")
Back to Journals » Patient Related Outcome Measures » Volume 13
Evaluating the Impact of Therapy on Quality of Life in Type 2 Diabetes: A Literature Review of Utilities Associated with Treatment-Related Attributes
Authors Valentine W, Norrbacka K, Boye KS
Received 28 May 2021
Accepted for publication 7 April 2022
Published 12 May 2022 Volume 2022:13 Pages 97—111
DOI https://doi.org/10.2147/PROM.S322390
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Lynne Nemeth
William Valentine,1 Kirsi Norrbacka,2 Kristina Secnik Boye3
1Ossian Health Economics and Communications, Basel, Switzerland; 2Eli Lilly Finland, Helsinki, Finland; 3Eli Lilly and Company, Indianapolis, IN, USA
Correspondence: William Valentine, Ossian Health Economics and Communications GmbH, Bäumleingasse 20, Basel, 4051, Switzerland, Tel +41 61 271 6214, Email [email protected]
Introduction: Treatment-related attributes and process characteristics such as dosing frequency, timing flexibility, ease of use of injection devices and unpleasant side-effects may have small but measurable effects on quality of life (QoL) in people with type 2 diabetes (T2D). A literature review was performed to identify recently published utility values quantifying the effect of treatment-related attributes on QoL.
Methods: Literature search strategies were designed using high-level medical subject heading (MeSH) terms supplemented with free-text terms and searches were run in March 2020 in the PubMed, Embase and Cochrane Library databases. For inclusion, studies were required to be published in full-text form, in English, since 2010 and report utility values (elicited using either direct or indirect methods) for treatment-related attributes or process characteristics including side effects, change in weight/body mass index (BMI), dosing frequency and timing flexibility, device attributes (e.g. needle handling, requirement for reconstitution) and convenience (e.g. waiting time).
Results: A total of 30 studies were included in the review, of which all but three were conducted in people with T2D. The EQ-5D was the most commonly used elicitation method (fourteen studies), followed by time tradeoff (TTO) methodology. Treatment-related adverse events and inconveniences such as needle handling in administration devices and waiting time were consistently associated with lower QoL, whereas lower dosing frequency and increased timing flexibility with dosing were consistently associated with utility benefits. The relationship between change in BMI and QoL was non-linear and influenced by baseline BMI.
Conclusion: Treatment-related attributes and process characteristics are associated with minor changes in QoL, which should be taken into account in long-term health economic modeling of new treatments and administration devices.
Keywords: quality of life, utilities, treatment-related attributes, side effects
Introduction
Type 2 diabetes (T2D) is a chronic progressive disease, typically requiring intensification of treatment to counter progressively worsening glycemic control. Whilst available pharmacologic treatments are effective in terms of reducing hyperglycemia, some commonly used drugs are associated with administration complexities or unpleasant side effects that may have a negative influence on quality of life (QoL). For example, insulin initiation or intensification is known to be associated with weight gain,1 sodium-glucose cotransporter-2 (SGLT-2) inhibitors have been linked with an increased risk for mycotic genital infections2 and glucagon-like peptide-1 (GLP-1) receptor agonists are associated with transient gastrointestinal side effects.3 The negative QoL effect of factors such as unpleasant side effects or complex dosing regimens may be sufficient to reduce adherence to treatment, which may ultimately reduce the effectiveness of treatment4 and increase the risk for long-term complications.
Recognition of the fact that interventions themselves can have a direct effect on QoL5 has led to efforts from manufacturers to focus on aspects such as convenience, dosing frequency and timing flexibility when developing new treatments and administration devices. The influence of these parameters on patient QoL can be determined using utility values, which can in turn be used to inform health economic models of novel treatments and devices. Although the utility benefits/decrements associated with treatment-related attributes may be relatively minor in comparison with major long-term complications such as myocardial infarction or stroke, as T2D is a chronic disease, patients may face these inconveniences on a daily basis. Therefore, the alleviation of minor inconveniences such as injection site reactions or the need to reconstitute a solution for injection may translate into tangible QoL benefits over the lifetime of the patient. Further, for treatments that have similar efficacy in terms of glycemic control and reduction of hypoglycemic events, the QoL impact of factors such as side-effects, weight gain/loss, convenience and dosing frequency and flexibility may be important determinants of the results of health economic analyses.
The aim of the current review was to identify health state utility values, elicited using either direct or indirect methods, associated with treatment-related attributes and process characteristics for pharmacologic treatments for T2D. Previous reviews have focused on the impact of diabetes-related complications on QoL but the current review is among the first to explore the influence of treatment-related attributes on QoL. These included weight loss/gain or change in body mass index (BMI), dosing frequency and timing flexibility, device-related attributes for injectable treatments (e.g. needle handling, dose selection requirements), injection site reactions, convenience (e.g. requirements for reconstitution, waiting time) and adverse events (e.g. gastrointestinal disturbances, mycotic genital infections and urinary tract infections [UTIs]).
Methods
The literature review was performed using the PubMed, Embase and Cochrane Library databases (Supplementary Tables 1–5). Search strategies were designed in alignment with recommendations outlined in the UK-based National Institute for Health and Care Excellence (NICE) Decision Support Unit (DSU) Technical Support Document 9.6 Search strategies utilized high level Medical Subject Heading (MeSH) terms supplemented with free-text terms and search syntax was adjusted as required for use across the different databases (full details of the search strategies used are provided in the Supplementary Tables 1–5). Supplementary hand searches were also performed to identify pertinent studies presented at major congresses in late 2019 and 2020 (specifically the 55th annual meeting of the European Association for the Study of Diabetes [EASD], the virtual meeting of the American Diabetes Association [ADA] and the 2020 virtual ISPOR annual US meeting). Relevant abstracts presented at 2019 ISPOR meetings have been published and therefore relevant publications were captured within the literature database searches. Studies published only in abstract form prior to 2019 were excluded on the basis that study results were likely have been subsequently published in full-text form.
The time horizon of the searches was limited to articles published since 2010 and all searches were performed in March 2020. For inclusion in the review studies were required to be published in full-text form (except for recent abstracts as outlined above) in English, and present utility or disutility values for health states related to acute or long-term T2D related complications or treatment-related attributes or process characteristics. Treatment-related attributes and process characteristics captured in the review included treatment modality (injection or oral treatment), weight or BMI loss or gain, dosing frequency, dosing timing flexibility, injection and injection device related properties including injection site reaction, needle handling, requirement for reconstitution, waiting time, and unpleasant side effects (e.g. gastrointestinal disturbances, mycotic genital infections and UTIs). Utility benefits or decrements associated with treatment-related attributes or process characteristics can be elicited using direct methods such as standard gamble (SG) or time trade off (TTO) or indirect methods such as the EQ-5D or SF-6D, each of which are associated with relative merits and limitations. Both direct and indirect methods were included in the review.
