")
Back to Journals » International Journal of General Medicine » Volume 13
Evaluation of Serum Level of FGF23 and 1,25(OH)2D3 in Primary Hyperparathyroidism Patients Before and After Parathyroidectomy
Authors Hassani S, Afkhamizadeh M , Teimouri A , Najaf Najafi M, Vazifeh Mostaan L, Mohebbi M
Received 10 March 2020
Accepted for publication 28 May 2020
Published 11 June 2020 Volume 2020:13 Pages 289—295
DOI https://doi.org/10.2147/IJGM.S253246
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Solmaz Hassani,1 Mozhgan Afkhamizadeh,1 Ali Teimouri,2 Mona Najaf Najafi,3 Leila Vazifeh Mostaan,4 Masoud Mohebbi1
1Metabolic Syndrome Research Center, Mashhad University of Medical Sciences, Mashhad, Iran; 2Student Research Committee, Mashhad University of Medical Sciences, Mashhad, Iran; 3Clinical Research Development Unit, Imam Reza Hospital, Mashhad University of Medical Sciences, Mashhad, Iran; 4Cancer Research Center, Mashhad University of Medical Sciences, Mashhad, Iran
Correspondence: Masoud Mohebbi
Emam Reza Hospital, Mashhad 9137913316, Iran
Tel +98-9155123712
Fax +98-5138022370
Email [email protected]
Purpose: Parathyroid hormone (PTH) and fibroblast growth factor 23 (FGF23) play critical roles in phosphate homeostasis. To the best of our knowledge, there are limited data on the impact of FGF23 and PTH on serum calcium, 1,25(OH)2D3, and phosphate in patients with primary hyperparathyroidism (PHPT). We examined these parameters and their correlations in PHPT patients before and after parathyroidectomy (PTX).
Patients and Methods: In this prospective cohort study, 29 PHPT patients who met the inclusion criteria were selected. The patient’s blood samples were taken three times: before the operation, 24 h after the operation, and 1 week after the operation. The concentrations of serum calcium, FGF23, 1,25(OH)2D3, phosphate, PTH, and alkaline phosphatase were measured in a referral laboratory at each of the three steps. Moreover, 25(OH)D was primarily measured just before the surgery.
Results: Of 29 patients included in this study with a mean age of 52.37± 12.3 years, majority were females (75.8%). Serum FGF23 and 1,25(OH)2D3 levels were high before PTX and decreased after the operation; however, the difference was not statistically significant. FGF23 levels were significantly correlated with 1,25(OH)2D3 at each of the three steps (r=0.964, P < 0.01; r=0.985, P < 0.0; and r=0.976, P < 0.05). The variations in calcium, phosphate, creatinine, and PTH were preoperatively and postoperatively significant.
Conclusion: Although 1,25(OH)2D3 and FGF23 levels were preoperatively higher in PHPT, their variations were not meaningful. There was a statistically direct significant relationship between 1,25(OH)2D3 and FGF23 preoperatively and postoperatively; however, the correlations between FGF23 and calcium, phosphate, and PTH were not significant.
Keywords: vitamin D, parathyroid glands, surgery, parathyroid hormone, fibroblast growth factor 23, endocrine disease
Introduction
The occurrence of hypercalcemia can mainly be attributed to primary hyperparathyroidism (PHPT)1 as PHPT is characterized by hypercalcemia with an elevated or inappropriate parathyroid hormone (PTH) level.1 The prevalence rate of PHPT is 0.1–1% with an incidence rate of 25–30 cases per 100.000 persons worldwide.1,2 PHPT appears in the early postmenopausal years more remarkably.1
About 80% of multiglandular and PHPT diseases are attributed to solitary benign adenoma. Moreover, 4-gland parathyroid hyperplasia accounts for about 15–20% of PHPT cases. Furthermore, parathyroid carcinoma is a rare factor leading to PTPH and accounts for about 1% of PHPT cases.3 Only 5–10% of all PHPT cases are heredity, and the other are caused by some mutations, including hyperparathyroid jaw-tumor syndrome (HPT-JT), multiple endocrine neoplasia types 1, 2a, and 4 (MEN 1, MEN 2a, and MEN 4, respectively), neonatal severe primary hyperparathyroidism (NSHPT), familial isolated hyperparathyroidism (FIHP), and familial hypocalciuric hypercalcemia (FHH).1
There are risk factors (namely low physical activity, low calcium intake, hypertension, high body weight, lithium therapy, loop diuretic usage, and external radiation on neck), which are associated with developing PHPT.4–7
