Back to Journals » Risk Management and Healthcare Policy » Volume 13
Evaluating Surgical Risk Using FMEA and MULTIMOORA Methods under a Single-Valued Trapezoidal Neutrosophic Environment
Authors Cheng PF ![]() , Li DP, He JQ
, Li DP, He JQ ![]() , Zhou XH, Wang JQ, Zhang HY
, Zhou XH, Wang JQ, Zhang HY
Received 22 December 2019
Accepted for publication 23 June 2020
Published 23 July 2020 Volume 2020:13 Pages 865—881
DOI https://doi.org/10.2147/RMHP.S243331
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Kent Rondeau
Peng-Fei Cheng,1,2 Dan-Ping Li,1,* Ji-Qun He,3,4,* Xiang-Hong Zhou,1,2 Jian-Qiang Wang,2,5 Hong-Yu Zhang2,5
1School of Business, Hunan University of Science and Technology, Xiangtan 411201, People’s Republic of China; 2Hunan Engineering Research Center of Intelligent Decision Making and Big Data on Industrial Development, Xiangtan 411201, People’s Republic of China; 3Xiangya Hospital, Central South University, Changsha 410008, People’s Republic of China; 4Xiangya Nursing School, Central South University, Changsha 410011, People’s Republic of China; 5School of Business, Central South University, Changsha 410083, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ji-Qun He
Xiangya Hospital, Central South University, Changsha, People’s Republic of China
Email [email protected]
Background: Human errors during operations may seriously threaten patient recovery and safety and affect the doctor–patient relationship. Therefore, risk evaluation of the surgical process is critical. Risk evaluation by failure mode and effect analysis (FMEA) is a prospective technology that can identify and evaluate potential failure modes in the surgical process to ensure surgical quality and patient safety. In this study, a hybrid surgical risk–evaluation model was proposed using FMEA and multiobjective optimization on the basis of ratio analysis plus full multiplicative form (MULTIMOORA) method under a single-valued trapezoidal neutrosophic environment. This work aimed to determine the most critical risk points during the surgical process and analyze corresponding solutions.
Methods: A team for FMEA was established from domain experts from different departments in a hospital in Hunan Province. Single-valued trapezoidal neutrosophic numbers (SVTNNs) were used to evaluate potential risk factors in the surgical process. Cmprehensive weights combining subjective and objective weights were determined by the best–worst method and entropy method to differentiate the importance of risk factors. The SVTNN–MULTIMOORA method was utilized to calculate the risk-priority order of failure modes in a surgical process.
Results: The hybrid FMEA model under the SVTNN–MULTIMOORA method was used to calculate the ranking of severity of 21 failure modes in the surgical process. An unclear diagnosis is the most critical failure in the surgical process of a hospital in Hunan Province.
Conclusion: The proposed model can identify and evaluate the most critical potential failure modes of the surgical process effectively. In addition, such a model can help hospitals to reduce surgical risk and improve the safety of surgery.
Keywords: failure mode and effect analysis, surgical process, MULTIMOORA, best–worst method, single-valued trapezoidal neutrosophic numbers
Introduction
Surgical operations are a key health-care service and an important means to cure patients effectively.1 In general, surgery comprises a series of processes, such as diagnosis, preoperative preparation, surgical operation, and postoperative care. However, any surgical procedure has risks,2 and various human errors, such as diagnosis and clinical errors, may occur during operation. Certain human errors may be unharmful to a patient, whereas other errors may lead to serious results or death.3 Ensuring surgical safety by risk assessment and reduction during the operation is crucial for surgeons and patients.4–6 Therefore, an effective risk-evaluation method should be determined to identify the most critical risks in the surgical process, and measures must be taken to reduce surgical risk.
Failure mode and effect analysis (FMEA) was initially adopted to assess complex processes in the aerospace industry to identify possible causes of damage and determine remedial measures.7 FMEA is an available and effective instrument for identifying and evaluating potential or critical failures in a system. This analysis helps in developing risk-management strategies,8 such as supplier selection9 and yacht-system design.10 FMEA is also used in medical fields to evaluate critical failures, such as surgical cancelation factors11 and hazards in surgical wards12 and health-care management,13,14 and to take remedial measures before substantial damage or failure occurs, in order to improve patient safety.15 Traditional FMEA assesses and prioritizes the risk of failure modes on the basis of the risk-priority number (RPN). RPNs can be computed by multiplying occurrence (O), severity (S) and detection (D) (RPN=O×S×D).16 However, restricted to its practical application, FMEA has numerous shortcomings.17–20 Risk factors in FMEA are estimated on the basis of their subjective quantification by the crisp number scale of 1–10. However, practical applications involve vague and uncertain information that cannot be described by quantified crisp numbers accurately. In the classical FMEA, risk factors O, S, and D are assumed to be equally important and discrepancies in relative weights among risk factors neglected, which is unreasonable in real life. Obtaining the risk-priority ranking by RPNs remains controversial.
Numerous researchers have incorporated the fuzzy theory into FMEA to express the vague and uncertain information in risk evaluation accurately.21–23 In practical applications, risk-evaluation information is expressed in linguistic terms of a fuzzy set (FS),24 such as triangular fuzzy numbers,25 trapezoidal fuzzy numbers,26,27 intuitionistic fuzzy numbers,28,29 and interval-valued intuitionistic fuzzy numbers.30 As the extension of traditional FSs31 and intuitionistic FSs,32 single-valued trapezoidal neutrosophic fuzzy sets (SVTNFSs) can express additional uncertain information. Given the complexity of the surgical environment, various experiences and expertise of experts, the assessment information provided by experts is usually uncertain and vague. The evaluation information provided by experts in a limited time may be neutral, uncertain or inconsistent because their knowledge, attention or information processing capacities are distinctive.33 Using SVTN numbers (SVTNNs) to express risk-evaluation information for the surgical process is suitable, because SVTNFSs can effectively describe uncertain and inconsistent information.34–36
Several researchers have emphasized the importance of risk factors in risk ranking of failure modes to consider discrepancies in risk factors in FMEA.18 By contrast, FMEA is modified by calculating the weights of risk factors in different ways.37,38 The analytic hierarchy process is commonly used to determine the subjective weight.39,40 A new method for calculating subjective weight, ie, the best–worst method (BWM), has been examined by Rezaei.41 Compared with the analytic hierarchy–process method, the BWM can provide more consistent comparisons and requires less information and computation.42–44 Moreover, numerous studies have determined the comprehensive weights of risk factors by integrating subjective and objective weights.45 In the FMEA case, objective weights of risk factors can be determined by a powerful multicriteria decision-making (MCDM) technique, ie, the entropy method.46 Therefore, on the basis of the aforementioned discussion, the comprehensive weights of risk factors were obtained by the BWM and entropy method in this study.
Multiple risk factors should be considered, given the difficulty and complexity of defining the risk of potential failure modes by FMEA team members. Determining the risk priority of failure modes can be considered an MCDM problem.42 Numerous MCDM techniques have been adopted to resolve risk-priority ranking. Examples of such techniques include visekriterijumska optimizacija I kompromisno resenje (VIKOR), preference-ranking organization methods for enrichment evaluations, and technique for order preference by similarity to ideal solution (TOPSIS).37,42,47,48 Multiobjective optimization on the basis of ratio analysis plus full multiplicative form (MULTIMOORA) method49,50 was derived from multiobjective optimization by ratio analysis (MOORA).51 MULTIMOORA determines ranking results on the basis of the three perspectives (ie, the ratio system, reference point, and full multiplicative form).52 This method can effectively solve multiobjective and MCDM problems. Compared with other methods, MULTIMOORA is simple, effective, and can easily compare and select alternatives.49,51,53,54 The MULTIMOORA method has been widely used in decision-making in such topics as climate,55 economies,56 and electronics,57 due to its flexibility, simplicity, and robustness.58,59 The risk-assessment environment of the surgical process is complex. Risk evaluation of the surgical process by FMEA not only has multiple criteria but also multiple objectives, including maximizing O and S while minimising D. As such, the MULTIMOORA method can be used to obtain the risk-priority ranking of the surgical process to simplify the evaluation and enhance the robustness of ranking results.
This study investigated an effective surgical risk–evaluation method using the FMEA and MULTIMOORA methods under the SVTN environment. The most critical failures during a surgical process in a hospital were systematically identified and evaluated to reduce surgical risk and ensure operational security, using a hospital in Hunan Province as an example. The extended MULTIMOORA method overcomes the drawbacks of traditional FMEA in evaluation information, differentiation in importance of risk factors, and priority of failure modes. This study included the following work to achieve the objectives mentioned previously. Firstly, the potential failure modes of surgical processes were listed, and the causes and potential effects of the listed failure modes were analyzed systematically. Secondly, given the complex surgical environment and the distinct experiences and expertise of experts, SVTNN was used to represent the uncertain or inconsistent linguistic evaluation of risk factors provided by experts. Thirdly, comprehensive weights were obtained by combining the BWM with the entropy method to distinguish importance weights and deal with the same importance of risk factors in the classical FMEA. Finally, an extended MULTIMOORA method was applied to obtain the risk priority of the identified failure modes in FMEA.
Methods
At a hospital (denoted “X”) in Hunan Province, potential risks in the surgical process were evaluated to improve the quality and safety of the operating room. A cross-functional team for FMEA was established from domain experts from different departments, including inpatient wards, operating rooms, and the anesthesiology department. The multidisciplinary FMEA team comprised a surgeon, the head nurse of the operating room, an anesthesiologist, and a deputy head nurse. The surgeon ( ) is a professor who has worked in the field for nearly 30 years. The head nurse of the operating room (
) is a professor who has worked in the field for nearly 30 years. The head nurse of the operating room ( ) is an associate professor who has worked in the field for 27 years. The anesthesiologist (
) is an associate professor who has worked in the field for 27 years. The anesthesiologist ( ) is an associate professor who has worked in the field for 20 years. The deputy head nurse (
) is an associate professor who has worked in the field for 20 years. The deputy head nurse ( ) is an associate professor who has worked in the field for 25 years. Given that the surgeon has a deep understanding of the harm caused by mistakes during an operation, he carried large weight in assessing the O, S, and D of surgical failure modes. Therefore, given the qualifications and distinct experience of the four experts, the weight vector was assigned and denoted
) is an associate professor who has worked in the field for 25 years. Given that the surgeon has a deep understanding of the harm caused by mistakes during an operation, he carried large weight in assessing the O, S, and D of surgical failure modes. Therefore, given the qualifications and distinct experience of the four experts, the weight vector was assigned and denoted  . All experts completed the questionnaire related to surgical risk assessment independently.
