Back to Journals » The Application of Clinical Genetics » Volume 15
Evaluating the Association Between Genetic Polymorphisms Related to Homocysteine Metabolism and Unexplained Recurrent Pregnancy Loss in Women
Authors Nguyen Ngoc N ![]() , Tran Ngoc Thao M
, Tran Ngoc Thao M ![]() , Trieu Tien S
, Trieu Tien S ![]() , Vu Tung S, Le H, Ho Sy H
, Vu Tung S, Le H, Ho Sy H ![]() , Nguyen Thanh T, Trinh The S
, Nguyen Thanh T, Trinh The S ![]()
Received 6 March 2022
Accepted for publication 27 May 2022
Published 7 June 2022 Volume 2022:15 Pages 55—62
DOI https://doi.org/10.2147/TACG.S365281
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Martin Maurer
Nhat Nguyen Ngoc,1 My Tran Ngoc Thao,2 Sang Trieu Tien,3 Son Vu Tung,4 Hoang Le,5 Hung Ho Sy,6 Tung Nguyen Thanh,1 Son Trinh The1
1Military Institute of Clinical Embryology and Histology, Vietnam Military Medical University, Hanoi, 12108, Vietnam; 2Département de formation Biologie moléculaire et cellulaire, Sorbonne University, Paris, 75006, France; 3Department of Biology and Genetics, Vietnam Military Medical University, Hanoi, 12108, Vietnam; 4Department of Epidemiology, Vietnam Military Medical University, Hanoi, 12108, Vietnam; 5IVFTA, Tam Anh General Hospital, Hanoi, 100000, Vietnam; 6Department of Obstetrics and Gynecology, Hanoi Medical University, Hanoi, 100000, Vietnam
Correspondence: Son Trinh The; Tung Nguyen Thanh, Military Institute of Clinical Embryology and Histology, Vietnam Military Medical University, Hanoi, 12108, Vietnam, Email [email protected]; [email protected]
Objective: To investigate the relationship between unexplained recurrent pregnancy loss (URPL) and polymorphisms of homocysteine metabolism-related genes in women.
Materials and Methods: A case–control study included 90 women with two or more consecutive unexplained pregnancy losses and 92 controlled women without miscarriage history; the female participants were in the age category of 18– 35 years. The high-resolution melting technique was used to detect the single-nucleotide variants related to homocysteine metabolism disorder, namely MTHFR C677T, MTHFR A1298C, MTR A2756G, and MTRR A66G polymorphism.
Results: The MTHFR C677T polymorphism had significantly correlation with URPL. Indeed, the frequency of the677T allele and genotypes (677CT, 677TT) in the URPL group was significantly higher than that in the control group (p < 0.05). However, the allele, as well as genotype distribution of MTHFR A1298C, MTR A2756G, and MTRR A66G polymorphisms showed no significant difference (p > 0.05). MTHFR 677CT-1298AC genotype combination led to a 9.0-fold increased risk of URPL (OR 9.0; 95% CI, 2.25– 35.99; p = 0.001), while the risk increased 10.0-fold (OR 10.0; 95% CI, 1.8– 55.53; p = 0.008) when participants had more than the 3 variant loci.
Conclusion: The MTHFR C677T polymorphism was a risk factor for URPL, and determining the MTHFR C677T polymorphism had a potential prediction of URPL risk. Moreover, the MTHFR C677T and MTHFR A1298C joint mutants might have a synergistic effect on URPL. Conversely, there is a lack of evidence suggesting the URPL risk of MTHFR A1298C, MTR A2756G, and MTRR A66G polymorphisms.
