")
Back to Journals » Drug Design, Development and Therapy » Volume 13
Evaluating guselkumab: an anti-IL-23 antibody for the treatment of plaque psoriasis
Authors Yang EJ , Smith MP , Ly K , Bhutani T
Received 2 December 2018
Accepted for publication 25 February 2019
Published 18 June 2019 Volume 2019:13 Pages 1993—2000
DOI https://doi.org/10.2147/DDDT.S137588
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Cristiana Tanase
Eric J Yang,1,2 Mary Patricia Smith,1,3 Karen Ly,1,4 Tina Bhutani1
1Department of Dermatology, University of California San Francisco, San Francisco, CA, USA; 2Chicago Medical School, Rosalind Franklin University of Medicine and Science, North Chicago, IL, USA; 3Icahn School of Medicine at Mount Sinai, New York, NY, USA; 4School of Medicine, Wayne State University, Detroit, MI, USA
Abstract: The approval of guselkumab marks the entry of the IL-23 inhibitor class into the therapeutic armamentarium for patients with moderate-to-severe plaque psoriasis. This class specifically targets the upstream portion of the type 17 helper T (Th17) axis, which has been implicated as a key driver of the abnormal inflammatory state observed in psoriasis. Guselkumab is highly efficacious, with over 85% of the patients achieving ≥75% reduction in Psoriasis Area and Severity Index from baseline (PASI 75) and over 70% of the patients achieving PASI 90 response in its Phase III clinical trials. Additionally, this medication is well-tolerated, with non-serious infections such as nasopharyngitis and upper respiratory infections (URIs) being the most common adverse events (AEs) reported in its clinical trials. Guselkumab offers yet another effective treatment option in the rapidly growing list of available biological therapies for moderate-to-severe plaque psoriasis.
Keywords: biologics, guselkumab, IL-23 inhibitor, plaque psoriasis, biologic selection
Introduction
Psoriasis vulgaris is a chronic systemic inflammatory disease that affects 2%–3% of the world’s population1,2 and is associated with serious comorbidity, including increased risk for depression,3–5 diminished quality of life,6 psoriatic arthritis,7 metabolic disease,8,9 major adverse cardiac events (MACEs),10,11 and overall increased mortality.12 Patients with mild, localized psoriasis can often be appropriately managed with a topical regimen, but patients with more severe and widespread disease or large quality of life impairment typically require treatment with phototherapy, oral immunosuppressants, or biologic medications. Due to the chronic inflammation observed in this debilitating condition,13–15 systemic therapies are now thought to potentially play an increasingly important role in decreasing the risk of comorbid disease and long-term sequelae associated with moderate-to-severe psoriasis.16–19
Biologic medications currently approved for the treatment of moderate-to-severe plaque psoriasis include tumor necrosis factor alpha (TNF-α) inhibitors (adalimumab, etanercept, infliximab, and certolizumab pegol), IL-17 pathway inhibitors (ixekizumab, brodalumab, and secukinumab), IL-12/23 inhibitors (ustekinumab), and IL-23 inhibitors (guselkumab and tildrakizumab). Therapies targeting IL-23 are the most recent pharmacological development stemming from our rapidly evolving understanding of the immunology of psoriasis, and even more IL-23 inhibitors are currently in the pipeline for approval.20
Methods
A literature search of the MEDLINE health literature database was conducted for the term “guselkumab.” Searches were limited to English-language articles published prior to November 27, 2018. Reference lists of the identified articles were manually searched for additional articles of interest.
Pathophysiology
Although there has been an explosion of novel targeted therapies for psoriasis over the past decade, its complex pathophysiology still remains incompletely characterized. Immune cell populations are increased in psoriatic lesions,21 and serum levels of pro-inflammatory cytokines are elevated in affected patients,22 thus suggesting that immune dysregulation plays a key contributory role in psoriasis. Thus, immunomodulatory therapies remain a mainstay in the treatment of this chronic disease.
Recent advances in the understanding of the pathophysiology of psoriasis have implicated the IL-23/Th17 axis, which contributes to inflammatory bowel disease (IBD) and multiple sclerosis23 and also to be a key contributor to psoriasis. In the current pathophysiological model of psoriasis, pro-inflammatory cytokines, such as IL-1β, IL-6, and TNF-α, activate myeloid dendritic cells, which subsequently release IL-12 and IL-23.24 IL-12 induces differentiation of type 1 helper T (Th1) cells, which secrete pro-inflammatory cytokines TNF-α and IFN-γ, whereas IL-23 induces differentiation of type 17 helper T (Th17) cells, which secrete pro-inflammatory cytokines IL-17A, IL-17F, and IL-22. These cytokines ultimately promote secretion of more pro-inflammatory cytokines by activated keratinocytes, thus creating a positive feedback loop resulting in constitutive inflammation.
Ustekinumab was the first biologic medication targeting the IL-23/Th17 axis approved for the treatment of psoriasis and has subsequently been followed by the approval of several IL-17 inhibitors, all of which have excellent efficacy. IL-23 is a heterodimeric cytokine consisting of a p19 and a p40 subunit,25 and it is implicated as a key driver of Th17 differentiation and proliferation, which contributes to chronic inflammation in psoriasis. Ustekinumab targets the p40 subunit of IL-23, which is shared with IL-12. Although IL-12 was initially thought to be a pathogenic factor contributing to increased immune dysfunction,26,27 animal studies have now indicated that deficiencies in the IL-12 immune response result in worsening of inflammatory disease.28–31 Thus, a need has arisen for an inhibitor specific for IL-23 while sparing the IL-12 immune response, which is now thought to be integral in maintaining normal immunity.