. All experts completed the questionnaire related to surgical risk assessment independently.
Potential failure modes and their causes and effects during operations in the hospital were listed on the basis of the literature and expert opinions. A questionnaire was sent to each expert to collect information related to the importance of each failure mode and the linguistic evaluation of risk factors O, S, and D. Then, a hybrid FMEA method using MULTIMOORA was used to determine the most likely contributors to severe surgical failure by the ranking of failure modes. The specific steps involved in such stages are described in the following sections. Figure 1 shows the flowchart of the proposed hybrid risk-evaluation model.
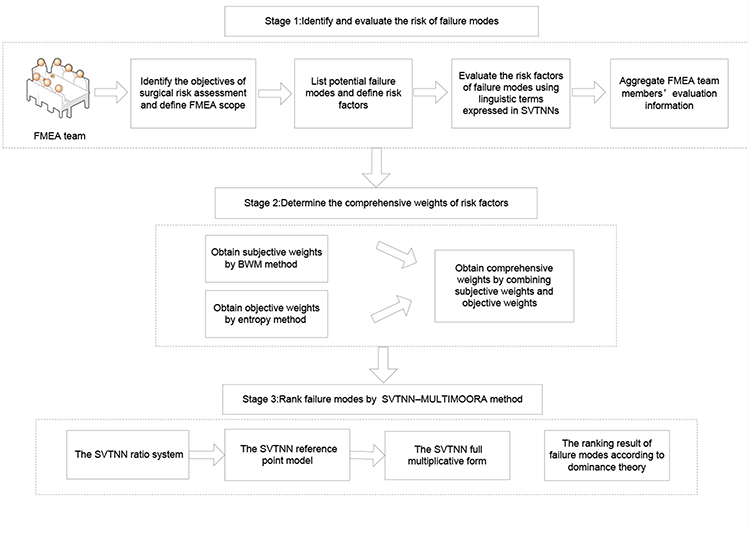 |
Figure 1 Flowchart of the proposed surgical risk evaluation model. |
Identifying and Evaluating Risk of Failure Modes
In general, surgery comprises a series of processes, ie, diagnosis, preoperative preparation, surgical operation, and postoperative care. Various risks may occur in each phase of the surgical process. Risk assessment subjective and FMEA scope should be determined to evaluate the risk of the surgical process.  potential failure modes
potential failure modes  with respect to
with respect to  risk factors
risk factors  in surgery should be evaluated by
in surgery should be evaluated by  cross-functional experts
cross-functional experts  in the FMEA team. The linguistic evaluation of risk factors provided by FMEA team members was transformed into SVTNNs, and the decision matrix was obtained. The specific steps are given as follows.
in the FMEA team. The linguistic evaluation of risk factors provided by FMEA team members was transformed into SVTNNs, and the decision matrix was obtained. The specific steps are given as follows.
Identifying and Listing Risk of Failure Modes
Based on previous studies, failures that may occur during operations include infection, adverse reactions to anesthetics and medicine used in surgical operations,2 laboratory-test errors, delayed diagnosis,4 improper scheduling, unrealistic operating rooms, insufficient medicine, insufficient required instruments and materials, insufficient staff, unavailable equipment, facility malfunctions, unavailable instruments and materials, incorrect sterilization,11 errors in disinfection, isolation of infection, vital signs, medication delivery, ward rounds, surgical-site marking, postoperative care,12,60–63 and missing information, nonexistent severity labels,64 improper transport of patients, poor intraoperative management of surgical tools, and poor surgical record-keeping.65 Figure 2 shows the hierarchical structure of the surgical process risk–analysis problem in accordance with the failures of the surgical process in previous studies and expert opinions of the FMEA team. Table 1 shows the failure modes and their relative failure causes and effects.
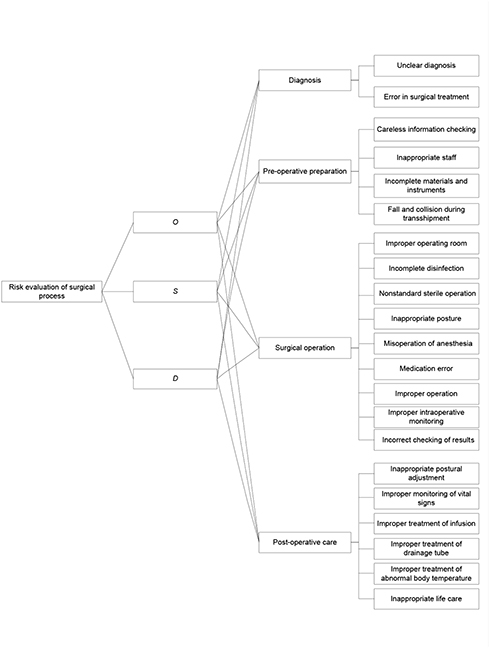 |
Figure 2 Hierarchical structure of surgical process risk analysis. |
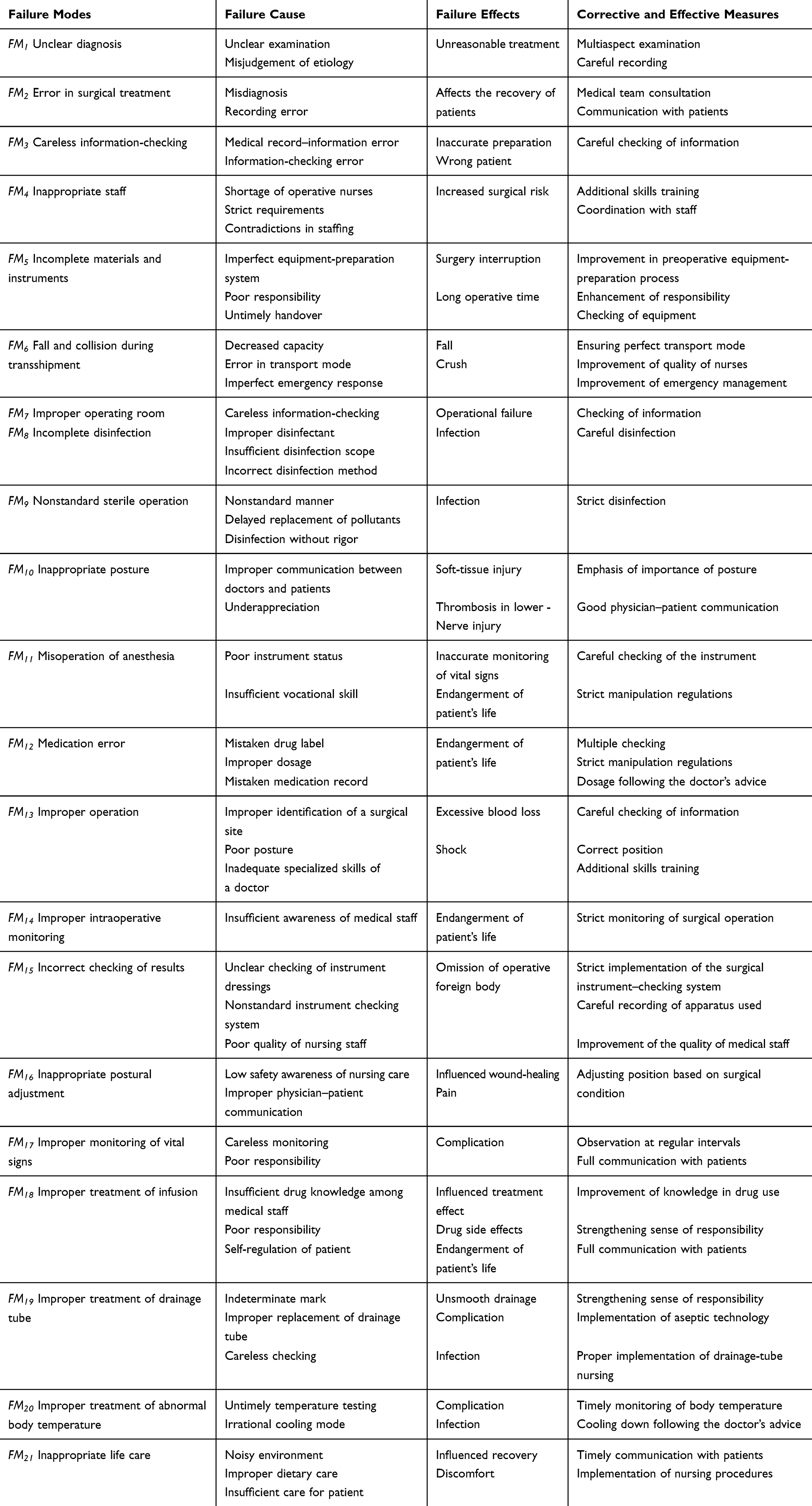 |
Table 1 FMEA of the Surgical Process |
Evaluating Risk Factors of Failure Modes
In the traditional FMEA method, risk values of failure modes are evaluated by crisp numbers, which are inadequate or insufficient for assessing risks in real life.30 FMEA team members tend to use linguistic terms to express evaluation information. SVTNNs can depict indeterminate and inconsistent information well.34,35 As such, the proposed model adopts linguistic variables expressed in SVTNNs to evaluate the ratings of failure modes with regard to various risk factors. The definitions of neutrosophic set66,67 and SVTNN68 are presented in Appendix A. Each FMEA team member ( ) should give their opinion on the basis of a seven-point scale. Linguistic variables can be represented by SVTNNs (Table 2). Individual evaluation matrices are characterized by
) should give their opinion on the basis of a seven-point scale. Linguistic variables can be represented by SVTNNs (Table 2). Individual evaluation matrices are characterized by  .
