Back to Journals » Advances in Medical Education and Practice » Volume 11
Evaluation of Awareness, Knowledge, and Attitudes Towards Basic Life Support Among Non-Medical Students at Two Academic Institutions in Jeddah, Saudi Arabia
Authors Alnajjar H, Hilal RM, Alharbi AJ, Alharthi OH, Batwie RA, AlShehri RM, Algethami MR ![]()
Received 20 July 2020
Accepted for publication 17 November 2020
Published 23 December 2020 Volume 2020:11 Pages 1015—1021
DOI https://doi.org/10.2147/AMEP.S271130
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Hani Alnajjar,1 Rawan Mostafa Hilal,2 Arwa Jabir Alharbi,2 Omimah Hasan Alharthi,2 Raghad Ateeg Batwie,2 Raghad Mohammed AlShehri,2 Mohammed R Algethami3
1Department of Anesthesia, University of Jeddah, Jeddah, Saudi Arabia; 2Medical College, King Abdulaziz University, Jeddah, Saudi Arabia; 3Preventive Medicine Resident, Joint Program, Ministry of Health, Jeddah, Saudi Arabia
Correspondence: Rawan Mostafa Hilal
Medical School, King Abdulaziz University, P.O.Box: 3575, Alsharqiah 32654, Jeddah, Saudi Arabia
Tel +966599888471
Email [email protected]
Background: Cardiac arrests are a leading cause of mortality in Saudi Arabia. Prompt and quick intervention using early cardiopulmonary resuscitation (CPR) can be a life-saving strategy. Sufficient knowledge and awareness regarding CPR are important in initial care, particularly during an out-of-hospital cardiac arrest. We aim to assess the knowledge, awareness, and attitude toward CPR among the students of King Abdulaziz University and Jeddah University.
Materials and Methods: A descriptive, cross-sectional study design with a sample of 1053 non-medical students, regardless of their academic year, was conducted from May to July 2019 at both universities. Data were analyzed through chi-square and analysis of variance where a P-value < 0.05 was considered statistically significant.
Results: Out of 1053 students, 28.7% received CPR training. Also, the majority of the subjects were female 71%. The science department provided the largest response. Results showed that chest pain was the most observed early sign of cardiac arrest among participants by a percentage of 84.6. Majority of the participants (90.9%) felt no hesitation in performing early CPR on a family member. Additionally, committing a mistake was the most feared factor that deterred students from performing CPR.
Conclusion: Knowledge and awareness of CPR among non-medical university students were poor, despite positive attitudes toward it. Integrating mandatory CPR courses in the orientation and in the first year of the undergraduate curriculum could increase awareness and improve the outcomes of out-of-hospital cardiac arrest (OHCA).
Keywords: basic life support, cardiopulmonary resuscitation, cardiopulmonary resuscitation training, out-of-hospital cardiac arrest, cardiac arrest
Introduction
Cardiopulmonary Resuscitation (CPR) is an emergency procedure that is used in cases of cardiac arrest, delaying CPR can increase mortality and morbidity rates.1 This procedure comprises two major components: chest compressions and rescue breaths by means of artificial ventilation to maintain circulation and send oxygen to the organs.2 Adequate knowledge and quality of CPR application can contribute to better outcomes in cases of cardiac arrest.2 This is because the time between recognizing a cardiac arrest and the arrival of emergency medical services (EMS) can be lengthy up to 8 minutes in some districts.3 Despite major technological advancements such as automated external defibrillators (AEDs), striking disparities remain in survival rates between those experiencing in-hospital and out-of-hospital cardiac arrests (OHCAs).4
In the United States, OHCAs account more than 450,000 deaths annually.5 In Saudi Arabia, a prevalence of sudden cardiac arrests (SCAs) number was 7.76 out of 1000 hospital admissions at King Abdulaziz University hospital in 2016.6 We have no available data for OHCAs in Jeddah.
