Back to Journals » International Journal of Women's Health » Volume 18
Evaluation of Adherence to Clinical Guidelines for Antimicrobial Prescribing in Pregnant Patients: A Retrospective Cross-Sectional Observational Study in Tabuk, Saudi Arabia
Authors Prabahar K ![]() , Alshareef H
, Alshareef H ![]() , Alqifari SF
, Alqifari SF ![]() , Althagfi WM, Albalawi SA, Almarwani LM, Alshahrani SH, Alanazi RF, Aljabri A
, Althagfi WM, Albalawi SA, Almarwani LM, Alshahrani SH, Alanazi RF, Aljabri A
Received 8 November 2025
Accepted for publication 19 February 2026
Published 23 February 2026 Volume 2026:18 580043
DOI https://doi.org/10.2147/IJWH.S580043
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Vinay Kumar
Kousalya Prabahar,1 Hanan Alshareef,1 Saleh F Alqifari,1 Waad M Althagfi,2 Sarah A Albalawi,2 Lujain M Almarwani,2 Shahad H Alshahrani,2 Raghad F Alanazi,2 Ahmed Aljabri3
1Department of Pharmacy Practice, Faculty of Pharmacy, University of Tabuk, Tabuk, Saudi Arabia; 2Faculty of Pharmacy, University of Tabuk, Tabuk, Saudi Arabia; 3Department of Pharmacy Practice, Faculty of Pharmacy, King Abdulaziz University, Jeddah, Saudi Arabia
Correspondence: Kousalya Prabahar, Department of Pharmacy Practice, Faculty of Pharmacy, University of Tabuk, Tabuk, 71491, Saudi Arabia, Email [email protected]
Background: Antimicrobial therapy during pregnancy is vital for managing infections and protecting maternal-fetal health. However, altered pharmacokinetics and potential teratogenicity complicate prescription, necessitating strict adherence to clinical guidelines. This study assessed the appropriateness of antimicrobial prescriptions among pregnant women in Tabuk, Saudi Arabia and examined demographic factors associated with prescribing practices, as well as the incidence of adverse effects.
Methods: A retrospective cross-sectional observational study was conducted in the outpatient antenatal clinics of three government hospitals in Tabuk, Saudi Arabia, from October 2022 to September 2023, focusing on pregnant women. Data on patient demographics (age, education, employment, parity), clinical details (gestational age, infection type), and antimicrobial prescriptions (drug, dose, duration, trimester) were extracted and evaluated for compliance with American College of Obstetricians and Gynecologists (ACOG) and Health Service Executive (HSE) guidelines. Documented adverse drug reactions were categorized by type and severity. Associations between infection type and antimicrobial prescription appropriateness were evaluated using Chi-square tests. Associations between demographic variables and antimicrobial prescription appropriateness were evaluated using multivariate analysis, with odds ratios (ORs) and 95% confidence intervals (CIs) calculated for categorical variables. Statistical significance was set at p < 0.05. Data were analyzed using SPSS version 27.
Results: A total of 403 medical records were analyzed. Urinary tract infections were the most frequent indication (38%), followed by respiratory infections (22.1%) and bacterial vaginosis (14.1%). Amoxicillin and nitrofurantoin were the most prescribed antimicrobials. Overall, 77.4% of prescriptions were guideline-compliant, while 22.6% were inappropriate, predominantly due to incorrect drug selection for the trimester or infection type (9.4%), dosing errors (7.2%), and inappropriate duration (6.0%). Notably, the use of nitrofurantoin in the third trimester and trimethoprim in the first trimester were common concerns. Adverse effects occurred in 14.9% of the patients, with two cases of suspected nitrofurantoin-associated hemolytic anemia. No significant association was observed between infection type and appropriateness of antimicrobial prescription. Educational status was significantly associated with appropriate prescription (aOR: 1.82; 95% CI: 1.05– 3.15; p = 0.038), whereas maternal age, employment status, and gestational trimester were not significant predictors.
Conclusion: Most antimicrobial prescriptions during pregnancy were guideline-compliant, though notable errors, particularly involving nitrofurantoin and trimethoprim, persisted. Higher maternal education was associated with greater likelihood of receiving appropriate prescriptions. These findings highlight the importance of adhering to trimester-specific prescribing guidelines, implementing antimicrobial stewardship measures, and providing ongoing education for healthcare providers to enhance maternal and fetal safety.
Keywords: pregnancy, antimicrobial prescribing, guideline compliance, maternal health, Saudi Arabia
Introduction
Antimicrobial therapy plays a crucial role in managing infections during pregnancy, safeguarding maternal and fetal health.1,2 Pregnant women are particularly vulnerable to infections owing to physiological and immunological changes that may predispose them to conditions such as urinary tract infections (UTIs), respiratory infections, and intra-amniotic infections.3,4 Prompt and effective antimicrobial treatment is essential to prevent adverse maternal outcomes and reduce the risk of complications, such as preterm labor, miscarriage, and neonatal infections.5
From an epidemiological perspective, infections during pregnancy are common and represent a major cause of maternal morbidity worldwide. UTIs affect approximately 2–10% of pregnant women, making them one of the most frequent indications for antimicrobial therapy during antenatal care.6 Bacterial vaginosis has been reported in up to 10–30% of pregnancies and is associated with adverse outcomes such as preterm labor and low birth weight, while respiratory tract infections remain a leading cause of outpatient visits during pregnancy.7 Physiological changes during pregnancy, including urinary stasis, altered immunity, and hormonal effects on mucosal barriers, increase susceptibility to infection and may alter disease severity.8
Pregnant women represent a particularly vulnerable population in whom inappropriate antimicrobial prescribing carries dual risks: treatment failure or toxicity in the mother, and potential teratogenic or neonatal harm to the fetus. Even commonly used antimicrobials may pose trimester-specific safety concerns, emphasizing the need for evidence-based prescribing.
The use of antimicrobials during pregnancy is complex, necessitating a careful balance between therapeutic benefits and potential risks to both the mother and the fetus. Physiological changes in pregnancy alter drug pharmacokinetics and pharmacodynamics, affecting efficacy and safety.9 Moreover, certain antimicrobials pose teratogenic risks or may cause fetal toxicity, particularly when used in specific trimesters. For example, nitrofurantoin, which is effective against UTIs, is generally avoided in the third trimester because of concerns about neonatal hemolytic anemia.10
Despite the availability of clinical guidelines, studies have reported variability in antimicrobial prescription patterns among pregnant women, with instances of inappropriate choice, dosing, or duration.11–13 Such inappropriate prescriptions may not only compromise treatment efficacy but also contribute to antimicrobial resistance, adverse drug reactions, and suboptimal pregnancy outcomes.14 Inappropriate antimicrobial use in hospital settings is a well-recognized driver of antimicrobial resistance, which poses a growing threat to maternal and neonatal health.15 Repeated or incorrect antibiotic exposure facilitates the emergence of resistant pathogens, limiting treatment options and increasing the risk of treatment failure and nosocomial infections.16 In obstetric care, where prophylactic and empirical antibiotic use is common, non-compliance with guidelines can accelerate local resistance trends and undermine infection control efforts. Strengthening antimicrobial stewardship within maternity services is essential to mitigate these risks.