.
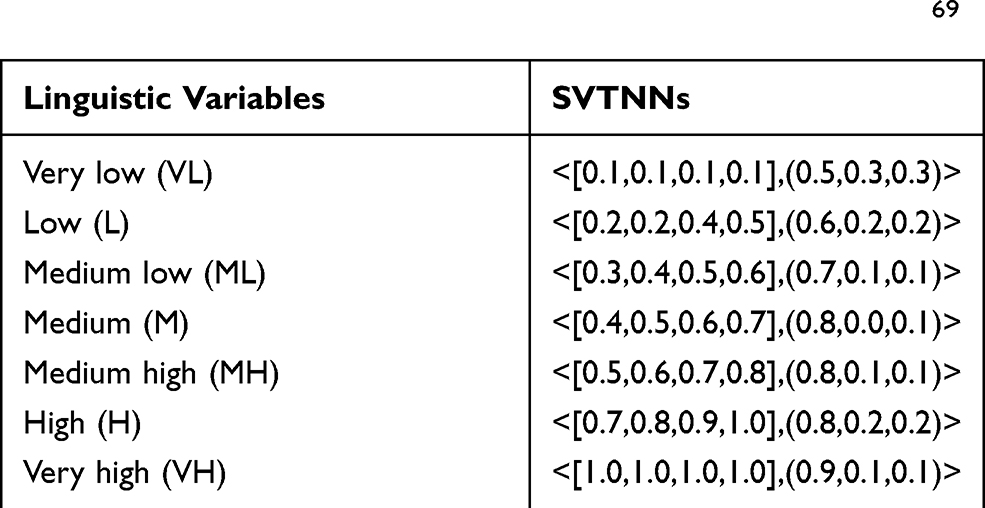 |
Table 2 Linguistic Variables of SVTNNs for Linguistic Terms69 |
From the SVTNN evaluation of risk factors provided by the FMEA team, the weight (1) vector of team members can be utilized to aggregate all individual evaluation matrices into the group-evaluation matrix
vector of team members can be utilized to aggregate all individual evaluation matrices into the group-evaluation matrix  .
.

Determining Comprehensive Weights of Risk Factors
Without weighting information for risk factors, traditional FMEA risk assessment may lead to an inaccurate risk ranking of failure modes. Therefore, weights of risk factors should be calculated to obtain an accurate risk ranking. Using a method proposed in a prior study,41 weighting information for risk factors from subjective and objective perspectives can be computed using the BWM and entropy method. Therefore, comprehensive weights can be determined.
Calculating Subjective Weights Using BWM
Step 1: Determine a set of decision criteria.
In this step, the criteria  is considered to obtain a decision.
is considered to obtain a decision.
Step 2: Determine the best (eg, most desirable, most important) and the worst (eg, least desirable, least important) criterion.
Step 3: Determine the preference of the best criterion over all other criteria using a number between 1 and 9. The resulting best-to-others vector would be  , where
, where  indicates the preference of the best criterion B over criterion j. Therefore,
indicates the preference of the best criterion B over criterion j. Therefore,  = 1.
= 1.
Step 4: Determine the preference of all criteria over the worst criterion by using a number between 1 and 9. The resulting others-to-worst vector would be  , where
, where  indicates the preference of the criterion j over the worst criterion W. Therefore,
indicates the preference of the criterion j over the worst criterion W. Therefore,  = 1.
= 1.
Step 5: Find the optimal weights  .
.
The optimal weight for the criteria is that which for each pair of  and
and  , we have
, we have  and
and  . A solution where the maximum absolute differences
. A solution where the maximum absolute differences  and
and  for all j are minimal should be sought to satisfy these conditions for all j. Given the nonnegativity and condition for the weights, the problem results are presented as:
for all j are minimal should be sought to satisfy these conditions for all j. Given the nonnegativity and condition for the weights, the problem results are presented as:




Equation 2 is equivalent to:




Solving Equation 2), the optimal weights  and ξ* are obtained.
and ξ* are obtained.
Then, the consistency ratio (CR) is calculated using ξ* and the corresponding consistency index:
(4)
Table 3 shows the maximum values of ξ (consistency index) for different values of  .
.
 |

If CR is ≤0.1, then the consistency is good and acceptable. Otherwise,  and
and  can be revised to achieve a consistent solution.
can be revised to achieve a consistent solution.
The BWM is limited in deriving a unique optimum weight vector when the number of criteria is more than three, which may lead to multiple optimal solutions. An improved method70 was used to obtain the optimal weights with n criteria. If  is used instead of
is used instead of  , then the problem can be solved:
, then the problem can be solved:




Equation 5 can be transferred to this linear programming problem:






Computing Objective Weights
The main idea of the entropy method is that if the information entropy of the index is small, then the amount of information provided is large and the weight high. Therefore, the weight-determination method was performed on the basis of entropy under an SVTNN environment:71
(7) (8)
Then, the entropy weight can be computed:
(9)
Obtaining Comprehensive Weights of Risk Factors
From the subjective and objective weight vectors derived from the above two steps, the synthetic weight of each risk factor was calculated:
(10)
where  (
( ) is the adjustment parameter.
) is the adjustment parameter.
Ranking of Failure Modes by SVTNN–MULTIMOORA
The classical MULTINOORA method consists of three parts: the ratio system, the reference-point model, and the full multiplicative form.30,54 It was extended into an SVTNN environment to rank failure modes in this study. The steps are:
Step 1: SVTNN ratio system.
The SVTNN group decision matrix  can be translated into the normalized decision matrix
can be translated into the normalized decision matrix  using the vector-normalization method:
using the vector-normalization method:



After standardization, the summarising ratio (12) of each failure mode was computed.Normalized ratios were added or subtracted to optimize
of each failure mode was computed.Normalized ratios were added or subtracted to optimize
where  stands for the number of risk factors to be minimized and
stands for the number of risk factors to be minimized and  the normalised assessment of the ith failure mode with respect to all risk factors. If the value of
the normalised assessment of the ith failure mode with respect to all risk factors. If the value of  is small, then the risk ranking is high.
is small, then the risk ranking is high.
Step 2: SVTNN reference-point model.
The SVTNN maximal objective reference point (SVTNN–MORP) vector (13) was found in accordance with the normalised SVTNN decision matrix
was found in accordance with the normalised SVTNN decision matrix  . In consideration of the SVTNNs, SVTNN–MORP was defined:
. In consideration of the SVTNNs, SVTNN–MORP was defined:

Then, the distance of each failure mode from the SVTNN-MORP can be calculated:
(14)
Therefore, the ranking orders of all failure modes can be determined in accordance with the deviation from the reference point and the min–max metric of Tchebycheff. If the value of  is large, then the risk ranking is high.
is large, then the risk ranking is high.
Step 3: SVTNN full multiplicative form.
The overall utility of the (15) th failure mode can be expressed as an SVTNN using the formula:
th failure mode can be expressed as an SVTNN using the formula:

where  denotes the product of factors of the
denotes the product of factors of the  th failure mode to be minimized, with
th failure mode to be minimized, with  being the number of factors to be minimized,
being the number of factors to be minimized,  denoting the product of factors of the
denoting the product of factors of the  th failure mode to be maximized, and n-g being the number of factors to be maximized. If the value of
th failure mode to be maximized, and n-g being the number of factors to be maximized. If the value of  is small, then the risk ranking is high.
is small, then the risk ranking is high.
Step 4: Determine the risk level of each failure mode.
On the basis of the three ranking lists derived from the previous steps of SVTNN–MULTIMOORA, the final ranking of all failure modes was obtained by utilizing the dominance theory (for more details, please refer to Brauers et al49).
Results
Evaluation of Risk Factors
The FMEA team members  in hospital X evaluated the ratings of failure modes for each risk factor using the linguistic variables described in Table 2. Then, the original evaluation information provided by the team members for these failure modes with respect to each risk factor was obtained (Table 1 in Appendix B). Table 2 shows that linguistic evaluations were converted into SVTNNs. Then, the SVTNWAA operator35 was utilized to aggregate the evaluation of the individual FMEA team members with the weight vector of the FMEA team members
in hospital X evaluated the ratings of failure modes for each risk factor using the linguistic variables described in Table 2. Then, the original evaluation information provided by the team members for these failure modes with respect to each risk factor was obtained (Table 1 in Appendix B). Table 2 shows that linguistic evaluations were converted into SVTNNs. Then, the SVTNWAA operator35 was utilized to aggregate the evaluation of the individual FMEA team members with the weight vector of the FMEA team members  . The group-evaluation matrix was obtained (Table 4).
. The group-evaluation matrix was obtained (Table 4).
