Back to Journals » Journal of Pain Research » Volume 14
Evaluating the Quality of Reports About Randomized Controlled Trials of Acupuncture for Low Back Pain
Authors Liu X ![]() , Xu Z, Wang Y
, Xu Z, Wang Y ![]() , Luo H, Zou D, Zhou Z, Zhuang L
, Luo H, Zou D, Zhou Z, Zhuang L ![]()
Received 23 February 2021
Accepted for publication 1 April 2021
Published 21 April 2021 Volume 2021:14 Pages 1141—1151
DOI https://doi.org/10.2147/JPR.S308006
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Houman Danesh
Xin Liu,1 Ziqiao Xu,1 Yuting Wang,1 Huiling Luo,1 Donglei Zou,1 Ziyuan Zhou,2 Lixing Zhuang3
1Clinical Medical College of Acupuncture Moxibustion and Rehabilitation, Guangzhou University of Chinese Medicine, Guangzhou, 510000, People’s Republic of China; 2Faculty of Science, The University of Hong Kong, Hong Kong, 999077, People’s Republic of China; 3Department of Rehabilitation, The First Affiliated Hospital of Guangzhou University of Chinese Medicine, Guangzhou, 510000, People’s Republic of China
Correspondence: Lixing Zhuang
Department of Rehabilitation, The First Affiliated Hospital of Guangzhou University of Chinese Medicine, No. 16 Airport Road, Baiyun District, Guangzhou, People’s Republic of China
Tel +86 13822287775
Email [email protected]
Objective: This study aims to improve the reporting quality of randomized controlled trials (RCTs) by evaluating RCTs of acupuncture for low back pain (LBP) based on the CONSORT and STRICTA statements.
Methods: Literature from the Cochrane Library, Medline, Embase, Ovid, China National Knowledge Infrastructure (CNKI), WanFang database, and Chongqing Weipu (VIP) was systematically searched from 2010 to 2020. The general characteristics and the overall quality score (OQS) of the literature were evaluated by two investigators. The agreement between investigators was calculated using Cohen’s kappa statistics.
Results: A total of 31 RCTs were extracted in the final analysis. Based on the CONSORT statement, the items “title and abstract”, “background and objectives”, “intervention”, “outcomes”, “statistical methods”, “baseline data”, “outcomes and estimation” and “interpretation” have a positive rate of greater than 80%. The items “implementation”, “generalizability” and “protocol” have a positive rate of less than 30%. Based on the STRICTA statement, the items “style of acupuncture”, “needle retention time”, “number of treatment sessions”, “frequency and duration of treatment” and “precise description of the control or comparator” have a positive rate of greater than 80%. The item “extent to which the treatment was varied” has a positive rate of less than 30%. The agreements among most items are determined to be moderate or good.
Conclusion: The reporting quality of RCTs of acupuncture for LBP is moderate. Researchers should rigidly follow the CONSORT and STRICTA statements to enhance the quality of their studies.
Keywords: acupuncture, quality of reporting, low back pain, CONSORT, STRICTA
Introduction
Low back pain (LBP), which is defined by an area of pain that is typically localized between the edge of the ribs and the crease of the hips,1 is a problematic symptom. Once someone has problems with any part of the spine or part attached to the spine, such as lumbar intervertebral discs, ligaments, fascia, and muscles, LBP can occur.2 The incidence of LBP was 7.3% globally in 2015,1 meaning that approximately 540 million people suffered from LBP. In addition, it has been reported that one out of every six patients suffering from musculoskeletal problems is diagnosed with LBP.3 Although the number of LBP patients is large, LBP is usually tolerable. The prognosis represents a threat to LBP patients. Disability, for example, is the worst prognosis of LBP, representing a heavy burden to families and society.4 Due to poor medical conditions and harsh working conditions, the incidence of LBP in low-income countries or regions is rather high.5 According to the guidelines of LBP,6 nonsteroidal anti-inflammatory drugs (NASIDs) are recommended as the first-line therapy. Acupuncture is also recommended. However, NASIDs might cause bleeding7 and lead to gastrointestinal damage.8 Thus, patients have to pay extra money for other medicines that can protect the gastrointestinal tract. Compared with NASIDs, acupuncture seems safer because it has been reported to have fewer adverse events.9 Currently, acupuncture is increasingly accepted as a complementary or alternative therapeutic method. In America, approximately 54% of the population uses complementary or alternative therapy, especially for LBP.10 In China, the use of acupuncture is even higher. Therefore, acupuncture for LBP has attracted the attention of researchers, so many trials have been performed.
Established in 1996 and updated in 2017, the Consolidated Standards for Reporting Trials (CONSORT)11,12 has the goals of improving the transparency of trials and avoiding resource waste. The STandards for Reporting Interventions in Controlled Trials of Acupuncture (STRICTA)13,14 was established in 2002 and updated in 2010. As an extension of CONSORT for acupuncture, STRICTA has the goal of increasing the rigor of acupuncture trial design. To the best of our knowledge, there is no article evaluating the quality of acupuncture for LBP based on CONSORT and STRICTA statements. Based on the above two statements, this study evaluates the reporting quality of acupuncture for LBP.
