")
Back to Journals » Infection and Drug Resistance » Volume 16
Evaluation and Analysis of the Rationality of Clinical Use of Carbapenems in Surgical Departments of a Tertiary Hospital in Southwest China
Authors Huang Z, Yao G, Zhang C, Zhou X, Zou G, Zhuo C
Received 19 January 2023
Accepted for publication 22 March 2023
Published 17 April 2023 Volume 2023:16 Pages 2259—2269
DOI https://doi.org/10.2147/IDR.S403787
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Zhongyue Huang,1,* Gaoqiong Yao,2,* Chengzhi Zhang,2 Xin Zhou,2 Guanyang Zou,3,* Chao Zhuo4,*
1Institute of Medical Information/Medical Library, Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing, People’s Republic of China; 2Department of Pharmacy, First Affiliated Hospital of Chongqing Medical University, Chongqing, People’s Republic of China; 3School of Public Health and Management, Guangzhou University of Chinese Medicine, Guangzhou, Guangdong Province, People’s Republic of China; 4State Key Laboratory of Respiratory Disease, The First Affiliated Hospital of Guangzhou Medical University, Guangzhou, Guangdong Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Guanyang Zou, No. 232, Waihuan East Road, Panyu District, Guangzhou, Guangdong Province, 510006, People’s Republic of China, Email [email protected] Chao Zhuo, 195 Dongfeng West Road, Yuexiu District, Guangzhou, Guangdong Province, 510030, People’s Republic of China, Email [email protected]
Purpose: With the increasing frequency and intensity of carbapenem consumption, carbapenem-resistant organisms (CRO) have become a focus of anti-infection research. This study aimed to evaluate the rationality of the clinical use of carbapenems among inpatients in the surgical departments of a tertiary hospital in southwest China.
Patients and methods: A point-score system was established for evaluation based on the clinical practices in surgical departments and selected carbapenem prescriptions from June 2020 to June 2021 for hepatobiliary surgery, gastrointestinal surgery, and neurosurgery in the study hospital. Prescriptions with a total score ≥ 270 were defined as rational. Descriptive statistics were used to describe the characteristics and rationality of the prescriptions. The chi-square test, Mann–Whitney U-test, and Kruskal–Wallis H-test were used to compare characteristics between rational and irrational prescriptions. Linear regression analysis was used to determine the factors affecting the rationality of carbapenem prescriptions.
Results: According to 192 carbapenem prescription records, the median age of patients was 62 years [IQR, 48.0– 73.0], and 20% of patients had abdominal infections, 10% had lung infections, 14% had intracranial infections, and 3% had urinary tract infections. 56% of carbapenem prescriptions were irrational. Compared with rational carbapenem prescriptions, irrational prescriptions had a higher proportion of those with inappropriate indications (49% vs 0%, p < 0.05), incorrect variety selection (15% vs 0%, p< 0.05), and unreasonable assessment of etiology and efficacy (46% vs 8%, p < 0.05). Linear regression analysis suggested that the diagnosis of cholecystitis (standardized regression coefficient=0.183, p< 0.05) and replaced medication (standardized regression coefficient = 0.154, p< 0.05) influenced the rationality of carbapenem prescriptions.
Conclusion: Our study shows that the irrational use of carbapenems deserves attention, especially in surgical departments. Interventions for carbapenem use that are based on evaluation criteria should be developed to reduce the emergence and spread of carbapenem-resistant bacteria.
Keywords: carbapenem, prescription review, surgery
Introduction
Antimicrobial resistance (AMR) has been listed by the World Health Organization (WHO) as a serious global public health threat. Between 2000 and 2018, the global rate of antibiotic consumption increased by 46%, especially in low- and middle-income countries (LMICs), where it increased by 76%.1 Antimicrobial resistant infections directly caused 1.27 million deaths in 2019.2
With the increase in bacterial resistance to second- and third-generation cephalosporins and fluoroquinolones, carbapenems are increasingly used in clinical practice. They play an important role in the antibacterial treatment of multidrug-resistant bacterial infections, mixed aerobic and anaerobic bacterial infections, severe infections, and infections in immunocompromised patients.3,4
However, with the increasing use and intensity of carbapenem consumption, carbapenem-resistant organisms (CRO) have become a great concern.5–7 Owing to the special rectification of the clinical use of antimicrobial drugs in 2011, the intensity of antibiotic use in China decreased from 59.4% in 2011 to 36.8% in 2017, and antibiotic consumption decreased from 85.1 DDDs/100 patient-days to 49.7 DDDs/100 patient-days. However, the intensity of carbapenem consumption increased from 1.83 DDDs/100 person-day to 3.28DDDs/100 person-day in the same period.8,9 In some areas, the consumption of carbapenem has increased quickly.10,11 For example, the average annual growth rates of carbapenem use in Guangdong and Jiangsu provinces were 18% and 19%, respectively, from 2019 to 2020.12
The use of carbapenems in surgical departments, particularly prolonged use of carbapenems and inappropriate etiological evaluation, is even more concerning. In 2018, the National Health Commission of China issued evaluation criteria for the clinical use of carbapenems, which was mainly used by pharmacists to evaluate the rationality of carbapenem prescriptions afterwards.13 However, it is difficult for surgeons and other physicians to comply with these evaluation criteria because they are more suitable for the administrative regulation of carbapenem use. Doctors face complex situations when treating patients and may have different perceptions of this evaluation criteria than pharmacists. Based on China’s evaluation criteria for carbapenems and other relevant clinical guidelines such as those for abdominal infection and sepsis,14–16 we established evaluation criteria for carbapenems applicable to surgical departments. The evaluation criteria included five dimensions: indications, variety selection, usage-dosage-compatibility, etiology and efficacy evaluation, prescription management and consultation.
