Back to Journals » Journal of Hepatocellular Carcinoma » Volume 13
Evaluation of Prophylactic EGD versus Beta Blockade in Hepatocellular Carcinoma Patients on Anti-Angiogenic Cancer Treatments
Authors Kontoyiannis PD, Ayerbe C, Chan KH, Soliman S, Machicao V, Rowe JH ![]()
Received 7 November 2025
Accepted for publication 27 February 2026
Published 27 March 2026 Volume 2026:13 575052
DOI https://doi.org/10.2147/JHC.S575052
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Mohamed Shaker
Panayiotis D Kontoyiannis,1 Camila Ayerbe,2 Kok Hoe Chan,3 Sara Soliman,4 Victor Machicao,5 Julie H Rowe4
1Department of Internal Medicine, The University of Southwestern Medical Center, Dallas, TX, USA; 2Department of Internal Medicine and Pediatrics, The University of Southwestern Medical Center, Dallas, TX, USA; 3Department of Medicine, CAMC Institute for Academic Medicine, Charleston Area Medical Center, Charleston, WV, USA; 4Department of Internal Medicine, Division of Oncology, McGovern Medical School, The University of Texas Health Science Center at Houston, Houston, TX, USA; 5Department of Internal Medicine, Division of Hepatology, McGovern Medical School, The University of Texas Health Science Center at Houston, Houston, TX, USA
Correspondence: Julie H Rowe, Department of Internal Medicine, Division of Oncology, The University of Texas Health Science Center at Houston, 6410 Fannin St., Ste. 830, Houston, TX, 77030, USA, Email [email protected]
Introduction
Most patients diagnosed with hepatocellular carcinoma (HCC) in the United States have a concomitant diagnosis of cirrhosis. Esophageal variceal bleeding is one of the most serious and lethal complications in patients with cirrhosis. Gastrointestinal bleeding is a well-described complication of anti-vascular endothelial growth factor (VEGF) therapy and multi-kinase inhibitors; drugs commonly used in the treatment of HCC.
The performance of esophagogastroduodenoscopy (EGD) has been recommended in patients with either compensated or decompensated cirrhosis to ascertain the presence of varices, with the goal of starting primary prophylaxis in the patients at high risk for bleeding.1 The presence of large esophageal varices (>5 mm diameter) or red marks seen during EGD allow the identification of the patients at high risk of bleeding. Valid interventions to decrease the risk of variceal bleeding include the initiation of non-selective beta-blockers (NSBBs) or endoscopic variceal ligation (EVL). However, the best strategy in a patient with compensated cirrhosis is the use of NSBB, since it may also decrease the risk of decompensation, including decreasing the risk of development of ascites or hepatic encephalopathy.2
The recommendation of EGD prior to the initiation of anti-VEGF or multi-kinase therapy has been endorsed by the American Association for the Study of Liver Disease (AASLD) in their practice guidance.3 HCC clinical trials often include either an inclusion or exclusion criterion for EGD to be done within 6 months of enrollment of the study (ie, IMbrave150 evaluating atezolizumab and bevacizumab in advanced unresectable HCC or EMERALD-1 and EMERALD-1 included patients on durvalumab with or without bevacizumab with transarterial chemoembolisation).4,5 In clinical practice, there are scenarios in which systemic chemotherapy for patients with advanced HCC and cirrhosis is started before endoscopic investigation could be completed. We investigated the bleeding outcomes of patients starting systemic therapy for HCC without undergoing recent EGD investigation (in the preceding 6 months) before starting therapy, compared with a cohort of patients with endoscopic investigation completed in the preceding 6 months.
