Back to Journals » Journal of Pain Research » Volume 16
Evaluation of a New Method of Sciatic Nerve Block: A Prospective Pilot Study
Authors Wang L, Qu Y, Deng Y, Li J, Liu Y, Wu C
Received 17 February 2023
Accepted for publication 7 June 2023
Published 16 June 2023 Volume 2023:16 Pages 2091—2099
DOI https://doi.org/10.2147/JPR.S404489
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Jinlei Li
Supplementary video of "New SNB for TKA" [ID 404489].
Views: 567
Liwei Wang,1,* Yinyin Qu,1,* Ying Deng,1 Jun Li,1 Yanqing Liu,2 Changyi Wu1
1Department of Anesthesiology, Peking University Third Hospital, Peking University, Beijing, 100191, People’s Republic of China; 2Department of Orthopaedics, Peking University Third Hospital, Peking University, Beijing, 100191, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Changyi Wu, Department of Anesthesiology, Peking University Third Hospital, 49 North Garden Road, Haidian District, Beijing, 100191, People’s Republic of China, Tel +86-13522028771, Email [email protected] Yanqing Liu, Department of Orthopaedics, Peking University Third Hospital, 49 North Garden Road, Haidian District, Beijing, 100191, People’s Republic of China, Tel +86-13611346532, Email [email protected]
Purpose: The location of the sciatic nerve deep within the thigh tissue makes it challenging to locate while the patient is in a supine position. The posterior intermuscular septum of the thigh, which encircles the posterior surface of the adductor magnus muscle (AMM), is where the sciatic nerve is located. Our hypothesis was that administering local anesthetic injections into this area could block the sciatic nerve. Therefore, our aim was to evaluate the effectiveness of sciatic nerve block achieved by injecting local anesthetic into the posterior intermuscular septum of the thigh, named the AMM approach.
Methods: Twenty-six patients undergoing total knee arthroplasty were included in the study. We performed an ultrasound-guided sciatic nerve block by injecting 20 mL of 0.25% ropivacaine into the posterior surface of the adductor magnus muscle, using the AMM approach. Additionally, we administered a femoral nerve block with 20 mL of 0.4% ropivacaine. We assessed the sensory and motor effects of the blockade in the operated lower limb and recorded postoperative pain scores at 0, 4, 8, 12, 24, and 48 hours after the operation.
Results: The AMM approach successfully block the sciatic nerve in all 26 patients. The onset of the sensory and motor blockades was achieved within 5.4 ± 1.9 min and 8.7 ± 3.5 min, respectively. We achieved a satisfactory position with the first puncture in 19 of 26 patients (73.1%). The muscle strength of the tibialis anterior immediately after surgery was 4 (ranging from 2 to 5). Additional rescue analgesics were required in 5 of the 26 patients (19.2%) during the first 24 hours postoperatively.
Conclusion: The AMM approach is an innovative and effective method for sciatic nerve block. When combined with simultaneous femoral nerve block in patients undergoing total knee arthroplasty, it provides a useful analgesic treatment option.
Keywords: sciatic nerve block, adductor magnus muscle, tibialis anterior, femoral nerve block
Introduction
Sciatic nerve block (SNB) is a safe and effective way to provide pain relief during lower extremity surgical procedures. Accordingly, the addition of SNB to a femoral nerve block (FNB) has been found to provide better pain relief compared with an FNB alone.1–3 SNB can be applied using either an anterior or a posterior approach.4 An anterior SNB can be performed at the same time and from the same region as an FNB with the patient in the supine position, which limits the number of times the patient has to be moved. However, the sciatic nerve is located deep in the tissue and is positioned behind the femur,5 which often complicates the procedure. The operator needs to repeatedly locate the position of the sciatic nerve, and may have to perform multiple punctures, which increases the patient’s puncture-related discomfort. With the patient supine, the sciatic nerve can be recognized in the fat tissue below the adductor magnus muscle (AMM), which is located 1.5–2 cm posterior to the femur at the level of the upper middle thigh.6 The fascia surrounding the sciatic nerve is the one that surrounds the posterior surface of the adductor magnus, which is part of the posterior intermuscular septum of the thigh.7 Compared with the sciatic nerve, the AMM is much easier to locate by ultrasound.
Based on anatomical analyses, we hypothesized that the sciatic nerve could be blocked by injecting local anesthetic (LA) into the posterior surface of the AMM where the posterior intermuscular septum of the thigh is located. In the current study, we aimed to evaluate the sensory and motor blocks obtained via this new method (AMM approach) in patients undergoing total knee arthroplasty (TKA).
Materials and Methods
Study Design
Ethical approval for this study was obtained from the Ethics Committee of Peking University Third Hospital, China. The clinical trial was registered with the Chinese Clinical Trial Registry (clinical trial number ChiCTR2200056048, http://www.chictr.org.cn/index.aspx) on 2022/1/31. Patients scheduled for total knee arthroplasty under general anesthesia were enrolled between February 1, 2022 and October 31, 2022. Written informed consent was obtained from all patients. Our study protocol complied with the Declaration of Helsinki.
