Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Evaluation of Clinical Characteristics and Lung Function Trajectories in Young COPD Patients Within the General Population
Authors Nam JH ![]() , Rhee CK
, Rhee CK ![]() , Jo YS
, Jo YS ![]() , Kim S, Kim YS
, Kim S, Kim YS ![]() , Kim SH, Kim KH, Choi JY
, Kim SH, Kim KH, Choi JY ![]()
Received 5 November 2025
Accepted for publication 9 March 2026
Published 17 March 2026 Volume 2026:21 579212
DOI https://doi.org/10.2147/COPD.S579212
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Jung Hyun Nam,1 Chin Kook Rhee,2 Yong Suk Jo,2 Seohyun Kim,3 Yun Seok Kim,4 Sang Hyuk Kim,5 Kyung Hoon Kim,4 Joon Young Choi4
1Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, St. Vincent’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Republic of Korea; 2Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Seoul St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Republic of Korea; 3Division of Pulmonology and Critical Care Medicine, Department of Internal Medicine, Yeouido St. Mary’s Hospital, College of Medicine, the Catholic University of Korea, Seoul, Republic of Korea; 4Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Incheon St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Incheon, Republic of Korea; 5Division of Pulmonary, Allergy, and Critical Care Medicine, Department of Internal Medicine, Korea University Guro Hospital, Korea University College of Medicine, Seoul, Republic of Korea
Correspondence: Joon Young Choi, Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Incheon St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, 56 Dongsu-ro, Bupyeong-gu, Incheon, 21431, Republic of Korea, Email [email protected]
Purpose: Young chronic obstructive pulmonary disease (COPD), distinct from COPD in older individuals, often remains underdiagnosed despite its potential for early interventions. This study aimed to identify the characteristics of young COPD patients and the patterns of lung function trajectory.
Patients and Methods: This study was based on a large community-based cohort database in Korea. Young COPD was defined as COPD diagnosed in patients aged ≤ 50 years. We analyzed the clinical characteristics and lung function changes over 12 years, comparing young and old COPD patients.
Results: Among the 9,577 patients enrolled in this study, 815 (8.5%) were diagnosed with COPD. The young COPD group had a higher proportion of females, never-smokers and a higher body mass index (BMI), compared to the older COPD group. The prevalence of young COPD increased from 117 (3.64%) to 334 (6.88%) according to the lower limit of normal (LLN) criteria. Analysis of lung function over 12 years revealed that the rate of decline in FEV1 (L), FEF25-75% (L), and FEV1/FVC ratio was slower in young COPD than in old COPD. Multivariate Cox analysis identified female sex, higher FEV1 (%), and young COPD as independent predictive factors for time-to-first normalization of airflow obstruction. Old COPD and low FEV1 (%) were identified as independent risk factors for time-to-first dyspnea.
Conclusion: Young COPD is characterized by a higher proportion of females, non-smokers, and elevated BMI compared to old COPD. It has potential for lung function recovery and serves as an independent prognostic factor for the normalization of airflow obstruction.
Keywords: chronic obstructive pulmonary disease, cohort study, spirometry, normalized obstruction
Introduction
Chronic obstructive pulmonary disease (COPD) is a highly prevalent chronic lung disease associated with a high social burden and significant mortality worldwide.1–3 Although COPD is not be fully reversible, it is preventable and manageable with early diagnosis and intervention.4,5 It is predominantly diagnosed in individuals > 60 years of age6 but can also present in individuals aged 20–50 years, recently categorized as “young COPD”.7,8
Lung development continues until age 20–25, reaching peak lung function before gradually declining.9 Based on the life-course trajectory of lung function, the developmental course of COPD can be categorized into two key processes, which may overlap in certain populations.10,11 The first process involves individuals with a normal peak lung function, who may develop COPD due to accelerated pulmonary function decline caused by cumulative exposure to environmental risk factors, such as tobacco use.12,13 The second process involves individuals who, despite a normal rate of decline, start with a lower peak forced expiratory volume in 1 s (FEV1), leading to COPD in their later years through the normal aging process.14,15 Considering these lung function trajectories, young COPD patients form a distinct group that develops the disease despite lower cumulative environmental exposure compared to older COPD patients. Therefore, it is likely that this group may have a higher prevalence of low baseline peak lung function, predisposing genetic factors, and increased susceptibility to environmental stimuli, contributing to the unique clinical characteristics of young COPD.16,17 In addition to impaired peak lung function, specific factors associated with young COPD include childhood respiratory infections, asthma or airway hyperresponsiveness, and structural airway–lung size mismatch such as dysanapsis.18,19 Clinically, young COPD patients have been reported to include a higher proportion of females and never-smokers and to present with milder respiratory symptoms despite spirometric airflow limitation.20,21 These findings support the concept that young COPD represents a heterogeneous phenotype rather than simply an earlier stage of smoking-related COPD.
Young COPD, distinct from “old COPD”, tends to be underdiagnosed despite the potential for better outcomes with early treatment.22 For the early identification of individuals at risk for COPD, the lower limit of normal (LLN), defined as a FEV1/forced vital capacity (FVC) ratio less than the 5th percentile of the predicted value, has recently been used instead of the fixed ratio recommended by the Global Initiative for Chronic Obstructive Lung Disease (GOLD).17,23 Research has also indicated that middle-aged adults who were not categorized as having COPD using the fixed ratio, but were diagnosed using the LLN, had higher respiratory and cardiovascular morbidity and earlier mortality.24
Studies on young COPD face challenges owing to underdiagnosis and fewer hospital visits.25 Therefore, there are few previous studies on the clinical characteristics of young COPD patients, with a lack of studies investigating the long-term disease course. The present study assessed the clinical characteristics and lung function trajectories of young COPD patients using both the fixed ratio and LLN criteria in a community-based prospective cohort in Korea.
Materials and Methods
Study Design and Population
This study was based on the Ansan-Ansung cohort, a large-scale prospective cohort study based in Ansan (urban) and Ansung (rural) aimed at investigating factors associated with chronic diseases. This cohort is part of the Korea Genome and Epidemiology Study (KoGES) examining chronic diseases in Korea, supported by the National Genome Research Institute (Korea Centers for Disease Control and Prevention, Cheongju, Korea). Detailed information regarding the study design and protocol has been documented in a previous report.26 Participants aged 40–69 years were enrolled, with baseline measurements conducted between 2001 and 2002. The baseline examinations were followed biennially. We analyzed data from a baseline survey up to 6th biennial survey in 2013–2014. Among the 10,030 subjects, 453 were excluded because they either lacked a baseline pulmonary function test (PFT) or were undergoing asthma treatment.