In Saudi Arabia, there is currently a lack of comprehensive, national guidelines for antimicrobial prescribing during pregnancy. Consequently, clinicians often rely on international protocols such as American College of Obstetricians and Gynecologists (ACOG) guidelines17,18 and Health Service Executive (HSE) guidelines.19 Currently, there are limited comprehensive data examining antimicrobial prescription trends, appropriateness, and associated outcomes in pregnant women in real-world clinical settings. Although some recent regional research, such as a cross‑sectional assessment of antibiotic use among pregnant women in Marrakech, Morocco,20 reported high rates of antibiotic consumption and suboptimal practices, data on guideline adherence and detailed prescribing appropriateness in the Middle East remain sparse.12 Addressing this gap is vital for optimizing infection management, minimizing potential harms, and guiding healthcare policies.
This study aimed to assess antimicrobial prescription patterns among pregnant women, evaluate the appropriateness of prescriptions based on the most recent ACOG and HSE guidelines and investigate demographic factors influencing prescribing practices. Both guidelines provide evidence-based recommendations for antimicrobial use in pregnancy, focusing on safety and efficacy across trimesters. While both emphasize avoidance of teratogenic drugs and the use of narrow-spectrum agents whenever possible, minor differences exist in drug preferences and dosing recommendations for specific infections. For instance, ACOG guidelines more frequently reference US resistance patterns and FDA pregnancy risk categories, whereas HSE guidelines provide more detailed trimester-specific antibiotic choices for common infections such as UTIs and respiratory tract infections. Incorporating both sets of guidelines allowed for a comprehensive and balanced assessment of prescribing appropriateness. Additionally, the study explores the incidence of adverse effects associated with antimicrobial use during pregnancy, providing insights that may inform safer prescriptions and better maternal-fetal health outcomes.
Materials and Methods
Study Design and Setting
This retrospective cross-sectional observational study was conducted among pregnant women attending the outpatient antenatal clinics of three government hospitals in Tabuk, Saudi Arabia, between October 2022 and September 2023. These Ministry of Health hospitals provide free antenatal care as part of the national healthcare system and serve a mixed population from various socioeconomic backgrounds, including both urban and peri-urban residents, and function as secondary and tertiary referral centers for the Tabuk region. The study focused exclusively on pregnant women who received antimicrobial prescriptions in an outpatient setting, without inpatient admission or critical care involvement. The setting reflects routine, non-emergent antenatal care, allowing for evaluation of prescribing practices in a primary or secondary care context.
Study Population
Inclusion Criteria
Pregnant women of any gestational age who received at least one antimicrobial prescription during the study period (October 2022–September 2023) in an outpatient antenatal clinic were included.
Exclusion Criteria
Women who were hospitalized, presented to emergency departments, or received antimicrobials in inpatient or critical care settings were excluded. Prescriptions for prophylactic use unrelated to active infection (eg, surgical prophylaxis) were also excluded.
Handling of Multiple Visits
When women had multiple outpatient visits or received more than one antimicrobial prescription during the study period, only the first eligible prescription episode was included to avoid duplication and ensure independence of observations. Repeat prescriptions for the same infection episode were not counted separately.
Sample Size
The sample size was calculated using OpenEpi software.21 Assuming an expected proportion of appropriate prescriptions of 50% (a conservative estimate used due to the absence of prior local data), a 95% confidence level, and a 5% margin of error, the minimum sample size required was 384. However, 403 patients were included to account for potential data inconsistencies and improve generalizability. This exceeded the minimum required sample size and provided adequate statistical power for descriptive and inferential analyses in hospital-based prescribing audits.
Sampling Method
A consecutive sampling approach was used. All medical records of pregnant women attending outpatient antenatal clinics during the study period that met the inclusion criteria were reviewed until the required sample size was achieved. This method minimizes selection bias and ensures that all eligible cases within the study timeframe are included.
Data Collection
After receiving appropriate training, data were retrospectively extracted from electronic medical records and prescription charts using a standardized data extraction form. The collected variables included the following:
- Demographic information: Age, educational status, employment status, number of children.
- Clinical data: Date of last menstrual period, gestational age at the time of prescription, diagnosis, or indication for antimicrobial therapy.
- Antimicrobial prescription details: Drug name, dosage, frequency, route of administration, duration of therapy.
- Adverse effects: Documented side effects or complications potentially related to antimicrobial use during pregnancy. Severity of adverse effects, where recorded, was categorized as mild, moderate, or severe based on clinical documentation and the need for treatment modification or discontinuation.
Diagnoses were based on the treating clinician’s documentation in the electronic medical record. Where available, diagnoses were supported by laboratory investigations (eg, urine analysis or culture for UTIs, vaginal swab results for bacterial vaginosis). In cases where laboratory confirmation was not documented, diagnoses were made clinically according to routine antenatal care practice. No additional diagnostic standardization was applied retrospectively.
The variables were categorized as follows:
- Age: grouped as <30 years and ≥30 years.
- Educational status: no formal education, primary, secondary, and tertiary.
- Occupation: employed or unemployed.
- Gestational age: first, second, or third trimester.
- Infection type: UTI, respiratory tract infection, bacterial vaginosis, gastrointestinal infection, skin/soft tissue infection, intra-amniotic infection, and others.
Prescription-related variables included the antimicrobial agent, dose, frequency, route of administration, and duration. Antimicrobial agents were further categorized according to the World Health Organization (WHO) Anatomical Therapeutic Chemical (ATC) classification system.22 Each prescription was evaluated against trimester-specific safety recommendations according to ACOG and HSE guidelines.
Missing Data Handling
Variables with missing data were coded as “missing” and excluded from the corresponding analysis. The frequency of missing data did not exceed 5% for any key variable.
Assessment of Appropriateness
The main outcome was the antimicrobial prescription patterns, evaluated for appropriateness by comparing them against the ACOG17,18 and HSE19 antimicrobial prescription guidelines for pregnancy. A summary comparison of ACOG and HSE antimicrobial prescribing recommendations for the most common infections analyzed in this study is provided in Supplementary Table S1. Appropriateness was assessed based on the following criteria:
- Selection of antimicrobial agent relative to infection type and gestational age.
- Correct dosing regimen, frequency, and duration.
- Avoidance of contraindicated drugs during specific pregnancy trimesters.
Prescriptions were categorized as appropriate or inappropriate based on adherence to these criteria. Secondary outcomes included investigating demographic factors influencing prescribing practices and exploring the incidence of adverse effects associated with antimicrobial use during pregnancy.