A total of 27 participants between 58 and 77 years of age with a body mass index (BMI) of 23–36 kg /m2 and an American Society of Anesthesiologists (ASA) physical status of I–III were eligible for inclusion (Figure 1). Patients with allergies to medications used in our protocol, a reported history of analgesic drug use longer than three months, local or systemic infections, or an inability to accurately comprehend or take part in pain assessments because of psychiatric disorders were excluded from the analysis.
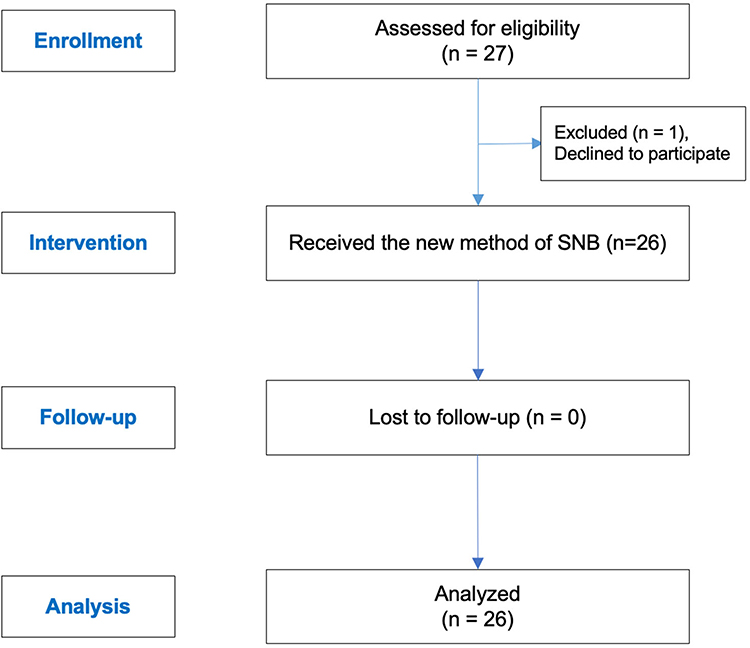 |
Figure 1 Study flowchart. Abbreviation: SNB, sciatic nerve block. |
Protocol
All patients were treated according to a standardized anesthetic regimen. After the patient entered the anesthesia preparation room, their noninvasive blood pressure (NIBP), electrocardiography (ECG) and pulse oxygen saturation (SpO2) were monitored. Peripheral intravenous access was established, and then 5 μg sufentanil was given before the nerve block procedure.
Peripheral Nerve Blocks
Patients were positioned in the supine position, and a low frequency (2 to 5 MHz) curved array ultrasound transducer was positioned 8 cm distal to the inguinal crease, perpendicular to the skin, which is the classic puncture point in anterior approach (C point). Scanning was performed to visualize the sartorius muscle, femoral artery, femoral vein, and femoral nerve on the deep side of the sartorius muscle. Additionally, the hyperechoic femur, adductor longus (AL), adductor brevis (AB), AMM, highlighted fascia, and the sciatic nerve located posterior and medial to the lesser trochanter were scanned. We then slid the ultrasonic probe distally by about 1.5–2 cm (M point), where we could obtain a clearer muscle image, making it easy to localize the AMM (Figure 2). After sterilizing the skin with an iodine-containing solution and applying 1% lidocaine, we inserted a short bevel 100-mm, 21-gauge insulated nerve block needle (SonoPlex STIM, Pajunk Medical Systems, USA) connected to a nerve stimulator (B. Braun Melsungen AG, Germany) and turn on a nerve stimulator with a pulse duration of 0.1 ms and a stimulating frequency of 2 Hz. The block was performed using an out of plane approach. The needle was slowly advanced until the needle tip was close to the posterior surface of the AMM, and proper needle positioning was confirmed by observing fluid distribution beneath the posterior surface of the AMM after injecting 5 mL 5% glucose solution. Subsequently, 20 mL of 0.25% ropivacaine was administered (Figure 3). The procedure of SNB is shown in the Supplementary Video. After the SNB, FNB was performed using 20 mL of 0.40% ropivacaine. All nerve block procedures were performed by the same anesthesiologist.
