")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Evaluating the Aspects of Quality of Life in Individuals with Substance Use Disorder: A Systematic Review Based on the WHOQOL Questionnaire
Authors Bratu ML, Sandesc D, Anghel T, Tudor R , Shaaban L , Ali A, Toma AO, Bratosin F , Turcu I, Gantsa A, Fericean RM, Bondrescu M , Barata PI
Received 12 October 2023
Accepted for publication 17 December 2023
Published 28 December 2023 Volume 2023:16 Pages 4265—4278
DOI https://doi.org/10.2147/JMDH.S440764
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Melania Lavinia Bratu,1– 3 Dorel Sandesc,4 Teodora Anghel,1 Raluca Tudor,5 Luai Shaaban,6 Ayesha Ali,7 Ana-Olivia Toma,8 Felix Bratosin,2,9 Izabela Turcu,10 Andrei Gantsa,11 Roxana Manuela Fericean,2,9 Mariana Bondrescu,2,12 Paula Irina Barata13,14
1Center for Neuropsychology and Behavioral Medicine, Department of Psychology, Faculty of General Medicine, “Victor Babes” University of Medicine and Pharmacy, Timisoara, Romania; 2Doctoral School, “Victor Babes” University of Medicine and Pharmacy, Timisoara, Romania; 3Center for Cognitive Research in Neuropsychiatric Pathology, Department of Neurosciences, “Victor Babes” University of Medicine and Pharmacy, Timisoara, Romania; 4Department of Anesthesia and Intensive Care, “Victor Babes” University of Medicine and Pharmacy, Timisoara, Romania; 5Second Discipline of Neurology, “Victor Babes” University of Medicine and Pharmacy, Timisoara, Romania; 6Faculty of General Medicine, Baskent University, Ankara, Turkey; 7Bhaskar Medical College, Hyderabad, Telangana State, India; 8Discipline of Dermatology, “Victor Babes” University of Medicine and Pharmacy, Timisoara, Romania; 9Department of Infectious Diseases, “Victor Babes” University of Medicine and Pharmacy, Timisoara, Romania; 10Iuliu Hatieganu University of Medicine and Pharmacy, Cluj-Napoca, Romania; 11Volgograd State Medical University, Volgograd, Russia; 12Department of Psychiatry, “Victor Babes” University of Medicine and Pharmacy, Timisoara, Romania; 13Department of Physiology, Faculty of Medicine, “Vasile Goldis” Western University, Arad, Romania; 14Center for Research and Innovation in Precision Medicine of Respiratory Diseases, “Victor Babes” University of Medicine and Pharmacy, Timisoara, Romania
Correspondence: Raluca Tudor, Email [email protected]
Abstract: Substance Use Disorder (SUD) has become a significant public health concern and it profoundly impacts an individual’s quality of life (QOL). This systematic review aimed to assess the QOL among patients with SUD, and to understand the differential impact of SUD on physical, mental, social, and environmental QOL domains, considering a variety of substances and identifying key factors that influence these outcomes. A comprehensive search was conducted in PubMed, Web of Science, Cochrane, and Scopus in January 2023, covering literature published until December 2022. The QOL was assessed using the World Health Organization Quality of Life (WHOQOL) instrument and the brief version of the WHOQOL, identifying the same four domains of QOL (physical, mental, social, and environmental). A total of 19 studies were selected for inclusion in the systematic review, based on individuals’ polysubstance use, and excluding those using only nicotine or alcohol. The analysis included 6079 patients, with only 40.3% women, and a mean age of 36.6 years. The substances most commonly involved in SUD were cocaine (47.1%), alcohol (46.3%), and amphetamine (43.6%), considering most individuals being polysubstance users. The highest variability in QOL scores was observed in the physical domain. Mental disorders were reported in 68.3% of the patients, while long-term use of drugs, criminal history, unemployment, and low levels of education were identified as significant predictors for lower QOL by some of the studies. Similarly, sleep problems and teeth decay were also identified as significant worsening factors for QOL. This systematic review highlights that the WHOQOL survey is widely accepted and applicable for individuals with SUD worldwide. The results suggest a substantial negative impact of SUD on the QOL of affected individuals. The findings underscore the need for comprehensive interventions to address the physical, psychological, social, and environmental dimensions of QOL among individuals with SUD.
Keywords: quality of life, substance abuse, substance addiction
Introduction
Substance use disorder (SUD), including the misuse of alcohol, narcotics, and opioids, has become a significant public health concern worldwide, with far-reaching consequences for both individuals and communities.1,2 The World Health Organization (WHO) reports that approximately 275 million people, or 5.6% of the global population aged 15–64 years, used illegal substances at least once in 2020, and over 36 million individuals suffered from drug use disorders.3 Alcohol use alone contributes to more than 3 million deaths annually, accounting for 5.1% of the global burden of disease and injury. Opioids have seen a dramatic increase in use and addiction, with the United States experiencing an opioid epidemic that has caused significant morbidity and mortality.4,5
The consequences of SUD extend beyond the physical health risks associated with the use of these substances. Individuals with substance abuse disorders often experience a decline in their quality of life (QOL), with negative impacts on their mental, emotional, social, and economic well-being.6,7 The WHO defines QOL as an individual’s perception of their position in life within the context of their culture and value systems and in relation to their goals, expectations, standards, and concerns.8 Understanding of the potential factors that may affect an individual’s QOL is essential to developing effective interventions and support systems to improve the lives of those affected.
Existing literature on substance abuse and QOL has demonstrated that individuals with substance use disorders generally report lower QOL scores compared to the general population.9,10 Furthermore, the severity of SUD, the type of substance used, and the duration of use have all been found to influence QOL.11 Alcohol-dependent individuals have been shown to experience reduced physical and mental health-related QOL compared to their non-dependent counterparts.12 Similarly, individuals with opioid use disorder report lower QOL across various domains, including physical health, psychological well-being, and social functioning.13 For instance, one study examined the health-related quality of life (HRQOL) of long-term patients with opioid addiction on opioid agonist therapy versus the Norwegian general population.14 It found that the average HRQOL and self-perceived health of these patients are significantly lower than that of the general population at baseline and at the 1-year follow-up term, and lower than what has been found among other severe somatic and psychiatric conditions. Moreover, around 5% had extremely poor HRQOLTherefore,it is evident that the detrimental effects of substance abuse on an individual’s QOL are multi-dimensional and far-reaching.