Although treatments such as sulfonylureas are known to be associated with an increased risk of hypoglycemic events, for the purpose of this review hypoglycemia was considered an acute complication. Studies that were conducted in mixed populations of patients with type 1 and type 2 diabetes were excluded if results were not presented according to type of diabetes as the focus of the review was T2D alone. Secondary studies (i.e. studies listing previously published utility values) and discrete choice experiments were also excluded. Reporting of results here is limited to treatment-related attributes and process characteristics.
Results
Literature Searches
Literature searches across the three databases yielded a total of 8566 hits, of which 1383 were duplicates, therefore resulting in a total of 7183 unique hits. First-round screening of titles and abstracts was performed by one investigator and identified a total of 241 hits for full-text review (Figure 1). During second-round screening a further 176 articles were excluded, resulting in a total of 65 articles for inclusion that detailed utility or disutility values associated with either T2D-related complications or treatment-related attributes or process characteristics. A further three articles were identified via bibliographies of included articles. Searches of ADA 2020 meeting abstracts identified one relevant abstract for inclusion; no relevant abstracts were identified from searches of the ISPOR US 2020 virtual meeting abstracts or EASD 2019 meeting abstracts. The final review therefore included a total of 69 studies. Of these, a total of 39 presented findings exclusively related to acute or long-term diabetes-related complications, 15 presented findings exclusively related to the influence of treatment-related attributes on QoL and 15 captured findings on both complications and treatment attributes. Therefore, a total of 30 articles presented utility/disutility values associated with treatment-related attributes or process characteristics (Table 1)7–36 These included a total of fifteen conducted in Europe,9–11,13–15,19–21,24,25,29,31,33,34 eight conducted in Asia,12,17,18,23,27,28,32,35 two in North America,16,36 one in Latin America,30 one in the Middle East,8 one in Africa,7 and two were multinational or the setting was not stated.22,26 Most studies were conducted in people with T2D although three were conducted in general population samples24,28,33 and one included both general population groups and groups with T2D.29 The most frequently used elicitation method was the EQ-5D (3L or 5L), which was used in fourteen studies,8,12–15,18,22,23,25,27,30,32,34,36 followed by TTO methodology used in ten studies,10,11,16,19–21,24,26,29,33 then the Short Form 6 Dimensions questionnaire (SF-6D; three studies),15,31,35 SG (three studies),9,17,28 Health Utilities Index-2 (HUI-2; one study),7 visual analog scale (one study),17 Health Utilities Index-3 (HUI-3; one study)7 and the 15D questionnaire (one study).15
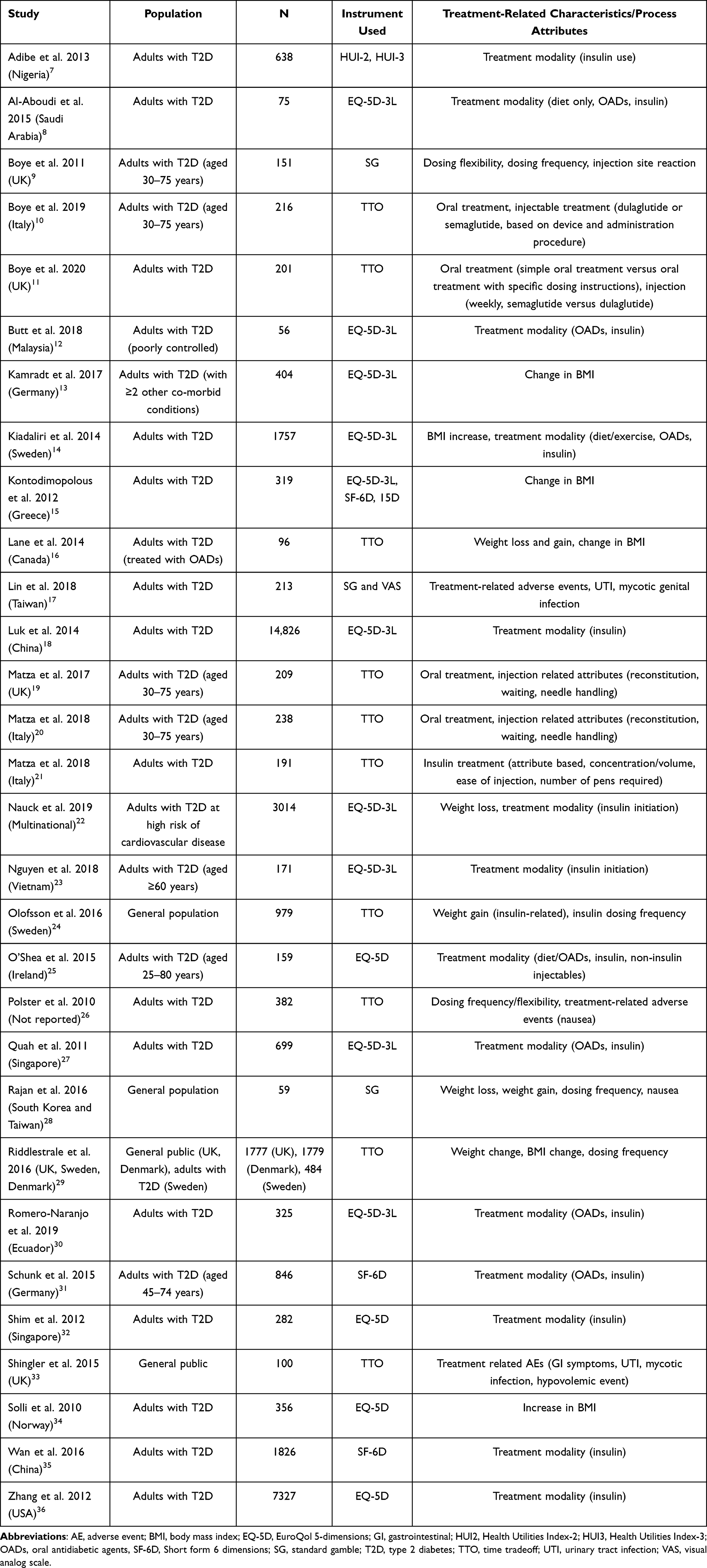 |
Table 1 Summary of Included Studies |
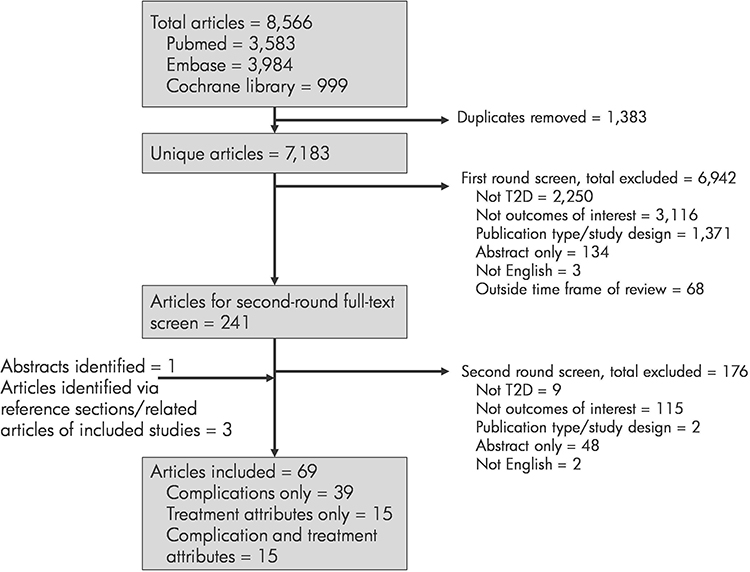 |
Figure 1 Summary of literature review process. Abbreviation: T2D, type 2 diabetes. |
Administration Route
A total of twenty studies presented utility or disutility values according to treatment type (diet/exercise alone, oral treatment, insulin or other injectables),7,8,10–14,18–20,22–25,27,30–32,35,36 however, only eight were comparative studies in terms of presenting data for patients on different treatment modalities.8,11,12,14,25,27,30,31 In particular, one recent UK-based study specifically assessed QoL according to administration route and also the effect of specific dosing instructions for orally administered treatments.11 Here, Boye et al. showed that patients value simplicity in terms of treatment. The mean (SD) utility value (determined using TTO methodology) associated with simple oral treatment was 0.890 (0.140). However, if oral treatment was associated with specific dosing instructions including the requirement for taking treatment on an empty stomach and fasting for 30 minutes afterwards, the mean (SD) utility value was significantly lower at 0.880 (0.146) (p <0.001).