Methods
We conducted a retrospective study of patients diagnosed with unresectable HCC deemed to candidates for systemic chemotherapy at our institution between January 1, 2018, and December 31, 2022. Our study complies with Declaration of Helsinki. Diagnoses among our patients included advanced stage HCC (BCLC Stage C) and intermediate stage HCC (BCLC B) that progressed despite locoregional therapy. Information on if any locoregional therapy such as transarterial chemoembolisation or ytrium-90 radioembolisation was not obtained. Data on demographics, clinical findings, and treatment outcomes were analyzed (Table 1). Data on EGD including whether procedure was done within 6 months prior to starting HCC systemic therapy and if done, what findings were seen. Data on beta blockade including the time of initiation were gathered. Patients could have received EGD and been on beta-blockade so are not mutually exclusive. Descriptive statistics, including percentages, medians, and interquartile ranges, were used. Fisher’s exact and the Wilcoxon rank-sum tests identified significant differences, with p-value <0.05 deemed statistically significant. The Cox proportional-hazards model compared overall survival (OS), using GraphPad Prism version 10.1.0 for data analysis.
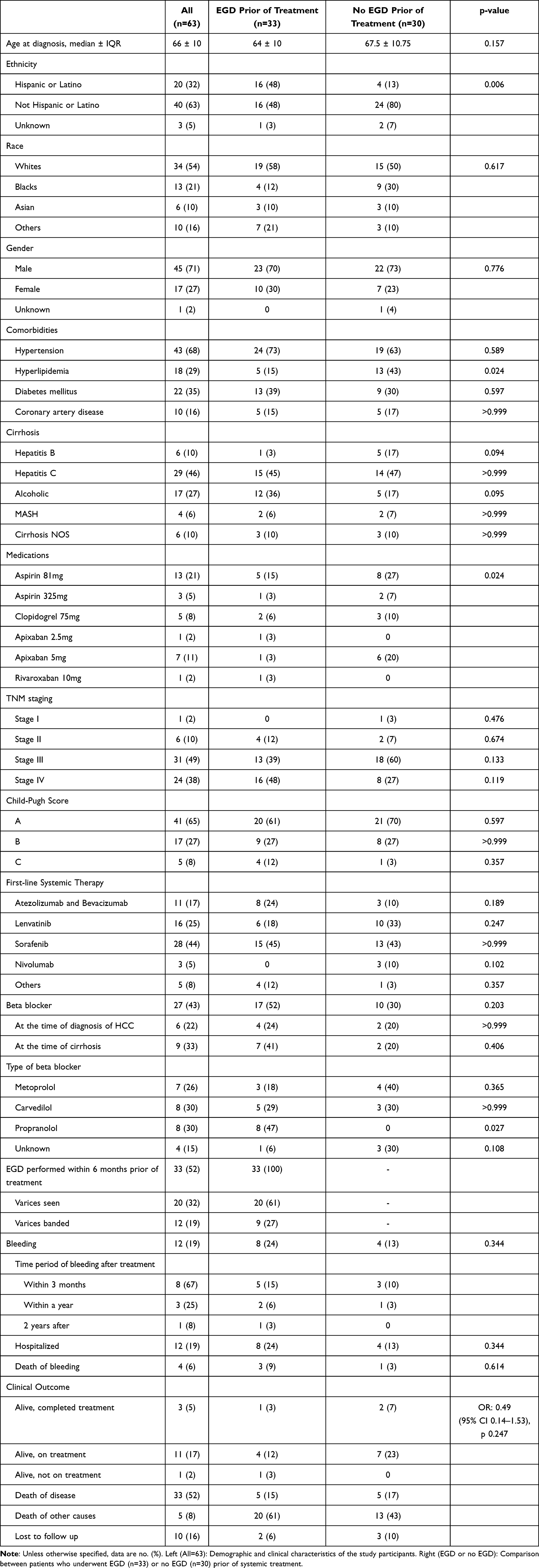 |
Table 1 Demographics and Clinical Characteristics of Study Participants |
Results
A total of 63 patients were started on systemic chemotherapy for HCC during the study period. The median age at time of starting treatment was 66 (range 49–89) years, with 71% male, 63% non-Hispanic, and 32% Hispanic ethnicity. All patients except one carried a diagnosis of cirrhosis. The main causes of cirrhosis were hepatitis C virus infection (46%) and alcoholic liver disease (27%). Medication-related bleeding risks were assessed, with 40% (n=25) of patients on therapies such as aspirin, clopidogrel, apixaban, and rivaroxaban. Sixteen (25%) patients were on antiplatelet agents (aspirin and/or clopidogrel) and 9 (14%) were on direct oral anticoagulants, including apixaban and rivaroxaban.