Data Analysis
Statistical analyses were performed using SPSS version 27 (IBM Corp., Armonk, NY, USA).Descriptive statistics summarized demographic and clinical characteristics. Continuous variables were presented as mean (SD), and categorical variables as frequencies and percentages, with 95% confidence intervals (95% CI) for key proportions (overall guideline compliance, adverse effect rates).
Associations between infection type and antimicrobial prescription appropriateness were evaluated using Chi-square tests. Associations between demographic variables and prescription appropriateness were evaluated using multivariate logistic regression, reporting adjusted odds ratios (aORs) with 95% CIs. Multivariate logistic regression was used to adjust for potential confounding factors, including maternal age (<30 vs ≥30 years), educational status (tertiary vs lower), occupation (employed vs unemployed), and gestational trimester (second vs others). Statistical significance was set at p < 0.05.
Ethical Considerations
The study protocol was reviewed and approved by the Local Research Ethics Committee, Tabuk Institutional Review Board [TU-077/023/220]. The study was conducted in accordance with the Declaration of Helsinki, and patient confidentiality was maintained by anonymizing data during collection and analysis.
Results
Demographic and Clinical Characteristics of Pregnant Women
A total of 403 pregnant women were included in the study. The mean age was 28.6 (5.2) years. Most participants (41.4%) had tertiary education and 25.6% had secondary education. The majority of participants (57.8%) were unemployed. The average number of living children prior to the current pregnancy was 2.1 (1.4). At the time of antimicrobial prescription, 41.7% of women were in their second trimester (Table 1).
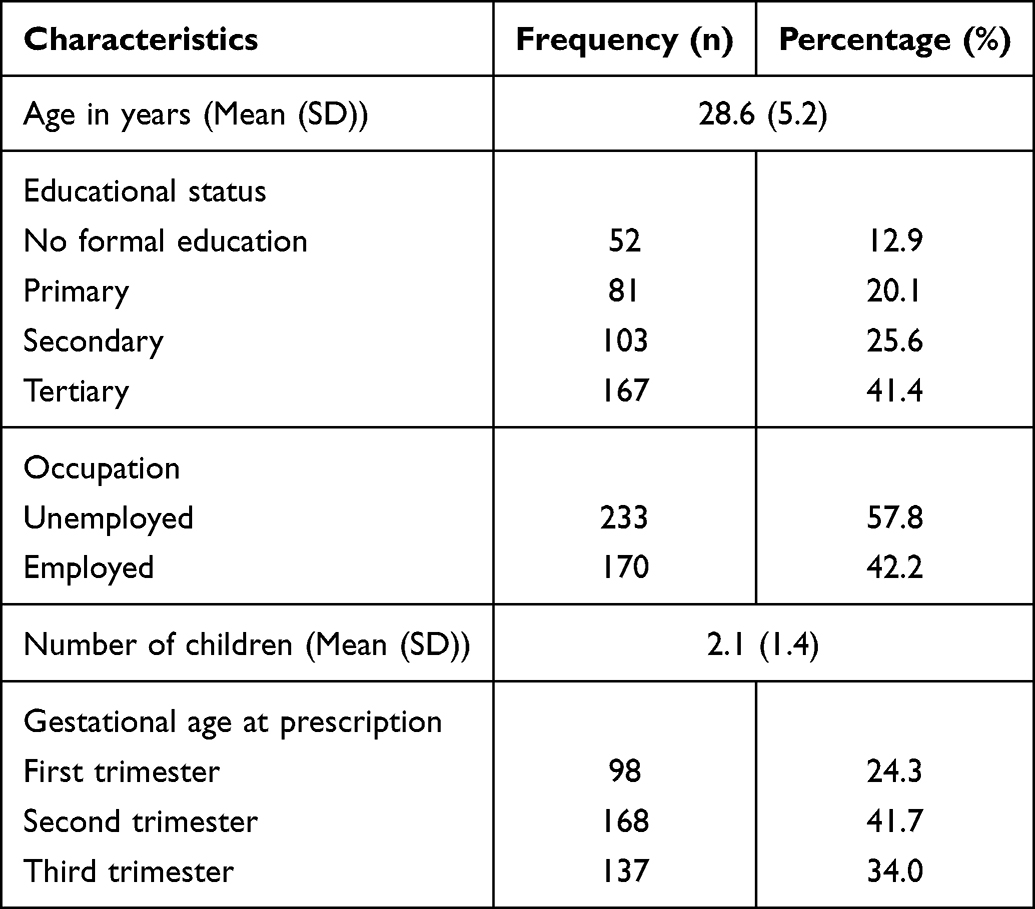 |
Table 1 Demographic and Clinical Characteristics of Pregnant Women (n = 403) |
Pregnancy-Related Comorbidities and Concomitant Medications
Among the study participants, 26.8% had at least one pregnancy-related comorbidity, most commonly gestational diabetes (14.6%), hypertensive disorders of pregnancy (7.9%), and anemia (4.3%). Routine antenatal supplements such as iron and folic acid were prescribed to the majority of participants (81.9%). Other concomitant medications included antihypertensive drugs (6.5%) and insulin therapy (5.9%). No clinically significant drug–drug interactions were documented in the medical records.
Indications for Antimicrobial Prescribing
The most common indication for antimicrobial use was UTI, accounting for 38.0% of the cases, followed by respiratory tract infections (22.1%) and bacterial vaginosis (14.1%). Other indications included gastrointestinal, skin and soft tissue infections and intra-amniotic infections (Table 2).
 |
Table 2 Indications for Antimicrobial Prescribing |
Trimester-Specific Distribution of Antimicrobials
Amoxicillin and nitrofurantoin were the most frequently prescribed antimicrobials during all trimesters. In the first trimester, amoxicillin accounted for 29.6% of the prescriptions, followed by nitrofurantoin (24.5%). During the second trimester, both agents were prescribed equally (24.4%). In the third trimester, amoxicillin was the most prescribed antimicrobial (24.8%), followed by cefuroxime (18.2%).
According to the WHO ATC classification, the majority of prescribed antimicrobials belonged to the beta-lactam antibacterials (J01C and J01D) group (42.7%), followed by nitrofuran derivatives (J01XE) (21.6%), imidazole derivatives (J01XD) (13.2%), macrolides (J01FA) (11.2%), and lincosamides (J01FF) (6.4%) (Table 3).