According to the clinical manifestations of PHPT, there are two types of PHPT: asymptomatic PHPT, and symptomatic PHPT (accounting for a small portion of PHPH cases, <20%).8
The most frequently observed signs and symptoms in symptomatic PHPT are nephrolithiasis, decreased renal function, peptic ulcer disease, pancreatitis, fragility fractures, bone pain, skeletal deformities, osteitis fibrosa cystica (OFC), hyperreflexia, proximal muscle weakness, and mental status changes.1
Asymptomatic Hyperparathyroidism also arouses a large number of PHPT cases (>80%). This disorder is recognized with an elevation of serum calcium levels in biochemical evaluations.8 In this regard, parathyroidectomy (PTX) is known as a treatment for PHPT.1
Fibroblast growth factor 23 (FGF23), mainly secreted by osteoblasts and osteocytes, controls phosphate hemostasis and vitamin D metabolism.9 The role of FGF23 in the kidney is αKlotho-dependent.9 When FGF23 attaches to the fibroblast growth factor receptor (FGFR) at the proximal convoluted renal tubules, sodium-phosphate co-transport protein (NPt2a) is down-regulated, and 1a-hydroxylase enzyme is inhibited. Consequently, FGF23 suppresses phosphate reabsorption from urine and decreases the active metabolite of vitamin D (1,25(OH)2D).10 At the distal convoluted renal tubules, FGF23 up-regulates the sodium-chloride co-transporter (NCC) and the epithelial calcium channel transient receptor potential vanilloid-5 (TRPV5), leading to an increase in the reabsorption of sodium and calcium from urine.10
The regulation mechanism of FGF23 contains three main regulators, including 1,25(OH)2D, PTH, and phosphate,11 the most important of which is 1,25(OH)2D as it increases the secretion of FGF23.11 The function of phosphate levels in regulating FGF23 is unknown yet.11 According to some animal studies, phosphate increases FGF23 levels; however, FGF23 levels of high-phosphate or low-phosphate diets were variable in human studies.11,12
Patients with PHPT displayed a high FGF23 level, while those with chronic kidney disease (CKD) undergoing parathyroidectomy showed a decrease in FGF23 level. Accordingly, PTH may increase FGF23 level.13,14 In contrast, hypoparathyroidism patients showed an increase in FGF23 level despite the low concentrations of PTH.15 According to these controversial findings, the effects of PTH on FGF23 may depend on mineral status and vitamin D level.11
The present study aimed to evaluate the relationships between PTH, 1,25(OH)2D3, and FGF23 levels in PHPT patients and the correlations between FGF23, calcium, and phosphate after PTX operation.
Patients and Methods
The present prospective cohort study was conducted from April 2018 to April 2019 on patients with PHPT complaints, who referred to Department of Endocrinology, Imam Reza Hospital, Mashhad, Iran.
With regard to the inclusion criteria of this study (ie, candidate for PTX), 29 patients with PHPT were evaluated.
Afterward, the patients undergoing asymptomatic primary hyperparathyroidism were selected based on the following criteria: serum calcium levels 1 mg/dl above the upper limit of the normal range (>11.5 mg/dl), below 50 years old, glomerular filtration rate (eGFR) < 60 mL/min, a history of fracture fragility, and T-score <2.5 SD.16 The exclusion criteria were as follows: being unwilling to continue the study, experiencing unsuccessful PTX, using Estrogen and Progestin, and taking vitamin D supplements.17
Factors such as serum phosphate, 1,25(OH)2D3, calcium vitamin D, alkaline phosphatase (ALP), PTH, urea, creatinine (Cr), FGF23, and 24-hour urine for calcium were first checked in the same laboratory. Furthermore, the patients’ serum phosphate, calcium, 1,25(OH)2D3, ALP, PTH, Cr, and FGF23 were checked 24 hours and 7 days after PTX.
Sample Size
Considering the limited number of patients, all PHPT patients, who were candidates for PTX and referred to Department of Endocrinology, Imam Reza Hospital, Mashhad, Iran, were included in the study.
Ethical Considerations
After explaining the objectives of the study to the patients, they were asked to submit their written informed consent to participate in the study. The patients’ information remained confidential and was recorded in the form of codes.