Keywords: unexplained recurrent pregnancy loss, homocysteine, MTHFR C677T, MTHFR A1298C, MTR A2756G, MTRR A66G
Introduction
According to the Practice Committee of the American Society for Reproductive Medicine, the term “recurrent pregnancy loss” (RPL) is defined as experiencing two or more spontaneous miscarriages occurring within 20 weeks of gestation.1,2 By studying the incidence of RPL through various researches worldwide, this condition was reported to affect up to 1–5% of women of reproductive age seeking pregnancy, which leaves a significant adverse impact on couples and society. Recurrent pregnancy loss is multifactorial; the recognized diverse causes of RPL include parental chromosomal abnormalities, immunological factors, uterine anomalies, endocrine disturbances, and even lifestyle. However, the causes are unidentifiable in 50% of the patients who are classified as experiencing unexplained recurrent pregnancy loss (URPL).3–5
Recently, it has been discovered that there exists an association between URPL and genetic polymorphisms related to inherited thrombophilic factors such as Factor V Leiden (FV), plasminogen activator inhibitor-1 (PAI-1), homocysteine metabolism, and so on.6,7 Homocysteine (Hcy) is an amino acid made from methionine by losing its terminal methyl group, and the remethylation generating methionine requires folate and vitamin B12. Three main enzymes are involved in the metabolic pathway: methylenetetrahydrofolate reductase (MTHFR), methionine synthase (MTR), and methionine synthase reductase (MTRR). Polymorphisms in the genes encoding for these enzymes have been suggested to be responsible for the altered enzyme activity that eventually accumulates homocysteine which may directly damage the endothelium and influence placental function as well as perfusion.8,9 Hence, hyperhomocysteine during pregnancy was associated with recurrent pregnancy loss, preeclampsia, and placental abruption.10–12 The human MTHFR gene contains 11 exons located on the short arm of chromosome 1p36.3. The gene encodes for methylenetetrahydrofolate reductase (MTHFR) that catalyzes the irreversible conversion of 5,10-methylenetetrahydrofolate to 5-methyltetrahydrofolate. The process provides the methyl group for the remethylation of homocysteine to methionine.13 Although some mutations within the MTHFR gene were determined, the two most common polymorphisms demonstrated to be accountable for reducing enzyme activity were MTHFR C677T and MTHFR A1298C.14,15 Indeed, MTHFR C677T has a replacement from C to T of nucleotide 677 (rs1801133) of the MTHFR gene, which can lead to amino acid substitution (Ala222Val). Concerning the MTHFR A1298C, it has a change in nucleotide 1298 (rs1801133) from A to C, which can result in amino acid substitution (Glu429Ala) in the structure of enzyme MTHFR. Recently, several studies have explored the association between these two polymorphisms and RPL, however, their contribution to the risk of RPL is controversial. In addition, MTRR is an enzyme that is required for the maintenance of the MTR active state; their combination takes part in the remethylation of homocysteine to methionine. Despite the crucial role of MTRR and MTR, few studies have explored the relationship between MTR A2756G (rs1805087, Asp919Gly), MTRR A66G (rs1801394, His595Try) polymorphism, and RPL.16–19
Furthermore, not many comprehensive studies on the homocysteine metabolic pathway have been carried out concerning the single nucleotide polymorphisms (SNPs) in all three genes together; various studies focused on the MTHFR mutations.20,21 Consequently, concerning the different genotypes of women affected with recurrent pregnancy loss, this prospective case-control study aimed to examine the association between polymorphisms in homocysteine metabolism-related genes: MTHFR, MTR, and MTRR with RPL in a Vietnamese population.
Materials and Methods
Subjects
Our case-control study enrolled a total of 182 Vietnamese women without lifestyle habits (smoking and alcohol use), the female participants were in the age category of 18–35 years; they were treated in IVF center - Military institute of clinical embryology and histology from May 2019 to May 2021. Ninety patients who had experienced two or more spontaneous abortions were all diagnosed with URPL after excluding chromosomal abnormalities, anatomical disorders, endocrine disorders, autoimmune disorders, or any uterine infections by a questionnaire survey of the obstetric history, and standardized clinical and laboratory examinations. The control group included 92 women who had at least one normal full-term pregnancy without any history of miscarriage or other gestational complications. This study was approved by the Ethical Review Committee of Vietnam Military Medical University.
Genotyping
Genomic DNA was extracted from peripheral blood with anticoagulant with the E.Z.N.A.® Blood DNA Mini Kit (Omega BIO-TEK, USA – Lot No. D339218115-42, Exp. Date 09/01/2022) following the protocol provided by the manufacturers. DNA samples were stored at −20°C until use.
The polymorphisms of MTHFR, MTR, and MTRR were detected by high resolution melting technology with the Folate Metabolism REAL-TIME PCR Genotyping Kit (DNA-Technology, Russia - LOT No. F0906U-2P, Exp. Date 06/09/2021). The reactions were carried out on the DTprime 5M1 real-time system, with the reaction conditions set to 80°C in 2 min, 94°C in 5 min, followed by 5 cycles of 94°C 30 s and 67°C 15 s and 45 cycles of 94°C 5 s and 67°C 15 s then finished with a ramping of temperature from 25°C to 75°C, each cycle lasts 30 s with Δ = 1°C. The fluorescence for gDNA control, intake control, and melting temperature were collected and then analyzed by the DTprimer. As a result, the genotypes for each gene would be annotated then used for statistic measurements.
Statistical Analysis
General clinical characteristics were presented as mean - standard deviation, the crude odds ratio (OR) at 95% confidence intervals (95% CIs) were calculated to appreciate the associations between alleles as well as genotypes and RPL by logistic regression. Differences in variables were statistically analyzed with the Student’s t-test, Mann–Whitney U-test, and Chi-square test, when appropriate. All data analyses were performed using SPSS software (version 26; IBM SPSS, NY, USA), the difference was considered statistically significant when P<0.05.
Result
The mean age was 30.20 ± 2.82 and 30.70 ± 2.44 in the URPL group and the control group, respectively. Otherwise, the height, weight, and body mass index of all participants were in the normal range.