Data Collection and COPD Definition
Trained investigators evaluated the participants’ socioeconomic status, lifestyle, psychological stress, and respiratory symptoms using the KoGES baseline questionnaire. Physical measurements were used to calculate the body mass index (BMI). For socioeconomic categorization, high income was defined as a monthly household income of ≥ 4 million won, whereas low income was defined as monthly household income < 2 million won per month. Smoking status, assessed via self-reported questionnaires, was categorized as never, former, or current smoker. Data regarding comorbidities and respiratory symptoms, including dyspnea, cough, and sputum, were collected. For cases of dyspnea, the modified Medical Research Council (mMRC) score and date of first occurrence were recorded. Chronic bronchitis was defined as frequent cough and sputum production for 3 months per year over 2 consecutive years.27,28 Lung function tests were conducted by a trained technician using a standardized spirometer (Vmax 2130; SensorMedics, Yorba Linda, CA, USA). Calibration and quality control followed established guidelines by the American Thoracic Society and European Respiratory Society guidelines.29,30
COPD was diagnosed using two distinct criteria based on baseline lung function measurements: the fixed ratio criterion required a pre-bronchodilator FEV1/FVC of < 0.70, while the LLN criterion required a FEV1/FVC ratio below the 5th percentile of the reference population.31 Young COPD was defined as COPD in individuals aged ≤ 50 years.25,32,33
Statistical Analyses
Clinical features were compared between young and old COPD patients using the chi-square test and Student’s t-test. Continuous variables are presented as means ± standard deviation, while categorical variables are presented as numbers and percentages. To assess the agreement between the fixed ratio and LLN for COPD diagnosis, Cohen’s kappa (κ) was calculated, with 0.00 ≤ κ ≤ 0.02 indicating slight, 0.21 ≤ κ ≤ 0.40 indicating fair, 0.41 ≤ κ ≤ 0.60 indicating moderate, 0.61 ≤ κ ≤ 0.80 indicating good, and 0.81 ≤ κ ≤ 1.00 indicating perfect agreement.34 The annual changes in lung function, including FEV1, FVC, forced mid-expiratory flow (FEF25–75%), and FEV1/FVC, over 12 years were assessed for young and old COPD patients through a longitudinal analysis using linear mixed models. Adjusted covariates included age, sex, BMI, smoking status, and baseline FEV1(L) and biomass exposure. An independent t-test was used to compare the change in lung function from baseline to the end of follow-up within old and young COPD group. Some of the patients initially classified as having COPD recovered from airflow obstruction during the follow-up period. Survival analysis was used to evaluate the difference in time to first normalized obstruction and time to first dyspnea between young and old COPD patients, with multivariable Cox regression analyses used to identify the covariates associated with these factors. All analyses were two-sided with a statistical significance level of p < 0.05, and they were conducted using R software (v. 4.3.2; R Development Core Team, Vienna, Austria).
Results
Group Differences in Baseline Characteristics: COPD Defined by the Fixed Ratio
Among the 9,577 study participants, 815 (8.5%) fulfilled the spirometric criteria for COPD based on a FEV1/FVC of < 0.7. Among these patients, 638 (84.5%) and 117 (15.5%) were classified as old and young COPD patients, respectively. Baseline characteristics of non-COPD, young COPD, and old COPD in the overall study population are presented in Supplementary Table 1. Table 1 presents the differences in baseline characteristics between the young and old COPD patients. Compared to old COPD, the young COPD group had a higher proportion of females (21.5% vs 33.3%, p = 0.002) and a higher BMI (23.2 ± 3.0 vs 24.0 ± 2.8, p = 0.002). Additionally, the young COPD group had higher proportions of urban residents (22.6% vs 37.3%, p < 0.001), individuals educated up to middle or high school level (42.1% vs 79.4%, p < 0.001), and individuals with a high household income. The young COPD group also had a higher proportion of individuals who had never smoked (25.6% vs 37.7%, p = 0.007) and a lower number of pack-years (32.3 ± 20.1 vs 25.3 ± 16.7, p < 0.001) compared to the old COPD group. There was no difference in biomass exposure between the two groups. Hypertension (HTN) was more prevalent in old COPD patients (48.1% vs 14.3%, p < 0.001), with no significant differences in other comorbidities.
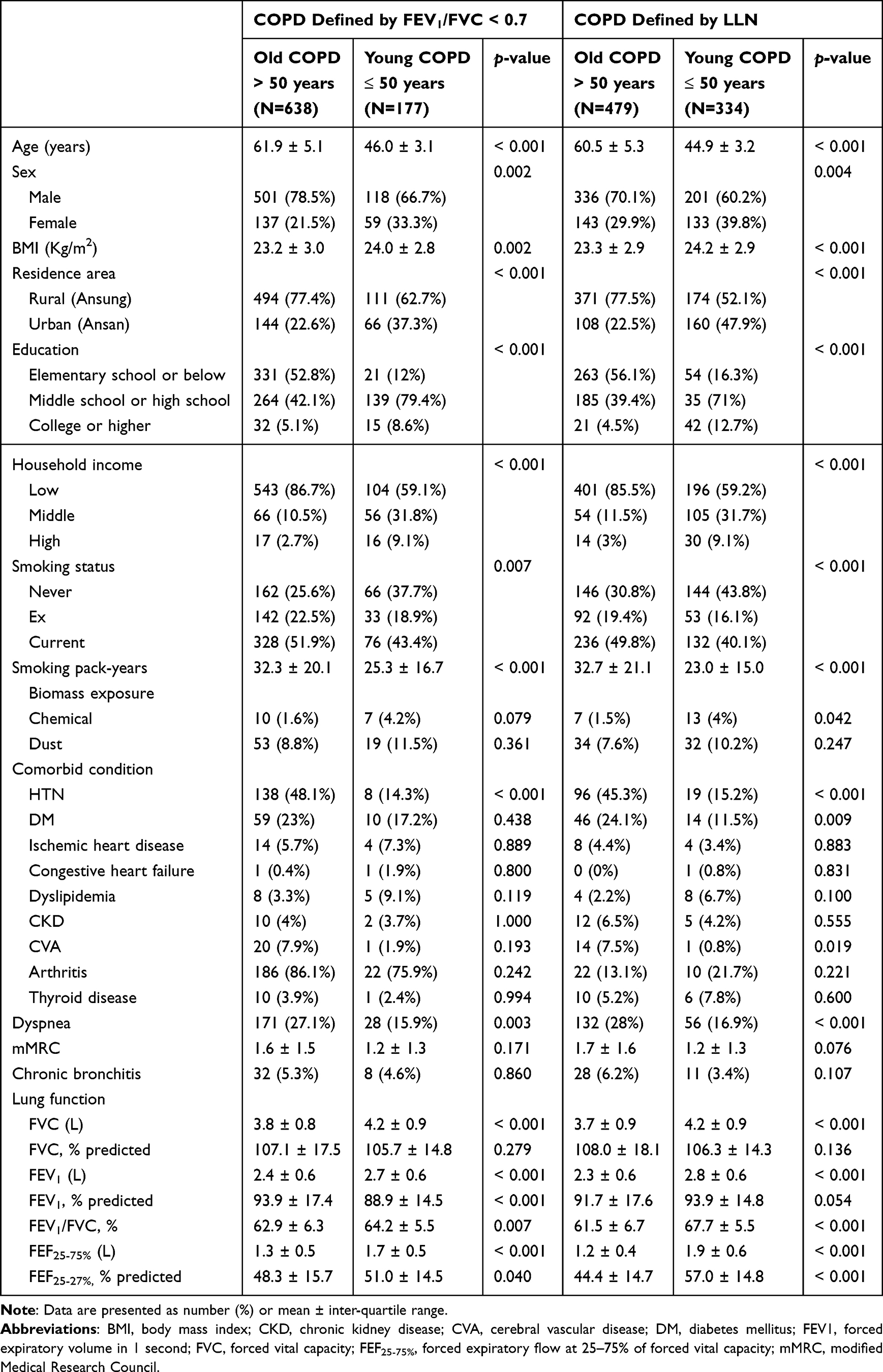 |
Table 1 Baseline Characteristics of Subjects Fulfilled the Spirometric Criteria for COPD |
A greater proportion of old COPD subjects experienced dyspnea (27.1% vs 15.9%, p = 0.003), but the mMRC grade showed no significant group difference. The prevalence of chronic bronchitis symptoms was also similar between the groups. Regarding lung function tests, young COPD patients had higher FVC(L), FEV1(L), FEV1/FVC ratio, FEF25–75%(L), and FEF25–75% % predicted values. While there was no group difference in the FVC % predicted values, the FEV1% predicted was higher in old COPD compared to young COPD (93.9 ± 17.4 vs 88.9 ± 14.5, p < 0.001).