Although it is well-documented that people with SUD experience a diminished QOL compared to the general population,15,16 it is less understood how specific dimensions of QOL are affected, how different substances affect QOL dimensions, and what factors could influence these dimensions. Different substances could affect QOL dimensions variably, and the understanding of this variability is necessary for tailored, substance-specific treatment strategies. In addition, while certain common factors affecting QOL in SUD patients are recognized, a comprehensive understanding that spans across different substances is lacking. The World Health Organization Quality of Life (WHOQOL) instrument, by capturing multiple dimensions of QOL,17–19 provides a valuable tool to conduct such a comprehensive review. Therefore, the unique contribution and objective of the current study is to systematically review and synthesize the available literature on the effect of substance use disorder on different QOL dimensions based on the WHOQOL instrument, to evaluate differences across different substances, and identify potential influencing factors.
Materials and Methods
Review Protocol
This systematic review was conducted in January 2023, utilizing four online databases: PubMed, Web of Science, Cochrane, and Scopus. The review encompassed literature published up until December 2022. The investigation covered the following medical subject headings (MeSH)20 keywords: “quality of life”, “substance abuse”, “substance addiction”, “substance dependence”, “substance use”, “substance use disorder”, “narcotic addiction”, “drug addiction”, “drug abuse”, “drug users”, and “drug addicts”. The search was restricted to English-language journal articles.
Employing a structured and systematic search strategy in compliance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)21 criteria and the International Prospective Register of Systematic Reviews (PROSPERO)22 guidelines, all pertinent scientific papers that used the WHOQOL in patients with substance use disorder were incorporated into the current analysis. This systematic review was registered on the Open Science Framework (OSF) platform.23
The main objectives of this systematic review are explained by the following research questions:
Research Question 1: What are the variations in QOL among individuals with SUD across different demographic and clinical groups?
Research Question 2: Which dimensions of QOL are most negatively impacted in individuals with SUD, and what factors are associated with these poorer outcomes?
Research Question 3: How do QOL dimensions vary among individuals using different types of substances, and what are the specific predictors used in each study’s model?
Quality of Life Assessment
Quality of Life (QOL) was assessed using the WHOQOL instrument and its short version (WHOQOL-BREF), which is a self-administered questionnaire employing a 5-point Likert scale format.24 The WHOQOL instrument has demonstrated robust psychometric properties in general populations, making it a reliable and valid tool for assessing the quality of life in patients with substance abuse. By employing this comprehensive instrument, the study aims to provide a thorough evaluation of QOL dimensions based on the WHOQOL for individuals affected by SUD.
The WHOQOL emphasizes the multifaceted nature of QOL by evaluating various dimensions. In the main version, a total of 100 items are employed, while in the BREF version there are 26 items that are divided into four distinct domains, which are intended to capture the diverse aspects of an individual’s quality of life. These BREF scale domains include Physical (7 items), Psychological (6 items), Social Relationships (3 items), and Environment (8 items). Each item is rated on a scale of 1 to 5, so the scores for each domain range from 7 to 35, 6 to 30, 3 to 15, and 8 to 40, respectively. Notably, the first two global rating items on QOL and perceived global health are not included in the aforementioned four domains. Therefore, the overall QOL score is calculated as the sum of all items.
Similarly, the full WHOQOL questionnaire comprises the same QOL domains that are calculated in a similar manner. The scores for each facet range from 4 to 20. The facets are grouped into the four domains: Physical (7 items), Psychological (6 items), Social Relationships (3 items), and Environment (8 items). Thus, their scores range from 28 to 140, 24 to 120, 12 to 60, and 32 to 160, respectively. Importantly, these domain scores are computed in a positive direction, meaning that higher scores are indicative of a higher quality of life.
For scoring conversion, the WHOQOL-BREF calculates four domain scores based on the mean scores of items within each domain. These mean scores are then multiplied by 4 to make them comparable with the scores used in the WHOQOL-100. This process involves two transformation methods: the first converts scores to a range between 4 and 20, aligning with the WHOQOL-100, and the second converts domain scores to a 0–100 scale. This system allows for a standardized comparison between the two versions of the WHOQOL. Additionally, it is noted that in the WHOQOL-BREF, items are rated on a 5-point Likert scale. The mean score for each domain is calculated, resulting in a score per domain between 4 and 20. This mean domain score is then multiplied by 4 to transform it into a scaled score, making it comparable with the scores used in the original WHOQOL-100.24 Thus, a higher score indicates a higher quality of life.
Selection Process
The main sources of information for the gathered material included the text, tables, figures, and additional web resources present in the articles. The initial stage of the selection process involved the elimination of duplicate submissions, followed by a thorough examination of each abstract and, ultimately, a complete review of the entire text. Additionally, the reference lists of the collected papers were meticulously inspected to identify relevant content.
The criteria for including a study in the analysis were as follows: (1) the research should focus on the quality of life among individuals and patients classified as substance abusers or SUD patients; (2) the study must have employed the WHOQOL questionnaire for assessment; (3) the research must have detailed all four aspects of the quality of life evaluation, which are physical, psychological, social, and environmental dimensions. Conversely, the exclusion criteria were: (1) studies that utilized alternative instruments to assess the quality of life; (2) studies lacking data on all four dimensions of the WHOQOL; (3) case reports, literature reviews, meta-analyses, letters to editors, and brief communications were also excluded from the selection; (4) studies that focused only on nicotine or alcohol use.