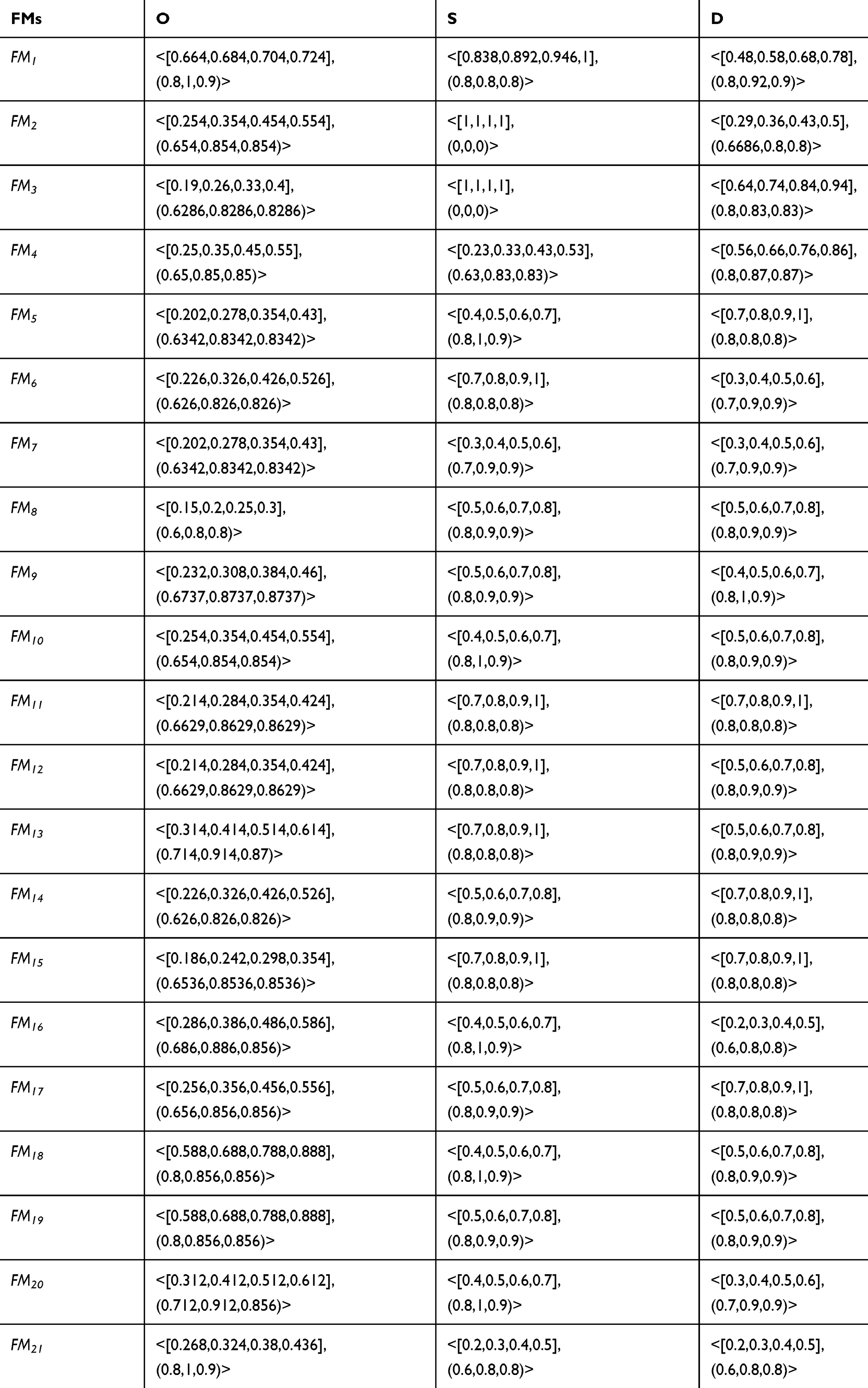 |
Table 4 Group-Evaluation Matrix |
Comprehensive Weight Information on Risk Factors
Rating vectors of the most and least important criteria were determined by FMEA team members in accordance with the BWM (Table 2 in Appendix B). Subjective weights provided by the team members were determined using Equation 6. Synthetic subjective weights of the risk factors were obtained by utilizing the weighted averaging operator with consideration of the importance weights of team members  . Table 5 shows the optimal weight and the CR of comparisons. The reliability of the BWM can be indicated by checking the consistency of pairwise comparisons.72 Table 5 shows that the CR values are close to 0, indicating the consistency of comparisons provided by team members. As such, the consistency results indicate the reliability of the subjective weights calculated from the BWM.
. Table 5 shows the optimal weight and the CR of comparisons. The reliability of the BWM can be indicated by checking the consistency of pairwise comparisons.72 Table 5 shows that the CR values are close to 0, indicating the consistency of comparisons provided by team members. As such, the consistency results indicate the reliability of the subjective weights calculated from the BWM.
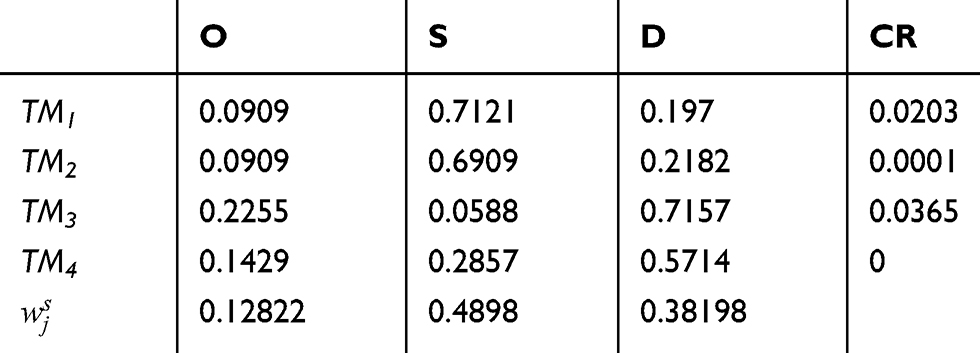 |
Table 5 Subjective Weights |
The objective weights of risk factors can be determined using Equation 7–Equation 9), as shown in
Table 6. Comprehensive weights of risk factors can be obtained using Equation 10 by combining the subjective and objective weights derived from the BWM and entropy method. Without losing the generality, we let  . Table 6 shows the comprehensive weights of risk factors.
. Table 6 shows the comprehensive weights of risk factors.
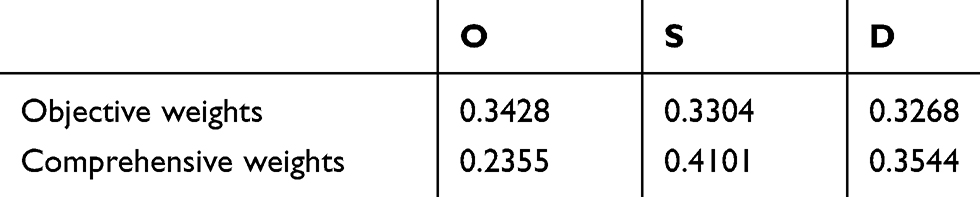 |
Table 6 Objective and Comprehensive Weights |
Ranking of Failure Modes
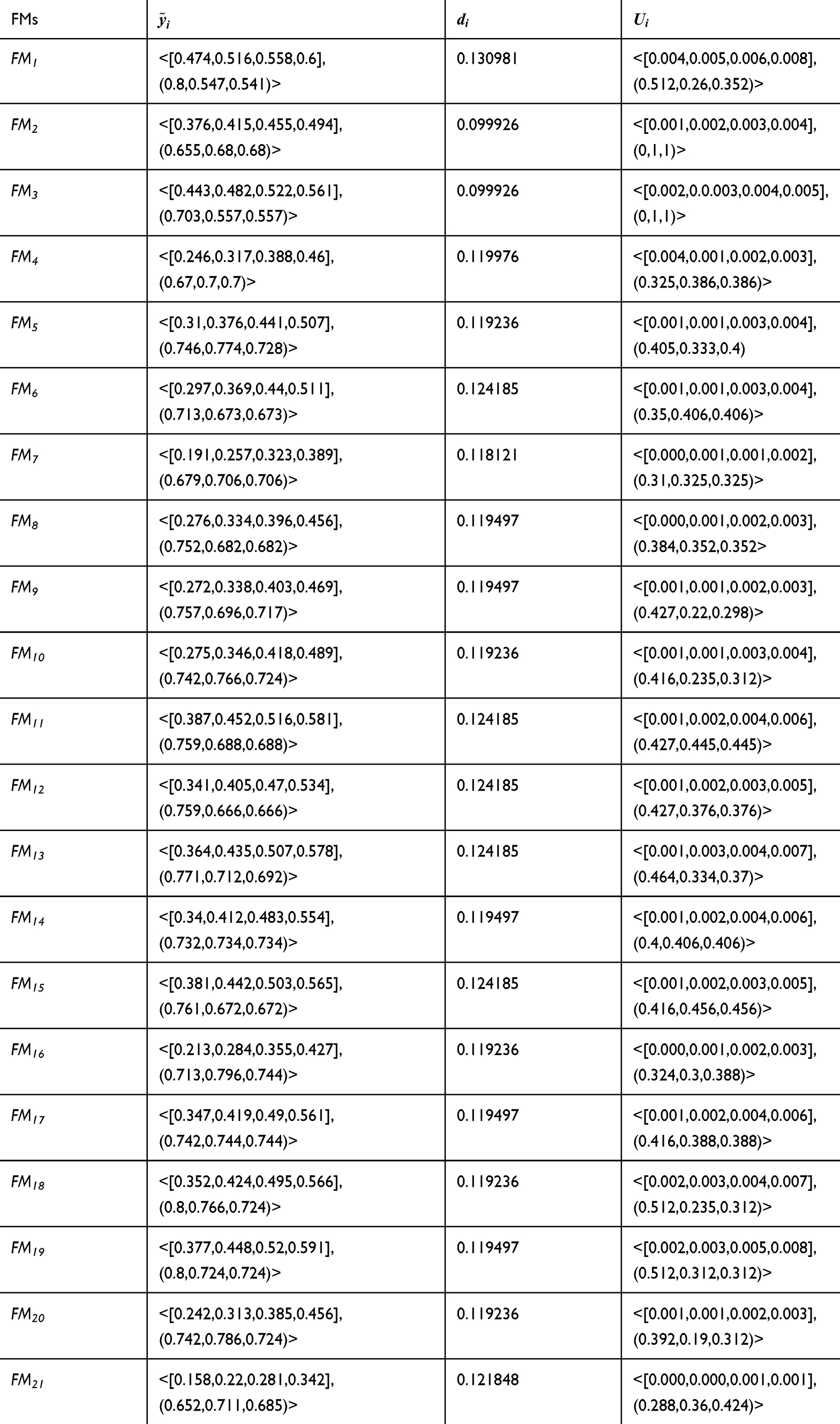
The ranking of failure modes during the surgical process in hospital X was determined using the SVTNN–MULTIMOORA method in accordance with three perspectives: the ratio system, reference-point model, and full multiplicative form. Firstly, the normalized SVTNN evaluation matrix  was computed using Equation 11 (Table 3 in Appendix B). Then, the summarizing ratio
was computed using Equation 11 (Table 3 in Appendix B). Then, the summarizing ratio  of each failure mode was obtained utilising Equation 12. The SVTNN maximal objective reference point of each risk factor was determined using Equation 13. The distance (
of each failure mode was obtained utilising Equation 12. The SVTNN maximal objective reference point of each risk factor was determined using Equation 13. The distance ( ) between the maximal objective reference point and each failure mode was calculated using Equation 14. The overall utility (
) between the maximal objective reference point and each failure mode was calculated using Equation 14. The overall utility ( ) of the
) of the  st failure mode can be expressed as an SVTNN using Equation 15. Following the aforementioned steps, the results computed by the ratio system, reference-point approach, and full multiplicative form are obtained, as shown in Table 7.