Group Differences in Baseline Characteristics: COPD Defined by LLN
Based on an FEV1/FVC ratio < LLN, 816 (8.5%) individuals fulfilled the spirometric criteria for COPD, including 479 (58.9%) old COPD and 334 (41.1%) young COPD patients. Supplementary Table 2 presents the numbers and respective proportions of COPD patients who fulfilled the spirometric criteria according to the fixed ratio and LLN criteria. When using the LLN instead of the fixed ratio, there was a noticeable decrease in COPD prevalence from 638 (13.52%) to 479 (10.15%) in the old COPD group. Conversely, the number of individuals classified as having COPD increased from 177 (3.64%) to 334 (6.88%) in the young COPD group when using the LLN criteria. COPD diagnosis based on a FEV1/FVC ratio < 0.7 and FEV1/FVC ratio < LLN showed good agreement in both groups, although old COPD patients exhibited a higher κ-value (0.673 vs 0.782).
The baseline characteristics of old and young COPD patients, defined using the LLN, are presented in Table 1. The young COPD group had a higher proportion of females and a higher BMI. The socioeconomic aspects also mirrored those observed with the fixed ratio criterion; young COPD patients more commonly resided in urban areas and had a higher education level and household income. However, there was no difference in the prevalence of mild depression between the two groups. Regarding smoking history, there was a higher percentage of never-smokers and a lower number of pack-years in the young COPD group. Contrary to what was seen when using the fixed ratio criterion, the young COPD group had a higher rate of exposure to chemicals (1.5% vs 4%, p = 0.042). Regarding comorbidities, while group differences were seen only in HTN when using the fixed ratio criterion, the prevalence rates of diabetes mellitus and cerebrovascular accidents, in addition to HTN, were higher among older patients when using the LLN criterion.
Despite a higher incidence of dyspnea in old COPD patients, there was no significant group difference in the mMRC grade. Regarding lung function, young COPD patients showed higher FVC(L), FEV1(L), FEV1/FVC ratio, FEF25–75%(L), and FEF25–27% % predicted values. There was no difference in the FVC % predicted values between the two groups. Although statistically insignificant, when using the LLN criterion, the young COPD group exhibited a higher average FEV1% predicted value compared to the old COPD group, which contrasted with the findings obtained using the fixed ratio criterion.
Lung Function Trajectories
The annual lung function changes over a 12-year period were compared between young and old COPD patients using linear mixed models. Number of participants who underwent lung function tests at each follow-up is shown in Supplementary Table 3. The annual rate of FEV1 decline was lower in young COPD (−38.3 mL/y vs −19.0 mL/y, p < 0.001) (Figure 1A). There was no difference in the annual rate of FVC(L) decline between the groups (−52.1 mL/y vs −47.5 mL/y, p = 0.171) (Figure 1B). The mean FEF25–75%(L) in old COPD showed a decrease of −25.9 mL/y, contrasting with the significant increase of +71.0 mL/y in young COPD (p < 0.001) (Figure 1C). The old COPD group experienced a FEV1/FVC ratio decline of −0.47/y, while the young COPD group showed an increase of +0.66/y, representing a statistically significant difference (p < 0.001) (Figure 1D). When comparing lung function changes between baseline and the end of follow-up, the young COPD group showed a significantly smaller decline in FEV1 compared to the old COPD group, while FEV1/FVC exhibited a slight increase (Supplementary Figure 1). Annual lung function changes were also compared with non-COPD individuals (Supplementary Figure 2).
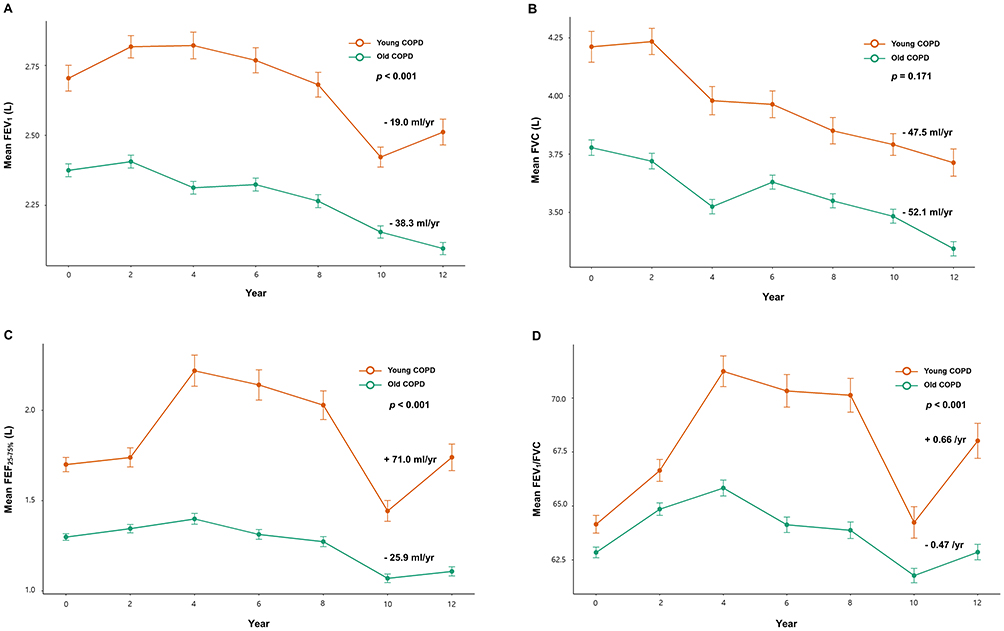 |
Figure 1 Lung function trajectory over time. (A) FEV1; (B) FVC; (C) FEF25–75%; (D) FEV1/FVC ratio. |
Subgroup Analysis by COPD Severity
Among patients classified as COPD based on FEV1/FVC of < 0.7, subgroup analysis was performed according to the severity of airflow obstruction using the GOLD grading system. Patients were categorized into mild COPD (GOLD 1; FEV1 ≥ 80% predicted) and moderate-to-severe COPD (GOLD 2–4; FEV1 < 80% predicted). The characteristics of young and old COPD patients, stratified by severity, are described in Supplementary Table 4. In the mild COPD subgroup, young COPD patients exhibited smaller mean FEV1 (L) and FVC (L) decline rates compared with older COPD patients, consistent with previously observed lung function trajectories (Supplementary Figure 3). However, in the moderate-to-severe COPD subgroup, there were no statistically significant differences in lung function changes between young and old COPD patients.
Normalization of Airflow Obstruction
In the linear mixed model analysis of annual lung function change, young COPD patients showed a tendency toward a mean FEV1/FVC ratio improvement. As shown in Figure 2A, young COPD patients demonstrated a significantly higher cumulative probability of airflow obstruction normalization compared with old COPD patients (p < 0.001).
