Back to Journals » Clinical Ophthalmology » Volume 14
Evaluating Rotational Stability of an Extended Depth of Focus Toric Intraocular Lens Using a Slit Lamp and Image-Based Analysis
Authors Sandoval HP, Lane S, Slade S, Donnenfeld ED ![]() , Potvin R
, Potvin R ![]() , Solomon KD
, Solomon KD
Received 15 July 2020
Accepted for publication 10 August 2020
Published 21 August 2020 Volume 2020:14 Pages 2405—2410
DOI https://doi.org/10.2147/OPTH.S272240
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Helga P Sandoval,1 Stephen Lane,2 Stephen Slade,3 Eric D Donnenfeld,4 Richard Potvin,5 Kerry D Solomon1
1Carolina Eyecare Physicians, LLC, Mt. Pleasant, SC, USA; 2Associated Eye Care, Stillwater, MN, USA; 3Slade & Baker Vision, Houston, TX, USA; 4Ophthalmic Consultants of Long Island, Long Island, NY, USA; 5Science in Vision, Bend, OR, USA
Correspondence: Kerry D Solomon
Carolina Eyecare Physicians, LLC, 1101 Clarity Road, Suite 100, Mt Pleasant, SC 29464, USA
Email [email protected]
Purpose: To evaluate the rotational stability of a toric extended depth of focus (EDOF) intraocular lens (IOL), using either slit lamp evaluation or image-processing software.
Setting: Three clinical practices in the USA.
Design: Prospective unmasked randomized clinical trial.
Methods: Subjects presenting for routine cataract surgery that were interested in improved near vision received toric EDOF lenses (TECNIS Symfony® Toric) in both eyes. The measures of interest in the current analysis were the change in orientation of the IOL between 1 day, 1 month and 3 months postoperative. Orientation was measured at the microscope on the day of surgery, and with the slit lamp at all other visits. Day 1, 1-month and 3-month images of the lens orientation were captured with a slit lamp camera. Differences in orientation were recorded and analyzed.
Results: A total of 150 eyes had IOL orientation data available. Image analysis showed mean absolute lens orientation changes from 1 day to 1 month and 3 months of less than 2 degrees. The percentage of lenses exhibiting rotation of ≤ 5 degrees between any measured time points was 97% or higher. Results were similar, but significantly more variable, when IOL orientation was measured at the slit lamp.
Conclusion: The toric EDOF lens evaluated here demonstrated rotational stability that exceeded the prior ANSI standard. The best method to determine IOL orientation changes was through image analysis.
Keywords: TECNIS symfony toric, toric IOL, rotational stability
Plain Language Summary
At the time of cataract surgery, the clouded lens of the eye is removed and an artificial replacement, an intraocular lens (or IOL) is placed in the eye. The surgeon can use measurements of the eye to determine the best power for that IOL, which means that patients may rely less on their glasses after surgery. Astigmatism is one form of defocus that the surgeon can address. Astigmatism correction has a direction, so that an astigmatic power and an orientation (0 to 180 degrees) must be calculated for correction. Because astigmatism is direction-specific, it is important that the IOL be placed in the correct orientation at the time of surgery and that the IOL stay in that orientation. The current study was designed to evaluate the orientation of 150 eyes soon after surgery and up to 3 months after surgery. After 3 months, a change in IOL orientation is very unlikely. The orientation of the IOLs in this study was measured in two ways – at a slit lamp (the device used by the surgeon to examine the eye) and using high-resolution images of the eye. Results showed that the astigmatism correcting IOL in this study rotated very little over the course of three months, with 97% of IOLs showing 5 degrees of orientation change (or less) over that time period. Comparing the methods used to evaluate rotation, the use of high-resolution images showed better consistency and accuracy than the use of the slit lamp.
