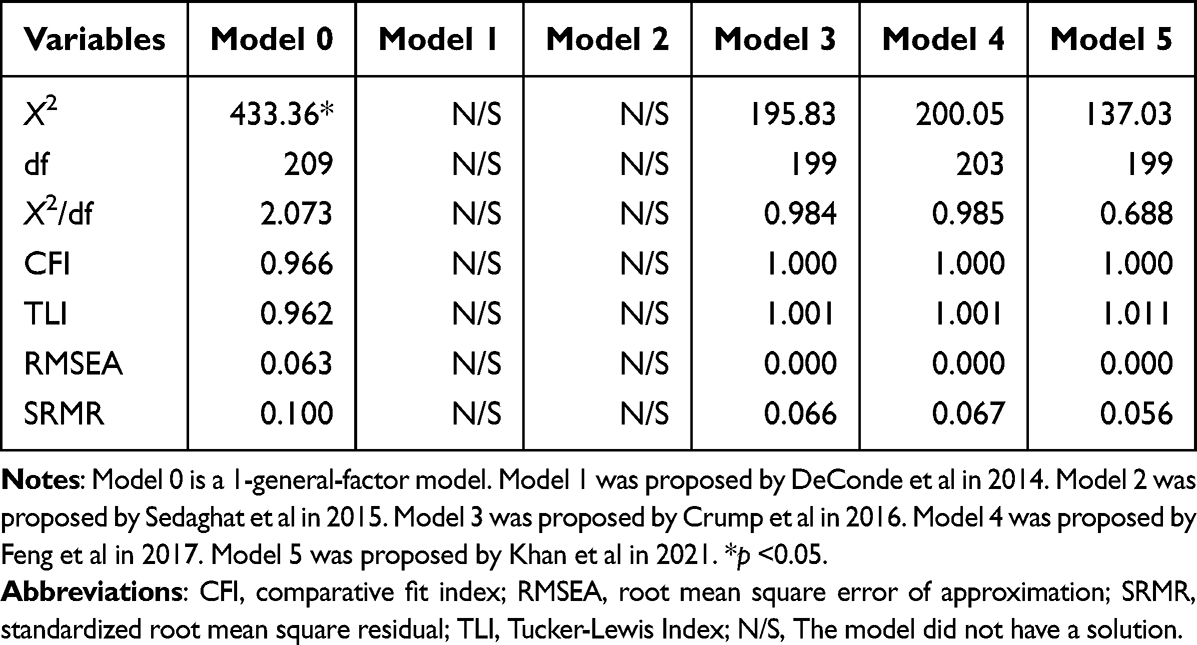 |
Table 2 Goodness-of-Fit Indices for the Sinonasal Outcome Test (SNOT-22) Questionnaire (n = 275) by Model |
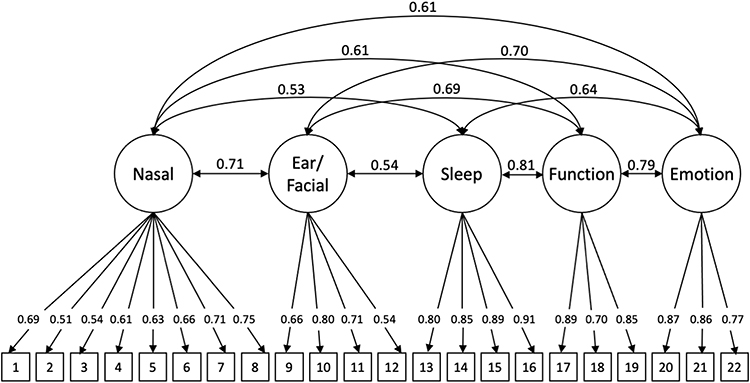 |
Figure 1 The Model is a five-factor (nasal, ear/facial, sleep, function, and emotion) model; the values assigned to arrows were freely estimated. |
The internal consistency was good for the total SNOT-22 score (ω = 0.95) and all domain scores (all ≥ 0.8; Table 3). For test-retest reliability, after excluding one patient who declined to participate, 24 participants, similar to the 275 participants in clinical features (Table S4), completed the second time questionnaires within a median interval of 13 days (range: 1–28 days). The ICC estimate was good for all domain scores, total SNOT-22 score, and ETDQ-7 scores (0.85–0.97; Table S5). Also, all SNOT-22 domains had moderate-to-high correlations with each other (r = 0.45–0.72; Table 3). The ETDQ-7 scores were moderately correlated with ear/facial (r = 0.61) and nasal (r =0.50) domain of the SNOT-22, and the correlations were significantly stronger than that between the ETDQ-7 and other SNOT-22 domain scores (r = 0.33–0.37; p < 0.05).