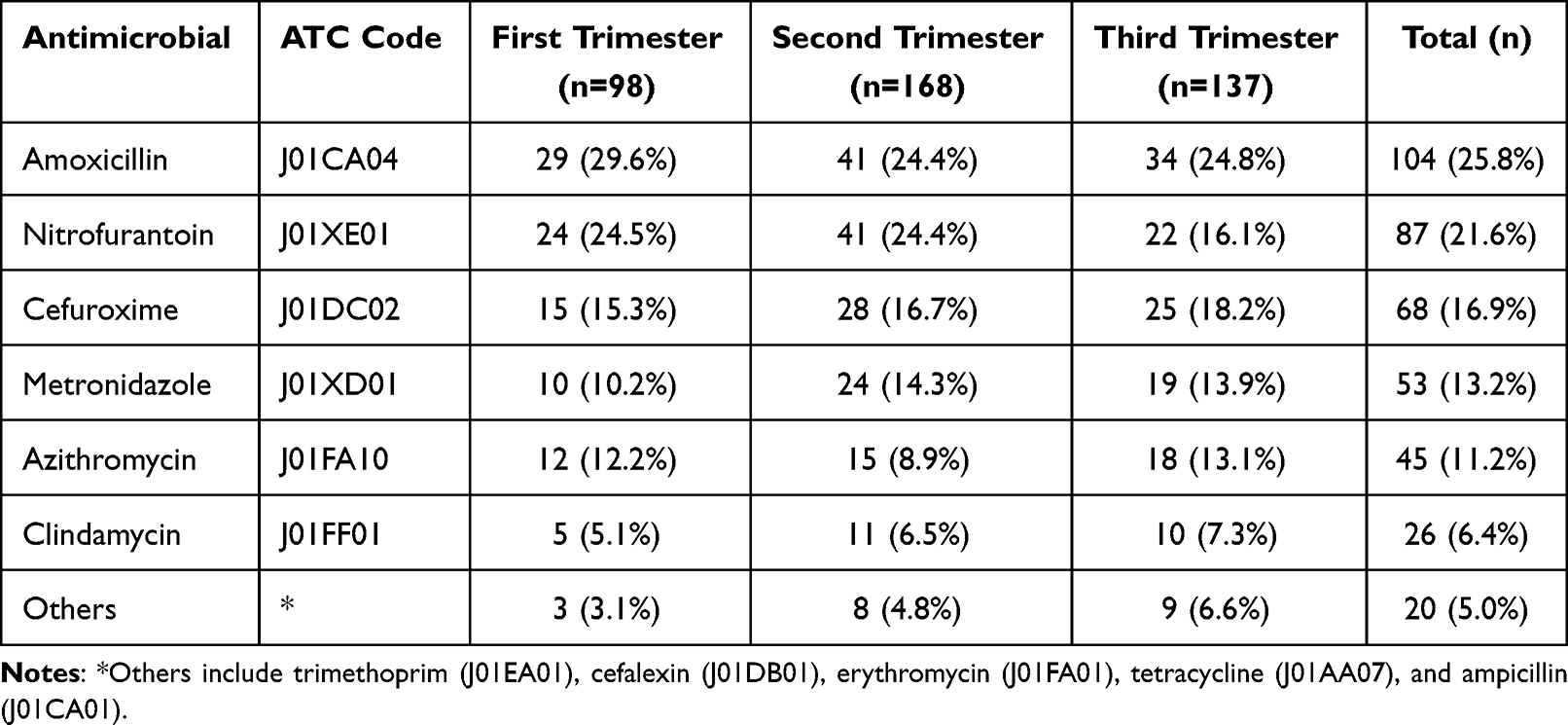 |
Table 3 Trimester-Specific Distribution of Antimicrobials |
Appropriateness of Antimicrobial Prescriptions
Overall, 312 prescriptions (77.4%) (95% CI: 73.1–81.3) were considered appropriate according to ACOG and HSE guidelines. Inappropriate prescriptions (22.6%) were primarily due to incorrect antimicrobial selection for the trimester or infection type (9.4%), followed by incorrect dosing/frequency (7.2%) and inappropriate duration (6.0%) (Table 4).
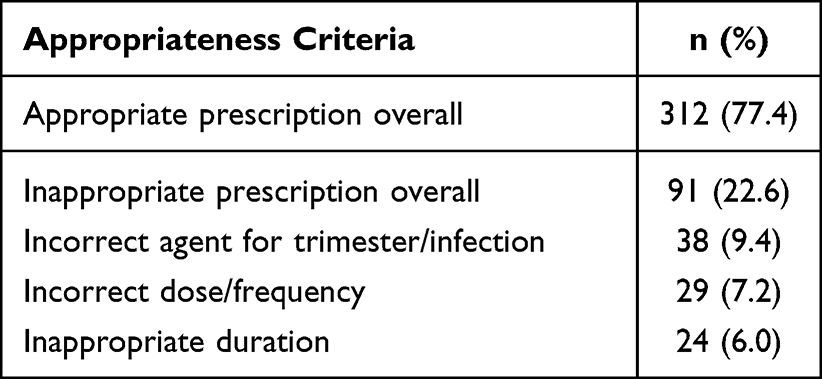 |
Table 4 Appropriateness of Antimicrobial Prescriptions |
Types of Inappropriate Prescriptions and Drugs Involved
Among the 91 inappropriate prescriptions, the most common issue was the use of incorrect agents for the trimester or infection type (41.8%), followed by incorrect dose or frequency (31.9%), and inappropriate duration (26.4%). Nitrofurantoin (16.5%) was commonly used inappropriately in the third trimester, while trimethoprim (14.3%) and tetracycline (11.0%) were also frequently misprescribed. Dosing errors primarily involved amoxicillin (12.1%), cefuroxime (11.0%), and azithromycin (8.8%). Duration-related issues were observed with metronidazole (9.9%), clindamycin (8.8%), and nitrofurantoin (7.7%) (Table 5).