Introduction
Presbyopia correction at the time of cataract surgery has become increasingly popular. Residual astigmatism after implantation of presbyopia correcting intraocular lenses (IOLs) can be a significant issue, reducing the effectiveness of the lens and increasing the retreatment rate.1 Relaxing incisions (corneal or limbal) and toric IOLs are the two most common methods of reducing astigmatism at the time of cataract surgery. A meta-analysis by Kessel et al2 concluded that visual and clinical outcomes, including the magnitude of residual astigmatism, were better with toric lenses relative to relaxing incisions. As such, astigmatism correction when using a presbyopia correcting IOL is an important consideration; this can be achieved with the use of toric presbyopia correcting intraocular lenses.
Rotational stability is a key factor in the success of toric IOLs. For each degree of misalignment, the effective corrective effect of the lens (cylinder power) is reduced by about 3%, though in fact there is both a reduction in the magnitude of the cylinder power correction and an axis change when toric IOLs are misoriented.3 The new ANSI standard for rotational stability of a toric IOL states that stability of the toric IOL axis shall be achieved if 90% of the toric IOLs in the treated eyes rotate less than or equal to five degrees between the final two consecutive visits.4
One presbyopia correcting toric lens in common use is an extended depth of focus (EDOF) toric IOL (Symfony® toric, Johnson and Johnson Vision, Santa Ana, CA). Gundersen examined the rotational stability of this EDOF toric lens in 30 patients and noted a median IOL rotation of 2 degrees from surgery to 3 months postoperatively.5 The author noted 96% of lenses had lens rotation ≤10°; 87% had rotation ≤5°. There was no apparent correlation between rotation and axial length.5 The purpose of the current study was to evaluate the rotation stability of this EDOF toric IOL. Rotation data analyzed here were a subset of the data collected in a larger multicenter prospective randomized clinical trial examining the effects of this EDOF lens when slight monovision was targeted in the non-dominant eye.
Methods
The EDOF toric lens mentioned above was bilaterally implanted in cataract patients in a multi-site, unmasked, randomized clinical trial designed to evaluate overall clinical outcomes. Institutional review board (IRB) approval was obtained from Salus IRB, Austin, TX, USA. The study was also registered with clinicaltrials.gov - record NCT03082599. The study was conducted in accordance with the Declaration of Helsinki. Subjects eligible for inclusion had to be 40 years old or older, have cataracts that required surgery in both eyes and be interested in astigmatism correction with an IOL. In addition, they had to have potential visual acuity of at least 0.2 logMAR (20/32 Snellen), with no ocular pathology that would be expected to affect postoperative visual outcomes. Exclusion criteria included severe dry eye, prior refractive or cataract surgery, uncontrolled diabetes, and those having a concurrent secondary procedure at the time of cataract surgery (eg, implantation of any surgical glaucoma device). No vulnerable subject populations were enrolled. All subjects included in the study reviewed and signed an IRB-approved informed consent. The dataset collected for this study is not available for sharing.
Subjects presenting for routine cataract surgery received bilateral toric EDOF lenses (TECNIS Symfony Toric – Johnson and Johnson Vision, Santa Ana, CA). While the primary intent of the study was to evaluate how a small amount of defocus in the non-dominant eye affected one group of participants, this distinction was not important to the current analysis. The current analysis involved evaluating IOL orientation data for all eyes at all visits. This was based on recording IOL orientation at the microscope at the time of surgery and in the slit lamp for postoperative evaluation. Preoperatively, toric power was calculated using Lenstar keratometry and the AMO Toric Calculator (https://www.amoeasy.com/). The “Include Posterior Corneal Astigmatism” box was checked for all calculations. Eyes were marked at the time of surgery to account for cyclotorsion using digital marking, using the Verion Guided System (Alcon, Fort Worth, USA) or Callisto (Carl Zeiss Meditec, Jena, Germany) at all sites.
