")
Back to Journals » International Journal of General Medicine » Volume 16
Evaluation of Clinical Indications of Three Treatments for Choledocholithiasis with Acute Cholangitis
Authors Chen L , Wu Z, Guo C, Wang G, Tu K, Jiang J
Received 10 July 2023
Accepted for publication 11 October 2023
Published 16 October 2023 Volume 2023:16 Pages 4669—4680
DOI https://doi.org/10.2147/IJGM.S429781
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Ling Chen,1 Zujian Wu,1 Chi Guo,1 Guoping Wang,1 Kui Tu,2 Jichang Jiang2
1General Surgery, Tongde Hospital of Zhejiang Province, Hangzhou, Zhejiang Province, 310012, People’s Republic of China; 2General Surgery, Affiliated Hospital of Zunyi Medical University, Zunyi, Guizhou Province, 563000, People’s Republic of China
Correspondence: Jichang Jiang, Email [email protected]
Objective: This study aimed to assess the efficacy of Endoscopic Retrograde Cholangiopancreatography (ERCP), common bile duct exploration, and percutaneous transhepatic cholangiography combined with common bile duct exploration for treating choledocholithiasis with acute cholangitis, to guide management strategies.
Methods: A retrospective evaluation was conducted on a cohort of 283 inpatients diagnosed with choledocholithiasis and acute cholangitis at the affiliated hospital. Patients were categorized into three groups: Group A (ERCP group), Group B(common bile duct exploration group), and Group C(PTCD combine common bile duct exploration group.) Parameters such as hepatic function recovery, inflammation level control, blood loss, postoperative hospital duration, and postoperative complications were compared.
Results: All groups exhibited notable reductions in postoperative biochemical parameters including alanine aminotransferase (ALT), aspartate aminotransferase (AST), gamma-glutamyl transferase (GGT), total bilirubin (TBIL), and WBC (P < 0.05). Group A had the least blood loss(P < 0.05), and shortest hospital stay(P < 0.05), but a higher incidence of pancreatitis(P < 0.05), with a total of 8 cases occurred(7.3%). Group C had a shorter hospital stay compared to Group B(P < 0.05).
Conclusion: For patients with fewer and smaller common bile duct stones and milder symptoms, it is recommended to primarily choose endoscopic retrograde cholangiopancreatography (ERCP), endoscopic sphincterotomy (EST), and endoscopic nasobiliary drainage (ENBD), it procedures offer quicker recovery and cause minimal trauma. For patients with numerous, larger common bile duct stones but stable conditions, bile duct exploration is recommended. For those with severe conditions and significant inflammation, PTCD and common bile duct exploration are advised.
Keywords: choledocholithiasis, acute cholangitis, ERCP, PTCD
Introduction
Choledocholithiasis, the most prevalent benign biliary obstruction disease in the biliary system, is particularly widespread in Asian regions such as China, Japan, and Korea, China exhibits a notably high prevalence of this condition. Although there is no precise incidence data available regarding gallbladder stones in China, the literature suggests a prevalence of approximately 9.2% in males and 16.1% in females, with an increasing occurrence of about 30% in older age groups. Among these patients, approximately 10–20% present with concurrent choledocholithiasis.1 Cholangitis represents a common complications of choledocholithiasis, with acute cholangitis being the primary manifestation in the majority of patients. Some individuals may initially present with acute obstructive purulent cholangitis at the time of medical consultation. It is worth noting that acute cholangitis is a significant cause of mortality in benign biliary diseases due to its propensity for infectious shock, rapid progression, and high mortality rate.2
Choledocholithiasis accompanied by acute cholangitis represents a common clinical emergency in hepatobiliary surgery, typically necessitating surgical intervention,3,4 The primary objectives of surgical treatment are lesion removal, alleviation of biliary obstruction, and establishment of effective drainage.5 In the past, open common bile duct exploration combined with T-tube drainage was the prevailing surgical approach. It was widely employed in clinical practice due to its relative simplicity and high success rates. However, this approach is associated with drawbacks such as significant trauma, slow postoperative recovery, prolonged hospital stays, and a higher incidence of postoperative complications. With the development of laparoscopic techniques, the treatment of choledocholithiasis with acute cholangitis has been improved. Since the late 20th century, the rapid integration of laparoscopic technology into hepatobiliary surgery has established laparoscopic common bile duct exploration with T-tube drainage as a novel surgical modality. This offers advantages such as reduced trauma, smaller incision, less bleeding, less interference with organ function, less patient suffering, less wound pain, faster return to normal activities, and fewer postoperative complications. Nonetheless, patients still endure prolonged T-tubes placement, which adversely affects their quality of life. In cases of combined acute cholangitis, laparoscopic surgery is relatively complex when employed as an emergency intervention, leading to extended operative time and increased postoperative complications. Over the years, significant progress has been made in the treatment of choledocholithiasis with acute cholangitis, thanks to the development and application of endoscopic and interventional techniques. Since the first performance of endoscopic retrograde cholangiopancreatography (ERCP) in 1968, followed by the introduction of endoscopic sphincterotomy (EST) in 1974 and endoscopic nasobiliary drainage (ENBD) in 1979, ERCP has emerged as the most commonly employed endoscopic technique. In addition to its diagnostic capabilities, ERCP can also facilitate biliary drainage and, in some cases, even achieve curative outcomes in patients with choledocholithiasis.6 However, it necessitates a high level of technical proficiency. The most commonly used interventional technique in hepatobiliary surgery is percutaneous trans-hepatic cholangiography drainage (PTCD), which has been increasingly used in hepatobiliary surgery since 1981 when PTCD was first reported in Zhongshan Hospital in Shanghai. PTCD is considered safe, straightforward, and effective in drainage, particularly suitable for middle-aged and elderly patients with multiple comorbidities who may not tolerate surgical interventions.7,8 Nevertheless, PTCD only ensures patency and drainage without providing a curative effect. These minimally invasive operations create the conditions for elective surgery in patients with acute cholangitis, especially in critically ill individuals, allowing physicians and patients additional time to develop a more suitable treatment plan.