Overview
Guselkumab (CNTO1959; Janssen Research & Development LLC, Spring House, PA, USA) is a fully human IgG1λ monoclonal antibody that binds to the p19 subunit of IL-23. The p19 subunit is also shared with IL-39, whose role in immunity and psoriasis remains largely uncharacterized.32 Guselkumab is FDA approved for the treatment of adults with moderate-to-severe plaque psoriasis who are candidates for systemic therapy or phototherapy.33 This medication is also used currently in clinical trials to investigate its use in hidradenitis suppurativa (NCT03628924), IBD (NCT03662542 and NCT03466411), and psoriatic arthritis (NCT03158285 and NCT03162796).
Practical considerations
The recommended dosing for guselkumab is 100 mg administered subcutaneously at weeks 0, 4, and every 8 weeks thereafter. Guselkumab is supplied as single-use 1 mL prefilled syringes containing a 100 mg dose of the medication, which may be administered by health care professionals or by the patients themselves after initial training of proper injection technique.
Guselkumab has no absolute contraindications, but it should be used with caution in patients with active tuberculosis, chronic infection, or a history of recurrent infections. Patients with a history or symptoms of active tuberculosis or uncontrolled medical conditions or a history of malignancy within the past 5 years (excluding nonmelanoma skin cancer) were excluded from participation in the pivotal Phase III trials.
Routine laboratory monitoring for patients on biologics has been argued not to offer notable benefit,34,35 but is still recommended by all the major professional dermatologic associations.34 However, the specific tests and frequency of monitoring can vary greatly,36 depending on provider experience and comfort by using biological treatments. In general, recommendations for laboratory monitoring for patients on guselkumab and other biological therapies typically consist of screening for tuberculosis infection, hepatitis B and C, and HIV prior to initiating treatment, as well as a complete metabolic panel (CMP) and complete blood count (CBC) at baseline and every 3–12 months thereafter.34,37,38 Patients are advised to avoid the use of live vaccines while being treated with guselkumab, but are recommended to receive other killed and attenuated vaccines as appropriate.33,38
Efficacy
Three pivotal randomized, controlled, double-blind Phase III trials investigated the efficacy of guselkumab in patients with moderate-to-severe plaque psoriasis: VOYAGE-I, VOYAGE-II, and NAVIGATE (Table 1).39–41
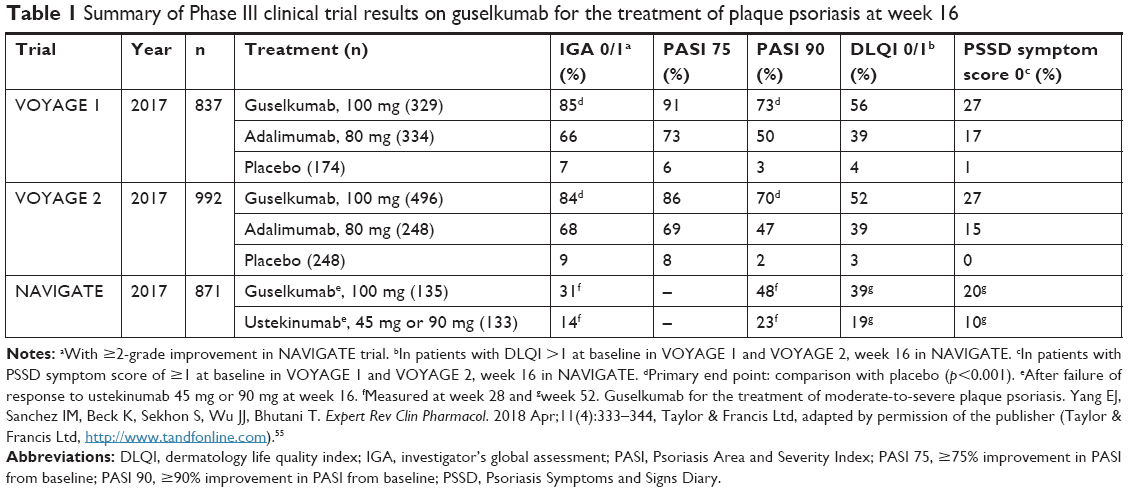 | Table 1 Summary of Phase III clinical trial results on guselkumab for the treatment of plaque psoriasis at week 16 |
Guselkumab was compared with adalimumab and placebo in both VOYAGE-I and VOYAGE-II.39,40 The coprimary efficacy end points in both studies were the proportion of patients treated with guselkumab with a ≥90% reduction in Psoriasis Area and Severity Index from baseline (PASI 90) and Investigator’s Global Assessment (IGA) 0/1 at week 16 compared with placebo. Both trials achieved these coprimary end points, with a greater proportion of patients at week 16 on guselkumab compared to adalimumab or placebo achieving PASI 90 (VOYAGE-I: 73.3% vs 49.7% vs 2.9%, VOYAGE-II: 70.0% vs 46.8% vs 2.4%) and IGA 0/1 (VOYAGE-I: 85.1% vs 65.9% vs 6.9%, VOYAGE-II: 84.1% vs 67.7% vs 8.5%) (p<0.001). High levels of efficacy were maintained with long-term continuous treatment using guselkumab, with 82.1% of the patients achieving PASI 90 and 82.4% achieving IGA 0/1 at week 100 in an extension study of the VOYAGE-I cohort.42
Both studies also demonstrated large improvements in quality of life measures at week 16 in the guselkumab group as compared to the placebo group, as measured by Psoriasis Symptom and Sign Diary (PSSD; VOYAGE-I: −41.9 vs −3.0, VOYAGE-II: −40.4 vs −8.3) and Dermatology Life Quality Index (DLQI; VOYAGE-I: −11.2 vs 0.6, VOYAGE-II: −11.3 vs 2.6) (p<0.001). Additionally, a greater proportion of patients receiving guselkumab with PSSD symptom score ≥1 at baseline achieved a PSSD symptom score of 0 at week 24 as compared to patients receiving adalimumab (VOYAGE-I: 36.3% vs 21.6%, VOYAGE-II: 35.1% vs 22.5%) (p<0.001).