 |
Table 3 Descriptive Statistics, Bivariate Correlations, and Convergent and Divergent Validity for Sinonasal Outcome Test (SNOT-22) Domains |
Finally, known-group validity was good for the total SNOT-22 score according to the recurrence status (Table S6). Specifically, patients with recurrent disease had significantly higher mean SNOT-22 scores and all domains’ scores, except the sleep domain, than those without recurrence. In addition, younger patients had significantly higher mean nasal, ear/facia, and functional domain scores, as well as mean SNOT-22 scores. Still, they only had slightly higher mean scores but were not statistically significant in the remaining two domains. After adjusting the confounding of the post-RT period and other clinical characteristics in multiple linear regression, recurrence status served as the most influential factor in the SNOT-22 domains (Table 4). In addition, patients whose questionnaires were collected beyond five years after the completion of primary treatment exhibited poorer otorhinologic-related QOL in both the nasal and ear domains.
 |
Table 4 Known-Group Validity for the Domains of the Sinonasal Outcome Test (SNOT-22) Adjusted by Multiple Linear Regression |
Discussion
Our study evaluated the SNOT-22 domain structure in the context of NPC patients. CFA supported a five-factor model including the domains of nasal, ear/facial, sleep, function, and emotion. The internal consistency and test-retest reliability of the SNOT-22 domain scores were good. All SNOT-22 domains were moderately to highly correlated with each other. ETDQ-7 scores were highly correlated with the SNOT-22 ear/facial scores. Known-group validity was good for the SNOT-22 according to the disease recurrence status. In general, the psychometric analyses supported the reliability and validity of the five-factor SNOT-22 model for assessing otorhinologic-related QOL in NPC patients.
As mentioned above, the QLQ-H&N35 and QLQ-C30, which serve as the most commonly used instruments for QOL assessment in NPC patients, do not include items regarding the local otorhinologic side effects of RT, such as CRS, in NPC patients. In contrast to the very limited emphasis on sinonasal and otologic symptoms in QLQ-H&N35 and QLQ-C30, the SNOT-22 questionnaire offers a comprehensive evaluation of otorhinologic conditions in patients with NPC. The SNOT-22, which assesses sinonasal and otologic symptoms in half of the questionnaire (11 of 22 items), has been examined for domain structures in previous studies in patients with CRS.16–20 The domain structures might be applied and evaluated directly in a patient with NPC because the SNOT-22 captures sinonasal/otologic symptom severity, some of the social and emotional impact of disease, and some of the consequences thereof for productivity and sleep, which are all highly considered in the QOL of NPC patients. Although the present study was the first to evaluate the SNOT-22 for otorhinologic-related QOL assessment in NPC patients (to the best of our knowledge), the SNOT-22 has already been used to measure QOL in NPC patients. Li et al found that patients who suffered from recurrent NPC and were treated via salvage endoscopic nasopharyngectomy had poor SNOT-22 scores in the early postoperative period and that the SNOT-22 scores improved to the baseline values ≥ 6 months after surgery.15 However, the change in SNOT-22 domain scores was not clarified by Li et al A similar study of patients with anterior skull base lesions used the SNOT-22 to assess sinonasal-related QOL.30 The above studies demonstrate that SNOT-22 is not specific to CRS; instead, it can be used to evaluate the impact on otorhinologic-related QOL, which may be crucial for NPC patients. Notably, some of the symptoms assessed by the SNOT-22 questionnaire may not exclusively originate from the otorhinologic system, especially when used for evaluating non-sinonasal diseases. For example, cough can be caused by postnasal drip, but it can also be attributed to dysphagia and aspiration as late complications of NPC. Such critical points will necessitate additional research for clarification.