Based on TNM staging, this cohort consisted of mostly Stage 3 (49%) and Stage 4 (38%) disease; however, 65% of cases were Child-Pugh A and 27% were Child-Pugh B. Initial chemotherapy included combination therapy with a VEGF inhibitor combined with an immune checkpoint inhibitor (bevacizumab and atezolizumab, respectively; n=11), VEGF-receptor multi-kinase inhibitor therapies including lenvatinib and sorafenib (n=44), and single-agent immune checkpoint inhibitors (n=3).
Of the 63 patients, 11 experienced a GI bleed. Only 27 were on NSBBs, of whom 6 were on or prescribed NSBBs at HCC presentation, with 9 receiving NSBBs at cirrhosis diagnosis. Of the 15 patients who were prescribed NSBBs at HCC or cirrhosis diagnosis, only 2 had a GI bleed: both with Child-Pugh A6 disease, one of whom experienced a GI bleed within the first 3 months of treatment and the other within the 2nd year of diagnosis of HCC but who was also on aspirin 81 mg and apixaban 5 mg. Thirty-three patients underwent EGD within the 6 months preceding treatment, revealing varices in 12 cases. Of these patients, 8 experienced bleeding within 3 months of chemotherapy. All 8 of these patients were hospitalized, and 3 died. The patients who died from their GI bleed had Child-Pugh scores of A6, B8, and B9. Of the 17 patients who were on NSBBs and had EGD prior to treatment, 3 had a GI bleed within the first 3 months of treatment, 2 of whom died. These 2 patients both had a Child-Pugh score of A6; one was on aspirin 81 mg and clopidogrel 75 mg and aspirin of 81 mg and apixaban 5 mg.
Additional subset analysis of patients who were Child-Pugh A were completed (Table 2). Among patients with Child-Pugh A (CPA) disease (n=41), no significant difference in bleeding outcomes was observed based on prophylactic EGD (p=0.597). Similarly, no significant difference was seen in bleeding outcomes between patients who received NSBBs without EGD and those who only underwent EGD (p=0.659). No statistical difference in bleeding outcomes was identified between patients who received VEGF-R versus multi-kinase inhibitors (p=0.193). Additionally, there were no difference in survival outcomes in patients who received EGD prior to systemic therapy compared to those who had no EGD (HR: 1.07, 95% CI 0.56–2.04; p=0.831) (Figure 1). When comparing patients who had no prior EGD but were on beta blocker (n=10) versus EGD was done prior to systemic treatment (n=20), a majority were CPA. A subgroup analysis among this population found no significant differences in bleeding (p>0.999) and no differences in survival (HR 0.97, 95% CI 0.37–2.58; p=0.9588). Of the 63 patients, 11 are alive and on treatment and 1 is alive but not on treatment; 33 patients are dead due to HCC and 10 patients are lost to follow-up (Figure 2).