In pooled analyses of both studies, a greater proportion of patients on guselkumab as compared to placebo at week 16 achieved scalp-specific IGA (ss-IGA) 0/1 (81.8% vs 12.4%), Physician’s Global Assessment of the hands and/or feet (hf-PGA) 0/1 (75.5% vs 14.2%), and fingernail PGA (f-PGA) 0/1 (46.7% vs 15.2%) (p<0.001).43 Additionally, more patients treated with guselkumab as compared to adalimumab at week 24 achieved ss-IGA 0/1 (85.0% vs 68.5%) and hf-PGA 0/1 (80.4% vs 60.3%) (p<0.001). However, no difference was appreciated at week 24 between the guselkumab and adalimumab treatment groups in terms of fingernail psoriasis severity as measured by hf-PGA 0/1 (60.0% vs 64.3%) (p=0.11). In a separate study of patients with moderate-to-severe palmoplantar pustulosis (PPP), a greater proportion of patients treated with guselkumab achieved at least 50% reduction in PPP area and severity index (PPPASI 50) as compared to placebo at week 16 (60% vs 21%) (p=0.009).44
VOYAGE-II additionally evaluated the time to loss of PASI 90 response in patients maintained on guselkumab as compared to patients withdrawn from the medication at week 28 of treatment. The median time to loss of PASI 90 response within the withdrawal group was 23 weeks after the last guselkumab dose, whereas the guselkumab group had a greater persistence of response (p<0.001). Through week 48, more patients maintained on guselkumab sustained PASI 90 response as compared to patients in the withdrawal group (88.6% vs 36.9%) (p<0.001).
In the NAVIGATE trial, patients without adequate response to ustekinumab, as measured by IGA ≥2 at week 16, were randomized to treatment with ustekinumab or guselkumab.41 The primary efficacy end point was the number of visits at which patients switched to guselkumab achieved IGA 0/1 and at least a 2-grade improvement from week 28 through week 40 as compared to patients remaining on ustekinumab. Patients switched to guselkumab achieved IGA 0/1 and at least 2-grade improvement at weeks 28–40 for 1.5 visits on average, more than the 0.7 visits observed in patients remaining on ustekinumab (p<0.001). Additionally, patients switched to guselkumab had superior improvement in psoriasis severity as compared to patients maintained on ustekinumab as measured by PASI 90 at week 28 (48.1% vs 22.6%) and week 52 (51.1% vs 24.1%) (p<0.001).
Safety
In its Phase III trials, guselkumab was well-tolerated and has a favorable safety profile for up to 1 year of treatment, without increased risk for serious adverse events (SAEs), malignancies, or MACEs as compared to placebo or other therapies (Table 2). No cases of reactivation of latent tuberculosis or exacerbations or new occurrences of IBD were reported with guselkumab treatment in its Phase III trials. The most common adverse event (AE) experienced with guselkumab was non-serious infections, including nasopharyngitis and upper respiratory infections (URIs).