This study was conducted following the Declaration of Helsinki and was approved by the vice-chancellor and ethics committee of research at Mashhad University of Medical Sciences (IR.MUMS.MEDICAL.REC.1398.069).
Statistical Analysis
The statistical Stata software (Release 12) was employed for the data analysis. In this study, P < 0.05 was considered as the significance level.
Descriptive statistics, including mean and standard deviation, were used to describe the data. Kolmogorov–Smirnov (K-S) test was used to compare a sample with a reference probability distribution. Moreover, the Pearson correlation coefficient and Spearman’s rank correlation coefficient were utilized to measure the rank correlation. Moreover, Friedman test was used to detect differences in the data before and after PTX. The means were also compared using Wilcoxon signed-rank test.
Results
In this study, there were 29 patients who met the inclusion criteria. In terms of gender and age, there were seven males (24.14%) patients with the age range of 52.3±12.3 years, four patients (13.79%) with 24-hour urine for calcium >400 mg/24 hours, and 12 patients (41.38%) with a history of nephrolithiasis (Table 1).
 |
Table 1 Pre-Parathyroidectomy Characteristics of Patients with Primary Hyperparathyroidism |
All the patients underwent parathyroid MIBI scans and parathyroid ultrasonography. According to MIBI scan, 26 patients (89.65%) had an adenoma; however, with regard to parathyroid ultrasonography, 16 patients (55.17%) had an adenoma. According to the post-operation pathology report, 27 patients (93.10%) had an adenoma, one patient (3.44%) had hypertrophic parathyroid, and one patient (3.44%) had reactivated follicular lymphadenopathy.
Moreover, six patients (20.68%) underwent bone mineral density (BMD) using dual-energy X-ray absorptiometry (DXA) at distal one-third radius, five patients (83%) showed osteoporosis, and one patient (17%) exhibited normal BMD.