Table 1 shows the alleles and genotype prevalences of tested polymorphisms in the URPL group and the control group. The frequencies in the T mutant allele of the MTHFR C677T and G mutant allele of the MTR A2756G were statistically significantly higher in the URPL than that in the control group, moreover, statistical analysis of these alleles using logistic regression showed the URPL risk increased 2.35-fold and 1.88-fold (OR 2.35; 95% CI, 1.43–3.86; P = 0.001 and OR 1.88; 95% CI, 1.08–3.24; P = 0.02), separately. Conversely, no different prevalences of MTHFR A1298C and MTRR A66G mutant allele were found between the two groups (P > 0.05). Concerning the genotypes, only MTHFR C677T polymorphism had significantly higher prevalences of 677CT and 677TT genotypes compared with the controls (OR 2.49; 95% CI, 1.32–4.71; P = 0.004 and OR 4.68; 95% CI, 1.19–18.32; P = 0.02, respectively). The genotype distributions of the three remaining variants were similar among women with unexplained recurrent spontaneous abortions and controls (p > 0.05).
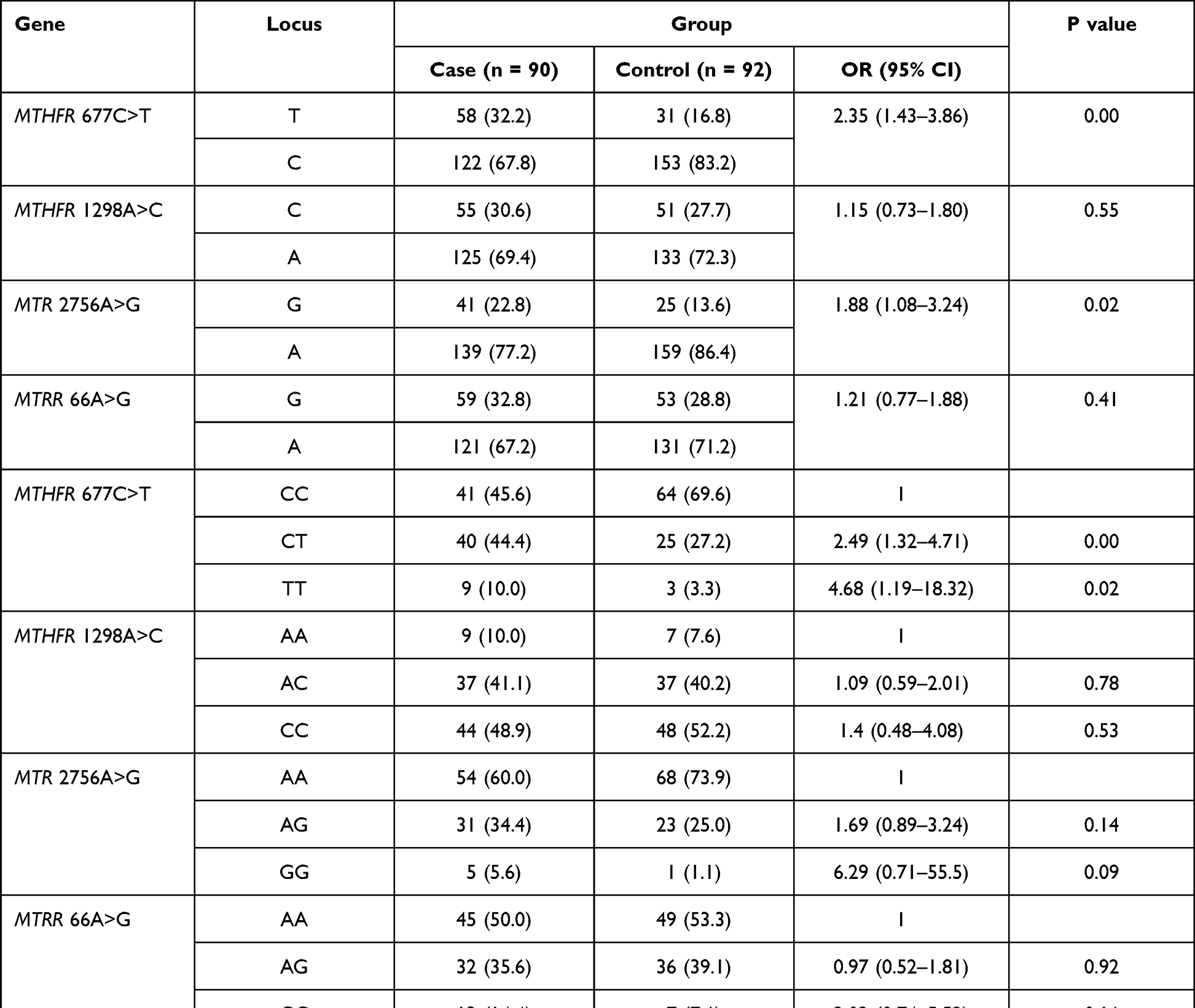 |
Table 1 Association Between Genetic Polymorphisms Related to Homocysteine Metabolism and the URPL |
Table 2 shows the number of mutations occurring on loci C677T and A1298C of the MTHFR gene, and the synergistic effect causing URPL of the two loci was analyzed by logistic regression. Firstly, the prevalence of linkage heterozygous genotype (677CT/1298AC) was significantly higher in the patients than that in the controls (13.3% versus 4.3%, P = 0.001). Moreover, patients carrying the compound heterozygous genotype were 9.0-fold (OR 9.0; 95% CI, 2.25–35.99) greater in risk of URPL than participants with the wild-type homozygous genotype (677CC/1298AA).