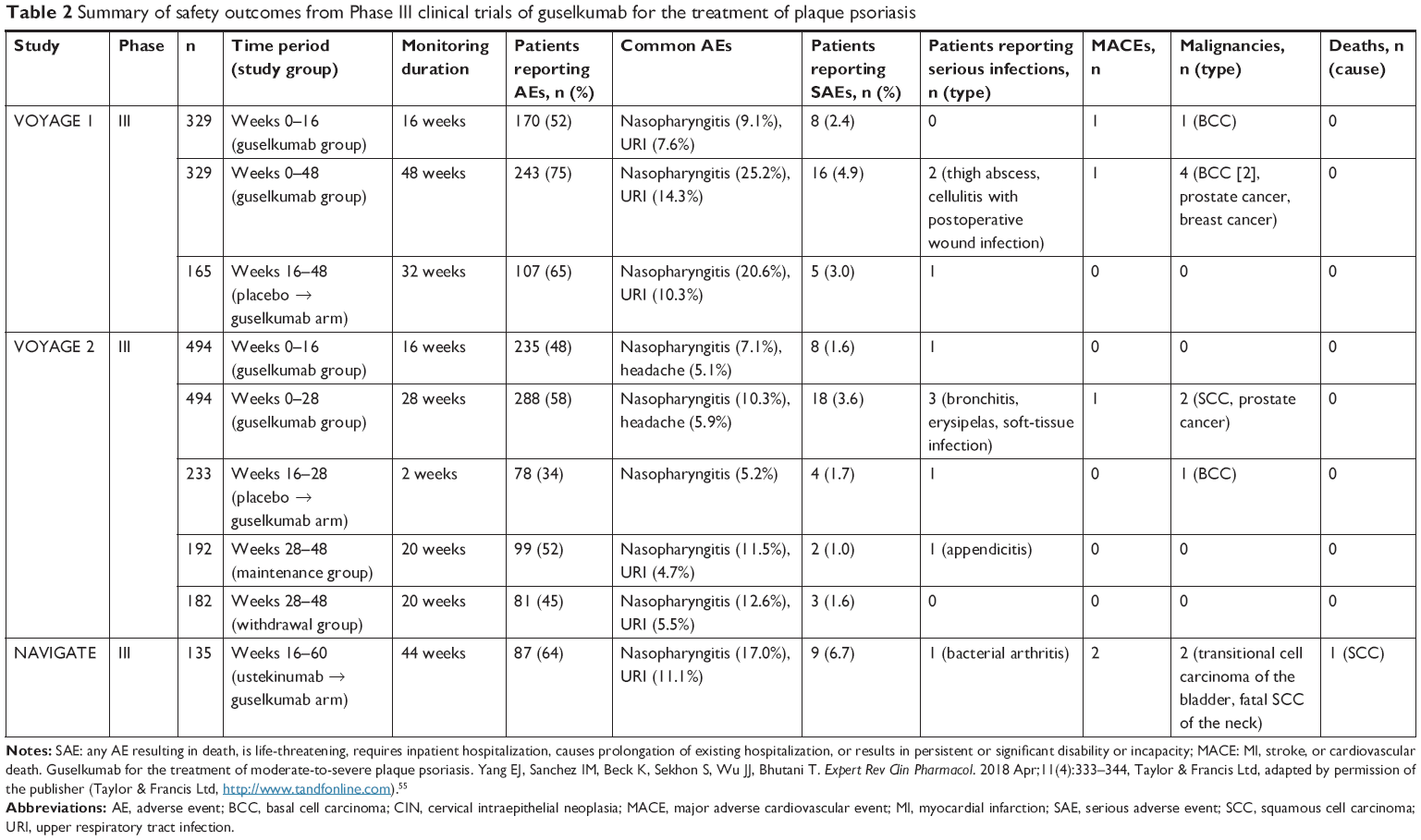 | Table 2 Summary of safety outcomes from Phase III clinical trials of guselkumab for the treatment of plaque psoriasis |
Discussion
Over the past 2 decades, the availability of more effective, safer psoriasis therapies has resulted in a treatment shift from oral immunosuppressants to more targeted biologic and small molecule medications for patients inadequately controlled on a topical regimen or phototherapy. In comparison to methotrexate, biologics have even better efficacy and safety, at least in the short-term, for patients with moderate-to-severe psoriasis. But due to the relative novelty of these medications, the long-term safety profile of IL-17 inhibitors and IL-23 inhibitors is yet to be determined and these safety concerns remain 1 large barrier to widespread adoption of these highly efficacious targeted therapies.45
With so many therapeutic options available for the treatment of psoriasis, dermatologists now have the enviable task of being able to select the optimal biologic for each of their patients. Oral immunosuppressants and TNF-α inhibitors have been used for over 20 years and thus have well-characterized safety profiles that are familiar to many physicians.46,47 However, there are now 3 available biologic classes that can be considered for the treatment of moderate-to-severe psoriasis: IL-12/23 inhibitors, IL-17 inhibitors, and IL-23 inhibitors.
One proposed benefit of the IL-23 inhibitor class over ustekinumab stems from its ability to spare IL-12, a cytokine now increasingly thought of as a key player in normal immunity. The Phase III NAVIGATE trial showed that patients not obtaining PASI 90 response to ustekinumab could receive even greater reduction in severity of their psoriasis by switching to guselkumab, as compared to staying on ustekinumab treatment. However, larger head-to-head studies comparing the efficacy and safety of IL-23 inhibitors against IL-12/23 inhibitors are still lacking. Although this observed benefit may occur secondary to guselkumab’s ability to spare IL-12, it is widely thought that other factors may be contributing to this effect, such as increased frequency of dosing and tighter binding affinity for IL-23. Nevertheless, the unique study design of the NAVIGATE trial demonstrates that guselkumab is a suitable option for patients not obtaining adequate response to ustekinumab. In contrast, ustekinumab is already approved for the treatment of psoriatic arthritis in adults, as well as plaque psoriasis in adolescents 12 years or older, populations still being investigated for guselkumab.48 Ustekinumab is also dosed every 12 months and thus may be a preferable option for patients reluctant to obtain injections or who have difficulties with medication compliance.