Postoperatively, eyes were adequately dilated to view at least one of the IOL axis marks on both sides. The toric IOL axis orientation was then determined by rotating the slit lamp beam and aligning it with the IOL axis indicator marks. At one site (KDS) ocular retroillumination photographs were taken at the 1-day, 1-month and 3-month postoperative visits using a 10X magnification. Using the proprietary image analysis software and following the instructions described by Kasthurirangan et al,6 the images for a given eye were registered to each other using iris and scleral landmarks. The relative change in IOL orientation from 1 day (baseline) to 1 month and 3 months was then determined. Figure 1 shows images taken at 1 day, 1 month and 3 months as well as the analyzed images.
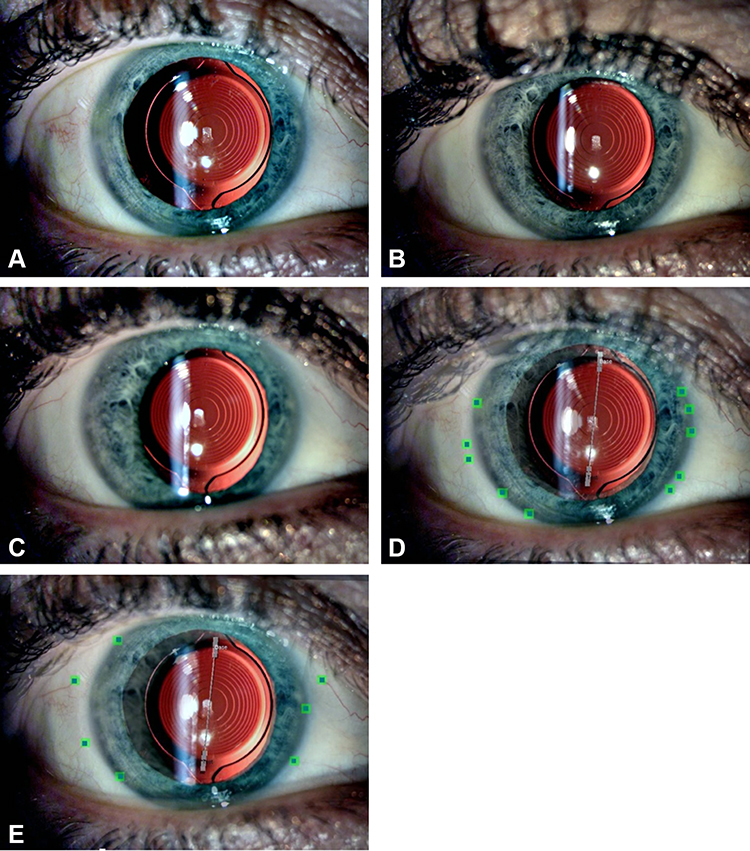 |
Figure 1 Slit lamp photographs taken at (A) Day 1 (baseline), (B) Month 1 and (C) Month 3. (D) Analyzed picture at Month 1 showing the blue squares that represent the baseline landmarks chosen by examiner while the green squares represent the ones chosen in the Month 1 image. (E) Analyzed picture at Month 3. Good image alignment is shown by the blue and green squares overlapping. |
Orientation data from the sites were collected on appropriate case report forms and subsequently imported into an Access database (Microsoft Corp., Redmond, USA) for preliminary analysis. The images collected were sent to a third-party consultant for processing; calculated orientation data were returned in an Excel file (Microsoft Corp., Redmond, USA). The Statistica data analysis software system, version 12 (TIBCO Software Inc., Palo Alto, CA, USA) was used for analysis of results, with parametric data comparisons made based on analysis of variance (ANOVA) and non-parametric data comparisons made using the Chi-squared test.
