Back to Journals » Medical Devices: Evidence and Research » Volume 19
Evaluation of a Sprayable Hydrogel for Surgical Adhesion Prevention in Rat and Rabbit Models
Authors Costella LA ![]() , Johnson K
, Johnson K ![]() , Hassan R
, Hassan R ![]() , Villani M, Villani R, Tison CK
, Villani M, Villani R, Tison CK
Received 7 November 2025
Accepted for publication 23 January 2026
Published 11 February 2026 Volume 2026:19 574967
DOI https://doi.org/10.2147/MDER.S574967
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Mohamad Bashir
Lauren A Costella,1 Kate Johnson,1 Rick Hassan,1 Mario Villani,2 Rosanna Villani,2 Christopher K Tison1
1Biotech Division, Luna Labs USA, LLC, Charlottesville, VA, USA; 2DaVINCI Biomedical Research Products, Lancaster, MA, USA
Correspondence: Lauren A Costella, Biotech Division, Luna Labs USA, LLC, 706 Forest St, Suite A, Charlottesville, VA, 22903, USA, Tel +14342209441, Email [email protected]
Purpose: To evaluate the effectiveness of a sprayable adhesion barrier in the prevention of postoperative adhesions.
Methods: Established rat and rabbit models of abdominal adhesion formation were used to evaluate AeroVeil efficacy. First, 24 Sprague-Dawley rats were randomly assigned to untreated control, Seprafilm-treated, or AeroVeil-treated test groups. Defects were created on abdominal wall and cecum surfaces, with sutures around the injury perimeter to increase the likelihood of adhesion formation. Treated animals were sprayed with recommended AeroVeil dosing over both injured surfaces; a Seprafilm sheet was placed between the two injured surfaces; control animals received no treatment. Additionally, AeroVeil application was compared to untreated controls in 24 New Zealand White rabbits. The abdominal wall and cecum surfaces were abraded to induce adhesion formation. AeroVeil animals were treated with the recommended product dose over both injured tissue sites; control animals were closed without treatment.
Results: The incidence, extent, and severity of postoperative adhesion formation were measured by blinded veterinary surgeons at 7 or 28 days. In the rat model, control animals formed adhesions between the cecum and abdominal wall injury sites in 7 of 8 animals. Incidence of this primary adhesion significantly reduced (p < 0.05) to 1 of 8 in Seprafilm-treated animals and 0 of 7 in AeroVeil treated animals, with similarly significant reduction in the extent and severity scores. In the rabbit model, application of AeroVeil decreased the incidence of adhesion formation, with a statistically significant decrease in total adhesion score across all tissue groups.
Conclusion: AeroVeil application reduced the incidence and severity of postoperative adhesion formation in two different animal models, with results in the rat model directly compared to an established clinical control (Seprafilm). These findings justify further investigation of AeroVeil in expanded animal models to facilitate clinical translation.
Plain Language Summary: A sprayable hydrogel has been demonstrated to form a barrier to postoperative adhesion formation, with effectiveness established in both rat and rabbit models.
Keywords: hydrogel, postoperative adhesion, chitosan, alginate, sprayable
Introduction
Postoperative adhesions are considered an unavoidable consequence and expected outcome of most operations.1 Local inflammation and fibrin accumulation in areas devoid of mesothelial cells with a corresponding loss in fibrinolytic activity during wound healing results in the formation of fibrous bands of scar tissue, capturing fibroblasts and mesothelial cells to form a firm, vascularized adhesion between adjacent tissues.1–3 The clinical implications are significant; adhesions are a leading cause of postoperative pain and responsible for up to 40% of all infertility cases, 60% of intestinal obstructions, and increasing difficulty in subsequent surgeries.3
There is a specific need for adhesion prevention in the gynecology sector. Pelvic adhesion formation has been reported after 65% of cesarean deliveries, leading to infertility, pain, and increased delivery times in subsequent births.4–7 Adhesiolysis, or the removal of adhesions, is 12 times more common during a repeat cesarean as compared to a primary procedure and doubles the risk of cesarean hysterectomy.6,8 The inpatient burden of adhesiolysis is also significant, with expenditures exceeding $2.5 billion each year and over 46% of cases involving the female reproductive tract.1,6 Though the incidence of adhesion formation is reduced in laparoscopic procedures, the total disease burden remains as high as 70% and will increase the complexity of follow-up procedures if not appropriately addressed.3
Despite clinical acceptance that adhesions cause significant complications, there are no widely adopted prevention mechanisms, with less than 15% of surgeons reporting use of an adhesion barrier product within the last year.9,10 Most existing products, including Seprafilm® (Baxter) and Interceed® (Ethicon), take the form of solid barrier films placed between injured tissues. This physical barrier prevents the formation of fibrous bands between neighboring tissues during the early phases of wound healing, allowing tissue surfaces to heal independently. However, these existing FDA-approved adhesion barrier products are not approved for laparoscopic application and are notoriously difficult to handle or apply over curved tissue surfaces, limiting application around the primary incision site and leaving the bulk of the abdominal cavity susceptible to adhesion formation.10 A sprayable hydrogel barrier applied to internal tissue surfaces prior to surgical closure could conform to tissue surfaces to maintain a physical barrier between healing tissues during the adhesion-formation window. As no such sprayable products have been approved by the FDA for adhesion prevention, the AeroVeil formulation has been developed as a novel adhesion barrier for preliminary evaluation in small animal models to support transition towards larger preclinical validation studies.
Materials and Methods
AeroVeil is comprised of two biopolymers, chitosan and alginate, that mimic the native extracellular matrix and have established biocompatibility profiles for medical use.11,12 Polycationic chitosan interacts with polyanionic alginate immediately upon mixing to form a polyelectrolyte complex. The inclusion of ionic crosslinkers further serves to enhance the stability of the resultant hydrogel structure. For functional application as an adhesion-prevention barrier, the hydrogel is applied in a thin coating over the target tissue surface using commercially available mixing tips (SA-3652, Nordson Medical) and sprayed with 12 psi carbon dioxide (CO2). This sprayable application enables controlled coating of the target tissues in a thin layer that provides barrier function while maintaining an appropriate resorption timeline. Iterative benchtop characterization in parallel with in vivo evaluation enabled optimization of the top-performing formulation. Study protocols for rat and rabbit studies were approved by DaVINCI Biomedical Research Products (Boston, MA) IACUC prior to study initiation.
Hydrogel Components
trūChitosan (MW 300 kDa, DA 95%) was reacetylated with acetic anhydride (Oakwood Products, Inc.) to form in a water-soluble chitosan product with a degree of deacetylation of 50% ± 5 by manufacturing partners at Parimer Scientific.12,13 The final molecular weight and degree of deacetylation were characterized using Gel Permeation Chromatography and Nuclear Magnetic Resonance Spectroscopy according to USP reference standards. Other components sourced at USP grade included sodium alginate (Spectrum Chemical, MW 222 kDa), sodium tripolyphosphate (NaTPP, Spectrum Chemical), calcium chloride (CaCl2, VWR), methylene blue (Sigma Aldrich), and sodium benzoate (C7H5NaO2,JT Baker). All other materials were sourced from VWR at analytical grade.