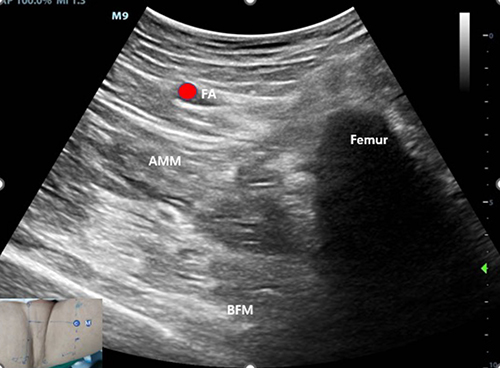 |
Figure 2 The short axis (transverse view) ultrasound image obtained with our new AMM approach. C point is the classic puncture point in anterior approach of SNB. M point is the puncture point in AMM approach. Abbreviations: FA, femoral artery; AMM, adductor magnus muscle; BFM, biceps femoris. |
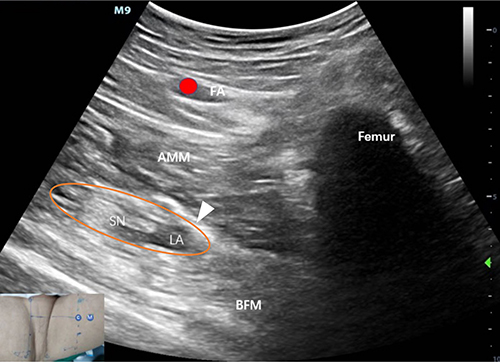 |
Figure 3 An ultrasound image obtained immediately after the injection of local anesthetics under the posterior surface of the AMM into the posterior intermuscular septum of the thigh. The white arrowhead demonstrated the location of needle tip. The Orange circle indicates the area where the sciatic nerve is located and where the local anesthetics was injected. C point is the classic puncture point in anterior approach of SNB. M point is the puncture point in AMM approach. Abbreviations: FA, femoral artery; AMM, adductor magnus muscle; SN, sciatic nerve; LA, local anesthetics, BFM, biceps femoris. |
Various measurements were taken during the study, including the depth of the needle (measured as the distance from the skin to the needle tip, as confirmed via the ultrasound image to be at the deep surface of the AMM), the duration of the nerve block procedure for all blocks (measured as the time from the start of patient positioning for the first SNB to the end of the FNB), and visibility scores for both the sciatic nerve and AMM. Visibility scores were assessed using a 6-point visibility scale, where a score of 0 indicated that no nerve/muscle was identified, and a score of 5 indicated complete visibility with multiple fascicles/perimysium identifiable (Table 1).8 The onset of sensory and motor blockades (from local anesthetic administration to the start of sensory and motor changes, respectively), the duration of sensory block (from local anesthetic administration to full sensory recovery), and the number of needle passes (classified as 0, 1, 2, or 3, with 0 representing deliberate needle tip withdrawal to skin level or additional skin puncture) were also measured.
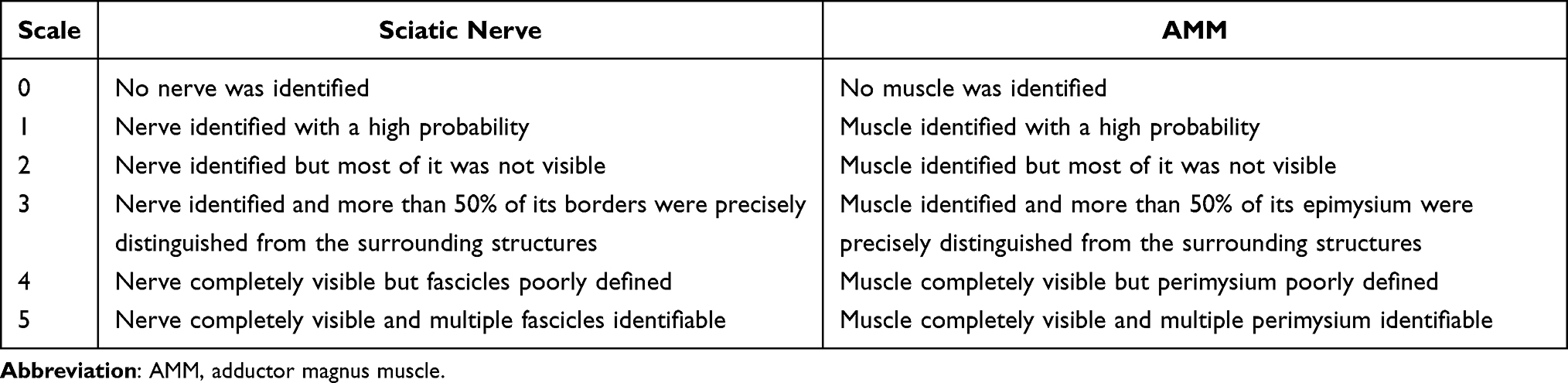 |
Table 1 Visibility Scores for Both the Sciatic Nerve and AMM |
Anesthesia
General anesthesia was administered 30 minutes after the nerve block via intravenous sufentanil 0.2 μg/kg, propofol 1.5–2 mg/kg, and cisatracurium 0.15 mg/kg. A laryngeal mask was inserted, and mechanical ventilation was initiated. During the surgery, general anesthesia was maintained by infusing propofol (0.08–0.1 mg/kg/min) and remifentanil (0.1–0.2 μg/kg/min) with BIS values fluctuating between 40–60. The same group of surgeons performed total knee arthroplasty on all patients in the supine position. Following the surgery, patients were transferred to the post-anesthesia care unit and monitored for complete recovery from anesthesia. Pain severity was assessed using a Visual Analogue Scale (VAS) both at rest and during movement (0 = “no pain”, 10 = “worst pain imaginable”). Patients were orally administered tramadol hydrochloride 100 mg every 12 hours. Intravenous tramadol hydrochloride 100 mg was additionally administered to patients with VAS scores ≥4.