Materials and Methods
Search Strategy
To identify all articles that studied the efficacy of acupuncture on LBP, the following databases were searched from January 2010 to December 2020: Cochrane Library, Medline, Embase, Ovid, China National Knowledge Infrastructure (CNKI), WanFang database, and Chongqing Weipu (VIP). In particular, we found that the trend of published articles about LBP was obviously increasing in the pilot search. Therefore, we aimed to search articles in the last 10 years. The following search terms were used in Chinese and English: (Acupuncture OR Acupuncture therapy OR Electro-acupuncture OR Manual acupuncture OR Warming acupuncture OR Auricular acupuncture OR Ear acupuncture OR Thread embedding acupuncture OR Motion style acupuncture) AND (Low Back Pain OR Back Pain, Low OR Back Pain, Low OR Low Back Pain OR Pain, Low Back OR Pain, Low Back OR Lumbago OR Lower Back Pain OR Back Pain, Lower OR Back Pain, Lower OR Lower Back Pains OR Pain, Lower Back OR Pains, Lower Back OR Low Back Ache OR Ache, Low Back OR Aches, Low Back OR Back Ache, Low OR Back Aches, Low OR Low Back Aches OR Low Backache OR Backache, Low OR Backaches, Low OR Low Backaches OR Low Back Pain, Postural OR Postural Low Back Pain OR Low Back Pain, Posterior Compartment OR Low Back Pain, Recurrent OR Recurrent Low Back Pain OR Low Back Pain, Mechanical OR Mechanical Low Back Pain OR low back pain).
Included and Excluded Criteria
Types of Studies
We searched for randomized controlled trials (RCTs) that compared acupuncture with at least one control strategy for the treatment of LBP. The intervention of the control group can be another form of acupuncture or conventional treatment. RCTs without available data for extraction were excluded.
Types of Participants
All LBP patients of any age, gender and ethnicity were eligible. The clinical diagnosis of LBP was followed by expert consensus based on the site, duration, frequency and severity of the pain, excluding pain from feverish illness or menstruation.15 Patients who suffered from LBP for at least 6 months with or without lumbar disc protrusion screened by computed tomography or magnetic resonance imaging were included.
Types of Intervention
Different forms of acupuncture techniques or needles, such as manual acupuncture, electroacupuncture, warming acupuncture, auricular acupuncture, thread embedding acupuncture, and motion style acupuncture, were included. In particular, acupuncture plus cupping, moxibustion and Chinese medicine were not included in this research. The intervention in the experimental group was acupuncture alone or acupuncture combined with medication, which is similar to the control group. The control group used placebo acupuncture, sham acupuncture, no treatment or conventional treatment.
Placebo acupuncture means that a semiblunt retractable needle did touch but did not pierce the skin.16 Sham acupuncture refers to a needle set on nonacupuncture points or acupuncture points not related to LBP.17 A modified nonfunctioning electroacupuncture stimulator was used to contrast with real electroacupuncture.
Selection of Reports
First, two investigators (HLL and DLZ) preliminarily searched RCTs according to the title and abstract on their own. Second, the investigators read the full text of reports for further selection following rigid inclusion and exclusion criteria. Third, after inspecting the selected reports for consistency, the studies were moved into the specified folders with different labels (included, excluded, undecided). Another magisterial investigator (LXZ) made a final decision regarding whether the reports in the “undecided” folder were included.
Data Extraction
Two investigators (HLL and DLZ) used Microsoft Excel 2019 to record study information, including author, publication year, language of the article, number of participants, intervention and course of treatment, from the final selection of RCTs. If the information was missing, then “no mention” was recorded. The investigators checked the sheet for consistency. Another magisterial investigator (ZLX) determined how to resolve any discrepancies noted in the sheets.
Assessment of Reporting Quality
Two investigators (ZQX and YTW) scored the reporting quality of RCTs of acupuncture for LBP individually based on the CONSORT and STRICTA statements. Before assessment, two investigators had a complete understanding of these two standards. Each item was scored 1 if it was reported and 0 if it was not mentioned or unclear (see the details in the Supplementary Materials). To assess the agreement between two investigators, Cohen’s κ-statistic18 was calculated using IBM SPSS Statistics version 26 (IBM SPSS Inc., Chicago, USA). According to Cohen’s definition, agreement was evaluated as perfect if κ was >0.8, good if 0.6 < κ ≤ 0.8, moderate if 0.4 < κ ≤ 0.6, fair if 0.2 < κ ≤ 0.4, and poor if κ was ≤0.2.
Results
A total of potentially relevant RCTs were identified from 7 databases. After reading the title, abstract and full text, 31 RCTs were extracted for the final analysis. The whole selection process is depicted in Figure 1, and the general characteristics of the 31 included RCTs are summarized in Table 1.