Formulation Preparation
AeroVeil is comprised of aqueous chitosan and alginate solutions, formulated and sterile filtered at Parimer Scientific. The specific components and rationale behind the incorporation of each are presented in Table 1. Solution 1 is an aqueous solution containing 1.5% w/v water-soluble chitosan with 1.5% w/v CaCl2 (an ionic crosslinker for sodium alginate). Solution 2 contains an aqueous solution of 0.5% w/v sodium alginate, 1.5% NaTPP (an ionic crosslinker for chitosan), and 0.01% w/v methylene blue dye for visualization. Both solutions also contain 0.1% sodium benzoate as a preservative. Each solution is sterile filtered through a 0.22 µm filter, drawn in plastic syringes (Becton Dickenson, 5 mL), and externally sterilized using ethylene oxide. Sterility was confirmed for 6 months per USP <71>, ensuring the solutions were free of viable microorganisms.
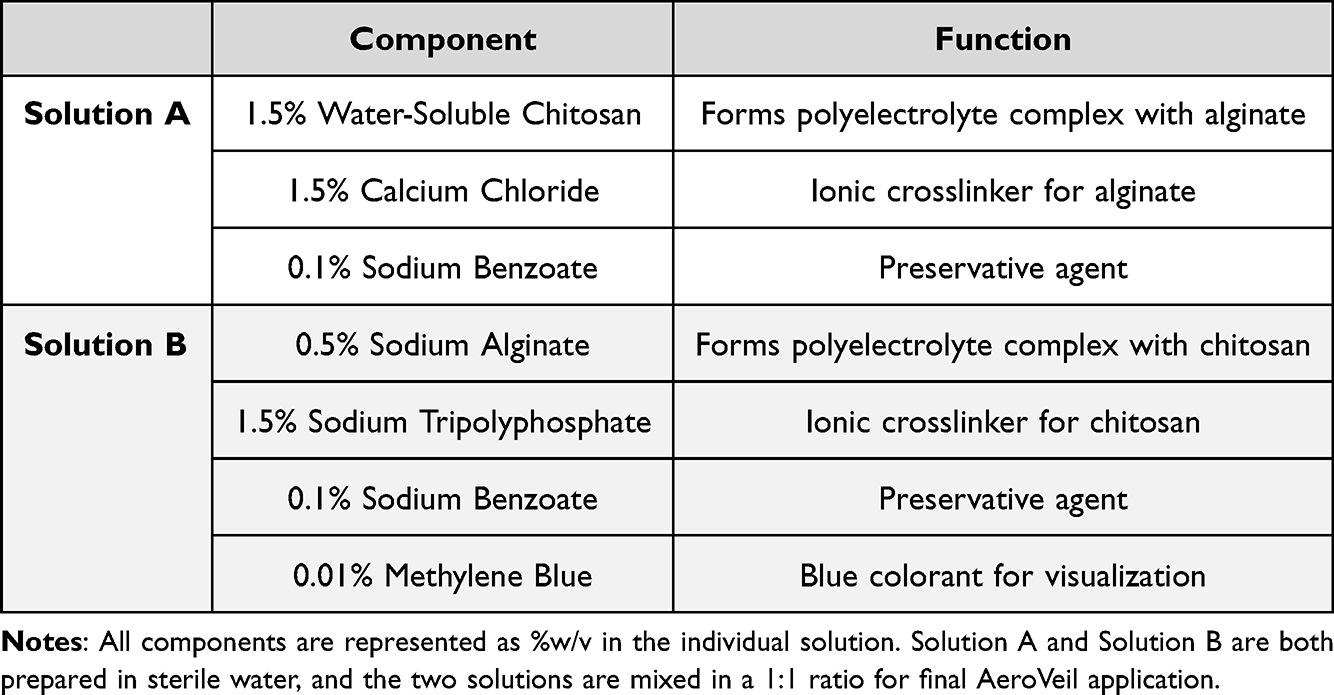 |
Table 1 AeroVeil Formulation Components |
Solution viscosity requires pressurization >10 psi to achieve proper mixing and aerosolization during delivery. Compatibility of the gelation reaction with CO2 is critical for laparoscopic use, which was used for these studies. The selected mix tip (Nordson FibriJet SA-3652) contains two luer-lock ports for the solutions with individual channels that do not mix the components or the pressurized gas until the end of the spray nozzle (Figure 1). AeroVeil forms a robust hydrogel immediately upon mixing, so delaying mixing until immediately prior to application prevents crosslinked hydrogel from clogging the spray tip.
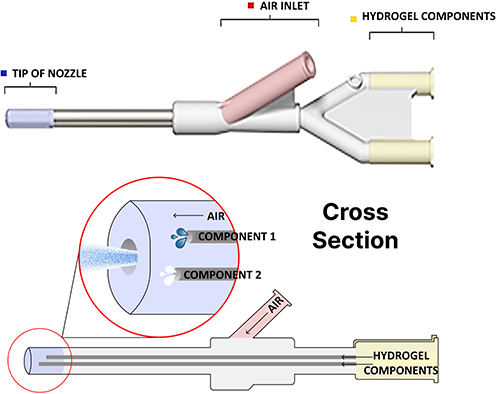 |
Figure 1 Schematic of spray tip used to deposit AeroVeil over tissue surface. Hydrogel components are kept separate until they reach the tip of the nozzle, where they are mixed and aerosolized with the compressed gas, set to 12 psi. |
Product dosage for this sprayable hydrogel is defined as a volume of hydrogel applied over a target area, which correlates directly to hydrogel thickness. The volume applied over the treatment area was recorded in preliminary animal models to determine the target product dosage for the instructions for use, with specific feedback and application data provided by practicing clinicians who were instructed to apply a thin coating over the target tissue. This resulted in a target identified dose of 0.1 mL/cm2, approximating a hydrogel thickness of 1 mm over the tissue surface. Preliminary biocompatibility evaluation of the final formulation was completed according to ISO-10993 to establish the safety of the final formulation for in vivo administration.
Benchtop Characterization
The concentration of each component in AeroVeil was identified based on preliminary benchtop testing to evaluate effects of concentration on solution viscosity, gelation kinetics, and tissue adhesion by spraying over bovine liver tissue warmed to 37 °C and bringing coated tissue surfaces in direct contact to assess gel displacement. These qualitative metrics were used in parallel with unpublished early animal model results to down-select to the final formulation detailed in Table 1. This final formulation was used for all subsequent evaluation, including the animal models described below.