A further two studies conducted in Ireland25 and Saudi Arabia8 reported utility values, elicited using the EQ-5D, for individuals treated with OADs alone, insulin alone or with OADs and the study conducted in Ireland also included a separate category for those treated with OADs plus non-insulin injectables. In both studies, as anticipated, individuals treated with diet/lifestyle intervention alone had the highest mean or median utility values, followed by those treated with OADs alone, insulin alone and then insulin in combination with OADs. The use of insulin alone or in combination with OADs is indicative of more severe disease, which is likely a key factor in the lower utility values reported in these groups. A total of nine studies reported a value for a utility decrement or benefit associated with insulin use.7,13,14,18,22,23,31,35,36 However, the findings of these studies were inconsistent, with some reporting a utility benefit associated with insulin use and others reporting a decrement.
Change in Weight or BMI
Treatment for T2D may result in either weight gain or loss, for example, initiation of insulin is commonly associated with weight gain and GLP-1 receptor agonists are typically associated with weight loss.
A total of nine studies were identified that reported disutility values associated with either a change in BMI or a change in bodyweight,13–16,22,24,28,29,34 of which six investigated the effect of a 1-unit change in BMI13–16,29,34 and five investigated the effects of an absolute or percentage change in bodyweight.16,22,24,28,29 A 1-unit increase in BMI was consistently associated with a QoL decrement, ranging from −0.002 to −0.0472 in cross-sectional studies of people with T2D based in Norway and Canada, respectively (Table 2).16,34 Notably, in their Canadian analysis (which used TTO methodology) Lane et al. noted that the relationship between change in BMI and QoL was non-linear and also strongly influenced by baseline BMI. Specifically, a 1-unit increase in BMI was associated with an overall mean disutility of −0.0472, but a 1-unit decrease in BMI was associated with a utility benefit of +0.0171.16 A 1-unit decrease in BMI also had a greater impact on QoL in those with higher baseline BMI, for people with T2D with a baseline BMI of 18–<25 kg/m2 a 1-unit decrease in BMI was associated with a utility benefit of +0.0077, whereas for those with a baseline BMI ≥30 kg/m2 the equivalent utility benefit was substantially greater at + 0.0212.16 This non-linearity was also seen in a study conducted in a general population sample in South Korea and Taiwan.28 Rajan et al. used SG methodology and reported that overall a 5% weight gain was associated with a mean disutility of −0.001, but a 5% weight loss was associated with a mean utility benefit of +0.029.28
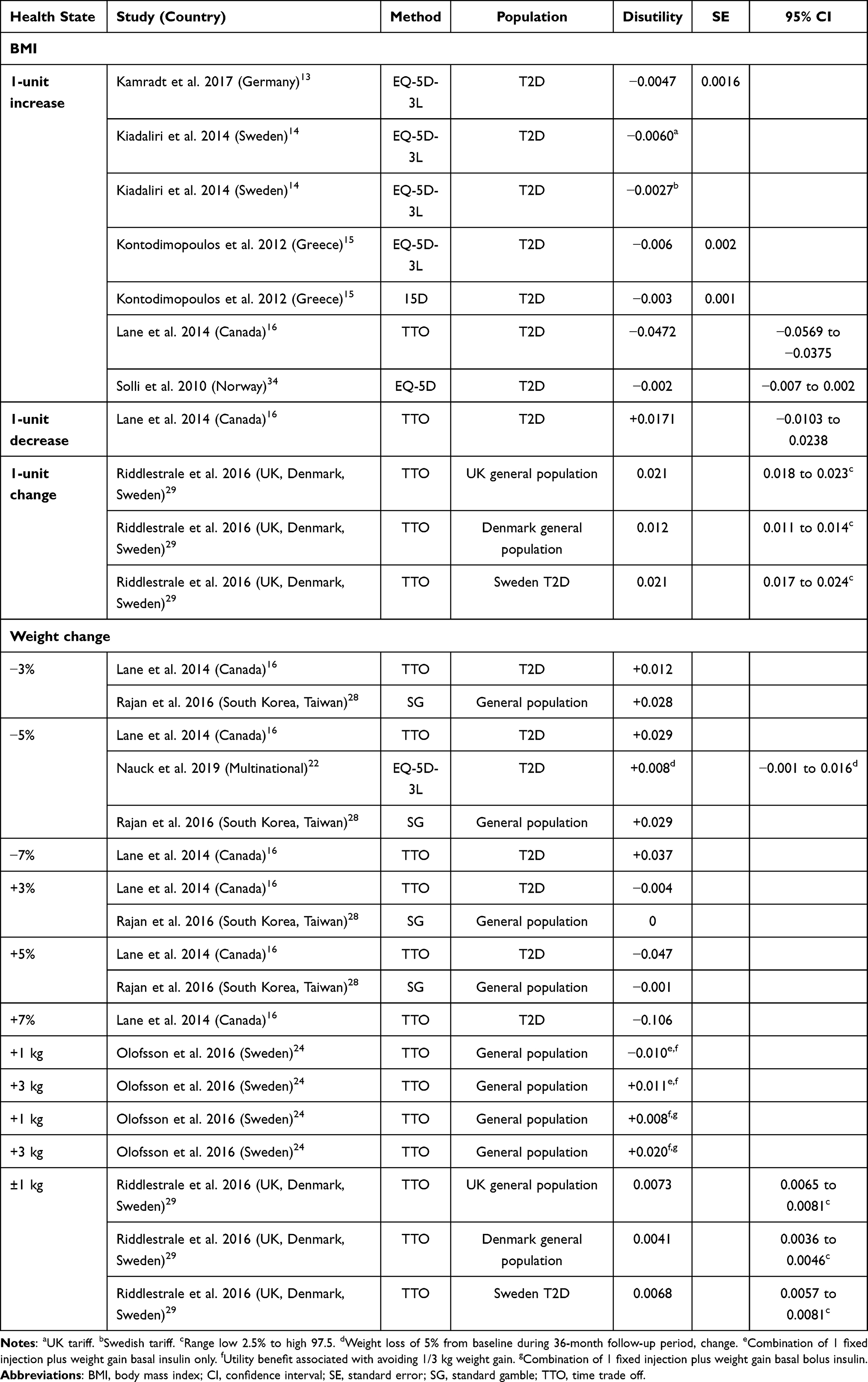 |
Table 2 Influence of Change in Body Weight and Change in BMI in T2D on Utility Scores |
Treatment-Related Adverse Events
The literature review process identified a total of four studies that presented either utility or disutility values for people experiencing treatment-related adverse events including UTIs, mycotic genital infections and nausea,17,26,28,33 two of which were conducted in people with T2D17,26 and two of which were conducted in general population samples.28,33 Three studies examined the effect of gastrointestinal effects/nausea on QoL.26,28,33 In the first of these, Shingler et al.33 used TTO methodology to assess the impact of treatment-related nausea, vomiting or diarrhea in a UK-based general population sample. The mean (SD) utility value for nausea was 0.68 (0.02) (compared with a mean value of 0.92 for a reference state of stable well-controlled diabetes). In another study also conducted in a general population sample (based in South Korea and Taiwan) that used SG methodology the authors reported a disutility of −0.034 for nausea.28 In the remaining study, conducted in people with T2D and using TTO methodology, Polster et al.26 reported that avoiding treatment-related nausea for 1 month was associated with a utility benefit of + 0.011. UTIs and mycotic genital infections were also shown to compromise QoL.17,33 In particular, in their UK-based analysis Shingler et al.33 reported that the mean (SD) utility value for patients with a mild or moderate UTI was 0.83 (0.01) but for patients with a severe UTI the corresponding value was considerably lower at 0.73 (0.02).