Results
A total of 150 eyes had orientation data available at 1 day postoperative and at the 1-month and/or 3-month visits. Image-based rotation data were available for 102 of these eyes at the 1-month visit and 103 eyes at the 3-month visit. Two eyes of 150 (1.3%) exhibited significant rotation between the day of surgery and the (baseline) 1-day visit. In both cases the IOL was reoriented and rotation data (from 1-day to 1-month and 3-months) were calculated from the reoriented lens position. One eye exhibited significant rotation at the 1-month visit and was reoriented. The change in position from Day 1 to 1 month was 17 degrees (based on image analysis); this was the estimated change in position from Day 1 to 3 months as well. One-month to three-month stability was measured from the reoriented position. The axial lengths of the two eyes that were reoriented the first day after surgery were both between 22 and 23mm, while the axial length of the eye that showed significant rotation at 1 month was 27.0 mm. Mean axial length for all eyes was 24.1 ± 1.5 mm, with a range from 21.8 to 27.9 mm.
The summary rotation data based on slit lamp measurement or the image-analysis system are shown in Table 1. Mean rotations are small, but the ranges indicate that there are some outliers. As can be seen, in all but one of the time period/method combinations listed the percentage of eyes with rotation ≤5 degrees was greater than 90%; in the single exception (1 day to 3 months, measured by slit lamp), the percentage was 89%. The percentage of eyes with rotation ≤5 degrees was statistically significantly higher for the image analysis system between 1 day and 1 month, and between 1 day and 3 months. There was no statistically significant difference in the percentage of eyes with rotation ≤5 degrees by method between the 1-month and 3-month visits, though the slit lamp measurement percentage was 5% lower. Note that the number of eyes with reported rotation of greater than 10 degrees was very low for all methods and time periods but was always higher for the slit lamp measurement method than for the image analysis method.
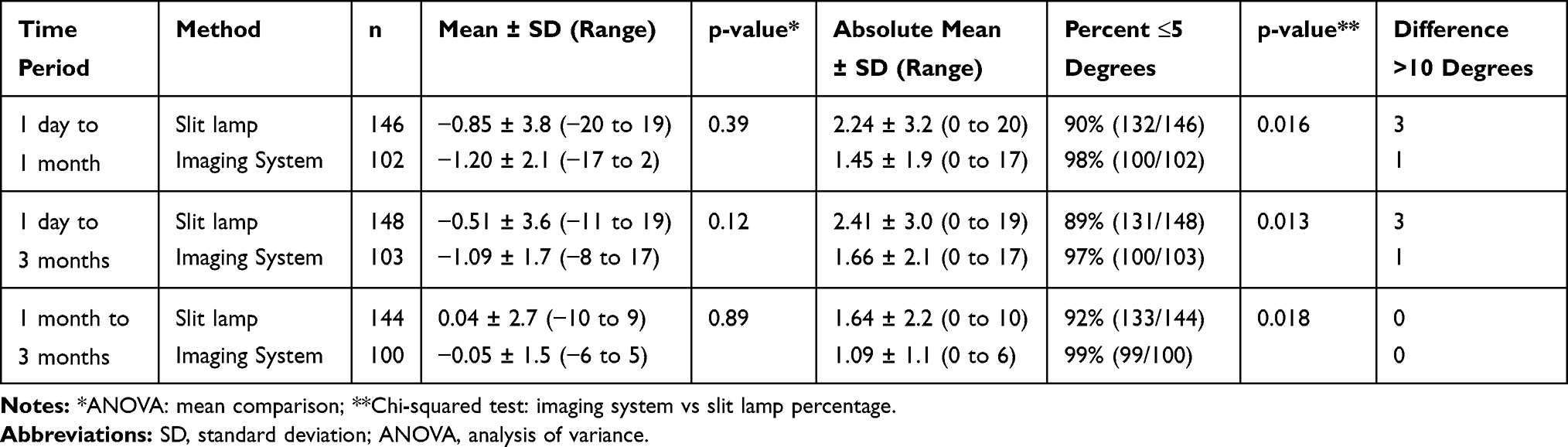 |
Table 1 Rotation Summary by Method and Time |
A repeated-measures analysis of variance (ANOVA) shows there was no statistically significant difference in the measured mean rotation at 1 month and 3 months (p = 0.85), no statistically significant difference in this mean rotation by measurement method (p = 0.12) and no interaction between the time period measured and the method of measurement (p = 0.80). However, an F-test to compare variances between groups shows that the variance in the image analysis group was statistically significantly lower than for the slit lamp group at both 1 month and 3 months (p < 0.01 in both cases).