Shelf-stability and gelation kinetics of the final formulation were assessed using oscillating rheometry (Anton Paar MCR-92) to confirm polymeric stability. Individual solutions were tested by creating a viscosity flow curve using a parallel plate setup (25 mm diameter, 1 mm gap) at 25 °C. Applied shear was increased logarithmically from 0.1–100 Hz while the corresponding viscosity (mPa-s) was measured. Hydrogel crosslinking function was measured via an amplitude sweep using a parallel plate setup (25 mm diameter, 0.1 mm gap) at 37 °C. AeroVeil solutions were sprayed over the plate surface through the FibriJet mixing tip according to the product instructions for use. The hydrogel structure forms immediately after mixing under CO2 pressure. Shear strain was increased logarithmically from 0.01–1000% at a constant frequency of 1 Hz as the Anton Paar system plotted the corresponding Storage and Loss Modulus values.
An initial assessment of hydrogel degradation was performed by measuring mass loss over time in simulated body fluid containing lysozyme. Hydrogel samples were submerged in saline solutions containing 1.5 µg/mL lysozyme and stored at 37 °C without agitation to simulate exposure to peritoneal fluid. Individual test specimens (n=3) were evaluated at Day 0, 1, 3, 7, 14, and 28. Solutions were filtered (0.22 µm) and dried to acquire the mass of hydrogel remaining. Average mass loss was plotted over time as an initial assessment of hydrogel degradation kinetics.
Rat Model of Surgical Adhesion
A rat abdominal adhesion model was used to evaluate the ability of AeroVeil formulations to prevent intra-abdominal adhesion formation.14–16 Blinded surgeons used an established scoring system to quantify the incidence, severity, and extent of peritoneal adhesions 7 days after surgery to assess AeroVeil treatment compared to untreated and Seprafilm-treated controls. Seprafilm (sodium hyaluronate and carboxymethylcellulose bioresorbable film) is recognized as the standard of care for postoperative adhesion formation after abdominal/pelvic surgeries.17 The 7 day time point is considered appropriate for an early evaluation of adhesion incidence as adhesions initially form within the first 3–5 days after surgery, though severity may continue to increase over time and symptoms may take longer to appear.1,2
Surgical defects were created on adjacent abdominal wall and cecum surfaces of 24 female Sprague Dawley rats (226–250 g, Charles River, Stone Ridge, NY) to induce adhesion formation between the two surfaces in untreated controls. The number of animals per group (n=8) was determined based on prior experience with the model at DaVINCI and data published in the literature, with these prior results providing confidence in achieving statistically significant results between control and test animals at these sample sizes.
Animals were anesthetized using isoflurane (2.5%) and prepped for aseptic surgery. A midline laparotomy was performed and the cecum was exteriorized and abraded with sterile gauze to create sub-serosal hemorrhages. A 1 cm x 2 cm section of the peritoneum was excised from the left side of the abdominal wall, and eight silk sutures were placed around the circumference of the defect to increase the likelihood of adhesion formation (Figure 2).
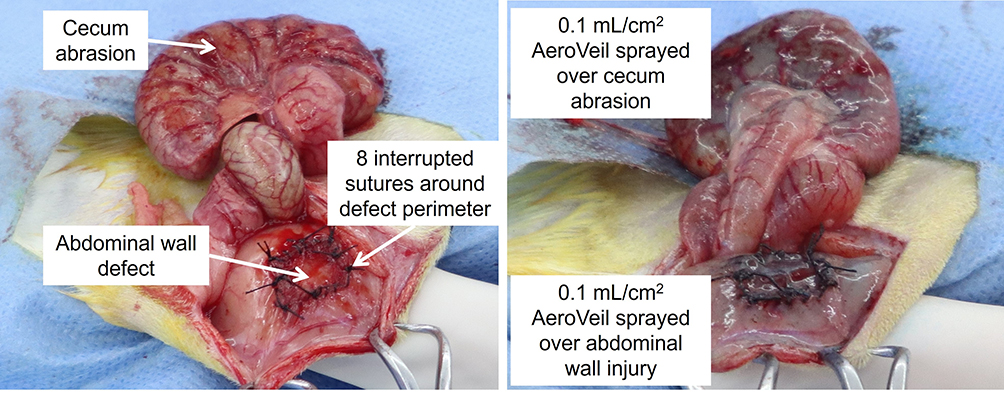 |
Figure 2 Representative images of adhesion model injury and AeroVeil application in a rat model. Left: Placement of 8, 6–0 silk, single suture knots at the border of the defect area on the abdominal wall and cecum after the induction of petechial bleeding via surface abrasion; Right: Injury sites following AeroVeil treatment, prior to closure. |
Animals were randomly allocated to control or treatment groups. N=8 control animals were closed without treatment, with wounds aligned upon closure such that adhesions were apt to form between the two surfaces. In treated animals, a 2×3 cm piece of Seprafilm was placed to cover the abdominal injury site and surrounding perimeter (N=8), or AeroVeil was sprayed over the surface of both injury sites (target dose, 0.1 mL/cm2) prior to closure. The incision was closed routinely, and animals recovered with twice-daily clinical wellness evaluations.
Surviving animals were euthanized using CO2 after 7 days. The defect site was exposed and observed for macroscopic evidence of reactivity or inflammation. Adhesions were evaluated by a blinded veterinary surgeon for the extent (0–4) and severity (0–3) of adhesions, which were summed for a total score of 0–7. Adhesions scored between the abdominal wall injury site to the cecum injury site were denoted as the “primary adhesion” that this model is designed to create. However, it was noted that “secondary adhesions” from either injury site to the surrounding visceral tissue were apt to form, particularly in instances where the primary adhesion was prevented. These secondary adhesions from the abdominal wall to the surrounding viscera and from the cecum to surrounding viscera were also scored for a more comprehensive analysis of efficacy. The total score for each animal was represented out of 21 (0–7 for each adhesion type).
Rabbit Model of Surgical Adhesions
AeroVeil performance was also assessed in a rabbit model (New Zealand White Rabbits, 8–11 months age, 3–4 kg, Covance Research Product, Denver PA).18,19 Twenty-four animals were randomized across control (untreated) and AeroVeil treatment groups, N=12 each. Animals were anesthetized with an injection of Ketamine (40 mg/kg), Acepromazine (0.5 mg/kg), and Glycopyrrolate (0.01 mg/kg), intubated, and maintained with isoflurane (0.5–3%) while prepped for aseptic surgery. A midline laparotomy was performed, and the cecum and bowel were exteriorized to enable abrasion of the ventral and intestinal surfaces to induce petechial bleeding over a 5 cm x 10 cm surface area. The cecum and bowel were returned to their anatomic position, and a 3×5 cm area of the peritoneum with underlying fascia was removed on the right lateral abdominal wall (Figure 3). In treated animals, AeroVeil was applied over the two injury sites at ~0.1 mL/cm2. The abdomen was closed in a routine manner using 4–0 polyethylene suture, and rabbits were recovered for twice daily observations.
 |
Figure 3 Representative images of adhesion model injury and AeroVeil application in a rabbit model. Left: Petechial bleeding represents creation of cecal abrasion and sidewall defect injuries; Right: Post-AeroVeil treatment sprayed over cecum and sidewall injury sites, immediately prior to closure. |
Eight animals from each group were survived 7 days and four animals from each group were survived 28 days. The n=8 sample size was defined to enable a statistical analysis of treatment effects, while the smaller evaluation at 28 days was designed to provide a preliminary visualization of in vivo degradation timelines. Animals were euthanized via injection with sodium pentobarbital. Extent (0–4), severity (0–4), and strength (0–3) of peritoneal adhesions were evaluated by blinded, trained personnel using a standard scoring system that assessed adhesion incidence and score across three tissue pairs – cecum to incision site, cecum to sidewall, or cecum to itself.19
Statistical Analysis
For both animal models, Fishers Exact Test was used to calculate statistical significance of changes in adhesion incidence. The Mann–Whitney U-test was used to assess differences in adhesion scores, with treatment groups compared directly to untreated controls. P-values below 0.05 were used to establish significance.