Furthermore, 19 patients (65.51%) underwent BMD using DXA at both femoral and lumbar spines, among whom there were nine patients (47.36%) with osteoporosis at both sites, one patient (5.26%) with osteopenia at both sites, two patients (10.52%) with osteoporosis at femoral site and osteopenia at lumbar site, one patient (5.26%) with osteopenia at femoral site and osteoporosis at lumbar site, and four patients (21.05%) with normal BMD at both sites.
The correlation coefficients of FGF23 and 1,25(OH)2D3 were 0.962 before PTX with a p-value of <0.0001, 0.951 and 0.962 a day and a week after PTX with the same p-value, respectively. As shown in Table 2, the results reveal a strong correlation between FGF23 and 1,25(OH)2D3 at pre-PTX, one day after PTX and one week after PTX stages (p < 0.0001) (Figures 1–3).
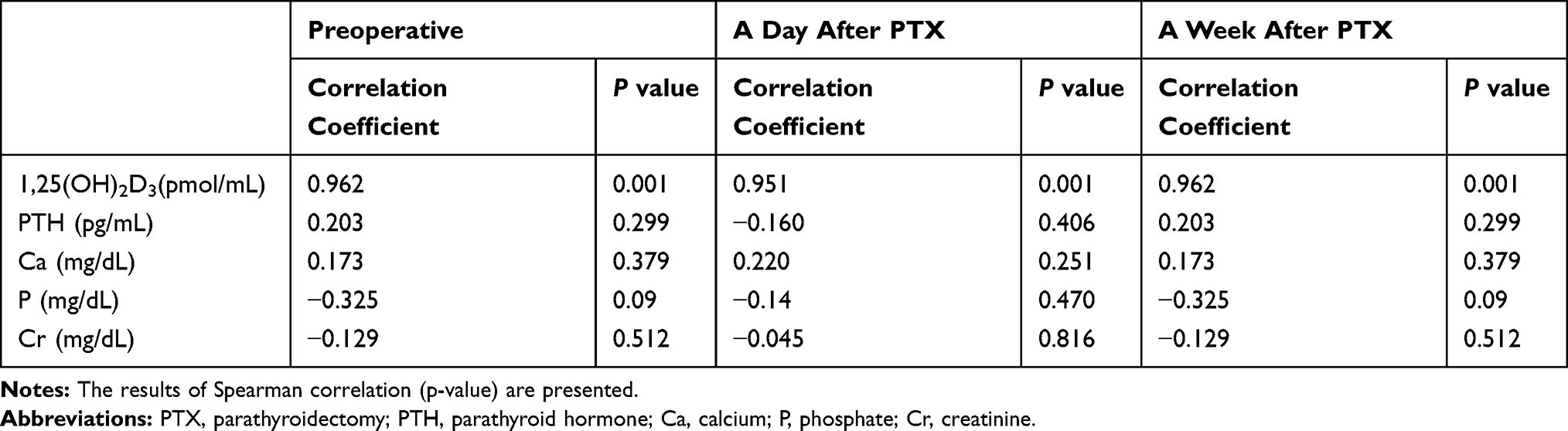 |
Table 2 Correlation Between FGF23 and Other Variables at Preoperative and Postoperative Stages |
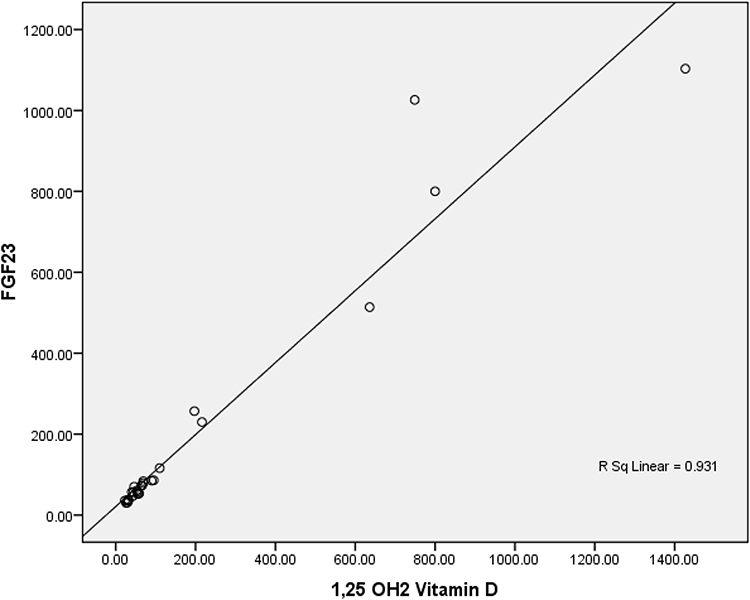 |
Figure 1 Correlation between serum FGF23 and 1,25(OH)2D3 levels before parathyroidectomy. |
 |
Figure 2 Correlation between serum FGF23 and 1,25(OH)2D3 levels a day after parathyroidectomy. |
 |
Figure 3 Correlation between serum FGF23 and 1,25(OH)2D3 levels a week after parathyroidectomy. |
As presented in Table 2, the correlation coefficients of FGF23 and PTH, serum calcium levels, and PTH were significant in pre-PTX, a day after PTX, and a week after PTX stages (p > 0.05).
As expected and shown in Table 3, there were a statistically significant increase in phosphate levels and a statistically significant decrease in serum calcium levels after PTX (p < 0.05).
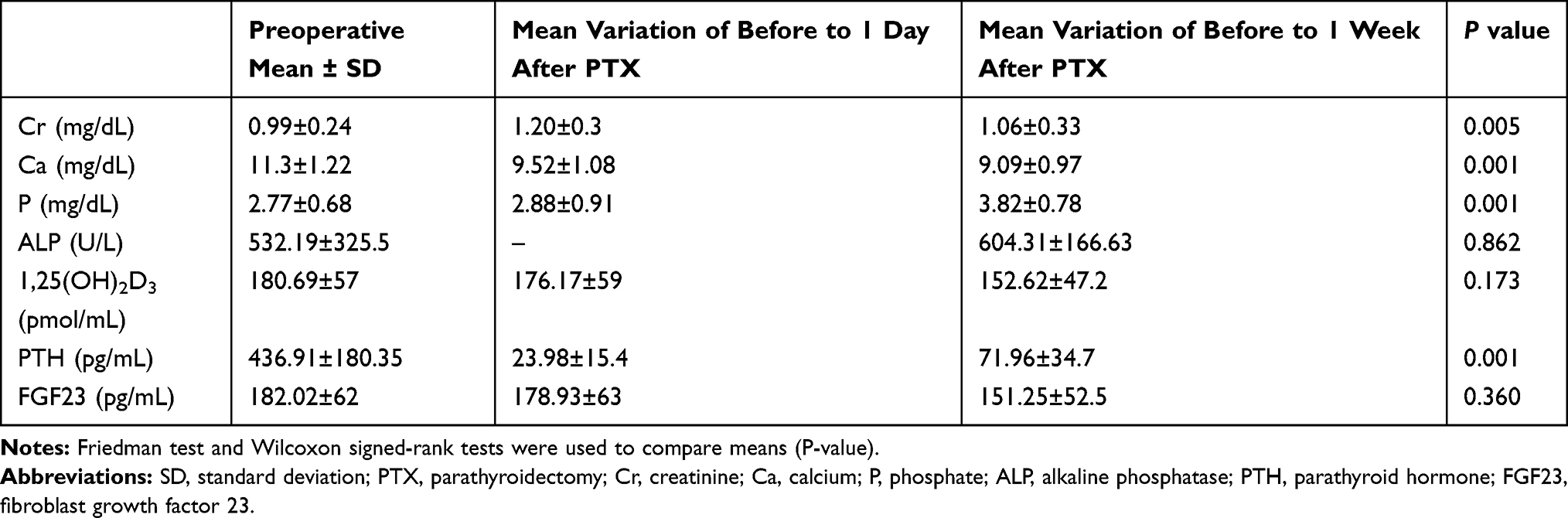 |
Table 3 Variations After Parathyroidectomy |
As shown in Table 3, the fluctuations of 1,25(OH)2D3, FGF23, Cr, and ALP levels were not statistically significant (p > 0.05).