st failure mode can be expressed as an SVTNN using Equation 15. Following the aforementioned steps, the results computed by the ratio system, reference-point approach, and full multiplicative form are obtained, as shown in Table 7.
 |



The final ranking was obtained by aggregating the three ranking lists yielded by different parts of SVTNN–MULTIMOORA in accordance with the dominance theory. The last column in Table 8 shows the final ranking of the 21 failure modes acquired by the proposed FMEA model. The results demonstrate that the five most serious failures of hospital X are unclear diagnosis, careless information-checking, improper treatment of drainage tubes, improper administration of infusions, and improper operations, which require urgent and corrective action. Inappropriate life care is the least important failure during the surgical process in hospital X, and requires less improvement. Based on the ranking results, the hospital should adopt measures for the most serious failure modes to avoid surgical risk and improve the safety of operations.
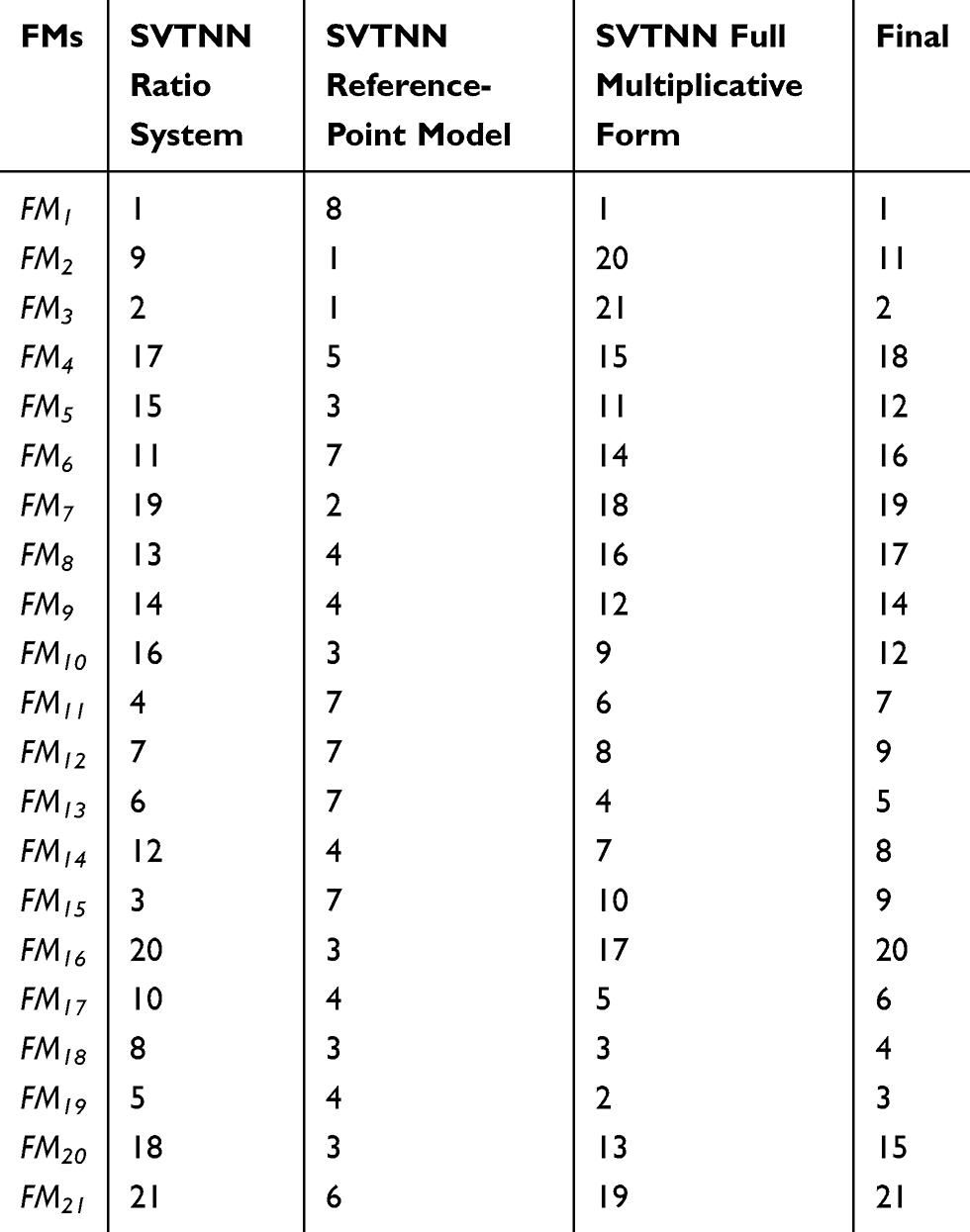 |
Table 8 Final Ranking of Failure Modes |
Analysis of causes, effects, and prevention methods showed that an unclear diagnosis results from unclear examination and misjudgement of etiology. An incorrect diagnosis may seriously affect the safety and healing of patients. The probability of diagnosis error was high, and should be emphatically improved. A suggested solution to the problem is to adopt the consultation model of multidisciplinary teams to explore suitable treatment plans. The second most serious failure in the surgical process was error in information-matching, which leads to erroneous preoperative preparation. As such, medical staff should be required to check the patient’s medical records, surgical treatments, surgical site, anesthesia methods, surgical instruments, and other information. This solution may be time-consuming and require improved personnel quality. Improper usage of drainage tubes and administration of infusions is caused by the poor professional quality of medical staff. Promoting professional knowledge, strong responsibility, sufficient communication, and strict guidelines for procedures are suggested to solve these failures. Improper procedures may cause serious consequences, but the possibility of procedural errors in hospital X is small. The staff in the operating room should carefully check information and correctly mark the operational siteto solve this problem.
Discussion
Surgery is one of the important methods of treating diseases and comprises a series of processes, including diagnosis, preoperative preparation, surgical operation, and postoperative care. Each process has accompanying risks and may seriously affect operation quality and patient safety. Therefore, the risk assessment of each segment of the surgical process is critical for the safety and quality of surgery, along with improvement in the physician–patient relationship.
The International Organization for Standardization suggests that FMEA is a prospective risk-analysis technology for high-risk processes.73,74 FMEA can be used systematically to define and evaluate potential risk-failure modes in the surgical process, analyze the causes and effects of potential failures, and implement effective measures to control them. However, the classical FMEA has limitations. The proposed hybrid FMEA in this study overcomes these shortcomings. The hybrid FMEA can identify several potential failures in the surgical process and consider linguistic evaluation of information provided by experts, instead of crisp ratings. The final risk ranking of failure modes obtained by the extended SVTNN–MULTIMOORA method helps the hospital’s medical team to focus on major surgical-process failures. Several critical failure modes that needed to be solved were obtained by evaluating the risk points in the surgical process of a hospital in Hunan Province.
Risk Factors
Among the MCDM techniques used in the proposed hybrid FMEA model, the BWM was used to determine the subjective weights of risk factors. Table 5 shows the importance of risk-factor rankings obtained by four experts. Three experts believed that the severity-of-failure mode is the most important factor, whereas another expert believed that its detectability is the most important factor. After the opinions of four experts had been comprehensively considered, the importance of risk factors was ranked as  . Risk factor S with, a weight of 0.4898, was the most important factor. As such, the S of failures is a concern in surgical-risk evaluation for effectively improving operation quality and security. The O of failures was the least important among the three risk factors. Experts agreed that the S of errors in the surgical process was more important than O. In generating subjective weights, inconsistencies may occur because of the complex judgment of experts.43 All CR values were close to 0, suggesting that the importance of risk factors provided by experts was consistent.
. Risk factor S with, a weight of 0.4898, was the most important factor. As such, the S of failures is a concern in surgical-risk evaluation for effectively improving operation quality and security. The O of failures was the least important among the three risk factors. Experts agreed that the S of errors in the surgical process was more important than O. In generating subjective weights, inconsistencies may occur because of the complex judgment of experts.43 All CR values were close to 0, suggesting that the importance of risk factors provided by experts was consistent.
The basic principle of the entropy method is that if the information entropy of the index is small, the index may provide additional information and the weight should be high. The importance ranking of risk factors based on entropy weight was  according to the evaluation of information provided by the experts. As such, the risk factor O provides more information than the others, but small differences exist among the entropy weights of the three risk factors.
according to the evaluation of information provided by the experts. As such, the risk factor O provides more information than the others, but small differences exist among the entropy weights of the three risk factors.
The comprehensive importance of risk factors was ranked as  on the basis of the principle of combining the subjective and objective weights. Considering the subjective judgment of experts and the amount of information provided by risk factors, S is more important than the other risk factors. If the S of failure mode is high, then additional attention should be given to this factor.
on the basis of the principle of combining the subjective and objective weights. Considering the subjective judgment of experts and the amount of information provided by risk factors, S is more important than the other risk factors. If the S of failure mode is high, then additional attention should be given to this factor.
Failure-Mode Ranking
According to the proposed hybrid FMEA model, the ranking result of failure modes was directly influenced by the comprehensive weight information of risk factors. The ranking result depends considerably on the proportion of  for subjective and objective weights.
for subjective and objective weights.  is the adjustment parameter and was set to 0.5 in this work, with a value range of [0, 1]. Different values of
is the adjustment parameter and was set to 0.5 in this work, with a value range of [0, 1]. Different values of  , ie,
, ie,  , were used to analyze the impact of
, were used to analyze the impact of  on failure-modes ranking. Figure 3 presents the influence of the ranking of each failure mode with various
on failure-modes ranking. Figure 3 presents the influence of the ranking of each failure mode with various  values.
values.