This study aimed to evaluate the rationality of the clinical use of carbapenems among inpatients in the surgical departments of a tertiary hospital in southwest China. This will help inform targeted intervention measures and promote the rational use of carbapenems.
Methods
Study Design and Setting
This retrospective study was conducted in a 3200-bed tertiary teaching hospital in Southwest China. The study included patients who were administered carbapenems (meropenem or imipenem) between June 2020 and June 2021. In addition, prescriptions were drawn from three noteworthy departments, gastrointestinal surgery, hepatobiliary surgery, and neurosurgery, all of which were surgical departments with high carbapenem consumption. We excluded carbapenem prescriptions with durations of less than 72h because these prescriptions might interfere with the assessment of efficacy. A total of 192 prescriptions of carbapenem were included in research samples.
Evaluation Criteria for the Rationality of Carbapenem Prescriptions
We established a point-scoring system for evaluation based on the clinical practices in surgical departments.13,17 The evaluation criteria were verified by two experts in infectious diseases, three experts in pharmacy and were considered practical in China context.
The evaluation system was based on indications (symptoms that required carbapenem treatment), variety selection of carbapenems, usage-dosage-compatibility, etiology and efficacy evaluation, prescription management and consultation with special-use antibacterial drugs (Table 1). Since it is difficult for surgeons to grasp the indications, the study refined the evaluation criteria for indications with reference to international clinical guidelines, such as the Abdominal Infection and Sepsis Guidelines.14,15
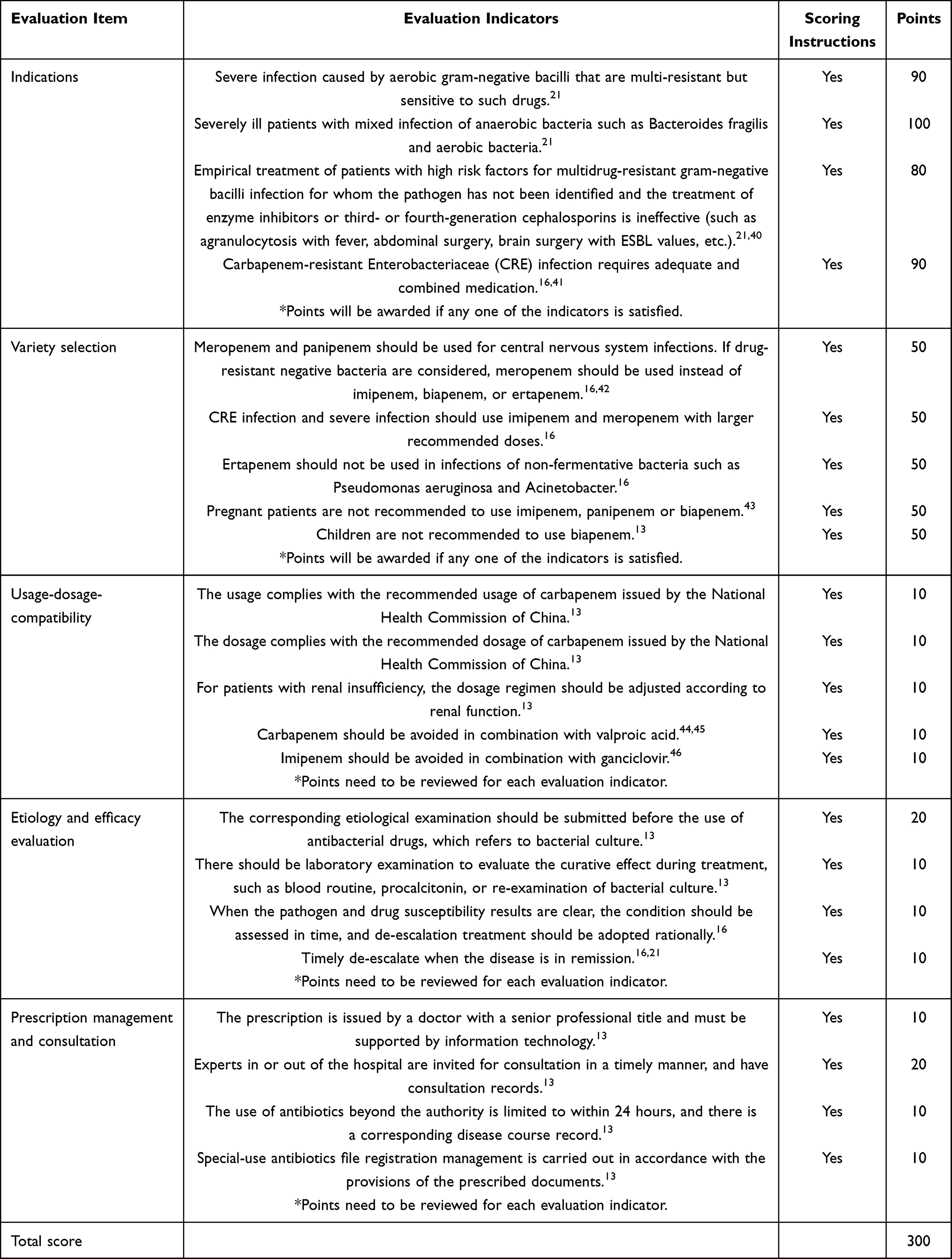 |
Table 1 Evaluation Criteria for the Rationality of Clinical Use of Carbapenems |
A greater impact (100 points) was assigned to indications that could have a major influence. For the evaluation of variety selection, usage-dosage-compatibility, etiology and efficacy, prescription management and consultation were assigned 50 points each. The maximum total score for the five evaluation sections was 300. Prescriptions with a total score of less than 270 were considered unreasonable. High threshold of irrationality of prescription has been implemented because carbapenems are antibiotics in a special-use category in China (Table 1).
Data Collection and Analysis
The hospital established a carbapenem prescription management group consisting of a prescription review working group and a prescription review expert group, responsible for extracting medical records and reviewing the results. The prescription data for the three selected departments were collected from the hospital information system. We conducted two prescription reviews: a preliminary review was conducted by two senior clinical pharmacists and a final review was conducted by two experienced infectious disease specialists. Each prescription was assigned a final score after two rounds of review. The hospital’s prescription review expert group discussed and confirmed the final score of the prescription if there was a discrepancy between the results of the two prescription reviews. The results of the prescription review were uploaded to the hospital information system and fed back to the relevant departments through the hospital’s Office Automated (OA) system.