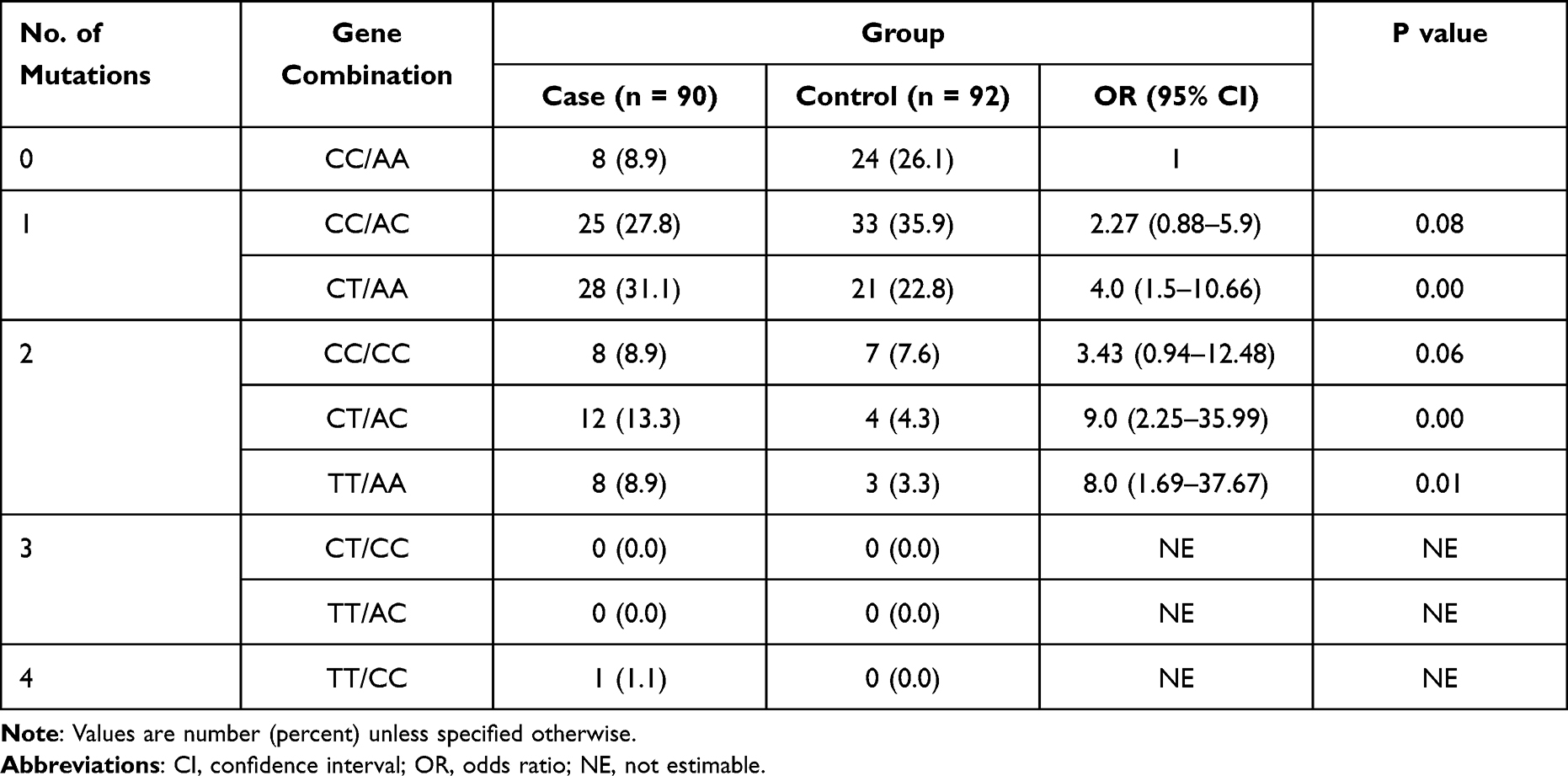 |
Table 2 The Synergistic Effect Causing URPL of the Two Loci on the MTHFR Gene |
Table 3 illustrates a certain number of loci containing the mutations among four reported loci and their association with the URPL. Although some enrolled women had 1 or 2 changed loci in total evaluated polymorphisms, their URPL risk did not increase significantly (OR 2.93; 95% CI, 0.58–14.78 and OR 4.0; 95% CI, 0.79–20.27, respectively). However, individuals who carried three or four mutant loci had a remarkable URPL risk which was 10.0 times greater than that in non-mutant women.