Dosing Frequency and Flexibility
Five studies were identified that examined the influence of dosing frequency and timing flexibility on QoL in people with T2D,9,24,26,28,29 of which, three utilized TTO methodology24,26,29 and two utilized SG9,28 (Table 3). Reducing the frequency of injections, either from daily to once weekly or from twice daily to once daily was consistently shown to confer a small utility benefit. In one UK-based study reducing the frequency of injections once daily to once per week conferred a mean utility benefit of +0.023, whilst timing flexibility with dosing conferred a mean utility benefit of +0.006.9
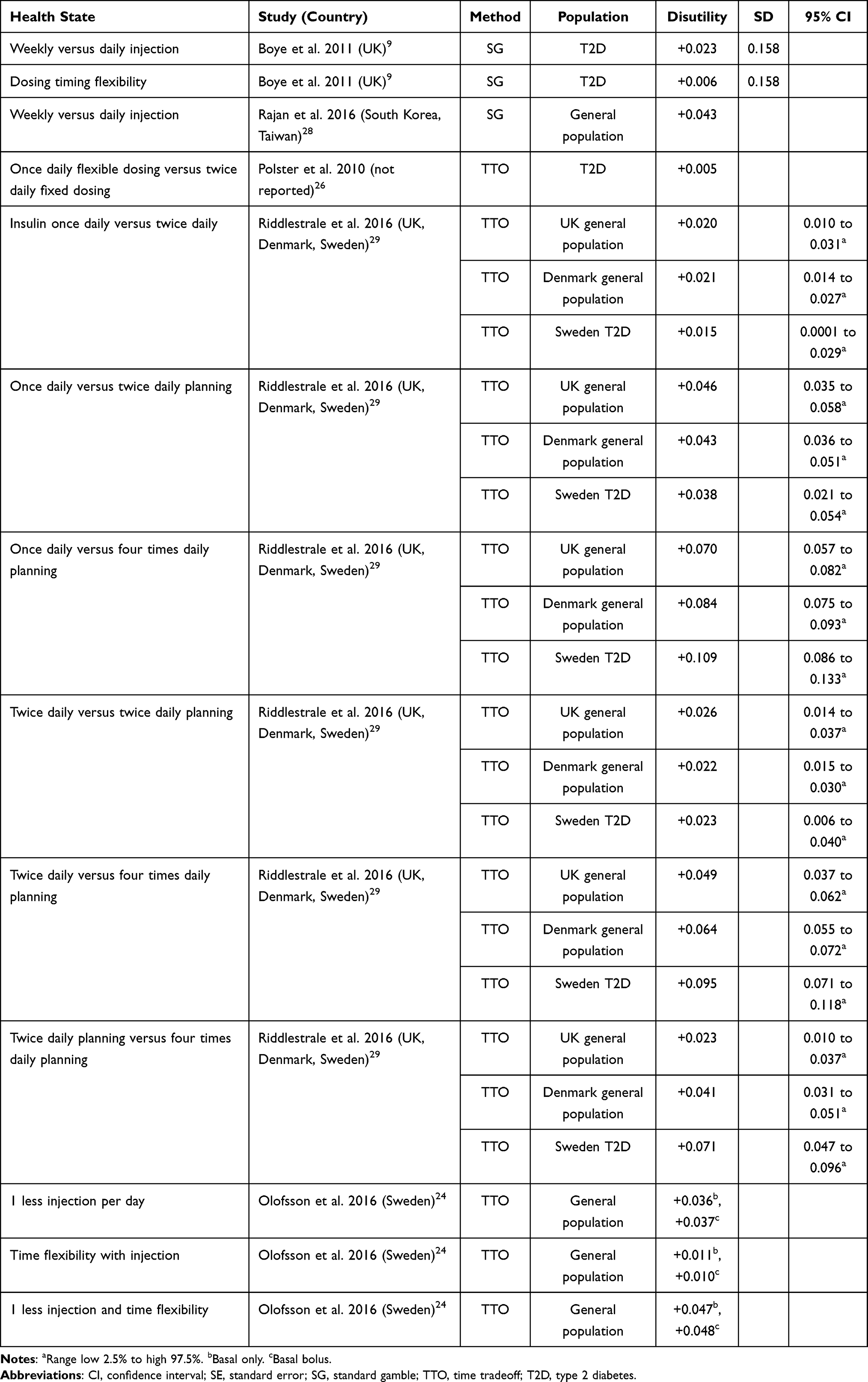 |
Table 3 Influence of Dosing Frequency and Flexibility on Utility Scores |
Similarly, a multinational study conducted in a UK and Denmark-based general population sample as well as a group of people with T2D in Sweden, Ridderstrale et al.29 investigated the effect of various different dosing frequency and timing flexibility scenarios. Reducing dosing frequency from twice daily to once daily was associated with a utility benefit of +0.020 and +0.021 in the general population samples in the UK and Denmark, respectively and +0.015 for people with T2D in Sweden. Further, reducing dosing frequency from four times daily (planned doses) to once daily was associated with a utility benefit of +0.070, +0.084 and +0.109, respectively across the three groups studied.29 Dosing flexibility in terms of timing has also been shown to confer a small utility benefit independent of dosing frequency. In a general population sample based in Sweden, having time flexibility around dosing was associated with a utility benefit of +0.011. Additionally, when combined the utility benefit associated with one less injection per day and having flexibility around timing was +0.047.24
Injection Device and Process Characteristics
A total of six studies examined utility benefits/decrements associated with device or process characteristics either alone or in combination with other treatment-related attributes such as dosing frequency, timing flexibility and the presence of injection site reaction9–11,19–21 (Table 4). Device attributes and process characteristics investigated included the requirement for needle handling, reconstitution of the injected solution, waiting time, and dose selection requirements. All six studies were conducted in Europe, and five used TTO methodology whilst the remaining study used SG. In the SG study Boye et al.9 investigated utility benefits/decrements associated with different combinations of factors including the presence/absence of injection site reaction, injection frequency and dosing timing flexibility, in people with T2D based in the UK. Reduced dosing frequency, timing flexibility and no injection site reaction were all shown to be associated with minor utility benefits. In particular, a once weekly injection with dosing timing flexibility and no injection site reaction was associated with a mean (SD) utility benefit of +0.024 (0.156).9 Two further studies conducted in people with T2D in the UK and Italy (both with identical methodology) used TTO methods to determine the QoL impact of process characteristics of a weekly injection including requirement for reconstitution, needle handling and waiting.19,20 In the UK-based study, a weekly injection with no inconvenience was associated with a disutility of −0.010 relative to oral treatment alone. In contrast, a weekly injection that required reconstitution, needle handling and waiting time was associated with a disutility of −0.030 relative to oral treatment alone and −0.020 relative to a weekly injection with no inconvenience.19 Similar findings were reported in the Italian study where the disutility for a weekly injection with no inconvenience relative to oral treatment alone was −0.009 and the disutility for a weekly injection with reconstitution, needle handling and waiting was −0.032 relative to oral treatment alone and −0.022 relative to a weekly injection with no inconveniences.20 Another further study by the same authors compared process characteristics associated with a concentrated formulation of insulin versus standard insulin with attributes of the concentrated formulation including less injection volume, less effort to press the injection button and fewer pens required. Matza et al. used TTO methodology to determine mean utility (SD) values of 0.889 (0.103) with the concentrated insulin formulation versus 0.882 (0.104) with the standard insulin formulation.21