Public awareness of proper CPR application is crucial and a life-saving step that can be controlled.7 Nevertheless, people tend to make presumptions that CPR ought to be performed by certified medical personnel only.7 Accordingly, it is necessary to estimate the society on their knowledge, awareness, and attitude toward BLS so that appropriate interventions could be implemented much more readily than a medical expert who might not be available.7 Moreover, a university hospital in Oman found that patients who suffered sudden cardiac arrest were transported to the hospital by family or friends without even providing CPR.8 A study conducted in Vienna in 2018 found poor BLS and AED knowledge and awareness among individuals.9 In Oman, despite the variety in their socio-demographic characteristics, the level of knowledge towards BLS was quite low.10 In Riyadh, Saudi Arabia, a study appraising knowledge and attitude towards BLS among university personnel and students found that more than 50% of university personnel and students had inadequate information regarding BLS.11 This lack of knowledge has contributed to an inability to perform CPR in many situations when it is sorely needed.12 In government schools in Riyadh, 77% of the students expressed a need for BLS training and 78.5% supported mandatory BLS training.11 Poor CPR knowledge and applications extend to university students; it was found that 87.9% of health students had very poor knowledge scores in BLS.11
Studies assessing knowledge, attitude, and awareness toward BLS in the middle east, including Saudi Arabia are lacking. In our study, we intended to estimate the awareness, depth of knowledge, and attitude toward non-medical students. Non-medical students are more in quantity than medical, additionally lacking trusted sources accessibility that can lead to mistaken information regarding CPR, especially some colleges, did not obligate CPR practices in the studying courses.
Materials and Methods
We conducted a cross-sectional study at King Abdulaziz University and Jeddah University, both in Jeddah, Saudi Arabia, from May to July 2019. We sought to estimate undergraduate students’ knowledge, awareness, and attitudes towards BLS.
We used random sampling method. Out of 82,156 King Abdulaziz University students, we excluded 27,000 postgraduate students and medical field specializing in medicine, nursing, pharmacy, dentistry, or applied medical science as they receive mandatory BLS training. To end up with 55,156 students, a total of 1053 students participated in the study. We included undergraduate university students, at least 18 years old and able to read written Arabic language. The non-medical field includes different university departments such as Science, Engineering, Economics and Administration, Arts and Humanities, Computing and Information technology. Besides, to the preparation year.
We distributed the questionnaire via web address and sent it through university emails and social media for public advertisement. Informed consent was obtained before filling the questionnaire. All data were collected electronically.
This questionnaire was created using the Google Forms web application. The information of the questionnaire was derived from the American Heart Association and adhered to its latest guidelines.13 A translated validated Arabic and English version of the questionnaire provided by a study handled in Jordan10 (see the supplementary material).
The final self-administered questionnaire comprised seven demographic data questions (related to sex, age, university college year, grade point average [GPA], university name, studying specialty and relationship status), and 22 multiple-choice questions assessing knowledge about skills and attitudes towards BLS. We evaluate participants’ knowledge on the following parameters: level of consciousness, respiratory signs, and cardiocirculatory evidence (Table 1). In addition to the clinical features of cardiac arrests, such as chest pain, breathing difficulties, cyanosis extra (Table 2). Also asked about the application of chest compressions (rate, location, depth and numbers related to artificial ventilation) (Table 3), and the correct use of the AED.