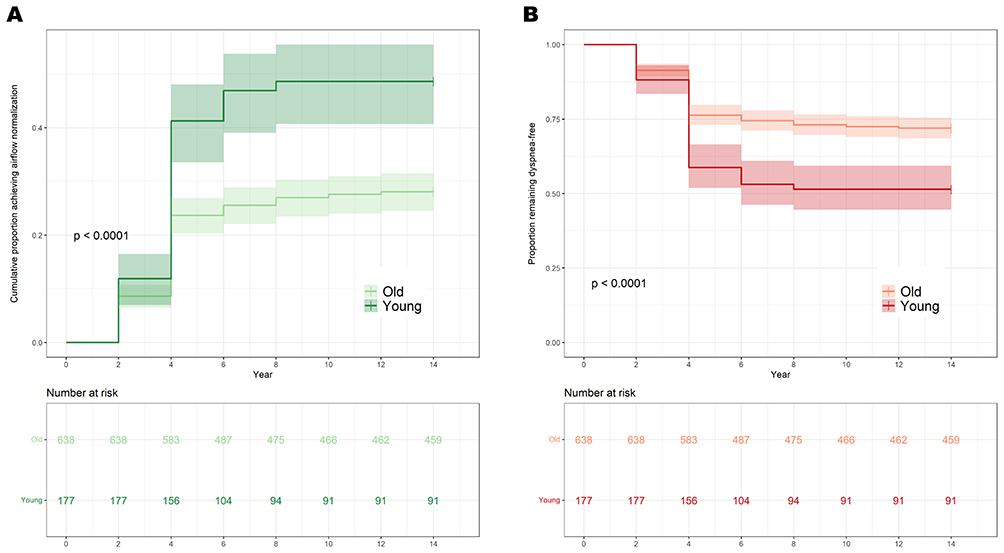 |
Figure 2 (A) Cumulative incidence of airflow obstruction normalization in young and old COPD. (B) Kaplan–Meier curve for the time to first dyspnea in young and old COPD. |
In the univariate Cox analysis, young COPD, female sex, and a higher FEV1% predicted value were associated with a shorter time for normalization of airflow obstruction (Table 2). Conversely, being a current smoker delayed the normalization of airflow obstruction. Younger age, female sex, and a higher FEV1% predicted value were found to be independent predictors of earlier normalization of airflow obstruction after adjusting for confounding factors.
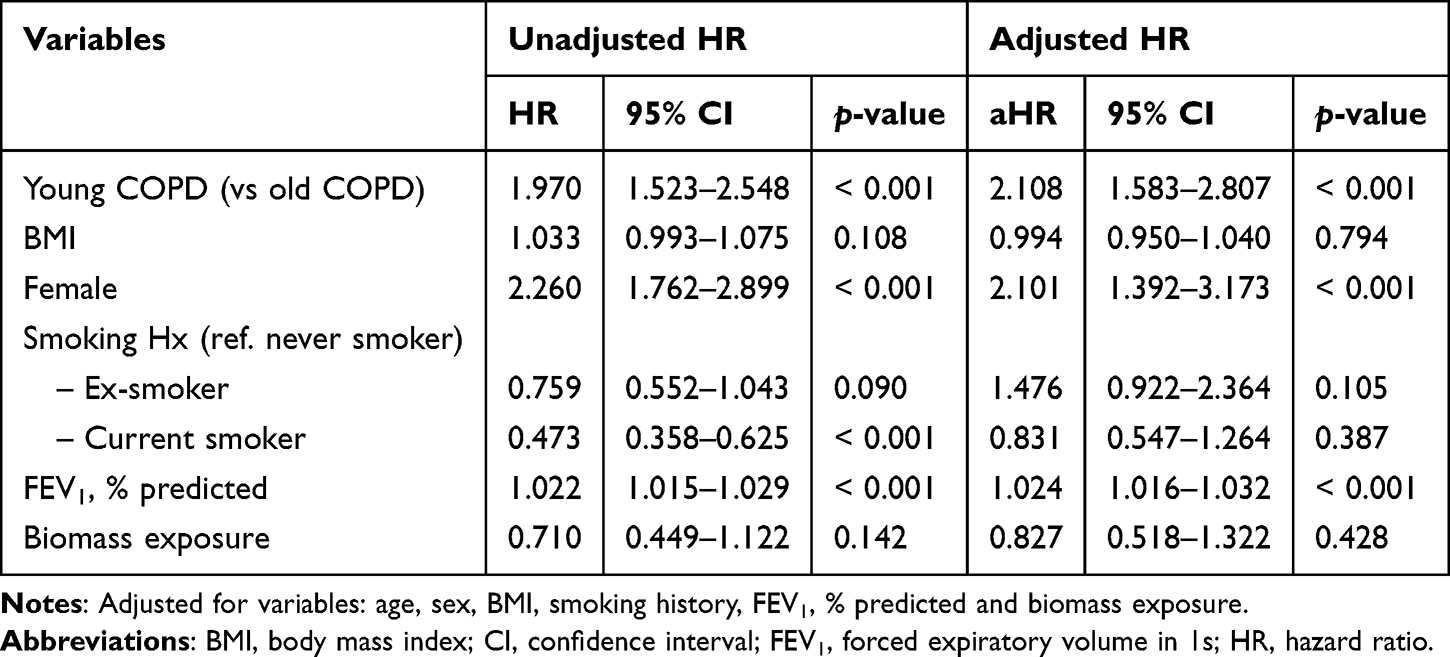 |
Table 2 Univariate and Multivariate Cox Regression Analysis for Time-to-First Normalized Obstruction |
Time to First Dyspnea
Figure 2B presents the Kaplan–Meier curve comparing the time to first dyspnea between young and old COPD patients, which was significantly longer in young COPD compared to old COPD patients (p < 0.0047). In the univariate analysis, young COPD patients and those with a higher baseline FEV1% predicted value exhibited a longer time to first dyspnea (Table 3). The multivariate analysis identified younger age and a higher baseline FEV1% predicted value as independent predictors for a longer time to first dyspnea.