Descriptive statistics were used to present the characteristics of the carbapenem prescriptions and patients. Continuous variables were expressed as medians and interquartile ranges (IQR), while categorical variables were expressed as counts and proportions. Univariate analysis compared the characteristics of rational and irrational prescriptions using the chi-square test, Mann–Whitney U-Test, and Kruskal–Wallis H-Test. Multicollinearity test was performed before multivariable analysis. Linear regression analysis was used to determine the factors affecting the rationality of carbapenem prescriptions. The dependent variable for the linear regression was the rationality of the prescription. The independent variables were general characteristics of the prescription. Analyses were performed using SPSS software (version 23.0). P < 0.05 were considered statistically significant.
Results
Comparison of Rational and Irrational Carbapenem Prescriptions According to Patient Characteristics
Of the included patients, the median age of patients was 62 years [IQR, 48.0–73.0]; 52% of patients were above 60 years old, 20% had abdominal infections, 10% had lung infections, 14% had intracranial infections, and 3% had urinary tract infections. Of the 192 carbapenem prescriptions, 48%, 32%, and 20% were selected from hepatobiliary surgery, gastrointestinal surgery, and neurosurgery, respectively. Meropenem was used in 59% of the prescriptions (Table 2).
 |
Table 2 Comparison of Rational and Irrational Carbapenem Prescriptions Based on Patient Characteristics |
56% of the prescriptions were irrational, with scores below 270. Compared with rational carbapenem prescriptions, irrational prescriptions were greater in hepatobiliary surgery department (55% vs 40%, p < 0.05) and were more often co-prescribed with meropenem (62% vs 56%, p < 0.05). No significant difference was found between the rational and irrational prescriptions based on patients’ age (p > 0.05) (Table 2).
Comparison of Rational and Irrational Carbapenem Prescriptions, by Evaluation Criteria
Based on the evaluation criteria, 72% of the prescriptions were medications with indications, and 92% and 96% of the prescriptions had correct variety selection and appropriate usage-dosage-compatibility, respectively. Only 63% and 53% of the prescriptions had reasonable etiology and efficacy evaluations and proper prescription management and consultation, respectively. Compared with rational carbapenem prescriptions, irrational prescriptions had a higher proportion of those with inappropriate indications (49% vs 0%, p < 0.05), incorrect variety selection (15% vs 0%, p<0.05), and unreasonable assessment of etiology and efficacy (46% vs 8%, p < 0.05). No significant differences were found between rational and irrational prescriptions in terms of prescription management and consultation (p > 0.05) (Table 3).
