Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Evaluation of Patient Experience With A Model of Coordinated Telematic Pharmaceutical Care Between Hospital and Rural Pharmacies in Spain: A Proof of Concept
Authors Morillo-Verdugo R ![]() , Morillo-Lisa R
, Morillo-Lisa R ![]() , Espolita-Suarez J, Delgado-Sanchez O
, Espolita-Suarez J, Delgado-Sanchez O ![]()
Received 15 February 2023
Accepted for publication 30 March 2023
Published 14 April 2023 Volume 2023:16 Pages 1037—1046
DOI https://doi.org/10.2147/JMDH.S406636
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Ramón Morillo-Verdugo,1 Rosa Morillo-Lisa,2 Jaime Espolita-Suarez,3 Olga Delgado-Sanchez4
1Pharmacy Hospital Service, Hospital Valme, Área de Gestión Sanitaria Sur de Sevilla, Sociedad Española de Farmacia Hospitalaria, Sevilla, Spain; 2Rural Community Pharmacy, Sociedad Española de Farmacia Rural, Zaragoza, Spain; 3Rural Community Pharmacy, Sociedad Española de Farmacia Rural, León, Spain; 4Pharmacy Hospital Service, Hospital Son Spases, Sociedad Española de Farmacia Hospitalaria, Palma de Mallorca, Spain
Correspondence: Ramón Morillo-Verdugo, Pharmacy Hospital Service, Hospital Valme, Área de Gestión Sanitaria Sur de Sevilla, Sociedad Española de Farmacia Hospitalaria, Avda/Bellavista s/n, Sevilla, CP 41014, Spain, Tel +34 955015467, Email [email protected]
Purpose: To determine the usefulness of a coordinated pharmaceutical care model between the specialized hospital setting and the rural community care setting, based on the incorporation of telepharmacy based on Capacity-Motivation-Opportunity (CMO) methodology to improve patient experience with hospital medication prescriptions.
Patients and Methods: Prospective cohort study in outpatients receiving telepharmacy based on CMO-based pharmaceutical care in rural areas in Spain between January and November 2021, conducted by the pharmacy department of four hospitals and 29 rural communities’ pharmacy. Each patient was followed for 48 weeks on both face-to-face and telematic visits, scheduled and unscheduled at the patients’ request. Patient experience (IEXPAC questionnaire), and satisfaction (EVASAF) were determined. Secondary variables included pharmaceutical care interventions, care coordination and clinical variables (compliance with pharmacotherapeutic objectives according to the clinical conditions of each patient), additionally measurement of individual holistic results (EQ5D-5L score) was evaluated.
Results: A new telepharmacy tool (called Telemaco) was developed for a multidisciplinary healthcare team (available at: https://inteligeniapps.com/telemaco/) that includes seven different functionalities. We evaluated the first 20 patients (50% women) were included. Their median age was 66.0 years (IQR=14). A total of 215 visits were made (adding 150 video calls). A total of 64 visits were unscheduled (29.7%). The patient´s experience showed improvement (7.4 vs 9.5, p< 0.005). The results of the EVASAF questionnaire were also higher (44 vs 48, p< 0.001). Overall, 573 pharmaceutical interventions were performed. A difference was observed in patients who achieved the intended pharmacotherapeutic objectives: 48.5 vs 88.2 (p< 0.001). The mean EQ-5D-5L score was 74.7 ± 3.3 at baseline and 80.6 ± 3.6 points at the end (p> 0.05).
Conclusion: Telepharmacy based on the CMO-PC model, using the “Telemaco” tool, has improved the patient experience, satisfaction, and offered other advantages over the traditional model, including more pharmaceutical interventions adapted to the needs of each patient.
Keywords: telepharmacy, pharmaceutical care, patient satisfaction, outcome assessment
A Letter to the Editor has been published for this article.
A Response to Letter by Dr Kolomboy has been published for this article.
Introduction
Changes in society, the healthcare system, and the profile of patients seen in outpatient hospital pharmacy units have become increasingly relevant, both from the point of view of economic management and healthcare strategy.1 It is therefore essential to respond to their needs with the aim of assessing health outcomes and guaranteeing the sustainability of the system in an environment with incessant pressure on costs. From this perspective, plans and strategies are being developed in hospital outpatient care, in different countries at the institutional level, and from scientific societies at the healthcare level.2–5
In Spain, in 2015, the Spanish Society of Hospital Pharmacy (SEFH) began to develop the “Strategic Map for Outpatient Care-MAPEX” initiative, whose main objective was to open a line of work around improving outpatient care by the Specialist Pharmacist, always with the idea of strengthening its leadership in pharmacotherapeutic management and care coordination.6
In this sense, a new pharmaceutical care (PC) model was proposed that would develop a multidisciplinary and multidimensional approach and ensure that the needs of the patient were met. It was called Capacity-Motivation-Opportunity (CMO) according to the pillars it addresses.7
Different studies have been carried out in an attempt to determine the usefulness of the new model in routine practise in different types of patients.8–12 Thus, significant aspects of therapeutics success have been evaluated, such as patient activation, therapeutic adherence, and patient experience. The results showed that this methodology had benefits both from the perspective of patients and of healthcare professionals working together with the pharmacist.