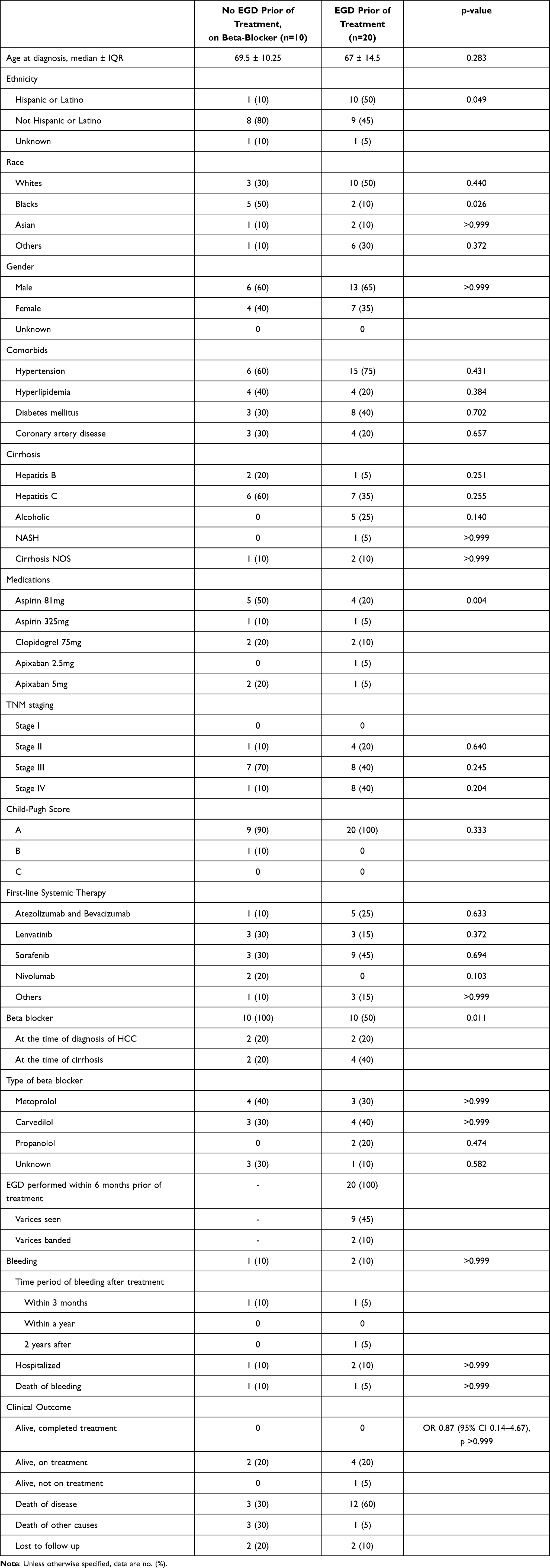 |
Table 2 Sub-Group Analysis of Child-Pugh A Patients Who Had No EGD but on Beta-Blocker versus EGD Prior to Systemic Treatment |
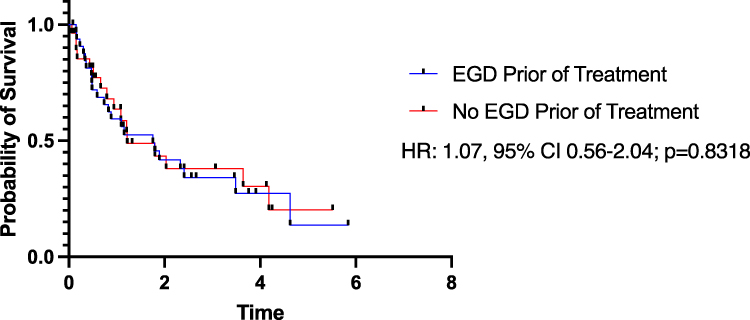 |
Figure 1 Survival curves of patients who had no EGD prior to treatment versus those who underwent EGD prior to treatment. |
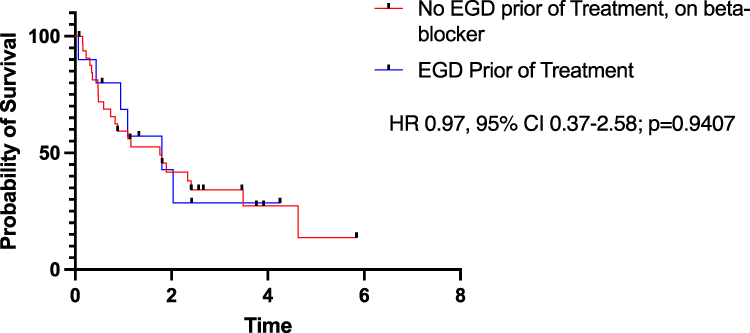 |
Figure 2 Survival curves of patients who had no EGD prior to treatment and on beta blocker versus those who underwent EGD prior to treatment. |
Discussion
The findings from our study highlight the complexity of gastrointestinal bleeding risk in patients with HCC undergoing systemic therapy. While it is well understood that cirrhosis-associated portal hypertension contributes significantly to GI bleeding, our study suggests that prophylactic EGD may not necessarily reduce bleeding risks compared to NSBBs alone in patients. In our study, there are differences in the Child-Pugh scores between those who had beta-blockade versus prophylactic EGD which may diminish the effectiveness of EGD in reducing bleeding risks. This lack of statistical differences and the small sample size underscore the need for further research to refine risk stratification and preventive strategies. Our study is not a clean comparison of two separate populations who underwent prophylactic EGD versus those were were only on beta blockade; the patients included in this study did undergo prophylactic EGD prior to systemic therapy (n=33), were started on beta-blockade (n=27), or underwent prophylactic EGD and beta-blockade (n=17). Future randomized studies should be done to evaluate if there are different clinical outcomes. The role of non-invasive tests to predict the presence of gastroesophageal varices has been explored with ultrasound, computed tomography, magnetic resonance imaging, and most recently transient elastrography (TE), which assess liver stiffness (LS). Based on the 2016 practice guidelines by the AASLD, it was proposed that patients with compensated cirrhosis with LS <20 kPa (determined by TE) and a platelet count >150,000/mm3 were very unlikely to have high‐risk varices (<5%), and endoscopy could be safely avoided in them.