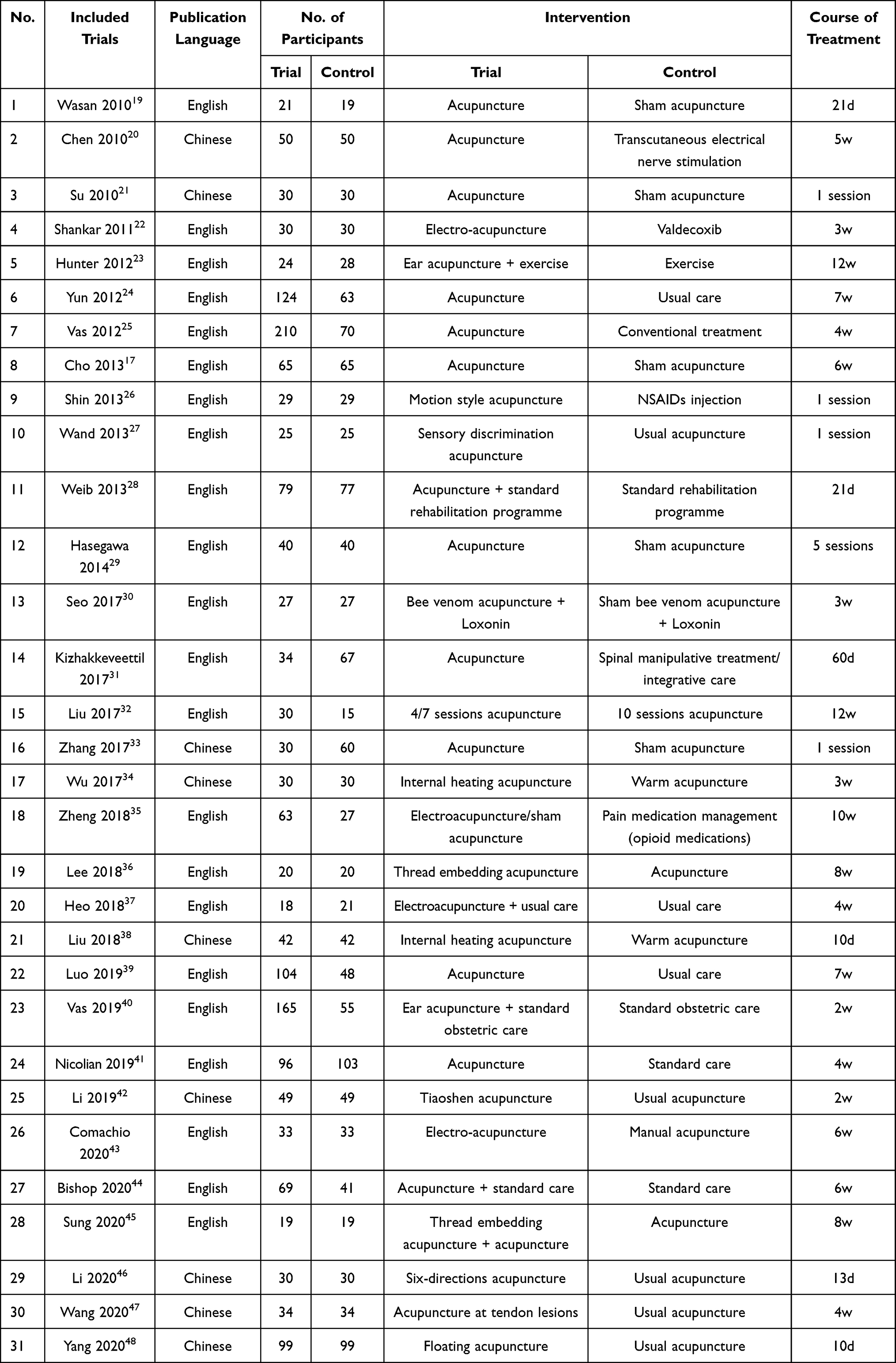 |
Table 1 General Characteristics of the Included 31 Studies |
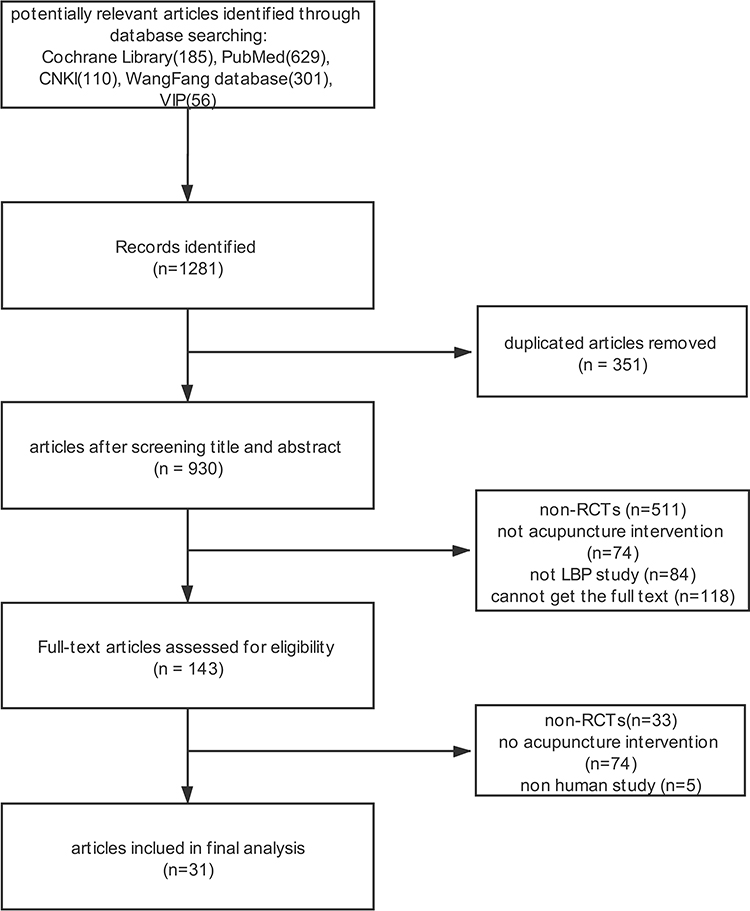 |
Figure 1 Flow chart of selection process. 31 RCTs were extracted for the final analysis. |
Year of Publication
In total, 31 RCTs were published in the last 10 years from 2010 to 2020. The average scores of each year based on the CONSORT and STRICTA statements are presented in the line chart (Figure 2).