The arrival of the SARS-COV-2 pandemic in 2020 has forced the immediate implementation of telepharmacy in all hospitals with magnificent results from a professional perspective. However, in most cases, this success has been achieved with the means and human and material resources already available at the time in each center or by making use of volunteers or solidarity funds from scientific societies. All this, moreover, with a focus on health emergencies and with an orientation centered, in most cases, on the logistical approach and the delivery of medication.13–15 Toward these objectives, the positioning and strategic framework of the telepharmacy society has been published for its expansion and development, including the four main areas of work on which to advance: pharmacotherapeutic monitoring, training and information, care coordination, and informed dispensing and delivery.16
Although telepharmacy has shown benefits, even at the most critical moments of the pandemic, it is necessary to establish initiatives that are not punctual, but structural, and extensive to the entire population so that they become a reference for care, particularly for populations with fewer resources and less access to the health system, such as patients in rural areas.17–19
Rural healthcare is the most affected, as it lacks sufficient staff, healthcare infrastructure, isolation rooms and communication tools. Patients in rural areas also do not have adequate access to the necessary healthcare services due to long travel times to healthcare facilities, communication difficulties or sometimes lack of digital skills of the users themselves.20,21
In this study, we applied telepharmacy to real-life outpatients treated in four centers throughout Spain to determine the usefulness of a coordinated PC model between the specialized hospital setting and the rural community care setting, based on the incorporation of telepharmacy based on CMO methodology to improve patient experience with hospital medication prescriptions.
Material and Methods
Technological Support Tool
For the development of the project, pharmacists from different levels of care, physicians, engineers, and computer scientists designed a computer application that considered the necessary functionalities to meet the needs of inter-level follow-up for each type of patient.
To this end, several joint work meetings and technical tests were carried out to verify the functioning of the established advances and their practical usefulness.
Once the tool was completed, all participants in the study received specific training in the tool and user manuals adapted to both patients and professionals.
All users received individual logins and passwords tailored to their specific profile.
Study Design and Participants
Experimental analytical before-after intervention study. The procedures carried out during the study were the usual in clinical practices, with the exception of those applied in the protocol based on the CMO methodology follow-up.
Patient recruitment was carried out in the hospital pharmacy services between January and November 2021 in four hospital pharmacy services in different parts of Spain, including patients who met the inclusion and exclusion criteria. The subjects included were 18 years of age or older. They had hospital medication prescribed for the treatment of any chronic pathology treated in the specialised care setting (treatments are prescribed by a specialist and dispensed by a hospital pharmacy). They had already been followed up in hospital pharmaceutical care for at least one year before the start of the study.
Patients who were unable to complete the necessary questionnaires during the study were excluded. Neither the patients nor the investigators were remunerated for their participation. The patients were required to sign an informed consent form.
Each patient was followed for 48 weeks in both face-to-face and telematic visits, scheduled and unscheduled at the patient’s request. The patients were evaluated and followed up until November 2022.
The study adhered to the International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use and the Declaration of Helsinki.22 The Ethics Committee of the Research Centre Comité de Ética de Investigación Sevilla Sur (#2629-N-20) approved the study protocol and any other information that needed preapproval.
Pharmaceutical Care Intervention
In summary, to carry out the proposed methodology, patients were first stratified into three priority levels according to their demographic, social, health, cognitive, functional, utilisation of clinical services and medications-related variables. Based on the outcome, each patient was then given a series of predetermined interventions, with more intensive follow-up the higher the patient’s level of complexity. These interventions were directed not only to patients but also to the rest of the professionals and included training and education, individualised follow-up of pharmacotherapy and coordination of members of the health team. For each priority level, a frequency of visits, both face-to-face and telematic, was established.
In addition, during each visit to the Hospital Pharmacy Service or rural pharmacy, a motivational interview was conducted with each patient. In each interview, pharmacotherapeutic objectives were established or re-evaluated in consensus with the rest of the medical team who attended the patient at that time. Lastly, all patients received permanent contact tools with study pharmacists to resolve any incident or doubt related to their treatment at any time during the study.23
Health Outcomes
Outcomes were measured at baseline and at the end (48 weeks) of the study.
The validated IEXPAC questionnaire was used to assess the evolution of the patient’s concept of experience.24 It was administered by technical support staff to avoid response bias.