Given the interplay between underlying cirrhosis and systemic therapy-related toxicities, future investigations should focus on comprehensive risk assessments to better delineate the relative contributions of cirrhosis-related portal hypertension versus anti-angiogenic treatment effects. As evidenced by the IMbrave 150 trial,4 the use of VEGF-receptor inhibitors carries an inherent bleeding risk, which raises important questions about optimal patient selection and monitoring, especially when eligibility criteria for clinical trials excludes patients with recent GI bleeds or require an EGD prior to enrollment, which may disqualify these high-risk patients at screening. Application of prophylactic beta blockade in lieu of EGD is not recommended based on these results of the study; however, it opens the question on whether there are other potential clinical evaluations or interventions that can be done for HCC patients prior to starting systemic therapy including anti-angiogenic therapy that increases risk of bleeding. In clinical practice, like the patients in this study, HCC patients present with more advanced liver disease as evident by Child-Pugh score, therefore the risks of bleeding may be inherently higher than in the clinical trial setting. Additional information such as tumor characteristics such as tumor diameter size and alpha-feto-protein would provide more clinical context on the disease spectrum on this patient population. Moreover, the evidence of multi-kinase inhibitors targeting the VEGF receptor such as lenvatinib, sorafenib, regorafenib, and cabozantinib, causing bleeding has been established, but there are differences among tumor types and comorbidities and additional factors that may contribute to bleeding, including potential use of anti-platelet and anticoagulants and dose of chemotherapy.6 A limitation in our study is that we did not include the timing of medication exposure of anti-platelet or anticoagulants. While our study did not find a significant difference in bleeding outcomes between the use of VEGF-inhibitors and multi-kinase inhibitors, larger, prospective studies are required to validate these findings and determine whether specific drug-related risks can be mitigated. Additionally, in our patient population, 11 patients experienced a GI bleed, 3 of whom were on anti-platelet and anticoagulants like direct thrombin inhibitors like apixaban. Due to the small sample size, it is unclear whether being on these therapies led to increased risk. However, a recent review found a significantly high risk of overall bleeding events for patients on concurrent VEGF TKIS and factor Xa inhibitors compared to VEGF TKIs alone (HR, 2.45; 95% CI, 1.28–4.69 [p=0.007]). Whether patients underwent EGD and received NSBBs is not known for the patient population in this review but should be investigated further and considered an important clinical factor in evaluating bleeding risk.7 Another critical area for further exploration is the development of individualized bleeding prevention strategies tailored to HCC patients. While beta-blockade has demonstrated efficacy in reducing variceal hemorrhage, the lack of clear superiority over EGD in our study suggests that a combination approach or alternative prophylactic measures should be investigated. Given that less than half of our cohort was on anticoagulation or anti-platelet medications, it is imperative to evaluate how concurrent medication use modifies bleeding risk and survival outcomes. However, there was not a notable increase of GI bleeding despite being on these therapies. Multicenter studies incorporating larger cohorts with diverse etiologies of cirrhosis and HCC are essential to assess the real-world applicability of various preventive strategies. Furthermore, refining predictive models for bleeding risks will be pivotal in guiding clinical decision-making.