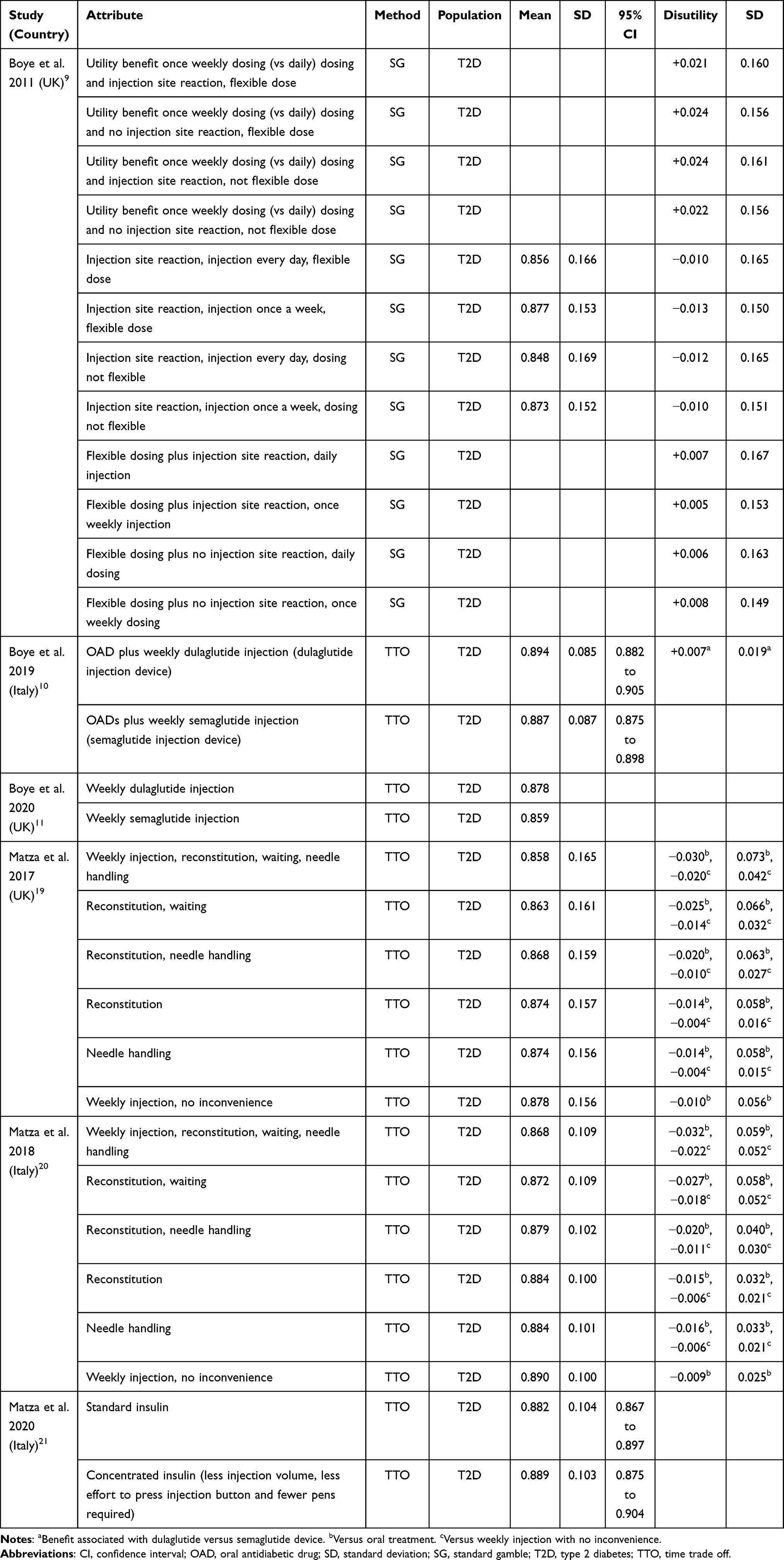 |
Table 4 Influence of Device-Related Attributes and Process Characteristics on Utility Scores |
Two further studies examined the influence of different injection devices on utility values. Specifically, two studies by Boye et al. conducted in the UK and Italy compared utility values with once weekly administration of dulaglutide and semaglutide based on device-related properties including needle handling and dose selection requirement.10,11 In both studies the dulaglutide administration device was associated with a small utility benefit compared with the semaglutide device and in people with T2D based in Italy the dulaglutide device was associated with a utility benefit of +0.007 relative to the semaglutide device.10
Discussion
One of the fundamental goals of treatment for people with T2D is to maintain good glycemic control, thereby reducing the risk for long-term diabetes-related complications, such as cardiovascular disease, that are associated with morbidity, increased mortality risk and substantial impairments in QoL. Whilst from the perspective of the treating physician efficacy and safety are the most important characteristics of individual treatments, the findings presented here suggest that from the patient perspective features such as tolerability, dosing frequency and timing flexibility, convenience and ease of administration may also have a small but important effect on QoL. Inconveniences such as needle handling and reconstitution of solutions may be minor and as such often overlooked in clinical trials. However, T2D is a chronic condition and the cumulative burden of dealing with these small inconveniences on a daily basis may be sufficient to have a measurable impact on QoL. The impact of treatment on everyday life was investigated in the multinational DAWN2 study in people with type 1 or type 2 diabetes. Here, 40% of participants noted that their diabetes medications interfered with their ability to lead a normal life.37 In response to this burden there is increasing recognition that assessment of patient QoL should form an integral part of routine care, with the recent ADA guidelines noting that treatment decisions should be a collaborative process between patients and physicians and that patient preferences should be taken into account.38 Moreover, there is also emerging evidence that the negative QoL effects of treatment-related gastrointestinal side effects or weight gain may have a detrimental effect on adherence to treatment, which in turn has been shown to influence effectiveness in terms of achieving glycemic control targets.39 Dosing frequency and device-related attributes are also increasingly gaining recognition as influencing QoL, and in turn, adherence and effectiveness. For example, in a real-world study from 2017 Alatorre et al.40 reported higher levels of adherence for dulaglutide once weekly compared with exenatide once weekly or liraglutide once daily. Alatorre et al. postulated that the simplicity of the dulaglutide administration device (a ready-to-use single-dose pen with no needle handling or reconstitution) may have been a contributing factor to the higher level of adherence reported with dulaglutide, particularly when compared with exenatide once weekly, which requires reconstitution and needle handling.
Treatment-related changes in BMI or bodyweight that can occur with initiation of insulin or GLP-1 receptor agonists were also shown to be important determinants of QoL. However, the relationship between change in bodyweight/BMI and QoL was shown to be non-linear, highly variable in terms of magnitude and influenced by baseline BMI. In terms of magnitude the reported disutility associated with a 1-unit increase in BMI was from −0.0027 in a study in people with T2D in Sweden,14 which used the EQ-5D, to a maximum of −0.0472 in a Canadian study using TTO methodology in OAD-treated adults with T2D.16 The Canadian study by Lane et al. also noted a non-linear relationship between