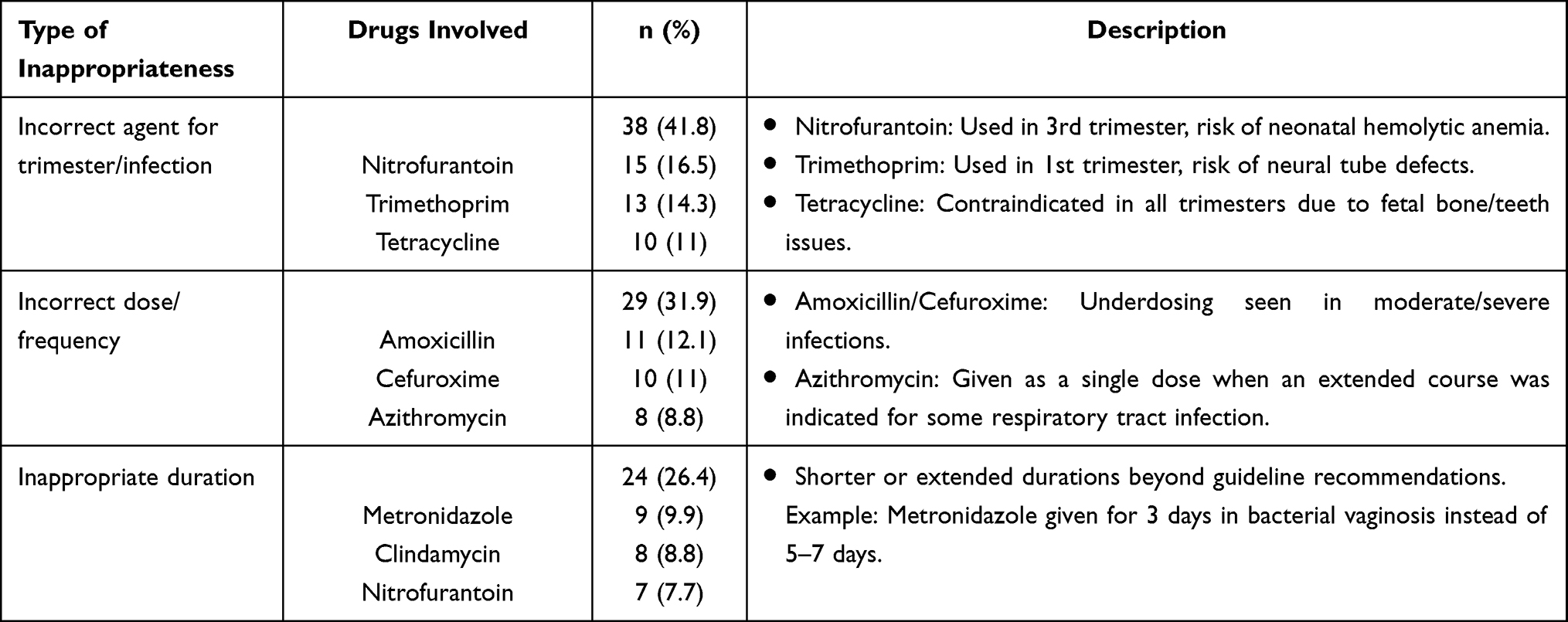 |
Table 5 Types of Inappropriate Prescriptions and Drugs Involved (n = 91) |
Adverse Effects of Antimicrobials
Adverse effects were reported in 14.9% of the patients. The most frequent adverse effects were gastrointestinal upset (6.9%), vaginal candidiasis (4.2%), and allergic reactions (3.2%). Two cases (0.5%) of suspected hemolytic anemia have also been reported (Figure 1).
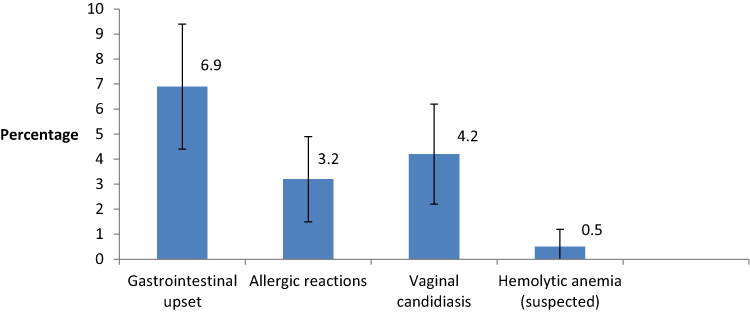 |
Figure 1 Adverse effects of antimicrobials. |
Severity and Clinical Management of Adverse Effects
Where severity was documented, most adverse effects were mild to moderate and did not necessitate discontinuation of antimicrobial therapy. Vaginal candidiasis cases required additional topical antifungal treatment. The two cases of suspected nitrofurantoin-associated hemolytic anemia prompted immediate discontinuation of the drug and referral for specialist assessment. No life-threatening or irreversible reactions were reported.
Association Between Infection Type and Appropriateness of Antimicrobial Prescription
Table 6 presents the association between infection type and antimicrobial prescription appropriateness among the study participants. The contribution of each infection type to the overall Chi-square statistic is also shown. Respiratory tract infections contributed the most to the overall χ2 (0.77), while skin and soft tissue infections and intra-amniotic infections contributed minimally (0.01–0.02). The overall Chi-square test indicated no statistically significant association between infection type and appropriateness of antimicrobial prescription (χ2 = 1.50, df = 6, p = 0.96). Inappropriate prescribing was not concentrated in any specific infection category.
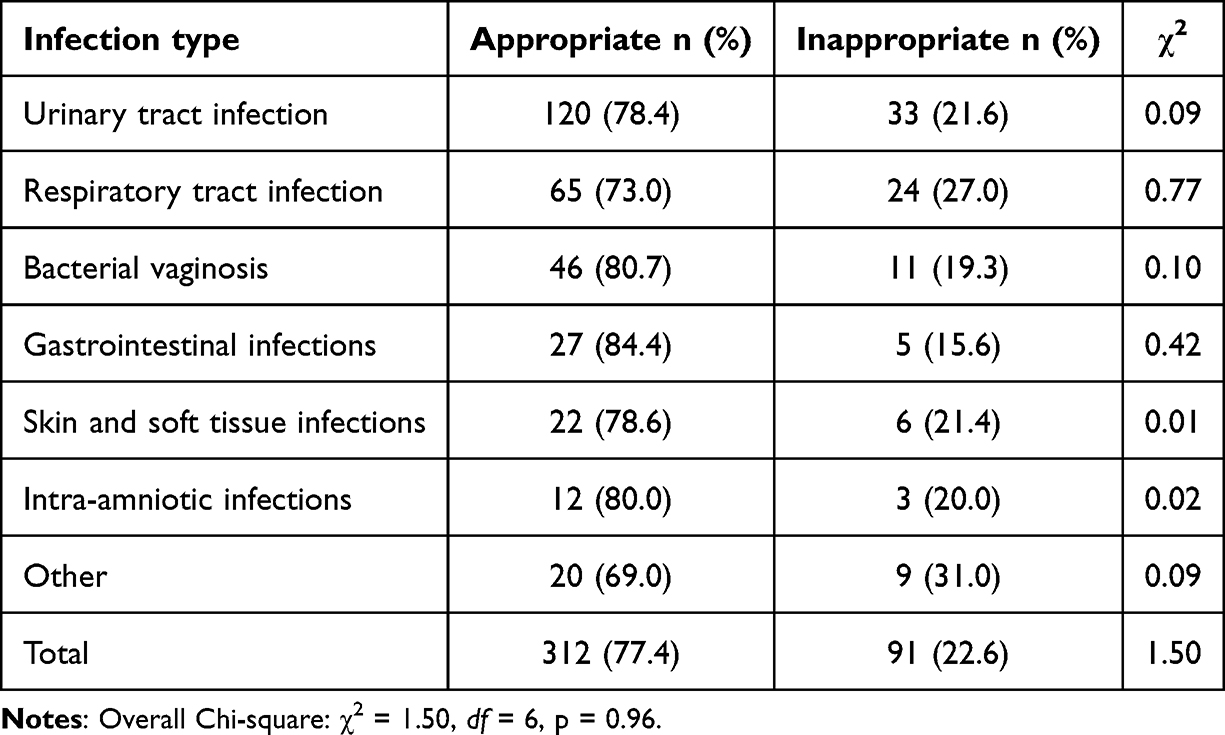 |
Table 6 Association Between Infection Type and Antimicrobial Prescription Appropriateness |
Association Between Demographic Variables and Antimicrobial Prescription Appropriateness
Multivariate analysis was conducted to examine the association between maternal demographic characteristics and the appropriateness of antimicrobial prescriptions. Educational status was significantly associated with guideline-compliant prescription (aOR: 1.82; 95% CI: 1.05–3.15; p = 0.038), with women having tertiary education more likely to receive appropriate therapy. Maternal age, employment status, and gestational trimester were not significantly associated with prescription appropriateness (p > 0.05). These findings suggest that higher maternal education may indirectly influence prescription adherence, possibly through improved health literacy or patient–provider communication (Table 7).