This questionnaire consists of two parts. The first includes 11 items that are scored from 1 (never) to 5 (always) according to their frequency. The sum of the item scores ranges from 11 to 55 which is converted into an overall score between 0 and 10.24
Patient satisfaction with the PC received, both in the hospital and in the rural pharmacy) was measured using the EVASAF questionnaire, a survey completed by patients about the PC they received in the hospital, or Armando et al questionnaire for PC in rural pharmacy.25,26
Secondary variables included PC interventions (performed according to the available taxonomy),27 coordination of care (number of scheduled and unscheduled visits, both in hospital and rural pharmacies, as well as joint visits), clinical variables (compliance with pharmacotherapeutic objectives according to the clinical conditions of each patient), and measurement of individual holistic results (difference in the EQ5D-5L questionnaire score base vs 48 weeks).28
Statistical Analysis
The study reported frequencies and percentages to describe qualitative values according to the size of the population, while quantitative values were presented as the total number of patients (n), median and interquartile range (IQR) with percentile 75–25. As there was no established method to calculate the sample size in the literature, the researchers established the first year of follow-up after the initial recruitment period as the minimum requirement.
To assess the differences in the variables collected before and after the intervention categorical variables were compared using a two-sided likelihood ratio chi-square test or McNemar test, while continuous variables were analyzed with the Wilcoxon-Test, as appropriate. Significant differences were quantified with 95% confidence intervals. The threshold for statistical significance was defined as p<0.05.
Data analysis was carried out using IBM SPSS 25.0 statistical software (IBM Corp., Armonk, NY, USA).
Results
Finally, the tool developed was called Telemaco (available at: https://inteligeniapps.com/telemaco/) and had the following seven functionalities:
- History of the characterisation and prioritisation of pharmacotherapeutic patients.
- Schedule of scheduled visits and record of unscheduled visits.
- Record of PC visits and interventions performed.
- Generic communication wall between participants.