This study aimed to retrospectively gather clinical data from patients admitted to the Department of Hepatobiliary Surgery of the Affiliated Hospital of Zunyi Medical University between January 2010 and December 2018. The objective was to investigate the advantages, disadvantages, and applicability of three treatment modalities, namely endoscopic retrograde cholangiopancreatography (ERCP) with endoscopic sphincterotomy (EST) and endoscopic nasobiliary drainage (ENBD), common bile duct exploration, and percutaneous transhepatic cholangiography drainage (PTCD) combined with common bile duct intervention. By comparing the therapeutic effects of these approaches on choledocholithiasis with acute cholangitis, we aim to provide valuable insights for future clinical management of this disease.
Materials and Methods
Inclusion Criteria
(1) All patients were ≥18 years old; (2) All patients had a preoperative diagnosis of choledocholithiasis by B ultrasound, CT, or MRI; (3) Patients exhibited at least two symptoms from the Charcot triad, including abdominal pain, chills and fever, and jaundice; (4) Complete clinical data were available for analysis.
Exclusion Criteria
(1) Patients with a previous history of upper abdominal surgery or disease that may cause severe abdominal adhesions; (2) Patients who combined with intrahepatic bile duct stones; (3) Patients who combined with biliary tract tumors.
Study Objects and Grouping
For this retrospective study, we collected data from 342 patients diagnosed with choledocholithiasis and acute cholangitis who were admitted to our hospital between January 2010 and December 2018. The study protocol was accepted by the ethical committee of the Affiliated Hospital of Zunyi Medical University (approval number: KLL-2023-507), this study was done according to the principals of the Declaration of Helsinki, all patients submitted written informed consent prior to the research. We declare that patient information will be kept confidential.283 patients were eligible according to the inclusion and exclusion criteria and were divided into three groups according to the different treatment modalities after admission: Group A was ERCP group (110 patients), of which 42 were male and 68 were female, with an average age of (50.41±15.28) years and 41 with medical comorbidities; Group B was common bile duct exploration group (90 patients), of which 40 were male and 50 were female, with an average age of (53.41±15.37) years, 36 combined with the medical disease, 34 with open surgery and 56 with lumpectomy, 1 postoperative death; Group C was PTCD + common bile duct exploration group (83 patients), of which 38 were male and 45 were female, with an average age of (52.87±13.96) years, 35 combined with medical diseases, 33 cases had open surgery and 50 cases had a lumpectomy.
Diagnostic Criteria for Postoperative Acute Pancreatitis
(1) Onset of new abdominal pain or exacerbation of pre-existing abdominal pain subsequent to endoscopic retrograde cholangiopancreatography (ERCP); (2) Serum amylase exceeding 3 times the upper limit of normal within 24 hours after surgery.
Surgical Methods
(1) Group A: All 110 patients underwent ERCP+EST+ENBD successfully in our endoscopy center. These patients were positioned either in a prone or left lateral posture, and a meticulously maneuvered electronic duodenoscope (model: TJF-260) was inserted via the oral cavity to reach the descending duodenum, where the papilla was identified in the middle section. Subsequently, a contrast catheter was inserted into the papilla to guide the placement of a guidewire into the bile duct, enabling the injection of contrast material through a contrast tube inserted into the common bile duct. This facilitated the visualization and assessment of stone location, quantity, and dimensions. An endoscopic sphincterotomy of the Oddi’s sphincter was then performed, employing a stone extraction basket and balloon to successfully remove and expel the stones into the intestine. Following stone removal, imaging was conducted once more by smoothly advancing a nasobiliary duct alongside the guidewire and securing it in place, allowing for observation of any signs of active bleeding in the papilla.
(2) Group B: All 90 patients underwent successful common bile duct exploration + T-tube drainage in the Department of Hepatobiliary Surgery of our hospital. These patients were positioned in a supine position and underwent standard disinfection and toweling procedures following the administration of general anesthesia. Subsequently, the abdominal cavity was accessed, and meticulous dissection was performed to separate the surrounding tissues from the gallbladder adhesions. The triangular structure of the gallbladder was identified, along with the anatomical relationship between the cystic duct, common hepatic duct, and common bile duct. A longitudinal incision was made in the anterior wall of the common bile duct, allowing for the aspiration of bile. The palpable common bile duct stones were removed using stone forceps, followed by the use of a choledochoscope to explore the bile ducts and identify the presence of stones within them. Stone forceps or a mesh basket were utilized to remove the stones, ensuring that the bile ducts were free from any obstruction. Additionally, a thorough examination of the bile ducts was conducted to identify bile duct strictures, malignant tissue, and any abnormalities in the duodenal papillae. Subsequently, a re-examined of the bile duct was performed to confirm the absence of remaining stones, and a T-tube was inserted based on the condition of the common bile duct. The common bile duct was closed with interrupted sutures and secured with silk. The abdominal cavity was rinsed and inspected for any signs of bleeding or bile leakage, and an abdominal drain was placed. Finally, the abdomen was closed.
(3) Group C: Group C consisted of 83 patients who initially underwent successful percutaneous transhepatic cholangiodrainage (PTCD) in our interventional department, followed by elective common bile duct exploration and T-tube drainage in our hepatobiliary surgery department. During the procedure, the patient was lying on a DSA bed, with the puncture site being located by ultrasound and fluoroscopy. After routine disinfection and the effective local anesthesia of 2% lidocaine 5 mL, the biliary puncture kit was used to penetrate the intrahepatic bile ducts, followed by pushing the contrast agent, exchanging the guidewire into a puncture sheath, and inserting the catheter for cholangiography to observe whether the right and left intrahepatic bile ducts were connected and the degree of bile duct dilatation. Upon completion of the imaging, the catheter was replaced with a guidewire, and a specialized external drainage tube was carefully guided along the guidewire to verify the patency of the drainage tube. Finally, a local bandage was applied and the drainage tube was secured. Once the patient’s general condition improved, common bile duct exploration and T-tube drainage were performed again.