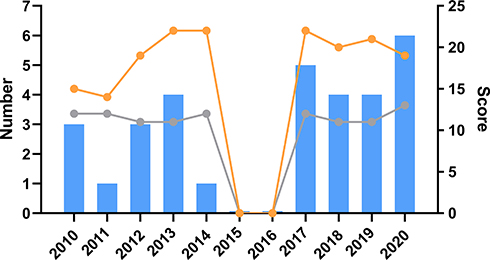 |
Figure 2 Year of publication. The blue bar is the number of RCTs published each year. The orange line is the median OQS with CONSORT statement of each year. The gray line is the median OQS with STRICTA statement of each year. |
Publication Language and Nationality of Authors
Among the 31 RCTs, 22 RCTs (71%) were published in English, whereas 9 (29%) were published in Chinese. The authors of these articles were from America, Australia, Brazil, China, France, Germany, India, Korea, New Zealand and Spain.
Invention
In the final extracted studies, different forms of acupuncture, including usual acupuncture (58.1%), electroacupuncture (12.9%), ear acupuncture (6.5%), internal heating acupuncture (6.5%), thread embedding acupuncture (6.5%), bee venom acupuncture (3.2%), floating acupuncture (3.2%) and motion style acupuncture (3.2%), were used.
Funding Resources
Sixteen studies (51.2%) reported their sources of funding. Nine (56.3%) received national funding, 2 (12.5%) received university funding, 4 (25.0%) received regional funding and 1 (6.3%) received personal funding. None of the included studies received funding from pharmaceutical companies.
Quality of Reporting
Reporting Quality Score Based on CONSORT Items
Based on the CONSORT statement, the data of overall quality of reporting are listed in Table 2. Among all included studies, the median overall quality score (OQS) was 20, ranging from 8 to 27. Good reporting included terms of “title and abstract”, “background and objectives”, “intervention”, “outcomes”, “statistical methods”, “baseline data”, “outcomes and estimation” and “interpretation” with a positive rate of greater than 80%. Nevertheless, poor reporting was noted for terms of “implementation”, “generalizability” and “protocol” with a positive rate of less than 30%. All items have moderate, good or perfect agreement, except for the items of “background and objectives-2.a” and “generalizability”, which have fair agreement. OQS details are listed in Table 2.
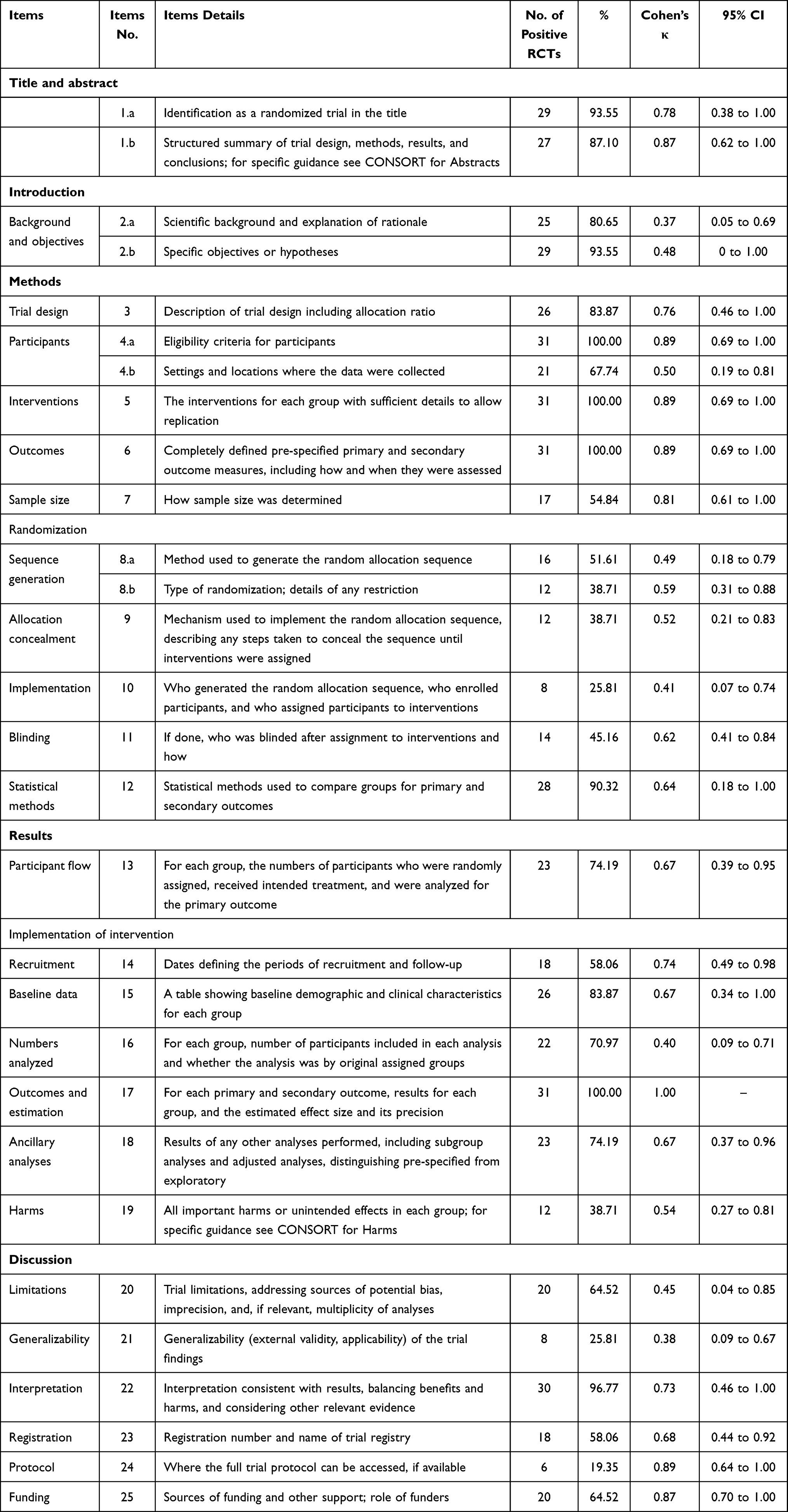 |
Table 2 Details of OQS Assessed with CONSORT Statement (n=31) |
Reporting Quality Score Based on STRICTA Items
Based on the STRICTA statement, the data of overall quality of reporting are listed in Table 3. Among all included studies, the median OQS was 12, ranging from 8 to 16. Good reporting was noted for the terms of “style of acupuncture”, “needle retention time”, “number of treatment sessions”, “frequency and duration of treatment” and “precise description of the control or comparator” with a positive rate of greater than 80%. Nevertheless, poor reporting was noted for the term “extent to which treatment was varied” with a positive rate of less than 30%. All items had moderate, good or perfect agreement. OQS details are listed in Table 3.