Outcomes
Postoperative pain was assessed at multiple time points, including immediately after surgery and at 4 h, 8 h, 12 h, 24 h, and 48 h post-surgery. Possible side effects, such as pruritus, vomiting, nausea, and dizziness, were also recorded.
In addition, a sensory assessment was conducted to evaluate the function of different nerves. This included the tibial nerve for the plantar aspect of the foot, the superficial peroneal nerve for the dorsal aspect of the foot, the sural nerve for the posterolateral area of the leg, and the posterior cutaneous nerve of thigh for the posterior area of the thigh. Pinpricks were administered at 1-min intervals to assess sensory function.
Motor block was assessed by monitoring ankle and knee movement. Muscle strength of the anterior tibialis and quadriceps femoris was evaluated immediately after surgery and at 4 h, 8 h, 12 h, 24 h, and 48 h post-surgery. Patients were asked to flex their ankle and knee joints, and muscle strength was scored on a scale of 0 to 5, with 5 indicating normal joint function.9 These scores were independently assessed by another anesthetist.
Statistical Analysis
As a pilot study, the sample size was determined empirically based on previous literature, which suggested a range of 10–40 participants.10 In this study, we recruited 26 patients. Categorical variables were reported as numbers and frequencies, while continuous variables were reported as mean ± standard deviation for normally distributed data, and as median and interquartile range (IQR, 25th-75th) for non-normally distributed data. Statistical analysis was performed using SPSS software (version 22.0, IBM Corporation, Armonk, NY, USA).
Results
In total, 27 patients were screened from February 2022 to October 2022 in this study. Among them, 1 patient refused to participate. Finally, 26 patients received the AMM approach of SNB. The patient demographics and operation duration are presented in Table 2.
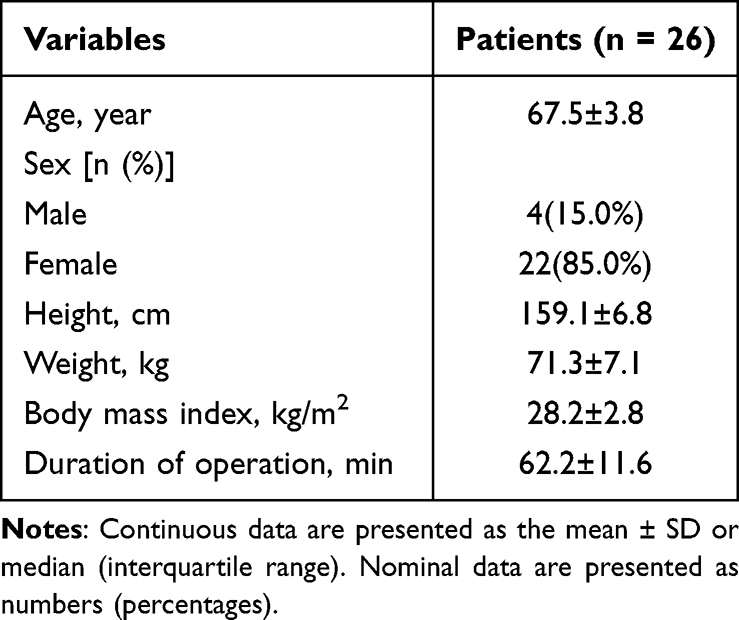 |
Table 2 Demographics and Operation Details |
Table 3 shows the SNB-related measurements, including the depth of the needle (7.1 ± 0.9 cm), duration of the nerve block procedure (10.6 ± 1.7 min), visibility score of the sciatic nerve (2.3 ± 1.0), and image quality of the sciatic nerve. The sciatic nerve image quality was poor in 8 out of the 26 patients (30.8%) with a visibility score of less than 2. The AMM visibility score was 3.8 ± 0.6, and the image quality was excellent for 22 out of the 26 patients (84.6%) with a visibility score of 4 or higher. The onset time of the sciatic nerve sensory block was 5.4 ± 1.9 min, and the onset time of the sciatic nerve motor block was 8.7 ± 3.5 min. The duration of the sciatic nerve blockade was 17.6 ± 3.0 h. Additionally, the number of needle passes (including deliberate needle tip withdrawal to the skin level or additional skin punctures) was as follows: 19 with 0 passes, 6 with 1 pass, 1 with 2 passes, and 0 with 3 passes.
 |
Table 3 SNB-Related Measurements |
The muscle strength of the anterior tibialis and quadriceps femoris immediately after surgery were displayed in Table 4. The muscle strength data at 4 h, 8 h, 12 h, 24 h, and 48 h after surgery were not reported, as all patients had anterior tibial muscle strength ≥ 3 points at 4 h after surgery. In the posterior area of the thigh, 24 patients (92.3%) experienced decreased skin sensation. During the first 24 h after surgery, two patients reported nausea and one patient had vomiting. Figure 4 shows the postoperative pain scores. Among the patients, four (15.4%) required additional rescue analgesics during the first night after surgery, while the others achieved a satisfactory analgesic effect without interfering with their sleep.