Evaluation Indexes
Statistical Methods
SPSS 22.0 software was used for data analysis. Normality tests were conducted to analyze numerical variables, and mean ±SD were used to represent normally distributed numerical data. The ANOVA was used for comparison between groups, and the q-test was used for further comparison between the two groups when differences were observed. Paired t-test was utilized to compare preoperative and postoperative measurements within the same group. M (P25, P75) notation was used for non-normally distributed data, and the rank sum test was employed for comparisons among multiple groups. Categorical variables were expressed as frequencies, and statistical significance was determined using the chi-square test or Fisher’s exact probability method, with a significance level set at P<0.05. For two comparisons following chi-square splitting among three groups, a significance level of P<0.016 was considered statistically significant.
Results
Preoperative General Condition of Patients
A total of 283 patients diagnosed with choledocholithiasis and acute cholangitis were enrolled in this study. These patients were divided into three groups: Group A (ERCP group) consisting of 110 patients, Group B (common bile duct exploration group) consisting of 90 patients, and Group C (PTCD + common bile duct exploration group) consisting of 83 patients. Statistical analysis revealed no significant differences in terms of age, sex, common bile duct diameter, presence of gallstone, presence of comorbidities (such as hypertension, coronary heart disease, diabetes mellitus, hyperlipidemia), performance of open surgery, or emergency surgery (P > 0.05). However, there were significant differences observed in the number of stones and stone diameter among the three groups (P = 0.032, P = 0.042) (refer to Table 1). Moreover, there were no statistical differences in the preoperative levels of serum ALT, AST, GGT, TBIL, WBC, and N% among t the three groups (P > 0.05) (refer to Tables 2–4).
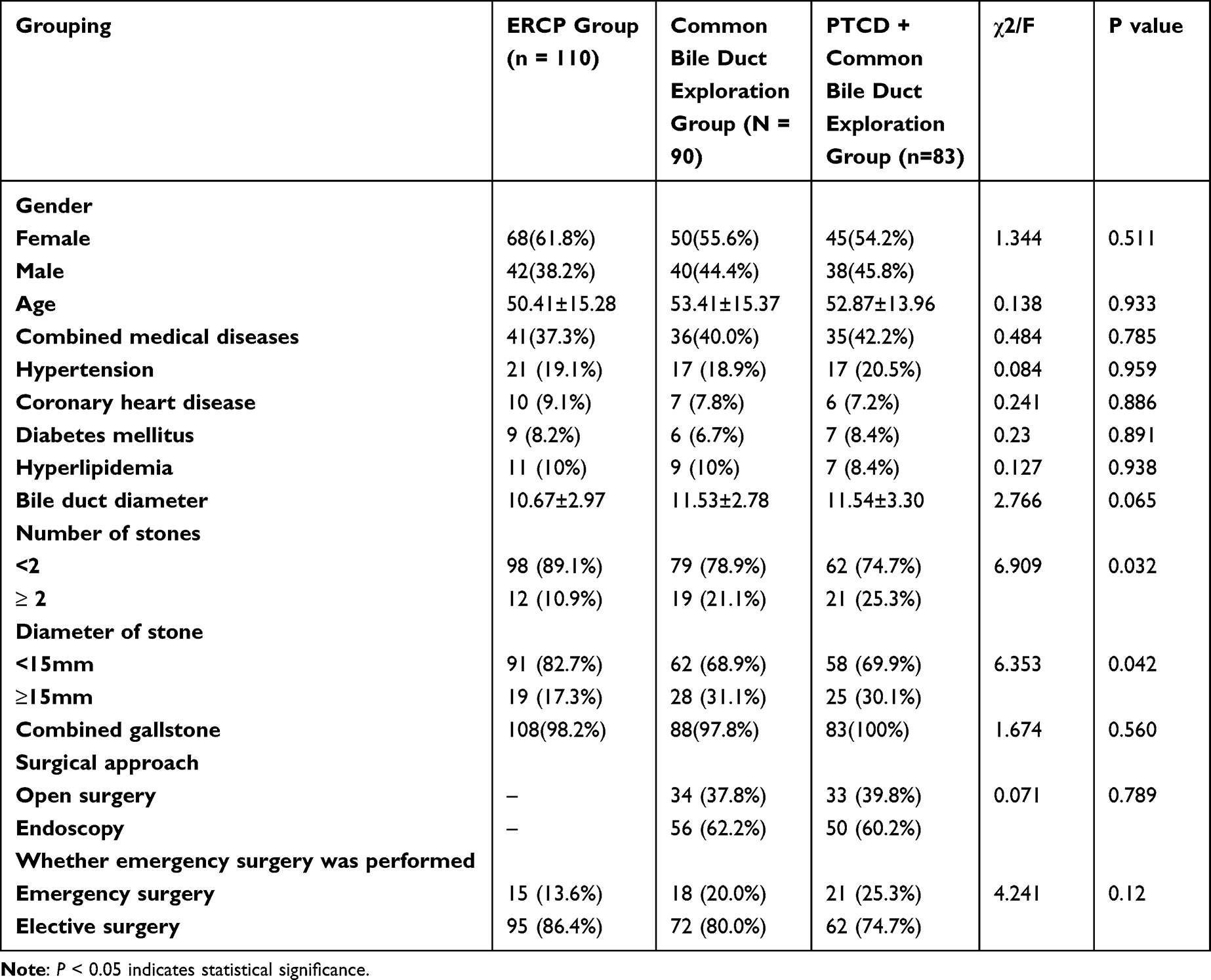 |
Table 1 Comparison of General Information |
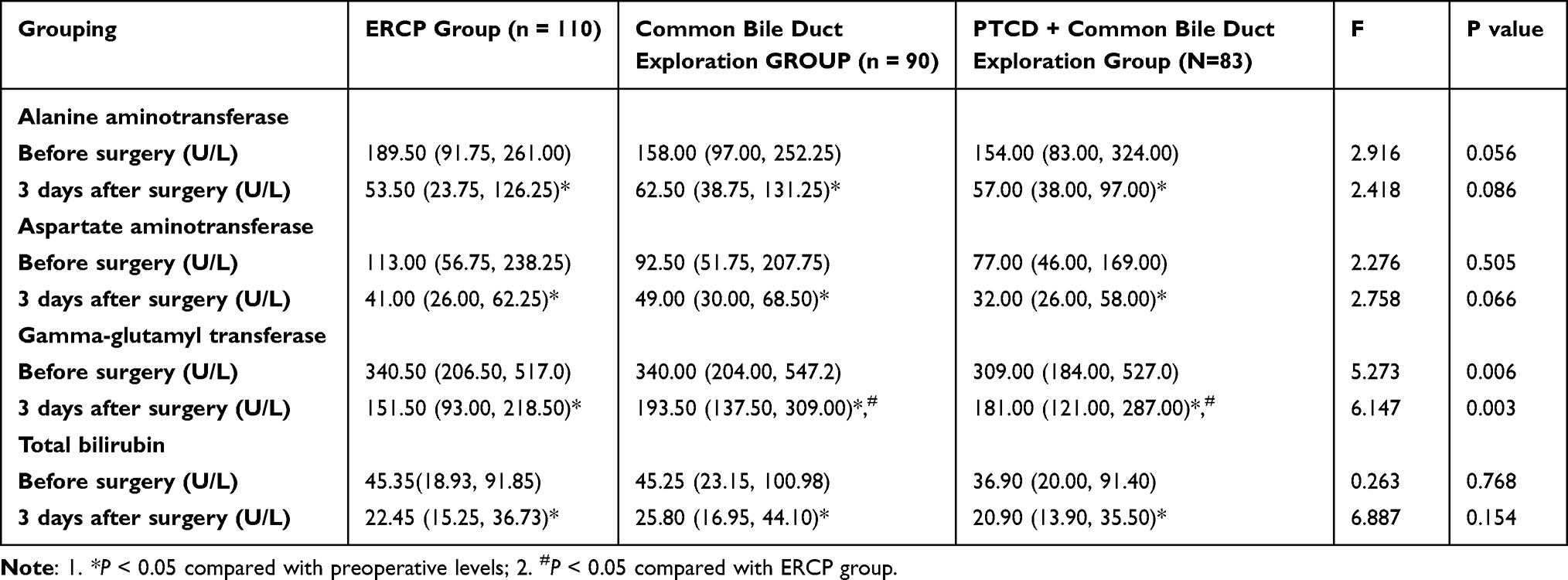 |
Table 2 Comparison of Live Function in the Three Groups |
 |
Table 3 Comparison of White Blood Cell Count in the Three Groups |
 |
Table 4 Comparison of the Percentage of Neutrophils in the Three Groups |
Comparison of the Liver Function Among the Three Kinds of Treatment
The preoperative levels of ALT, AST, GGT, and TBIL exhibited significant elevation across all three treatment groups. However, there were no statistically significant differences observed in the preoperative ALT, AST, GGT, and TBIL levels within each group (P > 0.05). The changes in ALT, AST, GGT, and TBIL values before and after surgery were utilized to assess the effectiveness of the three treatment approaches in liver function recovery and drainage reduction. After a 3-day postoperative period, the levels of ALT, AST, GGT, and TBIL showed a statistically significantly decrease in all three groups when compared to the preoperative values (P < 0.05). At the 3-day postoperative mark, no statistical differences were found in the ALT, AST, and TBIL levels among the three groups (P > 0.05). However, there were statistical differences in GGT levels among the three groups at this time point (P < 0.05). Further analysis revealed a more significant decrease in group