Previous studies have used separate SNOT-22 domains to evaluate specific CRS symptoms in the context of disease outcomes and treatment response (Table S1).16–20 The several proposed models of SNOT-22 domains have been examined in patients with CRS and been considered as informative tools in both research and clinical settings. Therefore, we aimed to identify the most suitable SNOT-22 model for NPC patients through CFA from the proposed five models. The χ2 difference test showed that Model 5 was significantly better than other models in our study. Additionally, Model 5 is a simple model without cross-loading, for which all factor loadings are > 0.5 (Figure 1); thus, it was subjected to further psychometric testing according to the principle of parsimony.31,32 One concern is that Model 5 showed a higher value of SRMR in the 2-year sensitivity analysis model compared to the overall analysis (Table S3). This could be attributed to the limited sample size in the 2-year model, resulting in model instability. Therefore, caution should be exercised when applying this model to patients within the 2-year post-treatment period.
In our study, patients with recurrent disease had significantly higher SNOT-22 total scores than those without recurrence. This result was compatible with Chan’s study, in which the QLQ-C30 and QLQ-H&N35 scores were significantly lower among patients treated for residual or recurrent NPC.33 Additionally, lower function and emotion domain scores were observed in both studies, regardless of whether the QLQ-C30 or SNOT-22 questionnaires were used, among patients with recurrent NPC. This result was reasonable because NPC patients with recurrence might receive secondary curative RT or salvage nasopharyngectomy, which are associated with a higher incidence of locoregional complications and impaired social functioning, as observed by Hammerlid et al34 Regarding the otorhinologic-related QOL in the different periods after primary treatment, the SNOT-22 scores showed significantly higher in nasal and ear/facial domain, as well as total score, 5 years later after RT, indicating some bothersome side effects lasted or late-onset side effects occurred (Table 4). Hsin’s study might explain this result,4 in which the 5-year incidence of post-irradiation CRS and otitis media with effusion in patients with NPC reached 16.7% and 29.4%, respectively. Therefore, otorhinologic-related QOL might be impaired 5 years later after RT. The diverse SNOT-22 scores in different time points after RT hinted that the period after primary treatment was a main confounder and should be considered and adjusted during further analysis. A longitudinal cohort study to survey the continuous change of the SNOT-22 scores after primary RT could be conducted in the future.
Regarding disease severity, some differences were observed in EORTC QLQ-C30 global scores between AJCC stage I–II and III–IV patients.35 However; these differences were not consistently significant in all symptoms scales and follow-up time points. In our study, patients with late-stage (III–IV) disease had slightly higher total scores but was not a significant difference in the domain scores. Two reasons might explain the insignificant difference. First, a similar radiation protocol and dose level (69.96 Gy) were used in the era of intensity-modulated radiotherapy regardless of the stages. Second, our data consisted of NPC patients across a broad period diagnosed with an evolving staging system; therefore, the disease severity result might be unstable.
The findings of our study must be considered in light of the following limitations. First, we excluded patients with difficulty in communication or poor performance status, where some of those patients may have had poor QOL. Therefore, our results could have overestimated the otorhinologic-related QOL of NPC patients. Second, only selected psychometric properties were examined for the SNOT-22 inventory in the context of NPC patients. Other ways of validation may be required in future studies involving large numbers of patients. Third, the very preliminary nature of the evaluation of known-groups validity left further validation in future research. In addition, a comparative analysis between the current SNOT-22 questionnaire and other frequently employed tools for assessing QOL in patients with NPC should be conducted. Fourth, the test-retest reliability included only 24 patients, so the findings from this analysis require a more rigorous evaluation. Lastly, residual confounding remained even though we had taken the diverse post-radiotherapy interval into adjustment, and the effect of the post-radiotherapy time on otorhinologic -related QOL should be further validated.
Conclusion
Our study suggested that a five-factor model (nasal, ear/facial, sleep, function, and emotion domains) might be applied for the SNOT-22 in NPC patients. Moreover, psychometric analyses indicated that the five-factor model was reliable and effective for assessing otorhinologic-related QOL and treatment impact in NPC patients.
Acknowledgment
We appreciate the Biostatistics Center at Kaohsiung Chang Gung Memorial Hospital for helping with the statistics work. We also appreciate all coworkers in the ENT department for their support in the patient collection.
Funding
This work was supported, in part, by grants from Chang Gung Memorial Hospital Research Program (CORPG8K0101 and CORPG8L0391). However, the funders had no role in the study design, data collection, analysis, publication decision, or manuscript preparation.
Disclosure
None of the authors has any conflict of interest.