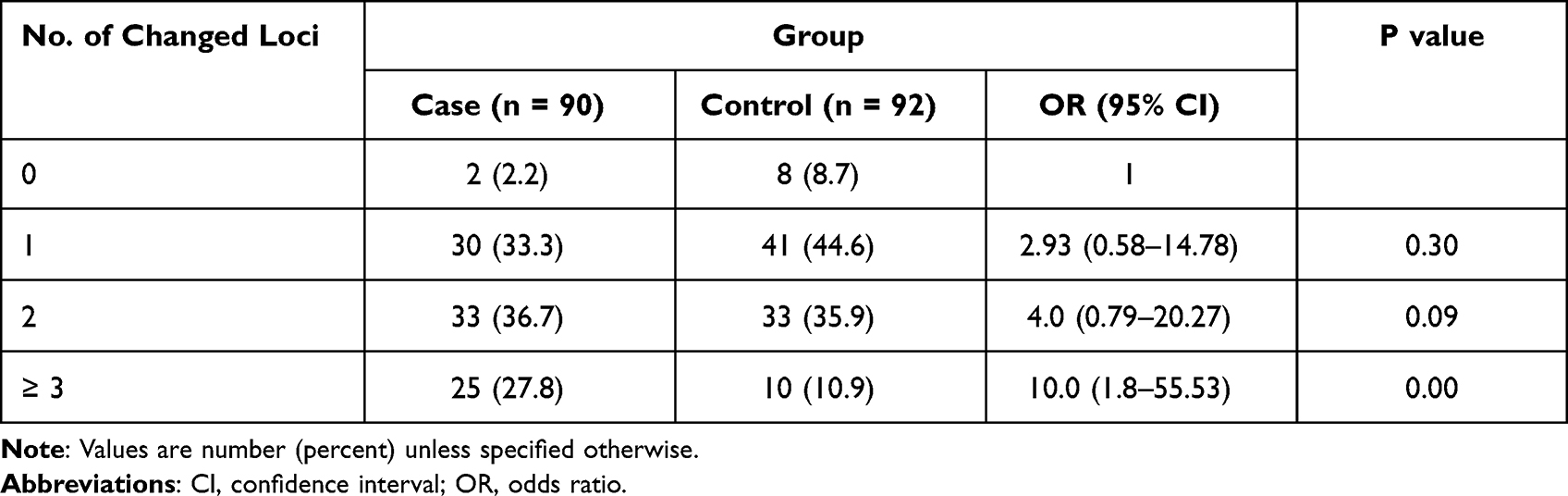 |
Table 3 Association Between the Number Changed Loci (MTHFR C677T, MTHFR A1298C, MTR A2756G, MTRR A66G) and the URPL |
Discussion
Recurrent pregnancy loss is a frustrating medical condition and shows high risks for developing depression and anxiety which affect both men and women.22 In recent years, various studies focusing on the causes of RPL have demonstrated that it may be multifactorial in many pregnancies; however, little has been understood about the underlying causes of approximately 50% of patients.23,24 Consequently, the emerging prevalence for RPL has brought much attention to the study of its possible risk factors, such as advanced maternal age, obesity, unhealthy lifestyle habits (including smoking, alcohol consumption), and especially genetic polymorphisms.25–27
Genetic polymorphisms have been intensively evaluated. Their findings suggested an essential role of the risk in the pathogenesis of recurrent pregnancy loss. More than 37 genes with 53 polymorphisms were discovered, including MTR, MTHFR, PAI-1, HLA-G, TNF, IL-6, FII, FV, FXIII, ITGB3, NOS3, KDR, TP53, VEGFA, CYP17CYP2D6, ANXA5, and so on. The four major causes of URPL were thrombophilia, disordered placental function, abnormal immunological responses, and metabolic regulation disturbance, but their results conflicted, especially when conducted in variant populations.6 This study focused on inherited thrombophilia of the Vietnamese population by examining the association between polymorphisms in homocysteine metabolism-related genes: MTHFR, MTR, and MTRR with RPL. Other risk factors were excluded to reduce the bias. Maternal age is a primary confounding matter strongly associated with recurrent pregnancy loss. Many studies reported that recurrent miscarriages often occur more frequently with increasing maternal age, the age threshold is usually defined as 35 years.28 Indeed, all participants were in the age category of 18–35 years and did not have significant differences between the mean ages between the two groups.