The differences between the measured orientation change determined with the slit lamp and the orientation change determined by the image processing method at both 1 and 3 months showed that at 1 month only 3 eyes of 100 (3%) had a rotation value difference between methods of greater than 5 degrees, and all differences were 8 degrees or less. At 3 months there were 7 eyes of 103 (6.8%) that had a rotation value difference between methods greater than 5 degrees, with a maximum difference of 12 degrees.
Discussion
The data analyzed here indicate that the toric EDOF lens implanted demonstrates good rotational stability, exceeding the ANSI standard (90% of lenses demonstrating rotation of ≤0.5 degrees) at both 1 and 3 months when evaluated using image analysis. Evaluation using slit lamp measurement demonstrated significantly more variability and significantly lower rates of rotation ≤0.5 degrees. Rates determined by slit lamp measurement met or exceeded the ANSI standard from 1 day to 1 month and from 1 month to three months.
In a large (302 patients) prospective study by Miyake et al, mean IOL rotation of the AcrySof® toric lens (Alcon, Fort Worth, Texas) was 4.5 degrees within the first postop day but was 1 to 2 degrees thereafter; 1.6% (6/378 eyes) had greater than 20 degrees of rotation, all of which had axial length >25.0 mm.7 Results reported here using image processing are similar, though no eyes had rotation greater than 20 degrees.
The correlation between long axial length and toric IOL rotation has been previously documented.8 There were too few eyes with significant IOL rotation in the current study to draw any statistical conclusions but the one eye in which a reorientation of the IOL was performed at 1-month post surgery had an axial length of 27 mm.
Prospective studies of the Tecnis® toric intraocular lens (Johnson and Johnson Vision, Santa Ana, CA) have demonstrated average absolute rotation of 2.7 degrees from 1 day to 6 months postop but was within 2 degrees when comparing between 1 to 3 months and 3 to 6 months; lens rotation was ≤5 degrees for 93%-94% of cases between 1 to 3 months and 3 to 6 months; 5 cases had rotation ≥10 degrees with 2.3% (4/174 cases) requiring repositioning procedures.6,9 Results here appear generally consistent with these findings.
Two 2018 prospective randomized studies also evaluated Tecnis (monofocal) toric IOL rotation. One study10 found a mean absolute rotation of 2.6 degrees at 3 months using image processing analysis; this is somewhat higher than observed here, but the baseline measure was the orientation on the day of surgery. Another, using slit lamp observation, found a mean absolute rotation of 3.3 degrees between the day of surgery and 12 months postoperative.11 The results from the current study appear slightly better than this. Again, the use of Day 1 data as the baseline may be a factor in this regard.
Generally, the rotation stability with presbyopia correcting toric lenses does not differ significantly from that reported for toric monofocal lenses. The average rotation after an apodized diffractive multifocal toric lens implantation was 2 to 3 degrees at 12 months with 97–98% of eyes having an absolute lens rotation of less than 10 degrees;12 this is similar to or better than results with the toric monofocal lens of the same toric material and design.7 Implantation of another multifocal toric intraocular lens (AT Lisa toric 909M, formerly Acri.Lisa toric 466TD, Carl Zeiss Meditec AG) demonstrated good rotation stability, with an average of 1.5 degrees of overall rotation; 96% of IOLs rotated by 5 degrees or less at 3 and 6 months.13 Marques et al14 examined the results with a Tecnis multifocal toric lens (Tecnis Multifocal Toric ZMT 150–400; Johnson and Johnson Vision, Santa Ana, CA) and noted an average rotation of about 3 degrees at 1 and 6 months; 1.6% (1/60 eyes) required repositioning due to IOL rotation of 12 degrees and 100% had IOL rotation <10 degrees; these results are similar to toric monofocal lens findings with the same material.6,9-11
Results in the current study show a significantly higher percentage of lenses rotating less than 5 degrees than was reported for the same IOL in an earlier, smaller study (97% vs 89% at 3 months). However, the earlier study was based on orientation evaluated using a tomography system. The results are similar to those obtained using slit lamp evaluation in the current study.