A (ERCP group) compared to groups B (common bile duct exploration group) and C (PTCD + common bile duct exploration group), with statistical differences (P = 0.001, P = 0.017). There were no statistical differences between group B (common bile duct exploration group) and group C (PTCD + common bile duct exploration group) (P > 0.05). The difference (D-value) in ALT, AST, GGT, and TBIL before and after surgery did not exhibit statistically significant differences among the three groups (P > 0.05) (refer to Table 2).
Comparison of Leukocyte Status Among the Three Surgical Approaches
The preoperative levels of WBC and N% were significantly higher in all three groups. However, there were no statistical differences observed in the preoperative WBC and N% levels within each group (P > 0.05). The WBC and N% values at 3 days after surgery and the changes in these values before and after surgery were compared. The WBC values at 3 days after surgery showed a significant decrease in all three groups compared to the preoperative values (P < 0.05). Nevertheless, there were no statistical differences in WBC values at 3 days after surgery among the three groups (P > 0.05), and no statistical differences were found in the pre- and post-operative WBC values among the groups (P>0.05). Regarding N%, statistical differences were observed in group A (ERCP group) at 3 days after surgery when compared to the preoperative values(P < 0.05). However, there were no statistical differences between groups B (common bile duct exploration group) and C (PTCD + common bile duct exploration group) (P > 0.05). Additionally, there were no statistical differences in N% at 3 days after surgery among the three groups (P > 0.05), and no statistical differences were found in the changes in N% before and after surgery between the groups (P > 0.05) (refer to Table 3 and Table 4).
Comparison of Intraoperative Bleeding and Postoperative Hospitalization Days Among the Three Surgical Approaches
In terms of intraoperative bleeding, Group A (ERCP group) had the least intraoperative bleeding, while Group B (biliary exploration group) exhibited the highest intraoperative bleeding volume. Group A (ERCP group) displayed a statistically significant reduction in intraoperative bleeding compared to both Group B (common bile duct exploration group) and Group C (PTCD + common bile duct exploration group), with statistical differences (P < 0.05). However, no statistical differences were observed between Group B (common bile duct exploration group) and Group C (PTCD + common bile duct exploration group) (P > 0.05). (refer to Table 5).
 |
Table 5 Comparison of Intraoperative Bleeding and Postoperative Hospitalization Days in the Three Groups |
In terms of postoperative hospitalization days, Group A (ERCP group) had the shortest postoperative hospitalization days and Group B (biliary probe group) had the longest. Group A (ERCP group) demonstrated significantly fewer postoperative hospitalization days compared to both Group B (common bile duct exploration group) and Group C (PTCD + common bile duct exploration group), with statistical differences (P < 0.05). Furthermore, Group C (PTCD + common bile duct exploration group) exhibited a shorter postoperative hospitalization duration than Group B (common bile duct exploration group), with statistical differences (P < 0.05). (refer to Table 5).