The MTHFR gene encodes the enzyme methylenetetrahydrofolate reductase (MTHFR), which is responsible for production of 5-methyltetrahydrofolate. Then 5-methyltetrahydrofolate provides the methyl group for the remethylation of methionine from homocysteine.13 Two predominant single-nucleotide polymorphisms in the MTHFR gene are 677C>T (rs1801133) and 1298A>C (rs1801131), reducing MTHFR enzyme function, especially in the homozygous recessive genotype. The prevalence of people carrying at least one of these variants was reported at 60–70%, while our figure was 75.56% in controls.29,30 The MTHFR 677T and 1298C allele frequencies depend on populations which were 16.8% and 27.7%, respectively, in controls of this study.31,32 Moreover, the MTHFR 677T allele frequency was higher in the URPL than in the control group; statistical analysis showed the URPL risk of women carrying the allele increased 2.35-fold. Homozygote and heterozygote genotype (MTHFR 677TT, MTHFR 677CT) increased the risk of URPL significantly to 4.68 and 2.49, separately. This was caused by reducing MTHFR enzyme function, carriers of the homozygote and heterozygote genotype retained approximately 30% and 65% of enzyme activity.15 Numerous studies have reported the associations between MTHFR C677T polymorphism and URPL; however, the results have been controversial. Indeed, a majority of the studies supposed MTHFR C677T SNP was the risk factor for the RPL, and others argued that there was no association between MTHFR C677T and the disease.33–35 The 677CT and 677TT genotype of MTHFR and composite heterozygote genotype (677CT/1298AC) were risk factors for URPL. The prevalence of linkage heterozygous genotype (677 CT/1298 AC) was associated with a 9.0-fold increase in the risk of RPL over individuals with homozygous wild-type genotype (677 CC/1298 AA). Our obtained result was consistent with other previously published papers with modest fluctuation in OR (95% CI) and produced one similar conclusion that the compound heterozygosity may be responsible for miscarriage risks.33,35,36
In variant MTR A2756G, a higher figure in women with recurrent pregnancy loss was observed in the frequency of both G allele and 2756 GG genotype (p < 0.05), proving that this polymorphism was related to the rising risk of URPL. In fact, this glycine substitution for aspartic acid at the 919 position of the protein might lead to the structural impairment and eventually cause the elevation of plasma homocysteine concentration which contributed to clinical conditions such as spontaneous miscarriage.37 Our conclusion was consistent with the previously published paper conducted in the Iranian population.38 Conversely, the MTR A2756G and MTRR A66G polymorphisms in RPL patients have been studied in the Korean population since 2013; the finding suggested that MTR A2756G and MTRR A66G polymorphisms were not possible predisposing markers for URPL.18
This report was the first to reveal the genetic susceptibility due to the SNPs (MTHFR C677T; MTHFR A1298C; MTR A2756G; MTRR A66G) in Vietnamese women and the risk of experiencing URPL. Participants with more than three changed loci demonstrated a remarkably high risk of experiencing URPL compared with control groups (OR 10.0; 95% CI; 1.8–55.53). This indicated that more aspects and correlations between these polymorphisms should carefully be investigated to shed light on the underlying risk of recurrent pregnancy loss and single-polynucleotide polymorphisms.
Conclusion
In conclusion, the MTHFR C677T polymorphism was a risk factor for URPL, and identifying the MTHFR C677T polymorphism had a potential prediction of URPL risk. Moreover, the MTHFR C677T and MTHFR A1298C joint mutants might have a synergistic effect on URPL. However, there was a lack of evidence suggesting the URPL risk of MTHFR A1298C, MTR A2756G, and MTRR A66G polymorphisms. Consequently, further genetic research needs to be conducted on a bigger sample size to investigate the correlation between these subjects.
Ethical Statements
All participants signed informed written consent to be part of the study. Our protocol was appropriate to the Declaration of Helsinki, and approved by the Ethical Review Committee of Vietnam Military Medical University (No. 1068/2019/VMMU-IRB).
Acknowledgment
We give many thanks to Military Institute of clinical Embryology and Histology for supporting this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declared no conflicts of interest for this work, and received no financial support for the research, authorship, and/or publication of this article.