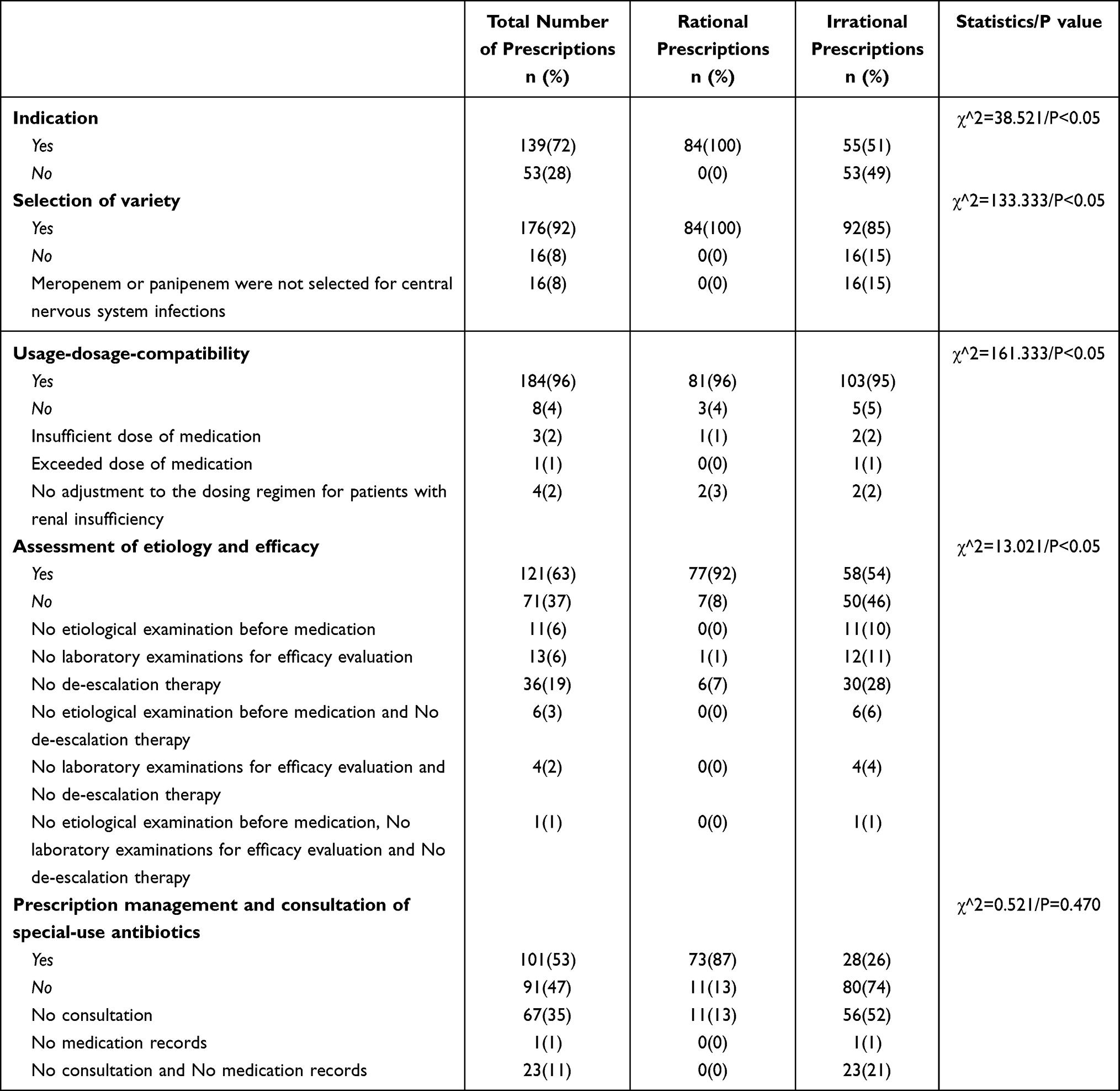 |
Table 3 Comparison of Rational and Irrational Carbapenem Prescriptions, by Evaluation Criteria |
Factors Influencing the Rationality of Carbapenem Prescriptions
Univariate analysis showed that the median scores of the rational prescriptions of hepatobiliary surgery (280 [270–290] vs 240 [180–270], p < 0.05), gastrointestinal (270 [270–270] vs 260 [253–268], p < 0.05) and neurosurgery (270 [260-273] vs. 260 [198-270], p < 0.05) were higher than the median score of unreasonable prescriptions (Table 4).
 |
Table 4 Analysis of Factors Influencing the Rationality of Carbapenem Prescriptions |
Further linear regression analysis showed that the diagnosis of cholecystitis was significantly associated with the rationality of carbapenem prescriptions. Compared with that of irrational prescriptions, the median (IQR) score for prescriptions with the diagnosis of cholecystitis was significantly higher for rational prescriptions (standardized regression coefficient=0.183, 270 [270–280] vs 260 [260–260], p < 0.05). In addition, replaced medication (standardized regression coefficient = 0.154, p < 0.05) was significantly associated with the rationality of prescriptions (Table 4).