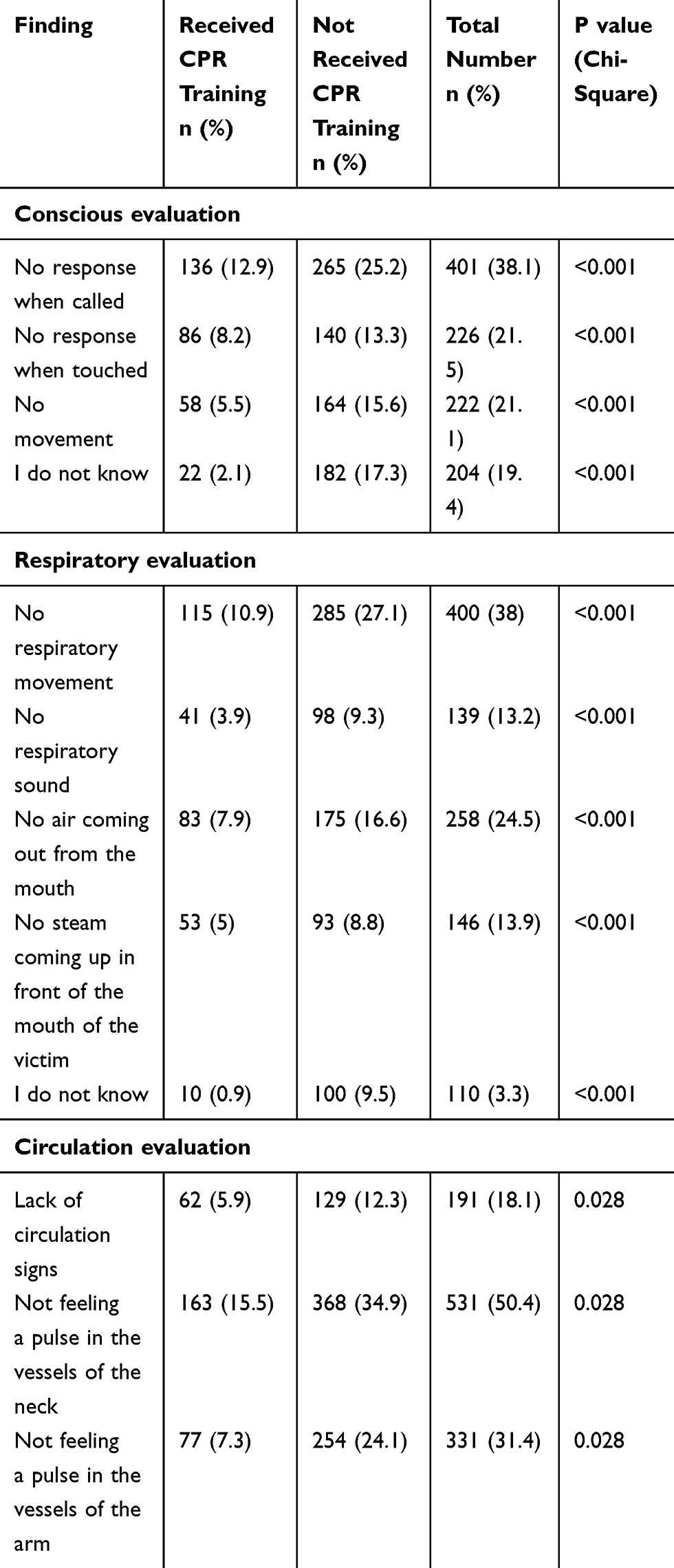 |
Table 1 Identification of Cardiac Arrest |
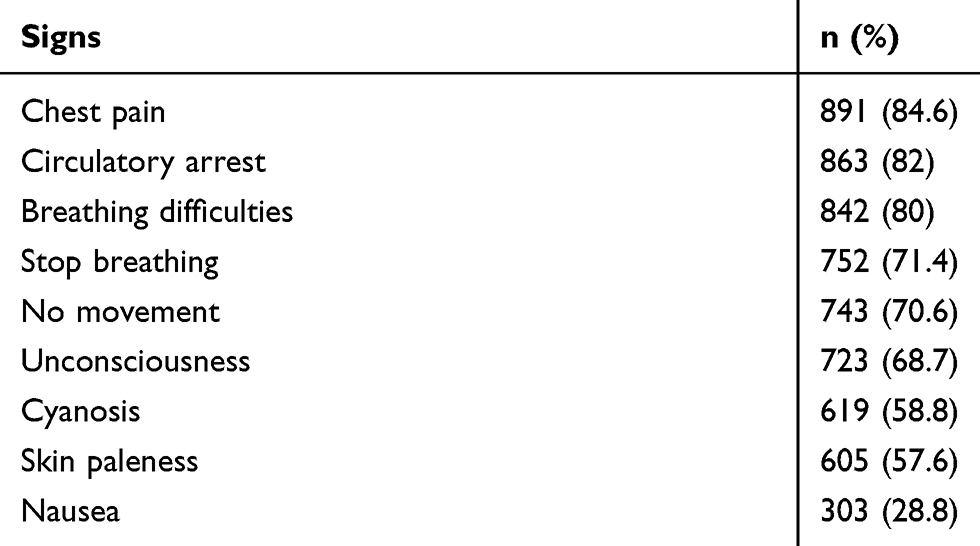 |
Table 2 Response Rates for Cardiac Arrest Signs |
 |
Table 3 Practical Application of CPR Between Those Who Received Training and Who Did Not |
Data were analyzed using the software SPSS version 25. Descriptive statistical analysis was used for continuous data including numbers and percentages, also mean and standard deviation used for age. A chi-square test was used to determine if there were differences between those who received BLS training and those who did not in terms of cardiac arrest recognition, the action performed when witnessing a cardiac arrest, and the practical application of CPR. There were no outliers to removed. Any p-value <0.05 was considered statistically significant.