QoL and change in BMI with the magnitude of the decrement associated with a 1-unit gain in BMI being approximately two-fold greater than the magnitude of the utility benefit associated with a 1-unit decrease in BMI.16 This non-linearity was also observed in a general population SG study conducted in South Korea and Taiwan but here the direction of effect was the opposite of that reported by Lane et al. In South Korea and Taiwan Rajan et al. noted that the detriment associated with a 5% gain in body weight was −0.001, whereas the utility benefit associated with 5% loss in body weight was +0.029.28 Further, in the Canadian analysis the QoL impact of a change in BMI was also strongly influenced by baseline BMI. The negative impact of BMI gain was greatest in those with the lowest baseline BMI (18–25 kg/m2) but the benefit of a 1-unit loss in BMI was greatest in those in the highest baseline BMI category (≥30 kg/m2).16 These findings concur with those of an earlier study by Matza et al.41 Here, the authors reported that a 3% decrease in bodyweight was associated with a utility benefit of +0.029 for those with a baseline BMI ≥30 kg/m2 but the corresponding figure for people with BMI <30 kg/m2 was substantially lower at +0.012. These earlier findings align with those of Lane et al.16 in terms of suggesting that baseline BMI is an important determinant of the value that patients attach to weight loss (or gain). Consequently, the influence of baseline BMI may also warrant consideration in future economic modeling analyses, particularly as novel treatments in the GLP-1 receptor analog class are often associated with weight loss.
It is possible that some of the variation in terms of the QoL impact of change in BMI/bodyweight may be due to differences in study populations as well as differences in utility elicitation methods used. In studies that focused on long-term complications, indirect methods, and in particular the EQ-5D, were the most commonly used utility elicitation methods. This may have been driven in part by their simplicity, meaning that they can relatively easily be incorporated into clinical studies and also the fact that several Health Technology Assessment (HTA) agencies have stated that EQ-5D-derived utilities are preferred in economic analyses submitted in applications for reimbursement.42,43 However, for studies that focused on the QoL impact of treatment-related side-effects, attributes and process characteristics, direct methods, including TTO and SG were also commonly used. Whilst these direct methods are more resource intensive and associated with a higher cognitive burden for respondents, they allow for a highly specific and nuanced description of health states and may therefore be more amenable to evaluating the impact of states that are concerned with very specific attributes and inconveniences associated with particular treatments or administration devices.44 Adaptations of SG and TTO methodology can also be used to more effectively assess the impact of temporary and/or mildly impaired states. Indeed, two studies included in the current review used chained SG methods for this purpose9,28 (in chaining, values are anchored to death via an intermediary health state, which allows for greater sensitivity when evaluating the effect of health states associated with minimal impairment42). The current review shows that SG and TTO methods have been widely used in studies of treatment-related attributes, possibly due in part to their sensitivity in terms of assessing the effect of treatment-related impairments and inconveniences. The use of these values in economic models alongside EQ-5D (or SF-6D or HUI2/3) derived utilities may be a concern to some in terms of utilizing values from several different sources and methods. However, the descriptive systems used in some generic preference-based questionnaires may lack the sensitivity to detect subtle treatment- or condition-specific changes in QoL. For example, the sensitivity of the EQ-5D has been shown to be low relative to other instruments in some specific conditions such as glaucoma or alcohol dependence.45,46 Therefore, accounting for treatment-related attributes in long-term health economic models may necessitate the use of a set of utilities drawn from studies using two or more different elicitation methods.