References
1. Practice Committee of the American Society for Reproductive Medicine. Definitions of infertility and recurrent pregnancy loss: a committee opinion. Fertil Steril. 2013;99(1):63. doi:10.1016/j.fertnstert.2012.09.023
2. Cao Y, Zhang Z, Zheng Y, et al. The association of idiopathic recurrent early pregnancy loss with polymorphisms in folic acid metabolism-related genes. Genes Nutr. 2014;9(3):402. doi:10.1007/s12263-014-0402-x
3. Diejomaoh MFE. Recurrent spontaneous miscarriage is still a challenging diagnostic and therapeutic quagmire. Med Princ Pract. 2015;24(Suppl 1):38–55. doi:10.1159/000365973
4. Kumar N, Ahluwalia J, Das R, et al. Inherited thrombophilia profile in patients with recurrent miscarriages: experience from a tertiary care center in north India. Obstet Gynecol Sci. 2015;58(6):514–517. doi:10.5468/ogs.2015.58.6.514
5. Nair RR, Khanna A, Singh K. MTHFR C677T polymorphism and recurrent early pregnancy loss risk in north Indian population. Reprod Sci. 2012;19(2):210–215. doi:10.1177/1933719111417888
6. Shi X, Xie X, Jia Y, Li S. Maternal genetic polymorphisms and unexplained recurrent miscarriage: a systematic review and meta-analysis. Clin Genet. 2017;91(2):265–284. doi:10.1111/cge.12910
7. Brenner B. Inherited thrombophilia and pregnancy loss. Thromb Haemost. 1999;82(2):634–640. doi:10.1055/s-0037-1615890
8. van Meurs JBJ, Pare G, Schwartz SM, et al. Common genetic loci influencing plasma homocysteine concentrations and their effect on risk of coronary artery disease. Am J Clin Nutr. 2013;98(3):668–676. doi:10.3945/ajcn.112.044545
9. Kamali M, Hantoushzadeh S, Borna S, et al. Association between thrombophilic genes polymorphisms and recurrent pregnancy loss susceptibility in the Iranian population: a systematic review and meta-analysis. Iran Biomed J. 2018;22(2):78–89. doi:10.22034/ibj.22.2.78
10. Harris EN, Chan JK, Asherson RA, Aber VR, Gharavi AE, Hughes GR. Thrombosis, recurrent fetal loss, and thrombocytopenia. Predictive value of the anticardiolipin antibody test. Arch Intern Med. 1986;146(11):2153–2156. doi:10.1001/archinte.1986.00360230069012
11. Coulam CB, Jeyendran RS, Fishel LA, Roussev R. Multiple thrombophilic gene mutations are risk factors for implantation failure. Reprod Biomed Online. 2006;12(3):322–327. doi:10.1016/s1472-6483(10)61004-8
12. Gaiday AN, Tussupkaliyev AB, Bermagambetova SK, et al. Effect of homocysteine on pregnancy: a systematic review. Chem Biol Interact. 2018;293:70–76. doi:10.1016/j.cbi.2018.07.021
13. Bailey LB, Gregory JF. Folate metabolism and requirements. J Nutr. 1999;129(4):779–782. doi:10.1093/jn/129.4.779
14. Ebadifar A, KhorramKhorshid HR, Kamali K, Salehi Zeinabadi M, Khoshbakht T, Ameli N. Maternal supplementary folate intake, Methylenetetrahydrofolate Reductase (MTHFR) C677T and A1298C polymorphisms and the risk of orofacial cleft in Iranian children. Avicenna J Med Biotechnol. 2015;7(2):80–84.
15. Frosst P, Blom HJ, Milos R, et al. A candidate genetic risk factor for vascular disease: a common mutation in methylenetetrahydrofolate reductase. Nat Genet. 1995;10(1):111–113. doi:10.1038/ng0595-111
16. Luo L, Chen Y, Wang L, et al. Polymorphisms of genes involved in the folate metabolic pathway impact the occurrence of unexplained recurrent pregnancy loss. Reprod Sci. 2015;22(7):845–851. doi:10.1177/1933719114565033
17. Li X, Jiang J, Xu M, et al. Individualized supplementation of folic acid according to polymorphisms of methylenetetrahydrofolate reductase (MTHFR), methionine synthase reductase (MTRR) reduced pregnant complications. Gynecol Obstet Invest. 2015;79(2):107–112. doi:10.1159/000367656
18. Kim JH, Jeon YJ, Lee BE, et al. Association of methionine synthase and thymidylate synthase genetic polymorphisms with idiopathic recurrent pregnancy loss. Fertil Steril. 2013;99(6):1674–1680. doi:10.1016/j.fertnstert.2013.01.108
19. Sata F, Yamada H, Kishi R, Minakami H. Maternal folate, alcohol and energy metabolism-related gene polymorphisms and the risk of recurrent pregnancy loss. J Dev Orig Health Dis. 2012;3(5):327–332. doi:10.1017/S2040174412000359
20. Kobashi G, Kato EH, Morikawa M, et al. MTHFR C677T polymorphism and factor V Leiden mutation are not associated with recurrent spontaneous abortion of unexplained etiology in Japanese women. Semin Thromb Hemost. 2005;31(3):266–271. doi:10.1055/s-2005-872430