The current systematic review was designed to focus specifically on illicit drugs and polysubstance use. Substance use disorder, according to the DSM-5, refers to a addiction disorder that impacts an individual’s brain and behavior, resulting in an inability to resist the consumption of legal or illicit drugs or pharmaceutical substances. Furthermore, based on DSM-5, alcohol and marijuana (cannabis) and nicotine are also considered substances capable to cause addiction.25
In the context of our review, we considered the following variables to be considered for reporting in this review: (1) study characteristics: study number and author, country of the study, the year of study development, study design, and quality assessment; (2) summary of findings: number of patients, average age, the proportion of female patients, study particularities, and substances used by the study participants; (3) evaluation of Quality-of-Life Dimensions (WHOQOL and WHOQOL-BREF: survey type, physical domain, mental domain, social domain, environmental domain, and quality of life worsening factors.
Data Extraction and Quality Assessment
The preliminary search results yielded a total of 9174 articles, out of which 422 were identified as duplicates. After excluding 8206 papers based on their abstracts, 551 full-text articles were assessed for eligibility. Ultimately, 19 articles were selected for inclusion in the systematic review, as presented in Figure 1. Based on the Study Quality Assessment Tools provided by the National Heart, Lung, and Blood Institute (NHLBI),26 two investigators independently evaluated the published material and documented their findings. These tools are tailored to specific study designs, enabling the detection of methodological or design concerns.
 |
Figure 1 PRISMA Flow Diagram. Notes: Adapted from Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PloS Med. 2009;6(7):e1000097. Creative Commons. |
For the remaining studies, the Quality Assessment Tool for Observational Cohort and Cross-Sectional Investigations was employed. Each question within the tool received a score of 1 point for “Yes” answers and 0 points for “No” and “Other” responses. Subsequently, the final performance score was calculated. Accordingly, studies with scores ranging from 0 to 4 were considered to be of fair quality, those with scores between 5 and 9 were deemed to be of good quality, and those with a score of 10 or higher were classified as excellent quality, as seen in Table 1. By assigning two independent researchers to evaluate the quality of the chosen articles, this approach aimed to minimize selection bias by encouraging a comprehensive selection and inclusion of studies. The dual evaluation also helped in identifying and filling any potential gaps in the data, thereby reducing missing data. Further, the use of a standardized assessment tool between the evaluators mitigated measurement bias, ensuring a more consistent and reliable evaluation. This methodology of dual evaluation is in line with common practices in systematic reviews.
 |
Table 1 Study Characteristics |
Results
The systematic review of studies on individuals with substance use disorder (SUD) presents a comprehensive overview of this population. Collectively, the studies analyzed involved 6079 participants. Notably, the gender distribution was diverse: women constituted 100% of the participants in two studies27,29 but represented only a small fraction in others, such as 0.6% in the study by Singh et al45 and 0% in Paiva’s et al study.44 Overall, the mean/median age of participants across studies was around 37 years, with the youngest average of 31.1 years33 and the oldest average of 47.5 years.36
A significant presence of mental disorders was reported In many studies, with percentages as high as 73.2% in the studies by Tracy et al27 and Brown et al29 and 100% in Paiva’s et al study.44 Substance use varied widely, with cocaine and heroin being the most prevalent in several studies. Cocaine usage was particularly high in Tracy’s et al study (62.1%)27 and Brown’s et al study (56.6%),29 while heroin was the sole substance used by all participants in the study by Mitchell et al.31
Other substances frequently reported included alcohol, with the lowest use in the study by Yen et al (23.1%)30 and 80.9% in Marques’ et al study,43 while marijuana had a significant usage in the study by Tracy et al27 (41.3%) and Muller et al35 (42.1%). The prevalence of opioid usage was also noteworthy, particularly in the study by Byrne et al32 (40.0%) and Tun et al39 (55.5%). Amphetamines were predominantly used in the study by Wang et al from Taiwan (60.1%)28 and Tun’s et al study from Myanmar (70.0%),39 as presented in Table 2.
 |
Table 2 Summary of Findings in the Included Studies |
In addition to substance use, the studies highlighted specific characteristics and comorbidities among participants. For instance, a considerable percentage of individuals in Wang’s et al study (42.9%)28 had a criminal history. Long-term injecting drug use was reported in 81.7% of participants in the study by Yen et al30 while sleep problems were prominent in 56.0% of participants in Saffari et al.40 Also, one study focused exclusively on methamphetamine users,33 another study on benzodiazepine users,32 and the study by Mitchell et al31 on African American heroin users, underscoring the diverse and specific nature of SUD populations.
Table 3, which evaluates the Quality-of-Life Dimensions using WHOQOL and WHOQOL-BREF questionnaires, indicates a broad spectrum of scores across the studies, reflecting the varied impacts of substance use disorders on quality of life. The average domain scores among all studies were 60.1 in the physical WHOQOL domain, 54.0 in the mental domain, 53.7 in the social domain, and 58.2 in the environmental domain, respectively (Figure 2). In the physical domain, scores varied from a low of 48.0 in Flores-Garcia et al36 to a high of 87.6 in Wang et al.28 This highlights the substantial variability in physical well-being experienced by individuals with substance use disorders, as seen in the different study populations. In the mental domain, the range was similarly diverse. The lowest score was observed in Flores-Garcia et al36 (46.4), focusing on young patients with mental disorders and ADHD, while the highest score was reported by Wang et al28 (69.2). This range underscores the significant impact of substance use disorders on mental health, varying greatly depending on individual circumstances and demographics.