The current review is one of the first to consolidate information relating to the utility benefits and decrements associated with attributes specific to treatments for T2D; previous reviews have largely focused on acute and long-term complications. However, a key limitation of the current analysis is that it was limited to articles published since 2010. The rationale for this was to limit the scope of the review to studies that reflect current clinical practice. Overall, studies published in the previous 10 years suggest that advances in treatment such as reducing dosing frequency and increasing timing flexibility, better tolerability, and efforts to make administration of injectable treatments easier and more convenient are associated with minor benefits in terms of QoL. Collectively, such parameters may influence other factors such as willingness to adhere to prescribed treatment regimens and subsequently treatment effectiveness. This review summarizes evidence that treatment-related attributes and process characteristics are associated with minor changes in QoL. These effects should be considered in long-term cost-utility analyses of new treatments and administration devices, particularly when comparing treatments with similar efficacy profiles.
Disclosure
WV is a current employee of Ossian Health Economics and Communications, which has received consulting fees from Eli Lilly. KSB is a current employee and shareholder of Eli Lilly. At the time of the review KN was an employee of Eli Lilly, she has since left the organization. The authors report no other conflicts of interest in this work.
References
1. Russell-Jones D, Khan R. Insulin-associated weight gain in diabetes–causes, effects and coping strategies. Diabetes Obes Metab. 2007;9(6):799–812. doi:10.1111/j.1463-1326.2006.00686.x
2. Lega IC, Bronskill SE, Campitelli MA, et al. Sodium glucose cotransporter 2 inhibitors and risk of genital mycotic and urinary tract infection: a population-based study of older women and men with diabetes. Diabetes Obes Metab. 2019;21(11):2394–2404. doi:10.1111/dom.13820
3. Madsbad S. Review of head-to-head comparisons of glucagon-like peptide-1 receptor agonists. Diabetes Obes Metab. 2016;18(4):317–332. doi:10.1111/dom.12596
4. García-Pérez LE, Alvarez M, Dilla T, Gil-Guillén V, Orozco-Beltrán D. Adherence to therapies in patients with type 2 diabetes. Diabetes Ther. 2013;4(2):175–194. doi:10.1007/s13300-013-0034-y
5. Polonsky WH, Henry RR. Poor medication adherence in type 2 diabetes: recognizing the scope of the problem and its key contributors. Patient Prefer Adherence. 2016;10:1299–1307. doi:10.2147/PPA.S106821
6. Papaioannou D, Brazier J, Paisley S. NICE DSU technical support document 9: the identification, review and synthesis of health state utility values from the literature; October, 2010. Available from: www.nicedsu.org.uk.
7. Adibe MO, Aguwa CN. Sensitivity and responsiveness of health utility indices (HUI2 and HUI3) among type 2 diabetes patients. Trop J Pharm Res. 2013;12(5):835–842.
8. Al-Aboudi IS, Hassali MA, Shafie AA, Hassan A, Alrasheedy AA. A cross-sectional assessment of health-related quality of life among type 2 diabetes patients in Riyadh, Saudi Arabia. SAGE Open Med. 2015;3:2050312115610129. doi:10.1177/2050312115610129
9. Boye KS, Matza LS, Walter KN, Van Brunt K, Palsgrove AC, Tynan A. Utilities and disutilities for attributes of injectable treatments for type 2 diabetes. Eur J Health Econ. 2011;12(3):219–230. doi:10.1007/s10198-010-0224-8
10. Boye KS, Matza LS, Stewart KD, et al. Patient preferences and health state utilities associated with dulaglutide and semaglutide injection devices among patients with type 2 diabetes in Italy. J Med Econ. 2019;22(8):806–813. doi:10.1080/13696998.2019.1609482
11. Boye K, Cutts K, Stewart K, Norrbacka K, Garcia-Perez LE, Matza LS. Preferences and health state utilities associated with routes of administration for oral semaglutide, injectable semaglutide, and dulaglutide. Diabetes. 2020;69:Suppl 1:93–LB.
12. Butt M, Ali AM, Bakry MM. Health-related quality of life in poorly controlled type 2 diabetes patients- association of patients’ characteristics with EQ-5D domains, mean EQ-5D scores, and visual analog scale score. Asian J Pharm Clin Res. 2018;11(1):93–98. doi:10.22159/ajpcr.2018.v11i1.19120
13. Kamradt M, Krisam J, Kiel M, et al. Health-related quality of life in primary care: which aspects matter in multimorbid patients with type 2 diabetes mellitus in a community setting? PLoS One. 2017;12(1):e0170883. doi:10.1371/journal.pone.0170883
14. Kiadaliri AA, Gerdtham UG, Eliasson B, Gudbjörnsdottir S, Svensson AM, Carlsson KS. Health utilities of type 2 diabetes-related complications: a cross-sectional study in Sweden. Int J Environ Res Public Health. 2014;11(5):4939–4952. doi:10.3390/ijerph110504939
15. Kontodimopoulos N, Pappa E, Chadjiapostolou Z, Arvanitaki E, Papadopoulos AA, Niakas D. Comparing the sensitivity of EQ-5D, SF-6D and 15D utilities to the specific effect of diabetic complications. Eur J Health Econ. 2012;13(1):111–112. doi:10.1007/s10198-010-0290-y
16. Lane S, Levy AR, Mukherjee J, Sambrook J, Tildesley H. The impact on utilities of differences in body weight among Canadian patients with type 2 diabetes. Curr Med Res Opin. 2014;30(7):1267–1273. doi:10.1185/03007995.2014.899207
17. Lin YJ, Wang CY, Cheng SW, Ko Y. Patient preferences for diabetes-related complications in Taiwan. Curr Med Res Opin. 2019;35(1):7–13. doi:10.1080/03007995.2018.1470970
18. Luk AOY, Zhang Y, Ko GTC, et al. Health-related quality of life in Chinese patients with type 2 diabetes: an analysis of the Joint Asia Diabetes Evaluation (JADE) program. J Diabetes Metab. 2014;5:333.