Figure 3 shows that based on the variable value of  , slight changes in the most critical failure modes can be observed under various circumstances. If
, slight changes in the most critical failure modes can be observed under various circumstances. If  is < 0.8, then FM1 is the most critical failure mode. Otherwise, FM3 is deemed the most critical. Given that the weight of the risk factor S was considerably higher than the other risk factors and the S of FM3 was higher than that of FM1, FM3 was more critical than FM1 when subjective weights account for a large proportion. When
is < 0.8, then FM1 is the most critical failure mode. Otherwise, FM3 is deemed the most critical. Given that the weight of the risk factor S was considerably higher than the other risk factors and the S of FM3 was higher than that of FM1, FM3 was more critical than FM1 when subjective weights account for a large proportion. When  <0.3, all ranking results changed slightly, and when
<0.3, all ranking results changed slightly, and when  was near 1, the ranking results were stable. Conclusively, each failure mode produced a minor change in the risk ranking when
was near 1, the ranking results were stable. Conclusively, each failure mode produced a minor change in the risk ranking when  changed from 0 to 1. A robust ranking result of failure modes was obtained, and the five most severe failures in the hospital comprised unclear diagnosis, careless information-checking, improper treatment of drainage tubes and improper infusion procedures.
changed from 0 to 1. A robust ranking result of failure modes was obtained, and the five most severe failures in the hospital comprised unclear diagnosis, careless information-checking, improper treatment of drainage tubes and improper infusion procedures.
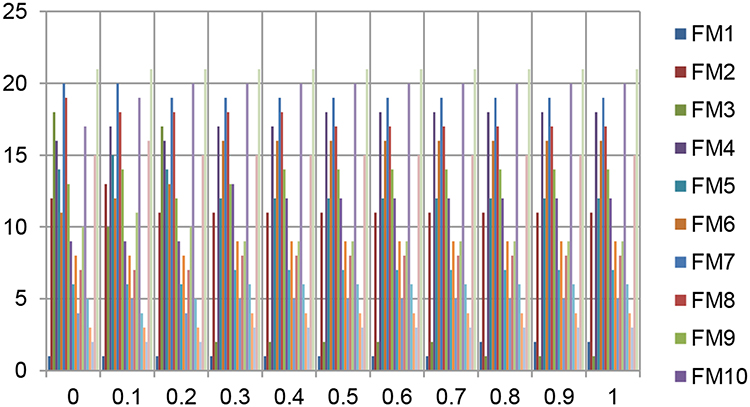 |
Figure 3 Ranking of failure modes for different ε-values. |
In summary, the professional skills and moral quality of the operating-room staff should be emphatically improved. Measures should be implemented, even given the high cost of manpower, money, and time. In modern society, medical errors and doctor–patient relationship problems often occur in hospitals. Highly professional and responsible staff should ensure that each patient and operation process is taken seriously to improve the quality and safety of operations and ease the relationship between doctors and patients.
Comparative Analysis with Other MCDM Methods
The proposed FMEA method was compared with the classical FMEA method, the crisp MULTIMOORA method,50 and the SVTNN–TOPSIS method75 to demonstrate its effectiveness and reliability further. Rankings are presented in Table 9 and Figure 4.
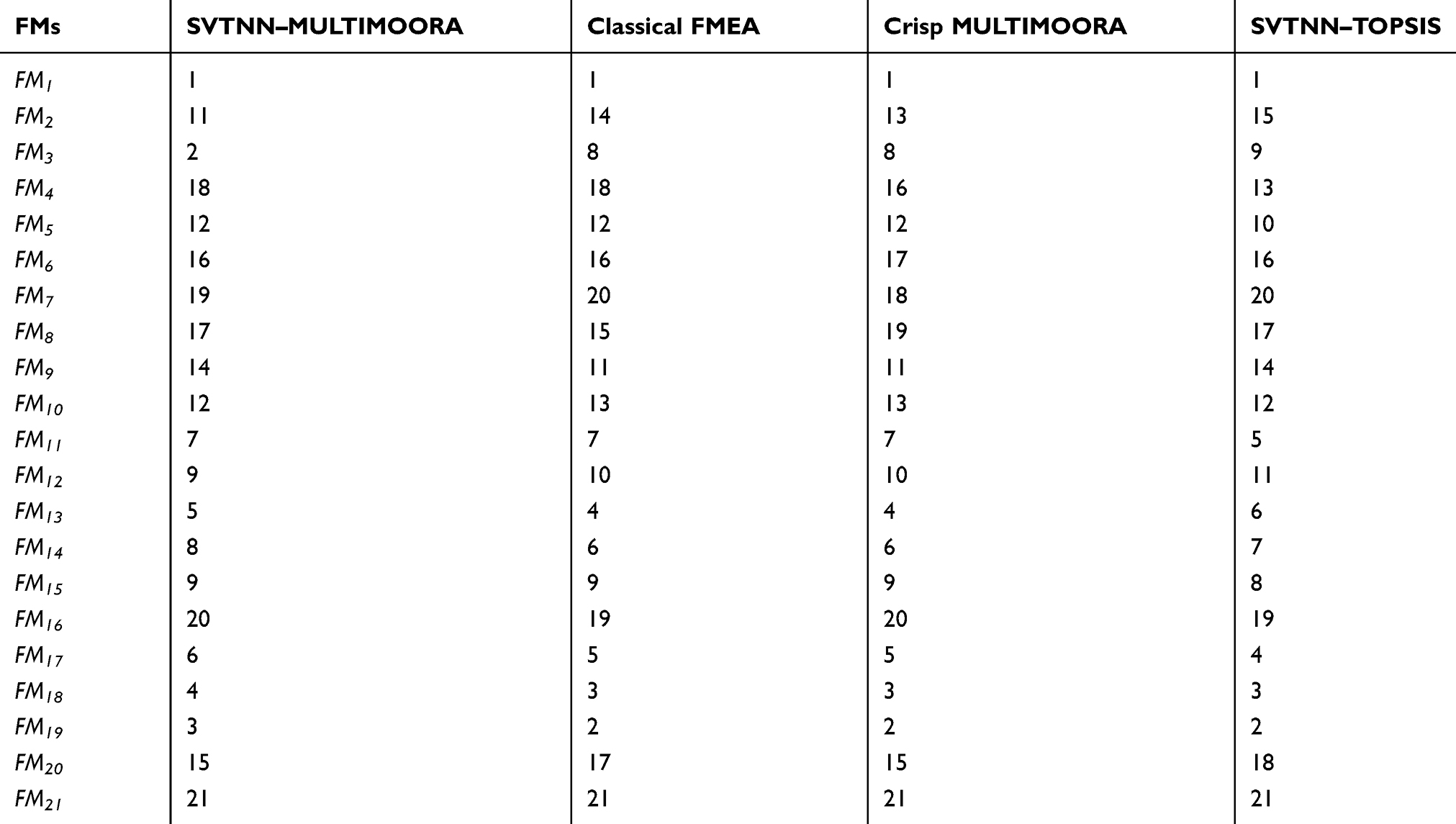 |
Table 9 Comparison of different methods |
Although the risk rankings of failure modes were unidentical, the most critical failure mode in all methods was FM1 and the least serious FM21. This finding is consistent with the results of the proposed model. Therefore, the proposed model is effective in properly ranking the failure modes.
However, the risk rankings among classical FMEA, crisp MULTIMOORA, and SVTNN–TOPSIS and the proposed method present several differences. Table 9 shows that the ranking results of crisp MULTIMOORA were consistent with those of the classical FMEA. The ranking order of FM3, FM9, FM10, FM12, FM13, FM14, FM17, FM18, and FM19 obtained using the two methods differed from those of the proposed model. A deviation in ranking results was observed because the imprecise and uncertain information in failure-mode evaluation was not considered in the classical FMEA or the crisp MULTIMOORA method. Therefore, the SVTNN–MULTIMORA method can provide more information for decision-makers than classical FMEA or crisp MULTIMOORA.
In the classical FMEA, assuming that the weights of risk factors are equal is unreasonable. For example, the evaluation information of FM2 under risk factor S is considerably larger thanunder the other two risk factors. FM2 ranked 14 in the classical FMEA. Given that the weight of S was higher than O in the proposed method, FM2 ranked 11, three places above that in the classical FMEA. These results were caused by the same weight of risk factors assigned in classical FMEA. Therefore, comprehensive weighting of risk factors by the BWM and entropy method is reasonable and applicable.
Figure 4 shows that the risk ranking obtained by SVTNN–TOPSIS differed from that acquired using the method proposed in this paper. This result is attributed to the failure mode that is close to the positive ideal value in TOPSIS, but may also be close to the negative ideal value. Moreover, the SVTNN–TOPSIS method considers only objective entropy weight and disregards the effect of experts’ subjective opinions on ranking results. Therefore, SVTNN–TOPSIS cannot fully reflect the risk of failure modes, thus affecting the accuracy of decision-making results. In the proposed SVTNN–MULTIMOORA method, the ranking of failure modes was determined in accordance with ranking results obtained by three decision-making methods: the SVTNN ratio system, the SVTNN reference-point method, and the SVTNN full multiplication model. Compared with other MCDM methods, the proposed method exhibits better applicability, potential, and ease of implementation. The proposed method also integrates subjective and objective weights and can obtain reasonable risk priority. The proposed hybrid SVTNN–MULTIMOORA model can obtain effective rankings.