In comparison to IL-17 inhibitors, guselkumab offers similarly high PASI responses (Table 3), while offering a few practical and safety advantages. IL-17 inhibitors have a warning for use in patients with IBD,49 as clinical trials have demonstrated both new cases and exacerbations of IBD with IL-17 inhibition.50,51 However, no Phase III clinical trials to date for IL-23 inhibitors have shown an increased risk of IBD. IL-23 inhibitors also have not been associated with an increased risk of Candida infections, which have been reported with use of IL-17 inhibitors.52 From a practicality standpoint, brodalumab also has a black box warning for suicidal ideation and behavior,49 and although it is unlikely that brodalumab causes these adverse effects,53 IL-23 inhibitors have no such black box warning that is required to be discussed with patients prior to initiating therapy. Thus, patients concerned about the possible safety risks of biologics may be more amenable to starting on guselkumab or other IL-23 inhibitors than brodalumab. Finally, guselkumab is dosed every 8 weeks, far less frequently than IL-17 inhibitors, which require injections every 2–4 weeks (Table 3).
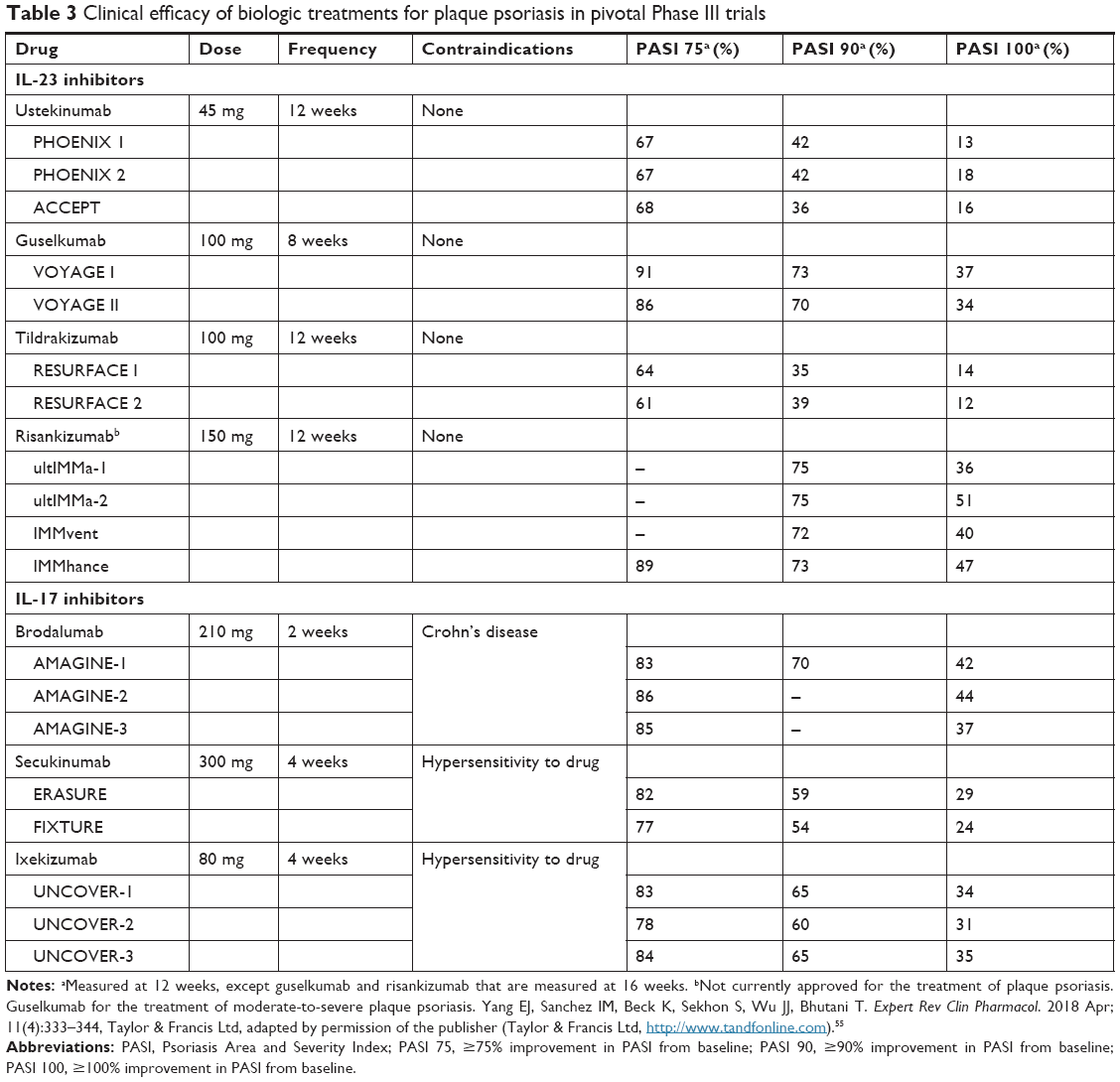 | Table 3 Clinical efficacy of biologic treatments for plaque psoriasis in pivotal Phase III trials |
Guselkumab is the first IL-23 inhibitor approved for the treatment of plaque psoriasis, a class that is likely to comprise a larger portion of the biologics market for psoriasis, with the recent approval of tildrakizumab and the likely approval of risankizumab in the near future. Guselkumab has superior efficacy in its Phase III trials VOYAGE-I and VOYAGE-II as compared to adalimumab, a commonly used potent biologic therapy for moderate-to-severe psoriasis patients. Additionally, guselkumab also has excellent efficacy in treating psoriasis in difficult-to-treat areas, such as the scalp, palms and soles, and fingernails. Importantly, these clinical trials demonstrate that guselkumab markedly improves quality of life in psoriasis patients, which is becoming an increasingly important consideration in treatment selection for this debilitating condition.54
As the scientific understanding of the pathophysiology of psoriasis continues to expand, dermatologists will have an increasing ability to deliver very specifically targeted therapy for their patients with moderate-to-severe psoriasis. Guselkumab appears to be a highly efficacious treatment with a favorable short-term safety profile, but data beyond 2 years of treatment with this newly approved medication are lacking. The role of guselkumab, as well as other IL-23 inhibitors, in the psoriasis therapeutic stepladder will continue to be clarified as more long-term safety data are collected for these medications.