References
1. Chen YP, Chan ATC, Le QT, Blanchard P, Sun Y, Ma J. Nasopharyngeal carcinoma. Lancet. 2019;394(10192):64–80. doi:10.1016/s0140-6736(19)30956-0
2. Hu CY, Wang WM, Chu XH, Ren ZH, Lyu J. Global, regional, and national burden of nasopharyngeal carcinoma from 1990 to 2017-results from the global burden of disease study 2017. Head Neck. 2020;42(11):3243–3252. doi:10.1002/hed.26378
3. Luo SD, Chen WC, Wu CN, et al. Low-dose aspirin use significantly improves the survival of late-stage NPC: a propensity score-matched cohort study in Taiwan. Cancers. 2020;12(6):1551. doi:10.3390/cancers12061551
4. Hsin CH, Tseng HC, Lin HP, Chen TH. Post-irradiation otitis media, rhinosinusitis, and their interrelationship in nasopharyngeal carcinoma patients treated by IMRT. Eur Arch Otorhinolaryngol. 2016;273(2):471–477. doi:10.1007/s00405-015-3518-8
5. Talmi YP, Horowitz Z, Bedrin L, et al. Quality of life of nasopharyngeal carcinoma patients. Cancer. 2002;94(4):1012–1017. doi:10.1002/cncr.10342
6. Chie WC, Hong RL, Lai CC, Ting LL, Hsu MM. Quality of life in patients of nasopharyngeal carcinoma: validation of the Taiwan Chinese version of the EORTC QLQ-C30 and the EORTC QLQ-H&N35. Qual Life Res. 2003;12(1):93–98. doi:10.1023/a:1022070220328
7. Bian X, Song T, Wu S. Outcomes of xerostomia-related quality of life for nasopharyngeal carcinoma treated by IMRT: based on the EORTC QLQ-C30 and H&N35 questionnaires. Expert Rev Anticancer Ther. 2015;15(1):109–119. doi:10.1586/14737140.2015.961427
8. Tsai WL, Chien CY, Huang HY, Liao KC, Fang FM. Prognostic value of quality of life measured after treatment on subsequent survival in patients with nasopharyngeal carcinoma. Qual Life Res. 2013;22(4):715–723. doi:10.1007/s11136-012-0213-8
9. Bjordal K, Hammerlid E, Ahlner-Elmqvist M, et al. Quality of life in head and neck cancer patients: validation of the European organization for research and treatment of cancer quality of life questionnaire-H&N35. J Clin Oncol. 1999;17(3):1008. doi:10.1200/jco.1999.17.3.1008
10. Tong MC, Lo PS, Wong KH, et al. Development and validation of the functional assessment of cancer therapy nasopharyngeal cancer subscale. Head Neck. 2009;31(6):738–747. doi:10.1002/hed.21023
11. Su Y, C-w M, Cheng W-Q, et al. Development and validation of quality of life scale of nasopharyngeal carcinoma patients: the QOL-NPC (version 2). Health Qual Life Outcomes. 2016;14. doi:10.1186/s12955-016-0480-0
12. Hsu MY, Jiang RS, Hsin CH, Liang KL. Validation of the Taiwanese version of the 22-item sino-nasal outcome test. J Taiwan Otolaryngol Head Neck Surg. 2013;48(1):55–63. doi:10.6286/2013.48.1.55
13. Hopkins C, Gillett S, Slack R, Lund VJ, Browne JP. Psychometric validity of the 22-item Sinonasal outcome test. Clin Otolaryngol. 2009;34(5):447–454. doi:10.1111/j.1749-4486.2009.01995.x
14. Ayoub N, Walgama E, Thamboo A, Nayak JV, Hwang PH. Efficacy of endoscopic sinus surgery for chronic rhinosinusitis following primary radiotherapy and concurrent chemotherapy for nasopharyngeal carcinoma. Int Forum Allergy Rhinol. 2017;7(11):1045–1051. doi:10.1002/alr.22002
15. Li W, Lu H, Liu J, et al. Quality of life following salvage endoscopic nasopharyngectomy in patients with recurrent nasopharyngeal carcinoma: a prospective study. Front Oncol. 2020;10. doi:10.3389/fonc.2020.00437
16. DeConde AS, Bodner TE, Mace JC, Smith TL. Response shift in quality of life after endoscopic sinus surgery for chronic rhinosinusitis. JAMA Otolaryngol Head Neck Surg. 2014;140(8):712–719. doi:10.1001/jamaoto.2014.1045