Comparison of Postoperative Complications Among the Three Surgical Approaches
Regarding postoperative complications, in Group A (ERCP group), 13 patients experienced complications(11.8%). Among them, 8 cases involved postoperative acute pancreatitis(7.3%), which improved with conservative treatment including infection control, enzyme suppression, and acid control. Three cases experienced postoperative bile duct reflux(2.7%), which also improved with conservative treatment. Two cases developed postoperative bile duct stricture(1.8%). Seven patients in Group B (common bile duct exploration group) had complications(7.8%), including 2 cases of biliary leakage(2.2%), of which 1 case died(1.1%) and 1 case improved after conservative treatment(1.1%), 1 case of postoperative backflow of the bile duct(1.1%), which improved after conservative treatment, and 4 cases of bile duct stricture(4.4%), 2 of which were treated with surgery(2.2%). Group C (PTCD + common bile duct exploration group) had 5 patients with complications(6.0%), including 1 case of postoperative acute pancreatitis(1.2%), which improved with conservative treatment, 1 case of bile leakage(1.2%), which improved with symptomatic treatment involving prolonged ducting time and anti-infection, and 3 cases of postoperative bile duct stricture(3.6%). There were no statistical differences (P > 0.05) in the occurrence of bile leakage, backflow of the bile duct, and bile duct stricture after the three surgical procedures. However, statistical differences (P = 0.005) were observed in the occurrence of postoperative pancreatitis. Further analysis revealed statistical differences between Group A (ERCP group) and Group B (common bile duct exploration group) (P < 0.016), while no statistical differences were observed between Group A (ERCP group) and Group C (PTCD+ common bile duct exploration group), as well as between Group B (common bile duct exploration group) and Group C (PTCD+ common bile duct exploration group) (P > 0.016) (refer to Tables 6). There were no statistical differences in the healing of the incision after open surgery in the common bile duct exploration group and the PTCD + common bile duct exploration group (P = 0.727) (refer toTable 7).
 |
Table 6 Comparison of Postoperative Complications Among the Three Surgical Approaches |
 |
Table 7 Comparison of Incision Healing After Open Surgery in the Common Bile Duct Exploration Group and PTCD + Common Bile Duct Exploration Group |
Comparison of Postoperative Residual Stones and Stone Recurrence Within Three Years Among the Three Surgical Approaches
In Group A (ERCP group), there were 6 cases of postoperative residual stones (5.5%). In Group B (common bile duct exploration group), there were 4 cases of postoperative residual stones (4.4%), and in Group C (PTCD + common bile duct exploration group), there were 3 cases of postoperative residual stones (3.6%). There were no statistical differences (P = 0.937). For Group A (ERCP group), there was 1 case of stone recurrence after three years (0.9%). In Group B (common bile duct exploration group), there were 2 cases of stone recurrence after three years (2.2%), and in Group C (PTCD + common bile duct exploration group), there were 2 cases of stone recurrence after three years (2.4%). Again, there were no statistical differences (P = 0.627) (refer to Table 8 and Table 9).
 |
Table 8 Comparison of the Incidence of Postoperative Residual Stones Among the Three Surgical Approaches |
 |
Table 9 Comparison of the Incidence of Postoperative Stone Recurrence Among the Three Surgical Approaches |
Discussion
Choledocholithiasis, a prevalent condition in China, is a common biliary system disorder.1 Cholangitis, a frequent complication of choledocholithiasis, typically manifests as acute cholangitis, with some patients presenting with acute severe characterized by rapid progression and a high mortality rate associated with infectious shock. Promptly alleviating the obstruction is crucial for the treatment of acute cholangitis. In the past, surgical intervention, particularly bile duct exploration, was the primary approach for managing acute cholangitis.3,4 Sometimes, however, the patients often recovered poorly and had a high mortality rate due to the age of some patients and the combination of various medical diseases. Minimally invasive techniques, such as endoscopic retrograde cholangiopancreatography (ERCP) and percutaneous transhepatic cholangiodrainage (PTCD), have gained popularity as alternative treatment options. Each approach offers distinct advantages. For example, ERCP is less invasive and simpler than surgery, allowing for stone removal, obstruction relief, and improved drainage. Nevertheless, ERCP may be terminated in cases of poor patient cooperation or failed intubation.9–11 PTCD, on the other hand, provides effective jaundice reduction through simple drainage. It is a safe and expedient procedure, particularly suitable for patients with compromised general health and multiple comorbidities. However, PTCD does not address the underlying cause of obstruction, namely stone removal.12 The common bile duct exploration is widely indicated and applied for a long time to remove the cause and usually drainage. Nonetheless, this method is more complex than the previous two and entails a slower postoperative recovery process. Overall, the selection of the most appropriate treatment modality depends on individual patient characteristics, and each approach has its own strengths and limitations.
In this study, we conducted a comprehensive analysis of clinical data from patients diagnosed with choledocholithiasis accompanied by cholangitis. We aimed to compare the treatment outcomes among three groups: the ERCP group, the common bile duct exploration group, and the PTCD + common bile duct exploration group. The preoperative general condition showed that the number of common bile duct stones and the diameter of the stones were statistically different between the three groups, with most of the patients in the ERCP group having less than 2 stones and less than 15 nm in diameter compared to the other two groups. Regarding the postoperative decrease in serum ALT, AST, GGT, and TBIL levels, all three treatment methods exhibited effectiveness in improving liver function and reducing jaundice. No statistically significant differences were observed between the three groups in the postoperative values of ALT and TBIL. However, there were statistically significant differences in the postoperative GGT values among the three groups, with the ERCP group showing superior performance compared to the other two groups. This difference can be attributed to the T-tube drainage employed in the other two groups, which stimulated the bile ducts and resulted in a slower decrease in GGT levels. In addition, we evaluated the impact of the three treatment methods on leukocyte count and neutrophil percentage. The results suggested that all three treatment methods were effective in controlling infection. In terms of leukocyte count, the differences between the three groups were not statistically significant. However, in terms of neutrophil percentage, the ERCP group exhibited a statistically significant decrease after surgery compared to before surgery. In contrast, no statistical differences were observed in the common bile duct exploration group and PTCD + common bile duct exploration group. The slower recovery and greater trauma associated with the common bile duct exploration group and PTCD + common bile duct exploration group likely contributed to the slower decrease in neutrophil percentage. Notably, in the common bile duct exploration group, the neutrophil percentage of 12 patients did not decrease at 3 days after surgery and was even higher than the preoperative levels.