Disclosure
T Bhutani is an investigator for AbbVie, Janssen, Merck, Eli Lilly, and Strata Skin Sciences and an advisor for Regeneron. The other authors report no conflicts of interest in this work.
References
Parisi R, Symmons DP, Griffiths CE, Ashcroft DM; Identification and Management of Psoriasis and Associated ComorbidiTy (IMPACT) project team. Global epidemiology of psoriasis: a systematic review of incidence and prevalence. J Invest Dermatol. 2013;133(2):377–385. doi:10.1038/jid.2012.339 | ||
Rachakonda TD, Schupp CW, Armstrong AW. Psoriasis prevalence among adults in the United States. J Am Acad Dermatol. 2014;70(3):512–516. doi:10.1016/j.jaad.2013.11.013 | ||
Gupta MA, Schork NJ, Gupta AK, Kirkby S, Ellis CN. Suicidal ideation in psoriasis. Int J Dermatol. 1993;32(3):188–190. | ||
Kurd SK, Troxel AB, Crits-Christoph P, Gelfand JM. The risk of depression, anxiety, and suicidality in patients with psoriasis: a population-based cohort study. Arch Dermatol. 2010;146(8):891–895. doi:10.1001/archdermatol.2010.186 | ||
Dowlatshahi EA, Wakkee M, Arends LR, Nijsten T. The prevalence and odds of depressive symptoms and clinical depression in psoriasis patients: a systematic review and meta-analysis. J Invest Dermatol. 2014;134(6):1542–1551. doi:10.1038/jid.2013.508 | ||
Rapp SR, Feldman SR, Exum ML, Fleischer AB Jr, Reboussin DM. Psoriasis causes as much disability as other major medical diseases. J Am Acad Dermatol. 1999;41(3 Pt 1):401–407. | ||
Villani AP, Rouzaud M, Sevrain M, et al. Prevalence of undiagnosed psoriatic arthritis among psoriasis patients: systematic review and meta-analysis. J Am Acad Dermatol. 2015;73(2):242–248. doi:10.1016/j.jaad.2015.05.001 | ||
Yeung H, Takeshita J, Mehta NN, et al. Psoriasis severity and the prevalence of major medical comorbidity: a population-based study. JAMA Dermatol. 2013;149(10):1173–1179. doi:10.1001/jamadermatol.2013.5015 | ||
Langan SM, Seminara NM, Shin DB, et al. Prevalence of metabolic syndrome in patients with psoriasis: a population-based study in the United Kingdom. J Invest Dermatol. 2012;132(3 Pt 1):556–562. doi:10.1038/jid.2011.365 | ||
Mehta NN, Azfar RS, Shin DB, Neimann AL, Troxel AB, Gelfand JM. Patients with severe psoriasis are at increased risk of cardiovascular mortality: cohort study using the General Practice Research Database. Eur Heart J. 2010;31(8):1000–1006. doi:10.1093/eurheartj/ehp567 | ||
Gelfand JM, Neimann AL, Shin DB, Wang X, Margolis DJ, Troxel AB. Risk of myocardial infarction in patients with psoriasis. JAMA. 2006;296(14):1735–1741. doi:10.1001/jama.296.14.1735 | ||
Gelfand JM, Troxel AB, Lewis JD, et al. The risk of mortality in patients with psoriasis: results from a population-based study. Arch Dermatol. 2007;143(12):1493–1499. doi:10.1001/archderm.143.12.1493 | ||
Joshi AA, Lerman JB, Dey AK, et al. Association between aortic vascular inflammation and coronary artery plaque characteristics in psoriasis. JAMA Cardiol. 2018;3(10):949–956. doi:10.1001/jamacardio.2018.2769 | ||
Mehta NN, Yu Y, Saboury B, et al. Systemic and vascular inflammation in patients with moderate to severe psoriasis as measured by [18F]-fluorodeoxyglucose positron emission tomography-computed tomography (FDG-PET/CT): a pilot study. Arch Dermatol. 2011;147(9):1031–1039. doi:10.1001/archdermatol.2011.119 | ||
Mehta NN, Torigian DA, Gelfand JM, Saboury B, Alavi A. Quantification of atherosclerotic plaque activity and vascular inflammation using [18-F] fluorodeoxyglucose positron emission tomography/computed tomography (FDG-PET/CT). J Vis Exp. 2012;63:e3777. | ||
Bhutani T, Patel T, Koo B, Nguyen T, Hong J, Koo J. A prospective, interventional assessment of psoriasis quality of life using a nonskin-specific validated instrument that allows comparison with other major medical conditions. J Am Acad Dermatol. 2013;69(2):e79–e88. doi:10.1016/j.jaad.2012.10.009 | ||
Gelfand JM. Does biologic treatment of psoriasis lower the risk of cardiovascular events and mortality?: a critical question that we are only just beginning to answer. J Am Acad Dermatol. 2018;79(1):69–70. doi:10.1016/j.jaad.2018.03.046 | ||