Discussion
This study focused on the irrational use of carbapenems in surgical departments. Based on the evaluation criteria for carbapenem use in surgical departments established in this study, we found that irrational carbapenem prescriptions in this hospital accounted for 56% of the total sampled prescriptions, which was higher than that in other hospitals.18–20 Although carbapenems remain the cornerstone of the treatment of serious infections, we must pay attention to their irrational use, especially in surgical departments, to alleviate the situation of gram-negative bacteria resistant due to carbapenem abuse.21
Similar to a study by Wagner et al,22 we found a higher proportion of irrational prescriptions for hepatobiliary surgery (55%), gastrointestinal surgery (30%), and neurosurgery (15%). This may be because most of patients in these surgical departments had infection symptoms, such as abdominal infection, intracranial infection, or lung infection; and were older; with underlying diseases. Based on established criteria, we identified the reasons for irrational carbapenem prescription in surgical departments. The selection of carbapenem varieties and usage-dosage-compatibility of carbapenems were relatively reasonable, with rational rates as high as 92% and 96%, respectively. The irrational use of carbapenems was mainly due to medication without indications, improper evaluation of the etiology and efficacy, and imperfect prescription management and consultation. For example, irrational prescriptions had a higher proportion of those with inappropriate indications than rational prescriptions (49% vs 0%, p < 0.05). The univariate analysis had also indicated that indications were related to the rationality of prescriptions. The prescription review revealed that the use of carbapenems in patients without serious infections (53, 28%) was the main manifestation of medications without indications. This indicates that surgeons tend to adopt conservative treatment options because of the fear of negative patient outcomes. Therefore, antibiotic prescriptions are often considered necessary by surgeons, even without a clear indication, conservative intervention to reduce the possible risk of infection.23 For instance, the non-discontinuation of antibiotics after surgery is a common problem for surgeons.17 But the use of special-use antibiotics such as carbapenems to avoid postoperative infections is mostly unreasonable. The view of Charani et al also confirms that surgeon’s fear of negative outcomes for patient outweighs their fear of adverse consequences from inappropriate use of antibiotics.24
This study found that the improper evaluation of etiology and efficacy also accounted for the irrational use of carbapenem because a higher proportion of prescriptions with improper efficacy and etiology evaluations were found in irrational prescriptions (46% vs 8%, p < 0.05). The inappropriate evaluation of etiology and efficacy was mainly due to a lack of etiological or laboratory examination before the use of carbapenem. Nearly a quarter (17.1%) of the carbapenems in this study were prescribed without prior etiological or laboratory examinations, a higher percentage compared to studies in a large UK teaching hospital (5%).25 A study by Bahrampour et al also showed that doctors tend to underestimate etiological examination and the empirical use of carbapenems is common as they believe that the use of extend-ed-spectrum antibiotics would have a rapid and good effect.26,27 Similarly, the proportion of irrational prescription with inappropriate prescription management and consultation was higher than that of reasonable prescriptions (74% vs 13%, p = 0.47). In our study, 41.1% of the carbapenems were prescribed without prior consultation. Surgeons’ knowledge of the rational use of carbapenems may be limited, whereas the lack of multi-disciplinary consultation before prescribing prevents infectious disease doctors, pharmacists and other professionals from judging the rationality of prescriptions, thereby increasing the possibility of unreasonable prescriptions.28 The univariate analysis also indicated the association between evaluation of etiology and efficacy, prescription management and consultation and the rationality of prescription.
Multivariable analysis showed that prescriptions with cholecystitis diagnosis were more reasonable. Existing literatures have showed that carbapenem is usually the priority choice for treatment of cholecystitis.29,30 While we identified the significant association between the replaced medication and the rationality of prescriptions, further research is needed to explore the reason behind this pattern.
Our study results should be interpreted in the context of Chinese health systems.
The large number of patients in surgical departments in China and the unbalanced allocation of medical resources lead to a heavier workload for surgeons, which may be one of the reasons why they cannot strictly follow the regulations of carbapenems use. A study by Massimo et al also found that an unbalanced doctor-patient ratio overwhelms surgeons, thereby reducing their compliance with guidelines and regulations.31 This phenomenon is more common in tertiary hospitals in China, owing to the imperfect tiered medical system.
Additionally, the doctor-patient relationship is in tension, which has a negative impact on doctors’ medication judgment. Poor communication between doctors and patients lead to a high frequency of doctor-patient conflicts in China.32 As a result, many surgeons are more audacious in prescribing antibiotics, particularly the special-use antibiotics such as carbapenems to achieve more “effective” treatment including addressing secondary infections after surgery. In particular, doctors are often under pressure when treating patients with severe infections. Consequently, they often prescribe carbapenems without a rigorous evaluation of the patient’s condition.