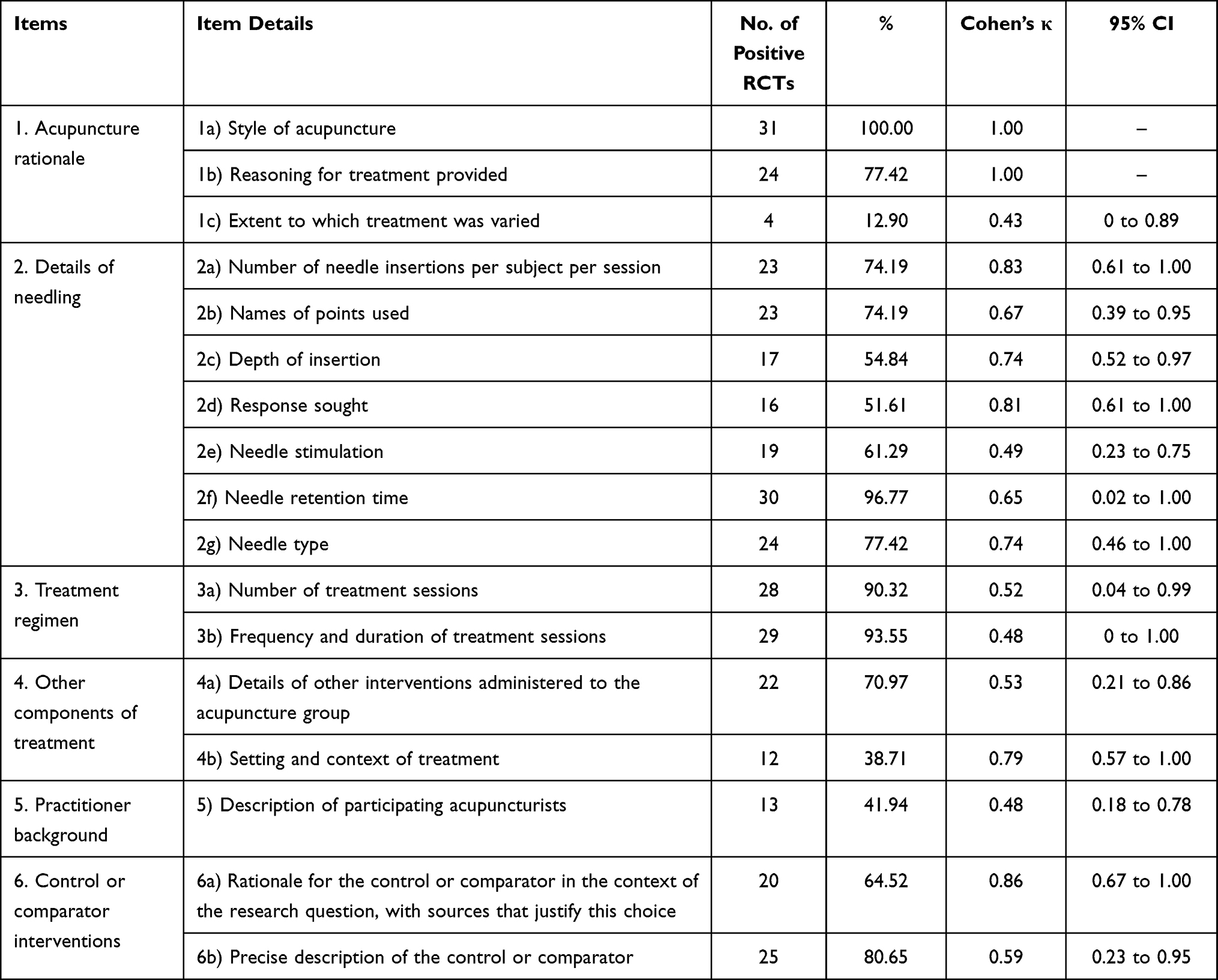 |
Table 3 The Details of OQS Assessed with STRICTA Statement (n=31) |
Discussion
This study first showed the reporting quality of RCTs that assessed the efficacy of acupuncture for LBP, adhering strictly to the CONSORT and STRICTA statements. Good quality RCTs not only reduce the bias of the trial but also contribute to the development of guidelines.49 Therefore, a good quality study has positive meaning.
The OQS of RCTs based on the CONSORT statement was not satisfactory enough. Almost every included study prominently illustrated that the study was an RCT in the title. However, the positive rate of the items of randomization was low, and the positive rate for the item “implementation” was even less than 30%. Most of the studies stated that they allocated patients randomized but without details. The studies did not mention the method used to generate the random allocation sequence or the mechanism used to implement the random allocation sequence. Moreover, only 8 RCTs (25.81%) reported the person who generated the random allocation sequence. Accurate randomization eliminates the selection bias to the maximum extent and ascertains how well the randomization materials are performed.50 Therefore, researchers should pay more attention to the randomization methodology to ensure that their study is randomized correctly and to improve the quality of the study.