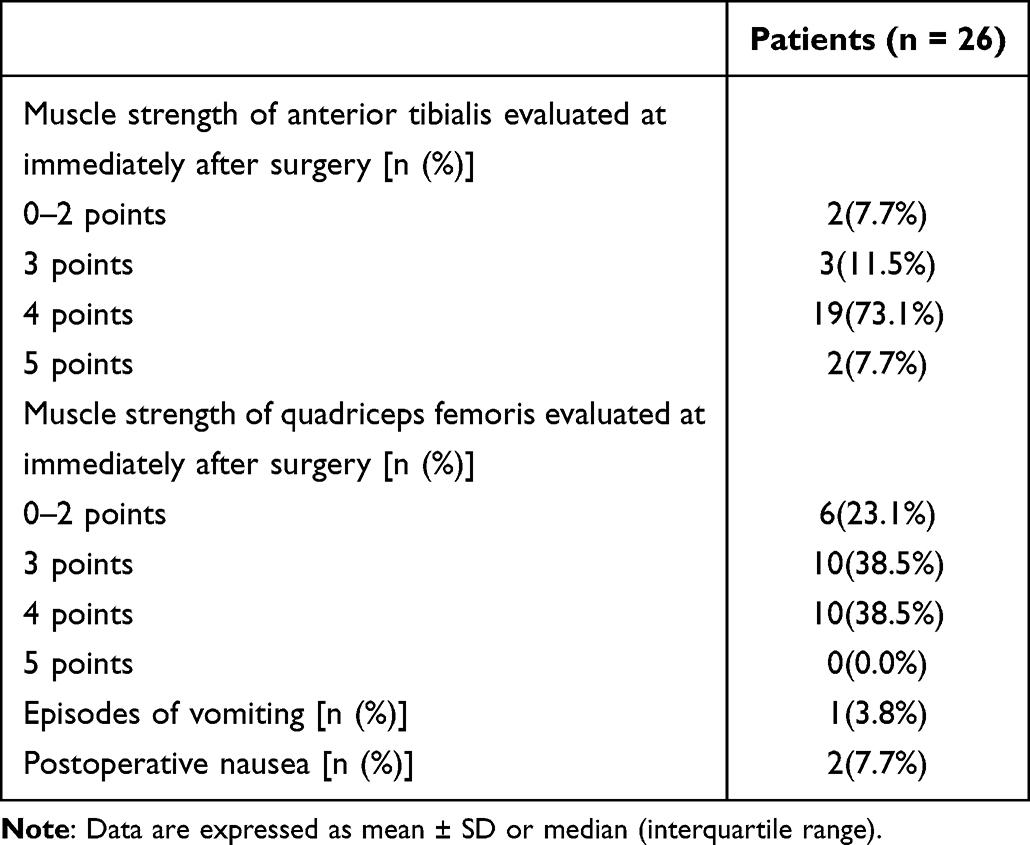 |
Table 4 Postoperative Data |
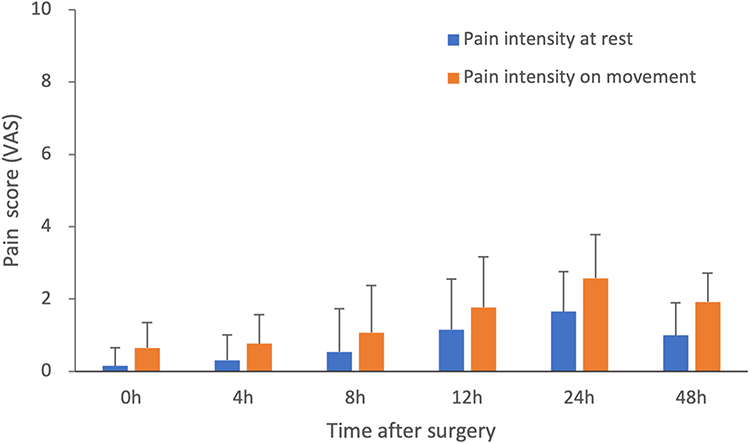 |
Figure 4 VAS scores at different time points postoperatively. |
Discussion
In this pilot study, we aimed to investigate a novel approach SNB and applied AMM approach in patients undergoing TKA. Local anesthetics were injected into the posterior intermuscular septum of the thigh under the posterior surface of the AMM. Our results demonstrated that this AMM approach of SNB was effective in providing satisfactory sensory and motor blocks in all study participants.