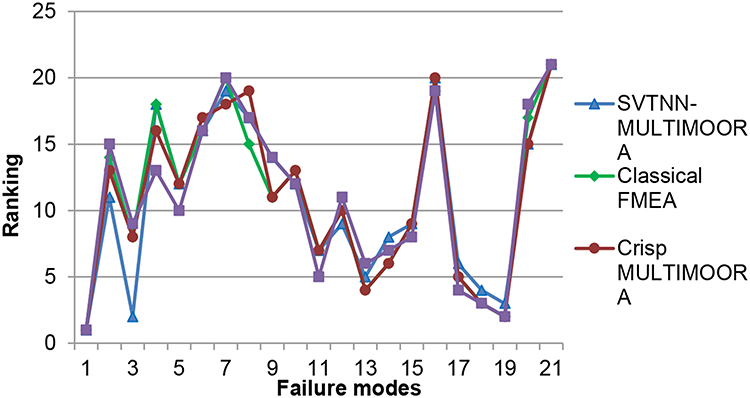 |
Figure 4 Ranking results of different methods. |
Future Research Orientation
The hybrid FMEA method was used to analyze risks in surgical processes of a hospital in Hunan Province systematically, identify all potential failures, and determine the most critical failures. This method proposes corresponding solutions and is superior to other risk-assessment methods. Although the proposed FMEA model can effectively assess the risk of the surgical process, several points, such as changes in the surgical environment and certain risk factors not considered in this study, should be studied in future. In addition, through communication with hospitals, data on surgical errors before and after intervention measures should be collected and corresponding changes compared and analyzed.
Conclusion
A reliable and practical risk-assessment model can reduce risks during surgery and disease treatment. FMEA is widely used to evaluate failure modes in many fields, although such a method has shortcomings. However, few studies have systematically assessed the risk of the surgical process by FMEA. A hybrid risk-assessment model of the surgical procedure was proposed in this study on the basis of extended FMEA. The method was helpful in identifying high-risk failure modes in the operation process and suggesting corresponding measures in advance to prevent the occurrence of surgical errors. Improving the quality of surgery and safety management and alleviating the doctor–patient relationship are conducive strategies.
Acknowledgments
This work was supported by the Human Philosophy Social Science Fund Projects (No. 18YBA150), the Key Project of Hunan Education Department (No. 18A201), Project of Hunan Federation of Social Sciences (No. XSP20YBC318), and the Hunan Provincial Natural Science Fund (Nos. 2018JJ5004, 2019JJ40088, and 2019JJ40479).
Disclosure
Peng-Fei Cheng reports grants and personal fees from the Department of Science and Technology of Hunan Province, Social Science Planning Office of Hunan Province, and the Department of Education of Hunan Province. Ji-Qun He reports grants and personal fees from the Hunan Provincial Natural Science Fund and Hunan Federation of Social Sciences during the study. The authors declare that they have no other possible conflicts of interest.
References
1. Li DP, He JQ, Cheng PF, Wang JQ, Zhang HY. A novel selection model of surgical treatments for early gastric cancer patients based on heterogeneous multicriteria group decision-making. Symmetry. 2018;10(6):223. doi:10.3390/sym10060223
2. Pomerantz RG, Lee DA, Siegel DM. Risk assessment in surgical patients: balancing iatrogenic risks and benefits. Clin Dermatol. 2011;29(6):669–677. doi:10.1016/j.clindermatol.2011.08.012
3. Thomas EJ, Studdert DM, Burstin HR, et al. Incidence and types of adverse events and negligent care in Utah and Colorado. Med Care. 2000;38(3):261–271. doi:10.1097/00005650-200003000-00003
4. Maria Laura C, Clemente P. FMEA: a model for reducing medical errors. Clinica Chimica Acta. 2009;404(1):75–78. doi:10.1016/j.cca.2009.03.015
5. Xie L, He JQ, Cheng PF, Xiao RS, Zhou XH. A multi-criteria 2-tuple linguistic group decision-making method based on TODIM for cholecystitis treatments selection. IEEE Access. 2019;7:127967–127986. doi:10.1109/ACCESS.2019.2939211
6. Bilimoria KY, Liu Y, Paruch JL, et al. Development and evaluation of the universal ACS NSQIP surgical risk calculator: a decision aid and informed consent tool for patients and surgeons. J Am Coll Surg. 2013;217(5):833–842.e833. doi:10.1016/j.jamcollsurg.2013.07.385
7. Bowles JB, Peláez CE. Fuzzy logic prioritization of failures in a system failure mode, effects and criticality analysis. Reliab Eng Syst Saf. 1995;50(2):203–213. doi:10.1016/0951-8320(95)00068-D
8. Sharma RK, Kumar D, Kumar P. Systematic failure mode effect analysis (FMEA) using fuzzy linguistic modelling. Int J Qual Reliab Manage. 2005;22(9):986–1004. doi:10.1108/02656710510625248
9. Shan -M-M, Li P, Liu H-C. Interval 2-tuple linguistic distance operators and their applications to supplier evaluation and selection. Mathematical Probl Eng. 2016;2016:1–12. doi:10.1155/2016/9893214
10. Helvacioglu S. Ozen fuzzy based failure modes and effect analysis for yacht system design. Ocean Eng. 2014;79(2):131–141.
11. Khasha R, Sepehri MM, Khatibi T. A fuzzy FMEA approach to prioritizing surgical cancellation factors. Int J Hosp Res. 2013;2(1):17–24.
12. Anderson O, Brodie A, Vincent CA, Hanna GB. A systematic proactive risk assessment of hazards in surgical wards: a quantitative study. Ann Surg. 2012;255(6):1086–1092. doi:10.1097/SLA.0b013e31824f5f36
13. Liu HC, Li P, You JX, Chen YZ. A novel approach for FMEA: combination of interval 2-Tuple linguistic variables and gray relational analysis. Qual Reliab Eng Int. 2015;31(5):761–772. doi:10.1002/qre.1633
14. Dong SC, Chung JH, Fu CY. A novel approach for evaluating the risk of health care failure modes. J Med Syst. 2012;36(6):3967–3974. doi:10.1007/s10916-012-9868-5
15. Magnezi R, Hemi A, Hemi R. Using the failure mode and effects analysis model to improve parathyroid hormone and adrenocorticotropic hormone testing. Risk Manag Healthc Policy. 2016;9:271–274. doi:10.2147/RMHP.S117472
16. Liu H-C, You J-X, Duan C-Y. An integrated approach for failure mode and effect analysis under interval-valued intuitionistic fuzzy environment. Int J Prod Econ. 2019;207:163–172. doi:10.1016/j.ijpe.2017.03.008
17. Liu H-C, Wang L-E, You X-Y, Wu S-M. Failure mode and effect analysis with extended grey relational analysis method in cloud setting. Total Qual Manage Bus Excellence. 2019;30(7–8):745–767. doi:10.1080/14783363.2017.1337506
18. Liu HC, Liu L, Liu N. Risk evaluation approaches in failure mode and effects analysis: a literature review. Expert Syst Appl. 2013;40(2):828–838. doi:10.1016/j.eswa.2012.08.010
19. Liu HC, You JX, Shan MM, Su Q. Systematic failure mode and effect analysis using a hybrid multiple criteria decision-making approach. Total Qual Manage Bus Excellence. 2019;30(5–6):537–564. doi:10.1080/14783363.2017.1317585
20. Kahraman C, Kaya İ, Şenvar Ö. Healthcare failure mode and effects analysis under fuzziness. Human Ecol Risk Assess. 2013;19(2):538–552. doi:10.1080/10807039.2012.737753
21. Safari H, Faraji Z, Majidian S. Identifying and evaluating enterprise architecture risks using FMEA and fuzzy VIKOR. J Intell Manuf. 2016;27(2):475–486. doi:10.1007/s10845-014-0880-0
22. Dağsuyu C, Göçmen E, Narlı M, Kokangül A. Classical and fuzzy FMEA risk analysis in a sterilization unit. Comp Ind Eng. 2016;101:286–294. doi:10.1016/j.cie.2016.09.015
23. Deng XY, Jiang W. Fuzzy risk evaluation in failure mode and effects analysis using a D numbers based multi-sensor information fusion method. Sensors. 2017;17(9):2086. doi:10.3390/s17092086
24. Wang WZ, Liu XW, Chen XQ, Qin Y. Risk assessment based on hybrid FMEA framework by considering decision maker’s psychological behavior character. Comp Ind Eng. 2019;136:516–527. doi:10.1016/j.cie.2019.07.051
25. Kumar AM, Rajakarunakaran S, Pitchipoo P, Vimalesan R. Fuzzy based risk prioritisation in an auto LPG dispensing station. Saf Sci. 2018;101:231–247. doi:10.1016/j.ssci.2017.09.011
26. Yazdi M, Daneshvar S, Setareh H. An extension to Fuzzy Developed Failure Mode and Effects Analysis (FDFMEA) application for aircraft landing system. Saf Sci. 2017;98:113–123. doi:10.1016/j.ssci.2017.06.009
27. Lavasani SM, Ramzali N, Sabzalipour F, Akyuz E. Utilisation of fuzzy fault tree analysis (FFTA) for quantified risk analysis of leakage in abandoned oil and natural-gas wells. Ocean Eng. 2015;108:729–737. doi:10.1016/j.oceaneng.2015.09.008
28. Tooranloo HS, Ayatollah AS. Pathology the internet banking service quality using failure mode and effect analysis in interval-valued intuitionistic fuzzy environment. Int J Fuzzy Syst. 2017;19(1):109–123. doi:10.1007/s40815-016-0265-y
29. Qian W, Wang Z-J, Li K. Medical waste disposal method selection based on a hierarchical decision model with intuitionistic fuzzy relations. Int J Environ Res Public Health. 2016;13(9):896. doi:10.3390/ijerph13090896
30. Zhao H, You JX, Liu HC. Failure mode and effect analysis using MULTIMOORA method with continuous weighted entropy under interval-valued intuitionistic fuzzy environment. Soft Comp. 2017;21(18):5355–5367. doi:10.1007/s00500-016-2118-x
31. Zadeh LA. Fuzzy sets. Inf Control. 1965;8(3):338–353. doi:10.1016/S0019-9958(65)90241-X
32. Atanassov KT, Rangasamy P. Intuitionistic fuzzy sets. Fuzzy Sets Syst. 1986;20(1):87–96. doi:10.1016/S0165-0114(86)80034-3