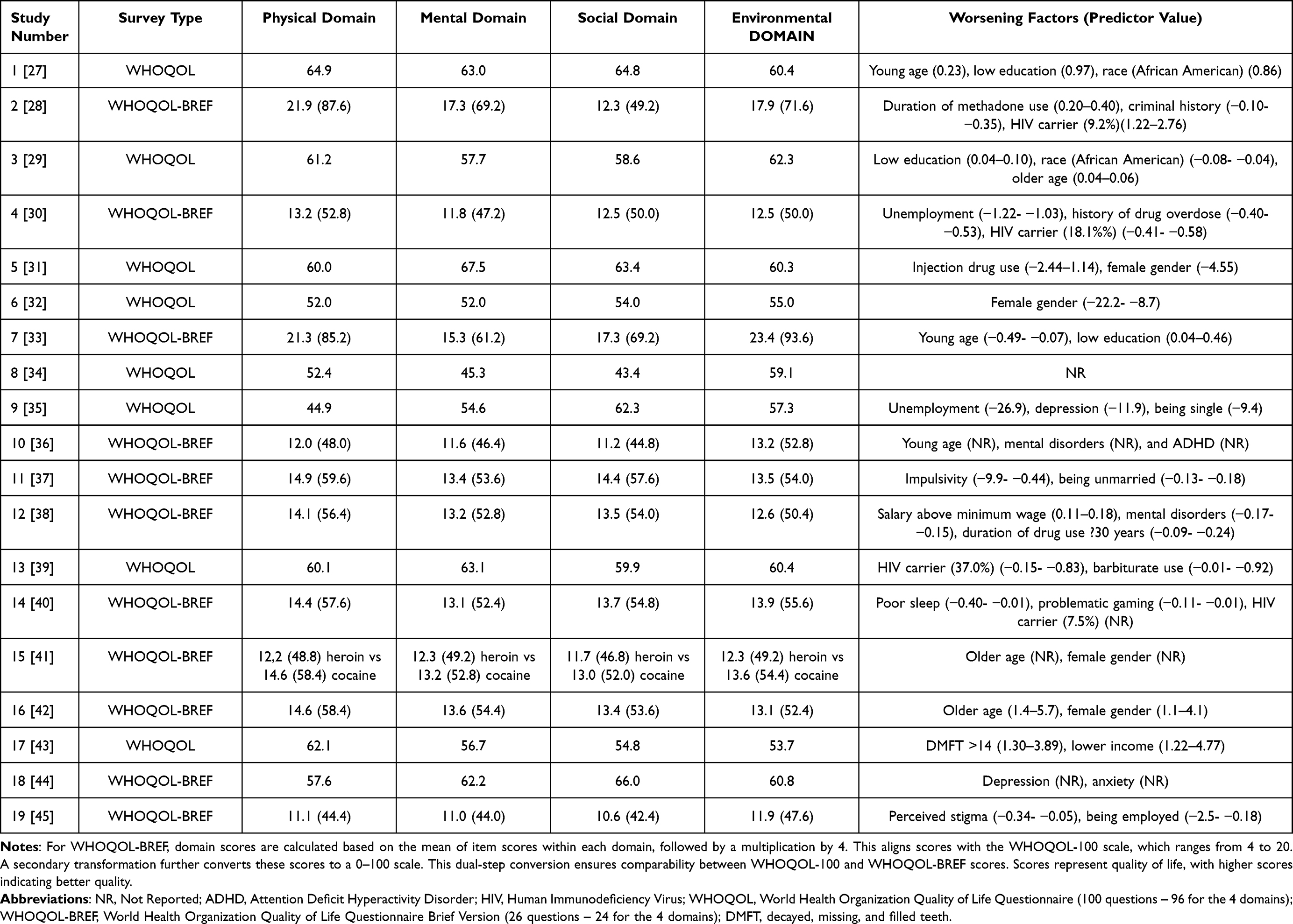 |
Table 3 Evaluation of Quality-of-Life Dimensions (WHOQOL and WHOQOL-BREF) |
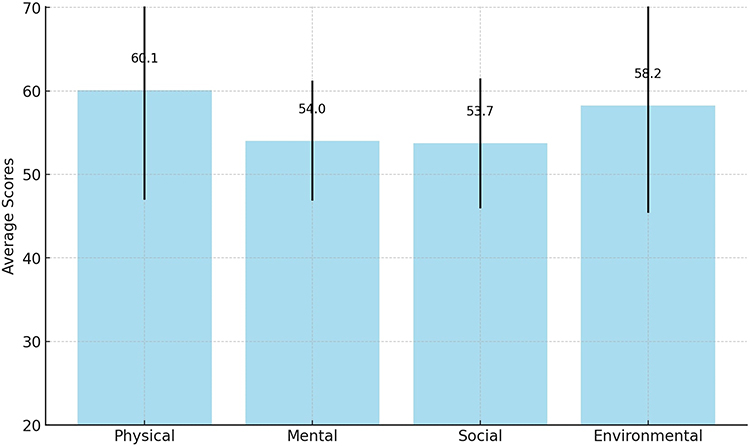 |
Figure 2 Average values of domain scores on the WHOQOL and WHOQOL-BREF questionnaires. |
Social domain scores exhibited substantial variation, ranging from 44.8 in Flores-Garcia et al36 to 69.2 in Rubenis et al,33 reflecting the diverse social challenges faced by individuals with substance use disorders. This variability could be attributed to the different demographic and social factors prevalent in each study’s participant group. Environmental domain scores also showed significant differences, with the lowest score in Flores-Garcia et al36 (52.8) and the highest in Rubenis et al33 (93.6). These scores indicate the varying degrees to which environmental factors impact the lives of individuals with substance use disorders.
Worsening factors or predictors of lower quality of life were identified across the studies. Factors such as young age, low education, and race (African American) were found to be negatively associated with quality of life in Tracy et al27 and Brown et al.29 Unemployment, criminal history, and HIV status were highlighted in Wang et al28 and Yen et al30 as contributing to lower scores. Female gender was a consistent factor in lower quality of life scores in studies by Mitchell et al,31 Byrne et al,32 and Rubenis et al.33 Furthermore, mental health issues such as depression, anxiety, and ADHD were linked to lower quality of life in various studies, emphasizing the complex interplay between mental health and substance use disorders.