The current study demonstrates that the method of evaluation of lens rotation is a significant factor; image analysis showed less variability than slit lamp evaluation measurements. This is not surprising, as several factors can influence slit lamp observation that do not affect image processing (eg, head tilt at the slit lamp, variable cyclotorsion effects). Angular measures using image processing can be performed slowly in a controlled setting – this is not always the case when evaluating IOL orientation at a slit lamp.
There are limitations to the current study. Evaluation of lens orientation at the time of surgery was not a reference point, so rotations occurring on the first day post surgery were not captured (with the exception of those few cases where IOL reorientation was required at Day 1). Because lens stability was the primary concern, lens orientation was not compared to the intended orientation from preoperative calculations. The effects of toric orientation on visual acuity were also not evaluated – visual acuity and refractive results for the study have been published earlier.15
In conclusion, the EDOF intraocular lens here demonstrated stability that exceeded the ANSI standard from 1 Day to 1 month and 3 months postoperative, and between 1 and 3 months. The most precise determination of lens rotation was based on image analysis. Slit lamp evaluation of lens orientation produced results that were significantly more variable than those achieved with image analysis. This resulted in a significantly lower percentage of IOLs being reported as rotating ≤5 degrees for the different time periods analyzed.
Acknowledgments
Sarah Y. Makari, OD is a consultant to Science in Vision who received compensation for writing assistance in preparation of the manuscript. Kiara Down is a third-party consultant who analyzed the toric images. She received compensation for her work. The results reported here were collected at 3 clinical practices (Solomon, Lane, Slade) in the USA.
Disclosure
Helga Sandoval reports grants from Johnson and Johnson Vision, during the conduct of the study. Stephen S. Lane was a consultant to Alcon, B&L, ClarVista, Ivantis, I-Veena, Kala, Mati, Ocular Therapeutix, Omeros, PowerVision, PRN, RPS, Shire, TearScieince, TearLab, VisionCare during the study. He is now Alcon’s CMO and has no other financial interests at the present time. Stephen Slade, MD is a consultant to Alcon, Allotex, Avedro, B&L, CorneaGen, EyeBrain, Eyegate, Glaukos, Johnson and Johnson Vision, LensTec, Occumetrics, Omega Ophthalmics, Presbyopia Therapies RxSight, Surgilum, Zeiss. Eric D. Donnenfeld is a consultant for Acufocus, Allergan, Alcon, AMO, Aquesys, Bausch & Lomb, CRST, Beaver-visitec Elenza, Glaukos, Icon Biosciences, Kala, Katena Lacripen, Mati Pharmaceuticals, Merck, Mimetogen, Novabay, Novaliq, Odyssey, Omega Ophthalmics, Pfizer, Ocuhub, Omeros, PRN, RPS, Shire, Strathspey Crown, Tearlab, TLC Laser Centers, TrueVision, Versant Ventures, and Zeiss. Richard Potvin is a consultant to Alcon Laboratories, and Carl Zeiss Meditec. Kerry D. Solomon is a consultant for Alcon Laboratories, Allergan, Aquesys, Bausch and Lomb, Clarvista Medical, Glaukos, Icon Bioscience, Imprimis, Integrity Digital Solutions, Johnson & Johnson Vision, Kala Pharmaceuticals, Lenstec, Mati Therapeutics, Octane Visionary VC Fund, Ocuhub, Omeros Corporation, Pogotec, PRN, Tearlab, Versuant. The authors report no other conflicts of interest in this work.