- Instant messaging chat between patients and professionals.
- Video calls.
- Monitoring of drug adherence and evaluation of PRO.
The tool had specific usage profiles for patients and pharmacists in hospitals and rural pharmacies.
Participant Characteristics
The baseline characteristics of the study population are described in Table 1. We evaluated the first 20 patients (10 men and 10 women) were included.
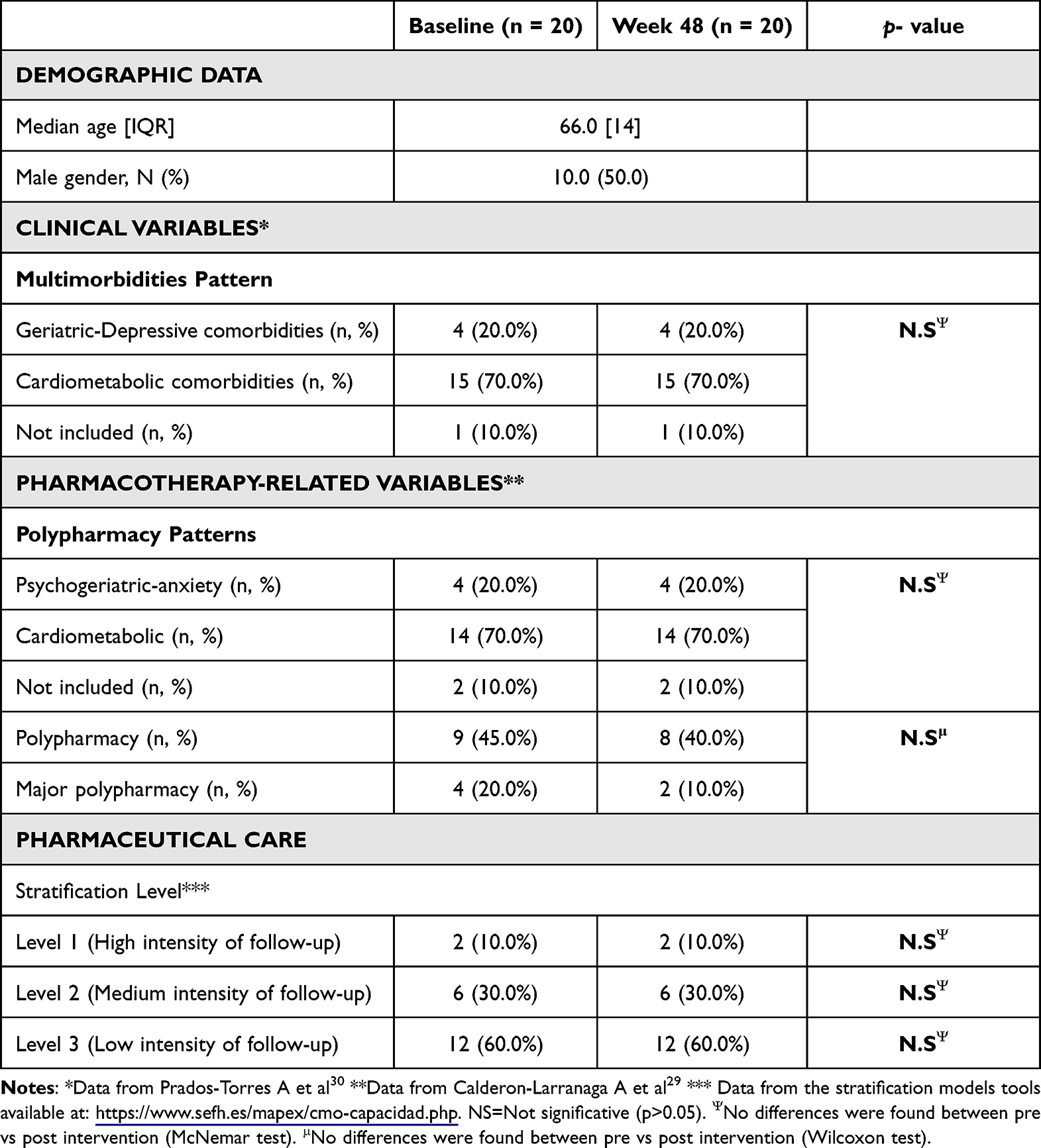 |
Table 1 Baseline Characteristics of Patients Included in the Study |
The participants had a median age of 66.0 years (IQR=14). The clinical characteristics and pharmacotherapeutic variables were also evaluated (Table 1). There were no significant differences in pharmacotherapeutic characteristics, according to Calderón-Larrañaga et al29 patterns, between baseline and 48 weeks, but the number of concomitant medications was higher at baseline (119 vs 114) due to a greater number of comorbidities (94), as described in Prados-Torres et al30 patterns. Throughout the study, no patients changed their stratification level.
Patient Experience
Based on the results of the IEXPAC questionnaire, an improvement in the experience of patients followed with the CMO based-methodology was observed. The mean score of the questionnaire was 9.50 at week 48, compared to 7.47 at baseline (p<0.005) (Figure 1).
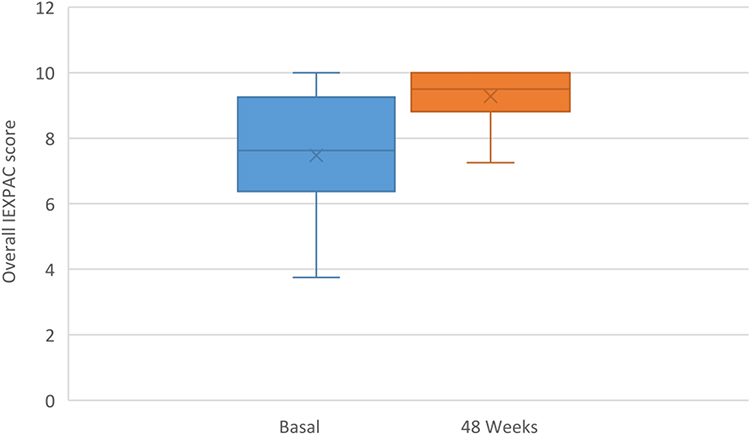 |
Figure 1 Evaluation of patient experience using the IEXPAC questionnaire. |
Patient Satisfaction
According to the EVASAF questionnaire, the score obtained in the cohort was significantly higher at week 48 than at the beginning (48 ± 1.1 vs 44 ± 1.3, p<0.001). Knowledge about medications and their possible interactions and adverse effects showed the most noticeable differences.
The mean EQ-5D-5L score was 74.7 ± 3.3 points at baseline and 80.6 ± 3.6 points at the end of the follow-up period, without significant difference (p>0.05).
Pharmaceutical Care Interventions
Throughout the study, 573 pharmacological interventions were performed, 91 at the initial visit, 312 up to week 24 and 170 up to week 48. This indicates an average of more than 28 interventions per patient during the follow-up period.
The most frequent interventions were review and validation of medications, review of objectives in relation to pharmacotherapy, follow-up planning, and motivation (Figure 2).