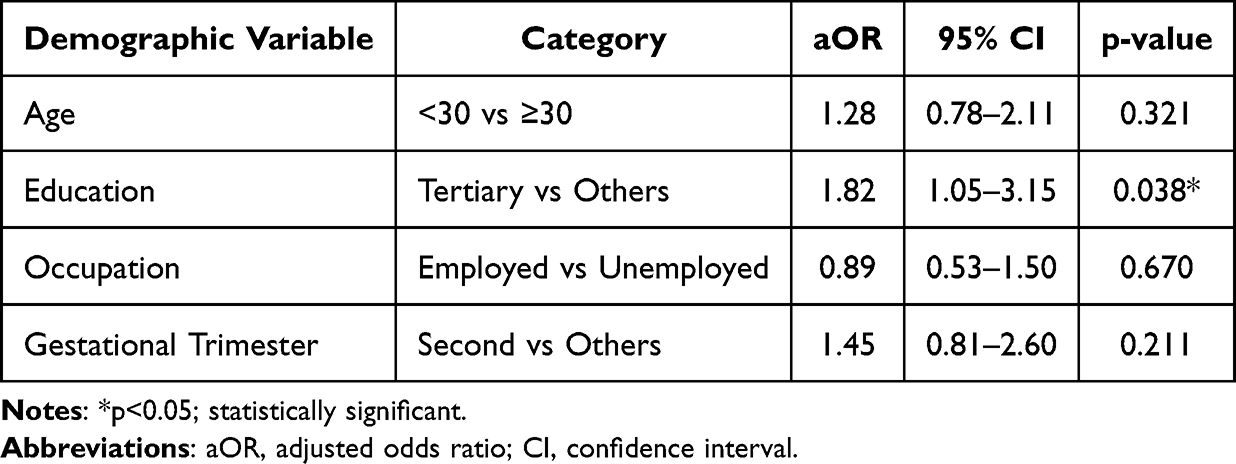 |
Table 7 Demographic Predictors of Antimicrobial Prescription Appropriateness in Pregnancy |
Discussion
This retrospective study assessed the appropriateness of antimicrobial prescriptions during pregnancy, adherence to ACOG and HSE guidelines, and factors influencing prescribing patterns. The findings highlight the critical aspects of antimicrobial stewardship in maternal healthcare and offer insights into optimizing infection management during pregnancy.
Our results showed that UTIs were the most frequent indication for antimicrobial therapy (38%), consistent with existing literature emphasizing UTIs as common pregnancy-related infections due to hormonal and anatomical changes that predispose women to urinary stasis and bacterial colonization.4,23,24 Respiratory tract infections and bacterial vaginosis are also prevalent, underscoring the importance of vigilant infection screening during prenatal care.
The trimester-specific prescription trends demonstrated that amoxicillin and nitrofurantoin were the most commonly used antimicrobials across all trimesters. This pattern aligns with the broad-spectrum efficacy and relatively safe profiles in pregnancy.25 This distribution indicates a predominant reliance on beta-lactams and nitrofurantoin for managing common infections during pregnancy. However, inappropriate use of nitrofurantoin in the third trimester, documented in this study, raises safety concerns. Logistic regression analysis showed that second-trimester prescriptions had higher odds of being appropriate compared to other trimester prescriptions (aOR: 1.45; 95% CI: 0.81–2.60; p = 0.211), although this did not reach statistical significance. Nitrofurantoin, though effective, poses a risk of neonatal hemolytic anemia when used late in pregnancy,26,27 and this prescribing practice contradicts the guideline recommendations.
The overall appropriateness rate (77.4%) is comparable to or slightly better than that of other studies conducted in similar low-income or middle-income settings.28,29 Nonetheless, the remaining 22.6% of prescriptions were inappropriate, with the most common errors involving incorrect antimicrobial selection for the trimester or infection type (9.4%), followed by dosing errors (7.2%) and incorrect duration (6.0%). These findings reflect persistent challenges in aligning clinical practice with guideline-based prescriptions, particularly in complex or ambiguous cases. One contributing factor to inappropriate antimicrobial selection and dosing may be the reliance on empirical therapy in the absence of routine antimicrobial susceptibility testing (AST). In outpatient antenatal settings, antimicrobials are frequently prescribed based on clinical judgment alone, without microbiological confirmation, particularly for common infections such as UTIs and respiratory tract infections. While empirical therapy is often necessary to avoid treatment delays, its widespread use may increase the risk of selecting suboptimal or contraindicated agents, inappropriate dosing, and unnecessary broad-spectrum exposure. The lack of AST may therefore partly explain the observed deviations from guideline-recommended prescribing and highlights an important opportunity to strengthen antimicrobial stewardship in maternal healthcare. Although the first-line antimicrobial agents were consistent between ACOG and HSE guidelines, minor differences exist in the agents to avoid and trimester-specific recommendations - for example, HSE advises avoiding trimethoprim in the first trimester, while ACOG cautions against nitrofurantoin at term. These differences may have influenced the classification of appropriateness in a small number of cases (Supplementary Table S1).
Notably, drugs such as trimethoprim, tetracycline, and third-trimester nitrofurantoin were identified as major contributors to inappropriate prescriptions. Trimethoprim, a folate antagonist, carries risks of neural tube defects when used during the first trimester,30 and tetracyclines are well-established teratogens linked to fetal bone and tooth abnormalities.31 These findings underscore the necessity of continual education on pharmacological safety during pregnancy, especially in rapidly changing clinical environments.
Importantly, 14.9% of the patients reported adverse effects related to antimicrobial use, with gastrointestinal discomfort and vaginal candidiasis being the most common. Although these adverse events were generally mild, two cases of suspected hemolytic anemia associated with nitrofurantoin were clinically significant in this study. Most reported adverse reactions were mild and manageable, aligning with previous studies indicating good tolerability of commonly used antimicrobials in pregnancy.1 The occurrence of vaginal candidiasis following antibiotic therapy is well recognized and was effectively treated with topical antifungals. However, the two cases of suspected nitrofurantoin-induced hemolytic anemia highlight the importance of trimester-specific prescribing and vigilance for hematologic adverse effects in late pregnancy. Prompt discontinuation and referral in these cases prevented further complications, emphasizing the value of close pharmacovigilance in antenatal care.