Discussion
The current systematic review evaluating the quality-of-life dimensions in individuals with substance use disorder, based on the WHOQOL framework, encompassed a diverse range of studies that included various patient populations, demographics, and substance use patterns. The patient populations across the studies were quite heterogeneous, with ages ranging from young adults to the elderly, varying gender proportions, and participants with different mental health disorders, criminal histories, and drug use behaviors. Substance use patterns across the studies also varied significantly, with some studies focusing on users of specific substances such as amphetamines, opioids, or benzodiazepines, while others investigated a broader range of substances, including cocaine, alcohol, marijuana, heroin, and ketamine. Several studies reported high prevalence rates of mental disorders among the participants, highlighting the potential relationship between SUD and mental health issues. Other specific characteristics noted in the studies were criminal history, long-term injecting drug use, sleep problems, and the presence of ADHD, teeth decay, or other mental disorders.
The WHOQOL-100 and WHOQOL-BREF are highly correlated, with the BREF version being a valid and reliable alternative to the lengthier WHOQOL-100. This was demonstrated in a study where both version sensitivity to change was tested in patients before and after liver transplantation. The study found that quality of life domains on both measures were highly correlated and sensitive to change following transplant.
Overall, the physical and psychological domains were the most affected, with patients reporting poor health, pain, discomfort, anxiety, depression, and lack of energy. The social and environmental domains were also affected, with patients reporting poor relationships, lack of social support, financial problems, and poor living conditions. The findings also showed that QOL was affected differently depending on the substance abused. For example, patients who abused cocaine or heroin had lower QOL scores than those who abused alcohol or marijuana. Patients who had a history of criminal behavior or who had been injecting drugs for more than ten years also had lower QOL scores.
The current study identified significantly lower WHOQOL domain scores among patients affected by substance abuse compared to the average scores previously identified in the general healthy population. For example, in other studies, the World Health Organization Quality of Life (WHOQOL) assessment tool, specifically the abbreviated version (WHOQOL-BREF), has been employed extensively in various populations to establish normative mean scores. Hawthorne et al41 conducted a study utilizing a random sample of adults from the Australian population, which yielded the following domain mean scores and standard deviations: Physical Health Domain mean of 73.5, Psychological Health Domain mean of 70.6, Social Relationships Domain mean score of 71.5, and Environmental Domain mean of 75.1, which are significantly higher compared with the average scores identified among SUD individuals in this systematic review. Nevertheless, this study provided critical insight into the QOL in the context of the Australian population, which can have particularities not attributable everywhere around the world.
Similarly, Noerholm et al42 investigated the QOL of the adult population in Denmark, utilizing the WHOQOL-BREF instrument. The findings from this study revealed the following domain mean scores and standard deviations: Physical Health Domain scoring a mean of 77; Psychological Health Domain with an average of 69; Social Relationships Domain with the same score 69; and the Environmental Domain averaging 74. These findings offer a valuable understanding of the QOL within the Danish population, that can facilitate cross-cultural comparisons with the data from other developed countries, and have a better representation of the average scores within the European population. Both studies contribute significantly to the literature on QOL by providing the baseline scores for the general population regarding the WHOQOL-BREF domains, which can be used for comparative purposes in future research. Establishing these normative values enables researchers and clinicians to better interpret the outcomes of the WHOQOL-BREF assessment tool within the context of the adult population, ultimately enhancing the efficacy of healthcare interventions and contributing to the improvement of public health outcomes.
In terms of sociodemographic determinants, a negative correlation between older age and physical QOL is consistent with previous research.29,33 The decline in physical health weakened immune systems, and increased risk of mental disorders in older age may account for these findings. Furthermore, homeless individuals with SUD were found to have a lower environmental QOL. Several factors that are associated with homelessness, such as pedal edema, abrasions, cuts, and rashes,43 are negatively impacting the comfort and QOL. Similarly, individuals with mental disorders are more susceptible to such physical health complications.44 Limited medical resources for homeless individuals and high basic needs that may hinder seeking mental health support contribute to this disparity.45 Studies have also identified a connection between enhanced mental health QOL and perceived social networks among SUD patients. Social support and stable relationships reportedly foster mental health QOL, potentially mitigating adverse QOL outcomes for SUD patients.46,47
Regarding clinical variables, an inverse relationship was observed between patients with mental disorders and their physical, mental health, and environmental QOL. Past-year prevalence rates for comorbid mental disorders ranged from 30–50% for mood disorders and 10–20% for anxiety disorders.48 A six-year cohort study and other research reported high, persistent comorbidity rates among SUD patients. Individuals with comorbid diagnoses often face limited access to essential mental health interventions, partly due to insufficient psychiatric training for physicians, inadequate collaboration among medical and mental health professionals, and underdiagnosis of comorbidities. Mental health diagnoses and psychopharmacological interventions are related to biopsychological QOL, “underscoring the importance of addressing SUD patient” mental health.49
Poor QOL is associated with severe SUD, which may serve as a predictor of treatment readiness. Research suggests that patients are more motivated to reduce the negative impacts of SUD on their QOL than to decrease substance use.50 A possible explanation for the negative relationship between severe SUD and mental health and environmental QOL is that these patients may be polysubstance users and inject drugs. Besides injectable drugs, alcohol abuse can also significantly impact the QOL. The inverse association between alcohol use disorders and good physical QOL is supported by prior studies that reported negative correlations between high alcohol use or chronic drinking and overall QOL levels.51 Alcohol use disorders can lead to social dysfunction, disrupt familial relationships, and provoke high-risk behaviors that may be influenced by difficulties in interpersonal interactions and financial management, which can be both a cause and consequence of alcohol abuse.52 It is important to recognize the complex and bidirectional nature of these relationships when considering the impact of alcohol use disorders on QOL.
The negative correlation between patients with cocaine use disorders and good mental health QOL can be attributed to the severity of cocaine dependence. A study investigating young, untreated regular cocaine users reported a decline in QOL associated with increased cocaine dependence severity.53 Cocaine use disorders are linked to substantial biopsychosocial challenges, resulting in reduced pharmacotherapy treatment outcomes. Some SUD patients may resort to cocaine use to alleviate withdrawal symptoms. The significant association between social QOL and trauma symptoms among SUD patients suggests that trauma symptoms have a more profound impact on social QOL. Prior research has emphasized the need for trauma-centered interventions for this population54 and comprehensive healthcare services to address both trauma symptoms and SUD.