The occurrence of common complications following ERCP include pancreatitis, bleeding, perforation, and infection. Pancreatitis is the most prevalent complication with an incidence rate of approximately 9.7%.13 In the ERCP group of this study, postoperative pancreatitis occurred in 8 cases (7%), which is similar to the values reported in the literature.14–17 Elevated amylase levels are commonly observed in patients post-surgery, and risk factors associated with pancreatitis include repeated intubation procedures (≥5 times), use of intra-pancreatic ductal contrast, papillotomy, papillary balloon dilation, and suspected sphincter of Oddi dysfunction.18–20 Therefore, it is crucial to thoroughly evaluate the patient’s medical history for risk factors of pancreatitis before surgery. During the procedure, efforts should be made to minimize operative time, reduce the amount of contrast agent used, and limit the number of pancreatic duct insertions, while ensuring satisfactory surgical outcomes. Routine monitoring of pancreatic enzyme changes is recommended post-surgery.
Bleeding is one of the most serious complications of ERCP, with an incidence of about 0.3%-2%.13,21 In this study, no bleeding complications occurred. It can manifest as intraoperative or postoperative bleeding. Coagulation disorders, use of anticoagulants before and within 3 days after ERCP and active cholangitis are considered risk factors for bleeding, and intraoperative injury to blood vessels is also a common cause of bleeding.22–25 For patients with a high risk of bleeding, it is advisable to avoid Oddi sphincterotomy whenever possible. In case of bleeding, priority is given to microscopic hemostasis, which can be done with electrocoagulation, titanium clips, balloon compression, etc. If bleeding persists, interventional or surgical treatment may be necessary. The incidence of perforation is approximately 0.08%-0.6%.26 In this study, no complications of perforation occurred. And it is mainly due to improper operation, with abnormal local anatomy, suspected sphincter of Oddi dysfunction, repeated intubation, prolonged operation, papillary sphincterotomy, and balloon dilation being considered as risk factors for perforation.27–30 Early detection of perforation followed by conservative measures like fasting and anti-infection protocols can effectively manage most patients. However, severe cases presenting with shock and diffuse peritonitis may require early surgical intervention. Infections are another potential complication following ERCP, with acute biliary cholangitis being the most common, occurring at an incidence of 0.5–3%.31–34 In this study, acute biliary cholangitis pancreatitis occurred in 3 cases (2.7%), which is similar to the values reported in the literature. Risk factors for infection include failure of bile duct drainage, residual postoperative stones, and the use of contrast agents, which can contribute to cholangitis and duodenoscopy-related infections, although such instances are infrequent. All patients exhibited improvement with conservative treatment. In this study, only one patient encountered a catheter insertion failure. Subsequently, the patient underwent laparoscopic common bile duct exploration to remove the stone. The incidence of postoperative pancreatitis in the ERCP group in this study was significantly higher than in the other two groups.
Complications commonly associated with PTCD include biliary tract infection, bleeding, bile leakage, and duct obstruction. Biliary tract infection, as a common complication of PTCD, In this study, no complications of biliary tract infection occurred, It can arise from biliary hypertension, lax aseptic practice, bile reflux, intestinal contents entering the bile duct, and prolonged drainage.35 The duration of drainage is positively correlated with the likelihood of infection.36 Preoperative antibiotics have been shown to reduce the incidence of infection.37 The incidence of biliary tract bleeding is low, mostly due to injury to intrahepatic vessels during puncture and, in a few cases, due to abnormal coagulation, so it is particularly important to choose a suitable puncture route. We believe that an ultrasound-guided puncture is significantly safer than a blind puncture, avoiding large vessels and bleeding. Consequently, it is essential to evaluate the patient’s coagulation function before surgery, exercise caution during the procedure, and closely monitor the patient postoperatively.Bile leakage is one of the complications of PTCD, one case of postoperative bile leakage (1.2%) occurred in the PTCD + common bile duct exploration group, which are similar to the values reported in the literature.38 Bile leakage often occurs due to catheter dislodgement or multiple punctures at the same site. In most cases, conservative treatment, including fasting, anti-infection, nutrition enhancement, and symptomatic treatment.39,40 PTCD may also present with pneumothorax and hemothorax, mostly due to poor selection of the puncture site. In this study, one case of postoperative pancreatitis (1.2%). Notably, all patients experienced improvement following conservative treatment.
The common complications associated with common bile duct exploration + T-tube drainage include postoperative infection, bleeding, and bile leakage.41 Common postoperative infections include cholangitis, incisional infection, and pneumonia. In this study, 8 patients(8.8%) in the common bile duct exploration group and 6 patients(7.2%) in the PTCD + common bile duct exploration group exhibited suboptimal incisional healing after surgery. Among the common bile duct exploration group, one patient developed postoperative biliary leakage and infection, leading to mortality due to severe infection causing multi-organ dysfunction 57 days after the procedure. However, the remaining patients with postoperative infections showed improvement following conservative treatment. In our study, of the 106 cases of laparoscopic Common Bile Duct exploration conducted in both the bile duct exploration group and the PTCD + bile duct exploration group, 100 cases were successfully completed, yielding a success rate of 94.3%. For patients in whom the procedure was unsuccessful, we conducted remedial open Common Bile Duct exploration. And we conducted 67 cases of open Common Bile Duct exploration, of which 66 cases were successfully completed, resulting in a success rate of 98.5%. Regarding the one unsuccessful case, we identified bile duct injury during the surgery, and we underwent a bilioenterostomy.