Results
Formulation Optimization
Benchtop characterization and early animal testing were used to select the final component concentrations (Table 1), and clinician input was used to identify 0.1 mL/cm2 (ie, 1 mm thick) as the target dosage for AeroVeil application. An oscillating rheometer was used to quantify solution viscosity and gelation kinetics and to establish AeroVeil gelation and stability. A viscosity flow curve (0.1–100 Hz) established that both polymer solutions are shear thinning, with viscosities between 100–125 (Solution 1) or 50–75 (Solution 2) mPa*s at rates exceeding 1 Hz. An amplitude sweep (1 Hz, strain 0.01–1000%) was used to characterize the sprayed hydrogel, which demonstrated a storage modulus of ~1500 Pa in the linear viscoelastic region at low strain rates before the gel began to yield. These rheometric properties were stable over the course of component storage (6 months at room temperature), with gelation kinetics maintained within 10% initial values to confirm product stability.
Formulations were submerged in saline solutions with 1.5 µg/mL lysozyme and stored at 37 °C to discern hydrogel degradation timelines. Mass loss calculated at various intervals revealed >90% of the hydrogel was degraded within 28 days, demonstrating bulk hydrogel degradation that will enable subsequent clearance and excretion through standard pathways. Hydrogel degradation kinetics will ultimately be validated in vivo.
AeroVeil Evaluation in Rat Model
One animal in the AeroVeil treatment group was found dead 48 hours after surgery with skin biting indicative of unexplained intrabdominal discomfort, but the remaining animals completed the full survival period. The extent, tenacity, and type of adhesions formed between the cecum and abdominal wall were evaluated and assigned ordinal scores. All surviving animals appeared healthy, and 7 of 8 (88%) control animals exhibited primary adhesions, establishing the severity of the model. 1 of 8 Seprafilm-treated and 0 of 7 animals treated with AeroVeil formed the primary adhesions the model was designed to create. Two AeroVeil-treated animals were completely free of adhesions, but secondary adhesions between the abdominal wall and surrounding healthy visceral tissue were observed in 5 of 7 animals. This was similar to Seprafilm-treated animals, where 3 of 8 animals were free of adhesions, but secondary adhesions were observed in 4 animals.
The average total score for primary abdominal to cecum injury adhesions in control animals was 5.8±2.4, but decreased to 0.4±1.1 in Seprafilm-treated animals and was 0.0 following AeroVeil treatment. Both treatments were statistically significant to untreated controls (p<0.005). The decrease in primary adhesion incidence between untreated control (88%) to Seprafilm (12.5%) and AeroVeil (0.0%) was also statistically significant (p=0.01 Seprafilm; p=0.001 AeroVeil). The incidence of secondary adhesions to the abdominal wall was 50% in control animals (total score 1.8±1.9), 50% in Seprafilm group (score 1.3±1.5) and 71.4% in the AeroVeil treated animals (score 2.9±2.6). Secondary adhesions to the cecum occurred in 75% of control animals (total score 2.3±1.8) and 25% of Seprafilm animals (0.8±1.5), but none were observed in AeroVeil-treated animals (score 0.0, significant p≤0.015). Total adhesion incidence dropped from 100% in controls to 62.5% and 71.4% in Seprafilm and AeroVeil treatment groups, respectively, with statistically significant (p<0.002) decreases in total adhesion score from 9.8±1.7 in the untreated control to 2.4±2.7 (Seprafilm) and 2.9±2.6 (AeroVeil). Results are presented in Table 2 and Figure 4.
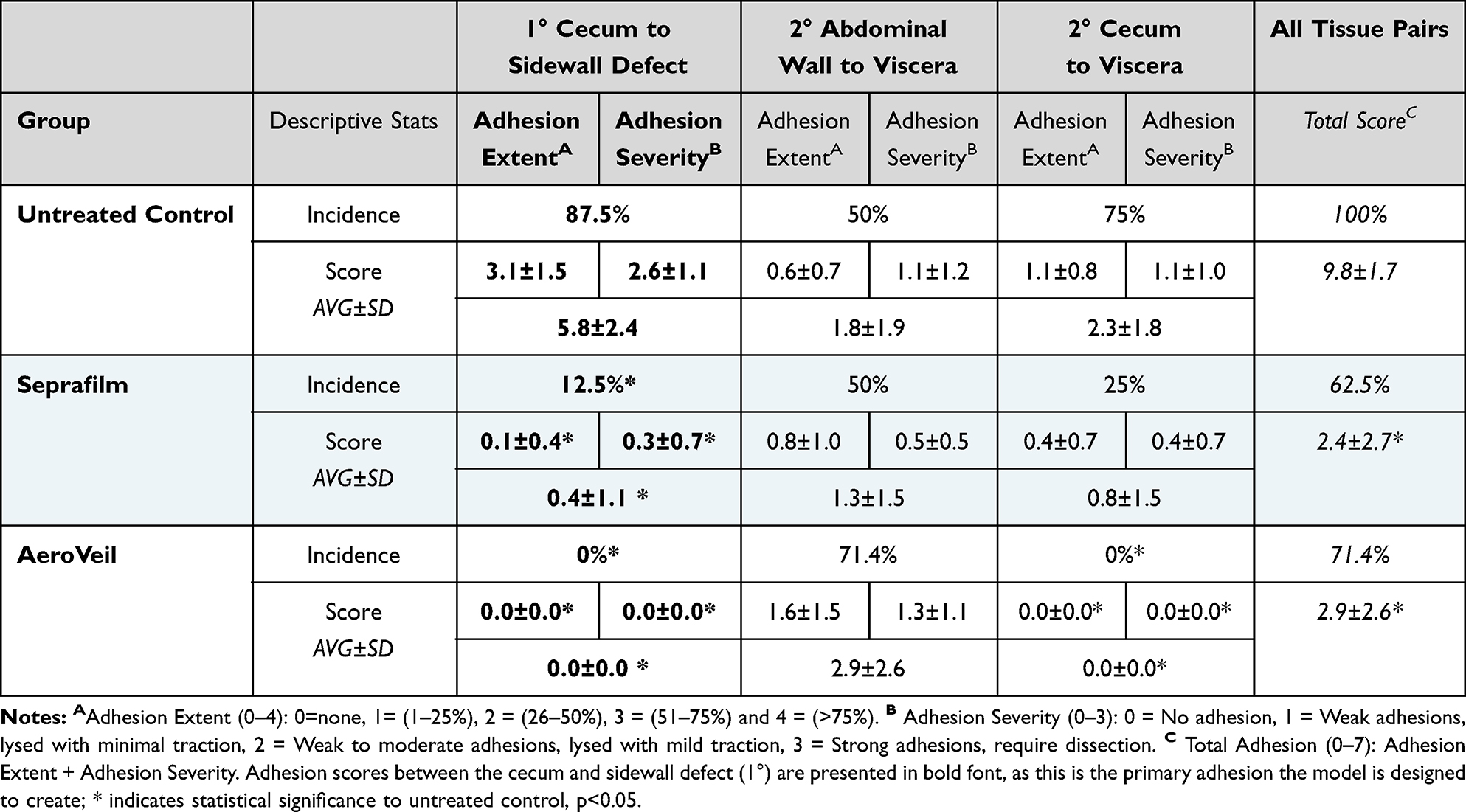 |
Table 2 Rat Model Results – Adhesion Incidence and Score |