19. Matza LS, Boye KS, Stewart KD, Davies EW, Paczkowski R. Health state utilities associated with attributes of weekly injection devices for treatment of type 2 diabetes. BMC Health Serv Res. 2017;17(1):774. doi:10.1186/s12913-017-2648-7
20. Matza LS, Boye KS, Jordan JB, et al. Patient preferences in Italy: health state utilities associated with attributes of weekly injection devices for treatment of type 2 diabetes. Patient Prefer Adherence. 2018;12:971–979. doi:10.2147/PPA.S159620
21. Matza LS, Osumili B, Stewart KD, et al. Patient preferences and health state utilities associated with mealtime insulin concentrations among patients with diabetes in Italy. Diabetes Ther. 2020;11(1):319–333. doi:10.1007/s13300-019-00718-8
22. Nauck MA, Buse JB, Mann JFE, et al.; LEADER Publication Committee for the LEADER Trial Investigators. Health-related quality of life in people with type 2 diabetes participating in the LEADER trial. Diabetes Obes Metab. 2019;21(3):525–532. doi:10.1111/dom.13547
23. Nguyen HTT, Moir MP, Nguyen TX, et al. Health-related quality of life in elderly diabetic outpatients in Vietnam. Patient Prefer Adherence. 2018;12:1347–1354. doi:10.2147/PPA.S162892
24. Olofsson S, Norrlid H, Persson U. Preferences for improvements in attributes associated with basal insulin: a time trade-off and willingness-to-pay survey of a diabetic and non-diabetic population in Sweden. J Med Econ. 2016;19(10):945–958. doi:10.1080/13696998.2016.1187152
25. O’Shea MP, Teeling M, Bennett K. Comorbidity, health-related quality of life and self-care in type 2 diabetes: a cross-sectional study in an outpatient population. Ir J Med Sci. 2015;184(3):623–630. doi:10.1007/s11845-014-1190-4
26. Polster M, Zanutto E, McDonald S, Conner C, Hammer M. A comparison of preferences for two GLP-1 products–liraglutide and exenatide–for the treatment of type 2 diabetes. J Med Econ. 2010;13(4):655–661. doi:10.3111/13696998.2010.529377
27. Quah JH, Luo N, Ng WY, How CH, Tay EG. Health-related quality of life is associated with diabetic complications, but not with short-term diabetic control in primary care. Ann Acad Med Singapore. 2011;40(6):276–286.
28. Rajan N, Boye KS, Gibbs M, et al. Utilities for type 2 diabetes treatment-related attributes in a South Korean and Taiwanese Population. Value Health Reg Issues. 2016;9:67–71. doi:10.1016/j.vhri.2015.11.006
29. Ridderstråle M, Evans LM, Jensen HH, et al. Estimating the impact of changes in HbA1c, body weight and insulin injection regimen on health related quality-of-life: a time trade off study. Health Qual Life Outcomes. 2016;14:13. doi:10.1186/s12955-016-0411-0
30. Romero-Naranjo F, Espinosa-Uquillas C, Gordillo-Altamirano F, Barrera-Guarderas F. Which factors may reduce the health-related quality of life of Ecuadorian patients with diabetes? P R Health Sci J. 2019;38(2):102–108.
31. Schunk M, Reitmeir P, Schipf S, et al. Health-related quality of life in women and men with type 2 diabetes: a comparison across treatment groups. J Diabetes Complications. 2015;29(2):203–211. doi:10.1016/j.jdiacomp.2014.11.010
32. Shim YT, Lee J, Toh MP, Tang WE, Ko Y. Health-related quality of life and glycaemic control in patients with type 2 diabetes mellitus in Singapore. Diabet Med. 2012;29(8):e241–8. doi:10.1111/j.1464-5491.2012.03689.x
33. Shingler S, Fordham B, Evans M, et al. Utilities for treatment-related adverse events in type 2 diabetes. J Med Econ. 2015;18(1):45–55. doi:10.3111/13696998.2014.971158
34. Solli O, Stavem K, Kristiansen IS. Health-related quality of life in diabetes: the associations of complications with EQ-5D scores. Health Qual Life Outcomes. 2010;8:18. doi:10.1186/1477-7525-8-18
35. Wan EY, Fung CS, Choi EP, et al. Main predictors in health-related quality of life in Chinese patients with type 2 diabetes mellitus. Qual Life Res. 2016;25(11):2957–2965. doi:10.1007/s11136-016-1324-4
36. Zhang P, Brown MB, Bilik D, Ackermann RT, Li R, Herman WH. Health utility scores for people with type 2 diabetes in U.S. managed care health plans: results from Translating Research Into Action for Diabetes (TRIAD). Diabetes Care. 2012;35(11):2250–2256. doi:10.2337/dc11-2478
37. Nicolucci A, Kovacs Burns K, Holt RI, et al.; DAWN2 Study Group. Diabetes attitudes, wishes and needs second study (DAWN2™): cross-national benchmarking of diabetes-related psychosocial outcomes for people with diabetes. Diabet Med. 2013;30(7):767–777. doi:10.1111/dme.12245
38. American Diabetes Association. Standards of medical care in diabetes – 2020. Diabetes Care. 2020;43(Suppl 1):S14–S31.
39. Buysman EK, Liu F, Hammer M, Langer J. Impact of medication adherence and persistence on clinical and economic outcomes in patients with type 2 diabetes treated with liraglutide: a retrospective cohort study. Adv Ther. 2015;32(4):341–355. doi:10.1007/s12325-015-0199-z
40. Alatorre C, Fernández Landó L, Yu M, et al. Treatment patterns in patients with type 2 diabetes mellitus treated with glucagon-like peptide-1 receptor agonists: higher adherence and persistence with dulaglutide compared with once-weekly exenatide and liraglutide. Diabetes Obes Metab. 2017;19(7):953–961. doi:10.1111/dom.12902
41. Matza LS, Yurgin N, Boye KS, Malley K, Shorr JM. Obese versus non-obese patients with type 2 diabetes: patient-reported outcomes and utility of weight change. Curr Med Res Opin. 2007;23(9):2051–2062. doi:10.1185/030079907X219454
42. National Institute for Health and Care Excellence. Guide to the methods of technology appraisal 2013. Available from: https://www.nice.org.uk/process/pmg9/resources/guide-to-the-methods-of-technology-appraisal-2013-pdf-2007975843781.
43. Kennedy-Martin M, Slaap B, Herdman M, et al. Which multi-attribute utility instruments are recommended for use in cost-utility analysis? A review of National Health Technology Assessment (HTA) guidelines. Eur J Health Outcomes. 2020;21:1245.
44. Wright DR, Wittenberg E, Swan JS, Miksad RA, Prosser LA. Methods for measuring temporary health States for cost-utility analyses. Pharmacoeconomics. 2009;27(9):713–723.
45. Günther OH, Roick C, Angermeyer MC, König HH. Responsiveness of EQ-5D utility indices in alcohol-dependent patients. Drug Alcohol Depend. 2008;92(1–3):291–295. doi:10.1016/j.drugalcdep.2007.07.016
46. Bozzani FM, Alavi Y, Jofre-Bonet M, Kuper H. A comparison of the sensitivity of EQ-5D, SF-6D and TTO utility values to changes in vision and perceived visual function in patients with primary open-angle glaucoma. BMC Ophthalmol. 2012;12:43. doi:10.1186/1471-2415-12-43
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.