Wu JJ, Sundaram M, Cloutier M, et al. The risk of cardiovascular events in psoriasis patients treated with tumor necrosis factor-alpha inhibitors versus phototherapy: an observational cohort study. J Am Acad Dermatol. 2018;79(1):60–68. | ||
Mehta NN, Shin DB, Joshi AA, et al. Effect of 2 psoriasis treatments on vascular inflammation and novel inflammatory cardiovascular biomarkers: a randomized placebo-controlled trial. Circ Cardiovasc Imaging. 2018;11(6):e007394. doi:10.1161/CIRCIMAGING.117.007394 | ||
Papp KA, Blauvelt A, Bukhalo M, et al. Risankizumab versus ustekinumab for moderate-to-severe plaque psoriasis. N Engl J Med. 2017;376(16):1551–1560. doi:10.1056/NEJMoa1607017 | ||
Bos JD, Hulsebosch HJ, Krieg SR, Bakker PM, Cormane RH. Immunocompetent cells in psoriasis. In situ immunophenotyping by monoclonal antibodies. Arch Dermatol Res. 1983;275(3):181–189. | ||
Arican O, Aral M, Sasmaz S, Ciragil P. Serum levels of TNF-alpha, IFN-gamma, IL-6, IL-8, IL-12, IL-17, and IL-18 in patients with active psoriasis and correlation with disease severity. Mediators Inflamm. 2005;2005(5):273–279. doi:10.1155/MI.2005.273 | ||
Iwakura Y, Ishigame H. The IL-23/IL-17 axis in inflammation. J Clin Invest. 2006;116(5):1218–1222. doi:10.1172/JCI28508 | ||
Nestle FO, Kaplan DH, Barker J. Psoriasis. N Engl J Med. 2009;361(5):496–509. doi:10.1056/NEJMra0804595 | ||
Oppmann B, Lesley R, Blom B, et al. Novel p19 protein engages IL-12p40 to form a cytokine, IL-23, with biological activities similar as well as distinct from IL-12. Immunity. 2000;13(5):715–725. | ||
McIntyre KW, Shuster DJ, Gillooly KM, et al. Reduced incidence and severity of collagen-induced arthritis in interleukin-12-deficient mice. Eur J Immunol. 1996;26(12):2933–2938. doi:10.1002/eji.1830261219 | ||
Neurath MF, Fuss I, Kelsall BL, Stuber E, Strober W. Antibodies to interleukin 12 abrogate established experimental colitis in mice. J Exp Med. 1995;182(5):1281–1290. | ||
Chu CQ, Wittmer S, Dalton DK. Failure to suppress the expansion of the activated CD4 T cell population in interferon gamma-deficient mice leads to exacerbation of experimental autoimmune encephalomyelitis. J Exp Med. 2000;192(1):123–128. | ||
Ferber IA, Brocke S, Taylor-Edwards C, et al. Mice with a disrupted IFN-gamma gene are susceptible to the induction of experimental autoimmune encephalomyelitis (EAE). J Immunol. 1996;156(1):5–7. | ||
Vermeire K, Heremans H, Vandeputte M, Huang S, Billiau A, Matthys P. Accelerated collagen-induced arthritis in IFN-gamma receptor-deficient mice. J Immunol. 1997;158(11):5507–5513. | ||
Bettelli E, Sullivan B, Szabo SJ, Sobel RA, Glimcher LH, Kuchroo VK. Loss of T-bet, but not STAT1, prevents the development of experimental autoimmune encephalomyelitis. J Exp Med. 2004;200(1):79–87. doi:10.1084/jem.20031819 | ||
Wang X, Wei Y, Xiao H, et al. A novel IL-23p19/Ebi3 (IL-39) cytokine mediates inflammation in Lupus-like mice. Eur J Immunol. 2016;46(6):1343–1350. doi:10.1002/eji.201546095 | ||
TREMFYA (guselkumab) [package insert]. Horsham (PA): Janssen Biotech Inc; 2017. | ||
Ahn CS, Dothard EH, Garner ML, Feldman SR, Huang WW. To test or not to test? An updated evidence-based assessment of the value of screening and monitoring tests when using systemic biologic agents to treat psoriasis and psoriatic arthritis. J Am Acad Dermatol. 2015;73(3):420–428.e1. doi:10.1016/j.jaad.2015.06.004 | ||
Hoffmann JH, Knoop C, Enk AH, Hadaschik EN. Routine laboratory parameter dynamics and laboratory adverse events in psoriasis patients on long-term treatment with adalimumab, etanercept, and ustekinumab. Acta Derm Venereol. 2017;97(6):705–710. doi:10.2340/00015555-2644 | ||
Halverstam CP, Lebwohl M. Practical management and monitoring of psoriasis in patients on biologic therapy. Psoriasis Forum. 2007;13:2. | ||
Nast A, Gisondi P, Ormerod AD, et al. European S3-guidelines on the systemic treatment of psoriasis vulgaris–update 2015–short version–EDF in cooperation with EADV and IPC. J Eur Acad Dermatol Venereol. 2015;29(12):2277–2294. doi:10.1111/jdv.13354 | ||
Lebwohl M, Bagel J, Gelfand JM, et al. From the Medical Board of the National Psoriasis Foundation: monitoring and vaccinations in patients treated with biologics for psoriasis. J Am Acad Dermatol. 2008;58(1):94–105. doi:10.1016/j.jaad.2007.08.030 | ||