 |
Figure 4 Results demonstrating AeroVeil application results in adhesion prevention in a rat model. Representative images in which primary adhesion between highlighted injury sites was (a) prevented with AeroVeil application, versus (b) untreated controls; Yellow arrows highlight injured tissue surfaces for evaluation in the model. (c) AeroVeil application resulted in statistically significant decreases in the incidence of adhesions between the cecum and sidewall (1°) and viscera (2°) surfaces, with a slight increase in 2° adhesions to the abdominal sidewall; (d) Primary adhesion scores were significantly reduced with the application of Seprafilm or AeroVeil treatment as compared to untreated controls. Asterisks (*) indicate statistical significance as compared to untreated control, p<0.05. |
AeroVeil Evaluation in Rabbit Model
Eight animals from each group were survived 7 days and four animals from each group were survived 28 days to visualize tissue response to hydrogel presence. Adhesion scoring utilized an established peritoneal tissue adhesion scoring system to assess the severity (scale 0–4), extent of total area (scale 0–4) and strength (scale 0–3) of adhesions that formed, with the incidence of adhesions specified across three tissue pairs – cecum to incision site, cecum to sidewall, or the cecum to itself. Representative images are shown in Figure 5.
 |
Figure 5 Representative images of adhesion formation at analysis in rabbit model. (Top) Representative image of adhesions formed from Cecum to Incision, Cecum to Sidewall, Cecum to Cecum Adhesion/Injury sites as viewed in untreated controls shown above AeroVeil treated samples (Bottom) Representative images of clear injury sites visualized at Day 7 with AeroVeil treatment. |
Adhesion incidence and severity was assessed across all tested animals in each group (N=12), shown in Table 3 and Figure 6; decreased incidence associated with AeroVeil application was observed for all tissue pairs. The primary cecum to sidewall adhesion occurred in 9 of 12 (66.7%) untreated controls and 2 of 12 AeroVeil-treated animals (16.7%), representing a significant decrease (p=0.04). Cecum to incision adhesions occurred in 5 of 12 of untreated controls and 1 of 12 AeroVeil treated animals, and the cecum adhered to itself in 100% of untreated controls and 58.3% of AeroVeil animals (p=0.04). Total incidence of adhesion formation was reduced from 100% in untreated controls to 33.3% in AeroVeil-treated animals.
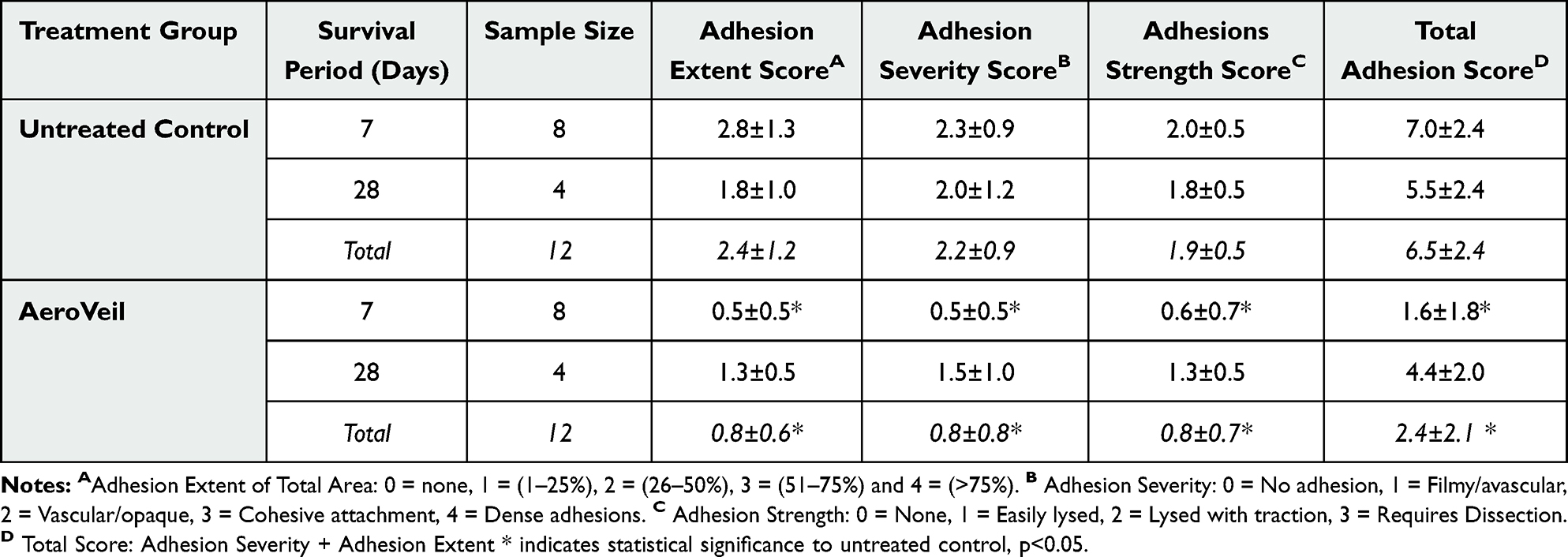 |
Table 3 Rabbit Adhesion Scoring Summary |
 |
Figure 6 Results demonstrating AeroVeil application results in adhesion prevention in a rabbit model. Representative images in which adhesions to the injured cecum were (a) prevented with AeroVeil as compared to (b) untreated control. Yellow arrow highlights injured tissue surfaces for evaluation in the model. (c) AeroVeil reduced the incidence and severity of adhesion formation as compared to untreated controls (N=12), with statistically significant decreases in the incidence of adhesions cecum to sidewall and cecum to cecum. (d) Average adhesion scores for extent, severity, and strength all decreased significantly, resulting in a 50% decrease in total adhesion score. Asterisks (*) indicate statistical significance as compared to untreated control, p<0.05. |
Average adhesion scores also decreased significantly across all categories. The extent, severity, and strength scores respectively decreased from 2.4±1.2, 2.2±0.9, and 1.9±0.5 in controls to 0.8±0.6, 0.8±0.8, and 0.8±0.7 in AeroVeil-treated animals. Total adhesion score dropped from 6.5±2.4 to 2.4±2.1 with the application of AeroVeil. All of these results were significant, p<0.02.