A few policy implications can be drawn from our study to promote the rational use of special-use antibiotics such as carbapenems. First, hospitals should establish evaluation criteria for the rationality of carbapenem use, tailored to each department.22 The evaluation criteria designed in this study are helpful for identifying the reasons for irrational prescriptions and can effectively guide doctors to use carbapenems rationally. In the clinical use of carbapenems, antibiotic selection and efficacy evaluation should be considered according to the corresponding patient indications to reduce inappropriate empirical medication. The role of pathogenic examinations also cannot be ignored. Therefore, we suggest that the laboratory examination rate should be used as an indicator for rationality evaluation of carbapenem prescriptions.33
Second, the multi-department cooperation system should be improved, to support the analysis of the rationality of carbapenem use. The hospital needs to promote a multi-disciplinary team (MDT) mechanism to improve the communication and cooperation efficiency of the MDT team during consultations.
Meanwhile, Antimicrobial Stewardship Program (ASP) interventions are still worthy of attention, because the effect of ASP in reducing the irrational use of carbapenems is evident.34–38 Hospital administrators should be aware of the importance of multidisciplinary collaboration in ASP, particularly involving surgeons. Studies have demonstrated that surgeons are less receptive to ASP interventions than other doctors. However, an ASP team involving surgeons can make ASP recommendations more acceptable, thereby promoting the rational use of carbapenems among surgeons.17
Finally, strengthening doctors’ education is important.35,37,39 Hospitals can regularly organize trainings or seminars, and case studies on carbapenem prescription evaluations can be conducted. Simultaneously, hospitals can increase the dissemination of carbapenem guidelines through convenient tools such as brochures, which will help increase doctors’ compliance with the guidelines.
The main limitations of this study are that it was a single-center study, limited to some surgical departments of a tertiary hospital in Southwest China, and the sample size was small. Additionally, the evaluation criteria established in this study did not consider other surgical factors, which may not reflect the complexity of clinical practice. Despite these limitations, we believe that our study is noteworthy because we established a criteria for evaluating the rationality of the clinical use of carbapenems in the surgical department, thus supporting the rational use of carbapenem.
Conclusion
Our study shows that the irrational use of carbapenems deserves more attention, especially in surgical departments. Therefore, interventions for carbapenem use should be developed to reduce the emergence and spread of carbapenem-resistant bacteria. The evaluation criteria for the rationality of the clinical use of carbapenems established in this study may be useful in such interventions.
Statement of Ethics
This study followed the guidelines for human studies and complied with the Declaration of Helsinki. Informed consent was obtained from the study participants prior to study commencement. This work obtained ethical approval from the Ethics Committee of the First Affiliated Hospital of Guangzhou Medical University, China (2019-53).
Acknowledgments
The authors thank all participants who participated in this study. The author expresses his gratitude to the First Affiliated Hospital of Chongqing Medical University and State Key Laboratory of Respiratory Disease for their support. We thank Wang Jiong for her work during the concept interpretation.
Funding
This research was funded by the National Natural Science Foundation of China (Grant Number 81861138056), the National Social Science Foundation of China (Grant Number 20&ZD122), the Investigator-Initiated Trial Fund of The First Affiliated Hospital of Guangzhou Medical University (Grant Number DSPC-MPM002).
Disclosure
The authors declare no conflict of interest.
References
1. Browne AJ, Chipeta MG, Haines-Woodhouse G, et al. Global antibiotic consumption and usage in humans, 2000–18: a spatial modelling study. Lancet Planetary Health. 2021;5(12):e893–e904. doi:10.1016/S2542-5196(21)00280-1
2. Murray CJ, Ikuta KS, Sharara F, et al. Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. Lancet. 2022;399(10325):629–655. doi:10.1016/S0140-6736(21)02724-0
3. Zequinão T, Telles JP, Gasparetto J, Tuon FF. Carbapenem stewardship with ertapenem and antimicrobial resistance-A scoping review. Rev Soc Bras Med Trop. 2020;53. doi:10.1590/0037-8682-0413-2020
4. Sadyrbaeva-Dolgova S, Aznarte-Padial P, Jimenez-Morales A, Expósito-Ruiz M, Calleja-Hernández MÁ, Hidalgo-Tenorio C. Pharmacist recommendations for carbapenem de-escalation in urinary tract infection within an antimicrobial stewardship program. J Infect Public Health. 2020;13(4):558–563. doi:10.1016/j.jiph.2019.09.014
5. López-Viñau T, Peñalva G, García-Martínez L, et al. Impact of an antimicrobial stewardship program on the incidence of carbapenem resistant Gram-negative bacilli: an interrupted time-series analysis. Antibiotics. 2021;10(5):586. doi:10.3390/antibiotics10050586
6. Peri AM, Doi Y, Potoski BA, Harris PN, Paterson DL, Righi E. Antimicrobial treatment challenges in the era of carbapenem resistance. Diagn Microbiol Infect Dis. 2019;94(4):413–425. doi:10.1016/j.diagmicrobio.2019.01.020
7. Nordmann P, Poirel L. Epidemiology and diagnostics of carbapenem resistance in gram-negative bacteria. Clin Infect Dis. 2019;69(Supplement_7):S521–S528. doi:10.1093/cid/ciz824
8. Hu F, Guo Y, Zhu D, et al. CHINET surveillance of bacterial resistance across China: report of the results in 2016. Chin J Infect Chemother. 2017;24:481–491.