While our systematic review found that there are some differences in QOL dimensions between different drugs, further research with larger samples and more controlled studies is needed to draw definitive conclusions and acknowledge the fact that the majority of drug users were identified as polydrug users. For instance, the study by Wang et al37 which exclusively enrolled methamphetamine users, reported lower QOL scores in all domains compared to Byrne’s study,32 which involved benzodiazepine users. Additionally, Mitchell’s study31 focused on African American heroin users and reported the highest mental domain score on the WHOQOL questionnaire. These findings suggest that there may be differences in QOL dimensions among those who use different drugs, but more research is needed to confirm these observations and control for confounding factors. The diversity of the patient populations, demographics, and substance use patterns in the included studies demonstrates the complexity and variability of substance abuse and its impact on quality of life.
Other recent systematic reviews and longitudinal studies have shed new light on the quality of life among patients with substance use disorders SUD, although the object of their study was not analyzed through the WHOQOL questionnaire. In 2022, a study encompassing a wide range of research highlighted several factors influencing QOL in SUD patients. This extensive analysis revealed that older age was associated with poorer physical QOL, while homeless individuals with SUD exhibited lower environmental QoL.55 Additionally, the study found that robust social support networks played a crucial role in enhancing mental health QOL.56 Another significant study published in 2023 examined HRQOL in SUD outpatients over 6 months, and reported initial low HRQOL scores, with a notable improvement observed in the first three months, especially in the mental health domain. Factors such as employment status, absence of comorbidities, and mental health were pivotal in these improvements. These findings collectively emphasize the multifaceted nature of QOL in SUD patients and the need for considering a range of sociodemographic and clinical factors in treatment and support strategies.
Although it is difficult to draw definitive conclusions from the systematic review due to the heterogeneity of the studies, it is evident that substance abuse affects a wide range of individuals with different backgrounds and life circumstances. Further research focusing on more specific patient populations and substance use patterns could provide valuable insights into the unique needs and challenges faced by different groups affected by substance abuse, ultimately informing more targeted and effective interventions and support services.
Our systematic review had several limitations that must be taken into consideration when interpreting the findings. First, the literature search was restricted to articles published in English, which might have led to the omission of relevant studies published in other languages. Second, the included studies demonstrated broad variability in terms of patient demographics, comorbidities, and patterns of substance use, and it is unclear whether the QOL is mainly associated with SUD or with other diagnoses of patients. Also, the proportion of female participants was not consistent across the studies, which might also affect the overall applicability of our findings. Moreover, one of our primary objectives was to determine if there were differences in QOL dimensions between different drugs. However, this goal may not have been adequately addressed due to the limited number of studies focusing on specific categories of drugs. Another limitation relates to the measurement of QOL dimensions considering the inconsistency in the QOL assessment since the included studies used both WHOQOL and WHOQOL-BREF questionnaires. However, including other instruments might have led to even greater inconsistency, given that different surveys assess different domains. Lastly, another significant limitation was the lack of comparison of QOL levels between SUD patients and other populations in the included studies. Despite these limitations, our systematic review offers valuable insights into the impact of substance use disorders on various aspects of QOL and provides an impetus for further research to fill the identified gaps in the literature.
Conclusion
The systematic review reveals a broad spectrum of QOL scores across physical, mental, social, and environmental domains in individuals with SUD. Notably, lower QOL scores were more prevalent among female patients, and those with mental disorders and injection drug users. However, it is important to acknowledge the limitations of this study, such as potential biases in self-reported data and the variability in QOL assessments by geographical, political, and population-wise factors. The findings, while suggesting a complex interplay between SUD, mental health, and QOL, should be considered preliminary. They emphasize the need for targeted interventions and highlight the role of demographic, clinical, and substance use factors in QOL. Future research, especially longitudinal studies, is essential to establish causal relationships and develop effective strategies for enhancing the well-being of individuals with SUD.
Acknowledgments
Disclosure
The authors report no conflicts of interest in this work.
References
1. McLellan AT. Substance misuse and substance use disorders: why do they matter in healthcare? Trans Am Clin Climatol Assoc. 2017;128:112–130.
2. Lo TW, Yeung JWK, Tam CHL. Substance abuse and public health: a multilevel perspective and multiple responses. Int J Environ Res Public Health. 2020;17(7):2610. doi:10.3390/ijerph17072610
3. Moonajilin MS, Kamal MKI, Mamun FA, et al. Substance use behavior and its lifestyle-related risk factors in Bangladeshi high school-going adolescents: an exploratory study. PLoS One. 2021;16(7):e0254926. doi:10.1371/journal.pone.0254926
4. Blanco C, Wiley TRA, Lloyd JJ, Lopez MF, Volkow ND. America’s opioid crisis: the need for an integrated public health approach. Transl Psychiatry. 2020;10(1):167. doi:10.1038/s41398-020-0847-1
5. Sullivan PS, Bradley HM, Rio CD, Rosenberg ES. The geography of opioid use disorder: a data triangulation approach. Infect Dis Clin North Am. 2020;34(3):451–464. doi:10.1016/j.idc.2020.06.006
6. Birkeland B, Foster K, Selbekk AS, et al. The quality of life when a partner has substance use problems: a scoping review. Health Qual Life Outcomes. 2018;16(1):219. doi:10.1186/s12955-018-1042-4
7. Kim YJ, Qian L, Aslam MS. The impact of substance use disorder on the mental health among COVID-19 patients: a protocol for systematic review and meta-analysis. Medicine. 2020;99(46):e23203. doi:10.1097/MD.0000000000023203
8. World Health Organization. The World Health Organization Quality of Life assessment (WHOQOL): position paper from the World Health Organization. Soc sci med. 1995;41(10):1403–1409. doi:10.1016/0277-9536(95)00112-K
9. Johannessen DA, Nordfjærn T, Geirdal AØ. Change in psychosocial factors connected to coping after inpatient treatment for substance use disorder: a systematic review. Subst Abuse Treat Prev Policy. 2019;14(1):16. doi:10.1186/s13011-019-0210-9
10. Zubaran C, Foresti K. Quality of life and substance use: concepts and recent tendencies. Curr Opin Psychiatry. 2009;22(3):281–286. doi:10.1097/YCO.0b013e328328d154
11. Armoon B, Fleury MJ, Bayat AH, et al. Quality of life and its correlated factors among patients with substance use disorders: a systematic review and meta-analysis. Arch Public Health. 2022;80(1):179. doi:10.1186/s13690-022-00940-0
12. Lee SB, Chung S, Seo JS, Jung WM, Park IH. Socioeconomic resources and quality of life in alcohol use disorder patients: the mediating effects of social support and depression. Subst Abuse Treat Prev Policy. 2020;15(1):13. doi:10.1186/s13011-020-00258-6
13. Laudet AB. The case for considering quality of life in addiction research and clinical practice. Addict Sci Clin Pract. 2011;6(1):44–55. doi:10.1136/bmj.b2495.