33. Ji P, Zhang HY, Wang JQ. A fuzzy decision support model with sentiment analysis for items comparison in e-commerce: the case study of PConline.com. IEEE Trans Syst Man Cybernetics. 2018;49(10):1993–2004. doi:10.1109/TSMC.2018.2875163
34. Liang RX, Wang JQ, Lin L. Multi-criteria group decision-making method based on interdependent inputs of single-valued trapezoidal neutrosophic information. Neural Comput Appl. 2018;30(1):241–260. doi:10.1007/s00521-016-2672-2
35. Liang RX, Wang JQ, Zhang HY. A multi-criteria decision-making method based on single-valued trapezoidal neutrosophic preference relations with complete weight information. Neural Comput Appl. 2018;30(11):3383–3398. doi:10.1007/s00521-017-2925-8
36. Liang RX, Wang JQ, Zhang HY. Evaluation of e-commerce websites: an integrated approach under a single-valued trapezoidal neutrosophic environment. Knowledge Based Syst. 2017;135:44–59. doi:10.1016/j.knosys.2017.08.002
37. Wang LE, Liu HC, Quan MY. Evaluating the risk of failure modes with a hybrid MCDM model under interval-valued intuitionistic fuzzy environments. Comp Ind Eng. 2016;102:175–185. doi:10.1016/j.cie.2016.11.003
38. Liu HC, Liu L, Liu N, Mao LX. Risk evaluation in failure mode and effects analysis with extended VIKOR method under fuzzy environment. Expert Syst Appl. 2012;39(17):12926–12934. doi:10.1016/j.eswa.2012.05.031
39. Mangla SK, Kumar P, Barua MK. Risk analysis in green supply chain using fuzzy AHP approach: a case study. Resour Conservation Recycl. 2015;104:375–390. doi:10.1016/j.resconrec.2015.01.001
40. Liu H-C, You J-X, You X-Y, Shan -M-M. A novel approach for failure mode and effects analysis using combination weighting and fuzzy VIKOR method. Appl Soft Comput. 2015;28(C):579–588. doi:10.1016/j.asoc.2014.11.036
41. Rezaei J. Best-worst multi-criteria decision-making method. Omega. 2015;53:49–57. doi:10.1016/j.omega.2014.11.009
42. Tian ZP, Wang JQ, Zhang HY. An integrated approach for failure mode and effects analysis based on fuzzy best-worst, relative entropy and VIKOR methods. Appl Soft Comput. 2018;72:636–646. doi:10.1016/j.asoc.2018.03.037
43. Nie RX, Tian ZP, Wang JQ, Zhang HY, Wang TL. Water security sustainability evaluation: applying a multistage decision support framework in industrial region. J Clean Prod. 2018;196:1681–1704. doi:10.1016/j.jclepro.2018.06.144
44. Li J, Wang JQ, Hu JH. Multi-criteria decision-making method based on dominance degree and BWM with probabilistic hesitant fuzzy information. Int J Mach Learn Cybernetics. 2019;10(7):1671–1685. doi:10.1007/s13042-018-0845-2
45. Liu HC, You JX, Chen SM, Chen YZ. An integrated failure mode and effect analysis approach for accurate risk assessment under uncertainty. IIE Trans. 2016;48(11):1027–1042. doi:10.1080/0740817X.2016.1172742
46. Arabzad SM, Razmi J, Ghorbani M. Classify purchasing items based on risk and profitability attributes; using MCDM and FMEA techniques. Res J Int Stud. 2011;1(21):80–85.
47. Lolli F, Ishizaka A, Gamberini R, Rimini B, Messori M. FlowSort-GDSS– a novel group multi-criteria decision support system for sorting problems with application to FMEA. Expert Syst Appl Int J. 2015;42(17–18):6342–6349. doi:10.1016/j.eswa.2015.04.028
48. Shahin A, Khodadady Z, Shirouyehzad H. Ranking electronic customer complaints by FMEA and TOPSIS with a case study in Isfahan Province Gas Company. Int J Proc Manage Benchmarking. 2014;5(1):19–36. doi:10.1504/IJPMB.2015.066027
49. Brauers WKM, Zavadskas EK. Multimoora optimization used to decide on a bank loan to buy property. Technol Econ Devel Econ. 2011;17(1):174–188. doi:10.3846/13928619.2011.560632
50. Brauers WKM, Zavadskas EK. Project management by MULTIMOORA as an instrument for transition economies. Technol Econ Devel Econ. 2010;16(1):5–24. doi:10.3846/tede.2010.01
51. Brauers WKM, Zavadskas EK. The MOORA method and its application to privatization in a transition economy. Control Cybernetics. 2006;35(35):445–469.
52. Chen X, Zhao L, Liang H. A novel multi-attribute group decision-making method based on the MULTIMOORA with linguistic evaluations. Soft Comp. 2018;22(16):5347–5361. doi:10.1007/s00500-018-3030-3
53. Brauers WKM, Baležentis A, Baležentis T. Multimoora for the EU member states updated with fuzzy number theory. Technol Econ Devel Econ. 2011;17(2):259–290. doi:10.3846/20294913.2011.580566
54. Liu H-C, Fan X-J, Li P, Chen Y-Z. Evaluating the risk of failure modes with extended MULTIMOORA method under fuzzy environment. Eng Appl Artif Intell. 2014;34:168–177. doi:10.1016/j.engappai.2014.04.011
55. Streimikiene D, Balezentis T. Multi-objective ranking of climate change mitigation policies and measures in Lithuania. Renewable Sustain Energy Rev. 2013;18:144–153. doi:10.1016/j.rser.2012.09.040
56. Kracka M, Zavadskas EK. Panel building refurbishment elements effective selection by applying multiple-criteria methods. Int J Strategic Prop Manage. 2013;17(2):210–219. doi:10.3846/1648715X.2013.808283
57. Baležentis T, Baležentis A. A survey on development and applications of the multi-criteria decision making method MULTIMOORA. J Multi Crit Dec Anal. 2014;21(3–4):209–222. doi:10.1002/mcda.1501
58. Brauers WKM, Zavadskas EK. Robustness of MULTIMOORA: a method for multi-objective optimization. Informatica. 2012;23(1):1–25. doi:10.15388/Informatica.2012.346
59. Tian ZP, Wang J, Wang JQ, Zhang HY. An improved MULTIMOORA approach for multi-criteria decision-making based on interdependent inputs of simplified neutrosophic linguistic information. Neural Comput Appl. 2017;28(1):585–597. doi:10.1007/s00521-016-2378-5
60. Julia N, Mills PD, Noel E, et al. Incorrect surgical procedures within and outside of the operating room: a follow-up report. Arch Surg. 2011;146(11):1235–1239. doi:10.1001/archsurg.2011.171
61. Bonfant G, Belfanti PG, Gabrielli D, et al. Clinical risk analysis with failure mode and effect analysis (FMEA) model in a dialysis unit. J Nephrol. 2010;23(1):111–118.
62. Siriphuwanun V, Punjasawadwong Y, Lapisatepun W, Charuluxananan S, Uerpairojkit K. Prognostic factors for death and survival with or without complications in cardiac arrest patients receiving CPR within 24 hours of anesthesia for emergency surgery. Risk Manag Healthc Policy. 2014;7:199–210. doi:10.2147/RMHP.S68797
63. Pikkel D, Sharabi-Nov A, Pikkel J. It is the left eye, right? Risk Manag Healthc Policy. 2014;7:77–80. doi:10.2147/RMHP.S60728
64. Chanamool N, Naenna T. Fuzzy FMEA application to improve decision-making process in an emergency department. Appl Soft Comput. 2016;43:441–453. doi:10.1016/j.asoc.2016.01.007
65. Li G. Implementation of a risk management plan in a hospital operating room. Int J Nurs Sci. 2015;2(4):348–354. doi:10.1016/j.ijnss.2015.10.007
66. Wang HB, Smarandache F, Zhang YQ, Sunderraman R. Interval neutrosophic sets and logic: theory and applications in computing. Comp Sci. 2005;65(vi):87.
67. Wu XH, Wang JQ, Peng JJ, Qian J. A novel group decision-making method with probability hesitant interval neutrosphic set and its application in middle level manager’s selection. Int J Uncertain Quantif. 2018;8(4):291–319. doi:10.1615/Int.J.UncertaintyQuantification.2018020671
68. Deli I, Subas Y Single Valued Neutrosophic Numbers and Their Applications to Multicriteria Decision Making Problem. 2014.
69. Ye J. Some weighted aggregation operators of trapezoidal neutrosophic numbers and their multiple attribute decision making method. Informatica. 2017;28(2):387–402. doi:10.15388/Informatica.2017.108
70. Rezaei J. Best-worst multi-criteria decision-making method: some properties and a linear model. Omega. 2016;64:126–130. doi:10.1016/j.omega.2015.12.001
71. Ji P, Zhang HY, Wang JQ. Fuzzy decision-making framework for treatment selection based on the combined QUALIFLEX–TODIM method. Int J Syst Sci. 2017;48(14):3072–3086. doi:10.1080/00207721.2017.1365968
72. Nie RX, Tian ZP, Wang XK, Wang JQ, Wang TL. Risk evaluation by FMEA of supercritical water gasification system using multi-granular linguistic distribution assessment. Knowledge Based Syst. 2018;162:185–201. doi:10.1016/j.knosys.2018.05.030
73. Trucco P, Cavallin M. A quantitative approach to clinical risk assessment: the CREA method. Saf Sci. 2006;44(6):491–513. doi:10.1016/j.ssci.2006.01.003
74. Asefzadeh S, Yarmohammadian MH, Nikpey A, Atighechian G. Clinical risk assessment in intensive care unit. 2013;4(5):592–598.
75. Biswas P, Pramanik S, Giri BC. TOPSIS strategy for multi-attribute decision making with trapezoidal neutrosophic numbers. Neutro Sets Syst. 2018;19:29–39.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.