Given the particularities of acupuncture, many problems still need to be solved when considering blindness. Although advanced placebo acupuncture needles51 that broke the stereotype that only naïve acupuncture studies can be double-blinded52 were invented, it is difficult to completely and simultaneously blind patients and intervenors.53 Therefore, most of the included RCTs blinded patients or investigators who analyzed the data. Despite the difficulties in blinding, researchers should make efforts employ blindness in the trials to eliminate the expectation bias that seems inevitable at present.
Due to the small sample size of the included RCTs, the positive rate of generalizability was less than 30%. This item is relatively subjective, and the agreement of the two investigators is low. Therefore, multicenter, large-scale RCTs are needed to improve generalizability.
To our surprise, only 6 RCTs (19.35%) reported that the protocol was accessed, whereas 18 RCTs (58.06%) reported their registration number. The importance of a protocol is that it describes the entire process and the details of a study. If one small step in the entire trial goes wrong, the whole trial may be worthless or might need to be performed again, wasting time and money. Magisterial experts can judge the feasibility of a study by reading the protocol and agree to the ethical assessment of the study. However, according to the results, the number of registered trials and trials with protocols that can be assessed is not equal. This finding indicates that some of the included trials might not have a rigorous design.
The OQS of RCTs based on the STRICTA statement do not reach satisfactory levels, especially for the item “extent to which the treatment was varied”. According to traditional Chinese medical theory,54 different syndromes require different treatments. This principle is also applicable in acupuncture. Therefore, LBP patients need personalized acupuncture therapeutic schedules. However, only 3 RCTs (9.68%) reported changes in acupuncture, and the remaining researchers spent more time on the acupuncture rationale. We also found that the OQS values of Chinese RCTs were greater than those of English RCTs based on the STRICTA statement. However, the OQS values of Chinese RCTs were lower than those of English RCTs based on the CONSORT statement. Given that acupuncture can be traced back over 3000 years in China, the Chinese formed a relatively perfect therapeutic system. Chinese researchers might think more apprehensively when making acupuncture schedules. However, regarding the standard trial design, Chinese researchers were less thoughtful than foreign researchers. We found that the OQS trend of each year was quite flat (Figure 2), and the average score of the included RCTs with STRICTA was 12 of 17, indicating that the reporting quality was always greater than moderate. Thus, we believe that spending more time on the acupuncture rationale is the key to enhancing the quality of acupuncture trials.
Although we systematically analyzed 31 RCTs, there are still some limitations in this study. Due to language barriers, we only included RCTs published in English and Chinese and excluded RCTs published in Korean or Japanese. Acupuncture is widely used in Korea and Japan, resulting in the loss of valuable data about the use of acupuncture for the treatment of LBP.
Conclusions
This study indicates that the reporting quality of RCTs that assessed the efficacy of acupuncture for LBP was moderate and needs further improvement to increase the level of evidence and guide clinical treatment better. In particular, the randomization methodology and acupuncture rationale should be explicitly explained in the article. These findings emphasize the need to improve the standard of operation. Therefore, we recommend that researchers draft acupuncture protocols rigidly based on the CONSORT and STRICTA statements to enhance the OQS of their studies, thereby convincing more people that acupuncture has good efficacy in the treatment of LBP.
Data Sharing Statement
The data used to support the findings of this study are included within the article and Supplementary Information.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. In particular, Nanbu Wang, who has the overseas experience in Massachusetts General Hospital, polished up this article and edited the layout of this article. Thanks for her contribution.
Funding
This work was supported by the National Administration of Traditional Chinese Medicine (GZY-KJS-2020-072), the Science and Technology Department of Guangdong Province (2018-5).
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Hartvigsen J, Hancock M, Kongsted A, et al. What low back pain is and why we need to pay attention. Lancet. 2018;391(10137):2356–2367. doi:10.1016/S0140-6736(18)30480-X
2. Navani A, Manchikanti L, Albers S, et al. Responsible, safe, and effective use of biologics in the management of low back pain: American Society of Interventional Pain Physicians (ASIPP) guidelines. Pain Physician. 2019;22(1):S1–S74. doi:10.36076/ppj/2019.22.s1
3. Jöud A, Petersson I, Englund M. Low back pain: epidemiology of consultations. Arthritis Care Res. 2012;64(7):1084–1088.