Ethical approval was obtained from the Unit of Biomedical Ethics at King Abdulaziz University (Reference no. 315-19).
Results
Of the study population, 1053 students who completed the questionnaire. The majority were female (71.2%) with a mean age of 21 years (SD = 2.22). Among the participants, 28.6% were in their fourth year of undergraduate students and had a GPA greater than 3.5 out of 5 (87.1%). Detailed demographic information is presented in Table 4.
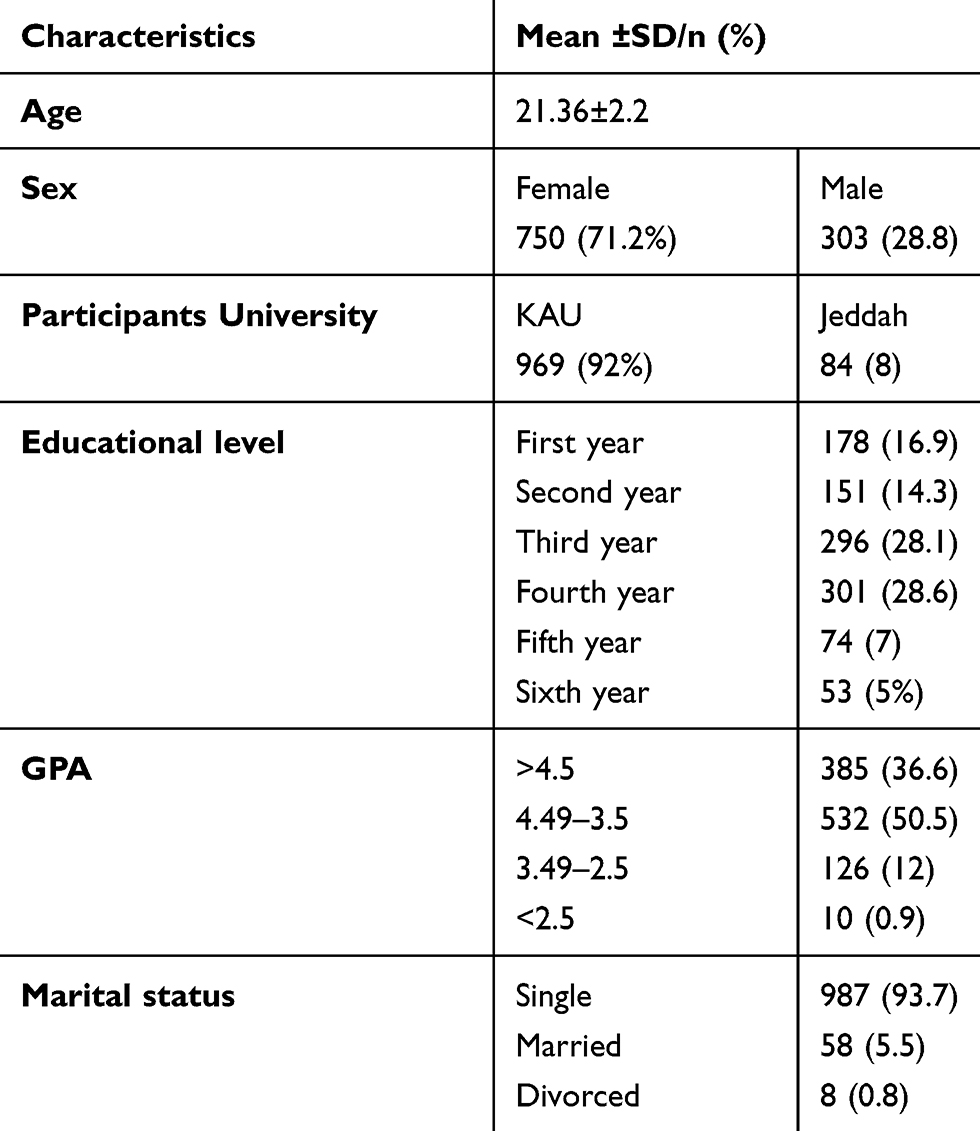 |
Table 4 Demographic Characteristics of the Participants (N =1053) |
We found that 751 (71.3%) students had not received any CPR training. Where is 302 (28.7%) received CPR training, among those (10.7%) of the students underwent CPR training courses offered by the university, 64 (6.1%) students took it through school, 54 (5.1%) at specialized training centers, and (6.8%) took the CPR training from other places.