Evaluating discrete timepoints (Figure 7), AeroVeil-treated animals demonstrated reduced scores for adhesion extent (AeroVeil 0.5±0.5; control 2.8±1.3), severity (AeroVeil 0.5±0.5; control 2.3±0.9) and strength (AeroVeil 0.6±0.7; control 2.2±0.5) on Day 7, with significance p≤0.005. Adhesion incidence (100% control) was reduced to 50% in AeroVeil treated animals. Adhesions that formed in AeroVeil treated animals were qualitatively small, filmy, and easily lysed. Day 28 results also supported AeroVeil treatment, with reduced adhesion scores and incidence as compared to the control group for all-scoring metrics, though statistical significance was lost due to low sample size. AeroVeil-treated animals demonstrated reduced scores for adhesion extent (AeroVeil 1.3±0.5; control 1.8±1.0), severity (AeroVeil 1.5±1.0; control 2.0±1.2) and strength (AeroVeil 1.3±0.5; control 1.8±0.5) at Day 28. Though gel remnants were observed at Day 7, there was no sign of gel presence at 28 days, providing in vivo support that the hydrogel had degraded.
 |
Figure 7 Supplemental results from the rabbit model summarize differences at time points. Statistically significant decreases in adhesion scores were observed at Day 7 (N=8), though these decreases were not significant at Day 28 due to a smaller sample size (N=4). Asterisks (*) indicate statistical significance as compared to untreated control, p<0.05. |
Discussion
AeroVeil is a hydrogel comprised of water-soluble chitosan and sodium alginate developed to decrease the incidence and severity of postoperative adhesions. The sprayable nature of this design is proposed to enable application within tight spaces between tissues and conformation to irregular tissue shape, and the inclusion of methylene blue dye will support visualization of application to ensure even coverage across the entire injured tissue surface. Benchtop testing showed that the sprayed application of hydrogel layers <5 mm thick remained in place over the applied tissue surfaces, with in vivo implementation by practicing clinicians informing a target thickness of 1 mm (dosage 0.1 mL/cm2). AeroVeil has been demonstrated biocompatible according to standard ISO testing, and the hydrogel will naturally degrade over 28 days, maintaining integrity as a physical barrier to adhesion formation during the critical window (3–7 days after surgery).1–3 These properties indicate that AeroVeil could be particularly well suited for application following gynecologic procedures or cesarean deliveries to prevent postoperative adhesion formation and improve uterine healing outcomes. The product was applied by surgeons with minimal training, and consistent performance was observed across all test groups.
Preliminary safety and efficacy of AeroVeil application was evaluated in established models of adhesion formation in rats and rabbits.14,15,17–19 These models were also used in the preliminary evaluation of Seprafilm prior to clinical translation and have been well established in the evaluation of adhesion prevention products.18–20 In the rat model, AeroVeil performed similar to or better than the predicate device (Seprafilm) in preventing adhesion formation. Treatment effectively prevented primary adhesion formation between the abdominal wall and cecum injury sites, which the model is designed to create and is the definitive metric of efficacy (Figure 4). However, the prevention of these primary adhesions exposed the potential for the formation of secondary adhesions between the injury sites and other internal tissues not protected by AeroVeil (Figure 8). These secondary adhesions were also scored for a more comprehensive analysis of product efficacy in vivo. There was no statistical change in the incidence, extent, or severity of secondary adhesions to the abdominal wall across treatment groups, likely caused by the abdominal wall suture ends irritating the untreated liver surface, resulting in secondary adhesion formation in some animals. In clinical practice, all sites at risk of adhesion formation would be covered to expand protection as seen in the cecum, which did not form secondary adhesions with AeroVeil treatment. AeroVeil treatment reduced total adhesion incidence similar to Seprafilm, with a significant decrease in the average total postoperative adhesion score (extent + severity) observed for both groups as compared to untreated controls. Treatment sites were observed macroscopically at the time of analysis by a surgeon blinded to treatment group for changes in wound healing or inflammatory response. No differences in tissue response were observed, regardless of treatment group.
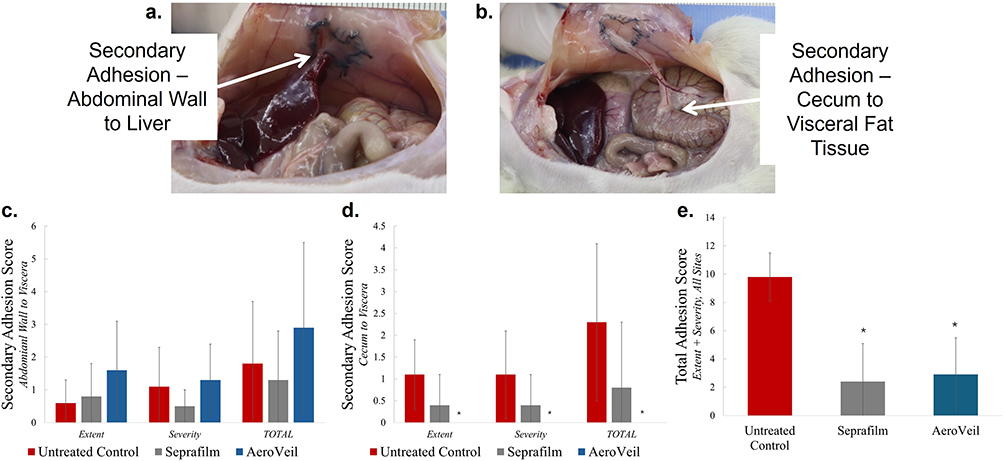 |
Figure 8 Supplemental results from the rat model examine the incidence and severity of secondary adhesion formation. (a) Representative image of secondary (2°) adhesion between the abdominal wall and surrounding viscera (eg, liver) in AeroVeil-treated animal; (b) Representative image of 2° adhesion between cecum and visceral tissue; (c) Secondary adhesions to the abdominal wall were observed across all control and treatment groups; (d) AeroVeil prevented secondary adhesions to the cecum surface; (e) AeroVeil was statistically similar to Seprafilm in reducing total adhesion score across all tissue pairs. Asterisks (*) indicate statistical significance as compared to untreated control, p<0.05. |
After establishing performance comparable to Seprafilm in rats, AeroVeil effectiveness was further evaluated in a rabbit model. 8 animals from each group were analyzed at day 7, while an additional 4 animals were survived to 28 days for an initial assessment of hydrogel degradation rate. Test groups were analyzed together (n=12) as well as separately across the 7 and 28 day timepoints. Compiled results (n=12) showed that AeroVeil treatment decreased incidence and adhesion scores across all tissue pairs (cecum to midline incision, cecum to abdominal wall, and cecum to itself) over 28 days (Figure 6). At gross necrospy, AeroVeil-treated animals demonstrated significantly reduced scores for adhesion extent, severity, and strength as compared to untreated controls. Adhesions that did form in treated animals were thin, filmy, and easily lysed (Figure 5). Notably, a single animal within the AeroVeil-treated group (28 days) accounted for a majority of the adhesions observed in this subset (Figure 7). Overall, total adhesion incidence was reduced from 100% in controls to 67% across all treated animals, with statistically significant decreased adhesion scores confirming effectiveness of AeroVeil. Macroscopic evaluation of the injury sites showed comparable wound healing to untreated controls, and there were no indications of localized or systemic toxicity or inflammatory response induced by hydrogel application over the wounded tissue in any animals. Coupled with preliminary biocompatibility validation, including acute systemic toxicity, pyrogenicity, genotoxicity, and tissue implantation analysis, these results support product safety for continued translation to clinical evaluation.