4. Vos T, Allen C, Arora M, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016;388(10053):1545–1602.
5. Hoy D, Smith E, Cross M, et al. Reflecting on the global burden of musculoskeletal conditions: lessons learnt from the global burden of disease 2010 study and the next steps forward. Ann Rheum Dis. 2015;74(1):4–7. doi:10.1136/annrheumdis-2014-205393
6. Qaseem A, Wilt T, Mclean R, et al. Noninvasive treatments for acute, subacute, and chronic low back pain: a clinical practice guideline from the American College of Physicians. Ann Intern Med. 2017;166(7):514–530. doi:10.7326/M16-2367
7. Perahia D, Bangs M, Zhang Q, et al. The risk of bleeding with duloxetine treatment in patients who use nonsteroidal anti-inflammatory drugs (NSAIDs): analysis of placebo-controlled trials and post-marketing adverse event reports. Drug Healthc Patient Saf. 2013;5(1):211–219. doi:10.2147/DHPS.S45445
8. Smecuol E, Bai J, Sugai E, et al. Acute gastrointestinal permeability responses to different non-steroidal anti-inflammatory drugs. Gut. 2001;49(5):650–655. doi:10.1136/gut.49.5.650
9. Clarkson C, O’mahony D, Jones D. Adverse event reporting in studies of penetrating acupuncture during pregnancy: a systematic review. Acta Obstet Gynecol Scand. 2015;94(5):453–464. doi:10.1111/aogs.12587
10. Wolsko P, Eisenberg D, Davis R, et al. Patterns and perceptions of care for treatment of back and neck pain: results of a national survey. Spine. 2003;28(3):292–298. doi:10.1097/01.BRS.0000042225.88095.7C
11. Begg C, Cho M, Eastwood S, et al. Improving the quality of reporting of randomized controlled trials. The CONSORT statement. JAMA. 1996;276(8):637–639. doi:10.1001/jama.1996.03540080059030
12. Boutron I, Altman D, Moher D, et al. CONSORT statement for randomized trials of nonpharmacologic treatments: a 2017 update and a CONSORT extension for nonpharmacologic trial abstracts. Ann Intern Med. 2017;167(1):40–47. doi:10.7326/M17-0046
13. Macpherson H, Altman D, Hammerschlag R, et al. Revised STandards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA): extending the CONSORT statement. PLoS Med. 2010;7(6):e1000261. doi:10.1371/journal.pmed.1000261
14. Macpherson H, White A, Cummings M, et al. Standards for reporting interventions in controlled trials of acupuncture: the STRICTA recommendations. Complement Ther Med. 2001;9(4):246–249. doi:10.1054/ctim.2001.0488
15. Dionne C, Dunn K, Croft P, et al. A consensus approach toward the standardization of back pain definitions for use in prevalence studies. Spine. 2008;33(1):95–103. doi:10.1097/BRS.0b013e31815e7f94
16. Schlaeger J, Takakura N, Yajima H, et al. Double-blind acupuncture needles: a multi-needle, multi-session randomized feasibility study. Pilot Feasibil Stud. 2018;4:72. doi:10.1186/s40814-018-0265-9
17. Cho Y, Song Y, Cha Y, et al. Acupuncture for chronic low back pain: a multicenter, randomized, patient-assessor blind, sham-controlled clinical trial. Spine. 2013;38(7):549–557. doi:10.1097/BRS.0b013e318275e601
18. Cohen JA. Coefficient of agreement for nominal scales. Educ Psychol Meas. 1960;20(1):37–46. doi:10.1177/001316446002000104
19. Wasan A, Kong J, Pham L, et al. The impact of placebo, psychopathology, and expectations on the response to acupuncture needling in patients with chronic low back pain. J Pain. 2010;11(6):555–563. doi:10.1016/j.jpain.2009.09.013
20. Chen LX, Duan JF, Wang YQ, et al. A randomized controlled study of acupuncture combined with percutaneous electrical nerve stimulation for chronic low back pain. J Cervicodynia Lumbodynia. 2010;31(02):137–138.
21. Su JT, Zhou QH, Li R, et al. Immediate analgesic effect of wrist-ankle acupuncture for acute lumbago:a randomized controlled trial. Chin Acupuncture Moxibustion. 2010;30(08):617–622.
22. Shankar N, Thakur M, Tandon O, et al. Autonomic status and pain profile in patients of chronic low back pain and following electro acupuncture therapy: a randomized control trial. Indian J Physiol Pharmacol. 2011;55(1):25–36.
23. Hunter R, Mcdonough S, Bradbury I, et al. Exercise and auricular acupuncture for chronic low-back pain: a feasibility randomized-controlled trial. Clin J Pain. 2012;28(3):259–267. doi:10.1097/AJP.0b013e3182274018
24. Yun M, Shao Y, Zhang Y, et al. Hegu acupuncture for chronic low-back pain: a randomized controlled trial. J Altern Complement Med. 2012;18(2):130–136. doi:10.1089/acm.2010.0779
25. Vas J, Aranda J, Modesto M, et al. Acupuncture in patients with acute low back pain: a multicentre randomised controlled clinical trial. Pain. 2012;153(9):1883–1889. doi:10.1016/j.pain.2012.05.033
26. Shin J, Ha I, Lee J, et al. Effects of motion style acupuncture treatment in acute low back pain patients with severe disability: a multicenter, randomized, controlled, comparative effectiveness trial. Pain. 2013;154(7):1030–1037. doi:10.1016/j.pain.2013.03.013
27. Wand B, Abbaszadeh S, Smith A, et al. Acupuncture applied as a sensory discrimination training tool decreases movement-related pain in patients with chronic low back pain more than acupuncture alone: a randomised cross-over experiment. Br J Sports Med. 2013;47(17):1085–1089. doi:10.1136/bjsports-2013-092949
28. Weiss J, Quante S, Xue F, et al. Effectiveness and acceptance of acupuncture in patients with chronic low back pain: results of a prospective, randomized, controlled trial. J Altern Complement Med. 2013;19(12):935–941. doi:10.1089/acm.2012.0338
29. Hasegawa T, Baptista A, De Souza M, et al. Acupuncture for acute non-specific low back pain: a randomised, controlled, double-blind, placebo trial. Acupuncture Med. 2014;32(2):109–115. doi:10.1136/acupmed-2013-010333
30. Seo B, Han K, Kwon O, et al. Efficacy of bee venom acupuncture for chronic low back pain: a randomized, double-blinded, sham-controlled trial. Toxins. 2017;9(11):361. doi:10.3390/toxins9110361
31. Kizhakkeveettil A, Rose K, Kadar G, et al. Integrative acupuncture and spinal manipulative therapy versus either alone for low back pain: a randomized controlled trial feasibility study. J Manipulative Physiol Ther. 2017;40(3):201–213. doi:10.1016/j.jmpt.2017.01.002
32. Liu L, Skinner M, Mcdonough S, et al. Acupuncture for chronic low back pain: a randomized controlled feasibility trial comparing treatment session numbers. Clin Rehabil. 2017;31(12):1592–1603. doi:10.1177/0269215517705690
33. Zhang XW, Ma LS, Han YY, et al. Needling point specificity for analgesic effect of wrist-ankle acupuncture on low-back pain: a randomized controlled trial. Shanghai J Trad Chin Med. 2017;51(04):77–82.