Blauvelt A, Papp KA, Griffiths CE, et al. Efficacy and safety of guselkumab, an anti-interleukin-23 monoclonal antibody, compared with adalimumab for the continuous treatment of patients with moderate to severe psoriasis: results from the phase III, double-blinded, placebo- and active comparator-controlled VOYAGE 1 trial. J Am Acad Dermatol. 2017;76(3):405–417. doi:10.1016/j.jaad.2016.11.041 | ||
Reich K, Armstrong AW, Foley P, et al. Efficacy and safety of guselkumab, an anti-interleukin-23 monoclonal antibody, compared with adalimumab for the treatment of patients with moderate to severe psoriasis with randomized withdrawal and retreatment: results from the phase III, double-blind, placebo- and active comparator-controlled VOYAGE 2 trial. J Am Acad Dermatol. 2017;76(3):418–431. doi:10.1016/j.jaad.2016.11.042 | ||
Langley RG, Tsai TF, Flavin S, et al. Efficacy and safety of guselkumab in patients with psoriasis who have an inadequate response to ustekinumab: results of the randomized, double-blind, phase III NAVIGATE trial. Br J Dermatol. 2017;178(1):114–123. | ||
Griffiths CEM, Papp KA, Kimball AB, et al. Long-term efficacy of guselkumab for the treatment of moderate-to-severe psoriasis: results from the Phase 3 VOYAGE 1 trial through two years. J Drugs Dermatol. 2018;17(8):826–832. | ||
Foley P, Gordon K, Griffiths CEM, et al. Efficacy of guselkumab compared with adalimumab and placebo for psoriasis in specific body regions: a secondary analysis of 2 randomized clinical trials. JAMA Dermatol. 2018;154(6):676–683. doi:10.1001/jamadermatol.2018.0793 | ||
Terui T, Kobayashi S, Okubo Y, Murakami M, Hirose K, Kubo H. Efficacy and safety of guselkumab, an anti-interleukin 23 monoclonal antibody, for palmoplantar pustulosis: a randomized clinical trial. JAMA Dermatol. 2018;154(3):309–316. doi:10.1001/jamadermatol.2017.5937 | ||
van de Kerkhof PC, Reich K, Kavanaugh A, et al. Physician perspectives in the management of psoriasis and psoriatic arthritis: results from the population-based Multinational Assessment of Psoriasis and Psoriatic Arthritis survey. J Eur Acad Dermatol Venereol. 2015;29(10):2002–2010. doi:10.1111/jdv.13150 | ||
Menter A, Thaci D, Wu JJ, et al. Long-term safety and effectiveness of adalimumab for moderate to severe psoriasis: results from 7-year interim analysis of the ESPRIT registry. Dermatol Ther (Heidelb). 2017;7(3):365–381. doi:10.1007/s13555-017-0198-x | ||
Strober B, Crowley J, Langley RG, et al. Systematic review of the real-world evidence of adalimumab safety in psoriasis registries. J Eur Acad Dermatol Venereol. 2018;32:2126–2133. doi:10.1111/jdv.2018.32.issue-12 | ||
STELARA (ustekinumab) [package insert]. Horsham (PA): Janssen Biotech Inc; 2016. | ||
SILIQ (brodalumab) [package insert]. Bridgewater (NJ): Valeant Pharmaceuticals; 2017. | ||
Lebwohl M, Strober B, Menter A, et al. Phase 3 studies comparing brodalumab with ustekinumab in psoriasis. N Engl J Med. 2015;373(14):1318–1328. doi:10.1056/NEJMoa1503824 | ||
Gordon KB, Blauvelt A, Papp KA, et al; UNCOVER-1 Study Group; UNCOVER-2 Study Group; UNCOVER-3 Study Group. Phase 3 trials of ixekizumab in moderate-to-severe plaque psoriasis. N Engl J Med. 2016;375(4):345–356. doi:10.1056/NEJMoa1512711 | ||
Conti HR, Gaffen SL. IL-17-mediated immunity to the opportunistic fungal pathogen candida albicans. J Immunol. 2015;195(3):780–788. doi:10.4049/jimmunol.1500909 | ||
Lebwohl MG, Papp KA, Marangell LB, et al. Psychiatric adverse events during treatment with brodalumab: analysis of psoriasis clinical trials. J Am Acad Dermatol. 2018;78(1):81–89.e85. doi:10.1016/j.jaad.2017.08.024 | ||
Mrowietz U, Kragballe K, Reich K, et al. Definition of treatment goals for moderate to severe psoriasis: a European consensus. Arch Dermatol Res. 2011;303(1):1–10. doi:10.1007/s00403-010-1080-1 | ||
Yang EJ, Sanchez IM, Beck K, Sekhon S, Wu JJ, Bhutani T. Guselkumab for the treatment of moderate-to-severe plaque psoriasis. Expert Rev Clin Pharmacol. 2018;11(4):333–344. doi:10.1080/17512433.2018.1445967 |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.