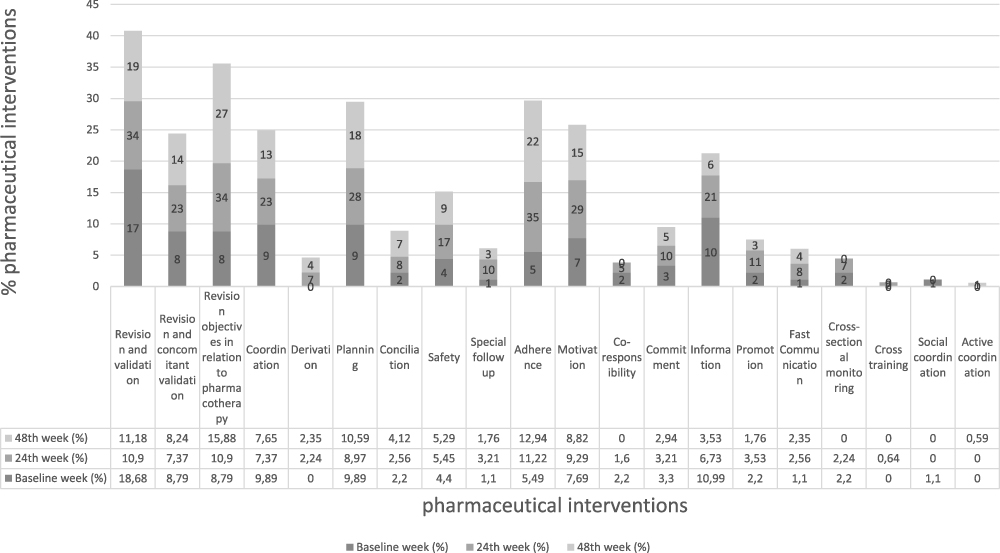 |
Figure 2 Percentage and type of pharmaceutical interventions carried out during the study. |
Significant differences were found in the percentage of patients who met the pharmacotherapeutic objectives planned by the health team for each of the prescribed treatments at the end of follow-up: 48. 5 ± 3.0 vs 88.2 ± 1.3 (p< 0.001).
Care Coordination
A total of 215 visits were carried out throughout the study, 33 in the hospital, 70 in the community pharmacy, and 112 jointly. Additionally, 150 follow-up video calls were established for the patients followed throughout the study. A total of 64 visits were not scheduled (29.7%).
Discussion
In this study, we prospectively compared the influence of the development and application of a coordinated PC model between hospital and community pharmacy in rural areas, applying a technological tool specifically designed for monitoring through telepharmacy and applying the CMO PC methodology in outpatients from four different centres across Spain and 29 community pharmacies. The proposed PC model proposes a refocusing of pharmacists from being experts in the drug to experts in the patient’s relationship with their pharmacotherapy. In this sense, the multidimensional approach to the patient is fundamental to achieve better therapeutic results. We found that this methodology improves patient experience and satisfaction compared to the traditional model. The number of interventions performed and the number of face-to-face and telematic visits carried out demonstrate the usefulness and ease of implementation in routine practise.
In recent years, with the advent of the humanization of care and shared decision making, it is essential to measure the patient experience, the interaction of users with healthcare professionals on a day-to-day basis, and the quality of care. This aspect has already been specifically assessed in this model using validated tools such as IEXPAC. However, until now, it had not been evaluated with the incorporation of an accompanying telematic tool, such as the one developed in this project. In our study, the outpatient experience using telepharmacy and based on the CMO approach PC improved significantly after 48 weeks of follow-up, in contrast to the previous long-traditional PC. In addition, patient satisfaction, a more classic aspect, which measures the protocolization of professional actions, also improved significantly in the rural cohort.
Previous research indicates that the implementation of telepharmacy in rural areas does not result in a lower quality of drug use compared to traditional pharmacies. These findings suggest that telepharmacies can serve as a viable solution for expanding drug access, without compromising the quality of grug use, and may be beneficial for communities considering the adoption of telepharmacy.31,32
Additionally, Inch et al conducted a study in Scotland and found that delivering community pharmacy services through teletechnology was both feasible and acceptable.33
Other studies carried out in the same time frame as ours have used tools that do not ensure confidentiality or the integration of the data in the patients’ medical record systems, a fundamental aspect for compliance with data protection laws in an environment as novel and transcendent as that of new technologies.20,21,34 In our case, the tool has been designed to comply with both aspects.
Despite including telepharmacy as a key element in the development of these PC initiatives, none of them has combined, as in our case, a tool specifically developed for this element and a patient-centred PC model based on a multidimensional approach to patients.
In our study, outpatient satisfaction was measured using the EVASAF questionnaire, a validated questionnaire specifically designed to determine pharmaceutical care in outpatient pharmacy consultations. This survey was included as a result of pharmacists’ awareness of the impact of their work on patient outcomes and therapeutic optimisation, based on the multidisciplinary interventions carried out, including in interlevel care. Our results corroborated that the coordinated, patient-centred model is superior to traditional care and improves this problem.35 However, obviously, given the characteristics of the population analysed, this result should be considered with caution, as some variables may have a confounding influence.
Another important concern in outpatients is adherence to treatment, a variable negatively impacted by the therapeutic complexity resulting from chronic comorbidities. A future line of follow-up for this care strategy will include a specific analysis of this factor, both for inpatient and community medications, analysing the most determinant elements. The indirect results based on the percentage of patients who meet their goals in relation to pharmacotherapy make us optimistic about the impact of this approach on this important item.