The results showed that 891 (84.6%) of students considered chest pain as a sign of cardiac arrest, 863 (82%) recognized circularity arrest (no palpable pulse), and 842 (80%) understood breathing difficulties as signs of cardiac arrest. The rest of the response rates for cardiac arrest signs are shown in Table 2.
There was no difference between students who had received formal BLS training and those who had not when selecting “no response to verbal stimuli” as a sign of recognizing a decreased level of consciousness; they were 136 (45%) and 265 (35.3%), respectively, with (p value= 0.00). Students who received BLS training were more likely to recognize respiratory signs of cardiac arrest than their peers (Table 1).
Regarding cardiac evaluation, the number of participants who had not received CPR training and could not accurately feel a pulse in the neck was higher than those who had received training 368 (34.9%) (Table 1).
Among participants, 200 (18.7%) of students had witnessed a cardiac arrest. The majority 94 (8.9%) called an ambulance, 32 (3%) provided both chest compressions and mouth-to-mouth ventilation, 20 (1.9%) asked someone to call for help, 19 (1.8%) provided chest compression solely, 14 (1.3%) watched and left, and 12 (1.1%) only offered mouth-to-mouth breathing. Students who received formal BLS training were more likely to perform chest compressions.
Among participants, 326 (31%) responded that they had adequate knowledge to perform chest compression if they witnessed a sudden cardiac arrest. And, 348 (33%) could give both chest compression and ventilation, 330 (31.3%) could not act, and 228 (21.7%) would only provide chest compressions. Most participants answered correctly, even though they did not receive formal training regarding chest compression rates, determining adequate heart rate, and compression/ventilation ratio. Regarding the meaning of the chest compression, 136 (45%) of students who received CPR defined it as applying strong compression to the chest at specific intervals (Table 3).
When participants were asked, “To who would you provide CPR without hesitation?”, responses indicated that 957 (90.9%) would provide CPR on their friends, 840 (79.8%) would provide CPR to neighbour's, and 916 (87%) would resuscitate anyone.
When asked, “Would you perform CPR for a family member if you witnessed a cardiac arrest situation?”, more females (693, 65.8%) than males (264, 25.1%) answered “yes”. In comparison, 96 (9.1%) were hesitant to apply CPR protocol to a family members. When students were asked, “Why would you not perform CPR on a family member?” 70.2% were afraid of making a mistake, and 8.2% were concerned about the complications of CPR, such as rib fracture. Students were concerned about performing CPR on a stranger for fearing of committing a mistake (61.3%), followed by concerns about litigation (9.3%) and acquiring an infectious disease (7.5%).
The relationship between age and willingness to provide CPR was not significant (p = 0.33). Additionally, we examined the relationship between gender and willingness to perform CPR on a stranger. Females were more willing than males (Table 5).
 |
Table 5 Distribution of Attitude in Response to a Sudden Cardiac Arrest According to Gender |
Discussion
BLS courses are designed to deliver knowledge to a broad range of non-healthcare professionals regarding unpredictable and dangerous situations. A minority of non-medical students (28.7%) in our sample had formal BLS training courses. In King County, Washington state, USA, 79% of the community were reported to have received formal BLS training.14 In Poland,15 China,16 Australia,17 and Slovenia,18 those numbers were 75%, 74.4%, 64%, and 64%, respectively. We attribute this difference in the number of BLS-trained students in Saudi Arabia to the educational design and training courses of BLS and CPR in our universities and communities. It has only recently acknowledged that public awareness of BLS application and CPR are very poor as the courses were only available to medical personnel. In contrast, in countries such as Turkey, Slovenia, and Japan, BLS courses are required to obtain a driver’s license.