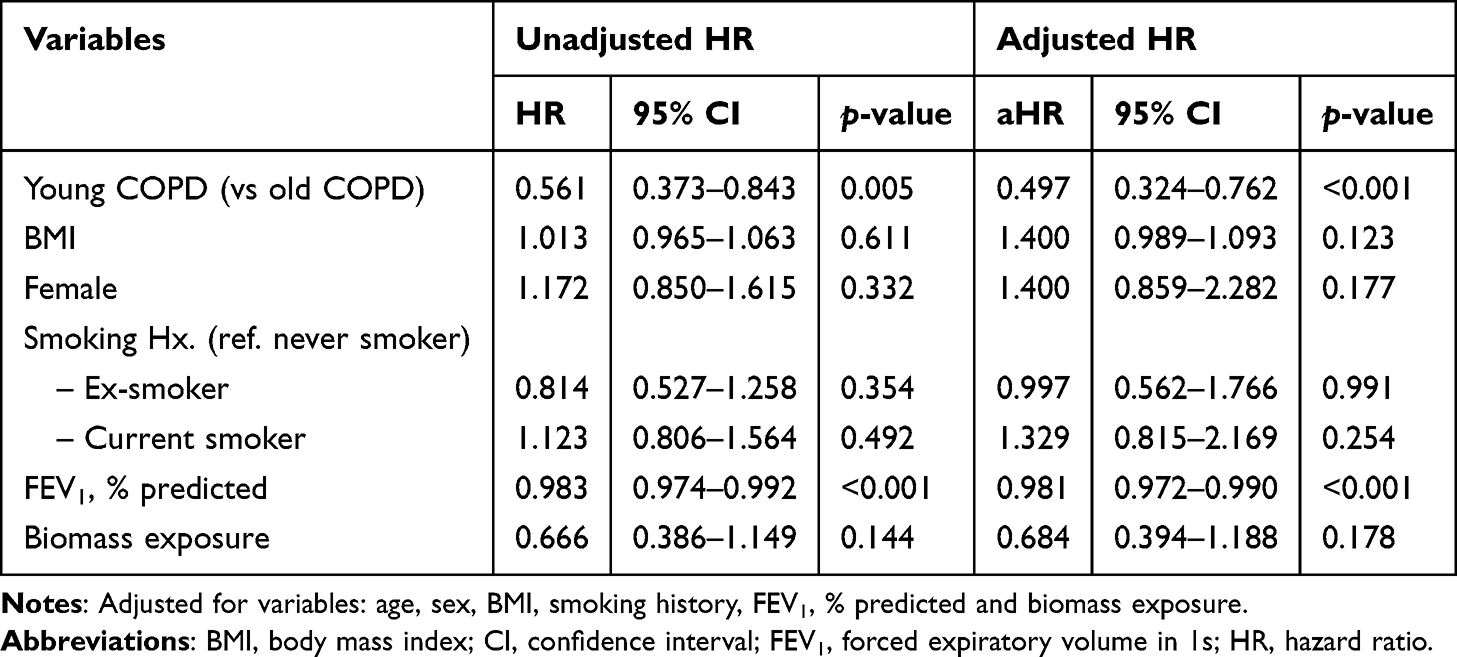 |
Table 3 Univariate and Multivariate Cox Regression Analysis for Time-to-First Dyspnea |
Discussion
This study, conducted over a 12-year period on a prospective community-based cohort aged 40–69 years, investigated the clinical characteristics and lung function trajectories of young COPD patients. Regardless of the diagnostic criteria, ie., a FEV1/FVC ratio < 0.7 or < LLN, the young COPD group consistently exhibited a higher proportion of females and individuals who had never smoked, along with a higher BMI and fewer symptoms of dyspnea, compared to the old COPD group. Notably, fewer old COPD patients met the spirometric criteria for COPD when using the LLN compared to the fixed ratio. Conversely, in the young COPD group, fewer patients fulfilled the spirometric criteria for COPD when using the fixed ratio versus the LLN criterion. When comparing lung function trajectories over 12 years, old COPD showed a faster FEV1 decline, while young COPD exhibited a + 0.66/y increase in FEV1/FVC ratio and a + 71.0 mL/y rise in FEF25–75%(L). In the subgroup analysis based on COPD severity, these lung function trajectories were observed only in mild COPD, while no significant differences in annual lung function changes were found between young and old COPD in the moderate-to-severe group. Multivariate Cox analysis revealed that young COPD was an independent predictor of a higher probability of airflow obstruction normalization and a longer time to first dyspnea.
A study of three longitudinal cohorts demonstrated that the pathogenesis of COPD involves diverse lung function trajectories, primarily driven by accelerated lung function decline with aging and lower peak lung function.14 These mechanisms are not mutually exclusive, and individuals within a population-based cohort may exhibit varying combinations of these patterns.11,35 Young COPD patients, closer to the 20–25 age range when lung function peaks, may have lower peak lung function than the overall COPD population. An ongoing birth cohort study using linear mixed-effects analysis of the FEV1/FVC ratio has demonstrated that individuals with a consistently low lung function trajectory were at an increased risk for COPD later in life, even without rapid lung function decline.36 In the European Community Respiratory Health Survey, involving 4,636 adults aged 20–44 years, airway hyper-responsiveness, a family history of asthma, and childhood respiratory infections were identified as risk factors for young COPD, with cigarette smoking, sex, age, and BMI being risk factors shared with old COPD.16 In a contemporary Danish population-based cohort of 105,630 individuals, young COPD patients (aged < 50 years) diagnosed using the LLN criterion demonstrated higher tobacco consumption, a higher likelihood of asthma treatment, and more episodes of bronchitis/pneumonia compared to individuals without COPD.37
Recent studies indicate that young COPD is linked to structural and functional abnormalities, such as dysanapsis,38 and is often associated with a family history of respiratory diseases or early life respiratory events before age 5.39 The association of dysanapsis with baseline airflow obstruction and the risk of incident COPD is not influenced by age, sex, or height.40 In this study, the young COPD group had higher proportions of females and individuals who never smoked, along with a higher BMI, compared to the old COPD group. These findings suggest that patients with these characteristics may represent a subgroup with dysanapsis that differs significantly from the commonly recognized features of COPD.
Limited research on mild and young COPD is mainly due to few individuals experience respiratory symptoms severe enough to necessitate a hospital visit. In this study, using a fixed ratio to define COPD, FEV1(%) in young COPD patients was found to be lower than that in older COPD patients, but the proportion of individuals experiencing dyspnea was significantly lower in the young COPD group. Identifying young adults with early COPD who do not exhibit respiratory symptoms, and implementing preventive measures before the disease progresses, can improve long-term health outcomes.41 Based on this concept, an international group has published an operational definition for COPD diagnosis in young adults using the LLN.33
In a study directly comparing fixed ratio criteria with four LLN criteria, the use of all LLN-based criteria resulted in a greater number of individuals with airflow limitation at a younger age and fewer individuals at an older age compared to the fixed ratio criteria.42 In this study, using LLN criteria increased the prevalence of COPD from 3.6% to 6.9% in young COPD compared to using a fixed ratio, while conversely, it decreased from 13.5% to 10.2% for old COPD. Additionally, when the fixed ratio was used, FEV1(%) in old COPD patients was significantly higher than that in young COPD patients; however, when using the LLN criteria, there was no statistically significant difference in FEV1(%) between the two groups. These findings were consistent with previous cross-sectional studies indicating that the use of the fixed ratio in younger ages may lead to underestimation of early COPD.43–45 These findings suggest LLN use in younger populations may overestimation of COPD but aid surveillance.46 Conversely, the fixed ratio criteria may be superior for surveillance purposes in older populations. Clinically, the higher prevalence of young COPD identified using LLN criteria suggests improved detection of early airflow limitation in younger individuals who may be under-recognized by fixed ratio–based definitions.47 This supports the use of LLN-based criteria for earlier identification of potentially reversible disease in younger populations.