Our study had some limitations. First, participation and the number of patients were small and heterogeneity was present at the beginning of the study because the developed tool is new and the PC model was not yet implemented in most of the hospitals participating in the study. A larger number of patients or a follow-up of more than 48 weeks to allow the patient more time to test the impact and differences between the traditional and the new PC model supported by new technologies could shed some light on the difference in mean value between the traditional and the new format. In fact, longer study periods will be necessary to determine whether the effects observed after telecare follow-up and interventions by the CMO pharmacist are sustained over time. Lastly, the study only recruited patients from four hospital pharmacy services in different parts of Spain, which limits the generalizability of the findings to other settings and populations. Despite these limitations, this is the first study we are aware of that determines the impact of patient-centered PC with that of traditional follow-up based on face-to-face care and little interlevel coordination. Given the ease of application of both the telepharmacy tool and the PC methodology and its interventions, future research in other countries could validate this model in different health systems.
Finally, to demonstrate the potential benefits of the implementation of telepharmacy, it will be necessary to support innovation and research projects with novel designs that are at the same time robust, multicenter, multidisciplinary, and even international, and not only in rural areas. To achieve this ambitious goal, leadership and institutional support from various scientific societies and healthcare entities will be necessary. To this end, in Spain, a methodological support document strategy has been developed for its homogeneous expansion, including, among others, an implementation guide, a model for prioritising candidate patients, and, of course, indicators to monitor its progress.36–39
Conclusion
In conclusion, telepharmacy based on the CMO-PC model, using the new technological tools called “Telemaco”, has improved the patient experience, increased patient satisfaction, and offered other advantages over the traditional model, including more pharmaceutical interventions adapted to the needs of each patient. Extension of the cohort in number and follow-up time could confirm whether this methodology could be considered as the gold standard in double PC of patients in the near future.
Acknowledgments
To all participant in the project:
Alicia Lazaro Lopez, Maria Blanco Crespo, Ana Maria Horta Fernandez (Hospital de Guadalajara), Luis Ortega Valín (Complejo Hospitalario de León), Jose Sebastian Roldan Gonzalez, Jose Jimenez Casaus, Sonia Fernandez Cañabate (Complejo Hospitalario de Zamora), Transito Salvador Gomez, Mercedes Gimeno Gracia, Lucia Sopena Carrera, Raquel Fresquet, Arantxa Magallón (Hospital Lozano Blesa, Zaragoza).
M Pilar Fabian Sanz, Azucena Ojeda Saez, Francisco Aceituno Romero, Raquel Avila Torvisco, Lucila Menendez Bueno, Bernardina Moro Mediano, Mª Lourdes Sanchez-Seco Fraile, Isabel Calvo Ruiz, Amor Lopez Gonzalez, Clara Eugenia Navarro Castro, Nuria Muñoz Muñoz, Elena Amaro Lopez, Patricia Redondo Lajas, Begoña Gonzalez Paramino, Ana Belen Prieto Nieto, Cristina Lobato Valencia, Alvaro Perez Asensio, Ana de Paula Blanco, Isabel Garcia Garcia, Patricia Molina Lomba, Enrique Eguizabal Martinez, Antonio Ramos, Juan Jimenez, Andrea Martinez Seguer, Ana Maria Azagra Saez, Mª Pilar Baras Bandrés (Oficinas de Farmacia, Sociedad Española de Farmacia Rural)
Alvaro Serrano, Ricardo Serrano y Daniel Ruiz (4Clavis Consulting S.L).
Enrique Contreras Macias for his support at statistical level.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. WHO library. Telemedicine. opportunities and developments in members states. Ginebra (Suiza); 2010. Available from: www.who.int/goe/publications/goe_telemedicine_2010.pdf.
2. European Patients Forum. Carta sobre el Empoderamiento de los Pacientes. Luxemburgo; 2020. Avialable from: https://www.eu-patient.eu/globalassets/campaign-patient-empowerment/charter/charter_es-final.pdf.
3. Alexander E, Butler CD, Darr A, et al. ASHP Statement on Telepharmacy. Am J Health Syst Pharm. 2017;74(9):236–241. doi:10.2146/ajhp170039
4. US National Association of Boards of Pharmacy. Telepharmacy: the new frontier of patient care and professional practice. Mount Prospect (Illinois, EEUU); 2017. Available from: https://nabp.pharmacy/wpontent/uploads/2016/07/Innovations_June_July_Final.pdf.
5. Canadian Society of Hospital Pharmacist. Telepharmacy guidelines. Ottawa (Canadá); 2017. Avialable from: https://www.cshp.ca/sites/default/files/files/publications/Official%20Publications/Telepharmacy%20Guidelines_2018.pdf.
6. Sociedad Española de Farmacia Hospitalaria [Spanish Society of Hospital Pharmacy]. Proyecto Mapex: marco Estratégico de Telefarmacia [MAPEX Project. Strategic Framework in Telepharmacy]. Madrid; 2020. Available from: https://www.sefh.es/mapex/index.php/documentacion.