It was found a noticeable improvement of bystander CPR rates in Denmark from 19.4% in 2001 to 43.3% in 2010, and a decrease of the annual cardiac arrest cases to 34.4% per 100,000 people in 2010 lead to a remarkable increase in survival rates arriving at the hospital to 6.4% at 2010.19 In Saudi Arabia, out of 429 cases of OHCA, the rates of sudden cardiac arrest were only 3.5% between January and December in 2016 at University Hospital, Western Region, Saudi Arabia.6 A study obligated at a tertiary care hospital in Riyadh, between 1989 and 1995, showed survival rates of OHCA to hospital discharge was 5.1% for adults and 7.4% for children.20 Furthermore, mortality rates of OHCA reached 95.8% with low rates of performing CPR by bystanders, according to a study published in 2015, King Khalid University Hospital, Riyadh, Saudi Arabia.21 Despite these outcomes, Saudi Arabia still needs more statistical researches about OHCA survival rate.
BLS training in schools is also highly relevant; American Heart Association guidelines recommend requiring CPR training program for graduation from secondary schools.22 A study established in Denmark targeted high school students to investigates the knowledge and fears of performing CPR before and after participation in 45-minute sessions of CPR training, a significant improvement of choosing the correct answers noticed and the prevalence of students who are willing to perform CPR increased from 30% to 90%.23 At the College of Dentistry at King Saud University, third-year dental students had more profound knowledge than their older peers.24 This difference might be because of a recent adjustment in the university curriculum where CPR training has now been made an obligatory part of the medical specialty curriculum.
Universities were the primary source of BLS training and information, followed by schools and specialized training centers. This could explain the low knowledge levels in our community, particularly compared to China, where almost a quarter of middle school students learn CPR from television and books.16 Today, more CPR training center programs are open by medical organizations in Saudi Arabia, such as the Saudi Red Crescent Authority to the general population for free to improve the knowledge and competence of the public in the application of this life-saving skill.
Identifying the early signs of cardiac arrest can save critical time needed to save a victim’s life. We found that 84.6% and 82% of the participants were able to identify chest pain and circulatory arrest, respectively, as early signs of cardiac arrest. Therefore, these should be given priority. The number of participants who could identify the signs of cardiac arrest was significantly higher among those who took CPR and BLS training. A study found that among the general Turkish population, only 38.6% were able to identify chest pain and 60.7% recognized circulatory discontinuation.7 These findings emphasize the educational variations between the general population and university students when recognizing cardiac arrest signs.
Previous research has been limited to identifying the relationships between gender, age, and willingness to perform CPR. Our sample chiefly consists of a young demographic with a mean age of 21 years. Similarly, in Vienna, Austria, researchers found that a younger age group was more willing to initiate CPR.9 This can be explained through the fact that BLS programs mostly target this age group for educational purposes.
Interestingly, the number of females who were willing to perform CPR was much higher than males in our study, which contrasts with the Vienna study.9 Moreover, despite Saudi Arabian culture being sensitive to mouth-to-mouth ventilation, especially between men and women, Saudi Arabian society has surmounted this barrier for the sake of intervening in an OHCA. This could be related to the higher emotional intelligence of women and may clarify why females were more impulsive and empathetic toward the victim.25 Despite the high rate of willingness to perform CPR on a family member or a stranger, we were able to identify some limiting factors.
Participants were primarily concerned with making a harmful mistake. A minority of participants had second thoughts regarding litigation or infection transmission. A Jordanian study perceived a similar limitation.10 Apprehension concerning making a mistake is more likely related to not having enough experience in CPR and not associated with any particular technique teaching method.