34. Wu H, Jin W, Zhou YM, et al. Low back pain of cold-dampness type treated with internal heating acupuncture needle: a randomized controlled trial. Pract Clin J Integr Trad Chin West Med. 2017;17(01):6–8.
35. Zheng Z, Gibson S, Helme R, et al. Effects of electroacupuncture on opioid consumption in patients with chronic musculoskeletal pain: a multicenter randomized controlled trial. Pain Med. 2019;20(2):397–410. doi:10.1093/pm/pny113
36. Lee H, Choi B, Jun S, et al. Efficacy and safety of thread embedding acupuncture for chronic low back pain: a randomized controlled pilot trial. Trials. 2018;19(1):680. doi:10.1186/s13063-018-3049-x
37. Heo I, Hwang M, Hwang E, et al. Electroacupuncture as a complement to usual care for patients with non-acute low back pain after back surgery: a pilot randomised controlled trial. BMJ Open. 2018;8(5):e018464. doi:10.1136/bmjopen-2017-018464
38. Yang L, Fei L, Wang JH. Comparative study on the efficacy of internal heat acupuncture and warm acupuncture on osphyalgia of the Hanshi type. Clin J Chin Med. 2018;10(25):36–38.
39. Luo Y, Yang M, Liu T, et al. Effect of hand-ear acupuncture on chronic low-back pain: a randomized controlled trial. J Trad Chin Med. 2019;39(4):587–598.
40. Vas J, Cintado M, Aranda-Regules J, et al. Effect of ear acupuncture on pregnancy-related pain in the lower back and posterior pelvic girdle: a multicenter randomized clinical trial. Acta Obstet Gynecol Scand. 2019;98(10):1307–1317. doi:10.1111/aogs.13635
41. Nicolian S, Butel T, Gambotti L, et al. Cost-effectiveness of acupuncture versus standard care for pelvic and low back pain in pregnancy: a randomized controlled trial. PLoS One. 2019;14(4):e0214195. doi:10.1371/journal.pone.0214195
42. Li JX, Xie JJ, Guo XQ, et al. Effect of “Tiaoshen Acupuncture” on postpartum low back pain: a randomized controlled trial. Chin Acupuncture Moxibustion. 2019;39(01):24–27.
43. Comachio J, Oliveira C, Silva I, et al. Effectiveness of manual and electrical acupuncture for chronic non-specific low back pain: a randomized controlled trial. J Acupunct Meridian Stud. 2020;13(3):87–93.
44. Bishop A, Ogollah R, Bartlam B, et al. Evaluating acupuncture and standard care for pregnant women with back pain: the EASE back pilot randomised controlled trial (ISRCTN49955124). Pilot Feasibil Stud. 2016;2(1):72. doi:10.1186/s40814-016-0107-6
45. Sung W, Hong Y, Jeon S, et al. Efficacy and safety of thread embedding acupuncture combined with acupuncture for chronic low back pain: a randomized, controlled, assessor-blinded, multicenter clinical trial. Medicine. 2020;99(49):e22526. doi:10.1097/MD.0000000000022526
46. Li ZM, Bao WL. Clinical effect of small six directions-needling on nonspecific low back pain. J Kunming Med Univ. 2020;41(01):137–140.
47. Wang LC, Dong BQ, Lin XX, et al. Randomized clinical control study on treatment of non-specific low back pain by acupuncture at tendon lesions and meridian points. J Pract Trad Chin Intern Med. 2020;34(03):13–15.
48. Yang QY, Liao YM, Tan XZ, et al. A multi-center, randomized controlled study on the treatment of nonspecific low back pain with floating acupuncture. China Med Pharm. 2020;10(20):15–19.
49. Higgins JPT, Thomas J, Chandler J, et al. Cochrane handbook for systematic reviews of interventions version 6.2; 2021. Available from: http://www.training.cochrane.org/handbook.
50. Berger V, Bears J. When can a clinical trial be called ‘randomized’? Vaccine. 2003;21(5–6):468–472. doi:10.1016/S0264-410X(02)00475-9
51. Streitberger K, Kleinhenz J. Introducing a placebo needle into acupuncture research. Lancet. 1998;352(9125):364–365. doi:10.1016/S0140-6736(97)10471-8
52. Mark L. Double-blind studies of acupuncture. JAMA. 1973;225(12):1532. doi:10.1001/jama.1973.03220400058020
53. Vase L, Baram S, Takakura N, et al. Can acupuncture treatment be double-blinded? An evaluation of double-blind acupuncture treatment of postoperative pain. PLoS One. 2015;10(3):e0119612. doi:10.1371/journal.pone.0119612
54. Sun GR, Zheng HX. Basic theory of traditional Chinese medicine. China Press Trad Chin Med. 2017.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.