Future research can leverage machine learning and advanced predictive modeling to incorporate dynamic factors such as liver function trends, biomarker profiles, and real-time non-invasive monitoring of portal hypertension metrics. The ultimate goal should be to establish a comprehensive approach to GI bleeding prevention, balancing the oncologic benefits of systemic therapy with minimized toxicity risks. In conclusion, while our study provides valuable insights into the risks of GI bleeding in HCC patients, further high-powered, longitudinal studies are required to elucidate the most effective risk mitigation strategies. Given the life-threatening implications of bleeding events in this population, a multidisciplinary approach integrating hepatology, oncology, and gastroenterology expertise will be essential in optimizing patient outcomes.
Conclusion
In patients with CPA, the performance of EGD prior to treatment did not impact bleeding outcomes. Similarly, no disparity in bleeding outcomes was noted between the use of VEGF-R and multi-kinase inhibitors. Subsequent studies are essential to validate the survival benefits of prophylactic EGD versus non-selective beta blockers being initiated prior to initiation of HCC systemic therapy.
Bleeding risk in HCC patients is a multifactorial issue influenced by underlying cirrhosis, portal hypertension, and the use of systemic therapies. While prophylactic strategies such as variceal screening and medical therapies such as NSBBs are recommended, further research is needed to optimize bleeding prevention and management in this high-risk population. Future studies should focus on comparative effectiveness of different prophylactic strategies, including beta-blockers versus endoscopic interventions, to guide clinical practice.
Ethics and Consent Statements
Approval for this research protocol (HSC-MS-22-0880) was obtained on November 3, 2022, by the Committee for the Protection of Human Subjects (CPHS) at the University of Texas Health Science Center at Houston (UTHealth). Based on the review of CPHS at UTHealth, waiver of consent was obtained due to study posing no more than minimal risk to subjects as information being record by investigators in such a manner that subjects cannot be identified, directly or through identifiers linked to the subjects and does not adversely impact subject’s rights and welfare. Our study complies with Declaration of Helsinki.
Disclosure
The authors report no conflicts of interest in this work.
References
1. D’Amico G, Pagliaro L, Bosch J. Pharmacological treatment of portal hypertension: an evidence based approach. Semin Liver Dis. 1999;19:475–10. doi:10.1055/s-2007-1007133
2. Villanueva C, Albillos A, Genescà J, et al. β blockers to prevent decompensation of cirrhosis in patients with clinically significant portal hypertension (PREDESCI): a randomised, double-blind, placebo-controlled, multicentre trial [published correction appears in Lancet. 2019 Jun 22;393(10190):2492. doi: 10.1016/S0140-6736(19)31404-7]. Lancet. 2019;393(10181):1597–1608. doi:10.1016/S0140-6736(18)31875-0
3. Garcia-Tsao G, Abraldes JG, Berzigotti A, Bosch J. Portal hypertensive bleeding in cirrhosis: risk stratification, diagnosis, and management: 2016 practice guidance by the American Association for the study of liver diseases. Hepatology. 2017;65:310–335. doi:10.1002/hep.28906
4. Finn RS, Qin S, Ikeda M, et al. Atezolizumab plus bevacizumab in unresectable hepatocellular carcinoma. N Engl J Med. 2020;382:1894–1905. doi:10.1056/NEJMoa1915745
5. Sangro B, Kudo M, Erinjeri JP, et al. Durvalumab with or without bevacizumab with transarterial chemoembolisation in hepatocellular carcinoma (EMERALD-1): a multiregional, randomised, double-blind, placebo-controlled, Phase 3 study. Lancet. 2025;405(10474):216–232. doi:10.1016/S0140-6736(24)02551-0
6. Das A, Mahaptra S, Bandyopadhyay D, et al. Bleeding with vascular endothelial growth factor tyrosine kinase inhibitor: a network meta-analysis. Crit Rev Oncol Hematol. 2021;157:103186. doi:10.1016/j.critrevonc.2020.103186
7. Patel SH, George TL, Wang TF, et al. Increased bleeding risk associated with concurrent vascular endothelial growth factor receptor tyrosine kinase inhibitors and low-molecular-weight heparin. Cancer. 2021;127:938–945. doi:10.1002/cncr.33337
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.