7. Morillo-Verdugo R, Calleja-Hernandez MA, Robustillo-Cortes MLA. A new pharmaceutical care concept: more capable, motivated, and timely. Hosp Pharm. 2019;54:348–350. doi:10.1177/0018578719867657
8. Cantillana-Suárez MG, Robustillo-Cortés MLA, Gutiérrez-Pizarraya A, Morillo-Verdugo R. Impact and acceptance of pharmacist-led interventions during HIV care in a third-level hospital in Spain using the capacity-motivation-opportunity pharmaceutical care model: the IRAFE study. Eur J Hosp Pharm. 2021;28:e157–e163. doi:10.1136/ejhpharm-2020-002330
9. Guzmán Ramos MI, Manzano Garcia M, Robustillo-Cortés MA, Gutiérrez Pizarraya A, Morillo-Verdugo R. Influence of CMO pharmaceutical care model-based intervention on readmission rate in high risk HIV patients: the INFARDAR study. Rev Esp Quimioter. 2021;34:459–467. doi:10.37201/req/025.2021
10. Caso-González A, Núñez-Rodríguez J, González-Pérez Y, Leralta-González C, Sanz-Alonso V, Obaldia-Alaña C. Eficacia de una intervención farmacéutica basada en el modelo CMO sobre la adherencia a fármacos biológicos y la experiencia del paciente con enfermedad reumática (Estudio ADhER-2). [Effectiveness on adherence to biological drugs and experience of a pharmaceutical intervention based on CMO model in patients with rheumatic disease (AdhER-2 study)]. An Sist Sanit Navar. 2022;45(2):e1004. Spanish. doi:10.23938/ASSN.1004
11. Morillo-Verdugo R, Vélez-Díaz-Pallarés M, Fernández-Pacheco García-Valdecasas M, Fernández-Espínola S, Sánchez-Rubio Ferrández J, Navarro-Ruiz A. Application of the CMO methodology to the improvement of primary adherence to concomitant medication in people living with-HIV. The PRICMO Project. Farm Hosp. 2021;45:247–252.
12. Morillo-Verdugo R, Robustillo-Cortés MA, Manzano García M, Almeida-González CV. Influence of pharmacist intervention, based on CMO model, to improve activation in HIV patients. Rev Esp Quimioter. 2019;32:40–49. doi:10.1056/NEJM199803263381301
13. Ibrahim OM, Ibrahim RM, Al Meslamani Z, Al Mazrouei N. Role of telepharmacy in pharmacist counselling to coronavirus disease 2019 patients and medication dispensing errors. J Telemed Telecare. 2023;29(1):18–27. doi:10.1177/1357633X20964347
14. Dat TV, Tu VL, Quan NK, et al. Telepharmacy: a systematic review of field application, benefits, limitations, and applicability during the COVID-19 pandemic. Telemed J E Health. 2022;29:209–221. doi:10.1089/tmj.2021.0575
15. Jirjees F, Odeh M, Aloum L, Kharaba Z, Alzoubi KH, Al-Obaidi HJ. The rise of telepharmacy services during the COVID-19 pandemic: a comprehensive assessment of services in the United Arab Emirates. Pharm Pract. 2022;20(2):2634. doi:10.18549/PharmPract.2022.2.2634
16. Morillo-Verdugo R, Margusino-Framiñán L, Monte-Boquet E, et al. Spanish society of hospital pharmacy position statement on telepharmacy: recommendations for its implementation and development. Farm Hosp. 2020;44(4):174–181. English. doi:10.7399/fh.11515
17. Le T, Toscani M, Colaizzi J. Telepharmacy: a new paradigm for our profession. J Pharm Pract. 2020;33(2):176–182. doi:10.1177/0897190018791060
18. Baldoni S, Amenta F, Ricci G. Telepharmacy services: present status and future perspectives: a review. Medicina. 2019;55(7):327. doi:10.3390/medicina55070327
19. Mohamed Ibrahim O, Ibrahim RM, Abdel-Qader DH, Al Meslamani AZ, Al Mazrouei N. Evaluation of Telepharmacy Services in Light of COVID-19. Telemed J E Health. 2021;27(6):649–656. doi:10.1089/tmj.2020.0283
20. Al Meslamani AZ, Kassem AB, El-Bassiouny NA, Ibrahim OM. An emergency plan for management of COVID-19 patients in rural areas. Int J Clin Pract. 2021;75(10):e14563. doi:10.1111/ijcp.14563
21. Al Mazrouei N, Ibrahim RM, Al Meslamani AZ, Abdel-Qader DH, Mohamed Ibrahim O. Virtual pharmacist interventions onabuse of over-the-counter medications during COVID-19 versus traditional pharmacist interventions. J Am Pharm Assoc. 2021;61(3):331–339. doi:10.1016/j.japh.2021.02.003
22. Association WM. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310:2191–2194. doi:10.1001/jama.2013.281053