Limitations
Our study had several limitations. First, it was only conducted in two government universities in Jeddah and did not involve private universities. Second, the self-administered questionnaire was designed specifically to be completed by a respondent without intervention of the researchers during data collection. Third, more accurate results could have been obtained by including an equal number of participants who had taken the BLS training compared to those who had not. Finally, our study might face the risk of selection bias as the students who are more interested and curious about BLS subject might be more willing to fill the questionnaire, and they may have lower or higher knowledge about the research topic than the rest of the population.
Besides, university students have a standard educational level, which does not necessarily represent the entire population with various academic levels.
Conclusion
Our study found that most of the non-medical students did not receive any BLS training. Overall, there was a low CPR knowledge and awareness level among university students in Saudi Arabia. Further studies with larger sample sizes are necessary to confirm further our findings, as well as co-operation between government and private universities. Our findings support the need for more formal teaching and training of each member in our society about BLS. To reach this goal, we must concentrate on educating the community’s future leader university students; this can be achieved by integrating BLS courses and certification in the general university curriculum, regardless of the student’s area of specialization. We recommend obligating BLS certification when obtaining or renewing a driver’s license.
Acknowledgments
We are highly indebted to Road of Change Summer School (a program conducted to teach medical students the essentials of research writing) for their guidance and constant supervision, as well as for providing necessary information regarding the research. Special thanks to Mazen Humayran, Hassan Almohammadi, Khaled Alshuqayfi, and Jawad Alnajjar for their invaluable help with data collection during this study. We would also like to express our thanks to Maha Safhi our advisor, who provided insight and expertise that greatly assisted this research. Lastly, our deepest gratitude to Anas Bifari for analyzing our data.
Disclosure
The authors declare that they have no financial or other conflicts of interest for this work.
References
1. Cooper S, Johnston E, Priscott D. Immediate life support (ILS) training. Impact in a primary care setting? Resuscitation. 2007;72(1):92–99. doi:10.1016/j.resuscitation.2006.06.004
2. Kleinman ME, Perkins GD, Bhanji F, et al. ILCOR scientific knowledge gaps and clinical research priorities for cardiopulmonary resuscitation and emergency cardiovascular care: a consensus statement. Circulation. 2018;137(22):e802–e819. doi:10.1161/CIR.0000000000000561
3. Sasson C, Rogers MAM, Dahl J, Kellermann AL. Predictors of survival from out-of-hospital cardiac arrest a systematic review and meta-analysis. Circ Cardiovasc Qual Outcomes. 2010;3(1):63–81.
4. Bhanji F, Donoghue AJ, Wolff MS, et al. Part 14: education: 2015 American Heart Association guidelines update for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2015;132(18 suppl 2):S561–S573. doi:10.1161/CIR.0000000000000268
5. Meaney PA, Bobrow BJ, Mancini ME, et al. Cardiopulmonary resuscitation quality: improving cardiac resuscitation outcomes both inside and outside the hospital: a consensus statement from the American Heart Association. Circulation. 2013;128(4):417–435. doi:10.1161/CIR.0b013e31829d8654
6. Alzahrani A, Alnajjar M, Alshamarni H, Alshamrani H, Bakhsh A. Prevalence and outcomes of sudden cardiac arrest in a university hospital in the Western Region, Saudi Arabia. Saudi J Med Med Sci. 2019;7(3):156. doi:10.4103/sjmms.sjmms_256_18
7. Özbilgin Ş, Akan M, Hancı V, Aygün C, Kuvaki B. Evaluation of public awareness, knowledge and attitudes about cardiopulmonary resuscitation: report of İzmir. Turk J Anaesthesiol Reanim. 2015;43(6):396–405.