17. Sedaghat AR, Gray ST, Caradonna SD, Caradonna DS. Clustering of chronic rhinosinusitis symptomatology reveals novel associations with objective clinical and demographic characteristics. Am J Rhinol Allergy. 2015;29(2):100–105. doi:10.2500/ajra.2015.29.4140
18. Crump RT, Liu G, Janjua A, Sutherland JM. Analyzing the 22-item Sino-Nasal outcome test using item response theory. Int Forum Allergy Rhinol. 2016;6(9):914–920. doi:10.1002/alr.21770
19. Feng AL, Wesely NC, Hoehle LP, et al. A validated model for the 22-item Sino-Nasal outcome test subdomain structure in chronic rhinosinusitis. Int Forum Allergy Rhinol. 2017;7(12):1140–1148. doi:10.1002/alr.22025
20. Khan AH, Reaney M, Guillemin I, et al. Development of Sinonasal Outcome Test (SNOT-22) domains in chronic rhinosinusitis with nasal polyps. Laryngoscope. 2021. doi:10.1002/lary.29766
21. Young YH, Hsieh T. Eustachian tube dysfunction in patients with nasopharyngeal carcinoma, pre- and post-irradiation. Eur Arch Otorhinolaryngol. 1992;249(4):206–208. doi:10.1007/bf00178470
22. McCoul ED, Anand VK, Christos PJ. Validating the clinical assessment of eustachian tube dysfunction: the Eustachian Tube Dysfunction Questionnaire (ETDQ-7). Laryngoscope. 2012;122(5):1137–1141. doi:10.1002/lary.23223
23. Lee C-T, Lin C-Y, Tsai M-C, Strong C, Lin Y-C. Psychometric evaluation and wording effects on the Chinese version of the parent-proxy Kid-KINDL. Health Qual Life Outcomes. 2016;14(1):123. doi:10.1186/s12955-016-0526-3
24. Browne MW, Cudeck R. Alternative ways of assessing model fit. Sociol Methods Res. 1992;21(2):230–258. doi:10.1177/0049124192021002005
25. Trizano-Hermosilla I, Alvarado JM. Best alternatives to cronbach’s alpha reliability in realistic conditions: congeneric and asymmetrical measurements. Front Psychol. 2016;7. doi:10.3389/fpsyg.2016.00769
26. Koo TK, Li MY. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropr Med. 2016;15(2):155–163. doi:10.1016/j.jcm.2016.02.012
27. Akoglu H. User’s guide to correlation coefficients. Turk J Emerg Med. 2018;18(3):91–93. doi:10.1016/j.tjem.2018.08.001
28. Fisher RA. Frequency distribution of the values of the correlation coefficient in samples from an indefinitely large population. Biometrika. 1915;10(4):507–521.
29. Fisher RA. On the’probable error’of a coefficient of correlation deduced from a small sample. Metron. 1921;1:1–32.
30. McCoul ED, Anand VK, Bedrosian JC, Schwartz TH. Endoscopic skull base surgery and its impact on sinonasal-related quality of life. Int Forum Allergy Rhinol. 2012;2(2):174–181. doi:10.1002/alr.21008
31. Vandekerckhove J, Matzke D, Wagenmakers E-J. Model comparison and the principle of parsimony. In: The Oxford Handbook of Computational and Mathematical Psychology. Oxford University Press; 2015:300–319.
32. Busemeyer JR, Wang Z, Townsend JT, Eidels A. The Oxford Handbook of Computational and Mathematical Psychology. Oxford University Press; 2015:300–319.
33. Chan YW, Chow VLY, Wei WI. Quality of life of patients after salvage nasopharyngectomy for recurrent nasopharyngeal carcinoma. Cancer. 2012;118(15):3710–3718. doi:10.1002/cncr.26719
34. Hammerlid E, Bjordal K, Ahlner-Elmqvist M, et al. A prospective study of quality of life in head and neck cancer patients. Part I: at diagnosis. Laryngoscope. 2001;111(4 Pt 1):669–680. doi:10.1097/00005537-200104000-00021
35. Liao KC, Chuang HC, Chien CY, et al. Quality of life as a mediator between cancer stage and long-term mortality in nasopharyngeal cancer patients treated with intensity-modulated radiotherapy. Cancers. 2021;13(20):5063. doi:10.3390/cancers13205063
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.