Based on the findings of this study, we suggest that for patients with mild symptoms, good general condition, less than 2 common bile duct stones, and stones less than 15 mm in diameter, ERCP can be preferred approach following conservative treatment. This method is relatively less traumatic for patients, with faster postoperative recovery and shorter hospitalization duration. However, it is worth noting that postoperative pancreatitis is more likely with this approach. For patients who face challenges with ERCP but are in good general condition and can tolerate the surgery, direct common bile duct exploration + T-tube drainage can be considered. In cases of acute onset, severe disease, poor general condition, and multiple combined medical diseases, we recommend initiating PTCD for bile ducts drainage while simultaneously administering conservative treatment. Subsequent surgery should be performed once the patient’s general condition improves. This approach aims to enhance surgical success rates, minimize the need for secondary surgeries, and reduce postoperative complications. Considering that most patients with PTCD have heavy inflammation and stones which are not easily treated, ERCP is typically not selected following PTCD.
Conclusions
1. For patients with fewer and smaller common bile duct stones and milder symptoms, it is recommended to primarily choose endoscopic retrograde cholangiopancreatography (ERCP), endoscopic sphincterotomy (EST), and endoscopic nasobiliary drainage (ENBD), it procedures offer quicker recovery and cause minimal trauma.
2. For patients with numerous, larger common bile duct stones but stable conditions, bile duct exploration is recommended. Meanwhile, for patients with severe conditions and significant inflammation, PTCD and common bile duct exploration are advised.
Disclosure
The authors report conflicts of interest in this work.
References
1. Freitas ML, Bell RL, Duffy AJ. Choledocholithiasis: evolving standards for diagnosis and management. World J Gastroenterol. 2006;12(20):3162–3167. doi:10.3748/wjg.v12.i20.3162
2. Qin YS, Li V, Yang FC, et al. Risk factors and incidence of acute pyogenic cholangitis. Inter J Hepatobiliary Pancreas. 2012;11(6):650–654. doi:10.1016/S1499-3872(12)60240-9
3. Sakpal SV, Babel N, Chamberlain RS. Surgical management of hepatolithiasis. Hpb Official J Inter Hepato Pancreato Biliary Assoc. 2009;11(3):194–202. doi:10.1111/j.1477-2574.2009.00046.x
4. Tsuyuguchi T, Miyakawa K, Sugiyama H, et al. Ten ‐year long ‐term results after non ‐surgical management of hepatolithiasis, including cases with choledochoenterostomy. J Hepatobiliary Pancreat Sci. 2014;21(11):795. doi:10.1002/jhbp.134
5. Cheng YF, Lee TY, Sheen-Chen SM, et al. Treatment of complicated hepatolithiasis with intrahepatic biliary stricture by ductal dilatation and stenting: long-term results. World J Surg. 2000;24(6):712–716. doi:10.1007/s002689910114
6. Gurusamy KS, Giljaca V, Takwoingi Y, et al. Endoscopic retrograde cholangiopancreatography versus intraoperative cholangiography for diagnosis of common bile duct stones The Cochrane Library. Cochrane Data Syst Rev. 2015;33(2):1391–1396.
7. Wang P, Sun B, Huang B. Comparison between percutaneous transhepatic rigid cholangioscopic lithotripsy and conventional percutaneous transhepatic cholangioscopic surgery for hepatolithiasis treatment. Surg Laparosc Endosc Percutan Tech. 2016;26(1):54. doi:10.1097/SLE.0000000000000222
8. Fidelman N. Benign biliary strictures: diagnostic evaluation and approaches to percutaneous treatment. Tech Vasc Interv Radiol. 2015;18(4):210–217. doi:10.1053/j.tvir.2015.07.004
9. Prachayakul V, Aswakul P. Endoscopic retrograde cholangiopancreatography-related perforation: management and prevention. World J Clin Cases. 2014;2(10):522–552. doi:10.12998/wjcc.v2.i10.522
10. Kawaguchi Y. Randomized controlled trial of pancreatic stenting to prevent pancreatitis after endoscopic retrograde cholangiopancreatography. World J Gastroenterol. 2012;18(14):1635. doi:10.3748/wjg.v18.i14.1635
11. Ajaypal S, Andres G, Banke A. Biliary strictures: diagnostic considerations and approach. Gastroenterol Rep. 2014;3(1):22–31.
12. Chandrashekhara SH, Gamanagatti S, Singh A, et al. Current status of percutaneous transhepatic biliary drainage in palliation of malignant obstructive jaundice: a review. Indian J Palliat Care. 2016;22(4):378–387. doi:10.4103/0973-1075.191746
13. Kochar B, Akshintala VS, Afghani E, et al. Incidence, severity, and mortality of post-ERCP pancreatitis: a systematic review by using randomized, controlled trials. Gastrointest Endosc. 2015;81(1):143–149. doi:10.1016/j.gie.2014.06.045
14. Coelho-Prabhu N, Shah ND, Van Houten H, et al. Endoscopic retrograde cholangiopancreato- graphy: utilisation and outcomes in a 10-year population-based cohort. BMJ Open. 2013;3(5):e002689–e002689. doi:10.1136/bmjopen-2013-002689