Conclusion
AeroVeil application resulted in a decrease in the incidence of primary adhesions between the injured cecum and abdominal wall in both models, and statistically significant improvements in overall adhesion score were observed across most scoring pairs for all treated animals as compared to untreated controls. These results indicate that AeroVeil may be equally or more effective than the current standard of care, and the sprayable form factor could enable transition to other indications (including minimally invasive procedures), with the potential to improve clinical outcomes following surgical intervention. Additional large animal studies are required with a thorough evaluation of systemic and local tissue response and hydrogel resorption to facilitate clinical translation.
Research Involving Vertebrate Animals
All animal procedures cited in this manuscript were conducted in strict compliance with the US Federal Animal Welfare Act and the regulations of the Office of Laboratory Animal Welfare (OLAW) under the National Institutes of Health (NIH). Each of the protocols for the studies involving Sprague Dawley rats and New Zealand White rabbits were reviewed and approved by the Institutional Animal Care and Use Committee (IACUC) at DaVINCI Biomedical Research Products. The rat protocol was approved under IACUC #DB-786 and OLAW Inter-Institutional Assurance #X23-01975-003. The rabbit protocol was approved under IACUC #DB-545and OLAW IIA #A1618-37.
All animal care and experimental procedures adhered to the standards set forth in the Guide for the Care and Use of Laboratory Animals: Eighth Edition (National Academies Press), with maximum effort to minimize undue suffering. Humane endpoints consistent with these guidelines were also predefined prior to each study.
All animals received appropriate analgesic care and were continuously monitored for signs of distress. Anesthesia was induced and maintained according to DaVINCI SOP DAV-SURG-003. Specifically, for the rat study anesthesia was induced in a chamber filled with isoflurane at 2.5%-4%. After induction, anesthesia was maintained with isoflurane delivered through a nose cone at 0.5–2.5%. Rabbits were pre-anesthetized with an injection of Ketamine (40 mg/kg), Acepromazine (0.5 mg/kg), and Glycopyrrolate (0.01 mg/kg); animals were then intubated and maintained under anesthesia with isoflurane at 1–2% delivered through a precision vaporizer on a non-rebreathing system. Euthanasia was performed at the conclusion of each study via lethal intravenous injection of sodium pentobarbital (150 mg/kg), according to the established guidelines from the American Veterinary Medical Association (AVMA) for the Humane Euthanasia of Animals.
Funding
Research reported in this publication was supported by the National Institute Of General Medical Sciences of the National Institutes of Health under Award Numbers R44GM105142 and R43GM144991, and the Eunice Kennedy Shriver National Institute Of Child Health & Human Development of the National Institutes of Health under Award Number R44HD114305. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Disclosure
Lauren Costella, Kate Johnson, Rick Hassan, and Christopher Tison are all employees of Luna Labs USA, LLC, maker of AeroVeil. Christopher Tison is also part-owner of Luna Labs USA, LLC.
Mario Villani and Rosanna Villani are employees of DaVINCI Biomedical Research Products, which was hired by Luna Labs USA, LLC as a contract research organization to complete the tests presented in this paper. Mrs Lauren Costella has a patent US 11,623,029 issued to Luna Labs USA, LLC, a patent EP 3606572 issued to Luna Labs USA, LLC, a patent CN 110494172 issued to Luna Labs USA, LLC. Ms Kate Johnson reports grants from Eunice Kennedy Shriver National Institute Of Child Health & Human Development of the National Institutes of Health, during the conduct of the study. Dr Christopher Tison has a patent US 11,623,029 issued to Luna Labs USA, LLC, a patent EP 3606572 issued to Luna Labs USA, LLC, a patent CN 110494172 issued to Luna Labs USA, LLC. The authors report no other conflicts of interest in this work.
References
1. Fatehi Hassanabad A, Zarzycki AN, Jeon K, Deniset JF, Fedak PWM. Post-operative adhesions: a comprehensive review of mechanisms. Biomedicines. 2021;9(8):867. doi:10.3390/biomedicines9080867
2. Lauder CIW, Garcea G, Strickland A, Maddern GJ. Abdominal adhesion prevention: still a sticky subject? Dig Surg. 2010;27(5):347–13. doi:10.1159/000314805
3. Capella-Monsonís H, Kearns S, Kelly J, Zeugolis DI. Battling adhesions: from understanding to prevention. BMC Biomed Eng. 2019;1(1):5. doi:10.1186/s42490-019-0005-0
4. Penzias A, Bendikson K, Falcone T. Practice committee of the American society for reproductive medicine in collaboration with the society of reproductive surgeons. Postoperative adhesions in gynecologic surgery: a committee opinion. Fertil Steril. 2019;112(3):458–463. doi:10.1016/j.fertnstert.2019.06.027
5. Practice Committee of the American Society for Reproductive Medicine. Control and prevention of peritoneal adhesions in gynecologic surgery. Fertil Steril. 2006;86(5 Suppl 1):S1–5. doi:10.1016/j.fertnstert.2006.07.1483
6. Sikirica V, Bapat B, Candrilli SD, Davis KL, Wilson M, Johns A. The inpatient burden of abdominal and gynecological adhesiolysis in the US. BMC Surg. 2011;11(1):13. doi:10.1186/1471-2482-11-13
7. González-Quintero VH, Cruz-Pachano FE. Preventing adhesions in obstetric and gynecologic surgical procedures. Rev Obstet Gynecol. 2009;2(1):38–45.