8. Nadar SK, Mujtaba M, Al-Hadi H, et al. Epidemiology, outcomes and coronary angiography findings of patients following out-of-hospital cardiac arrest: a single-centre experience from oman. Sultan Qaboos Univ Med J. 2018;18(2):e155–e160. doi:10.18295/squmj.2018.18.02.006
9. Krammel M, Schnaubelt S, Weidenauer D, et al. Gender and age-specific aspects of awareness and knowledge in basic life support. PLoS One. 2018;13(6):e0198918. doi:10.1371/journal.pone.0198918
10. Jarrah S, Judeh M, Aburuz ME. Evaluation of public awareness, knowledge and attitudes towards basic life support: a cross-sectional study. BMC Emerg Med. 2018;18(1). doi:10.1186/s12873-018-0190-5
11. Al-Mohaissen MA. Knowledge and attitudes towards basic life support among health students at a Saudi women’s university. Sultan Qaboos Univ Med J. 2017;17(1):e59–e65. doi:10.18295/squmj.2016.17.01.011
12. Al-Turki YA. Knowledge and attitudes towards cardiopulmonary resuscitation among university students in Riyadh, Saudi Arabia [Internet]. Saudi Med J. 2008;29. Available from www.smj.org.sa. Accessed December 4, 2020.
13. Neumar RW, Shuster M, Callaway CW, et al. Part 1: executive summary: 2015 American Heart Association guidelines update for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2015;132(18 suppl 2):S315–S367. doi:10.1161/CIR.0000000000000252
14. Sipsma K, Stubbs BA, Plorde M. Training rates and willingness to perform CPR in King County, Washington: a community survey. Resuscitation. 2011;82(5):564–567. doi:10.1016/j.resuscitation.2010.12.007
15. Rasmus A, Czekajlo MS. A national survey of the Polish populationʼs cardiopulmonary resuscitation knowledge. Eur J Emerg Med. 2000;7(1):39–43. doi:10.1097/00063110-200003000-00008
16. Chen M, Wang Y, Li X, et al. Public knowledge and attitudes towards bystander cardiopulmonary resuscitation in China. Biomed Res Int. 2017;2017.
17. Celenza T, Gennat HC, O’brien D, Jacobs IG, Lynch DM, Jelinek GA. Community competence in cardiopulmonary resuscitation [Internet]. Available from: www.elsevier.com/locate/resuscitation.
18. Parrinello G
19. Wissenberg M, Lippert FK, Folke F, et al. Association of national initiatives to improve cardiac arrest management with rates of bystander intervention and patient survival after out-of-hospital cardiac arrest. JAMA. 2013;310(13):1377–1384. doi:10.1001/jama.2013.278483
20. Conroy KM, Jolin SW. Original contributions cardiac arrest in Saudi Arabia: a 7-year experience in Riyadh. J Emerg Med. 1999;17(4):617–623. doi:10.1016/S0736-4679(99)00049-9
21. Bin Salleeh HM, Gabralla KA, Leggio WJ, Al Aseri ZA. Out-of-hospital adult cardiac arrests in a university hospital in central Saudi Arabia. Saudi Med J. 2015;36(9):1071–1075. doi:10.15537/smj.2015.9.12081
22. Cave DM, Aufderheide TP, Beeson J, et al. American Heart Association Emergency Cardiovascular Care CommitteCouncil on Cardiopulmonary, Critical Care, Perioperative and Resuscitation, Council on Cardiovascular Diseases in the Young, Council on Cardiovascular Nursing, Council on Clinical Cardiology, and Advocacy Coordinating Committee. Importance and implementation of training in cardiopulmonary resuscitation and automated external defibrillation in schools a science advisory from the American Heart Association. 2011. Available from: http://circ.ahajournals.org/cgi/content/full/10.1161/CIR.0b013e31820b5328/DC1.
23. Aaberg AMR, Larsen CEB, Rasmussen BS, Hansen CM, Larsen JM. Basic life support knowledge, self-reported skills and fears in Danish high school students and effect of a single 45-min training session run by junior doctors; a prospective cohort study. Scand J Trauma Resusc Emerg Med. 2014;22(1). doi:10.1186/1757-7241-22-24
24. Alotaibi O, Alamri F, Almufleh L, Alsougi W. Basic life support: knowledge and attitude among dental students and staff in the college of dentistry, King Saud University. Saudi J Dent Res. 2016;7(1):51–56. doi:10.1016/j.sjdr.2015.06.001
25. Al A, Preparatory A, Deanship Y. English. J Educ Pract. 2014; 5. Available from: www.iiste.org. Accessed December 4, 2020.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.