A recent study from the ECLIPSE cohort comparing young and old COPD patients found that the proportion of those experiencing substantial FEV1 decline tended to be higher in young COPD patients, whereas modest decline was more common in older COPD patients. Although the difference was not statistically significant, the proportion of patients showing improvement was higher in young COPD patients than in older ones.48 Our community-based cohort study, conducted over a 12-year period, found that the annual rate of FEV1 decline was slower in young COPD patients than in old COPD patients. Moreover, young COPD patients exhibited an increased FEF25–75% and FEV1/FVC ratio over the 12-year follow-up, in contrast with old COPD patients. Notably, this difference was only significant in patients with mild COPD, while no significant changes were observed in those with moderate-to-severe COPD. Improvements in lung function have been observed in younger COPD patients, with a subset even achieving normalized obstruction. This finding challenges the traditional definition of “irreversible obstruction” in COPD. Analysis of the KOCOSS cohort revealed that a subset of patients exhibited normalized ratios during longitudinal follow-up. These patients tended to be younger, had higher BMIs, were less likely to be smokers, and exhibited a slower lung function decline compared to those with persistently fixed ratios.49 However, no differences in exacerbation rates were observed. Our results also indicated that younger patients were more likely to show normalized obstruction over time. These findings suggest that age-related differences in lung plasticity and repair capacity may play a key role in COPD progression. Aging reduces lung tissue repair and regenerative capacity, making COPD more irreversible, whereas younger individuals may have greater lung plasticity, enhancing reversibility and airflow obstruction normalization.50
Following the observation in our study that both FEF25–75% and the FEV1/FVC ratio eventually recovered in young COPD patients, we conducted a multivariate Cox analysis demonstrating that young COPD was independently associated with normalized airflow obstruction. Moreover, time to first dyspnea was significantly longer in young COPD patients. Overall, these findings suggested that young COPD patients were more likely to experience less profound lung function decline than old COPD patients, which might relate to the normalization of airflow obstruction, and may take longer to perceive dyspnea. This could result in less frequent use of healthcare systems for COPD treatment due to low awareness of respiratory symptoms. Recent studies have focused on the early diagnosis and management of COPD, aiming to normalize airflow obstruction.8,51 A study using the Doetinchem Cohort Study data revealed three lung function trajectories in adults aged 20–59 years, demonstrating that baseline smokers who quit during follow-up experienced a slower FEV1 decline.52 Thus, young adults with risk factors for low peak lung function, such as a history of premature or childhood respiratory infections as well as traditional COPD risk factors, including smoking, should undergo COPD screening using the LLN criteria even in the absence of symptoms.53
Our findings also suggest potential strategies for early screening of young COPD. Young COPD patients in our cohort were more often female, never-smokers, and had higher BMI, which may contribute to underdiagnosis when screening relies mainly on smoking history. Recent evidence indicates sex-specific associations between extrapulmonary factors and reduced lung function in young adults, supporting the role of complementary risk profiling.54 Targeted spirometry using LLN-based criteria in individuals with these risk characteristics may enable earlier detection and intervention, particularly given the greater potential for airflow normalization observed in younger patients.
The main strengths of our study were the prospective design, inclusion of a large population, and incorporation of serial spirometry results over a 12-year follow-up period. However, the study had limitations. First, it was conducted among individuals aged 40–69 years, while excluding individuals aged < 40 years from the young COPD group and those aged ≥ 70 years from the old COPD group. Therefore, there may be differences in prevalence rates compared to previous studies that typically defined young COPD patients as 20–50 years of age. Second, pre-bronchodilator rather than post-bronchodilator spirometry was used to define COPD, potentially resulting in the inclusion of individuals with reversible airflow limitation, such as those with asthma. However, since serial pre-bronchodilator FEV1 measurements are generally sufficient for comparing the impact of different interventions on the annual rate of FEV1 change, many studies have used pre-bronchodilator values instead of post-bronchodilator values to assess COPD patients in longitudinal outcome analyses.55–58 Third, due to the lack of relevant information, it was not possible to compare the risk factors of respiratory disease family history or early life events between the groups, where these factors have been identified in several studies on young COPD. Fourth, the use of percent of predicted values instead of z-scores may introduce anthropometric biases. Future studies should consider z-scores for more standardized lung function assessment. Fifth, smoking cessation status could not be incorporated as a time-varying factor during follow-up, limiting assessment of its dynamic impact on lung function decline. Sixth, the relatively small number of young COPD patients resulted in wider confidence intervals, which may limit the precision of effect estimates and warrants cautious interpretation of the findings. Furthermore, detailed information on pharmacological treatment during follow-up was not available, precluding evaluation of potential differences in treatment strategies between young and old COPD groups and their influence on lung function trajectories. In addition, information on structural lung changes assessed by computed tomography was not available in this cohort, precluding comparison of radiologic phenotypes between young and old COPD groups. Furthermore, α1-antitrypsin deficiency was not evaluated, as its prevalence is known to be extremely low in Asian populations and related data were not collected in the cohort. Finally, as the study recruited a local cohort from a specific area of South Korea, the subjects may not represent the entire population. Therefore, further studies including different ethnic groups are needed.
Conclusion
Distinct from old COPD group, the young COPD group was characterized by a higher proportion of females and individuals who had never smoked, along with fewer complaints of dyspnea. COPD could potentially be underdiagnosed when using the fixed ratio criteria, particularly among young individuals having a slower lung function decline compared to older age groups. Since normalized airflow obstruction is an independent predictor of COPD, early screening, diagnosis, and management of these individuals could lead to improved prognosis.
Ethical Declaration
The Ethics Committee of Incheon St. Mary’s Hospital approved the study protocol (IRB No. OC23ZISI0033) and waived the requirement for informed consent due to the retrospective nature of the study. All data were anonymized to ensure patient confidentiality. This study was conducted in accordance with the Declaration of Helsinki.
Acknowledgment
This study was conducted with bioresources from National Biobank of Korea, The Korea Disease Control and Prevention Agency, Republic of Korea (KBN-2023-005).
Funding
There is no funding to report.