References
1. Gundersen KG, Makari S, Ostenstad S, Potvin R. Retreatments after multifocal intraocular lens implantation: an analysis. Clin Ophthalmol. 2016;10:365–371. doi:10.2147/OPTH.S100840
2. Kessel L, Andresen J, Tendal B, Erngaard D, Flesner P, Hjortdal J. Toric intraocular lenses in the correction of astigmatism during cataract surgery: a systematic review and meta-analysis. Ophthalmology. 2016;123:275–286. doi:10.1016/j.ophtha.2015.10.002
3. Tseng SS, Ma JJ. Calculating the optimal rotation of a misaligned toric intraocular lens. J Cataract Refract Surg. 2008;34:1767–1772. doi:10.1016/j.jcrs.2008.05.057
4. American National Standards Institute, Inc. American National Standard for Ophthalmics – Toric Intraocular Lenses. New York, NY: ANSI Z80.30; 2018.
5. Gundersen KG. Rotational stability and visual performance 3 months after bilateral implantation of a new toric extended range of vision intraocular lens. Clin Ophthalmol. 2018;12:1269–1278. doi:10.2147/OPTH.S173120
6. Kasthurirangan S, Feuchter L, Smith P, Nixon D. Software-based evaluation of toric IOL orientation in a multicenter clinical study. J Refract Surg. 2014;30:820–826. doi:10.3928/1081597X-20141117-01
7. Miyake T, Kamiya K, Amano R, Iida Y, Tsunehiro S, Shimizu K. Long-term clinical outcomes of toric intraocular lens implantation in cataract cases with preexisting astigmatism. J Cataract Refract Surg. 2014;40:1654–1660. doi:10.1016/j.jcrs.2014.01.044
8. Zhu X, He W, Zhang K, Lu Y. Factors influencing 1-year rotational stability of AcrySof Toric intraocular lenses. Br J Ophthalmol. 2016;100:263–268. doi:10.1136/bjophthalmol-2015-306656
9. Waltz KL, Featherstone K, Tsai L, Trentacost D. Clinical outcomes of TECNIS toric intraocular lens implantation after cataract removal in patients with corneal astigmatism. Ophthalmology. 2015;122(1):39–47. doi:10.1016/j.ophtha.2014.06.027
10. Jung NY, Lim DH, Hwang SS, Hyun J, Chung TY. Comparison of clinical outcomes of toric intraocular lens, Precizon vs Tecnis: a single center randomized controlled trial. BMC Ophthalmol. 2018;18:292. doi:10.1186/s12886-018-0955-3
11. Miháltz K, Lasta M, Burgmüller M, Vécsei-Marlovits PV, Weingessel B. Comparison of two toric IOLs with different haptic design: optical quality after 1 year. J Ophthalmol. 2018;2018:4064369. doi:10.1155/2018/4064369
12. Lehmann R, Modi S, Fisher B, Michna M, Snyder M. Bilateral implantation of +3.0 D multifocal toric intraocular lenses: results of a US food and drug administration clinical trial. Clin Ophthalmol. 2017;11:1321–1331. doi:10.2147/OPTH.S137413
13. Bellucci R, Bauer NJ, Daya SM, et al., Lisa Toric Study Group. Visual acuity and refraction with a diffractive multifocal toric intraocular lens. J Cataract Refract Surg. 2013;39:1507–1518.
14. Marques EF, Ferreira TB, Simões P. Visual performance and rotational stability of a multifocal toric intraocular lens. J Refract Surg. 2016;32:444–450. doi:10.3928/1081597X-20160502-01
15. Sandoval HP, Lane S, Slade S, Potvin R, Donnenfeld ED, Solomon KD. Visual and refractive clinical outcomes with an extended depth of focus toric intraocular lens targeted for binocular emmetropia or slight myopia in the non-dominant eye. J Cataract Refract Surg. 2019;45:1398–1403. doi:10.1016/j.jcrs.2019.05.019
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.