The first anterior SNB approach was described by Beck in 1963.11 The introduction of ultrasound guidance allowed for direct visualization of the sciatic nerve. However, the depth and anisotropy of the sciatic nerve can make it difficult to visualize, it is still regarded as a time-consuming and advanced technique.8,12,13
Conventional two-dimensional ultrasound machines are limited in terms of the ability to distinguish the SN from the surrounding tissue,14 which could affect the success rate and effect of the block procedure. In our study, the image quality of the SN was poor in 8 of the 26 patients (30.8%, visibility score <2). Kim et al compared several different positions for SN identification and reported that the anterior approach had an approximate visibility score of 2.5,8 which is similar to our results. Furthermore, Barrington et al reported that 37.5% of their patients had a poor or average image quality,15 which is consistent with our results. Zhu et al reported that in 10 of their 26 patients (38.5%) who underwent the anterior approach, the obtained image of the SN had poor quality (visibility score <2).16 Our new method uses two well-defined ultrasonographic landmarks, the AMM and the femur, which can be obtained easily at the level of the upper middle thigh. The AMM, which is attached to the femur, covers the sciatic nerve.17 In our study, the AMM image quality was excellent for 22 of the 26 patients (84.6%).
With the poor image of the traditional method and the deep anatomical position of SN, the anterior SNB showed a greater number of needle passes. For instance, Van Elstraete et al reported that the first attempt to locate the sciatic nerve was successful in only 7 of 20 patients (35.0%),18 while Zhu et al reported that a satisfactory position was achieved during the first attempt in only 8 of 26 patients (30.8%), and 8 of 26 patients (30.8%) required more than two attempts to obtain a satisfactory position.16 In the present study, we obtained a satisfactory position during the first attempt in 19 of 26 patients (73.1%), and only one patient (3.8%) required three attempts to obtain a satisfactory position. The reason for the repeated punctures in that patient might have been related to the age (over 70 yrs) or higher BMI (32 kg/m2).
A previous study reported a block onset time of 9.42 ± 1.08 min using the anterior approach,19 while Yektaş et al reported a sensory block onset time of 12.88 ± 4.87 min and a motor block onset time of 13.55 ± 4.75 min, also in patients treated with the anterior approach.13 In our study, we observed that the sensory and motor block onset times were 5.4 ± 1.9 min and 8.7 ± 3.5 min, respectively, which were shorter compared to those reported in previous studies. However, the differences in the definition of onset time across studies may have contributed to this finding. Specifically, in our study, onset time was defined as the time from the administration of the local anesthetic to the initial onset of sensory and motor changes, while in other studies, onset time was defined as the time from the administration of local anesthetics to the patient’s complete absence of sensation or movement.
Previous studies have indicated that a sensory block in the posterior femoral cutaneous nerve, which runs parallel to the SN in the gluteal region, was rarely achieved after the anterior approach (14.9%).20 In this observational study, we not only observed successful SNB, but also found that administering the local anesthetic into the posterior intermuscular septum of the thigh resulted in a higher proportion of successful posterior femoral cutaneous nerve block (92.3%).
In this study, we assessed the impact of our new SNB approach by measuring muscle strength immediately after surgery and at various time points up to 48 hours postoperatively. Our findings demonstrate that the new approach does not result in significant weakness in the anterior tibialis or gastrocnemius muscles. Specifically, more than 80% of patients had a score of more than three points in the anterior tibialis muscle strength assessment immediately after surgery, while more than 84% of patients had a score of more than three points in the gastrocnemius muscle strength assessment. The favorable outcome observed in our study can be attributed to the precise location of the local anesthetic injection, which reduces the risk of nerve damage. In our study, we minimized the risk of nerve injury by injecting the local anesthetic into the fascial space surrounding the sciatic nerve. This approach allowed our patients to perform ankle pump exercises immediately after the surgery, which is crucial for preventing the formation of venous thrombosis in the lower limbs.21,22 Ropivacaine at low concentrations has been found to produce a sensory block but has no effect or a limited effect on motor nerves, thus preserving muscle strength.23–25 We used a lower concentration of ropivacaine (0.25%) for SNB, which might be another reason why we observed a strong sensory block, but a weaker motor block.
Adequate pain relief after TKA is very important as it can promote postoperative rehabilitation,26 which is essential for a satisfactory outcome. Our data demonstrated that the new SNB method provided good postoperative pain relief at rest or during movement. This was especially the case immediately after the operation, as well as 4 h and 8 h afterward. This was consistent with the findings of a previous study,27–29 and was likely associated with the decreased demand for postoperative analgesics in our patient group during the first 24 h after surgery.
The injection of local anesthetics under the fascia surrounding the posterior surface of the adductor magnus, as a part of the posterior intermuscular septum of the thigh, is consistent with safety-driven initiatives30 to deposit local anesthetics between muscles, along anatomical fascial planes,31 or perivascularly rather than perineurally32 for a variety of peripheral nerve block techniques. Our newly developed technique is distinguished by its ease of administration and minimal impact on the muscle strength of the gastrocnemius and tibialis anterior. These attributes make it highly suitable for the management of postoperative pain, particularly when maintaining ankle joint mobility is a priority.