The presence of pregnancy-related comorbidities such as gestational diabetes, hypertension, and anemia may also influence antimicrobial selection and dosing. For instance, renal or hepatic alterations associated with these conditions can affect drug clearance and increase susceptibility to adverse effects.32 Additionally, routine antenatal supplements such as iron and folic acid may interfere with antimicrobial absorption, particularly with agents like nitrofurantoin and tetracyclines.19 However, potential interactions may occur between nitrofurantoin and iron supplements (reduced absorption) or between metronidazole and certain antihypertensives, emphasizing the need for monitoring in such cases. These interactions underscore the importance of considering comorbidities and concomitant medications when evaluating antimicrobial safety and appropriateness in pregnancy.
No significant association was observed between infection type and prescription appropriateness (p = 0.96), indicating that inappropriate prescribing occurred across all infection categories. Multivariate analysis demonstrated that higher maternal education (tertiary) was significantly associated with guideline-compliant prescribing (aOR: 1.82; 95% CI: 1.05–3.15; p = 0.038), whereas maternal age, employment status, and gestational trimester were not significant predictors. This suggests that higher maternal education may indirectly influence guideline adherence, possibly through improved patient–provider communication or more accurate symptom reporting, rather than directly affecting prescriber behavior.33–35 It is important to note that this association does not imply a causal relationship. The most direct determinants of prescription appropriateness, such as prescriber training, experience, and guideline awareness, were not evaluated in this study and warrant further investigation.
Strengths
The study used standardized and internationally recognized guidelines (ACOG and HSE) for prescription assessment to enhance the reliability and comparability of findings. A robust sample size (n = 403) improves the generalizability and power of the statistical analysis. The inclusion of adverse drug reaction data provides valuable pharmacovigilance insights specific to pregnant women. Analysis of demographic factors adds depth to the understanding of potential socioeconomic influences on healthcare quality.
Limitations
The retrospective design limits causal inference and depends heavily on the accuracy and completeness of medical records. By including only the first eligible prescription for each patient, the study does not capture the cumulative burden of inappropriate antimicrobial prescribing over multiple visits, which may lead to an underestimation of overall prescription inappropriateness per patient. Additionally, the study did not standardize diagnostic criteria for infections. Variation in clinician documentation and interpretation may have led to misclassification of infection types, potentially affecting the assessment of antimicrobial appropriateness. This study focused exclusively on pregnant women treated in outpatient antenatal clinics, excluding those who were hospitalized, presented to emergency departments, or received care in critical care settings. As a result, the findings may not be generalizable to more severe or complex infections that require inpatient or emergency management, where antimicrobial prescribing patterns and clinical considerations differ significantly. Additionally, adverse effects and guideline deviations may be more pronounced in these higher-risk groups, potentially leading to an underestimation of inappropriate prescribing and its consequences. The study did not assess prescriber-related factors such as professional training, specialty, or familiarity with guidelines, which are likely to have a direct impact on prescription appropriateness. While an association was observed between maternal education and prescription appropriateness, this may reflect indirect influences and should not be interpreted as evidence of patient-driven prescribing decisions. The absence of neonatal outcome data means that the study cannot directly assess the fetal impacts of inappropriate prescribing, a key consideration in maternal-fetal medicine. The findings may not be generalizable to private healthcare settings with different prescription patterns and resource availability.
This study relied on secondary data from medical records, which may have been incomplete or inconsistently documented. Mild adverse effects, such as nausea, abdominal pain, diarrhea, or headache, may have been underreported by participants or not documented in the medical records if considered clinically irrelevant. Similarly, some adverse events, such as transient elevations in liver enzymes, may have gone undetected due to the absence of routine laboratory testing. These factors could have resulted in underestimation of the true frequency and severity of antimicrobial-related adverse effects.
Conclusion
Most antimicrobial prescriptions during pregnancy were guideline-compliant; however, potentially unsafe use of nitrofurantoin in the third trimester and trimethoprim in the first trimester was observed. Higher maternal education was associated with greater likelihood of receiving appropriate prescriptions, while age, employment status, gestational trimester, and infection type were not significant predictors.
These findings underscore the importance of adhering to trimester-specific prescribing guidelines, implementing routine AST for common and recurrent infections, particularly suspected UTIs, where feasible, and providing ongoing education for healthcare providers. Addressing these gaps has the potential to improve antimicrobial stewardship, reduce preventable adverse drug events, and ultimately enhance maternal and neonatal health outcomes across Saudi Arabia and similar regional healthcare settings.
Data Protection and Privacy
The data referenced in this study complied with relevant data protection and privacy regulations.
Ethics Approval and Consent to Participate
The study was approved by the Local Research Ethics Committee, Tabuk Institutional Review Board (TU-077/023/220). The data was collected from the medical records and hence waived from informed consent.
Acknowledgments
This research study has not received any funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Nguyen J, Madonia V, Bland CM, et al. A review of antibiotic safety in pregnancy—2025 update. Pharmacotherapy. 2025;45(4):227–12. doi:10.1002/phar.70010
2. Yasin R, Jiang L, Das JK, Bhutta ZA. Interventions to prevent and manage infections in pregnancy. Neonatology. 2025;122(Suppl 1):32–41. doi:10.1159/000543690
3. Kumar M, Saadaoui M, Al Khodor S. Infections and pregnancy: effects on maternal and child health. Front Cell Infect Microbiol. 2022;12:873253. doi:10.3389/fcimb.2022.873253
4. Baimakhanova B, Sadanov A, Trenozhnikova L, et al. Understanding the burden and management of urinary tract infections in women. Diseases. 2025;13(2):59. doi:10.3390/diseases13020059
5. Thinkhamrop J, Hofmeyr GJ, Adetoro O, Lumbiganon P, Ota E. Antibiotic prophylaxis during the second and third trimester to reduce adverse pregnancy outcomes and morbidity. Cochrane Database Syst Rev. 2015;2015(6):CD002250. doi:10.1002/14651858.CD002250.pub3
6. Ansaldi Y, Martinez de Tejada Weber B. Urinary tract infections in pregnancy. Clin Microbiol Infect. 2023;29(10):1249–1253. doi:10.1016/j.cmi.2022.08.015
7. Kenfack-Zanguim J, Kenmoe S, Bowo-Ngandji A, et al. Systematic review and meta-analysis of maternal and fetal outcomes among pregnant women with bacterial vaginosis. Eur J Obstetrics Gynecol Reprod Biol. 2023;289:9–18. doi:10.1016/j.ejogrb.2023.08.013
8. Bhatia P, Chhabra S. Physiological and anatomical changes of pregnancy: implications for anaesthesia. Indian J Anaesth. 2018;62(9):651–657. doi:10.4103/ija.IJA_458_18
9. Costantine M, Kranias EG. Physiologic and pharmacokinetic changes in pregnancy. Front Pharmacol. 2014;5:5. doi:10.3389/fphar.2014.00065
10. Cimolai N, Cimolai T. Nitrofurantoin and pregnancy. CMAJ. 2007;176(13):1860–1861. doi:10.1503/cmaj.1070028
11. Lim AH, Ab Rahman N, Ong SM, et al. Impact evaluation of guidelines on antibiotic utilisation & appropriateness in Malaysian public primary care: an interrupted time series analysis. J Pharm Policy Pract. 2024;17(1):2355666. doi:10.1080/20523211.2024.2355666
12. Baraka MA, AlLehaibi LH, AlSuwaidan HN, et al. Patterns of infections and antimicrobial drugs’ prescribing among pregnant women in Saudi Arabia: a cross sectional study. J Pharm Policy Pract. 2021;14(1):9. doi:10.1186/s40545-020-00292-6
13. Orwa SA, Gudnadottir U, Boven A, et al. Global prevalence of antibiotic consumption during pregnancy: a systematic review and meta-analysis. J Infect. 2024;89(2):106189. doi:10.1016/j.jinf.2024.106189
14. Chae J, Choi JY, Kim B, Kim DS. Antibiotic use during pregnancy in south korea using 2011–2020 national health insurance claims data. Antibiotics. 2023;12(8):1242. doi:10.3390/antibiotics12081242
15. Sharma S, Chauhan A, Ranjan A, et al. Emerging challenges in antimicrobial resistance: implications for pathogenic microorganisms, novel antibiotics, and their impact on sustainability. Front Microbiol. 2024:15. doi:10.3389/fmicb.2024.1403168
16. Karnwal A, Jassim AY, Mohammed AA, Al-Tawaha ARMS, Selvaraj M, Malik T. Addressing the global challenge of bacterial drug resistance: insights, strategies, and future directions. Front Microbiol. 2025;16:1517772. doi:10.3389/fmicb.2025.1517772
17. Urinary Tract Infections in Pregnant Individuals. Available from: https://www.acog.org/clinical/clinical-guidance/clinical-consensus/articles/2023/08/urinary-tract-infections-in-pregnant-individuals.