8. Sikirica V, Broder MS, Chang E, Hinoul P, Robinson D, Wilson M. Clinical and economic impact of adhesiolysis during repeat cesarean delivery. Acta Obstet Gynecol Scand. 2012;91(6):719–725. doi:10.1111/j.1600-0412.2012.01395.x
9. Tanigaki S, Batra A, Chan T-F, et al. Adhesion barriers in gynecologic surgeries and cesarean section: an Asia-Pacific expert panel consensus recommendation. Int J Gynecol Obstet. 2025;168(2):436–448. doi:10.1002/ijgo.15903
10. Schreinemacher MHF, ten Broek RP, Bakkum EA, van Goor H, Bouvy ND. Adhesion awareness: a national survey of surgeons. World J Surg. 2010;34(12):2805–2812. doi:10.1007/s00268-010-0778-8
11. Kibungu C, Kondiah PPD, Kumar P, Choonara YE. Recent Advances in Chitosan and Alginate Based Hydrogels for Wound Healing Application. Front Mater. 2021;8–2021. doi:10.3389/fmats.2021.681960
12. Rinaudo M. Chitin and chitosan: properties and applications. Prog Polym Sci. 2006;31(7):603–632. doi:10.1016/j.progpolymsci.2006.06.001
13. Hwang KT, Kim JT, Jung ST, Cho GS, Park HJ. Properties of chitosan-based biopolymer films with various degrees of deacetylation and molecular weights. J Appl Polym Sci. 2003;89(13):3476–3484. doi:10.1002/app.12561
14. Harris ES, Morgan RF, Rodeheaver GT. Analysis of the kinetics of peritoneal adhesion formation in the rat and evaluation of potential antiadhesive agents. Surgery. 1995;117(6):663–669. doi:10.1016/S0039-6060(95)80010-7
15. Arnold P, Green C, Foresman P, Rodeheaver G. Evaluation of resorbable barriers for preventing surgical adhesions. Fertil Steril. 2000;73(1):157–161. doi:10.1016/S0015-0282(99)00464-1
16. Zeng Q, Yu Z, You J, Zhang Q. Efficacy and safety of seprafilm for preventing postoperative abdominal adhesion: systematic review and meta-analysis. World J Surg. 2007;31(11):2125–21312072. doi:10.1007/s00268-007-9242-9
17. Gonzalez R, Rodeheaver GT, Moody DL, Foresman PA, Ramshaw BJ. Resistance to adhesion formation: a comparative study of treated and untreated mesh products placed in the abdominal cavity. Hernia J Hernias Abdom Wall Surg. 2004;8(3):213–219. doi:10.1007/s10029-004-0213-x
18. Kim JY, Cho WJ, Kim JH, et al. Efficacy and safety of hyaluronate membrane in the rabbit cecum-abdominal wall adhesion model. J Korean Surg Soc. 2013;85(2):51–57. doi:10.4174/jkss.2013.85.2.51
19. Diamond MP, Linsky CB, Cunningham T, et al. DeCherney a H. A model for sidewall adhesions in the rabbit: reduction by an absorbable barrier. Microsurgery. 1987;8(4):197–200. doi:10.1002/micr.1920080406
20. Diamond MP, Burns EL, Accomando B, Mian S, Holmdahl L. Seprafilm® adhesion barrier: (1) a review of preclinical, animal, and human investigational studies. Gynecol Surg. 2012;9(3):237–245. doi:10.1007/s10397-012-0741-9
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Synergy of Polydopamine Nanovaccine and Endostar Alginate Hydrogel for Improving Antitumor Immune Responses Against Colon Tumor

Yang Y, Wang N, Tian XX, Wang X, Yang J, Leng XG, Zhang HL
International Journal of Nanomedicine 2022, 17:4791-4805
Published Date: 12 October 2022
Alginate-Based Hydrogels with Amniotic Membrane Stem Cells for Wound Dressing Application
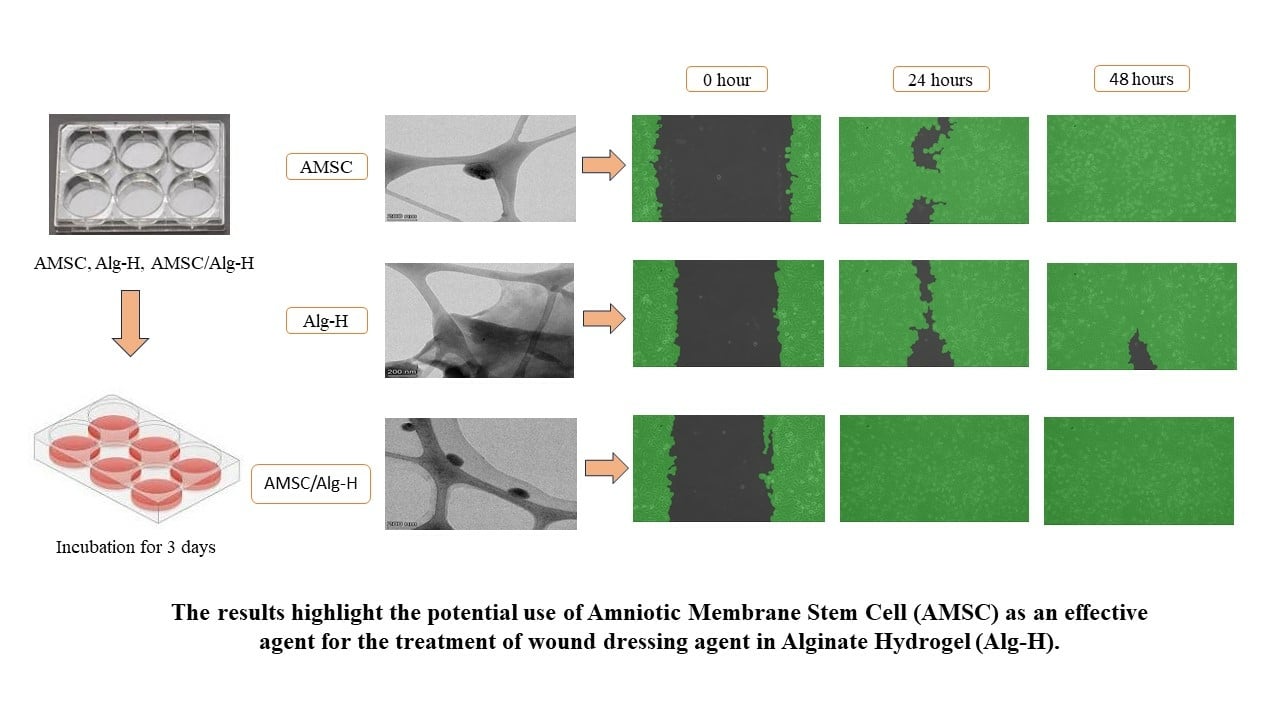
Fitriani N, Wilar G, Narsa AC, Elamin KM, Wathoni N
Stem Cells and Cloning: Advances and Applications 2025, 18:1-13
Published Date: 10 January 2025