Although our study provides promising results for the medial mid-thigh AMM approach for SNB, several limitations need to be considered. First, the effect of a low concentration (0.25%) of ropivacaine was tested in this study. Future studies should investigate the effect of higher concentrations of local anesthetics to determine the optimal dosage for this new method. Additionally, the study had a higher proportion of female patients compared to male patients, and future studies should balance the gender distribution. Moreover, our study included patients with a BMI ≥ 25 kg/m2, and only one patient with a BMI of 23 kg/m2. Thus, the effectiveness of our technique in patients with lower BMIs should be further evaluated. Finally, randomized controlled trials are needed to compare the efficacy of the medial mid-thigh AMM approach with other proximal approaches for SNB.
Conclusion
Overall, our findings suggest that the medial mid-thigh AMM approach for SNB is both accessible and dependable, with promising implications for postoperative pain management in lower limb procedures such as total knee arthroplasty. Nonetheless, the precise mechanisms underlying this novel technique warrant further investigation.
Data Sharing Statement
We agree to share all the data for this study. The data that support the findings of this study are available from the corresponding author upon any reasonable request.
Acknowledgments
The authors want to thank the Department of Anesthesiology and Department of Orthopaedics, Peking University Third Hospital for the help and support in preparation of the manuscript and research studies.
Funding
This work was supported by Innovation & Transfer Fund of Peking University Third Hospital (BYSYZHKC2022103), and the National Natural Science Foundation of China (82271289).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ben-David B, Schmalenberger K, Chelly JE. Analgesia after total knee arthroplasty: is continuous sciatic blockade needed in addition to continuous femoral blockade? Anesth Analg. 2004;98(3):747–749. doi:10.1213/01.ANE.0000096186.89230.56
2. Mahadevan D, Walter RP, Minto G, Gale TC, McAllen CJ, Oldman M. Combined femoral and sciatic nerve block vs combined femoral and periarticular infiltration in total knee arthroplasty: a randomized controlled trial. J Arthroplasty. 2012;27(10):1806–1811. doi:10.1016/j.arth.2012.05.018
3. Zorrilla-Vaca A, Li J. The role of sciatic nerve block to complement femoral nerve block in total knee arthroplasty: a meta-analysis of randomized controlled trials. J Anesth. 2018;32(3):341–350. doi:10.1007/s00540-018-2480-1
4. Ota J, Hara K. Ultrasound-guided sciatic nerve block. Masui Japanese J Anesthesiol. 2008;57(5):580–587.
5. Uz A, Apaydin N, Cinar SO, et al. A novel approach for anterior sciatic nerve block: cadaveric feasibility study. Surg Radiol Anat. 2010;32(9):873–878. doi:10.1007/s00276-010-0642-4
6. Osaka Y, Kashiwagi M, Nagatsuka Y, Miwa S. Ultrasound-guided medial mid-thigh approach to sciatic nerve block with a patient in a supine position. J Anesth. 2011;25(4):621–624. doi:10.1007/s00540-011-1169-5
7. Kendir S, Torun B, Akkaya T, Comert A, Tuccar E, Tekdemir I. Re-defining the anatomical structures for blocking the nerves in adductor canal and sciatic nerve through the same injection site: an anatomical study. Surg Radiol Anat. 2018;40(11):1267–1274. doi:10.1007/s00276-018-2094-1
8. Kim HJ, Chin KJ, Kim H, et al. Ultrasound-Guided Anterior Approach to a Sciatic Nerve Block: influence of Lower Limb Positioning on the Visibility and Depth of the Sciatic Nerve. J Ultrasound Med. 2020;39(8):1641–1647. doi:10.1002/jum.15258
9. Hu J, Wang Q, Zeng Y, Xu M, Gong J, Yang J. The impact of ultrasound-guided transmuscular quadratus lumborum block combined with local infiltration analgesia for arthroplasty on postoperative pain relief. J Clin Anesth. 2021;73:110372. doi:10.1016/j.jclinane.2021.110372
10. Hertzog MA. Considerations in determining sample size for pilot studies. Res Nurs Health. 2008;31(2):180–191. doi:10.1002/nur.20247
11. Beck GP. Anterior approach to sciatic nerve block. Anesthesiology. 1963;24:222–224. doi:10.1097/00000542-196303000-00011
12. Yoshida T, Nakamoto T, Hashimoto C, Aihara S, Nishimoto K, Kamibayashi T. An Ultrasound-Guided Lateral Approach for Proximal Sciatic Nerve Block: a Randomized Comparison With the Anterior Approach and a Cadaveric Evaluation. Reg Anesth Pain Med. 2018;43(7):712–719. doi:10.1097/AAP.0000000000000835
13. Yektaş A, Balkan B. Comparison of sciatic nerve block quality achieved using the anterior and posterior approaches: a randomised trial. BMC Anesthesiol. 2019;19(1):225. doi:10.1186/s12871-019-0898-0
14. Choquet O, Capdevila X. Case report: three-dimensional high-resolution ultrasound-guided nerve blocks: a new panoramic vision of local anesthetic spread and perineural catheter tip location. Anesth Analg. 2013;116(5):1176–1181. doi:10.1213/ANE.0b013e31828b34ae
15. Barrington MJ, Lai SL, Briggs CA, Ivanusic JJ, Gledhill SR. Ultrasound-guided midthigh sciatic nerve block-a clinical and anatomical study. Reg Anesth Pain Med. 2008;33(4):369–376. doi:10.1097/00115550-200807000-00015
16. Zhu LJ, Gong CJ, Zhang ZF, Zhang QW, Peng PP, Ni Y. Efficacy and safety of ultrasound-guided above-knee lateral approach for popliteal sciatic nerve block in surgeries below the knee: a randomized controlled trial. Ann Palliat Med. 2021;10(5):5188–5197. doi:10.21037/apm-21-10
17. Cherry P, Walls DJCI. Pocket atlas of sectional anatomy. Computed tomography and magnetic resonance imaging. Clin Imaging. 2006;32(2):413.