According to Table 3, the concentration of serum PTH before PTX was 436.91 pg/mL and decreased by 23.98 pg/mL one day after PTX and raised once more by 71.96 pg/mL one week after PTX. In this regard, the variations were significant (P=0.001).
Discussion
According to the findings of the present study, there is a statistically significant positive relationship between 1,25(OH)2D3 and FGF23 preoperatively and postoperatively.
Using different methods and approaches, a large number of studies have investigated the effect of PHPT on FGF23 levels. For example, Kobayashi et al studied the association between serum FGF23 levels in PHPT patients.18 In their study, FGF-23 significantly increased in PHPT patients, in comparison to 18 PTX patients and the control group; however, postoperative FGF-23 levels declined significantly, in comparison to the preoperative levels.18 In the present study, post-PTX FGF-23 levels declined in comparison to pre-PTX; however, the variations were not statistically significant.
Witteveen et al investigated the relationship between FGF23 and PTH in PHPT patients and the euparathyroid patients undergoing successful PTX. They found out that FGF23 was considerably higher in PHPT patients, compared to the euparathyroid patients. Moreover, a significant relationship between PTH and FGF23 levels was also reported in their study.9
Yamashita et al noticed a significantly higher plasma FGF23 level in the PHPT patients, compared to the control group. They observed no variation in post-PTX FGF23 levels, while the calcium levels were normalized.19
They observed a positive correlation of FGF23 with PTH and serum calcium and a negative correlation of FGF23 with 1,25(OH)2D3.19 Unlike the study of Yamashita et al, in our study, FGF23 correlated positively with 1,25(OH)2D3.
Tebben et al found the similarity between FGF23 levels one day and six weeks after PTX and reported no significant correlation between FGF23 levels and serum calcium, phosphate, 25(OH)2D, and PTH levels in the post-PTX and pre-PTX stages.20
This study has potential limitations include, absence of healthy patients as a control group, the insufficient sample size due to the rarity of PHPT disease, and a short follow up period.
Conclusion
According to the findings, although 1,25(OH)2D3 and FGF23 levels were preoperatively higher in PHPT, their variations were not statistically significant. Moreover, there was a positive and significant correlation between 1,25(OH)2D3 and FGF23 preoperatively and postoperatively. The correlations between FGF23 and calcium, phosphate, and PTH were not significant; however, the variations of these parameters were significant.