15. Adler DG, Cohen J, Pike IM, et al. Quality indicators for ERCP. Am J Gastroenterol. 2015;81(1):54–66.
16. Kim SB, Kim KH, Kim TN. Comparison of outcomes and complications of endoscopic common bile duct stone removal between asymptomatic and symptomatic patients. Dig Dis Sci. 2016;61(4):1172–1177. doi:10.1007/s10620-015-3965-5
17. Vila JJ, Artifon EL, Otoch JP. Post-endoscopic retrograde cholangiopancreatography complications: how can they be avoided. World J Gastrointest Endosc. 2012;4(6):241. doi:10.4253/wjge.v4.i6.241
18. Halttunen J, Meisner S, Aabakken L, et al. Difficult cannulation as defined by a prospective study of the Scandinavian Association for Digestive Endoscopy (SADE) in 907 ERCPs. Scand J Gastroenterol. 2014;49(6):752–758. doi:10.3109/00365521.2014.894120
19. Donatelli G, Dumont JL, Cereatti F, et al. Revision of biliary sphincterotomy by re-cut, balloon dilation or temporary stenting: comparison of clinical outcome and complication rate (with video). Endosc Int Open. 2017;5(5):E395–E401. doi:10.1055/s-0043-106183
20. Mine T, Morizane T, Kawaguchi Y, et al. Clinical practice guideline for post-ERCP pancreatitis. J Gastroenterol. 2017;52(9):1013–1022. doi:10.1007/s00535-017-1359-5
21. Rustagi T, Jamidar PA. Endoscopic retrograde cholangiopancreato- graphy-related adverse events: general overview. Gastrointest Endosc Clin N Am. 2015;25(1):97–106. doi:10.1016/j.giec.2014.09.005
22. Cho CL, Yuen KK, Yuen CH, et al. Splenic laceration a er endoscopic retrograde cholangiopancreatography. Xianggang Yi Xue Za Zhi. 2008;14(2):145–147.
23. Soler Humanes R, Suárez Muñoz MÁ, García García B. A post-endoscopic retrograde cholangiopancreatography subcapsular hepatic hematoma. Rev Esp Enferm Dig. 2017;109(11):803. doi:10.17235/reed.2017.5123/2017
24. McArthur KS, Mills PR. Subcapsular hepatic hematoma after ERCP. Gastrointest Endosc. 2008;67(2):379–380. doi:10.1016/j.gie.2007.06.008
25. Inoue H, Tano S, Takayama R, et al. Right hepatic artery pseudoa-neurysm: rare complication of plastic biliary stent insertion. Endoscopy. 2011;43:E396. doi:10.1055/s-0030-1256942
26. Karaahmet F, Kekilli M. The presence of periampullary diverticulum increased the complications of endoscopic retrograde cholangiopancreatography. Eur J Gastroenterol Hepatol. 2018;30(9):1009–1012. doi:10.1097/MEG.0000000000001172
27. Srivastava S, Sharma BC, Puri AS, et al. Impact of completion of primary biliary procedure on outcome of endoscopic retrograde cholangiopancreatographic related perforation. Endosc Int Open. 2017;5(8):E706–E709. doi:10.1055/s-0043-105494
28. Weiser R, Pencovich N, Mlynarsky L, et al. Management of endoscopic retrograde cholangiopancreatography-related perforations: experience of a tertiary center. Surgery. 2017;161(4):920–929. doi:10.1016/j.surg.2016.10.029
29. Takano Y, Nagahama M, Yamamura E, et al. Perforation of the papilla of vater in wire-guided cannulation. Can J Gastroenterol Hepatol. 2016;2016:5825230. doi:10.1155/2016/5825230
30. Avgerinos DV, Llaguna OH, Lo AY, et al. Management of endoscopic retrograde cholangiopancreatography: related duodenal perforations. Surg Endosc. 2009;23(4):833–838. doi:10.1007/s00464-008-0157-9
31. Wan X, Chen S, Zhao Q, et al. The efficacy of temporary placement of nasobiliary drainage following endoscopic metal stenting to prevent post-ERCP cholangitis in patients with cholangiocarcinoma. Saudi J Gastroenterol. 2018;24(6):348. doi:10.4103/sjg.SJG_94_18
32. Khashab MA, Tariq A, Tariq U, et al. Delayed and unsuccessful endoscopic retrograde cholangiopancreatography are associated with worse outcomes in patients with acute cholangitis. Clin Gastroenterol Hepatol. 2012;10(10):1157–1161. doi:10.1016/j.cgh.2012.03.029
33. Kapral C, Mühlberger A, Wewalka F, et al. Quality assessment of endoscopic retrograde cholangiopancreatography: results of a running nationwide Austrian benchmarking project after 5 years of implementation. Eur J Gastroenterol Hepatol. 2012;24(12):1447. doi:10.1097/MEG.0b013e3283583c6f
34. Colton JB, Curran CC. Quality indicators, including complications, of ERCP in a community setting: a prospective study. Gastrointest Endosc. 2009;70(3):457–467. doi:10.1016/j.gie.2008.11.022
35. Kim JH. Endoscopic stent placement in the palliation of malignant biliary obstruction. Clin Endosc. 2011;44(2):76–86. doi:10.5946/ce.2011.44.2.76
36. O’Neill SB, O’Connor OJ, Ryan MF, et al. Interventional radiology and the care of the oncology patient. Radiol Res Pract. 2011;2011:1–11. doi:10.1155/2011/160867
37. Lewis CA, Cardella JF, Citron SJ. Quality improvement guidelines for percutaneous transhepatic cholangiography and biliary drainage. J Vasc Interv Radiol. 2003;14(9):S243–S246.
38. Nennstiel S, Weber A, Frick G, et al. Drainage-related complications in percutaneous transhepatic biliary drainage: an analysis over 10 Years. J Clin Gastroenterol. 2015;49(9):764. doi:10.1097/MCG.0000000000000275
39. Bao G, Liu H, Ma Y, et al. The clinical efficacy and safety of differ⁃ ent biliary drainages in malignant obstructive jaundice treatment. Am J Transl Res. 2021;13(6):
40. Inamdar S, Slattery E, Bhalla R, et al. Comparison of adverse events for endoscopic vs percutaneous biliary drainage in the treatment of ma⁃ lignant biliary tract obstruction in an inpatient national cohort. JAMA Oncol. 2016;2(1):
41. Steel AW, Postgate AJ, Khorsandi S, et al. Endoscopically applied radiofrequency ablation appears to be safe in the treatment of malignant biliary obstruction. Gas Tro Intest Endosc. 2011;73(1):149–153. doi:10.1016/j.gie.2010.09.031
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.