Disclosure
Dr Sang Kim reports personal fees from AstraZeneca, Daewon, Handok, Hallym, grants from Korea University Guro Hospital and Korean Academy of Tuberculosis and Respiratory Diseases, outside the submitted work. The other authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper. The abstract of this paper was presented at the European Respiratory Society Congress 2025 as an oral presentation with interim findings. The abstract was published in “Conference Abstracts” in European Respiratory Journal: https://doi.org/10.1183/13993003.congress-2025.OA6434
References
1. Vogelmeier CF, Criner GJ, Martinez FJ, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report. GOLD executive summary. Am J Respir Crit Care Med. 2017;195(5):557–12. doi:10.1164/rccm.201701-0218PP
2. Rehman AU, Hassali MAA, Muhammad SA, Harun SN, Shah S, Abbas S. The economic burden of chronic obstructive pulmonary disease (COPD) in Europe: results from a systematic review of the literature. Eur J Health Econ. 2020;21:181–194. doi:10.1007/s10198-019-01119-1
3. Guarascio AJ, Ray SM, Finch CK, Self TH. The clinical and economic burden of chronic obstructive pulmonary disease in the USA. Clinicoecon Outcomes Res. 2013;5:235–245. doi:10.2147/CEOR.S34321
4. Welte T, Vogelmeier C, Papi A. COPD: early diagnosis and treatment to slow disease progression. Int J Clin Pract. 2015;69(3):336–349. doi:10.1111/ijcp.12522
5. Laucho-Contreras ME, Cohen-Todd M. Early diagnosis of COPD: myth or a true perspective. Eur Respir Rev. 2020;29(158):200131. doi:10.1183/16000617.0131-2020
6. Afonso AS, Verhamme KM, Sturkenboom MC, Brusselle GG. COPD in the general population: prevalence, incidence and survival. Respir Med. 2011;105(12):1872–1884. doi:10.1016/j.rmed.2011.06.012
7. Sanchez-Salcedo P, Divo M, Casanova C, et al. Disease progression in young patients with COPD: rethinking the Fletcher and Peto model. Eur Respir J. 2014;44(2):324–331. doi:10.1183/09031936.00208613
8. Martinez FJ, Agusti A, Celli BR, et al. Treatment trials in young patients with chronic obstructive pulmonary disease and pre–chronic obstructive pulmonary disease patients: time to move forward. Am J Respir Crit Care Med. 2022;205(3):275–287. doi:10.1164/rccm.202107-1663SO
9. Kohansal R, Martinez-Camblor P, Agustí A, Buist AS, Mannino DM, Soriano JB. The natural history of chronic airflow obstruction revisited: an analysis of the Framingham offspring cohort. Am J Respir Crit Care Med. 2009;180(1):3–10. doi:10.1164/rccm.200901-0047OC
10. Papi A, Beghé B, Fabbri LM. Rate of decline of FEV1 as a biomarker of survival? Am J Respir Crit Care Med. 2021;203:663–665. doi:10.1164/rccm.202010-3784ED
11. Ross JC, Castaldi PJ, Cho MH, et al. Longitudinal modeling of lung function trajectories in smokers with and without chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2018;198(8):1033–1042. doi:10.1164/rccm.201707-1405OC
12. Agustí A, Melén E, DeMeo DL, Breyer-Kohansal R, Faner R. Pathogenesis of chronic obstructive pulmonary disease: understanding the contributions of gene–environment interactions across the lifespan. Lancet Respir Med. 2022;10(5):512–524. doi:10.1016/S2213-2600(21)00555-5
13. Cerveri I, Corsico AG, Grosso A, et al. The rapid FEV1 decline in chronic obstructive pulmonary disease is associated with predominant emphysema: a longitudinal study. COPD. 2013;10(1):55–61. doi:10.3109/15412555.2012.727920
14. Lange P, Celli B, Agustí A, et al. Lung-function trajectories leading to chronic obstructive pulmonary disease. N Engl J Med. 2015;373(2):111–122. doi:10.1056/NEJMoa1411532
15. Lamprecht B, McBurnie MA, Vollmer WM, et al. COPD in never smokers: results from the population-based burden of obstructive lung disease study. Chest. 2011;139(4):752–763. doi:10.1378/chest.10-1253
16. De Marco R, Accordini S, Marcon A, et al. Risk factors for chronic obstructive pulmonary disease in a European cohort of young adults. Am J Respir Crit Care Med. 2011;183(7):891–897. doi:10.1164/rccm.201007-1125OC
17. Svanes C, Sunyer J, Plana E, et al. Early life origins of chronic obstructive pulmonary disease. Thorax. 2010;65(1):14–20. doi:10.1136/thx.2008.112136
18. Qin C, Gao J, Sang X, Liu M, Liu J. Childhood respiratory risk profiles associate with lung function and COPD among the old population. Ann Med. 2025;57(1):2470954. doi:10.1080/07853890.2025.2470954
19. Yang A, Bon J. Unraveling dysanapsis: genetic insights into airway lung mismatch and COPD. Am J Respir Crit Care Med. 2024;210:1391–1392. doi:10.1164/rccm.202406-1256ED
20. Wang Z, Li Y, Lin J, et al. Prevalence, risk factors, and mortality of COPD in young people in the USA: results from a population-based retrospective cohort. BMJ Open Respir Res. 2023;10(1):e001550. doi:10.1136/bmjresp-2022-001550
21. Tan L, Li Y, Wang Z, et al. Comprehensive appraisal of lung function in young COPD patients: a single center observational study. BMC Pulm Med. 2024;24(1):358. doi:10.1186/s12890-024-03165-9
22. Marcus BS, McAvay G, Gill TM, Vaz Fragoso CA. Respiratory symptoms, spirometric respiratory impairment, and respiratory disease in middle‐aged and older persons. J Am Geriatr Soc. 2015;63(2):251–257. doi:10.1111/jgs.13242
23. Postma DS, Bush A, van den Berge M. Risk factors and early origins of chronic obstructive pulmonary disease. Lancet. 2015;385(9971):899–909. doi:10.1016/S0140-6736(14)60446-3
24. Çolak Y, Afzal S, Nordestgaard BG, Vestbo J, Lange P. Young and middle-aged adults with airflow limitation according to lower limit of normal but not fixed ratio have high morbidity and poor survival: a population-based prospective cohort study. Eur Respir J. 2018;51(3):1702681. doi:10.1183/13993003.02681-2017
25. Cosío BG, Casanova C, Soler-Cataluña JJ, et al. Unravelling young COPD and pre-COPD in the general population. ERJ Open Res. 2023;9(1):00334–2022. doi:10.1183/23120541.00334-2022
26. Kim Y, Han B-G, Group K. Cohort profile: the Korean genome and epidemiology study (KoGES) consortium. Int J Epidemiol. 2017;46(2):e20. doi:10.1093/ije/dyv316
27. Ferré A, Fuhrman C, Zureik M, et al. Chronic bronchitis in the general population: influence of age, gender and socio-economic conditions. Respir Med. 2012;106(3):467–471. doi:10.1016/j.rmed.2011.12.002
28. de Oca MM, Halbert RJ, Lopez MV, et al. The chronic bronchitis phenotype in subjects with and without COPD: the PLATINO study. Eur Respir J. 2012;40(1):28–36. doi:10.1183/09031936.00141611
29. Miller MR, Hankinson J, Brusasco V, et al. Standardisation of spirometry. Eur Respir J. 2005;26(2):319–338. doi:10.1183/09031936.05.00034805
30. American Thoracic Society. Standardization of spirometry, 1994 update. Am J Respir Crit Care Med. 1995;152(3):1107–1136. doi:10.1164/ajrccm.152.3.7663792
31. Celli BR, MacNee W, Agusti A, et al. Standards for the diagnosis and treatment of patients with COPD: a summary of the ATS/ERS position paper. Eur Respir J. 2004;23(6):932–946. doi:10.1183/09031936.04.00014304
32. Colak Y, Afzal S, Nordestgaard BG, Lange P, Vestbo J. Importance of early COPD in young adults for development of clinical COPD. Findings from the Copenhagen General Population Study. Am J Respir Crit Care Med. 2021;203(10):1245–1256. doi:10.1164/rccm.202003-0532OC