23. Morillo-Verdugo R, Calleja-Hernández MÁ, Robustillo-Cortés MLA, Poveda-Andrés JL. A new definition and refocus of pharmaceutical care: the Barbate document. Farm Hosp. 2020;44(4):158–162. English. doi:10.7399/fh.11389
24. Mira JJ, Nuño-Solinís R, Guilabert-Mora M, et al. Development and validation of an instrument for assessing patient experience of chronic illness care. Int J Integr Care. 2016;16:13. doi:10.5334/ijic.2443
25. Monje-Agudo P, Borrego-Izquierdo Y, Robustillo-Cortés Mde L, Jiménez-Galán R, Almeida-González CV, Morillo-Verdugo RA. Diseño y validación de una encuesta de satisfacción con la atención farmacéutica recibida en las consultas de farmacia hospitalaria. [Design and validation of a satisfaction survey with pharmaceutical care received in hospital pharmacy consultation]. Farm Hosp. 2015;39:152–156. Spanish. doi:10.7399/fh.2015.39.3.8366
26. Carle PD, Uema SA, Pérez SR, Pallarés MM, Uthurry NH, Dáder MJ. Validación de un cuestionario de satisfacción de pacientes con el servicio de dispensación en farmacias comunitarias [Validation of a questionnaire on patient satisfaction with the dispensing service in community pharmacies]. Aten Primaria. 2007;39(11):591–596. Spanish. doi:10.1157/13112195
27. Morillo Verdugo R, Villarreal Arevalo AL, Alvarez DSM, Robustillo Cortes ML. Development of a taxonomy for pharmaceutical interventions in HIV+ patients based on the CMO model. Farm Hosp. 2016;40(n06):544–568. English. doi:10.7399/fh.2016.40.6.10567
28. D Crosswalk Index Value Calculator. Available from https://euroqol.org/eq-5d-instruments/eq-5d-5l-about/valuation-standard-value-sets/crosswalk-index-value-calculator/.
29. Calderon-Larranaga A, Gimeno-Feliu LA, Gonzalez-Rubio F. Polypharmacy patterns: unravelling systematic associations between prescribed medications. PLoS One. 2013;8(12):e84967. doi:10.1371/journal.pone.0084967
30. Prados-Torres A, Poblador-Plou B, Calderón-Larrañaga A, et al. Multimorbidity patterns in primary care: interactions among chronic diseases using factor analysis. PLoS One. 2012;7:e32190. doi:10.1371/journal.pone.0032190
31. Allan J, Webster E, Chambers B, Nott S. This is streets ahead of what we used to do”: staff perceptions of virtual clinical pharmacy services in rural and remote Australian hospitals. BMC Health Serv Res. 2021;21(1):1306. doi:10.1186/s12913-021-07328-w
32. Pathak S, Haynes M, Qato DM, Urick BY. Telepharmacy and quality of medication use in rural areas, 2013–2019. Prev Chronic Dis. 2020;17:E101. doi:10.5888/pcd17.200012
33. Inch J, Notman F, Watson M, et al., Telepharmacy Research Team. Tele-pharmacy in rural Scotland: a proof of concept study. Int J Pharm Pract. 2017;25(3):210–219. doi:10.1111/ijpp.12376
34. Al Meslamani AZ, Aldulaymi R, El Sharu H, Alwarawrah Z, Ibrahim OM, Al Mazrouei N. The patterns and determinants of telemedicine use during the COVID-19 crisis: a nationwide study. J Am Pharm Assoc. 2022;62(6):1778–1785. doi:10.1016/j.japh.2022.05.020
35. Morillo-Verdugo R, Lazaro-Lopez A, Alonso-Grandes E, et al. Patient experience evaluation of the CMO-based pharmaceutical care model vs usual care in people living with HIV. J Multidiscip Healthc. 2022;15:2991–3003. doi:10.2147/JMDH.S392398
36. Morillo-Verdugo R, Collado-Borell R, Arrondo-Velasco A, et al. Implementation of pharmaceutical care through Telepharmacy: a guide for professionals and patients. Farm Hosp. 2022;46(7):115–122.
37. Sanmartín-Fenollera P, Mangues-Bafalluy I, Talens-Bolos A, et al. Telepharmacy scorecard: activity and quality indicators for the pharmaceutical care in a hospital pharmacy service. Farm Hosp. 2022;46(7):92–105.
38. Monte-Boquet E, Hermenegildo-Caudevilla M, Vicente-Escrig E, et al. The telepharmacy patient prioritisation model of the Spanish Society of Hospital Pharmacy. Farm Hosp. 2022;46(7):106–114.
39. Morillo-Verdugo R, Robustillo-Cortes MLA, Navarro-Ruiz A, et al. Clinical impact of the capacity-motivation-opportunity pharmacist-led intervention in people living with HIV in Spain, 2019–2020. J Multidiscip Healthc. 2022;15:1203–1211. doi:10.2147/jmdh.S361305
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.