9. Hu F, Zhu D, Wang F, Wang M. Current status and trends of antibacterial resistance in China. Clin Infect Dis. 2018;67(suppl_2):S128–S134. doi:10.1093/cid/ciy657
10. Qu X, Yin C, Sun X, et al. Consumption of antibiotics in Chinese public general tertiary hospitals (2011–2014): trends, pattern changes and regional differences. PLoS One. 2018;13(5):e0196668. doi:10.1371/journal.pone.0196668
11. Hao Y, Chen S, Chang H, et al. Temporal association between Carbapenems usage and antimicrobial resistance in gram-negative bacteria at a tertiary hospital in Nanjing, China. Diagn Microbiol Infect Dis. 2020;98(2):115083. doi:10.1016/j.diagmicrobio.2020.115083
12. National Health Commission of the People’s Republic of China. 2020 national bacterial resistance surveillance report. 2020.
13. National Health Commission of the People’s Republic of China. Expert consensus on the clinical application of carbapenems in China. 2018.
14. Solomkin JS, Mazuski JE, Bradley JS, et al. Diagnosis and management of complicated intra-abdominal infection in adults and children: guidelines by the Surgical Infection Society and the Infectious Diseases Society of America. Surg Infect. 2010;11(1):79–109. doi:10.1089/sur.2009.9930
15. Evans L, Rhodes A, Alhazzani W, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021. Intensive Care Med. 2021;47(11):1181–1247. doi:10.1007/s00134-021-06506-y
16. Tamma PD, Aitken SL, Bonomo RA, Mathers AJ, van Duin D, Clancy CJ. Infectious Diseases Society of America 2022 guidance on the treatment of extended-spectrum β-lactamase producing Enterobacterales (ESBL-E), carbapenem-resistant Enterobacterales (CRE), and Pseudomonas aeruginosa with difficult-to-treat resistance (DTR-P. aeruginosa). Clin Infect Dis. 2022;75(2):187–212. doi:10.1093/cid/ciac268
17. Badia JM, Batlle M, Juvany M, et al. Surgeon-led 7-VINCut antibiotic stewardship intervention decreases duration of treatment and carbapenem use in a general surgery service. Antibiotics. 2020;10(1):11. doi:10.3390/antibiotics10010011
18. Poline J, Postaire M, Parize P, et al. Stewardship program on carbapenem prescriptions in a tertiary hospital for adults and children in France: a cohort study. Eur J Clin Microbiol Infect Dis. 2021;40(5):1039–1048. doi:10.1007/s10096-020-04103-3
19. Suzuki H, Perencevich E, Goto M, et al. A comprehensive assessment of carbapenem use across 90 Veterans Health Administration hospitals with defined stewardship strategies for carbapenems. J Antimicrob Chemother. 2021;76(5):1358–1365. doi:10.1093/jac/dkab008
20. Zhang D, Cui K, Lu W, et al. Evaluation of carbapenem use in a tertiary hospital: antimicrobial stewardship urgently needed. Antimicrob Resist Infect Control. 2019;8(1):1–7. doi:10.1186/s13756-018-0449-3
21. Patrier J, Timsit J-F. Carbapenem use in critically ill patients. Curr Opin Infect Dis. 2020;33(1):86–91. doi:10.1097/QCO.0000000000000622
22. Wagner JL, Rhodes NJ, Scheetz MH, et al. Opportunities for antimicrobial stewardship among carbapenem-treated patients in 18 North American hospitals. Int J Antimicrob Agents. 2020;55(6):105970. doi:10.1016/j.ijantimicag.2020.105970
23. Charani E, Tarrant C, Moorthy K, Sevdalis N, Brennan L, Holmes A. Understanding antibiotic decision making in surgery—a qualitative analysis. Clin Microbiol Infect. 2017;23(10):752–760. doi:10.1016/j.cmi.2017.03.013
24. Charani E, Ahmad R, Rawson T, Castro-Sanchèz E, Tarrant C, Holmes A. The differences in antibiotic decision-making between acute surgical and acute medical teams: an ethnographic study of culture and team dynamics. Clin Infect Dis. 2019;69(1):12–20. doi:10.1093/cid/ciy844
25. Olusoga A, Howard P, Walker C, Atack K, Waterhouse A. Carbapenem stewardship in a large teaching English hospital-are we improving? Access Microbiol. 2020;2(2):164. doi:10.1099/acmi.fis2019.po0162
26. Perron J, Baldolli A, Isnard C, de La Blanchardière A, Saint-Lorant G. Assessing the relevance of carbapenem prescriptions by an antibiotic stewardship team. Médecine et Maladies Infectieuses. 2020;50(4):346–351. doi:10.1016/j.medmal.2019.06.004