21. Settin A, Elshazli R, Salama A, ElBaz R. Methylenetetrahydrofolate reductase gene polymorphisms in Egyptian women with unexplained recurrent pregnancy loss. Genet Test Mol Biomarkers. 2011;15(12):887–892. doi:10.1089/gtmb.2011.0049
22. Voss P, Schick M, Langer L, et al. Recurrent pregnancy loss: a shared stressor—couple-orientated psychological research findings. Fertil Steril. 2020;114(6):1288–1296. doi:10.1016/j.fertnstert.2020.08.1421
23. McNamee K, Dawood F, Farquharson R. Recurrent miscarriage and thrombophilia: an update. Curr Opin Obstet Gynecol. 2012;24(4):229–234. doi:10.1097/GCO.0b013e32835585dc
24. Jauniaux E, Farquharson RG, Christiansen OB, Exalto N. Evidence-based guidelines for the investigation and medical treatment of recurrent miscarriage. Hum Reprod. 2006;21(9):2216–2222. doi:10.1093/humrep/del150
25. Kesmodel U, Wisborg K, Olsen SF, Henriksen TB, Secher NJ. Moderate alcohol intake in pregnancy and the risk of spontaneous abortion. Alcohol Alcohol. 2002;37(1):87–92. doi:10.1093/alcalc/37.1.87
26. Boots C, Stephenson MD. Does obesity increase the risk of miscarriage in spontaneous conception: a systematic review. Semin Reprod Med. 2011;29(6):507–513. doi:10.1055/s-0031-1293204
27. Ness RB, Grisso JA, Hirschinger N, et al. Cocaine and tobacco use and the risk of spontaneous abortion. N Engl J Med. 1999;340(5):333–339. doi:10.1056/NEJM199902043400501
28. du Fossé NA, van der Hoorn MLP, van Lith JMM, le Cessie S, Lashley EELO. Advanced paternal age is associated with an increased risk of spontaneous miscarriage: a systematic review and meta-analysis. Hum Reprod Update. 2020;26(5):650–669. doi:10.1093/humupd/dmaa010
29. Burda P, Schäfer A, Suormala T, et al. Insights into severe 5,10-methylenetetrahydrofolate reductase deficiency: molecular genetic and enzymatic characterization of 76 patients. Hum Mutat. 2015;36(6):611–621. doi:10.1002/humu.22779
30. Wilcken B, Bamforth F, Li Z, et al. Geographical and ethnic variation of the 677C>T allele of 5,10 methylenetetrahydrofolate reductase (MTHFR): findings from over 7000 newborns from 16 areas world wide. J Med Genet. 2003;40(8):619–625. doi:10.1136/jmg.40.8.619
31. National Center for Biotechnology Information. Frequency and association of 1691 (G>A) FVL, 20210 (G>A) PT and 677 (C>T) MTHFR with deep vein thrombosis in the population of Bosnia and Herzegovina. Available from: https://pubmed.ncbi.nlm.nih.gov/27785407/.
32. Mahmutbegović E, Marjanović D, Medjedović E, et al. Prevalence of F5 1691G>A, F2 20210G>A, and MTHFR 677C>T polymorphisms in Bosnian women with pregnancy loss. Bosn J Basic Med Sci. 2017;17(4):309–314. doi:10.17305/bjbms.2017.1954
33. Al-Achkar W, Wafa A, Ammar S, Moassass F, Jarjour RA. Association of methylenetetrahydrofolate reductase C677T and A1298C gene polymorphisms with recurrent pregnancy loss in Syrian Women. Reprod Sci. 2017;24(9):1275–1279. doi:10.1177/1933719116682874
34. Yang Y, Luo Y, Yuan J, et al. Association between maternal, fetal and paternal MTHFR gene C677T and A1298C polymorphisms and risk of recurrent pregnancy loss: a comprehensive evaluation. Arch Gynecol Obstet. 2016;293(6):1197–1211. doi:10.1007/s00404-015-3944-2
35. Xu Y, Ban Y, Ran L, et al. Relationship between unexplained recurrent pregnancy loss and 5,10-methylenetetrahydrofolate reductase) polymorphisms. Fertil Steril. 2019;111(3):597–603. doi:10.1016/j.fertnstert.2018.11.011
36. Zetterberg H, Regland B, Palmér M, et al. Increased frequency of combined methylenetetrahydrofolate reductase C677T and A1298C mutated alleles in spontaneously aborted embryos. Eur J Hum Genet. 2002;10(2):113–118. doi:10.1038/sj.ejhg.5200767
37. Biselli JM, Goloni-Bertollo EM, Haddad R, Eberlin MN, Pavarino-Bertelli EC. The MTR A2756G polymorphism is associated with an increase of plasma homocysteine concentration in Brazilian individuals with Down syndrome. Braz J Med Biol Res. 2008;41(1):34–40. doi:10.1590/s0100-879x2006005000195
38. Association of the methionine synthase gene polymorphism with recurrent miscarriage in Mazandaran Province - Search Results. Available from: https://pubmed.ncbi.nlm.nih.gov/?term=Association+of+the+methionine+synthase+gene+polymorphism+with+recurrent+miscarriage+in+Mazandaran+province.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.