33. Martinez FJ, Han MK, Allinson JP, et al. At the root: defining and halting progression of early chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2018;197(12):1540–1551. doi:10.1164/rccm.201710-2028PP
34. Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977;33:159–174. doi:10.2307/2529310
35. Bui DS, Lodge CJ, Burgess JA, et al. Childhood predictors of lung function trajectories and future COPD risk: a prospective cohort study from the first to the sixth decade of life. Lancet Respir Med. 2018;6(7):535–544. doi:10.1016/S2213-2600(18)30100-0
36. Berry CE, Billheimer D, Jenkins IC, et al. A distinct low lung function trajectory from childhood to the fourth decade of life. Am J Respir Crit Care Med. 2016;194(5):607–612. doi:10.1164/rccm.201604-0753OC
37. Çolak Y, Afzal S, Nordestgaard BG, Vestbo J, Lange P. Prevalence, characteristics, and prognosis of early chronic obstructive pulmonary disease. The Copenhagen General Population Study. Am J Respir Crit Care Med. 2020;201(6):671–680. doi:10.1164/rccm.201908-1644OC
38. McGinn EA, Mandell EW, Smith BJ, Duke JW, Bush A, Abman SH. Dysanapsis as a determinant of lung function in development and disease. Am J Respir Crit Care Med. 2023;208(9):956–963. doi:10.1164/rccm.202306-1120PP
39. Cosío BG, Pascual-Guardia S, Borras-Santos A, et al. Phenotypic characterisation of early COPD: a prospective case–control study. ERJ Open Res. 2020;6(4):00047–2020. doi:10.1183/23120541.00047-2020
40. Smith BM, Kirby M, Hoffman EA, et al. Association of dysanapsis with chronic obstructive pulmonary disease among older adults. JAMA. 2020;323(22):2268–2280. doi:10.1001/jama.2020.6918
41. Soriano JB, Polverino F, Cosio BG. What is early COPD and why is it important? Eur Respir J. 2018;52(6):1801448. doi:10.1183/13993003.01448-2018
42. Çolak Y, Nordestgaard BG, Vestbo J, Lange P, Afzal S. Comparison of five major airflow limitation criteria to identify high-risk individuals with COPD: a contemporary population-based cohort. Thorax. 2020;75(11):944–954. doi:10.1136/thoraxjnl-2020-214559
43. Liu S, Zhou Y, Liu S, et al. Clinical impact of the lower limit of normal of FEV1/FVC on detecting chronic obstructive pulmonary disease: a follow-up study based on cross-sectional data. Respir Med. 2018;139:27–33. doi:10.1016/j.rmed.2018.04.011
44. Hoesein FAM, Zanen P, Lammers J-WJ. Lower limit of normal or FEV1/FVC< 0.70 in diagnosing COPD: an evidence-based review. Respir Med. 2011;105(6):907–915. doi:10.1016/j.rmed.2011.01.008
45. Çolak Y, Løkke A, Marott JL, Lange P, Vestbo J. Impact of diagnostic criteria on the prevalence of COPD. Clinical Respir J. 2013;7(3):297–303. doi:10.1111/crj.12007
46. Jo YS, Kim KJ, Rhee CK, Yoo KH, Jung K-S, Park Y-B. Prevalence, characteristics, and risk of exacerbation in young patients with chronic obstructive pulmonary disease. Respir Res. 2022;23(1):212. doi:10.1186/s12931-022-02144-0
47. Hwang YI, Kim CH, Kang H-R, et al. Comparison of the prevalence of chronic obstructive pulmonary disease diagnosed by lower limit of normal and fixed ratio criteria. J Korean Med Sci. 2009;24(4):621–626. doi:10.3346/jkms.2009.24.4.621
48. Vila M, Agustí A, Vestbo J, et al. Contrasting the clinical and biological characteristics of young and old COPD patients. ERJ Open Res. 2025;11(1):00671–2024. doi:10.1183/23120541.00671-2024
49. Kim YS, Hwang YI, Lee JH, et al. Clinical significance of normalized airflow obstruction in patients with chronic obstructive pulmonary disease. Respir Med. 2023;218:107398. doi:10.1016/j.rmed.2023.107398
50. Brandsma C-A, de Vries M, Costa R, Woldhuis RR, Königshoff M, Timens W. Lung ageing and COPD: is there a role for ageing in abnormal tissue repair? Eur Respir Rev. 2017;26(146):170073. doi:10.1183/16000617.0073-2017
51. Fazleen A, Wilkinson T. Early COPD: current evidence for diagnosis and management. Therap Adv Respir Dis. 2020;14:1753466620942128. doi:10.1177/1753466620942128
52. van Oostrom SH, Engelfriet PM, Verschuren WM, et al. Aging-related trajectories of lung function in the general population—The Doetinchem Cohort Study. PLoS One. 2018;13(5):e0197250. doi:10.1371/journal.pone.0197250
53. Lyngsø AM, Backer V, Gottlieb V, Nybo B, Østergaard MS, Frølich A. Early detection of COPD in primary care-The Copenhagen COPD Screening Project. BMC Public Health. 2010;10:1–7. doi:10.1186/1471-2458-10-524
54. Doi K, Hirano T, Oishi K, et al. Gender difference in the relationship between extrapulmonary factors and reduced lung function in early adulthood. J Clin Med. 2024;13(6):1769. doi:10.3390/jcm13061769
55. Tashkin DP, Wang H-J, Halpin D, et al. Comparison of the variability of the annual rates of change in FEV 1 determined from serial measurements of the pre-versus post-bronchodilator FEV 1 over 5 years in mild to moderate COPD: results of the lung health study. Respir Res. 2012;13:1–10. doi:10.1186/1465-9921-13-1
56. Buhr RG, Barjaktarevic IZ, Quibrera PM, et al. Reversible airflow obstruction predicts future chronic obstructive pulmonary disease development in the SPIROMICS cohort: an observational cohort study. Am J Respir Crit Care Med. 2022;206(5):554–562. doi:10.1164/rccm.202201-0094OC
57. Martinez FJ, Han MK, Lopez C, et al. Discriminative accuracy of the CAPTURE tool for identifying chronic obstructive pulmonary disease in US primary care settings. JAMA. 2023;329(6):490–501. doi:10.1001/jama.2023.0128
58. Kronborg T, Hangaard S, Cichosz SL, Hejlesen O. Increased accuracy after adjustment of spirometry threshold for diagnosing COPD based on pre-bronchodilator FEV1/FVC. Respir care. 2019;64(1):85–90. doi:10.4187/respcare.06148
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Long-Term Study of Adverse Outcomes Associated With Oral Corticosteroid Use in COPD

Tse G, Emmanuel B, Ariti C, Bafadhel M, Papi A, Carter V, Zhou J, Skinner D, Xu X, Müllerová H, Price D
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:2565-2580
Published Date: 15 November 2023
Prevalence and Risk Factors of Chronic Obstructive Pulmonary Disease Among Users of Primary Health Care Facilities in Morocco
Al wachami N, Arraji M, Iderdar Y, Mourajid Y, Boumendil K, Bouchachi FZ, Jaouhar S, Guennouni M, Laamiri F, Elkhoudri N, Bandadi L, Louerdi ML, Hilali A, Chahboune M
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:375-387
Published Date: 5 February 2024
Association Between Advanced Lung Cancer Inflammation Index and Mortality in US Adults with Chronic Obstructive Pulmonary Disease
Su X, Rao H, Zhao C, Zhang X, Li D
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:2481-2492
Published Date: 18 July 2025
Risk of Hospitalized Cardiovascular Events Associated with LAMA/LABA/ICS FDC versus LABA/ICS FDC in Patients with Chronic Obstructive Pulmonary Disease: A Nationwide Cohort Study
Sun SH, Lu MJH, Chen CY, Tsai NH, Pan SW, Dong YH
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:3765-3777
Published Date: 20 November 2025
Reliability of Pulmonary Function Tests in Patients with Chronic Obstructive Pulmonary Disease
Arslan F, Şen E, Şirin B, Köktürk N, Ulubay G, Aydogan Eroglu S, Gemicioglu B, Sönmez Ö, Şerifoğlu İ, Dilektasli AG, Öztürk Şahin B, Doğan İ, Gürhan N, Günen H, Ensen N
International Journal of Chronic Obstructive Pulmonary Disease 2026, 21:554115
Published Date: 21 January 2026