14. Aas CF, Vold JH, Skurtveit S, et al. Health-related quality of life of long-term patients receiving opioid agonist therapy: a nested prospective cohort study in Norway. Subst Abuse Treat Prev Policy. 2020;15(1):68. doi:10.1186/s13011-020-00309-y
15. Chacon NC, Walia N, Allen A, et al. Substance use during COVID-19 pandemic: impact on the underserved communities. Discoveries. 2021;9(4):e141. doi:10.15190/d.2021.20
16. Pan Z, Zhang J, Cheng H, et al. Trends of the incidence of drug use disorders from 1990 to 2017: an analysis based on the Global Burden of Disease 2017 data. Epidemiol Psychiatr Sci. 2020;29:e148. doi:10.1017/S2045796020000657
17. Skevington SM, Lotfy M, O’Connell KA, et al. The World Health Organization’s WHOQOL-BREF quality of life assessment: psychometric properties and results of the international field trial. A report from the WHOQOL group. Qual Life Res. 2004;13(2):299–310. doi:10.1023/B:QURE.0000018486.91360.00
18. Wong FY, Yang L, Yuen JWM, Chang KKP, Wong FKY. Assessing quality of life using WHOQOL-BREF: a cross-sectional study on the association between quality of life and neighborhood environmental satisfaction, and the mediating effect of health-related behaviors. BMC Public Health. 2018;18(1):1113. doi:10.1186/s12889-018-5942-3
19. WHOQOL GROUP T; World Health Organization. Development of the World Health Organization WHOQOL-BREF Quality of Life Assessment. Psychological Medicine. 1998;28(3):551–558. doi:10.1017/S0033291798006667
20. Dhammi IK, Kumar S. Medical subject headings (MeSH) terms. Indian J Orthop. 2014;48(5):443–444. doi:10.4103/0019-5413.139827
21. Moher D, Liberati A, Tetzlaff J, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097. doi:10.1371/journal.pmed.1000097
22. Schiavo JH. PROSPERO: an International Register of Systematic Review Protocols. Medical Reference Services Quarterly. 2019;38(2):171–180. doi:10.1080/02763869.2019.1588072
23. Foster ED, Deardorff A. Open Science Framework (OSF). J Med Libr Assoc. 2017;105(2):203–206. doi:10.5195/jmla.2017.88
24. O’Carroll RE, Smith K, Couston M, Cossar JA, Hayes PC. A comparison of the WHOQOL-100 and the WHOQOL-BREF in detecting change in quality of life following liver transplantation. Qual Life Res. 2000;9(1):121–124. doi:10.1023/A:1008901320492
25. Jahan AR, Burgess DM. Substance Use Disorder. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2022.
26. Farrah K, Young K, Tunis MC, Zhao L. Risk of bias tools in systematic reviews of health interventions: an analysis of PROSPERO-registered protocols. Syst Rev. 2019;8(1):280. doi:10.1186/s13643-019-1172-8
27. Tracy EM, Laudet AB, Min MO, et al. Prospective patterns and correlates of quality of life among women in substance abuse treatment. Drug Alcohol Depend. 2012;124(3):242–249. doi:10.1016/j.drugalcdep.2012.01.010
28. Wang PW, Wu H-C, Yen C-N, et al. Change in quality of life and its predictors in heroin users receiving methadone maintenance treatment in Taiwan: an 18-month follow-up study. Am J Drug Alcohol Abuse. 2012;38(3):213–219. doi:10.3109/00952990.2011.649222
29. Brown S, Jun MK, Min MO, et al. Impact of dual disorders, trauma, and social support on quality of life among women in treatment for substance dependence. J Dual Diagn. 2013;9(1):61–71. doi:10.1080/15504263.2012.750147
30. Yen YF, Chou P, Lin Y-S, et al. Factors associated with health-related quality of life among injection drug users at methadone clinics in Taipei, Taiwan. J Chin Med Assoc. 2015;78(5):292–298. doi:10.1016/j.jcma.2015.01.001
31. Mitchell SG, Gryczynski J, Schwartz RP, et al. Changes in quality of life following buprenorphine treatment: relationship with treatment retention and illicit opioid use. J Psychoactive Drugs. 2015;47(2):149–157. doi:10.1080/02791072.2015.1014948
32. Byrne P, Ducray K, Smyth BP, et al. The impact of sex upon needs and quality of life within a population on methadone treatment. J Addict Med. 2016;10(1):60–67. doi:10.1097/ADM.0000000000000187
33. Rubenis AJ, Fitzpatrick RE, Lubman DI, et al. Impulsivity predicts poorer improvement in quality of life during early treatment for people with methamphetamine dependence. Addiction. 2018;113(4):668–676. doi:10.1111/add.14058
34. Manning V, Garfield JBB, Lam T, et al. Improved quality of life following addiction treatment is associated with reductions in substance use. J Clin Med. 2019;8(9):1407. doi:10.3390/jcm8091407
35. Muller AE, Skurtveit S, Clausen T. Performance of the WHOQOL-BREF among Norwegian substance use disorder patients. BMC Med Res Methodol. 2019;19(1):44. doi:10.1186/s12874-019-0690-3
36. Flores-García L, Lensing MB, Ytterstad E, et al. Quality of life in substance use disorder patients with and without attention deficit hyperactivity disorder 12 months after treatment: a naturalistic follow-up study. ADHD Atten Def Hyp Disord. 2019;11(3):299–310. doi:10.1007/s12402-019-00297-5