18. Van Elstraete AC, Poey C, Lebrun T, Pastureau F. New landmarks for the anterior approach to the sciatic nerve block: imaging and clinical study. Anesth Analg. 2002;95(1):214–218. doi:10.1097/00000539-200207000-00038
19. Alsatli RA. Comparison of ultrasound-guided anterior versus transgluteal sciatic nerve blockade for knee surgery. Anesthesia Essays Res. 2012;6(1):29–33. doi:10.4103/0259-1162.103368
20. Ota J, Sakura S, Hara K, Saito Y. Ultrasound-guided anterior approach to sciatic nerve block: a comparison with the posterior approach. Anesth Analg. 2009;108(2):660–665. doi:10.1213/ane.0b013e31818fc252
21. Wang S, Lu H, Li S. Prevention of deep venous thrombosis in patients undergoing knee arthroplasty by intermittent pneumatic compression apparatus. Am J Transl Res. 2021;13(9):10765–10770.
22. Li T, Yang S, Hu F, Geng Q, Lu Q, Ding J. Effects of ankle pump exercise frequency on venous hemodynamics of the lower limb. Clin Hemorheol Microcirc. 2020;76(1):111–120. doi:10.3233/CH-200860
23. Casati A, Santorsola R, Cerchierini E, Moizo E. Ropivacaine. Minerva Anestesiol. 2001;67(9 Suppl 1):15–19.
24. Zhai W, Wang X, Rong Y, Li M, Wang H. Effects of a fixed low-dose ropivacaine with different volume and concentrations on interscalene brachial plexus block: a randomized controlled trial. BMC Anesthesiol. 2016;16(1):80. doi:10.1186/s12871-016-0248-4
25. Li H, Shi R, Shao P, Wang Y. Evaluation of Sensory Loss Obtained by Circum-Psoas Blocks in Patients Undergoing Total Hip Replacement: a Descriptive Pilot Study. J Pain Res. 2022;15:827–835. doi:10.2147/JPR.S354829
26. Teunkens A, Vanhaecht K, Vermeulen K, et al. Measuring satisfaction and anesthesia related outcomes in a surgical day care centre: a three-year single-centre observational study. J Clin Anesth. 2017;43:15–23. doi:10.1016/j.jclinane.2017.09.007
27. Qin L, You D, Zhao G, Li L, Zhao S. A comparison of analgesic techniques for total knee arthroplasty: a network meta-analysis. J Clin Anesth. 2021;71:110257. doi:10.1016/j.jclinane.2021.110257
28. Dong P, Tang X, Cheng R, Wang J. Comparison of the Efficacy of Different Analgesia Treatments for Total Knee Arthroplasty: a Network Meta-Analysis. Clin J Pain. 2018;34(11):1047–1060. doi:10.1097/AJP.0000000000000631
29. Tanikawa H, Harato K, Ogawa R, et al. Local infiltration of analgesia and sciatic nerve block provide similar pain relief after total knee arthroplasty. J Orthop Surg Res. 2017;12(1):109. doi:10.1186/s13018-017-0616-x
30. Sites BD, Neal JM, Chan V. Ultrasound in regional anesthesia: where should the “focus” be set? Reg Anesth Pain Med. 2009;34(6):531–533. doi:10.1097/AAP.0b013e3181c0f025
31. Choquet O, Morau D, Biboulet P, Capdevila X. Where should the tip of the needle be located in ultrasound-guided peripheral nerve blocks? Curr Opin Anaesthesiol. 2012;25(5):596–602. doi:10.1097/ACO.0b013e328356bb40
32. Swenson JD, Davis JJ. Ultrasound-guided regional anesthesia: why can’t we all just stay away from the nerve? Anesthesiology. 2008;109(4):748–749. doi:10.1097/ALN.0b013e3181863831
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.