Acknowledgments
This research was funded by the Mashhad University of Medical Sciences (MUMS).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Silva BC, Cusano NE, Bilezikian JP. Primary hyperparathyroidism. Best Pract Res Clin Endocrinol Metab. 2018;32(5):593–607. doi:10.1016/j.beem.2018.09.004
2. Madkhali T, Alhefdhi A, Chen H, Elfenbein D. Primary hyperparathyroidism. Ulus Cerrahi Derg. 2016;32(1):58–66. doi:10.5152/UCD.2015.3032
3. Khan AA, Hanley DA, Rizzoli R, et al. Primary hyperparathyroidism: review and recommendations on evaluation, diagnosis, and management. A Canadian and international consensus. Osteoporos Int. 2017;28(1):1–19. doi:10.1007/s00198-016-3716-2
4. Paik JM, Curhan GC, Taylor EN. Calcium intake and risk of primary hyperparathyroidism in women: prospective cohort study. BMJ. 2012;345:e6390. doi:10.1136/bmj.e6390
5. Boehm BO, Rosinger S, Belyi D, Dietrich JW. The parathyroid as a target for radiation damage. N Engl J Med. 2011;365(7):676–678. doi:10.1056/NEJMc1104982
6. Vaidya A, Curhan GC, Paik JM, Kronenberg H, Taylor EN. Hypertension, antihypertensive medications, and risk of incident primary hyperparathyroidism. J Clin Endocrinol Metab. 2015;100(6):2396–2404. doi:10.1210/jc.2015-1619
7. Szalat A, Mazeh H, Freund HR. Lithium-associated hyperparathyroidism: report of four cases and review of the literature. Eur J Endocrinol. 2009;160(2):317–323. doi:10.1530/EJE-08-0620
8. Suliburk JW, Perrier ND. Primary hyperparathyroidism. Oncologist. 2007;12(6):644–653. doi:10.1634/theoncologist.12-6-644
9. Witteveen JE, van Lierop AH, Papapoulos SE, Hamdy NAT. Increased circulating levels of FGF23: an adaptive response in primary hyperparathyroidism? Eur J Endocrinol. 2012;166(1):55–60. doi:10.1530/EJE-11-0523
10. Erben RG. Physiological actions of fibroblast growth factor-23. Front Endocrinol (Lausanne). 2018;9:267. doi:10.3389/fendo.2018.00267
11. Martin A, David V, Quarles LD. Regulation and function of the FGF23/klotho endocrine pathways. Physiol Rev. 2012;92(1):131–155. doi:10.1152/physrev.00002.2011
12. Perwad F, Azam N, Zhang MYH, Yamashita T, Tenenhouse HS, Portale AA. Dietary and serum phosphorus regulate fibroblast growth factor 23 expression and 1,25-dihydroxyvitamin D metabolism in mice. Endocrinology. 2005;146(12):5358–5364. doi:10.1210/en.2005-0777
13. Sato T, Tominaga Y, Ueki T, et al. Total parathyroidectomy reduces elevated circulating fibroblast growth factor 23 in advanced secondary hyperparathyroidism. Am J Kidney Dis. 2004;44(3):481–487. doi:10.1016/S0272-6386(04)00817-0
14. Kawata T, Imanishi Y, Kobayashi K, et al. Parathyroid hormone regulates fibroblast growth factor-23 in a mouse model of primary hyperparathyroidism. J Am Soc Nephrol. 2007;18(10):2683–2688. doi:10.1681/ASN.2006070783
15. Gupta A, Winer K, Econs MJ, Marx SJ, Collins MT. FGF-23 is elevated by chronic hyperphosphatemia. J Clin Endocrinol Metab. 2004;89(9):4489–4492. doi:10.1210/jc.2004-0724
16. McDow AD, Sippel RS. Should symptoms be considered an indication for parathyroidectomy in primary hyperparathyroidism? Clin Med Insights Endocrinol Diabetes. 2018;11:1179551418785135. doi:10.1177/1179551418785135
17. Ix JH, Chonchol M, Laughlin GA, Shlipak MG, Whooley MA. Relation of sex and estrogen therapy to serum fibroblast growth factor 23, serum phosphorus, and urine phosphorus: the heart and soul study. Am J Kidney Dis. 2011;58(5):737–745. doi:10.1053/j.ajkd.2011.06.011
18. Kobayashi K, Imanishi Y, Miyauchi A, et al. Regulation of plasma fibroblast growth factor 23 by calcium in primary hyperparathyroidism. Eur J Endocrinol. 2006;154(1):93–99. doi:10.1530/eje.1.02053
19. Yamashita H, Yamashita T, Miyamoto M, et al. Fibroblast growth factor (FGF)-23 in patients with primary hyperparathyroidism. Eur J Endocrinol. 2004;151(1):55–60. doi:10.1530/eje.0.1510055
20. Tebben PJ, Singh RJ, Clarke BL, Kumar R. Fibroblast growth factor 23, parathyroid hormone, and 1alpha,25-dihydroxyvitamin D in surgically treated primary hyperparathyroidism. Mayo Clin Proc. 2004;79(12):1508–1513. doi:10.4065/79.12.1508
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.