27. Bahrampour Juybari K, Vosooghi V, Zahmatkesh M, Mirmohammadkhani M, Paknazar F. Compliance of imipenem and meropenem administration with the national antimicrobial stewardship program in a referral teaching hospital in Iran. Hosp Pract. 2022;50(1):49–54. doi:10.1080/21548331.2021.2022358
28. Lee C-R, Lee JH, Kang L-W, Jeong BC, Lee SH. Educational effectiveness, target, and content for prudent antibiotic use. Biomed Res Int. 2015;2015. doi:10.1155/2015/214021
29. Gluhovschi C, Gadalean F, Velciov S, et al. Acute acalculous cholecystitis associated with abscesses—an unknown dual pathology. Biomedicines. 2023;11(2):632. doi:10.3390/biomedicines11020632
30. Suh S-W, Choi YS, Choi S-H, et al. Antibiotic selection based on microbiology and resistance profiles of bile from gallbladder of patients with acute cholecystitis. Sci Rep. 2021;11(1):2969. doi:10.1038/s41598-021-82603-8
31. Sartelli M, Hardcastle C, Catena F, et al. Antibiotic use in low and middle-income countries and the challenges of antimicrobial resistance in surgery. Antibiotics. 2020;9(8):497. doi:10.3390/antibiotics9080497
32. Lancet T; Lancet. Protecting Chinese doctors. Lancet. 2020;395:90. doi:10.1016/S0140-6736(20)30003-9
33. Xin C, Xia Z, Li G. The impact of pharmaceutical interventions on the use of carbapenems in a Chinese hospital: a pre–post study. Infect Drug Resist. 2019;12:3567. doi:10.2147/IDR.S229009
34. Akazawa T, Kusama Y, Fukuda H, et al. Eight-Year Experience of Antimicrobial Stewardship Program and the Trend of Carbapenem Use at a Tertiary Acute-Care Hospital in Japan—the Impact of Postprescription Review and Feedback. Oxford University Press US; 2019:ofz389.
35. Fortini A, Faraone A, Di Pietro M, et al. Antimicrobial stewardship in an Internal Medicine ward: effects on antibiotic consumption and on the use of carbapenems. Intern Emerg Med. 2018;13(8):1219–1226. doi:10.1007/s11739-018-1916-9
36. García-Rodríguez JF, Bardan-Garcia B, Juiz-Gonzalez PM, Vilarino-Maneiro L, Alvarez-Diaz H, Marino-Callejo A. Long-term carbapenems antimicrobial stewardship program. Antibiotics. 2020;10(1):15. doi:10.3390/antibiotics10010015
37. Yusef D, Hayajneh WA, Bani Issa A, et al. Impact of an antimicrobial stewardship programme on reducing broad-spectrum antibiotic use and its effect on carbapenem-resistant Acinetobacter baumannii (CRAb) in hospitals in Jordan. J Antimicrob Chemother. 2021;76(2):516–523. doi:10.1093/jac/dkaa464
38. Faraone A, Poggi A, Cappugi C, et al. Inappropriate use of carbapenems in an internal medicine ward: impact of a carbapenem-focused antimicrobial stewardship program. Eur J Intern Med. 2020;78:50–57. doi:10.1016/j.ejim.2020.03.017
39. Okeah BO, Morrison V, Huws JC. Antimicrobial stewardship and infection prevention interventions targeting healthcare-associated Clostridioides difficile and carbapenem-resistant Klebsiella pneumoniae infections: a scoping review. BMJ open. 2021;11(8):e051983. doi:10.1136/bmjopen-2021-051983
40. Wilson APR. Sparing carbapenem usage. J Antimicrob Chemother. 2017;72(9):2410–2417. doi:10.1093/jac/dkx181
41. Li Y-Y, Wang J, Wang R, Cai Y. Double-carbapenem therapy in the treatment of multidrug resistant Gram-negative bacterial infections: a systematic review and meta-analysis. BMC Infect Dis. 2020;20(1):1–13.
42. Schneider F, Gessner A, El-Najjar N. Efficacy of vancomycin and meropenem in central nervous system infections in children and adults: current update. Antibiotics. 2022;11(2):173. doi:10.3390/antibiotics11020173
43. Bookstaver PB, Bland CM, Griffin B, Stover KR, Eiland LS, McLaughlin M. A review of antibiotic use in pregnancy. Pharmacotherapy. 2015;35(11):1052–1062. doi:10.1002/phar.1649
44. Wu -C-C, Pai T-Y, Hsiao F-Y, Shen L-J, Wu F-L-L. The effect of different carbapenem antibiotics (ertapenem, imipenem/ cilastatin, and meropenem) on serum valproic acid concentrations. Ther Drug Monit. 2016;38(5):587–592. doi:10.1097/FTD.0000000000000316
45. Al-Quteimat O, Laila A. Valproate interaction with carbapenems: review and recommendations. Hosp Pharm. 2020;55(3):181–187. doi:10.1177/0018578719831974
46. Heo Y-A. Imipenem/cilastatin/relebactam: a review in Gram-negative bacterial infections. Drugs. 2021;81:377–388. doi:10.1007/s40265-021-01471-8
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.