18. Weinstock D. Guidance Update: diagnosis and management of PROM. The ObG project. Available from: https://www.obgproject.com/2017/12/29/acog-guidance-update-diagnosis-management-prom-prelabor-rupture-membranes/.
19. Prescribing antimicrobials in pregnancy and lactation. HSE.ie. Available from: https://www.hse.ie/eng/services/list/2/gp/antibiotic-prescribing/conditions-and-treatments/pregnancy-infections/prescribing-antimicrobials-in-pregnancy-and-lactation/prescribing-antimicrobial-in-pregnancy-and-lactation10-20.html.
20. Aoutil N, Cherkaoui M, Bouskraoui M. Prevalence and factors associated with the irrational use of antibiotics by pregnant women in the city of Marrakech, Morocco: a cross-sectional study. BMC Pregnancy Childbirth. 2025;25(1):990. doi:10.1186/s12884-025-08089-8
21. OpenEpi Menu. Available from: https://www.openepi.com/Menu/OE_Menu.htm.
22. ATCDDD - ATC/DDD Index. Available from: https://atcddd.fhi.no/atc_ddd_index/.
23. Rodrigues F, Coelho P, Mateus S, et al. Rising trends of urinary infections among pregnant women: insights from a Portuguese Hospital (2018–2022). Bacteria. 2025;4(1):10. doi:10.3390/bacteria4010010
24. Storme O, Tirán Saucedo J, Garcia-Mora A, Dehesa-Dávila M, Naber KG. Risk factors and predisposing conditions for urinary tract infection. Ther Adv Urol. 2019;11:1756287218814382. doi:10.1177/1756287218814382
25. Ghouri F, Hollywood A. Antibiotic prescribing in primary care for Urinary Tract Infections (UTIs) in pregnancy: an audit study. Med Sci. 2020;8(3):40. doi:10.3390/medsci8030040
26. Bruel H, Guillemant V, Saladin-Thiron C, Chabrolle JP, Lahary A, Poinsot J. Hemolytic anemia in a newborn after maternal treatment with nitrofurantoin at the end of pregnancy. Arch Pediatr. 2000;7(7):745–747. doi:10.1016/s0929-693x(00)80155-4
27. Matuszkiewicz-Rowińska J, Małyszko J, Wieliczko M. Urinary tract infections in pregnancy: old and new unresolved diagnostic and therapeutic problems. Arch Med Sci. 2015;11(1):67–77. doi:10.5114/aoms.2013.39202
28. Gamberini C, Donders S, Al-Nasiry S, Kamenshchikova A, Ambrosino E. Antibiotic use in pregnancy: a global survey on antibiotic prescription practices in antenatal care. Antibiotics. 2023;12(5):831. doi:10.3390/antibiotics12050831
29. Guimarães FS, Dal-Pizzol TDS, Silveira MPT, Bertoldi AD. Prevalence of systemic antibacterial use during pregnancy worldwide: a systematic review. PLoS One. 2024;19(9):e0309710. doi:10.1371/journal.pone.0309710
30. Andersen JT, Petersen M, Jimenez-Solem E, et al. Trimethoprim use in early pregnancy and the risk of miscarriage: a register-based nationwide cohort study. Epidemiol Infect. 2013;141(8):1749–1755. doi:10.1017/S0950268812002178
31. Abadie RB, Keller CL, Jones NT, et al. Review of teratogenic effects of leflunomide, accutane, thalidomide, warfarin, tetracycline, and angiotensin-converting enzyme inhibitors. Cureus. 2023;15(12):e50465. doi:10.7759/cureus.50465
32. Wiles K, Chappell L, Clark K, et al. Clinical practice guideline on pregnancy and renal disease. BMC Nephrol. 2019;20:401. doi:10.1186/s12882-019-1560-2
33. Roodbeen R, Vreke A, Boland G, et al. Communication and shared decision-making with patients with limited health literacy; helpful strategies, barriers and suggestions for improvement reported by hospital-based palliative care providers. PLoS One. 2020;15(6):e0234926. doi:10.1371/journal.pone.0234926
34. Vermeir P, Vandijck D, Degroote S, et al. Communication in healthcare: a narrative review of the literature and practical recommendations. Int J Clin Pract. 2015;69(11):1257–1267. doi:10.1111/ijcp.12686
35. Hironaka LK, Paasche-Orlow MK. The implications of health literacy on patient-provider communication. Arch Dis Child. 2008;93(5):428–432. doi:10.1136/adc.2007.131516
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Impact of Spondyloarthritis on Pregnancy Outcome: A Descriptive Analysis from a Specialized Center in Qatar
Al Emadi S, Hadwan NN, Saleh R, Satti E, Singh R
Open Access Rheumatology: Research and Reviews 2024, 16:21-29
Published Date: 22 January 2024
Experiences and Perspectives of Women Undergoing Oocyte Cryopreservation in Riyadh, Saudi Arabia: A Mixed-Methods Study
Alzahrani FA, Al-Jaroudi D, Alsufyan HA, Alzahrani AA, Alshehri SA, Jalwi S, Miskeen E
International Journal of Women's Health 2025, 17:879-895
Published Date: 22 March 2025