37. Wang Y, Zuo J, Hao W, et al. Quality of life in patients with methamphetamine use disorder: relationship to impulsivity and drug use Characteristics. Front Psychiatry. 2020;11:579302. doi:10.3389/fpsyt.2020.579302
38. Yamada C, Tsutsumi A, Izutsu T, et al. Quality of life among people who use drugs living in poor urban communities in the Philippines. Int J Drug Policy. 2021;93:103160. doi:10.1016/j.drugpo.2021.103160
39. Tun S, Balasingam V, Singh DS, El-Khoury J. Factors associated with quality of life (QOL) scores among methadone patients in Myanmar. PLOS Glob Public Health. 2022;2(8):e0000469. doi:10.1371/journal.pgph.0000469
40. Saffari M, Chen H-P, Chang C-W, et al. Effects of sleep quality on the association between problematic internet use and quality of life in people with substance use disorder. BJPsych Open. 2022;8(5):E155. doi:10.1192/bjo.2022.557
41. Morales-Manrique CC, Tomás-Dols S, Zarza-González M, Vidal-Infer A, Alvarez FJ, Valderrama-Zurián JC. Comparative study of the perceived quality of life of patients in treatment for cocaine and heroin dependence in Spain: differences by gender and time in treatment. Subst Use Misuse. 2014;49(10):1353–1358. doi:10.3109/10826084.2014.880482
42. Moreira Tde C, Figueiró LR, Fernandes S, et al. Quality of life of users of psychoactive substances, relatives, and non-users assessed using the WHOQOL-BREF. Cien Saude Colet. 2013;18(7):1953–1962. doi:10.1590/s1413-81232013000700010
43. Marques TCN, Sarracini KLM, Cortellazzi KL, et al. The impact of oral health conditions, socioeconomic status and use of specific substances on quality of life of addicted persons. BMC Oral Health. 2015;15(38). doi:10.1186/s12903-015-0016-8
44. Paiva CB, Ferreira IB, Bosa VL, Narvaez JC. Depression, anxiety, hopelessness and quality of life in users of cocaine/crack in outpatient treatment. Trends Psychiatry Psychother. 2017;39(1):34–42. PMID: 28403321. doi:10.1590/2237-6089-2015-0065
45. Singh S, Kumar S, Sarkar S, Balhara YPS. Quality of life and its relationship with perceived stigma among opioid use disorder patients: an exploratory study. Indian J Psychol Med. 2018;40(6):556–561. doi:10.4103/IJPSYM.IJPSYM_171_18
46. Hawthorne G, Herrman H, Murphy B. Interpreting the WHOQOL-Bref: preliminary population norms and effect sizes. Social Indicators Res. 2006;77:37–59.
47. Noerholm V, Groenvold M, Watt T, Bjorner JB, Rasmussen NA, Bech P. Quality of life in the Danish general population-normative data and validity ofWHOQOL-BREF using Rasch and item response theory models. Qual Life Res. 2004;13(2):531–540. doi:10.1023/B:QURE.0000018485.05372.d6
48. Edidin JP, Ganim Z, Hunter SJ, et al. The mental and physical health of homeless youth: a literature review. Child Psychiatry Hum Dev. 2012;43(3):354–375. doi:10.1007/s10578-011-0270-1
49. McCloughen A, Foster K, Huws‐Thomas M, et al. Physical health and well-being of emerging and young adults with mental illness: an integrative review of international literature. Int J Ment Health Nurs. 2012;21(3):274–288. doi:10.1111/j.1447-0349.2011.00796.x
50. Fleury MJ, Grenier G, Cao Z, et al. Typology of currently or formerly homeless individuals based on their use of health and social services. Community Ment Health J. 2021;57(5):948–959. doi:10.1007/s10597-020-00693-6
51. Birkeland B, Weimand B, Ruud T, et al. Perceived family cohesion, social support, and quality of life in patients undergoing treatment for substance use disorders compared with patients with mental and physical disorders. Addict Sci Clin Pract. 2021;16(1):44. doi:10.1186/s13722-021-00252-8
52. Rathinam B, Ezhumalai S. Perceived social support among abstinent individuals with substance use disorder. J Psychosoc Rehabil Ment Health. 2022;9(1):81–87. doi:10.1007/s40737-021-00237-5
53. Reissner V, Kokkevi A, Schifano F, et al. Differences in drug consumption, comorbidity and health service use of opioid addicts across six European urban regions (TREAT-project). Eur Psychiatry. 2012;27(6):455–462. doi:10.1016/j.eurpsy.2010.10.001
54. Lin CY, Chang KC, Wang J-D, et al. Quality of life and its determinants for heroin addicts receiving a methadone maintenance program: comparison with matched referents from the general population. J Formos Med Assoc. 2016;115(9):714–727. doi:10.1016/j.jfma.2015.07.007
55. De Maeyer J, Vanderplasschen W, Lammertyn J, et al. Current quality of life and its determinants among opiate-dependent individuals five years after starting methadone treatment. Qual Life Res. 2011;20(1):139–150. doi:10.1007/s11136-010-9732-3
56. Lee SB, Chung S, Seo JS, et al. Socioeconomic resources and quality of life in alcohol use disorder patients: the mediating effects of social support and depression. Subst Abuse Treat Prev Policy. 2020;15(1):1–8.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.